Embed Size (px)
Citation preview
DOCU ENT RESUUE
40 036 CE 011 327
TITLE Nursing Education LI High Blood Pressure Control.Report:of the Task Force on the Role of Nursing inHigh Blood.Pressure ControL.-
-NSTITUTION National InstitUtes of Health (DREW), Bethesda, Hd.High' Blood- PresSure Information Center.
SpONSAGENCY Public-Health Service, (DHBW), Washington, D.C.,HE.PORTA0 DHET-NIH-76-1082
._.TUBLATE (76)Ai0T2-: 4.21).
apRs PRICE.1)ESCRIPTORS
ABSTR1CT-
P-$0.8 HC-$2.06 Plus PoStage.Attitudes; *Behavioral Oblectives; ClinicalDiagnosis; Guidelines; Health Education;*HyperienSion; *Job Skills; Medical Services;*Nursing;-*Professional Education; StudentEvaluation; Task Performance;.Teaching Guides;Teaching Methods
This curriculum guide on,high blood pressure(hypertension) for nursing educators has five sections: (1)
-Introduction and Objectives provides information regarding the-eStablishment and objectives of the. 'National Task Force on-,the Role-of;Nursing.in High-Blood Pressure Control and 'briefly-discusses.Aluising!S role -in- hypertension control; (2) Goals for UndetectedjltpertenSive-PopulationS presents ouidelines for use in nursingAeneric,:graduate, practitioner, and continuing education progras on"theHletection of high blood -pressure and inclddes One primary goal,fOur, secondary goals, and nine.behavioral dbjectiveS,.,each. having one1-.6:fifteen subobjectives regarding performance Skills,' cognitive
an4 attitudes; (3) ratient OutcoMeS_for.Detected HypertenSive_ PopUlationS covers-guidelines for.use in the aforementioned nursing-,-eduCational programS- on the careof,patients.with detected. .
hYp4itenAion and inCludes 7 patient.- outCoMe.goals related, to either_Mit4Wizing 'disruption of health status or promotion,of health and 70behaVioral-ohjective8, some, having-one to nine subobjectivesdeliheating..-ntrse.performanCe :skills, cognitive skills, andAttitude's.: 14). .Achieving Objectives .briefly:disCusses approaches forlisingtheiguide -in planning contentrteaching:thethods,. and learningexperiences, .evaluating nurse competende,'-and identifying learning--need.at:Amd. (5). nursing .Per'spectiventhe.,Carrent State of .Knowledge:AUfaiiiii*es:SomecUrrent views on hypertenSion management salient for,nArsing-practica, A list of 56 references-ls Appended. (EH)
4***************************************************-** *..1[4,60ents- acquired by ERIC indlude'many informal unpublished
_materialsnot available from other-sources, amc makeA every effortAbOobtain.the-best aopy ayailable: Nevertheless, items of marginal
repr*incibility-'ate often encountered and-this- affects'.the quality;àf .'-=tW4iciCfiche, and hardcopy-reproductions ERIC makes available
*.:Via.;ithe-.-ERIC Document Reproduction Service (EDRS)..EDRS is 'notreAponsibleyfor the guality_of the original document. Reproductions *$11-ppiledTby--EDRS -ate the best that can-be.made from the original.
NursingEducation
in High BloodPressureControlReport of the
Task Force on theRole of Nursing in
High BloodPressure Control
Sponsored by:National High Blood Pressure Education Program,
National Heart, Lung, and Blood institute
American Heart AssociationAmerican Nurses' Association
National League tor NursingNational Student Nurses Association
U.S. DEPARTMENT OF HEALTH,EDUCKRON. AND WELFARE
Public Health ServiceNational Institutes Oi Health
DHEW Publication No. (NIH) 76-1052.
U.S. DEPARTMENT OF HEALTHEDUCATION & WELFARENATIONAL INSTITUTE OF
EDUCATIONTHIS DOCUMENT HAS BEEN REPRODIKED EXACTLY AS RECEIVED FROMTHE PERSON OR ORGANIZATION ORIGINATING IT, POINTS OF VIEW OR OPINIONSSTATED DO NOT NECESSAR!LY REPRE:SENT OFFICIAL NA DONAL INSTITUTE OFEDUCATION POSITION OR POLICY
TABLE OF CONTENTS
Task Force Membership
Introduction and Objectives
Goals for Undetected HypertensivePopulations
Patient Outcomes for DetectedHypertensive Populations
4
13
Achieving Object ves 23
Nursing Perspectives on the CurrentState of Knowledge 26
References 32
1
TASK FO CE MEMBERSHIP
Elizabeth C. Giblin, R.N., Ed.D. (Chairperson)American Nursing AssociationProfessor of Physiological NursingSchool of NursingUniversity of WashingtonSeattle, Washington
Anne M. Ackerman, R.N., MClinical Specialist in CardiovascularNursing
George Washington University HospitalWashington, D.C.
Mary Ann Anderson, R.N., M.S.Assistant DeanCollege of NursingHoward UniversityWashington, D.C.
Grace E. Brown, R.N.,B.S .A.
ChairpersonCouncil on Cardiovascular NursingAmerican Heart AssociationRiverdale, New York
Sheila P. Burke, R.N.,B.S.N.Student Affairs DirectorNational Student Nurses AssociationNew York, New York
Mary Ann Christ, R.N.,Clinician II/InstructorSchool of NursingUniversity of _RochesterRochester, New York
Josephine M. Jones, R.N.,M.P.H.Nurse Therapist and CoordinatorNursing Management of Hypertensi nWorkshop
Atlanta Hypertension Detection andFollow-up Program, Atlanta, Georgia
Susan Leddy, R.N., Ph.D.ConsultantNursing EducationNational League for N singNew York, New York
2
Patricia M. MacElveen, R.N.,Ph.D.Assistant Professortepartment of Psychosocial NursingUniversity of WashingtonSeattle, Washington
Nova Jane McCombs' R.N.ChiefHealth Care Education UnitAdult Health SectionGeorgia Department of Human ResourcesAtlanta, Georgia
Harriet C. Moidel, R.N., M.A.Professor, School of NursingUniversity of CaliforniaLos Angeles, California
Marjorie M. Ragan, R.N.,M.S.N.Clinical Specialist in HypertensionVeterans Administration HospitalWashington, D.C.
Kathleen A. Ritchey R.N.,M.S.N.Cardiovascular Clinical Nurse SpecialistVeterana Administration HospitalWashington, D.C.
Alice M. Robinson, R.N. M.S."DirectorSpecialized Consultants in NursingNew York, New York
Margaret A. Williams, R.N.,Ph.D.Project CoordinatorNursing Activity and Utilization Study-San Joaquin General HospitalStockton, California
Alice M. McGill, R.N.,Ph.D. (Consultant)CoordinatorPrevention Control and Education
ProgramaNational Heart, Lung,and Blood instituteNational Institutes of HealthBethesda, Maryland
INTRODUCTI N AND OBJECTIVES
Since its establishment in 1972. tL National HighBlood Pressure Education Program coordinated by theNational Heart, Lung, and Blood Institute has been spon-soring large scale efforts to raise the awareness ofhealth professionals and the public regarding the magni-tude of the high blood pressure problem in this country,and the need to mobilize the resources of the healthprofessions including allied health personnel to facili-tate detection and control. Groundwork for these effortswas provided by four task forces that provided the database related to the detection, diagnosis, and the treat-ment.of hypertension; established recommendations forpUblic and professional education; studied the availableresources; and assessed Program impact on the problem.In Addition, guidelines for medical education were de-veloped by the Working Group on the Training andEvaluation of Physicians in High Blood Pressure. (1-5)During 1975, the Task Force on the Role of Nursing inHigh Blood Pressure Control was formed to review the roleof nursing and the educational preparation necessary toimpact this major public health problem.
As the largest health professional group in theUnited States, nurses are an invaluable resource notonly in terms of numbers, but also in terns of theirpresent and potential skills in screening and deliver-ing health care services to the over 23 million peoplewith high blood pressure needing control. Since nursesprovide the greatest percentage of direct care given toconsumers they have frequent opportunities for casefinding, for educating consumers to maximize participation in their own health care management, and for as-suring follow-up and continuity of care. (1, 2, 3, 4)
With the current demands on the health care sys-tem and serious resource distribution problems, anactive and expanded scope of involvement on the partof nurses is essential to the control of hypertension.(9, 6, 13) Through their varied sites of practicewithin hospitals, community health facilities, schools,nursing homes, industrjes, physicians' offices andclinics, nurses have access to large numbers of personsof all ages. The potential for their contribution topublic education, detection, and control of high bloodpressure must be operationalized.
Realization of this potential requires that: (1)
high blood pressure_be given greater emphasis withinthe generic and graduate nursing school curriculum;(2) nurses in practice be reached by continuing educa-
6
.tionefforts related to hypertension; -(3). -more nurses-becomehypertension nursing Specialists-and functionas:prinery. care agents for those persons with uncom-plicated-hypertension; and (4) more nurses take part'inresearch efforts related to care of hypertensiveii6rions'.-
.Some.nurses have been involved in detection and,iongterm management of patients with high bloodlpresSure in the community, in industry, and in clinics.Nurtes-. have been successful in achieving control oftbloOd:pressure,-adherence to the medical regtmen, and-reduction in dropouts; and cost efficiency has been,Outstanding in comparison to previous delivery ap--proaches. (6, 7, 9, 10, 11, 12)
-The identification of knowledge, behaviors, and,SkiliS necessary in the care of individuals with high'blood pressure is essential in order that such infor-nation becomes a part_of both basic nursing educationand-continuing education. In turn, public education
:.and-patient teaching will be better served. Nurses--have traditionally affirmed their role in personal andfaMily support in time of illness. The Task Force sees--this role- as continuing to be of high importance intheir.:contacts with persons with this long-term dis-Order, the treatment of which requires the person toH4dhere to regimens that may occasionally be irksome,that can cause unpleasant side effects, that can re--:Sult in-Substantial. monetary expenditure, and that can'affect life style. Skills in empathic Support, teach-ingiand motivation nay be called-on-to a high degreein:the latter sittations.
i The. Task Force on the Role of Nursing in High BloodPreSsure _Control was charged with developing behavioralObjectives to guide nursing,education and practice inthe detection, evaluation, and management of hyperten-SiVe -patients. The Task Force envisioned the use of.thSp-objectives in basid, advanced, and continuing_duCation'programs.
.The following were the working objectives of the-Taak,:torce: .
Define the scope of nursing in high blood es-_ure control.
Define behavioral_objectives including nursing-performance, cognitive skills, and attitudes in..relation to specified patient outcomes.
Consider educational methOdologies and instruc-tional techniques that nay be used to achievethe objectives.
7
Consider evaluation processes to determineachievement of objectives.
In.preparing this report, the Task Force reflectedthe basic philosophical positions of nursiAg. (8, 14)
Nursing practice has traditionally been dedicatedto the promotion,- maintenance, and restoration of healthfor all persons. Nurses have upheld the right of every-one to have access to health care without regard to age,sex, race, ethnicity, or socioeconomic status.
The magnitude and lifelong problem of hypertensiondemands the utilization of a collaborative health teameffort. The patient and family are an integral part ofthe health team and have the right to informationnecessary for knowledgeable participation in planningand decision making. The understanding of high bloodpressure and its control is important in the success of
a treatment program.
Nurses can play a majorrole in assisting patientsto adapt to the demands of lifelong treatment. Thenursing perspective of health care considers the in-dividual within the framework of a total person who isa meMber of a family and a community, and whose responsesto high blood pressure and its management are influencedby social-psycho/physiological needs. The patient hasthe right to in&vidually determane personal quality oflife. Increasing the patient's knowledge supports theopportunities for the individual to make informed de-cisiohs about health and illness. Maxim= physicalwell-being as defined by the health professional maynot be totally compatible with life style needs asidentified by the, patient. The core of nursing practiceis in assisting persons to achieve their highest poten-tial for healthfulness by the continuous assessment andpromotion of the health status and health assets.
Nurses are responsible for assisting the consumerto use the health care system and community resourcesby providing information assistance on referral. Con-tinuity of care and follow-up are essential in the long-term management of high blood pressure.
Nurses in all practice settings have opportunitiesfor detection of high blood pressure. With advancedpreparation and the use of medical guidelines, thenurse can assume major responsibilities in detectionprograms and in the primary care of those with highblood pressure. Nurses are responsible for affectingthe formulation of health policies, legislation, andprograms for those with long-term health problems.
6' 8
Nurses are also responsible for conducting researchdesigned to increase the knowledge base for nursing in-terventions. In addition, research is needed to investi-gate models for delivering nursing care to improve con-sumer satisfaction, and to insure long-term adherence tohealth regimens.
Basic knowledge is the foundation of competentnursing practice. The curriculum guidelines offered inthis report are for nursing education on hypertension.The attitudes, cognitive and performance skills explicat-ed are requisite to the preparation of all nurses if they-are to meet their obligations in responding to the pro-blem of high blood pressure. The model for nursing'scontribution to the control of high blood pressure out-lined in this report has been predicated on the basisof consumer needs and objectives and on the present stateof the art of treatment.
7
GOALS FOR UNDETECTED HYPERTENSIVE.POPULATIONS
The Task Force developed the following guidelinesfor use-in generic, graduate, and practitioner educa-tional programs as well as for continuing education,'including in-service programs. The objectives wereformulated to facilitate pretesting of cognitive andperformance skills, selecting content and teachingmethods, and evaluating learning outcomes. It wasanticipated that the objectives could also serve as abasis for developing standards, criteria, and norms foruse in peer revieW and quality care assessments.
The Task Force elected to develop the guidelinesfor instruction on the detection of high blood pressureapart from those for the care of the individual withdetected high blood pressureL This was done in orderto focus on the outcome goals for these two populations.The reader will need to use both sets of guidelines forthe details .deStribing the performance skills used forboth populations. These were purposefully not-repeated.
The Task Force reviewed the three areas consideredessential for facilitating detection of high blood pres-sure. These include: (1) consumers (the general public)informed of the importance of risk factors, early diag-nosis, and adequate long-term management; (2) measure-ment in the health care setting, organized detectionprograms including follow-up; and (3) referral sources.All nurses can assist with public education and withscreening. When participating in mass screening pro-grams nurses should make sure that referral sources areavailable. Nurse practitioners with advanced trainingcan provide the follow-up, diagnostic, and managementservices for referrals from screening programs.
The Task Force focused on the gdals and resourcesneeded for early detection of high bidod pressure as abasis for delineating the performance skills and therelated cognitive skills and attitudes for the guide-lines. -(49, 51, 53)
In the following outline it should be noted thatthe special skills expected of the nurse with advancedtraining are noted by an asterisk( ).
8
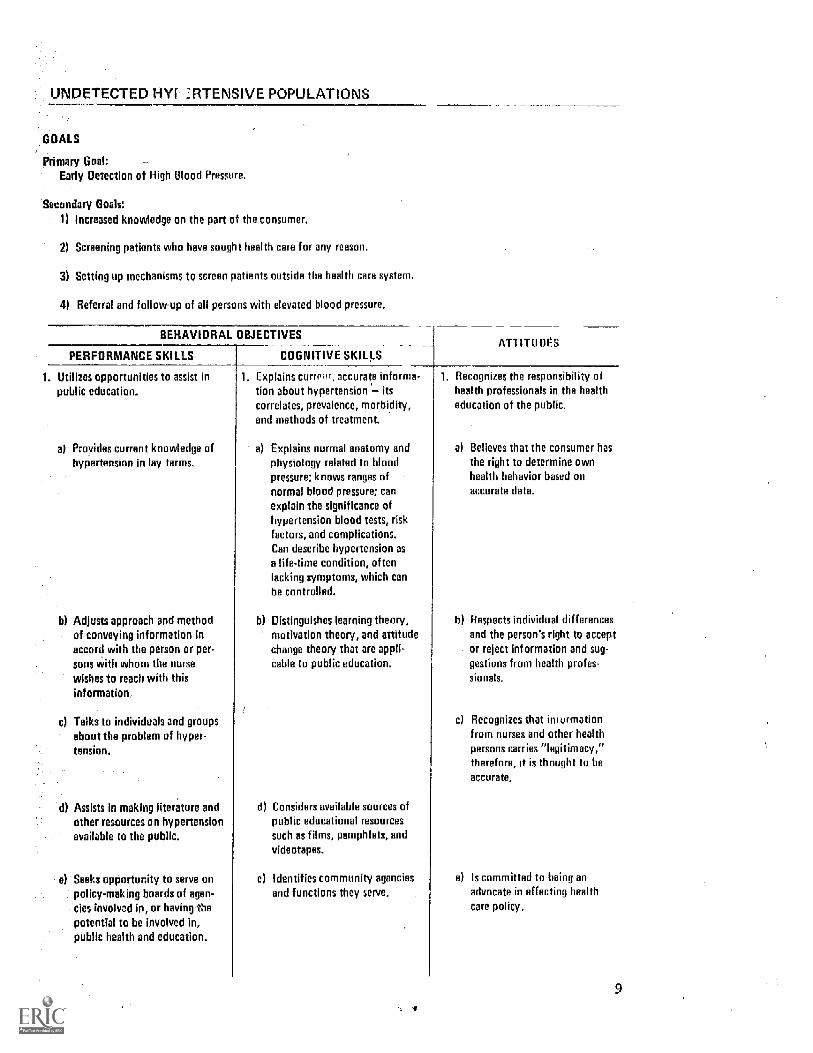
UNDETECTED LAW --]RTENSIVE POPULATIONS
GOALS
Primary Goal:Early Detection of High Blood Pressure.
Secondary Goals:
1) Increased knowledge on the part of the consumer.
2) Screening patients who have sought health care for any reason.
3) Setting up mechanisms to screen patients outside the health care system.
4) Referral and follow-up of all persons with elevated blood pressure.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS COGNITIVE SKILLSATTITU DES
1. Utilizes opportunities to assist inpublic education.
al Provides current knowledge ofhyPertension in lay terms.
b) Adjusts approach and methodof conveying information inaccord with the person or per-sons with whom the nursewishes to reach with thisinformation,
c) Talks to individuals and groupsabout the problem of hyper-tension.
d) Assists in making literature andother resources on hypertensionavailable to the public.
e) Seeks opportunity to sem onpolicy-making boards of agen-cies involved in, or having thepotential to be involved in,public health and education.
1. Explains currri.:. accurate info a
tion about hypertension its
correlates, prevalence, morbidity,and methods of treatment.
a) Explains normal anatomy andphysiology related to bloodpressure; knows ranges ofnormal blood pressure; canexplain the significance ofhypertension blood tests, riskfactors, and complications.Can describe hypertension asa life-time condition, oftenlacking symptoms, which canbe controlled.
h) Distinguishes learning theoni,motivation theory, and attitudechange theory that are appli-cable to public education.
d) Considers available sources ofpublic educational resourcessuch as films, pamphlets, and
videotapes.
el Identifies community agenciesand functions they serve.
1. Recognizes the responsibility ofhealth professionals in the healtheducation of the public.
a) Believes that the consumer hasthe right to determine ownhealth behavior based onaccurate data.
b) Respects individual differencesand the person's right to acceptor reject inf ormation and sug-gestions from health profes-sionals.
c) Recognizes that imurmationfrom nurses and other healthpersons carries -legitimacy,-therefore, it is thought to beaccurate.
e) Is committed to being anadvocate in effecting healthcare policy.
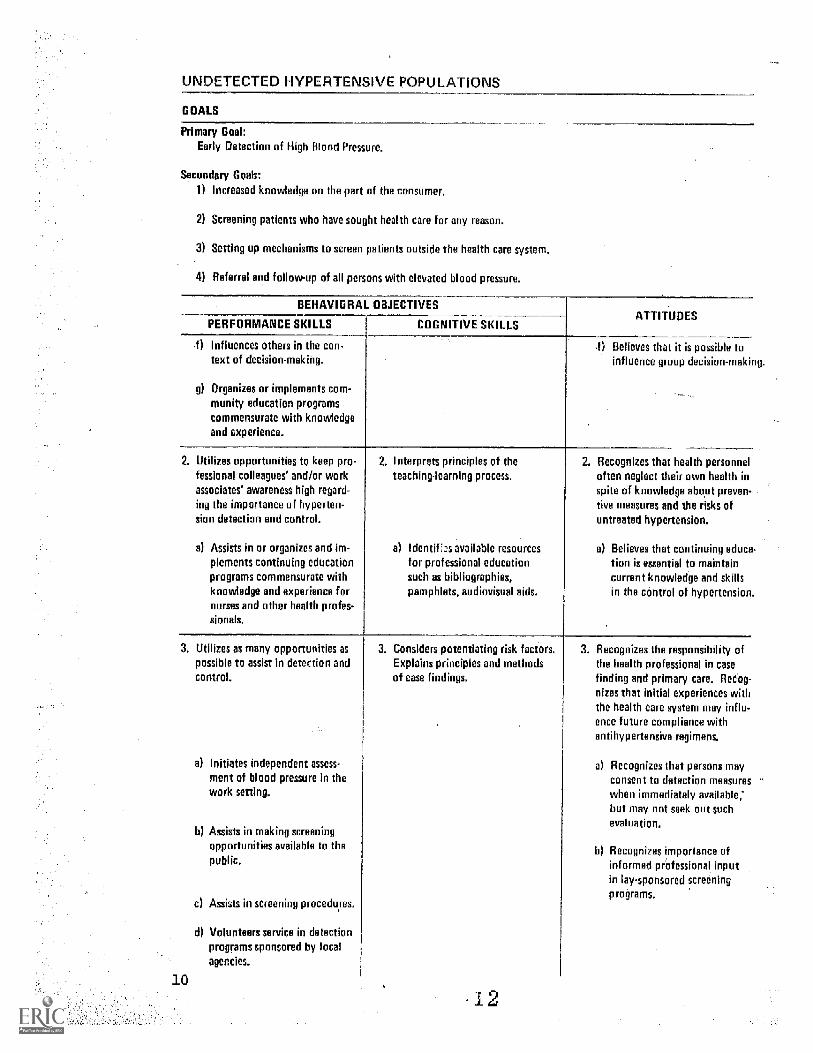
UNDETECTED HYPERTENSIVE POPULATIONS
GOALS
ary Goal:Early Detection High Blood Pressure.
Secondary Goals:
1) Increased knowledge on the part of the consumer.
2) Screening patients who have sought health care for any reason.
3) Setting up mechanisms to screen patient outside the health care system.
4) Referral and follow-up of all persons with elevated blood pressure.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS COGNITIVE SKILLSATTITUDES
f) Influences others in the con-text of decision-making,
g) Organizes or implements com-munity education programscommensurate with knowledgeand experience.
Believes that it is possible toinfluence group decision-makii
2. Utilizes opportunities to keep pro-fessional colleagues and/or workassociates' awareness high regard-
ing the importance of hyperten-sion detection and control.
a) Assists in or organizes and ire-plements continuing educationprograms commensurate withknowledge and experience fornurses and other health profes-sionals.
2. Integirets principles of theteaching-learning process
a) Identifs available resourcesfor professional educationsuch as bibliographies,pamphlets, audiovisual aids.
2. Recognizes that health personneloften neglect their own health inspite of knowledge about preven-tive measures and the risks ofuntreated hypertension.
a) Believes that continuing educetion is essential to maintaincurrent knowledge and skillsin the control of hypertension.
3. Utilizes as many opportunities aspossible to assist in detection andcontrol.
a) Initiates independent assess-ment of blood pressure in thework sating
b) Assist in making screeningopportunities available to thepublic
c) Assists in screening proceduyes.
d) Volunteers service in detectionprograms sponsored by localagencies.
3. Considers potentiating risk factors.Explains principles and methodsof case findings,
3. Recognizes the responsibility ofthe health professional in casefinding and primary care. Recog-nizes that initial experiences withthe health care system may influ-ence future compliance withantihypertensive regimens.
a) Recognizes that persons mayconsent to detection measureswhen immediately available;but may not seek out suchevaluation.
b) Recognizes importance ofinformed professional inputin lay-sponsored screeningprograms.
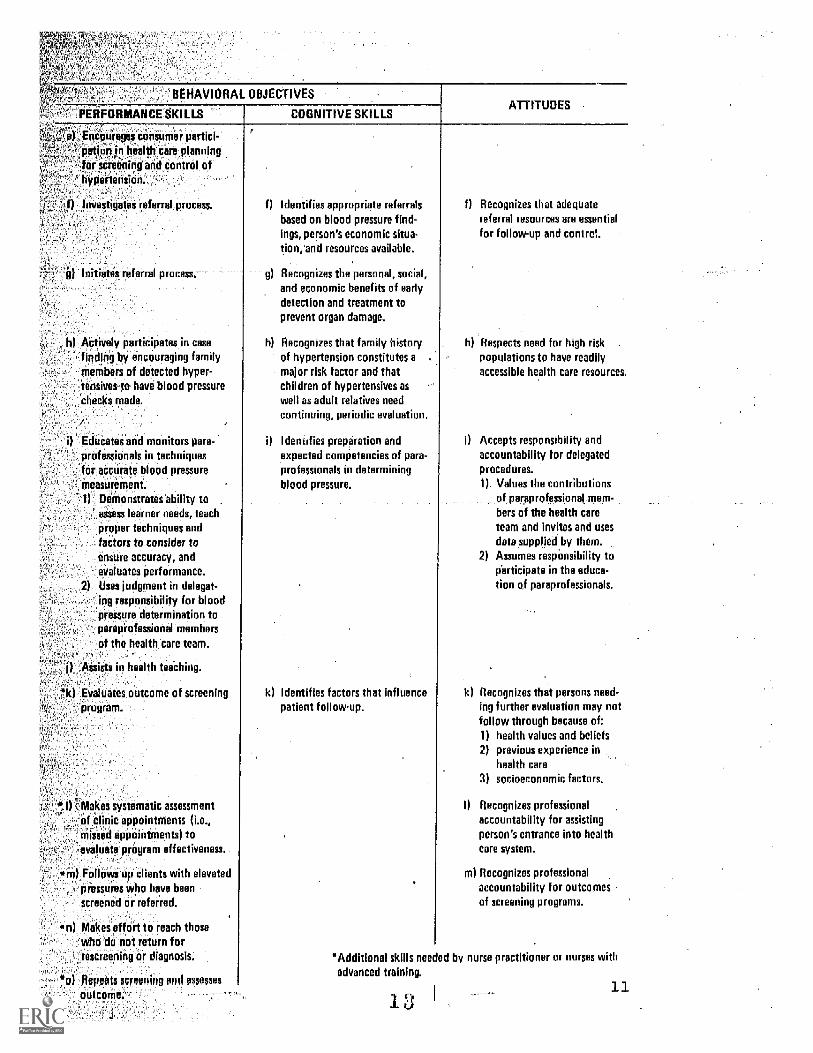
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS
Enccurages consumer partici-pation in health care planning:far sereening and control ofhypertension.
Investigates referral process.
nitiates refeffal process.
COGNITIVE SKILLSATTITUDES
, h) Actively panicipates in case
finding by encouraging family, members of detected hyper-
-tensives-to have blood pressure
'checks made.
_
i) Educates and monitors para-professionals in techniquesfor accurate blood pressuremeasurement.
1) Demonstrates ability toassess learner needs, teach
proper techniques andfactors to consider toensure accuracy, and
evaluates performance.
2) Uses judgment in delegat-ing responsibility for bloodpressure determination toparaprofessional members
of the health care team.
.Assists in health teaching.
*k) Evaluates outcome of screeningprogram.
akes systematic assessment
of clinic appointments (i.e.,missed appointments) toevaluate program effectiveness.
in) Follows up clients with elevatedpressures who have been
screened or referred.
*n) Makes effort to reach thosewho do not return forrescreening or diagnosis.
*o) ,Repeats screening and assess
outcome.
f) Identifies appropriate referralsbased on blood pressure find-ings, person's economic situa-tion, and resources available.
g) Recognizes the personal, social,and economic benefits of earlydetection and treatment toprevent organ damage_
h) Recognizes that family historyof hypenension constitutes amajor risk factor and thatchildren of hypertensives aswell as adult relatives needcontinuing, periodic evaluation.
Identifies preparation andexpected competencies of para-professionals in determiningblood pressure.
k) Identifies factors that influencepatient followup.
f Recognizes that adequate
referral resources are essentifor follow-up and contral.
h) Respects need for high risk .
populations to have readilyaccessible health care resources.
i) Accepts responsibility andaccountability for delegatedprocedures.1) Values the contributions
of paraprofessional mem-bers of the health careteam and invites and uses
data supplied by them.2) Assumes responsibility to
ciarticipate in the educa-tion of paraprofessionals.
k) Recognizes that persons need-ing further evaluation may notfollow through because of:1) health values and beliefs2) previous experience in
health care
3) socioeconomic factors.
I) Recognizes professional
accountability for assistingperson's entrance into healthcare system.
m) Recognizes professionalaccountability for outcomesof screening programs.
*Additional skills needed by nurse practitioner or nurses withadvanced training.
DETECTED HYPERTENSIVE POPULATIONS
In-developing the guidelines for educational pro-alms for the'dare of the patient with detected high
.
blood pressur=ai the Task Forde considered the desiredPatient_outcomes to)* the ultimate goals. These were-used_-as a focus'for:delineating the essential perfor-ance skills-and related cognitive skills and attitudes.
- The patient ontcoMes reflect the goals for minimiz--1.4g-disruptions to the health status of the patient andfor promotion of health assets.
Those related-to minimizing-disruption of health-status include: .-----
1. Stable blood pressure in accordance -ith thetherapeutic goal.
_Minimal therapeutic side effects of the medica-tion regimen.
_ Minimal pathophysiologicalphanges secdndary-to -hypertension.
Those related to promotion of health include:
'1.-Patient and family adjustment to health statusand therapy.
Maintenance of the life style compatible withpersonal health care goals.
Patient and family understanding of high bloodpressure and treatment appropriate for self-care.
Patient assuming responsibility for self-carewithin psychosocial and physical limitations.
The Task Force identified the assessments which thenurse is expected to perform and the judgment which sheis expected to make to guide the interventions, cella-boraton, and consultation with the physicians and otherhealth professionals to provide the needed medical andhealth service. The interventions identified focus oninstructing, guiding, and supporting patients in achiev-ing and maintaining self-care, on assisting the patientand family to cope with the demands of the medical re-gimen, and on recognizing existing behaviors that enhancehealth.
14 13
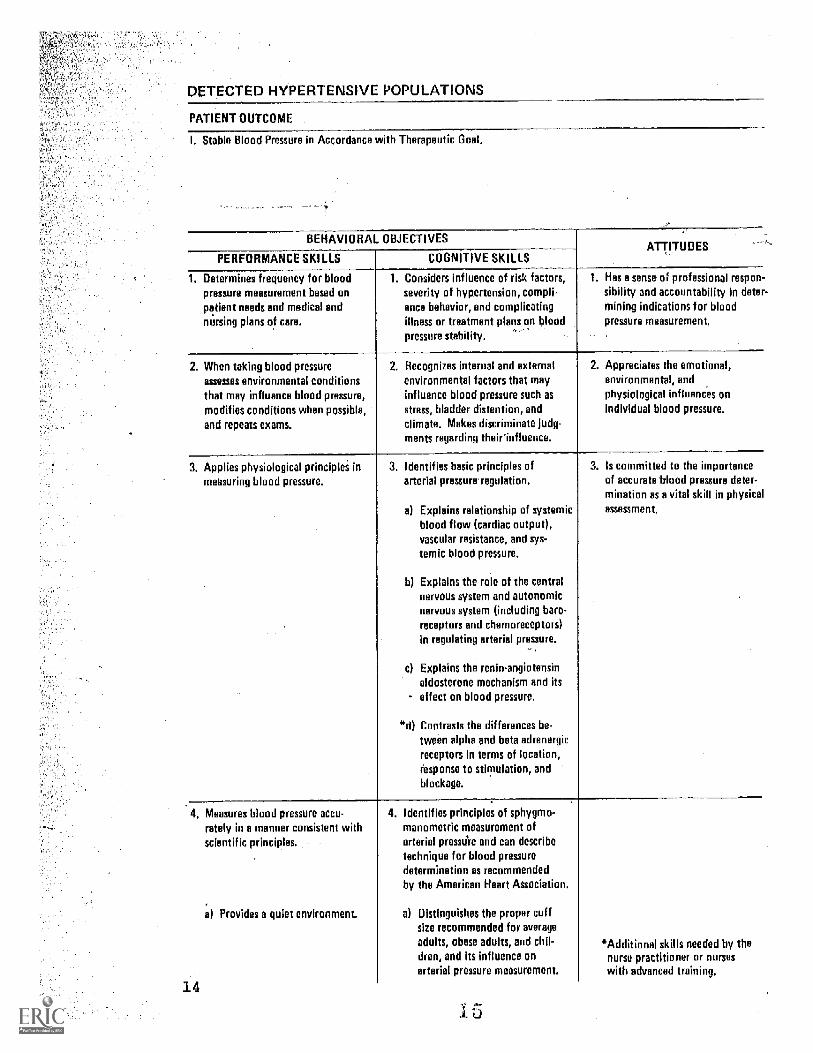
PETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
I. Stable Blood Pressure in Accordance with Therapeutic Goal.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKI LLS COGNITIVE SKILLSATTITUDES
1 etermines frequency for bloodpressure measurement based on
patient needs and medical andnursing plans of care.
1. Considers influence of risk factorsseverity of hypertension, compli-ance behavior, and complicatingillness or treatment plans on bloodpressure stability.
1. Has a sense of professional respon-
sibility and accountability in deter-mining indications for bloodpressure measurement.
2. When taking blood pressureassesses environmental conditionsthat may influence blood pressure,modifies conditions when possible,and repeats exams
2. Recognizes internal and externalenvironmental factors that mayinfluence blood pressure such as
stress, bladder distention, andclimate. Makes discriminate judg-ments regarding their influence.
2. Appreciates the emotional,environmental, andphysiological influences onindividual blood pressure.
3. Applies physiological principles inmeasuring blood pressure.
3. Identifies basic principles ofarterial pressure regulation.
a) Explains relationship of systemicblood flow (cardiac output),vascular resistance, and sys-temic blood pressure.
b) Explains the role of the centralnervous system and autonomicnervous system (including barn-receptors and chemoreceptors)in regulating arterial pressure.
c) Explains the renin-angiotensinaldosterone mechanism and itseffect on blood pressure.
"d) Contrasts the differences be-tween alpha and beta adrenergirreceptors in terms of location,response to stimulation, andblockage.
3. Is committed to the importanceof accurate blood pressure deter-mination as a vital skill in physicalassessment.
4. Measures blood pressure ecru-rately in a manner consistent wi hscientific principles.
14
a) Provides a quiet environment.
4. Identifies principles of sphygmo-manometric measurement ofarterial pressu're and can describetechnique for blood pressuredetermination es recommendedby the American Heart Association.
a) Distinguishes the proper cuffsize recommended for averageadults, obese adults, and chil-dren, and its influence onarterial pressure measurement.
*Additional skills needed by thenurse practitioner or nurseswith advanced training.
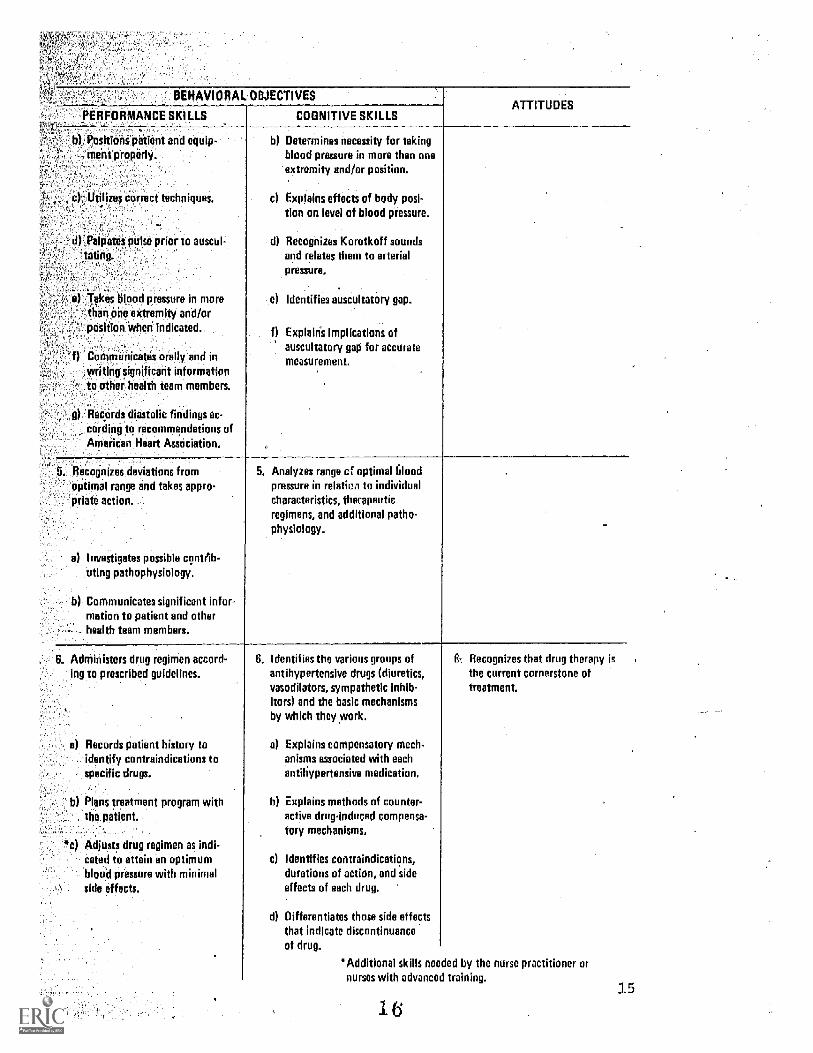
BEHAVIO
PERFORMANCE SKI LLS
ECTIVES
COGNITIVE SKILLSATTITUDES
Is Positions patient and equip-ment properly.
c)-' Utilizes correct techniques.
d),Palpares pulse prior to auscul-'toting.
Takes blood pressure in moreAhan one extremity and/orposition when indicated.:
Communicates orally and inwriting significant informationto other health team members.
g Records diastolic findings ac-cording to recommendations ofAmerican Heart Association.
b) Determines necessity for takingblood pressure in more than oneextremity and/or position.
c) Explains effects of body posi.tin on level of blood pressure.
d Recognizes Korotkoff soundsand relates them to arterialpressure.
-.e) Identifies auscultatory gap.
f) Explain's implications ofauscultatory gap for accuratemeasurement.
5. Recognizes deviations fromoptimal range and takes appro-priate action.
Investigates possible contrib-uting pathophysiology.
Communicates significant infor-mation to patient and otherhealth team members.
5. Analyzes range cf optimal filoodpressure in relatien to individualcharacteristics, therapeuticregimens, and additional patho-
physiology.
6. Administers drug regimen accord-ing to prescribed guidelines.
Records patient history toidentify contraindications tospecific drugs.
b) Plans treatment program withthe patient.
*c) Adjusts drug regimen as indi-cated to attain an optimumblood pressure with minimalside effects.
6. Identifies the various groups ofantihypertensive drugs (diuretics,vasodilators, sympathetic inhib-itors) and the basic mechanismsby which they work.
a) Explains compensatory mech-anisms associated with eachantihypertensive medication.
b Explains methods of counter-active drug-induced compensa-tory mechanisms.
c) Identifies contraindications,durations of action, and sideeffects of each drug.
d) Differentiates those side effectsthat indicate discontinuanceof drug.
6.. Recognizes that drug therapy isthe current cornerstone oftreatment.
*Additional skills needed by the nurse practitioner ornurses with advanced training.
1 615
DETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
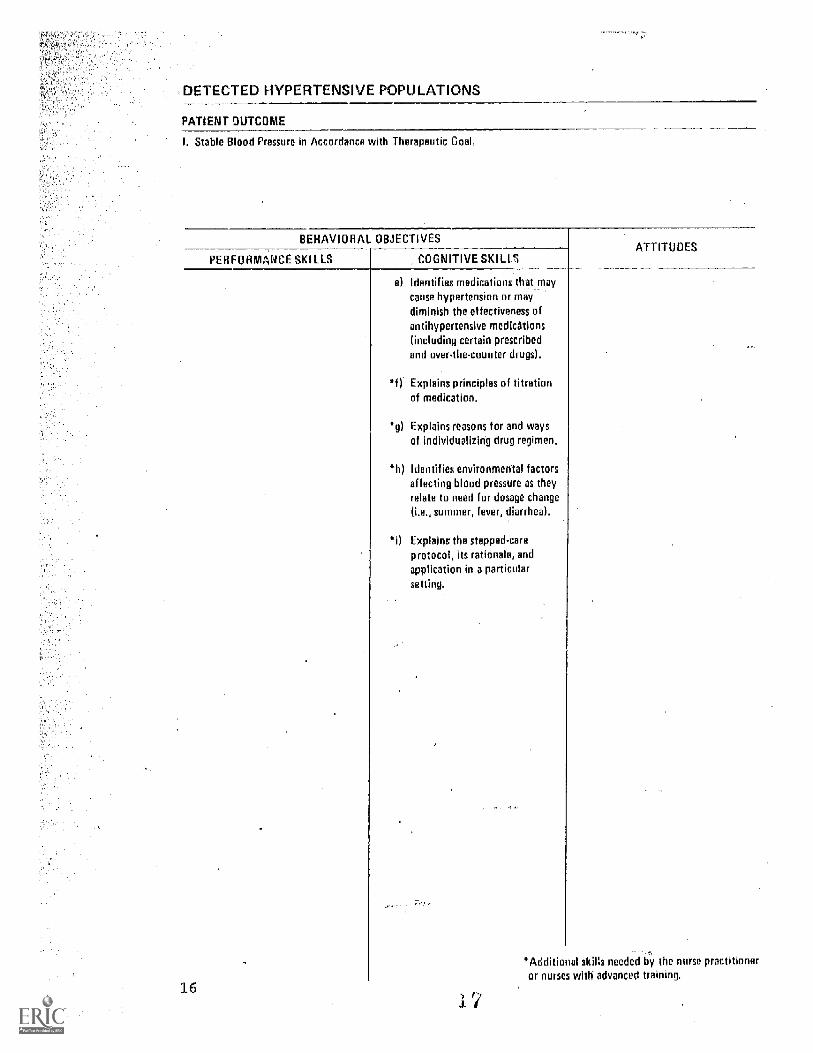
I. Stable Blood Pressure in Accordance with Therapeutic Goal.
BEHAVIORAL OBJECTIVES
PER FORMANCE SKI LLS COGNITIVE MU SATTITUDES
16
el Identifies medications that_maycause hypertension or maydiminish the effectiveness ofantihypertensive medications(including certain prescribedand over-the-counter drugs).
Explains principles of titrationof medication.
*g) Explains reasons for and waysof individualizing drug regimen.
4) Identifies environmental factorsaffecting blood pressure as theyrelate to need for dosage change
(i.e., summer, fever, diarrhea).
Explains the stepped-care
protocol, its rationale, andapplication in a particularsetting.
*Additional skins needed by the nurse practitioneror nurses with advanced training.
_DETECTED.HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
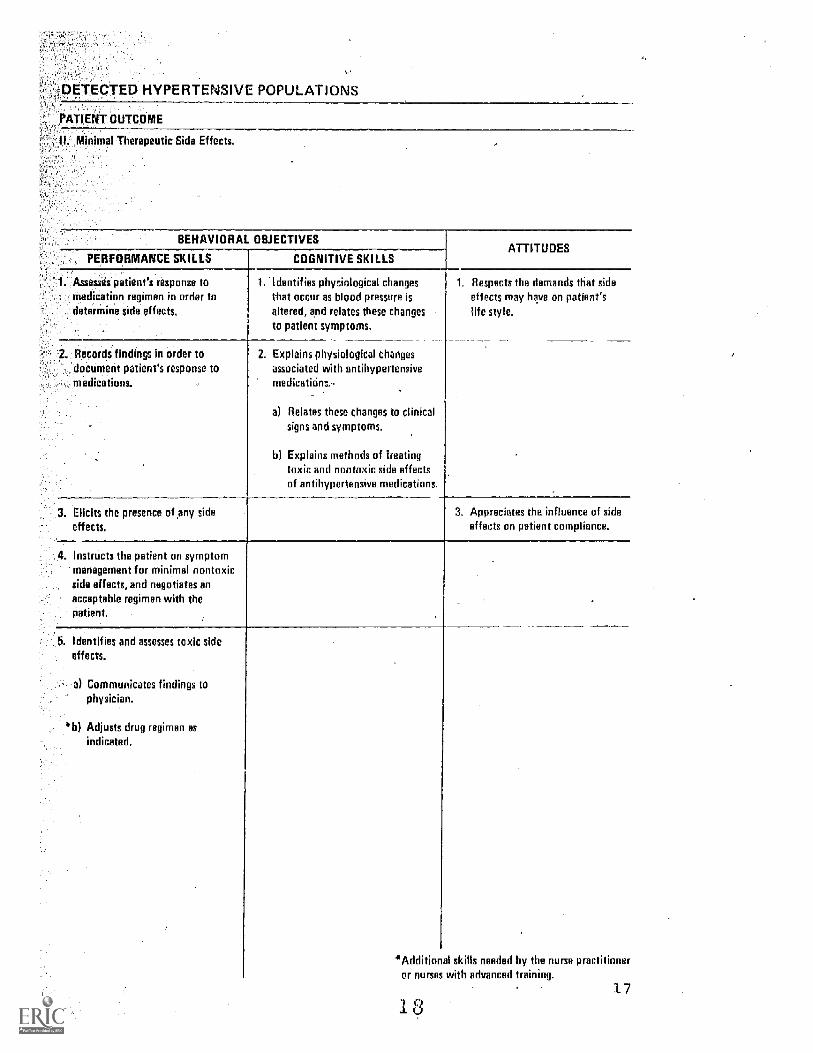
II. Minimal.Therapeutic Side Effects.
BEHAVIORAL OBJECTIVESATTITUDES
PERFORMANCE SKILLS COGNITIVE SKILLS
1. Assesses patient's response to, medication regimen in order todetermine side effects,
1. Identifies physiological changesthat occur as blood pressure isaltered, and relates these changesto patient symptoms.
1. Respects the demands that side
effects may heve on patient'slife style.
2. Records findings in order todocument patient's response tomedications. ..
2. Explains physiological changesassociated with antihypertensivemedicatinns,
a) Relates these changes to clinicalsigns and symptoms,
b) Explains methods of treatingtoxic and nontoxic side effectsof antihypertensive medications.
3. Elicits the presence of any sideeffects,
3. Appreciates the influence of sideeffects on patient compliance.
4. Instructs the patient on symptommanagement for minimal nontoxicside effects, and negotiates an
acceptable regimen with thepatient.
5. Identifies and assesses toxic sideeffects.
'a) Communicates findings tophysician.
*b Adjusts drug regimen asindicated.
*Additionalor nurses
skills needed by the nurse practitionerwith advanced traininn.
17
...-.DETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
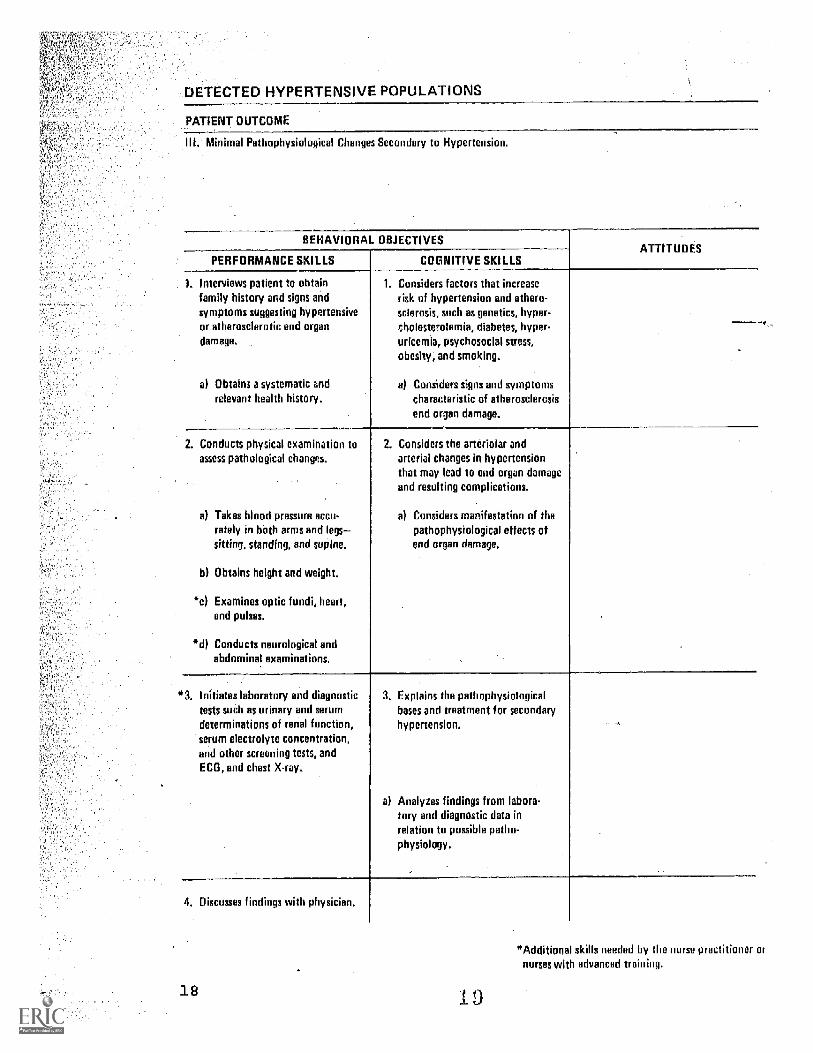
Minimal Pathophysiological Changes Secondary to Hypertension.
BEHAVIORAL OBJECTIVESATTITUDES
PERFORMANCE SKILLS COGNITIVE SKILLS
1. Interviews patient to obtainfamily history and signs andsymptoms suggesting hypertensiveor atherosclerotic end organ
damage.
a) Obtains a systema end
relevant health history.
I. Considers factors that increaserisk of hypertension and athero-sclerosis, such as genetics, hyper-
tholestrolemia, diabetes, hyper-uricemia, psychosocial stress,
obesity, and smoking.
a) Considers signs and symptomscharacteristic of atherosclercsisend organ damage.
2. Conducts physical examination toassess pathological changes.
a) Takes blood pressure accu-rately in both arms and legssitting, standing, and supine,
b) Obtains height and weight.
*c) Examines optic fundi, heart,and pulses.
0d) Conducts neurological andabdominal examinations.
2. Considers the arteriolar andarterial changes in hypertensionthat may lead to end organ damageand resulting complications.
a) Considers manifestation of thepathophysiological effects ofend organ damage.
'3 Initiates laboratory and diagnostictests such as urinary and serumdeterminations of renal function,serum electrolyte concentration,and other screening tests, andECG, and chest X-ray.
3. Explains the pathophysiologicalbases and treatment far secondaryhypertension.
a) Analyzes findings from labora-tory and diagnostic data inrelation to possible patho-physiology.
4. Discusses findings with physician.
18
"Additional skills needed by the nurse practitioner ornurses with advanced training.
, DETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
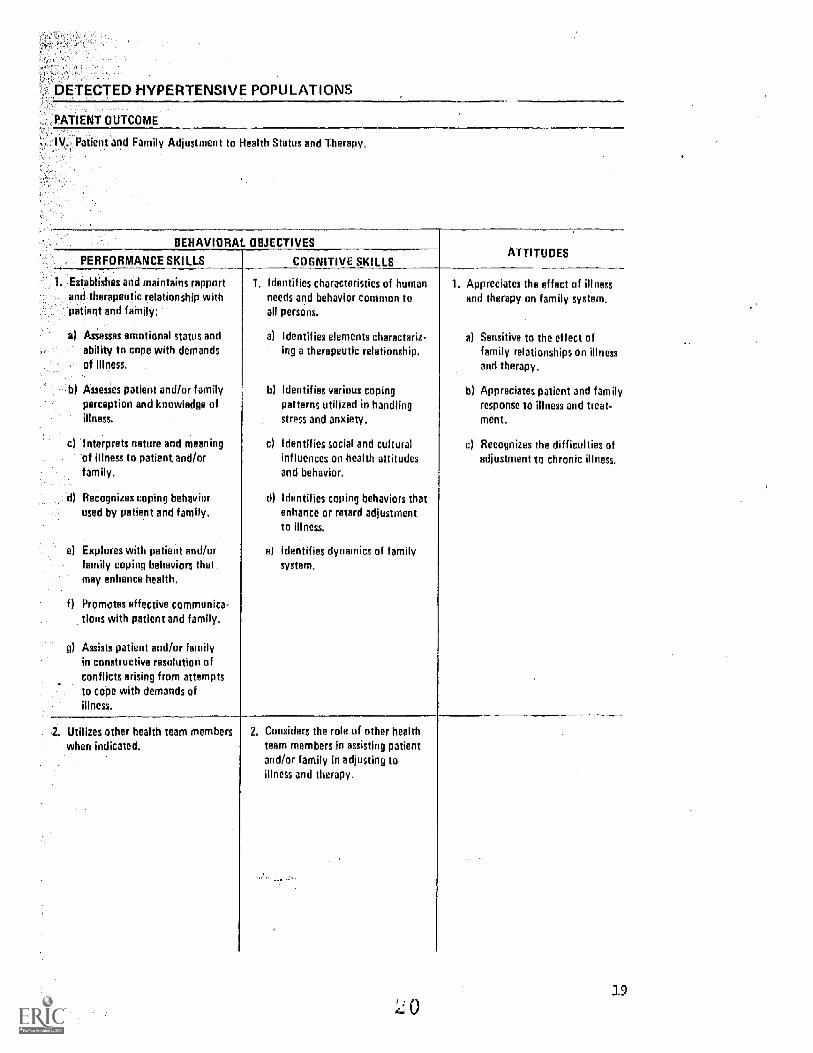
= IV. Patient and Family Adjustment to Health Status and Therapy.
BEHAVIORAL OBJECTIVESATTITUDES
PERFORMANCE SKILLS COGNITIVE SKILLS
1 Establishes and maintains rapportand therapeutic relationship withpatient and family:
a) Assesses emotional status andability to cope with demandsof illness,
b) Assesses patient and/or familyperception and knowledge ofillness.
c) Interprets nature and meaningof illness to patient and/orfamily.
d) Recognizes coping behaviorused by patient and family.
el Explores with patient and/orfamily coping behaviors thatmay enhance health.
f) Promotes effective communica-tions with patient and family.
g) Assists patient and/or familyin constructive resolution ofconflicts arising from attemptsto cope with demands ofillness.
1. Identifies characteristics of humanneeds and behavior common toall persons.
a) Identifies elements characteriz-ing a therapeutic relationship,
h) Identifies various copingpatterns utilized in handlingstress and anxiety.
c) Identifies social and culturalinfluences on health attitudesand behavior.
d) Identifies coping behaviors thatenhance or retard adjustmentto illness.
el Identifies dynamics of familysystem.
1. Appreciates the effect of illnessand therapy on family system.
a) Sensitive to the effect offamily relationships on illnessand therapy.
b) Appreciates patient and familyresponse to illness and treat-ment.
c) Recognizes the difficulties ofadjustment to chronic illness.
2. Utilizes other health team memberswhen indicated,
2. Considers the rale of other healthteam members in assisting patientand/or family in adjusting toillness and therapy.
19
DETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
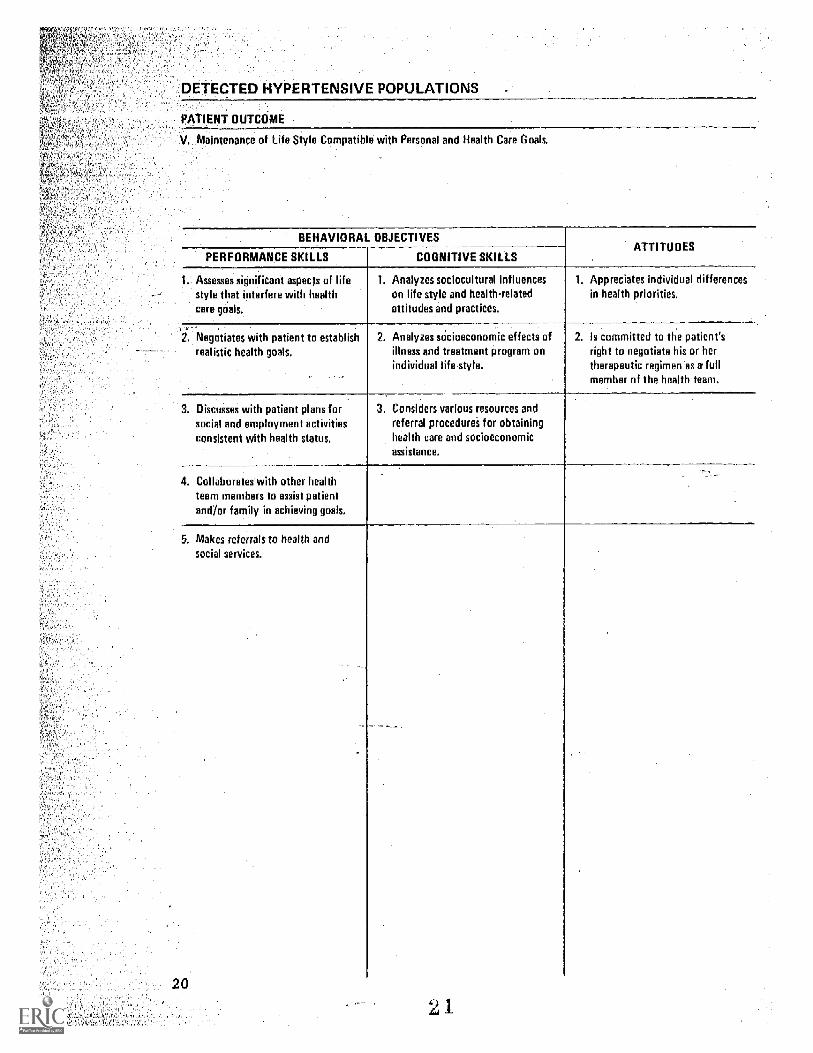
V. Maintenance of Life Style Compatible with Personal and Health Care Goals.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS COGNITIVE SKILLSATTITUDES
1. Assesses significant aspects of lifestyle that interfere with healthcare goals.
1. Analyzes sociocultural influenceson life style and health-relatedattitudes and practices.
1. Appreciates individual differencesin health priorities.
2 Negotiates with patient to establishrealistic health goals.
2. Analyzes socioeconomic effects ofillness and treatment program onindividual life style.
2. Is committed to the patient'sright to negotiate his or hertherapeutic regimen as a fullmember of the health team.
3. Discusses with patient plans forsocial and employment activitiesconsistent with health status.
3. Considers various resources andreferral procedures for obtaininghealth care and socioeconomicassistance.
4. Collaborates with other healthteam members to assist patientand/or family in achieving goals.
5. Makes referrals to health andsocial seMces.
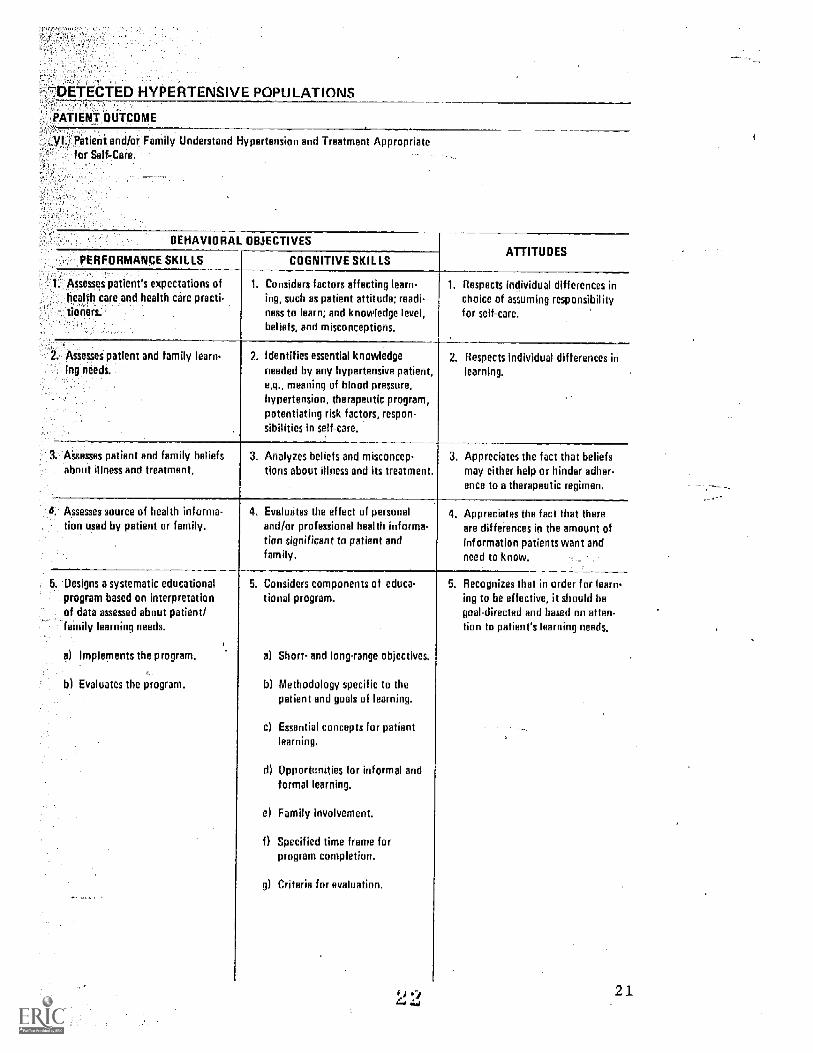
--DETECTED HYPERTENSIVE POPULATIONS
, PATIENT OUTCOME
Patient and/or Family Understand Hypertension and Treatment Appropriatefor Self-Care.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS COGNITIVE SKILLSATTITUDES
1. Assesses patient's expectations ofhealfh care and health care practi-tioners:--.:
1. Considers factors affecting learn-ing, such as patient attitude; readi-ness to learn; and knowledge level,beliefs, and misconceptions.
1. Respects individual differences inchoice of assuming responsibilityfor self-care.
2. Assesses patient and family learn-ing needs,
2. Identifies essential knowledgeneeded by any hypertensive patient,e.g., meaning of blood pressure,hypertension, therapeutic program,potentiating risk factors, respon-sibilities in self-care.
2. Respects individual differences inlearning.
I. Assesses patient and family beliefsabout illness and treatment.
3. Analyzes beliefs and misconcep-tions about illness and its treatment.
3, Appreciates the fact that beliefsmay either help or hinder adher-ence to a therapeutic regimen.
Assesses source of health informa-tion used by patient or family,
4. Evaluates the effect of personaland/or professional health informa-Van significant to patient andfamily,
4. Appreciates the fact that thereare differences in the amount ofinformation patients want andneed to know.
i. Designs a systematic educationalprogram based on interpretationof data assessed about patient/family learning needs.
a) Implements the program.
b) Evaluates the program.
5. Considers components of educe-tional program.
a) Short- and long-range objectives
b) Methodology specific to thepatient and goals of learning.
c) Essential concepts for patientlearning.
d) Opportcnities for informal andformal learning.
el Family involvement.
0 Specified time frame forprogram completion.
g) Criteria for evaluation.
5. Recognizes that in order for learn-ing to be effective, it should begoal-directed and based on atten-tion to patient's learning needs.
21
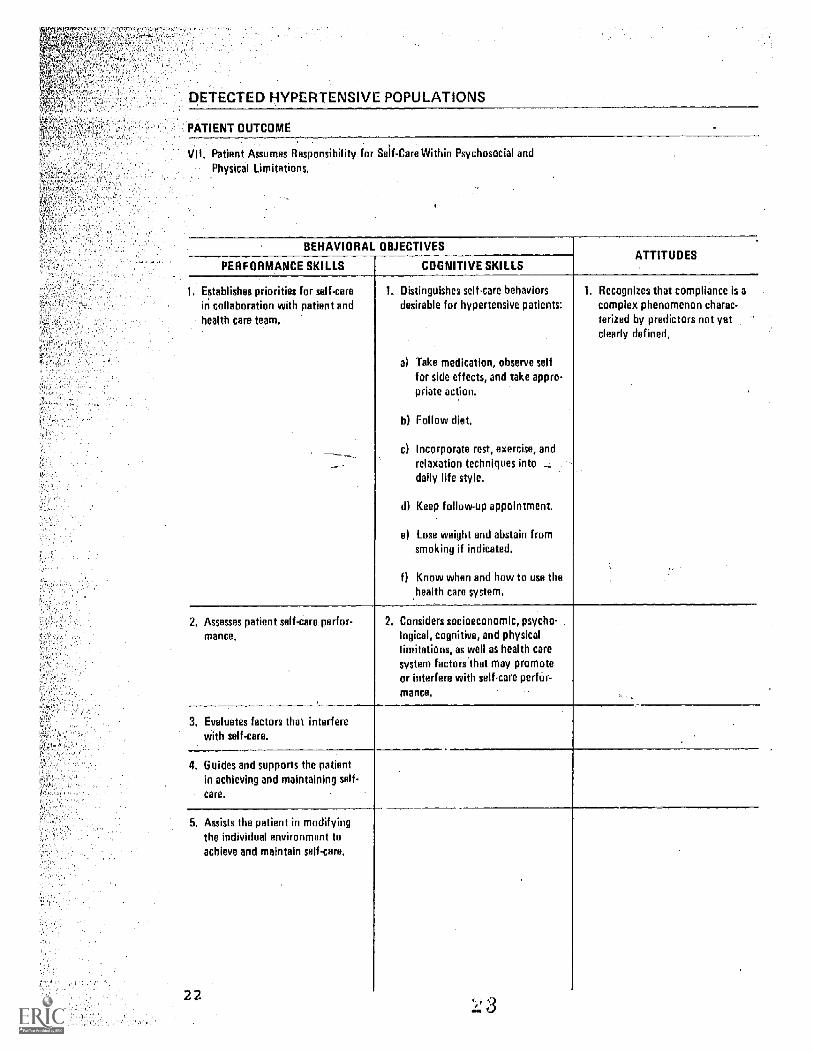
DETECTED HYPERTENSIVE POPULATIONS
PATIENT OUTCOME
VII. Patient Assumes Responsibility for Self-Care Within Ps-ychosocial andPhysical Limitations.
BEHAVIORAL OBJECTIVES
PERFORMANCE SKILLS COGNITIVE SKILLSATTITUDES
1 Establishes priorities for self-carein collaboration with patient andhealth care team.
Distinguishes selkare behaviorsdesirable for hypertensive patients:
a) Take medication, observe selffor side effects, and take appro-priate action.
b) Follow diet.
c) Incorporate rest, exercise, andrelaxation techniques intodaily life style.
d) Keep follow-up appointment.
e) Lose weight and abstain fromsmoking if indicated.
Know when and how to use thehealth care system.
1. Recognizes that compliance is acomplex phenomenon charac-terized by predictors not yetclearly defined.
2. Assesses patient self-dare perfor-
mance.
2. Considers socioeconomic, psycho-logical, cognitive, and physicallimitations, as well as health caresystem factors'that may promoteor interfere with self-care perfár-
mance.
3. Evaluates factors that interferewith self-care.
4. Guides and supports the patientin achieving and maintaining self-
care.
5. Assists the patient in modifyingthe individual environment toachieve and maintain self-care.
22
ACHIEVING OBJECTIVESpproaclies and Evaluations
The behavioral objectives were ,designed as a re-source for-Planning for the teaching-learning processand as a guide for seleeting contentl instructionalmethods, and-testing processes_used in the preparationof nurses for involvement in high blood pressure con-trol..
The responsibilities inherent in the control ofrhigh blood pressure are congruent with the practice ofnursing including the delivery of primary care, whichincludes autonomous thinking and decision making.Screening and long-term management by nurses is funda-mental to national efforts to deal with the millions
of persons needing diagnosis and follow-up care.
Working with patients and their families to helpcontrol high blood pressure requires mastery of essen-tial knowledge, analytical thinking, skilled perfor-mance of clinical procedures, and attitudes congruentwith responsible patient care.
The specific teaching strategy - the instructionalplan for any particular unit - will be influenced by thelearner's characteristics, background of knowledge, clini-cal performance skills, and content to be learned, aswell as by the available learning resources, the enviran-ment, and the teaching preferences of the instructor.The sequencing of learning experiences will depend on theprerequisite knowledge for the learning outcomes. Thus,strategies obviously will be different for the beginningnursing student as compared to nurses reviewing and up-dating skills in a continuing education program.
The verbs used to express' the cognitive and per-formance skills outlined in the behavioral objectiveswere specifically chosen to reflect high levels of think-ing involving interpretation, application, analysis,synthesis, and evaluation. (49, 51, 53) The kind ofbehaviors expected should be considered in structuringthe learning experiences and testing procedures, and inselecting resources.
:kv4riety of learning experiences for attainingthese objectives are suggested in current literature in-education and nursing education. (53, 47, 50, 52)
The innovative teacher can utilize any number of
23
teaching methods to facilitate the student's achieve-ment of the cognitive skills. Independent studies andaudiotutorial programs need to be evaluated for theireffectiveness, and for their appropriateness for use asindividualized methods of study for the students. Pro-blem-solving exercises, case reports with a multidis-cipline team, and peer review of patient records alsomay prove to be effective methods in hypertension educa-tion.
The attitudes., values, and beliefs critical tomodern nursing practice may be acquired in a variety ofstructured and unstructured ways such as through familyand other primary group experiences opportunities fordiscussions, sharing with peers; and exposure to de-Sired attittdes held by:others with:whom the studentidentifies The latter may be profesSional role models,patients-, friends, or relatives. (46, 50)
..Thoughtful'use of 'questioning to:aesist the-studenttoapply. understanding ofrelevant.concepts about .highblood 15-resstre and its managenent in-both siMulated andreal:patient.Situationa.will.enhance thedevelopment ofrequisite:judgment and decision making' indicated in thesets --of CognitiVe and perforMance skills. The .objec7tives, should be adapted .for.the needs-of-specific groups.6-fstudentsand'the'degree.ofresponsibility.in hyper---tension Care..the learners are;.exPected to...assume. All_nurses are.expected.:tojiave. ajpasic_understanding of'llomal-andpathblogical:physiblogical.mechanisms whichdetermine blood pressure regardless of ,their practiceSetting., They will'assist in'.case finding and inter-pretation-Of blood pressure'whether in a school,J.ndus-
connunity clinic, or hospital setting.
.Those who '. are screening for high blood pressure,providing care for hypertensive-individuals, or working'with high risk ,groups will need-in-depth, comprehensive''understanding of-factors that influence high blood pres-sure and its 'iveriagenent.
Thedelineated.patient outcomes and behavioral., objectives-may also be used in the orientation of newstaff'.and assesspent of.theknowledge and.performanceskills appropriate:to the practice situation and for in-service education programs. Both the teaching methodsand:.thetests uSed for evaluation.influence the think-ing-process and other performance skills which are de-veloped. Tests using methods which reflect specified'behavioral objectives proVide-a basis for adjusting.learning experience .to the students' -strengths anddeficiencies aS well as evaluating the effectiveness of-the teaching and the learning outcomes. Criterion-
24..f#J
erence testing as advocated by Gronlund (48) is seenrelevant for evaluation of both cognitive and per-nce outcomes.
'Use of such tests is viewed as particularly valu-le l'or pretesting of nurses in continuing education
in-service programs and for advanced educationalrograms. Results from pretesting as well as ongoingstinqlduring the educational program are useful for
identifying the learners' competencies and learningeedS. Results assist the instructor to tailor learn-
lug to the specific needs of the group and,-assist the students to monitor their own progress.
Educators recommend using pretests, followed by.-:periodic testing during the instructional program, asApie11 as a final evaluation'to measure the learning out-
:11Comes-achieved. Guides for the development and use of,arious methods are presented in Gronlund, Reilly, and
weer. (48, 51 52)
Few guides are currently available for evaluating_ patient outcomes. Nursing audit criteria are beingdeveloped for assessing the quality of care received by,patients with high blood pressure. (6) Peer reviewbased on guidelines developed by this Task Force providesa basis for evaluating the patient ourcomes and the re-lated nursing assessments and interventions. 'Such re-
,
views should disclose factors that influence the out-comes achieved.
25
NURSING PERSPECTIVES ON THE CURRENT STATE OF KNOWLEDGEPsychophysiological and Psychosocial Factors,Adherence and Patient Education
The report of the Working Group on Training andEvaluation of Physicians in High Blood Pressure outlinesthe basic knowledge which guides the medical managementof patients with high blood pressure. Much of this sameknowledge is needed by nurses. The report from theJoint National Committee provides an excellent summaryof the essential diagnostic and pharmaceutical manage-ment of these patients. (1)
Current information basic to understanding the re-gulation-of blood pressure, the pathophysiologic basisfor high blood pressure, and the current understandingof the diagnosis and medical management are well de-lineated in the general references which are appended.(15 31)
No singular approadh, however, will be adequate todeal with the- ramifications of high blood pressure. Toassist the individuals with high blood pressure to achieveand maintain an optimal level of health, one must con-sider not only the pathophysiological process but.theperson involved, the psychological and social environ-ment, and the response as a total person.
Because the knowledge base on these aspects ofhealth are being generated, an attempt has been madehere_to sunnarize some current perspectives salient fornursing practice. Interested readers may wish to ex-plore those areas further.
Considered from a psychophysiologic perspective,evidence suggests that the kind and quality of the in-dividual's life style, interaction with others, and thethreat perceived may influence the development of hyper-tension. Environmental siLn ms requiring continuousbehavioral adjustments by the individual were found tobe related to sustained elevations in blood pressure.(39)
Gilmore explicates the physiological mechanisns bywhich high blood pressure as a stress response is medi-ated and suggests that these tre defense responses to
threatening life situations. (34) Patel cites evidenceof the physiological bases of reduction of arterial pres-
. sure by relaxation training. (36) Exercise programsfor hypertensive individuals have been reported to re-duce arterial blood .pressure ,(35, 40) These reductions'may be related to modification of the stress response.(32) The knowledge base for psychophysiological per-spective is fragmented. The literature on psychological
26
and'embtional stress is valuable in ap roachihg the
PrOblem. (321 37)
The psychophysiologicalperspective provides a
-potential .framework for assessing the individual's per-
'deption and response to individual life situation. The
Stress:response may also be related to the management
of strategies for blood pressure control.
.The potential value of a relaxation...program for re-
ducingthe magnitude and duration of rises in blood
-41ressure:associated with everyday emotional stress has
'been- Cited. (36) Relaxation programs appear promising
hypertensiveS-;-as a preventive measure for
)ligh risk individuals, and as a supplement to the phar-
7:.MaCeutical regimen. A number of relaxation techniques
-forrreduction of .blood pressure are being investigated,
..j.ncli4ding progressive relaxation, meditation, yoga, and
:1oiofeedback. Significant decreases have been reported
-froin-Some -studies but not from others, (33, 36, 37)
'Variation in patient responses to relaxation pro-
-.grams and other interventions,may be related to the
_patients' appraisal of the threatening aspects of their
.aife situation, the degree of control which they per-
deive they have for reducing the threat, and the fee],-
ings are,engendered. (38)
The-_role of psychosodial factors in the etiology
and course of hypertension is still unclear. Since
there_was no physiologic explanation,_at one time mony
thought psychological factors were etiologic. The
"hYpertensive personality" was seen as a major cause of
...:aggressiveness, drive, and hostility. The emphasis on
Personality is now seen as too simplistic, but few per-
-*ins-advocate disregarding psychological factors en-
tirely. The .present understanding of the role of these
:factors has been summarized as". . . probably not
rtiologic, but. . .'some hypertensive patients may be
sensitized by various psychologital rrocesses to over-
react,physiologically to psychological stimuli after
.the disease has begun." (41)
The authors of a 1969 comprehensive review of psy-
dhosocial factors in essential hypertension concluded
that findings from animal and human studies indicated
that repeated arousal of the defense alarm response
'might be an important mechanism in the development and
course of essential hypertension. (42) Continuing ex-
periments using stress situations of various types have
shown that hypertensives tend to differ from normoten-
sives in their responses to stress, often by a pro-
tracted return to normal standards in physiologic in-
dices. (54)
27
Evidence concerning the role of environmental andpsychological factors points to their being interactivewith such factors as sex, race, heredity, diet, weight,and as yet unknown physiologic factors. Social andeconomic stressors, for example, may increasingly beshown to be interactive with race. Both blacks and whitesin the lowest social classes of a large sample drawnfrom a prepaid medical plan group had higher blood pres-sure than those blacks and whites in higher social class-es. (43) At the same time, findings from studies focus-ed on environmental stress may raise more questions thanthey answer. For example, blood pressure has been shownto increase when rural persons have become urbanized.But a recent study in Detroit showed that higher read-ings in blacks were Telated to being raised in that cityand not migrating from elsewhere. (44)
How persons cope with stress has been and is a richfield for study, although means of identifying the mannerby which an individual deals with stress have been betterdescribed than the means by which persons can be assist-ed to cope with stress, particularly that of an environ-mental nature. Many environmental stressors such asunemployment, overcrowding, poverty, and inadequate hous-ing prejudice are beyond the influence of the healthprofessionals' direct practices- Yet such situationsmay be of greatest concern to the consumer and take pri-ority over health matters. The literature on hyperten-sion helps to emphasize that a primarily asymptomaticdisorder may not-pose an important threat to persons,with other immediate priorities-in day-to-day living.
Few direct linkages have been provided in the lit-erature betWeen the association of stress and adherence(compliance) behaVior in chronic illness. (45) Use ofthe health belief model as a framework for consideringadherence behavior has-been suggested as proving to bepotentially more explanatory than demographic characteris-tics.alone. This model states that the_person's per-ceptions of his or her vulnerability to a disease, theseriousness of the disorder, and the relative benefits-and costs of recommended action are interacting factorsthat largely determine what the person does with re-Spect to health matters. (55) Certain beliefs abouthealth, social sanctions, or-cultural norms of appro-priate health and illness behavior, the person's rela-tionship with the people in the health care system, andsatisfaction with the care given are other factors thathave been identified as influencing the patients' ad-herence to therapeutic regimens.
Adherence to medical regimens is a complex pheno-menon. For persons with hypertension, the issue ofadherence is heightened because the disorder is generally
asymptomatic at the very time when following the pre--scribed plan of care would be the nost advantageous inpreventing end organ damage. Strategies that have beenreported to have some degree of success in increasingadherence to medical regimens are development of a con-tinuing relationship between the patient and care pro-vider, behavioral contracting, involvement of social
, support groups, patient education environmental mani-pulation, and combinations of several or all of thesestrategies. Continued research into factors that in-fluence and nay be predictive of adherence behavior isneeded.
The prevailing model of adherence or compliancebehavior has been criticized for the implied depictionof the patient as a passive recipient of instructions.Should the regimen not be followed as prescribed, thepatient is viewed as defaulting. (56) More inquiryis needed into the patient's perception of the influenceof the regimen on his or her life situation. In thefinal analysis, the extent of adherence is a personaldecision for everyone with high blood pressure; how-ever, this point of view is at present not frequentlyreflected in the literature.
The issue of adherence has been closely allied toiatient education in many reports and studies.
Nurses frequently assume major responsibility forpatient and family education in such matters as the'characteristics of high blood pressure medications.-diet, stress reduction, and exercise. Increasingly,owever, knowledge alone has not been found to be pre-diátive of,persons seeking health care or of thosefollowing optimum plans of care.
Both nursing and health education literature havebeen generally consistent in urging attention to the-pony factors entering into the teaching-learning pro-cess, including racial and ethnic characteristics of,the hypertensive individual, motivation, readinessto learn, learning styles, environment, and resourcesavailable. Less attention has been given to the1,1earner's perception of the interaction and potential,usefulness, the relationship between the teacher and_--the learner, and the teacher's characteristics.
Patient teaching should enabre persons who must'monitor and control their blood pressurn to participate,meaningfully in the planning for and management of their:iown health. Sensitive efforts to identify particularlearner needs which nay be related to social or cultur--al patterns are especially important. In lifelong man--agement of blood pressure periodic reassessment of
29
patient learning needs are necessary. This should bedone when changes in the healfh regimen are indicatedor changes are occurring in the patient's life or lifestyle which may affect his or her blood pressure suchas pregnancy, illness, or new stressors.
After searching the literature for,information re-lated to.educational programs for patients with highblood pressure, a nuMber of questions were left un-answered. These include the following:
Timing: Are programs implemented at the time ofdiagn6Sis-more or less effective than thosa,implementedlater in the treatment program? is following the.therapeutic.regimen dependent on stages of acceptance ofthe diagnosis and its consequences? If there are de-finable stages of acceptance of diagnosis, what are theindicators of these stages?
Motivation; What motivational factors influenceacquisition Of health/illness knowledge? What factorsinfluence adherence to a therapeutic reginen? How canthese factors be most,easily identified so that theteacher (nurse) can utilize the teadhing strategy or,strategies that best capitalize on these factors?
Content: is there a difference in acquisition ofknowledge and change in behavior wheh-one segment ofknowledge is presented at a tine (diet, medicationinformation, risk factors, blood pressure monitoring,etc.) versus providing information on all subjectsduring each teaching-learning encounter?
Continuous. Learning; What frequency, which methods,and what resources (human and .material) are the mosteffective for reinforcement of learning for persons witha chronic asynptomatic disorder requiring adherence toA therapeutic regimen for controI,of the disease pro-cess? Axe these different from reinforcement of learn-ing for persons with other chronic disorders?
Some other issues and problems recommended for in-
vestigation by nurse researchers include:
1. The efficacy of different teaching strategieson patient learning outcones.
2. The problens of coping with long-term therapyexperienced by hypertensive patients.
3. The efficacy of various nursing interventionsthat would complement medical treatment.
30
Factors influencing the cooperative efforts ofthe patient and health professionals for achiev-
..ing health goals.
The influence of psychosocial and cultural:factors on adherence behavior.
The'relationship between control of hyperten-_Sion and the psychophysiological characteristicsof individuals over time.
31
REFERENCES
National High Blood Pressure Education Program."Report to the Hypertension Information and Edu-
cation Advisory Committee," Task Force I, DataBase, September 1, 1973.
National High Blood Pressure Education Program."Report to the Hypertension Information and Edu-cation Advisory Committee," Task Force II, Pro-
fessional Education, September 1 1973.
National High Blood Pressure Education Program.
"Report to the Hypertension Information and Edu-cation Advisory Committee," Task Force III, Com-munity Education, SepteMber 1, 1973. DHEW Pub-lication No. (NIH) 74-595.
4 National High Blood Pressure Education Program."Report to the Hypertension Information and Edu-
cation Advisory Committee,"Task Force IV, Re-
source and Itpact Assessment.
5. Dustan, Harriet (Chairperson) . "Education of Physi-
cians in High Blood Pressure," Report of the Work-ing Group on the Training and Evaluation of Physi-cians in High Blood Pressure. Circulation, 1975,
pp. 13-27.
6. Shanahan, Maryanne, and Walker Patricia H. "ASilent Illness: Clinical Basis and ComparativeAnalysis of Nursing Audit Criteria for EssentialHypertension." 211!.11-Ly_lityiellftLia, 5-6-7:
15-25, May, June, July 1975.
7. Wilber, Joseph A., McCombs, Nova Jane. "TheAllied Health Professionals' Role." Drug_Therapy,June 1975,, pp. 83-91.
8. National League for Nursing. "Nursing Educationin the Seventies." New York: The League, 1973.
9. Finnerty, F.A., Jr. "The Nurse's Role in TreatingHypertension." New En land Journal of Nedicne,293:93-94, July 1975.
10. Finnerty, F.A., Jr., Mattiee Finnerty, F.A. III."Hypertension in the Inner City. I. Analysis of
Clinic Dropouts." Circulation, 47: 73, 1973.
32
11. Finnerty, F.A.1 Jr., Shaw, L.W., Hamelsback, C.K."Hypertension in the Inner City. II. Detection andFollow-up." Circulation, 47: 76, 1973.
12. Alderman, M.H., and Schoenbaum, E.E. "Detectionand Treatment of Hypertension at the Work Site."New England Journal of Medicine, 293:65-68, 1975.
Robinson, A.M. "The RN's Goal Under 90 mm HgDiastolic." RN Magazine, 293: 43-49, May 1974.
Schlotfeldt, Rozella. "Can We Bring Order Out ofthe Chaos in Nursing Education?" American Journalof Nursing, 76:105-106, January 1976.
l5. Preis, Edward D. The Nature and Plana ement ofHypertension. Bowie, MD: Robert J. Brady, 1974.
The HYpertension Handbook. Merck Sharp & Dohme incooperation with the National High Blood PressureEducation Program, 1974.
1 . Kaplan, Norman M. cliELEaljEllusE.ILarl. New York:Medcom Press, 1973.
Laragh, John H. Hypertension Manual: Mechanisms,Methods, Mana_ement. New York: Yorke MedicalBooks, 1974.
,19. Pickering, George W. Hi h Blood Pressure 2nd ed.)New York: Grune & Stratton, 1968.
20. Aagaard, George N. "The Management of Hypertension.journal of American Medical Associa ion 224:329-
1. Borhani, N.O. "The Control of Elevated Blood Pres-sure in the Community--an Epidemiologic Perspective."Heart and Lung, 3(3), May-June 1974.
22. "Correcting Common Error in BP Measurement." ProgrammedInstruction. American Journal of Nursin- 65:133,Octdber 1965.
Frohlich, E.D. "Hypertension 1973: Treatment--Whyand How." Annals of Internal Medicine 78:717-723,_
May 1973.
-24. Lew, Edward A. "High Blood Pressure, Other RiskFactors and Longevity: The insurance Viewpoint."American Journal of Medicine, 55(3):281, March 1974.
33
25. Wilber, J.A. "Hypertension--A Community Problem."American Journal of Medicine, 52:653-663, May 1972.
26. Wood, J.E. " Primary Prevention of Hypertension."Circulation, 42:A39-41, July 1970.
27. Kannell, W.B. Epidemiologic Assessment of theRole of Blood Pressure in Stroke. The FraminghamStudy. Journal of American Medical Association,214:301, 1970.
28. Karmen, W.B. Role of Blood Pressure in,theDevelopment of Congestive Heart Failure. TheFramingham Study. New En land Journal of Medicine,287:781, 1972.
29. Veterans Administration Cooperative Study Group onAntihypertensive Agents. "Effects of Treatment onMorbidity in Hypertension 1. Results in Patientswith Diastolic BP Averaging 115-129 mm Hg." Journalof American Medical Association, 202: 1098, 1967._
30. Veterans Admanistration Cooperative Study Group onAntihypertensive Agents. "Effects of Treatment onMorbidity in Hypertension, II. Results in Patientswith Diastolic BP Averaging 90-114 mm Hg-"-Journalof American Medical Association,213:1143, '1970.
31. Veterans Administration Cooperative Study Group onAntihypertensive Agents. "Effeqs of Treatment onMorbidity in Hypertension, III: Circulation,45:991, 1972.
32. Levi, Lennart, ed. "Emotions, Their Parameters andMeasurement." Psychol22ica1 Stress. New York:Raven Press, 1975.
33. Benson, H.; Rosner, B.A.; Marzetta, B.R.; Klemchuk,H.P. "Decreased Blood Pressure in Borderline Hyper-tensive Subjects Who Practiced Meditation." Journalof Chronic Disease, 27(3):163-169, March 1974.
Gilmore, Joseph P. "Physiology of Stzess." InStress and the_Heart, edited by Robert S. Eliot. NewYork: Futura Publishing Co., 1974.
35. Bonnano,.J.A., and Lies, J.I. "Effects of PhysicalTraining on Coronary Risk. rican Journal ofCardiblogy, 33:760, 1974.
36. Patel, Chandra. "Twelve Month Follow-up of Yogaand Biofeedback in the Management of Hypertension.The Lancet, (I) 7898:62-64, January 11, 1975.
34
Schwartz Gary E., and Shapiro, David. "Biofeed-back and Essential Hypertension: Current Findingsand Theoretical Concerns." Seminars in Psychiatry,5(4) :493-503, November 1973.
Shapiro, Davi_ "On the Psychophysiology of Stress:IA Commentary in Stress and the Heart, Robert S.Eliot, (ed.). New York: Futura Publishing Company,
Gutmann, Mary C., and Benson, Herbert. "Interactionof Environmental Factors and Systemic Arterial BloodPressure: A Review. Medicine, 50 (6) :543-553, 1971.
40. Boyer-, John L., and Kasch, Fred W. "Exercise Therapyin Hypertensive Men." Journal _of American_edicalAssociation, 211:1668-1671, March 9, 1970.
Weiner, H. "PsYchosomatic Research in EssentialHypertension: Retrospect and Prospect." InEachosor, edited byM. Roster, H. Musaph, and P. Visser. Basel: S. Karger,1970. P. 104.
42. Henry, James P., and Cassel, John C. "PsychosocialFactors in Essential Hypertension: Recent Epidemiologicand Animal Experimental Evidence." American Journal2.1LEELierraa, 90:171-200, September 1969.
Syme, S. Leonard, et al. "Social Class and RacialDifferences in Blood Pressure." American Journalof Public Health, 64:619-620, June 1974.
-44. Harburg, Ernest, et al. "Sociological Stressor Areasand Black-White Blood Pressure: Detroit." Journalof Chronic Disease, 26:595-611, 1973.
45 Kasl, Stanislav V., "Issues in Patient Adherence toHealth Care Regimens." Journal of Human Stress, 5-12,September 1975.
6. Conte, Adrea; Brandzel, Merle; Whitehead, Susan."Group Work with Hypertensive Patients." AmericanJournal of Nursing, 74:910-912, May 1974.
deTornyay, Rheba. St a e ies for Teachin NursinNew York: John Wiley and Sons, 1971.
Gronlund, Norman E. Preparing Criterion-ReferencedTests_for Classroom Instruction. New York: McMillan,1973.
Mager, Robert F. Preparing Instruciional_Ob'ectives.Palo Alto, Calif.:- Fearon, 1962.
35
50. Redman, Barbara K. The Process of Patient Teachin-in Nursing. (2nd d.) St. Louis: C.V. Mosby, 1972.
51. Reilly, Dorothy E. Behavioral Objectives in Nursing:Evaluation of Learner Attainment. New York: AppletorCentury-Crofts, 1975.
52. Schweer, Jean E. Creative Teaching in_CliniealNursing. (2nd ed.) St. Louis: C.V. Mosby, 1972.
53. Weisgerber, Robert A. Perspectives in InaividualizedLearning. Palo Alto, CA: F.E. Peacock, 1971.
54. Baumann, R., et al. "The Influence of Acute PsychicStress Situations on Biochemical and Vegatative Para-meters of Essential Hypertensives at the Early Stageof the Disease." Psychotherapy, Psychosomatics,22:131-140, 1973.
55. Becker, Marshall H. "The Health Belief Model andPersonal Health Behavior." Heal h Education_ Mono7graph, 2:4, Winter 1974.
56. Stimson, Gerry V. "Obeying Doctor's Orders: A Viewfrom the Other Side. Social Science Medicine, 8:97-'04, 1974.
36
NATIONAL HIGH BLOOD PRESSURE EDUCATION PROGRAM
ORDER FORMApril 1977
High Blood Pressure Information Center120/80 National Institutes of HealthBethesda, Maryland 20014(301) 652-7700
For more than sample copies of any item, a distribution plan must be attachedcontaining:
1. A description of your high blood pressure program and itsservices (including the sponsoring agency or group(s);
2. The audience for whom the materials are intended;%. Howtha 71,ntArinic will Iv digs,minatiad;4. The objective you wish to accomplish.
ALLOW SIX WEEKS FOR DELIVERY
Name
Street
City
Phone No. Include Area Code
ganiza ion
State
-Quantity
Zip
76
CONSUMER EDUCATION MATERIALS
Get Your Blood_Eressure_Taken Beforejour Number's_Up(fryer, 3-3/4" x 9" folded) Red, black, and white 6-panelflyer developed for a general audience.
Tomese La Presion Antes I e Le L e e Su Numerolyer, 3 4" x 9" ol e penis_ language version of "Get
Your Blood Pressure Taken Before Your NUMber's Up."
(76-690) S'k Ud Tiene Alta La Presion De Sangre, No Se Arriesque(fxr:-::', 3-374" x 9" folded) Orange and white 6-panel flyerin Spish with message if you have high blood pressure, don'ttake cliances. Directed to the diagnosed hypertensive.
(76-420) Don't Take Chances With Hithillood Pressure(flyer, 4" x 8-3 4" folded) Black and white 4-panel flyerdirected to Black audience.
483) Watch Your Blood Pressureboo let, 28 pages Outlines the nature and physical characteris icsof blood pressure both normal and high, with a description ofvarious types of hypertension.
What Every Woman Should Know About High Blood Pressure(flyer 3-3/4" x 8-112" folded) Buff and brown 6-panel flyerdirected to women. Text adapted from an article which appearedin Family Health Magazine.
High Blood Pressure Control Is Good Insurance(flyer 3-1/2" x 8-1/2", foldedl Red, white and blue 6-panel flyeraddresses hypertension control in relation to life expectancy andinsurance. Developc ,iith cooperation of Associated-LifeCompanies, Inc.
Q
MA _RIALS FOR HEALTH CARL P _CTITIONERS
(76-744 ) Guidelines for the Evaluation and Mana ement of the H ertensiveatient. A 20-page ocument wiic outlines recommen ations
screening, evaluation, and treatment of high blood pressure.Developed in cooperation with the American Academy of FamilyPhysicians.
Outline of Recommended Antihypertensive Regimensa desk top card, 12" x 9") Produced by the American Heart
Association and adapted from Task Force I Report of the NationalHigh Blood Pressure Education Program, this handy desk card out-lines regimens for groups with varying degrees of hypertension asindicated by diastolic pressure. It includes basic dosages andtime recommendations.
(76-627) Summary of the "The Public and High Blood Pressure: A Survey"Summary of a survey conducted for the National Heart and LungInstitute by Louis Harris & Associates which provides data onsources used by the public for health information and publicawareness and attitudes about hypertension.
Education of Physicians in High Blood Pressure(article reprint, Circulation, May 1975, 20 pages) Report of theWorking Group on the Training and Evaluation of Physicians in HighBlood Pressure, chaired by Harriet Dustan, M.D., recommendsperformance characteristics, learning objectives, and evaluationapproaches.
A S a Recommendations o_ the National Pharmac osion g 00. pressure artic e reprint, ourna o
American Pharmaceutical Association, April 1975, 8 pages) Presentsrecommendations ofa cross section of the profession on thepharmacist's role in community outreach, screening, evaluation andtreatment, therapy, monitoring and follow-up, patient education,and quality care assurance.
(77-1088) Report of the Joint National Committee on Detection,Evaluation, and Treatment of High Blood Pressure.16 page document with recommendations for diagnostic teststests, stepped care approaches and long-term maintenance.
(Available summer 1977)
GENERAL INFORMATION ON THE NATIONAL PROGRAM
76-632) Fact Sheet(flyer, 3-1/2" X 8-1/2" folded) Orange, black and white 8-panelflyer presents a description of the purpose of the National HighBleed Pressure Education Program, its organization and-services.
tity
(77-1086
MATERIALS FOR PROGRAM PLANNERS/MANAGERS
Handbook_for ovin- Hi-4 Blood Pressure Control in the Communi105 pages The Handbook contains meani Of identifying community
needs and resources, plans for determining appropriate programpriorities, mechanisms for evaluating program activities, and or-ganizational methods.
(75-715) Medical Basis for Co rehensive Comm Hrertension Control68 Pages Monograp prepare by the Special Tas Force on HYPerten-,sion for the Regional Medical Program Service which presents currentknowledge on the epidemiology of blood pressure; principles ofcommunity organization; and methods of developing optimal screening,referral, diagnosis, treatment and follow-up systems.
(75-755) High_Blood Pressure in the United StatesJerethiah Stamler, rePrinted from the Report of Proceedings,National Conference on High Blood Pressure, January 15, 1973.(55 pages) Provides an overview of the problem of hypertensionincluding the problem of inadequacy of care. It concludes with aseries ofTrogrammatic proposals for the e-P1 rol of hypertension.
(75-545) 120/80_Notebook(58 pageS) Contains suggestions, ideas, _ and other infor-mation for developing consumer education activities in communityhigh blood pressure programs.
-719) Catalog_of Audio-Visual Aids in Hypertension(110 pages) List' films, filMstripS, video cassettes, audio cassettesand Slides produced by corporations, associations, agencies, servicesand other resource organizations. Includes aids for professional,patient and consumer audiences.
(76-105 Supplement to Catalog of_Audio7Visual_ Aids_in_Hypertension(47 pages1 Updates Catalog of Audio-Visual aids in Hypertensionthrough February 1975.
(75-724 ) Patient Education In_ Hi h Blood Pressure_ Art Annotated Biblio ra h(63 pages_ ) A bibliography designed to assist in .the selection oeducational materials which are both scientifically- accurate andvisually attractive. It contains sections of materials for thegeneral public, for professionals.
(76-741) Guidelines_for_the Use of Volunteers_ for High _Blood PressureEducation, Detection and Control Prorams. (17 pageil Presentssuggestions for the types of hypertension control activities towhich volunteers can contribute and recommends approaches useful inrecruiting and training volunteers.
4 0
SPECIALTY ITEMS
The'following are aids in establishing (or conducting) community detec ion/education/-control programs Please include specific distribution information if quantities arerequested.
"Down With High Blood Pr ssure" lapel stick-on badge, 2" diameter.Red and white badge with message and high blood pressure symbol. Usefulfor screenings, patient education, meetings, etc.
"High Blood Pressure is a Time Bomb Only You Can Sto Take yourPills Eve Not Just When You Feel Bad." (16" x 2 heavystódk_ Black and white poster. Picture of:a healthy, smilingblack man with his daughter on his shoulders.
Same copy as above. Picture of middle aged black couple.
"Conozco Su Numero" Poster (16",x 21", heavy stock)Red, black and white Spanish-language poster using roulette wheel toillustrate that it's a gamble to take chances with high blood pressure.
FOR MORE INFORMATION
In!;addition to distributing materials listed here, the High Blood Pressure InformationCenter serves as a central ru 'onal clearinghouse for information on various aspects6f)lypertension .control and can assist in locating speakers and other sources ofpdUcat,ional materials and audiovisual aids.
HIGH BLOOD PRESSURE INFORMATION CENTER120/80 National Institutes of HealthBethesda, Maryland 20014
DISCRININATION PROHIBITED: Under provisions of applicablepublic laws enacted by Congress since 1964, no person inthe United States shall, on the ground of race, color,national origin, sex, or handicap, be excluded from partici-pation in, be denied the benefits of, or be subjected todiscrimination under any program or activity receivingFdderal financial assistance. In addition, Executive Order11141 prohibits discrimination on the basis of age by con-'tractors and subcontractors in the performance of Federalcontracts. Therefore, the NATIONAL HIGH BLOOD PRESSUREEDUCATION PROGRAM must be operated in compliance with theselaws and executive order.





























