Embed Size (px)
Citation preview

SURGERY FOR MOVEMENT DISORDERS
MOVEMENT DISORDERS, SUCH as Parkinson’s disease, tremor, and dystonia, areamong the most common neurological conditions and affect millions of patients.Although medications are the mainstay of therapy for movement disorders, neurosurgeryhas played an important role in their management for the past 50 years. Surgery is nowa viable and safe option for patients with medically intractable Parkinson’s disease,essential tremor, and dystonia. In this article, we provide a review of the history, neuro-circuitry, indication, technical aspects, outcomes, complications, and emerging neuro-surgical approaches for the treatment of movement disorders.
KEY WORDS: Deep brain stimulation, Dystonia, Essential tremor, Globus pallidus pars interna, Movementdisorders, Parkinson’s disease, Stereotaxis, Subthalamic nucleus, Ventralis intermedius nucleus
Neurosurgery 62[SHC Suppl 2]:SHC809–SHC839, 2008 DOI: 10.1227/01.NEU.0000297003.12598.B9
MOVEMENT DISORDERS
Ali R. Rezai, M.D.Center for Neurological Restoration, andDepartment of Neurosurgery,Cleveland Clinic,Cleveland, Ohio
Andre G. Machado, M.D., Ph.D.Center for Neurological Restoration, andDepartment of Neurosurgery,Cleveland Clinic,Cleveland, Ohio
Milind Deogaonkar, M.D.Center for Neurological Restoration, andDepartment of Neurosurgery,Cleveland Clinic,Cleveland, Ohio
Hooman Azmi, M.D.Center for Neurological Restoration, andDepartment of Neurosurgery,Cleveland Clinic,Cleveland, Ohio
Cynthia Kubu, Ph.D.Center for Neurological Restoration, andDepartment of Psychiatry,Cleveland Clinic,Cleveland, Ohio
Nicholas M. Boulis, M.D.Center for Neurological Restoration, andDepartment of Neurosurgery,Cleveland Clinic,Cleveland, Ohio
Reprint requests:Ali R. Rezai, M.D.,Center for Neurological Restoration,9500 Euclid Avenue, Desk S31,Cleveland OH 44122.Email: [email protected]
Received, May 30, 2007.
Accepted, November 1, 2007.
Historical Perspective
Various surgical approaches, such asresection, lesioning, stimulation, andothers, have been used to treat patients
with movement disorders. Craniotomies wereperformed for the resection of the motor cortex(68), cerebral peduncles (381, 382), and a vari-ety of subcortical lesioning procedures (326).Irving Cooper (72a) first reported the effects ofligation of the choroidal artery for Parkinson’sdisease (PD) in 1953. Six patients were treatedwith eight ligations, which resulted in signifi-cant alleviation of rest tremor, rigidity, andcontralateral cogwheeling. It was not until theintroduction of stereotaxis by Spiegel et al.(328) in 1947, and later by Leksell (206) in 1949,that a more accurate, less invasive, and moreconsistent placement of lesions in various sub-cortical locations became feasible.
The development of stereotaxy led to a vari-ety of lesioning procedures of the basal gangliaand the thalamus for the treatment of rigidityand tremor in the 1950s and 1960s. Various sur-gical techniques, lesion locations, lesion sizes,and outcomes were reported (77, 256, 327, 392).The motor thalamus and the pallidal targetslying in the ventral and posterior portions ofthe globus pallidus internus (GPi) as well asthe pallidal projections were considered to bethe most effective targets. However, it was theadvent of L-dopa in the mid-1960s and its sig-nificant clinical benefits that led to a dramaticdecrease in surgery for PD. For the next 20years, surgery for movement disorders was
predominantly limited to thalamotomy (8,115–117, 149, 167, 254, 275, 343) for the treat-ment of tremor and pallidotomy and thalamo-tomy for dystonia (224, 341, 371, 383). PD sur-gery was rarely performed during this time. Itwas not until the late 1980s that there was areemergence of interest in the neurosurgicaltreatment for PD due to the increasing realiza-tion of the limitations of PD medications andthe side effects of L-dopa. This led to a resur-gence of lesioning surgeries such as pallido-tomies for PD. The initial Leksell (336) target ofpallidal lesions for treatment of PD was modi-fied and repopularized by Laitinen et al. (196,197). Original analytical descriptions of thala-mic nuclei and circuitry by Hassler (142),Hassler et al. (143), and Macchi and Jones (230)and basal ganglia circuitry by Delong et al. (81,82) also served as a foundational substrate fornewer targets for therapeutic interventionsusing stereotactic techniques.
The ability of electrical impulses to modifyfunctional outcome in certain brain regionswas identified almost 200 years ago, in 1809,by Rolando (98). Aldini had previouslyattempted to stimulate the brains of executedcriminals immediately after death by applyingcurrent from voltaic piles (98). The use of elec-trical stimulation to understand and map thefunction of the human brain and its circuitrybecame commonplace in the 20th century (4,64, 65, 291). Early explorations by Hassler et al.revealed that acute low-frequency stimulationduring stereotactic exploration for ablation of
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC809
ONLINEDIGITAL
VIDEO

the pallidum could augment tremor, whereas high-frequencystimulation at 25 to 100 Hz had the opposite effect (143). Theseobservations paved the way for the future development ofchronic electrical stimulation therapies for the management ofmovement disorders.
The first systematic use of chronic deep brain stimulation(DBS) for the treatment of movement disorders is attributed toBechtereva et al. (22) in Russia. Beginning in 1967, theyreported benefits with chronic DBS of the thalamus, striatum,and pallidum. But it was not until the 1980s that Brice andMcLellan (54), Blond and Siegfried (52), Siegfried and Shulman(319), and Benabid et al. (34, 36) published reports of the use ofchronic electrical stimulation or DBS for the treatment of move-ment disorders, thus ushering in a new era of functional neu-rosurgery for movement disorders.
DBS has similar efficacy as that reported with various lesion-ing procedures (e.g., pallidotomy, thalamotomy). However, thesuperior safety profile of DBS relative to lesioning procedures,particularly bilateral thalamotomy and pallidotomy, has madeit the procedure of choice in countries where access to this tech-nology is available
DBS, with its inherent features of reversibility and adjustabil-ity, has gained popularity and emerged as the neurosurgicalstandard of care for movement disorders such as PD, dystonia,and essential tremor over the past 20 years (6, 9, 25, 32, 33, 37,70, 101, 187, 193, 201, 202, 227, 252, 268, 274, 280, 293, 294, 343,351, 357, 394). Since its inception, more than 40,000 DBSimplants have been performed in more than 500 centers world-wide (28). In addition to the widespread use of DBS for move-ment disorders, a number of clinical investigations using DBSare under way to explore its safety and efficacy for conditionssuch as Tourette’s syndrome (14, 88, 111, 155, 243, 266, 322,366), chronic pain (48, 69, 119, 188, 210, 295), and psychiatricdisorders such as depression (60, 109, 238, 310, 314) andobsessive-compulsive disorder (OCD) (73, 121, 122, 190, 242,386). Because DBS is the most commonly used neurosurgicalprocedure for the treatment of movement disorders, it is themajor focus of this article.
Neural Circuitry of Movement Disorders
Traditionally, surgical procedures have targeted the knownanatomic subcortical gray or white matter regions implicated inthe circuitry and the pathophysiology of movement disorders.As discussed above, a long history of lesioning procedures forthe treatment of movement disorders has provided a wealth ofempirical evidence supporting the presumed underlying neu-rocircuity associated with the aberrant motor symptoms.During the past two decades, technological advances in struc-tural and functional brain imaging and physiological brainmapping, coupled with animal research, have further advancedour understanding of the underlying neurocircuitry of specificmovement disorders, and led to additional refinement of thesurgical targets.
The use of animal models has contributed significantly to abetter understanding of the pathophysiology and underlying
neurocircuitry of PD and other movement disorders (2, 29, 39,41, 53, 56, 62, 83, 99, 120, 133, 135, 144, 152, 204, 205, 209, 223,234, 239, 241, 246, 248, 249, 262, 273, 283, 292, 320, 325, 332, 340,343, 385, 391). These data provided support for the concept ofthe cortico-striatal-pallidal-thalamic-cortical (CSPTC) circuits.Alexander et al. (7) hypothesized that a network of five parallel,segregated circuits exists that underlies a variety of functions.These circuits originate in various regions of the frontal lobesand then traverse through different nodes in the striatum, pal-lidum, and thalamus before returning to their cortical points oforigin. One of these circuits underlies complex motor functionand is implicated in the pathophysiology of PD.
The concept of a CSPTC motor circuit or loop implies that anumber of the nodes involved in the circuit are potential targetsfor neuromodulation including neurosurgical procedures suchas lesioning and DBS, somatic or stem cells, or gene therapy.
In the CSPTC circuitry model, the striatal structures, such asthe caudate and putamen, serve as the input structures,whereas the GPi and substantia nigra pars reticulata (SNr) arethe primary output structures. The motor circuit originates inthe precentral motor regions (especially Brodmann areas 4 and6). Information passing through the basal ganglia is organizedanatomically though “direct” and “indirect” pathways withinthe CSPTC circuit (Fig. 1). Information in the direct pathwaypasses monosynaptically from the putamen to the output struc-tures of the basal ganglia, the GPi, and the SNr. Informationfrom the indirect pathway passes multisynaptically throughthe globus pallidus externa (GPe) and the subthalamic nucleus(STN) before terminating on the GPi/SNr. The informationfrom both the direct and indirect pathways then projects tovarious thalamic relay nuclei, including the ventral oralis ante-rior (Voa) and ventral oralis posterior (Vop) nuclei (in Hassler’snomenclature) (230). This information is then projected back tothe frontal region of origin, thereby closing the circuit. Thedirect and indirect pathways appear to balance one another.The direct pathway is presumed to be responsible for the initi-ation of action and the indirect pathway for the braking ofaction or the ability to switch from one action to another.
Inhibitory γ-aminobutyric acid (GABA)ergic projections pre-dominate in these pathways. Other than the excitatory gluta-matergic projections from the cortex to the basal ganglia andthe returning excitatory thalamocortical projections, the onlyprojections within the deep subcortical brain structures thatare excitatory are the glutamatergic projections coursing fromthe STN to the GPi/SNr. The most common surgical targetedregions in this circuit are the STN, the GPi, and their associatedCSPTC motor circuit white matter inputs and outputs. Thereare other emerging targets in the CSPTC motor loop that arebeing further investigated, but, given the scope of this review,they will not be discussed.
Dopamine is one of the most powerful neurotransmittersinfluencing the motor CSPTC circuit. Dopamine can have eitheran excitatory or inhibitory role on striatal neurons, dependingon the dopamine receptor subtype: D1 receptors are associatedwith an excitatory effect, whereas D2 receptors are inhibitory.In general, dopaminergic inputs to the striatum serve to reduce
REZAI ET AL.
SHC810 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
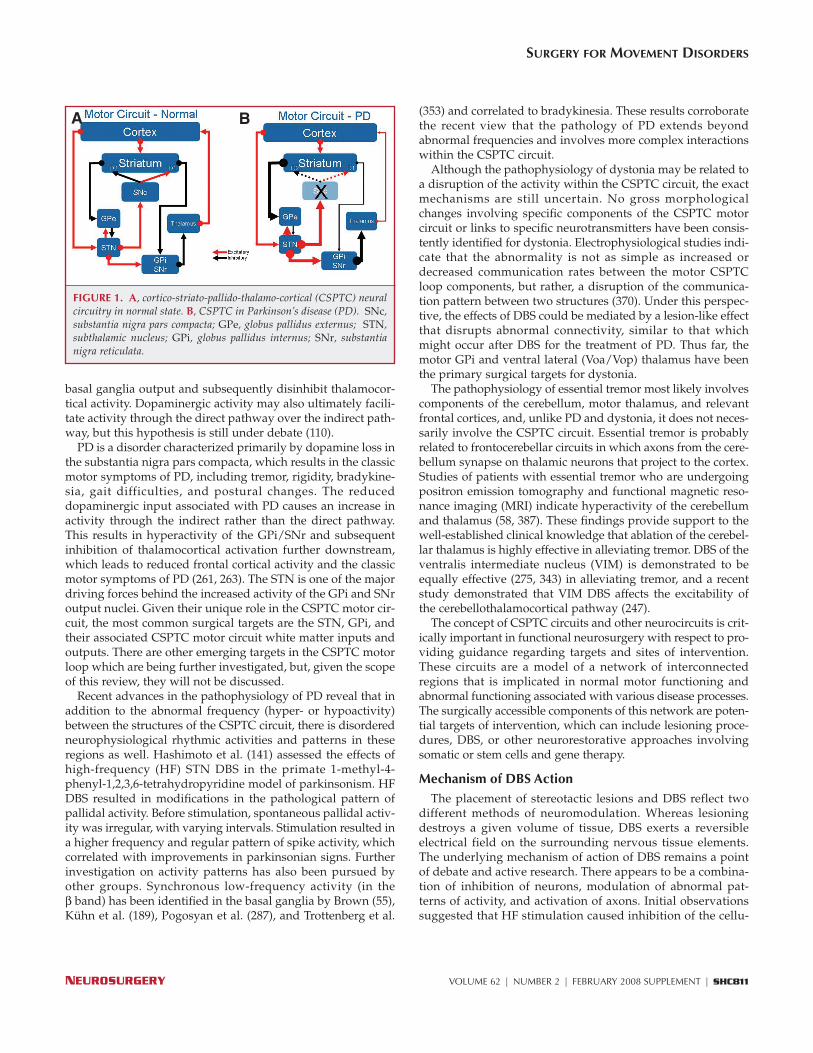
basal ganglia output and subsequently disinhibit thalamocor-tical activity. Dopaminergic activity may also ultimately facili-tate activity through the direct pathway over the indirect path-way, but this hypothesis is still under debate (110).
PD is a disorder characterized primarily by dopamine loss inthe substantia nigra pars compacta, which results in the classicmotor symptoms of PD, including tremor, rigidity, bradykine-sia, gait difficulties, and postural changes. The reduceddopaminergic input associated with PD causes an increase inactivity through the indirect rather than the direct pathway.This results in hyperactivity of the GPi/SNr and subsequentinhibition of thalamocortical activation further downstream,which leads to reduced frontal cortical activity and the classicmotor symptoms of PD (261, 263). The STN is one of the majordriving forces behind the increased activity of the GPi and SNroutput nuclei. Given their unique role in the CSPTC motor cir-cuit, the most common surgical targets are the STN, GPi, andtheir associated CSPTC motor circuit white matter inputs andoutputs. There are other emerging targets in the CSPTC motorloop which are being further investigated, but, given the scopeof this review, they will not be discussed.
Recent advances in the pathophysiology of PD reveal that inaddition to the abnormal frequency (hyper- or hypoactivity)between the structures of the CSPTC circuit, there is disorderedneurophysiological rhythmic activities and patterns in theseregions as well. Hashimoto et al. (141) assessed the effects ofhigh-frequency (HF) STN DBS in the primate 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine model of parkinsonism. HFDBS resulted in modifications in the pathological pattern ofpallidal activity. Before stimulation, spontaneous pallidal activ-ity was irregular, with varying intervals. Stimulation resulted ina higher frequency and regular pattern of spike activity, whichcorrelated with improvements in parkinsonian signs. Furtherinvestigation on activity patterns has also been pursued byother groups. Synchronous low-frequency activity (in theβ band) has been identified in the basal ganglia by Brown (55),Kühn et al. (189), Pogosyan et al. (287), and Trottenberg et al.
(353) and correlated to bradykinesia. These results corroboratethe recent view that the pathology of PD extends beyondabnormal frequencies and involves more complex interactionswithin the CSPTC circuit.
Although the pathophysiology of dystonia may be related toa disruption of the activity within the CSPTC circuit, the exactmechanisms are still uncertain. No gross morphologicalchanges involving specific components of the CSPTC motorcircuit or links to specific neurotransmitters have been consis-tently identified for dystonia. Electrophysiological studies indi-cate that the abnormality is not as simple as increased ordecreased communication rates between the motor CSPTCloop components, but rather, a disruption of the communica-tion pattern between two structures (370). Under this perspec-tive, the effects of DBS could be mediated by a lesion-like effectthat disrupts abnormal connectivity, similar to that whichmight occur after DBS for the treatment of PD. Thus far, themotor GPi and ventral lateral (Voa/Vop) thalamus have beenthe primary surgical targets for dystonia.
The pathophysiology of essential tremor most likely involvescomponents of the cerebellum, motor thalamus, and relevantfrontal cortices, and, unlike PD and dystonia, it does not neces-sarily involve the CSPTC circuit. Essential tremor is probablyrelated to frontocerebellar circuits in which axons from the cere-bellum synapse on thalamic neurons that project to the cortex.Studies of patients with essential tremor who are undergoingpositron emission tomography and functional magnetic reso-nance imaging (MRI) indicate hyperactivity of the cerebellumand thalamus (58, 387). These findings provide support to thewell-established clinical knowledge that ablation of the cerebel-lar thalamus is highly effective in alleviating tremor. DBS of theventralis intermediate nucleus (VIM) is demonstrated to beequally effective (275, 343) in alleviating tremor, and a recentstudy demonstrated that VIM DBS affects the excitability ofthe cerebellothalamocortical pathway (247).
The concept of CSPTC circuits and other neurocircuits is crit-ically important in functional neurosurgery with respect to pro-viding guidance regarding targets and sites of intervention.These circuits are a model of a network of interconnectedregions that is implicated in normal motor functioning andabnormal functioning associated with various disease processes.The surgically accessible components of this network are poten-tial targets of intervention, which can include lesioning proce-dures, DBS, or other neurorestorative approaches involvingsomatic or stem cells and gene therapy.
Mechanism of DBS ActionThe placement of stereotactic lesions and DBS reflect two
different methods of neuromodulation. Whereas lesioningdestroys a given volume of tissue, DBS exerts a reversibleelectrical field on the surrounding nervous tissue elements.The underlying mechanism of action of DBS remains a pointof debate and active research. There appears to be a combina-tion of inhibition of neurons, modulation of abnormal pat-terns of activity, and activation of axons. Initial observationssuggested that HF stimulation caused inhibition of the cellu-
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC811
FIGURE 1. A, cortico-striato-pallido-thalamo-cortical (CSPTC) neuralcircuitry in normal state. B, CSPTC in Parkinson’s disease (PD). SNc,substantia nigra pars compacta; GPe, globus pallidus externus; STN,subthalamic nucleus; GPi, globus pallidus internus; SNr, substantianigra reticulata.
BA

lar activity in the nucleus, thereby mimicking a transientlesion-like effect. Studies show that DBS can induce inhibitionof cellular activity or of neural network functions by either the“jamming” of neural transmission through stimulated nuclei,by direct inhibition of membrane action potentials, by retro-grade activation of upstream neuronal structures, or by theshutting down of neurotransmitter release in the STN (38).Recent experiments demonstrate that HF stimulation of theSTN is accompanied by increased release of glutamate anddopamine in the STN and striatum, respectively (203, 338).Similarly, increased release of GABA in axons from afferentconnections was observed in the GPi of parkinsonian patientsduring DBS surgery (40). It has also been demonstrated thatactivation of a DBS lead placed in the ventral thalamus canrapidly disrupt local synaptic function and neuronal firing,and thereby lead to a “functional deafferentation” and/or“functional inactivation” (13). A recent study of PD patientsafter placement of DBS electrodes in the STN suggests that HFstimulation produces early inhibition with subsequentrebound excitation and another period of inhibition. Thesefindings suggest that the observed inhibitory activity reflectsneuronal hyperpolarization (96). These data further suggestthat STN neuronal inhibition may be accompanied by directexcitation of the cell and/or its axon.
In summary, the growing literature demonstrates the com-plexity of the motor system and the potential mechanisms ofDBS action. The prevailing hypotheses postulate inhibition atthe neuronal level, activation at the axonal level, as well asinterruption of excessive and abnormally patterned neuronalactivity in the STN, GPi, and the interconnected components ofthe CSPTC network (20, 39, 133, 135, 264, 309, 385).
Surgery: The TeamSurgery for movement disorders is most optimally man-
aged in the context of a multidisciplinary team. In addition tothe neurosurgeon, this team should include a movement dis-orders neurologist, a neuropsychologist, a neurophysiologist,and physician extenders such as nurse practitioners andphysician’s assistants. The movement disorders neurologistcan help confirm an accurate diagnosis and rule out atypicalparkinsonism or psychogenic movement disorders. The ben-efit of surgery for a particular movement disorder is largelydependent on accurate diagnosis, as it is the underlyingpathophysiology and neurocircuitry of the specific move-ment disorder that is influenced by surgery. The movementdisorders neurologist can also optimize medications for indi-viduals who have not had adequate medication trials.Occasionally, medication adjustments by an expert can signif-icantly improve the functioning of a patient such that he orshe no longer requires surgery. The DBS programming can beperformed by the neurosurgeon, neurologist, or physicianextenders. As DBS programming results in changes in motorsymptoms, there must be close attention to concomitant med-ication adjustments coupled with rehabilitation (e.g., physi-cal and occupational therapies) to optimize an individualpatient’s motor outcome.
Surgical Patient Selection Criteria
In general, patients must be able to tolerate the various com-ponents of surgery and have the cognitive skills and social sup-port structure to comply with the demands of surgery and thepostoperative care. For those undergoing DBS surgery, boththe patient and the family members need to have a detailedunderstanding of reasonable outcomes, potential complica-tions, and the multiple steps involved in the preoperativeassessments, surgery, and perioperative and follow-up care.The patient needs to cooperate with follow-up programmingand medication adjustments in the outpatient setting. Ad-ditionally, the patient and family should have realistic expecta-tions about surgical outcome, and they should understand thatthe surgery will not cure the disease or stop its natural progres-sion. Neurosurgery for movement disorders can provideimprovements in disabling motor symptoms and motor func-tion. It is important to provide accurate information to thepatient and family members regarding those symptoms thatare likely to respond to surgery versus those that are not.
Patients should be in stable overall health with respect tocardiac, pulmonary, and systemic conditions such as hyperten-sion, diabetes, and cancer. Patients who require anticoagulants,such as warfarin or antiplatelet medication, must be able totolerate complete withdrawal from these medications beforesurgery. Consultation with other medical specialists may berequired before proceeding with surgery.
In recent years, there has been increasing recognition of theneurobehavioral changes associated with PD and other move-ment disorders, including cognitive, mood, and personalitychanges. Neuropsychological assessment is recommended aspart of the preoperative assessment to determine candidacyfor neurosurgical intervention for the treatment of movementdisorders. The neuropsychological assessment should includeassessment of cognition, neuropsychiatric symptoms, socialsupport, and goals for surgery. Patients with severe cognitivedysfunction or dementia on neuropsychological examinationshould be excluded from surgical intervention. Patients withmild cognitive impairment or frontal dysexecutive syndromemay still undergo surgery, but these individuals should havea strong social support structure and receive extra counseling,along with family members, regarding the potential forincreased risks for cognitive impairment and confusion post-surgery. Psychiatric conditions such as anxiety, depression,and mania must be identified and medically optimized by aspecialist preoperatively. Neurosurgical intervention inpatients with delusional psychosis or severe personality dis-order, such as borderline personality disorder, is generallynot recommended.
PD: Selection Criteria
PD is a progressive neurodegenerative disorder resulting inprominent motor abnormalities such as bradykinesia (slow-ness of movement), rigidity (muscle stiffness), tremor, and gaitand postural instabilities. In PD, there is progressive degener-ation of dopaminergic neurons. Administration of L-dopa and
REZAI ET AL.
SHC812 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com

synthetic dopamine agonists is the mainstay of medical treat-ment of PD. However, over time, patients experience a lessfavorable response to medications and may begin a cycle thatincludes increasing medication doses and multiple medica-tions with disabling side effects. Dose escalations can be asso-ciated with motor fluctuations and troublesome dyskinesias(83, 251, 260). Despite major advances in the understanding ofthe pathophysiology of PD and improvements in pharmaco-logical management, there are a substantial number of patientswho are considered refractory to medical management. Suchmedically refractory patients with significant motor complica-tions and disability can benefit from DBS of the STN or GPi.Neurosurgery has been shown to consistently benefit onlypatients with idiopathic PD. Atypical parkinsonism (supranu-clear palsy, nigrostriatal degeneration, etc.) or other disorderswith parkinsonian features have not been shown to respondfavorably to surgery.
In general, surgery is most likely to benefit symptoms affect-ing the extremities rather than axial symptoms that involveposture, balance, gait, and speech. Surgical candidates typi-cally have more than one of the following symptoms: severetremors; off-medication-related rigidity, freezing, dystonia, andbradykinesia; on-medication-related dyskinesias; and signifi-cantly disabling on-off-medication motor fluctuations. One ofthe most important predictors of neurosurgical treatmentresponse is the patient’s response to L-dopa. Patients whodemonstrate a significant improvement in motor symptomsduring L-dopa off-medication versus on-medication states aremost likely to benefit from surgery. The only exception to thisgeneral rule involves tremor. Tremor is the only identifiedmotor symptom that can improve with DBS regardless ofresponse to off-on-medication testing. Consequently, a formaloff-on test of L-dopa responsiveness can be very helpful in theselection of the best surgical candidates.
Tremor: Selection CriteriaEssential tremor is a benign condition (32, 173, 198, 222) that
can be managed for many years with medications. In thosepatients who have disabling extremity tremor despite optimalmedication management, surgery using the VIM targetbecomes an option. In general, patients with resting and distalpostural tremor fare the best with surgery, followed by thosewith proximal postural tremor. Patients with intention/actiontremor tend to benefit to a lesser degree. The more proximaland the action/intention features of tremor are the most diffi-cult and challenging tremor characteristics to treat surgically(44, 85, 169). Head, neck, and lower-extremity tremors are alsomore difficult to treat than upper-extremity tremors. Tremorsinvolving the head, neck, and axial regions usually requirebilateral surgery.
Dystonia: Selection CriteriaDBS offers a therapeutically viable option for patients with
severe, primary dystonia and also for a small subset of patientswith secondary dystonia. The key to favorable responses afterDBS in patients with dystonia is proper patient selection.
Patients who are refractory to all conservative measures,including medication trials (anticholinergics, baclofen, benzodi-azepines, or other muscle relaxants) and botulinum toxin injec-tions are potential candidates.
Dystonia is a heterogenous condition with variable expres-sion. It can be classified into primary or secondary dystoniaaccording to etiology. Primary idiopathic dystonia refers todystonia with no discernible etiological factor responsible forits onset. Patients with primary idiopathic dystonia have nor-mal imaging findings, cerebrospinal fluid composition, andlaboratory test examinations. A subset of patients with pri-mary dystonia have a DYT-1 mutation on chromosome 9q (12).Secondary dystonia refers to dystonia that is associated with aclearly preexisting, identifiable brain insult such as perinatalhypoxia, stroke, trauma, toxin exposure, or infectious sequelae.Tardive dystonia is another subset of dystonia that results fromsuper-sensitivity of the postsynaptic dopamine striatal recep-tors due to long-term administration of dopamine receptor-blocking agents such as neuroleptics (105, 219, 395).
Dystonia can also be classified according to the affected bodypart. In focal dystonia, a single region of the body is affected,such as in blepharospasm (eyes), cervical dystonia/torticollis(neck), and spasmodic dysphonia or laryngeal dystonia (182).In segmental dystonia, two or more adjacent body parts areaffected, such as cranial-cervical dystonia, crural dystonia, orbrachial dystonia. Generalized dystonia refers to dystoniainvolving most body parts.
Primary, generalized dystonia of DYT-1-positive (184, 195,201) or non-DYT-1 types, as well as patients with idiopathiccervical dystonia can obtain the best motor benefits with bilat-eral GPi DBS (363). Patients with juvenile-onset idiopathicdystonia whose age of onset is older than 5 years and who donot have multiple orthopedic deformities also have a goodresponse to surgery (280). Appendicular symptoms (e.g.,those affecting the limbs) appear to respond better than axialsymptoms (201). With regard to focal dystonia, ideal surgicalcandidates are those with cervical dystonia (201, 331). Theresults of DBS for secondary dystonia are inconsistent. In gen-eral, DBS for secondary dystonia is less effective than for pri-mary generalized dystonia, particularly in those patients withan identifiable structural brain abnormality. The only excep-tion is tardive dystonia, which has been reported to respondwell to surgery in a small number of patients (92, 331, 396).
Surgical TargetsThe three most common targets for movement disorder sur-
gery are the STN, GPi, and VIM thalamus. GPi and STN DBSimprove PD symptoms (e.g., tremor, rigidity, and bradykinesia)and also reduce drug-induced dyskinesias. STN DBS alsoreduces the medication burden, thereby reducing medication-associated side effects (80, 59, 368). Both the STN and the GPihave corresponding associative (cognitive), limbic, and motorterritories that require accurate surgical targeting of the motorcomponent. Presently, the most commonly used target for DBStherapy to treat PD is the STN, followed by the GPi. The GPi isalso the most commonly used target for dystonia (66, 100, 159,
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC813
185, 201, 280, 312, 331, 350, 351, 355, 396). The VIM target is themain target used for non-parkinsonian tremor. The VIM is veryeffective in alleviating PD-associated tremors, but is not effec-tive in the treatment of other cardinal PD symptoms. (342, 343).Thus, VIM DBS surgery is rarely performed for PD treatment.
The STN TargetThe STN was previously not considered a target because of
the fear of causing hemiballismus. However, in 1990, Bergmanet al. (42) showed that a lesion in the STN of a nonhuman pri-mate model could reverse the symptoms of PD. This earlywork, coupled with the evolving concept of the flexibility (e.g.,reversibility and adjustability) inherent in DBS for the treat-ment of movement disorders, resulted in Benabid et al. (34)and Pollak et al. (288) applying STN DBS for the treatment ofPD initially in 1993, with report of a subsequent case series in1995 (215). Since that time, STN DBS has become the most com-mon target for DBS surgery for PD. Targeting the STN has beendemonstrated to effectively treat the entire spectrum ofadvanced PD symptoms of tremor, rigidity, bradykinesia,motor fluctuations, and drug-induced dyskinesias, while alsoconsistently reducing the need for dopaminergic medicationpostoperatively.
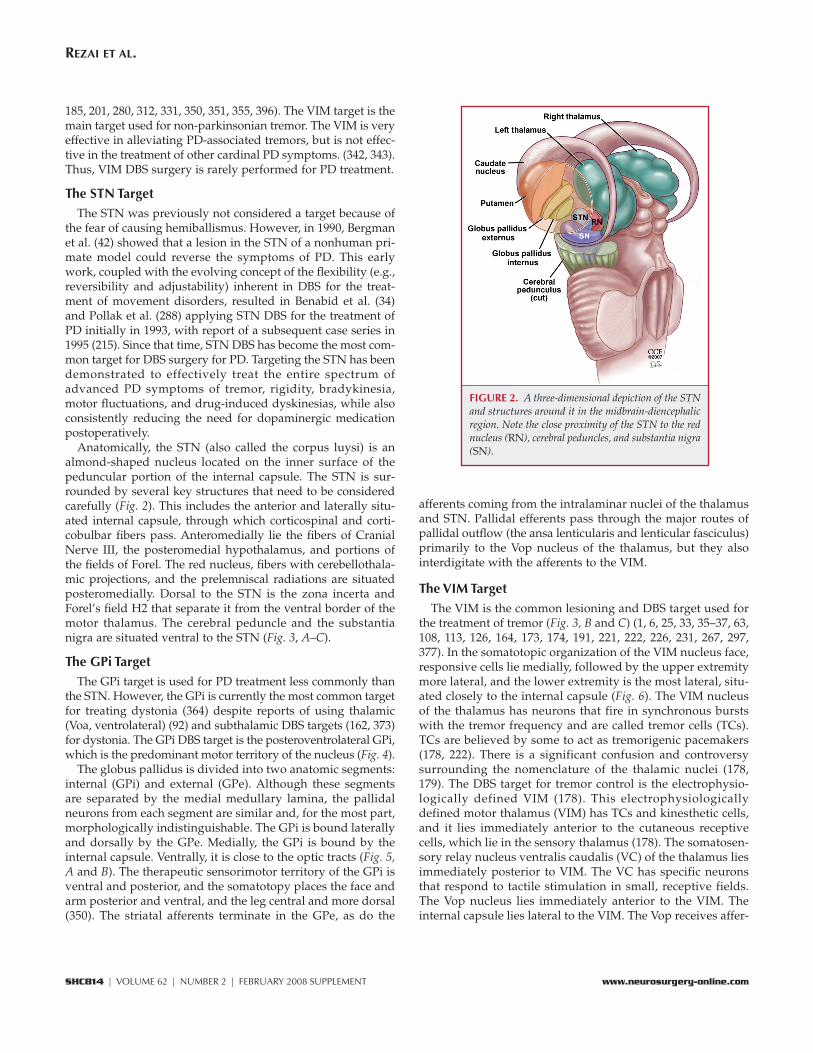
Anatomically, the STN (also called the corpus luysi) is analmond-shaped nucleus located on the inner surface of thepeduncular portion of the internal capsule. The STN is sur-rounded by several key structures that need to be consideredcarefully (Fig. 2). This includes the anterior and laterally situ-ated internal capsule, through which corticospinal and corti-cobulbar fibers pass. Anteromedially lie the fibers of CranialNerve III, the posteromedial hypothalamus, and portions ofthe fields of Forel. The red nucleus, fibers with cerebellothala-mic projections, and the prelemniscal radiations are situatedposteromedially. Dorsal to the STN is the zona incerta andForel’s field H2 that separate it from the ventral border of themotor thalamus. The cerebral peduncle and the substantianigra are situated ventral to the STN (Fig. 3, A–C).
The GPi TargetThe GPi target is used for PD treatment less commonly than
the STN. However, the GPi is currently the most common targetfor treating dystonia (364) despite reports of using thalamic(Voa, ventrolateral) (92) and subthalamic DBS targets (162, 373)for dystonia. The GPi DBS target is the posteroventrolateral GPi,which is the predominant motor territory of the nucleus (Fig. 4).
The globus pallidus is divided into two anatomic segments:internal (GPi) and external (GPe). Although these segmentsare separated by the medial medullary lamina, the pallidalneurons from each segment are similar and, for the most part,morphologically indistinguishable. The GPi is bound laterallyand dorsally by the GPe. Medially, the GPi is bound by theinternal capsule. Ventrally, it is close to the optic tracts (Fig. 5,A and B). The therapeutic sensorimotor territory of the GPi isventral and posterior, and the somatotopy places the face andarm posterior and ventral, and the leg central and more dorsal(350). The striatal afferents terminate in the GPe, as do the
afferents coming from the intralaminar nuclei of the thalamusand STN. Pallidal efferents pass through the major routes ofpallidal outflow (the ansa lenticularis and lenticular fasciculus)primarily to the Vop nucleus of the thalamus, but they alsointerdigitate with the afferents to the VIM.
The VIM TargetThe VIM is the common lesioning and DBS target used for
the treatment of tremor (Fig. 3, B and C) (1, 6, 25, 33, 35–37, 63,108, 113, 126, 164, 173, 174, 191, 221, 222, 226, 231, 267, 297,377). In the somatotopic organization of the VIM nucleus face,responsive cells lie medially, followed by the upper extremitymore lateral, and the lower extremity is the most lateral, situ-ated closely to the internal capsule (Fig. 6). The VIM nucleusof the thalamus has neurons that fire in synchronous burstswith the tremor frequency and are called tremor cells (TCs).TCs are believed by some to act as tremorigenic pacemakers(178, 222). There is a significant confusion and controversysurrounding the nomenclature of the thalamic nuclei (178,179). The DBS target for tremor control is the electrophysio-logically defined VIM (178). This electrophysiologicallydefined motor thalamus (VIM) has TCs and kinesthetic cells,and it lies immediately anterior to the cutaneous receptivecells, which lie in the sensory thalamus (178). The somatosen-sory relay nucleus ventralis caudalis (VC) of the thalamus liesimmediately posterior to VIM. The VC has specific neuronsthat respond to tactile stimulation in small, receptive fields.The Vop nucleus lies immediately anterior to the VIM. Theinternal capsule lies lateral to the VIM. The Vop receives affer-
REZAI ET AL.
SHC814 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
FIGURE 2. A three-dimensional depiction of the STNand structures around it in the midbrain-diencephalicregion. Note the close proximity of the STN to the rednucleus (RN), cerebral peduncles, and substantia nigra(SN).
ents from pallidal neurons (230) and the VIM receives affer-ents from the cerebellar neurons (cerebellothalamic fibers).There is some degree of overlap and interdigitation betweenthese two nuclei (230).
DBS Surgical TechniqueIn this section, we review the general principles and tech-
niques of DBS surgery, which is the most common surgicaltreatment for movement disorders today. Although there is
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC815
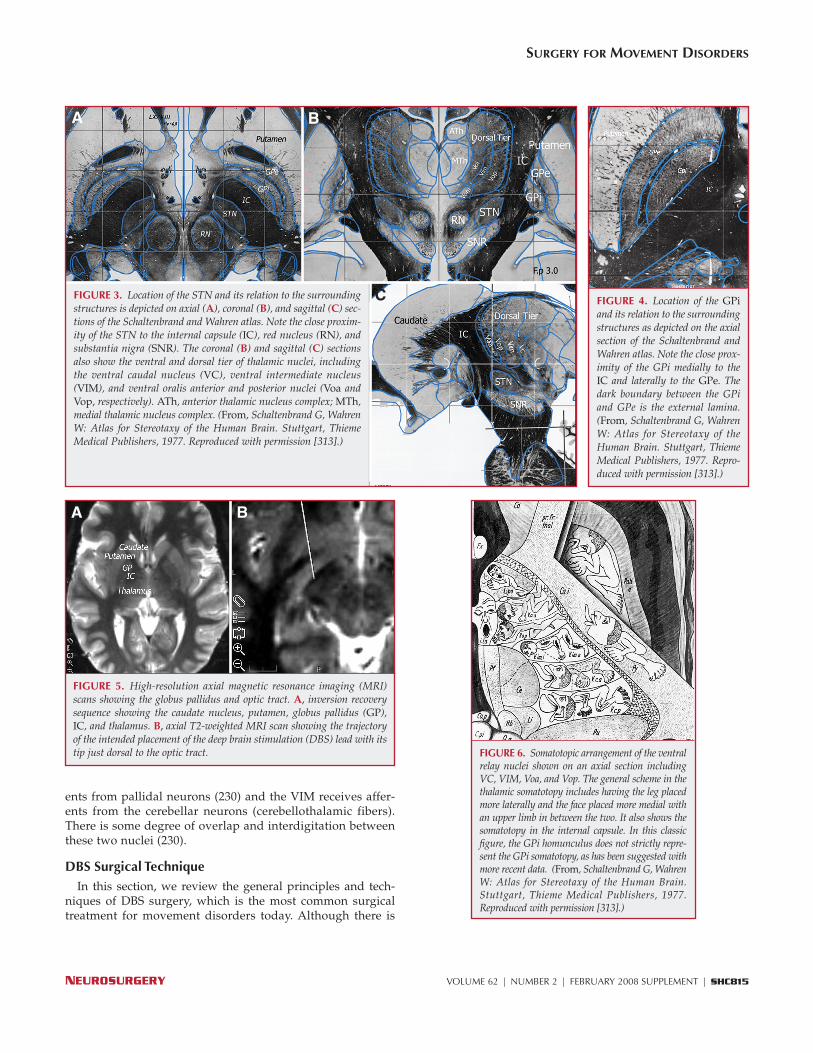
FIGURE 3. Location of the STN and its relation to the surroundingstructures is depicted on axial (A), coronal (B), and sagittal (C) sec-tions of the Schaltenbrand and Wahren atlas. Note the close proxim-ity of the STN to the internal capsule (IC), red nucleus (RN), andsubstantia nigra (SNR). The coronal (B) and sagittal (C) sectionsalso show the ventral and dorsal tier of thalamic nuclei, includingthe ventral caudal nucleus (VC), ventral intermediate nucleus(VIM), and ventral oralis anterior and posterior nuclei (Voa andVop, respectively). ATh, anterior thalamic nucleus complex; MTh,medial thalamic nucleus complex. (From, Schaltenbrand G, WahrenW: Atlas for Stereotaxy of the Human Brain. Stuttgart, ThiemeMedical Publishers, 1977. Reproduced with permission [313].)
C
BA
FIGURE 4. Location of the GPiand its relation to the surroundingstructures as depicted on the axialsection of the Schaltenbrand andWahren atlas. Note the close prox-imity of the GPi medially to theIC and laterally to the GPe. Thedark boundary between the GPiand GPe is the external lamina.(From, Schaltenbrand G, WahrenW: Atlas for Stereotaxy of theHuman Brain. Stuttgart, ThiemeMedical Publishers, 1977. Repro-duced with permission [313].)
BA
FIGURE 5. High-resolution axial magnetic resonance imaging (MRI)scans showing the globus pallidus and optic tract. A, inversion recoverysequence showing the caudate nucleus, putamen, globus pallidus (GP),IC, and thalamus. B, axial T2-weighted MRI scan showing the trajectoryof the intended placement of the deep brain stimulation (DBS) lead with itstip just dorsal to the optic tract. FIGURE 6. Somatotopic arrangement of the ventral
relay nuclei shown on an axial section includingVC, VIM, Voa, and Vop. The general scheme in thethalamic somatotopy includes having the leg placedmore laterally and the face placed more medial withan upper limb in between the two. It also shows thesomatotopy in the internal capsule. In this classicfigure, the GPi homunculus does not strictly repre-sent the GPi somatotopy, as has been suggested withmore recent data. (From, Schaltenbrand G, WahrenW: Atlas for Stereotaxy of the Human Brain.Stuttgart, Thieme Medical Publishers, 1977.Reproduced with permission [313].)

obtained preoperatively arethen loaded into a surgicalnavigation computer, and thefiducials are registered. Theframeless assembly is then used to plan a trajectory to the tar-get of interest. The reported advantages of the frameless sys-tems are related to arguments of increased efficiency of surgi-cal planning and imaging acquisition before the day of surgeryand enhancement of the patient’s comfort with less immobiliza-tion of the head and neck (Fig. 10).
Currently, there is no major advantage to using one systemversus another; the surgeon’s preference guides the selectionprocess. Relatively few centers perform frameless DBS surger-ies compared with the number that perform frame-based DBS.A randomized prospective study is necessary to determine thelevels of patient comfort, precision, outcome, and efficiencyinherent in one system versus another.
Imaging
VentriculographyIn the late 1960s, Guiot et al. (128, 129) defined the position
of various deep nuclei based on the distance between the ACand PC and the height of the thalamus, as obtained from ven-triculography (Fig. 11). This method was the cornerstone offunctional neurosurgery for decades and is still used in severalcenters worldwide (30, 34, 177). However, the advent of mod-ern imaging has, for the most part, replaced ventriculographywith computed tomographic (CT) and MRI scans.
CT ScansA thin-cut stereotactic CT scan (approximately 2-mm slices,
with no gap and no gantry tilt) can be easily obtained to localizethe AC and PC and subsequently be computationally fused withan MRI scan on a stereotactic planning station. CT scans are freefrom the image distortions inherent to MRI and allow the stereo-tactic space to be defined with a high degree of accuracy.
general agreement about the efficacy of DBS for movement dis-orders, there is some variance in the protocols for placement ofDBS leads (220, 272, 323, 358).
The surgical technique has its foundation in stereotacticprinciples. It has evolved from strong reliance on stereotacticatlases and incorporates advances in imaging and neurophys-iological mapping techniques. At present, most neurosur-geons performing DBS use a variety of these approaches tolocalize the target of interest. These variations are a result oftraining patterns, surgeon preferences, and surgical practicelogistics. There is no single correct approach, as long as out-comes are good and complications are kept to a minimum.The lack of randomized prospective studies comparing oneapproach to another is also a major barrier to advancementand standardization in this field.
The basic components of DBS implantation surgery involvestereotactic anatomic targeting, physiological target verifica-tion, DBS lead implantation, and implantable pulse generator(IPG) or power-source placement. The components of the sur-gery can all be done in one setting or in stages, depending onthe group’s preference. We review these components, high-lighting common practice patterns and acknowledging thevariance of practices across centers.
Headframes and Acquisition of Stereotactic CoordinatesThe least debated aspect of the surgery is the method chosen
for acquisition of stereotactic coordinates. Currently, bothframe-based and frameless techniques are commercially avail-able for localization within the stereotactic space.
Frame-based SystemsThe frame-based approach is the “gold standard” that has
been used for many years with proven precision and reliability.A variety of headframes can be used, such as the Leksell (Elekta,Stockholm, Sweden), Cosman-Roberts-Wells (Radionics,Burlington, MA), Riechert-Mundinger (Fischer-Leibinger,Freiburg, Germany), and other commercially available systems.Based on a survey of North American centers that perform DBSsurgeries, it appears that the Cosman-Roberts-Wells frame isthe most commonly used, followed by the Leksell frame (Fig. 7)(271). The stereotactic accuracy of each frame has been wellestablished (233), and these frame-based approaches representthe standard of care after decades of clinical use, consistency,and dependability. Placement of the headframe is achievedunder local anesthesia. The frame should be placed parallel to aline extending from the lateral canthus to the tragus, to approx-imately parallel the anterior commissure (AC)-posterior com-missure (PC) line (Fig. 8).
Frameless SystemsThe introduction of the frameless technique and device for
DBS lead placement (90, 150) has provided an alternativeapproach that has been embraced by some groups. The frame-based fiducials have been replaced by small screws that arevisible on computed tomography, which are secured to thepatient’s cranium before the surgery (Fig. 9). The images
REZAI ET AL.
SHC816 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
FIGURE 7. Leksell stereotacticf r a m e ( E l e k t a , S t o c k h o l m ,Sweden). The system is based onthe center-of-arc principle, andthe basic components are theCartesian coordinate frame, whichis attached to the patient’s headusing four pins, and the semicir-cular arc.
FIGURE 8. Method for place-ment of the Leksell headframe.The frame placement is performedunder local anesthesia with thepatient sitting up. The frameshould be placed parallel to a lineextending from the lateral can-thus to the tragus (orbitomeatalline depicted in red) to approxi-mate the plane of the anteriorcommissure-posterior commissure(AC-PC) line.
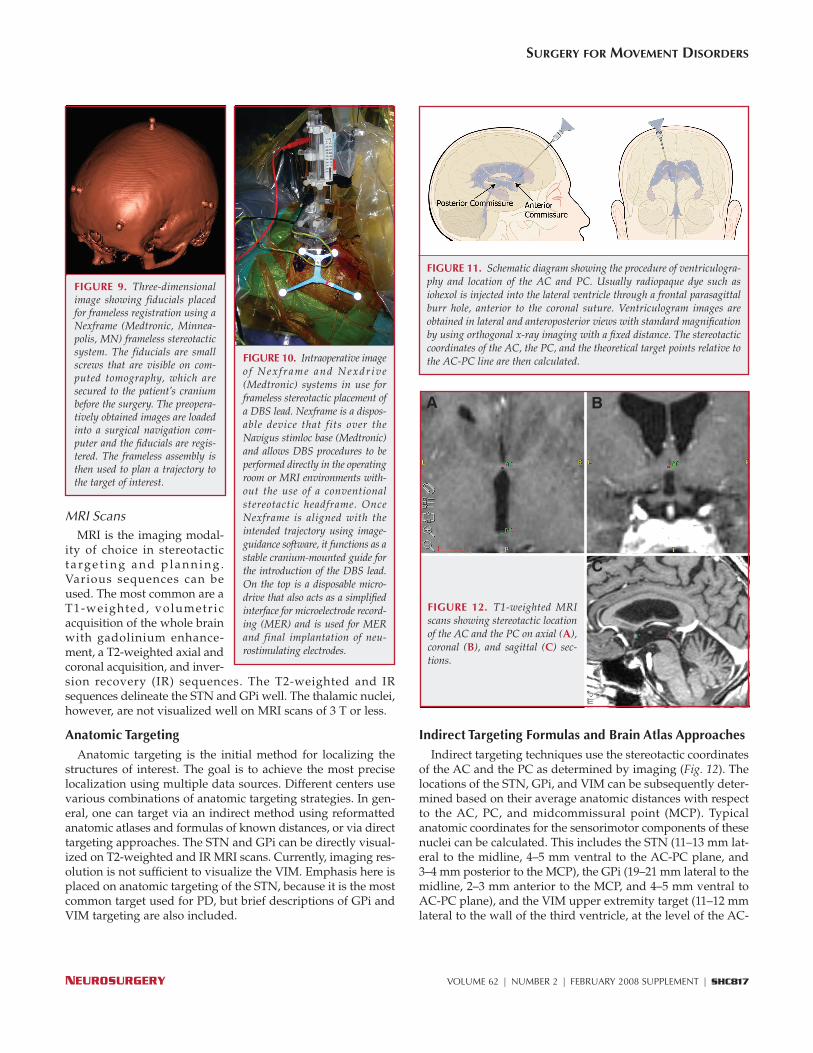
MRI ScansMRI is the imaging modal-
ity of choice in stereotactict a rg e t i n g a n d p l a n n i n g .Various sequences can beused. The most common are aT1-weighted, volumetricacquisition of the whole brainwith gadolinium enhance-ment, a T2-weighted axial andcoronal acquisition, and inver-sion recovery (IR) sequences. The T2-weighted and IRsequences delineate the STN and GPi well. The thalamic nuclei,however, are not visualized well on MRI scans of 3 T or less.
Anatomic TargetingAnatomic targeting is the initial method for localizing the
structures of interest. The goal is to achieve the most preciselocalization using multiple data sources. Different centers usevarious combinations of anatomic targeting strategies. In gen-eral, one can target via an indirect method using reformattedanatomic atlases and formulas of known distances, or via directtargeting approaches. The STN and GPi can be directly visual-ized on T2-weighted and IR MRI scans. Currently, imaging res-olution is not sufficient to visualize the VIM. Emphasis here isplaced on anatomic targeting of the STN, because it is the mostcommon target used for PD, but brief descriptions of GPi andVIM targeting are also included.
Indirect Targeting Formulas and Brain Atlas ApproachesIndirect targeting techniques use the stereotactic coordinates
of the AC and the PC as determined by imaging (Fig. 12). Thelocations of the STN, GPi, and VIM can be subsequently deter-mined based on their average anatomic distances with respectto the AC, PC, and midcommissural point (MCP). Typicalanatomic coordinates for the sensorimotor components of thesenuclei can be calculated. This includes the STN (11–13 mm lat-eral to the midline, 4–5 mm ventral to the AC-PC plane, and3–4 mm posterior to the MCP), the GPi (19–21 mm lateral to themidline, 2–3 mm anterior to the MCP, and 4–5 mm ventral toAC-PC plane), and the VIM upper extremity target (11–12 mmlateral to the wall of the third ventricle, at the level of the AC-
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC817
FIGURE 9. Three-dimensionalimage showing fiducials placedfor frameless registration using aNexframe (Medtronic, Minnea-polis, MN) frameless stereotacticsystem. The fiducials are smallscrews that are visible on com-puted tomography, which aresecured to the patient’s craniumbefore the surgery. The preopera-tively obtained images are loadedinto a surgical navigation com-puter and the fiducials are regis-tered. The frameless assembly isthen used to plan a trajectory tothe target of interest.
FIGURE 10. Intraoperative imageo f Nex f rame and Nexdr ive(Medtronic) systems in use forframeless stereotactic placement ofa DBS lead. Nexframe is a dispos-able device that fits over theNavigus stimloc base (Medtronic)and allows DBS procedures to beperformed directly in the operatingroom or MRI environments with-out the use of a conventionalstereotactic headframe. OnceNexframe is aligned with theintended trajectory using image-guidance software, it functions as astable cranium-mounted guide forthe introduction of the DBS lead.On the top is a disposable micro-drive that also acts as a simplifiedinterface for microelectrode record-ing (MER) and is used for MERand final implantation of neu-rostimulating electrodes.
FIGURE 11. Schematic diagram showing the procedure of ventriculogra-phy and location of the AC and PC. Usually radiopaque dye such asiohexol is injected into the lateral ventricle through a frontal parasagittalburr hole, anterior to the coronal suture. Ventriculogram images areobtained in lateral and anteroposterior views with standard magnificationby using orthogonal x-ray imaging with a fixed distance. The stereotacticcoordinates of the AC, the PC, and the theoretical target points relative tothe AC-PC line are then calculated.
C
BA
FIGURE 12. T1-weighted MRIscans showing stereotactic locationof the AC and the PC on axial (A),coronal (B), and sagittal (C) sec-tions.

PC plane, and anteroposterior location between two- and three-twelfths of the AC-PC distance anterior to the PC).
A standardized brain atlas can be used to locate the x, y. andz coordinates of the STN, GPi, and VIM in relation to the MCP(Figs. 3 and 4). The stereotactic atlas can be stretched and mor-phed using surgical navigation software to better fit eachpatient’s anatomy. However, despite these technologicaladvances, it is important to realize the limitations of the stereo-tactic atlases. The data in most atlases are based on a smallnumber of brains. The Schaltenbrand and Wahren atlas (313)uses one brain for the frontal series and one brain for the axialand sagittal series. The Talairach and Tournoux atlas is basedon one brain (339). The morphology and position of the STN isdifferent in each atlas (257, 301), and the actual size and theposition of the STN are highly variable among patients (136,301) and within the stereotactic atlases.
Direct TargetingWith the advances in neuroimaging technology, direct visu-
alization of the various nuclei has become possible. Althoughcomputed tomography offers excellent stereotactic precision, itcan be difficult to visualize various targets and periventricularlandmarks (375) when using it. MRI offers the advantage ofexcellent anatomic resolution in multiple planes. This allowsfor localization of the AC and the PC on T1-weighted images(Fig. 12), the visualization of the pallidum on IR and T2-weighted sequences (Fig. 5), and identification of the STN onaxial, sagittal, and coronal T2-weighted images (Fig. 13) (32).The advantage of directly visualizing deep targets is implicit;one works with the patient’s individual anatomic variationrather than relying on a fixed brain that was sectioned severaldecades ago. Some centers rely entirely on MRI scans to calcu-late anatomic targets (272, 330, 334). There are questions, how-ever, regarding the accuracy of the exact location of these tar-gets within the stereotactic space because of distortion on MRIscans (311). To reduce the possibility of MRI-related inaccura-cies, several centers use a protocol of merging the anatomicallysuperior MRI scans to stereotactically acquired CT scans (19,220, 323, 375).
Several authors have described strategies to further refineimage-based targeting. Arguing that the relationship of the AC-PC line and the STN may be variable and inconsistent, theypropose the use of a landmark that is physically closer to thetarget of interest (16, 24, 78, 330). In 2000, Bejjani et al. (24)described using the anterior border of the red nucleus as alandmark for the AP coordinate of the STN. This approach hasalso been used by others (17, 78). Axial and coronal T2-weighted images are particularly important for adequate visu-alization of the STN, as a sharp contrast can often be observedbetween the nucleus and the surrounding white matter. Thered nucleus and the STN can be clearly visualized. The STN liesanterior and lateral to the red nucleus and, in this regard, theanterior border of the red nucleus can be used as a landmarkfor the STN target (Figs. 3 and 13). Starr (330) later describedthe relationship between the center of the red nucleus and themiddle of the electrode array as another internal landmark for
targeting the STN. In the authors’ experience, the interpedun-cular distance can also serve as a good surrogate for the later-ality of the STN target (unpublished data).
The possibility of directly visualizing and targeting the STNand GPi has brought forth innovative imaging application pos-sibilities for DBS surgery. The use of intraoperative MRI to per-form DBS surgery is being investigated by Martin et al. (235).Their preliminary results show that successful DBS implanta-tion can be performed in patients under general anesthesiawith only anatomic targeting. This approach has multipleinherent advantages that will facilitate its acceptance and wide-spread use once additional studies demonstrate that the safetyand efficacy are equivalent to the traditional techniques.
Trajectory PlanningImaging is necessary for accurate targeting as well as for
planning of the surgical trajectory to the target. The strategy isto avoid surface and subcortical vessels and to have an angle ofapproach that passes through a large segment of the structureof interest. The precise entry point may be refined on the plan-ning console, such that the trajectory passes through the crownof a gyrus rather than into a sulcus, as well as away from thevessels associated with the wall of the ventricle, thereby help-ing to avoid hemorrhagic complications (Fig. 14).
Neurophysiological Assessment and VerificationAll surgeries for movement disorders are initially based
on anatomic targeting techniques. However, physiologicalverification of these targets is a necessary step before finalimplantation of the DBS electrode can occur. This is crucialbecause anatomic inaccuracies due to image distortion, brainshift, cerebrospinal fluid loss, and pneumocephalus can leadto final target deviation (124). A DBS lead that is misplacedby as little as 2 mm can result in inaccuracy when locatingthe final target.
In a more practical sense, neurophysiological techniques arenecessary to refine lead positioning within a target and to opti-mize clinical outcome and minimize stimulation-related sideeffects. In the lesioning era preceding DBS, physiological ver-ification was a major requirement before the creation of
REZAI ET AL.
SHC818 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
FIGURE 13. High resolution axial (A) and coronal (B) T2-weighted MRIscans showing the STN and structures in close proximity to it. STN, sub-thalamic nucleus; SNR, substantia nigra reticulate; RN, red nucleus.
BA

lesions. Presently used physiological techniques includemicroelectrode recording (MER), semi-MER, macrostimula-tion, and DBS lead stimulation. The degree of dependence onthese techniques varies widely. The exact detail of mapping foreach target is beyond the scope of this article; however, gener-alities are provided and details can be obtained in the refer-ences provided.
MERThe MER technique uses microelectrodes with high imped-
ances (typically �0.4 mΩ) with a tip diameter in the range of 2to 4 μm (124, 158, 207). These microelectrodes are capable ofrecording single units as well as delivering stimulation in themicroamp range (typically �100 mA). A hydraulic or electricalmicrodrive is used to advance a microelectrode in submilli-metric steps. United States Food and Drug Administration-approved microelectrodes are commercially available and aremade of tungsten or platinum/iridium.
Some centers use a single MER penetration as confirmationof the anatomic targets, whereas others rely on one or moretracks that reveal a set of acceptable criteria, such as anapproximately 5-mm long area of STN (231). There are alsocenters that use a multiple-track penetration approach for very
detailed physiological mapping of the borders of the nuclei.The hope is to improve treatment efficacy and limit postoper-ative side effects that are related to undesired stimulation ofbordering structures (123, 373). In a survey of 36 DBS centersin North America, Ondo and Bronte-Stewart (269) found that97% of centers use MER for assistance in lead placement. Theaverage number of tracks was 2.3 per electrode, with a rangeof 1 to 18 tracks. They also reported that most centers usemacrostimulation to assess the final clinical response.
Although most centers advance one microelectrode at a time,several centers advance multiple microelectrodes simultane-ously and assess a larger area of the target (24, 31). Deliveringstimulation through the microelectrode, when feasible, is per-formed at some centers to assess side effects resulting fromproximity of the track to other structures such as the internalcapsule (124, 372).
MER allows for the delineation of the physiological signa-ture of various nuclei and white matter tracts. Single neu-rons, multiunit activities, and local field potentials can be dis-cerned with characteristic sound and visual expressions. Thefrequency and pattern of activity are observed, thus helpingto confirm location based on characteristic physiological sig-natures. The boundaries between white matter and nuclei areimportant to distinguish, as are the length of the desirednucleus and an assessment of the surrounding structures. TheMER physiology of the STN, GPi, and VIM is discussedbriefly below.
The STNThe information obtained in the track, such as the presence
or absence of thalamus or SNr, could also aid in determiningthe trajectory in relation to the nucleus, i.e., medial, lateral,anterior, or posterior. Figure 15 shows a sample MER trajectoryaimed at the STN. The thalamus is typically the initial structureencountered by the MER. The specific thalamic nuclei recordeddepend on the AP angle of approach, but typically include thenucleus reticularis (Rt), the Voa, and the Vop. There are twotypical cell activities: bursting units (interburst frequency, 15 �19 Hz) and irregular tonic firing (∼28 Hz) cells. The backgroundactivity is substantially less dense than the background activityof the STN. After exiting the thalamus, a decrease of back-ground activity coupled with the resolution of, generally, fewerfiring units indicate the zona incerta (ZI) and fields of Forel.Activity in these areas has a similar bimodal distribution ofbursting and tonic firing units, usually with low firing rates. Asubstantial increase in background neuronal activity signalsthe entry into the STN. This increase in background activity,perhaps the most distinguishing characteristic of the STN com-pared with the other structures encountered in this procedure,can precede the resolution of single-unit activity indicative ofthe STN by 1 to 2 mm. Mean firing rates have been reported inthe 34- to 47-Hz range, with standard deviations in the 25-Hzrange. Bursting units are common. The pattern of activity istypically irregular. Cells that respond to passive movement ofthe limbs are encountered in the dorsolateral part of the STN.Within this motor area, lower extremity-related units tend to be
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC819
FIGURE 14. Navigation view on Framelink (Medtronic) software usinga contrast enhanced, T1-weighted MRI scan showing the enhancing ves-sels in the periventricular region. The trajectory (blue arrows and lines)is carefully planned to avoid these deep vessels and more superficial corti-cal vessels. The right upper panel demonstrates the images in a planeperpendicular to the planned trajectory (red point).
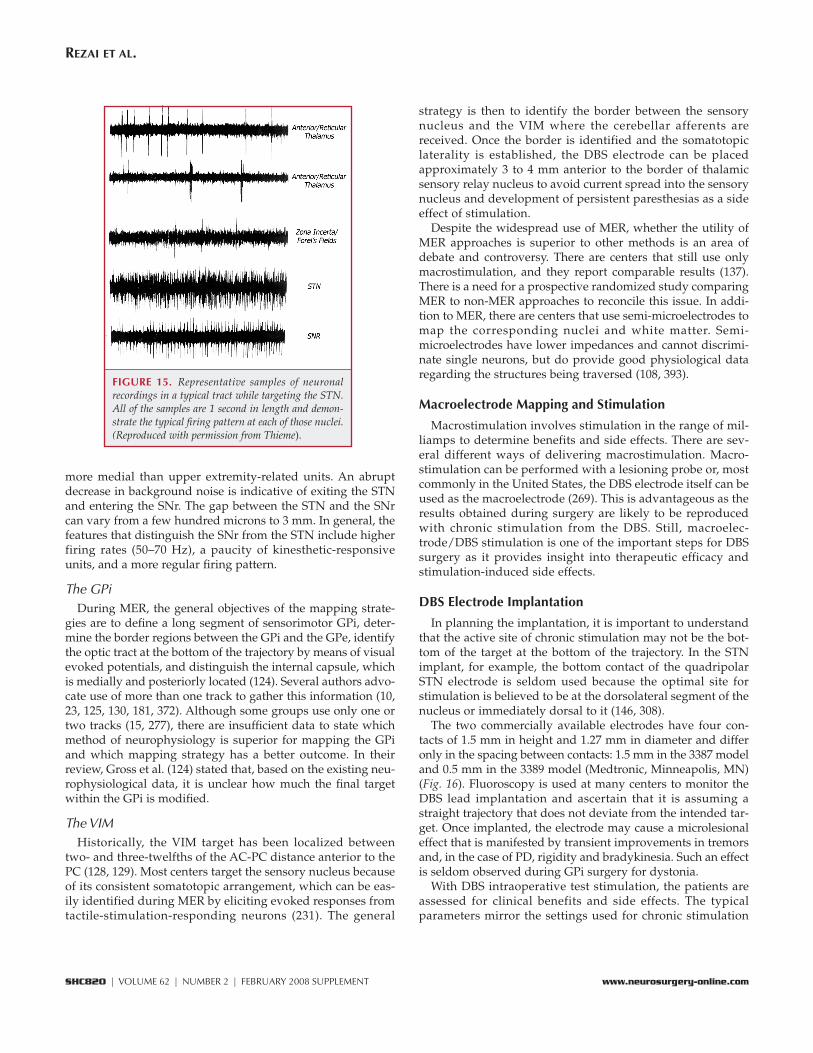
more medial than upper extremity-related units. An abruptdecrease in background noise is indicative of exiting the STNand entering the SNr. The gap between the STN and the SNrcan vary from a few hundred microns to 3 mm. In general, thefeatures that distinguish the SNr from the STN include higherfiring rates (50–70 Hz), a paucity of kinesthetic-responsiveunits, and a more regular firing pattern.
The GPiDuring MER, the general objectives of the mapping strate-
gies are to define a long segment of sensorimotor GPi, deter-mine the border regions between the GPi and the GPe, identifythe optic tract at the bottom of the trajectory by means of visualevoked potentials, and distinguish the internal capsule, whichis medially and posteriorly located (124). Several authors advo-cate use of more than one track to gather this information (10,23, 125, 130, 181, 372). Although some groups use only one ortwo tracks (15, 277), there are insufficient data to state whichmethod of neurophysiology is superior for mapping the GPiand which mapping strategy has a better outcome. In theirreview, Gross et al. (124) stated that, based on the existing neu-rophysiological data, it is unclear how much the final targetwithin the GPi is modified.
The VIMHistorically, the VIM target has been localized between
two- and three-twelfths of the AC-PC distance anterior to thePC (128, 129). Most centers target the sensory nucleus becauseof its consistent somatotopic arrangement, which can be eas-ily identified during MER by eliciting evoked responses fromtactile-stimulation-responding neurons (231). The general
strategy is then to identify the border between the sensorynucleus and the VIM where the cerebellar afferents arereceived. Once the border is identified and the somatotopiclaterality is established, the DBS electrode can be placedapproximately 3 to 4 mm anterior to the border of thalamicsensory relay nucleus to avoid current spread into the sensorynucleus and development of persistent paresthesias as a sideeffect of stimulation.
Despite the widespread use of MER, whether the utility ofMER approaches is superior to other methods is an area ofdebate and controversy. There are centers that still use onlymacrostimulation, and they report comparable results (137).There is a need for a prospective randomized study comparingMER to non-MER approaches to reconcile this issue. In addi-tion to MER, there are centers that use semi-microelectrodes tomap the corresponding nuclei and white matter. Semi-microelectrodes have lower impedances and cannot discrimi-nate single neurons, but do provide good physiological dataregarding the structures being traversed (108, 393).
Macroelectrode Mapping and Stimulation
Macrostimulation involves stimulation in the range of mil-liamps to determine benefits and side effects. There are sev-eral different ways of delivering macrostimulation. Macro-stimulation can be performed with a lesioning probe or, mostcommonly in the United States, the DBS electrode itself can beused as the macroelectrode (269). This is advantageous as theresults obtained during surgery are likely to be reproducedwith chronic stimulation from the DBS. Still, macroelec-trode/DBS stimulation is one of the important steps for DBSsurgery as it provides insight into therapeutic efficacy andstimulation-induced side effects.
DBS Electrode Implantation
In planning the implantation, it is important to understandthat the active site of chronic stimulation may not be the bot-tom of the target at the bottom of the trajectory. In the STNimplant, for example, the bottom contact of the quadripolarSTN electrode is seldom used because the optimal site forstimulation is believed to be at the dorsolateral segment of thenucleus or immediately dorsal to it (146, 308).
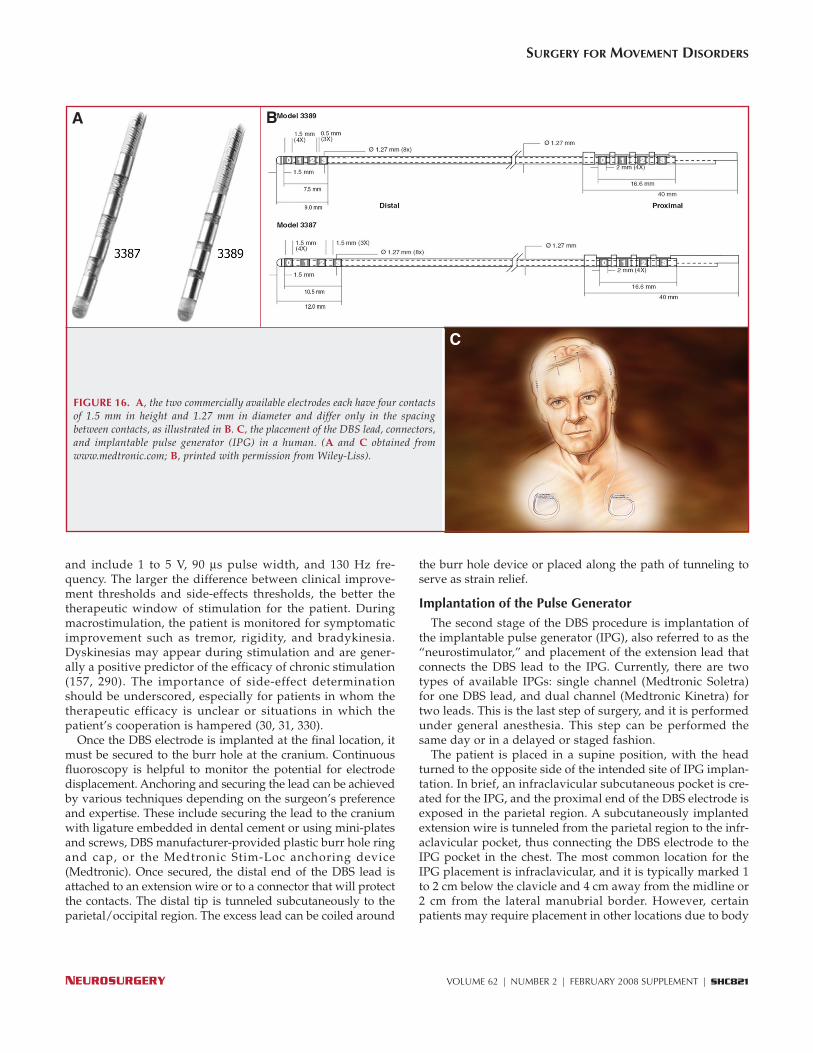
The two commercially available electrodes have four con-tacts of 1.5 mm in height and 1.27 mm in diameter and differonly in the spacing between contacts: 1.5 mm in the 3387 modeland 0.5 mm in the 3389 model (Medtronic, Minneapolis, MN)(Fig. 16). Fluoroscopy is used at many centers to monitor theDBS lead implantation and ascertain that it is assuming astraight trajectory that does not deviate from the intended tar-get. Once implanted, the electrode may cause a microlesionaleffect that is manifested by transient improvements in tremorsand, in the case of PD, rigidity and bradykinesia. Such an effectis seldom observed during GPi surgery for dystonia.
With DBS intraoperative test stimulation, the patients areassessed for clinical benefits and side effects. The typicalparameters mirror the settings used for chronic stimulation
REZAI ET AL.
SHC820 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
FIGURE 15. Representative samples of neuronalrecordings in a typical tract while targeting the STN.All of the samples are 1 second in length and demon-strate the typical firing pattern at each of those nuclei.(Reproduced with permission from Thieme).
and include 1 to 5 V, 90 μs pulse width, and 130 Hz fre-quency. The larger the difference between clinical improve-ment thresholds and side-effects thresholds, the better thetherapeutic window of stimulation for the patient. Duringmacrostimulation, the patient is monitored for symptomaticimprovement such as tremor, rigidity, and bradykinesia.Dyskinesias may appear during stimulation and are gener-ally a positive predictor of the efficacy of chronic stimulation(157, 290). The importance of side-effect determinationshould be underscored, especially for patients in whom thetherapeutic efficacy is unclear or situations in which thepatient’s cooperation is hampered (30, 31, 330).
Once the DBS electrode is implanted at the final location, itmust be secured to the burr hole at the cranium. Continuousfluoroscopy is helpful to monitor the potential for electrodedisplacement. Anchoring and securing the lead can be achievedby various techniques depending on the surgeon’s preferenceand expertise. These include securing the lead to the craniumwith ligature embedded in dental cement or using mini-platesand screws, DBS manufacturer-provided plastic burr hole ringand cap, or the Medtronic Stim-Loc anchoring device(Medtronic). Once secured, the distal end of the DBS lead isattached to an extension wire or to a connector that will protectthe contacts. The distal tip is tunneled subcutaneously to theparietal/occipital region. The excess lead can be coiled around
the burr hole device or placed along the path of tunneling toserve as strain relief.
Implantation of the Pulse GeneratorThe second stage of the DBS procedure is implantation of
the implantable pulse generator (IPG), also referred to as the“neurostimulator,” and placement of the extension lead thatconnects the DBS lead to the IPG. Currently, there are twotypes of available IPGs: single channel (Medtronic Soletra)for one DBS lead, and dual channel (Medtronic Kinetra) fortwo leads. This is the last step of surgery, and it is performedunder general anesthesia. This step can be performed thesame day or in a delayed or staged fashion.
The patient is placed in a supine position, with the headturned to the opposite side of the intended site of IPG implan-tation. In brief, an infraclavicular subcutaneous pocket is cre-ated for the IPG, and the proximal end of the DBS electrode isexposed in the parietal region. A subcutaneously implantedextension wire is tunneled from the parietal region to the infr-aclavicular pocket, thus connecting the DBS electrode to theIPG pocket in the chest. The most common location for theIPG placement is infraclavicular, and it is typically marked 1to 2 cm below the clavicle and 4 cm away from the midline or2 cm from the lateral manubrial border. However, certainpatients may require placement in other locations due to body
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC821
C
FIGURE 16. A, the two commercially available electrodes each have four contactsof 1.5 mm in height and 1.27 mm in diameter and differ only in the spacingbetween contacts, as illustrated in B. C, the placement of the DBS lead, connectors,and implantable pulse generator (IPG) in a human. (A and C obtained fromwww.medtronic.com; B, printed with permission from Wiley-Liss).
BA

habitus (very thin patients), age (pediatric patients), activitiesand hobbies, a history of previous surgery in the region, orcosmetic reasons.
Outcomes of DBS for Movement Disorders
The literature relevant to movement disorder surgery isextensive: There are more than 1000 published articles per-taining to DBS for movement disorders. In addition to theretrospective and case report format of much of the literature,the reversibility feature (turning DBS on and off) on-demandallows for controlled, blinded assessments, making it one ofthe better-studied neurosurgical interventions. In addition,validated rating scales for movement disorders have beenestablished and are used in most surgical trials. These stan-dardized, disease-specific rating scales allow for outcomes tobe expressed in a more objective fashion that is specific to thedisease of interest.
STN and GPi DBS for PD(see video at web site)
DBS has become the surgical procedure of choice for move-ment disorders, replacing stereotactic ablative procedures, forthe most part, in countries where access to this technology isavailable. Outcomes from DBS are expressed more frequentlyas absolute or as percent score reductions in the UnifiedParkinson’s Disease Rating Scale (UPDRS) Part III (motor) dur-ing the medication-off state. Thus, UPDRS Part III is a standardoutcome scale indicating motor benefits from a therapy. Dataon the impact of DBS upon activities of daily living (ADLs),percent reduction in dyskinesias, or incremental “on time” peri-ods without dyskinesias are inconsistently reported.Reductions in dyskinesias can be considered as a direct effect ofDBS or may be secondary to a reduction in medication require-ments (183, 369).
Prospective studies have reported on the outcomes of GPiand STN DBS for the cardinal symptoms of PD. Both targetsare shown to be beneficial (177, 183), although a trend existsamong these studies to indicate that STN DBS is more effec-tive. In addition, STN DBS tends to allow for a greater reduc-tion in the postoperative medication burden with consequentreduction in dyskinesias (80, 86, 181, 183, 282, 303). Direct com-parisons of GPi versus STN stimulation have been performedin small samples of patients. The outcome data from thesestudies were not conclusive enough to exclude the GPi as anaccepted DBS target for PD (368) and generally corroboratedthe advantage of using the STN in improving UPDRS Part IIIscores and L-dopa intake (15, 59). In addition, a recent reportof long-term bilateral pallidal stimulation in 11 PD patientsconfirmed the therapy’s sustained efficacy in alleviating dysk-inesias. However, motor scores that had been alleviated in thefirst year deteriorated during the 5-year follow-up to an extentgreater than would be expected from disease progressionalone. The lost motor benefits were not regained with addi-tional programming, but were successfully recaptured in fourpatients by repositioning the electrodes from the GPi to the
STN (378). As discussed below (in Complications of DBSSurgery), it is possible that STN stimulation is more prone tocognitive and behavioral complications (see Cognitive andNeurobehavioral Outcome and Complications with DBS).However, outcomes from upcoming randomized, prospectivelarge studies are expected to provide more insights into the rel-ative efficacy and risks associated with STN versus GPi DBSfor the treatment of PD.
The encouraging results of STN DBS originally reported byBenabid and the pioneering Grenoble group (26, 31, 180, 181,214–216, 289) motivated a large number of studies in the pastdecade that have further validated the safety and efficacy ofthis procedure (80, 67, 79, 93, 94, 102, 107, 134, 145, 160, 165,208, 212, 225, 258, 271, 276, 281, 304, 307, 315, 318, 344, 359, 360,362, 394). A meta-analysis of the literature published in 2006reviewed the literature from 1993 to 2004. The mean reductionin UPDRS Part III scores among the 34 articles included in thestudy was 52% (comparing the DBS-on, medication-off state tothe medication-off, DBS-off state). There was a large variationin reported outcomes, ranging from 82 to 17%. The meanreduction in UPDRS Part II scores was 49.9%, ranging from 72to 29.5%. As noted above, the preoperative response to L-dopais considered a good outcome predictor of response to sur-gery and is, therefore, a heavily considered determinationregarding a patient’s candidacy for surgery. The correlationbetween L-dopa response and positive outcomes after STNDBS was confirmed by this meta-analysis as well as otherstudies (384).
A few prospective, controlled studies have provided funda-mental contributions to the DBS literature and merit moredetailed discussion. In 2001, the DBS for PD Study Groupreported on the outcomes of 96 patients undergoing STN and38 patients undergoing GPi DBS. The improvements in UPDRSPart III motor subscores at the time of the 3-month follow-up(assessed with double-blind evaluations after patients wererandomly assigned to stimulation-on or -off states) were 49and 37% for these groups, respectively. A continuation of thisstudy was reported in 2005 with 3-year or longer follow-upperiod for 69 patients from the initial study. The 3-year orlonger follow-up data demonstrated that the effects of DBS forPD are long-lasting. The long-term benefits of DBS were latersubstantiated by Krack et al. (177). Forty-nine consecutivepatients treated with bilateral STN DBS were assessed at 1, 3,and 5 years after implantation. The mean reductions in UPDRSPart III scores at these time points were 66, 59, and 54%, respec-tively. ADLs were also improved. A significant decrease in effi-cacy was observed when the first and fifth years after surgerywere compared. Nevertheless, most of these patients weredependent upon others before surgery and continued to enjoyindependence throughout the entire follow-up period. Similar5-year follow-up results were reported by Schüpbach et al.(315), with 54% reductions in UPDRS Part III scores and a 40%maintained reduction in UPDRS Part II scores. Additional long-term outcome studies with follow-up periods ranging from 2 to4 years reported on mean UPDRS Part III reductions of 48% in25 patients (170), 43% in 20 patients (367), 55% in 22 patients
REZAI ET AL.
SHC822 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com

(271), 57% in 29 patients (148), and 45% in 20 patients (365). Thelatter study also reported on complete withdrawal of medica-tion (replaced by stimulation) in 10 out of 20 patients. Such adramatic and early reduction of medication intake may haveaccounted for some of the complications observed by theauthors, such as dysarthria and cognitive problems (200).
Thalamic (VIM) DBS for Tremor
(see video at web site)The standardized assessment of tremor can be achieved via
the Tremor Rating Scale (TRS) (151, 329). Stereotactic thalamo-tomies targeted at the VIM nucleus are well-established proce-dures for the management of tremors from PD or essentialtremor (8, 103, 115–117, 166, 167, 253–255, 343). In managingpatients with PD, thalamotomies alleviate tremors without sig-nificantly affecting the other cardinal symptoms of PD. Uni-lateral thalamotomies are considered relatively safe, but bilat-eral procedures carry an elevated risk of neurological deficitssuch as dysarthria and cognitive deterioration (237). Chronicstimulation was considered a potential alternative to thalamo-tomy, at least partly because the known tremor-alleviatingeffects of acute stimulation were used for physiological confir-mation during ablative stereotactic interventions (116, 255). Inaddition, thalamic chronic stimulation had already beendemonstrated to be feasible and safe for patients undergoingstereotactic interventions for chronic pain conditions (153, 154,192, 211, 298–300, 354). Benabid et al. (35, 36) initially appliedthalamic stimulation contralateral to thalamotomy in patientswith PD. Their preliminary experiences revealed a greater effi-cacy of thalamotomy over stimulation. In 1991, the results ofchronic VIM stimulation for tremor were reported in a series of32 patients with essential tremor or PD who had undergone 43thalamic stimulation implants (11 patients underwent bilateralstimulation). At a mean follow-up period of 13 months, 88% ofthe implanted DBS electrodes resulted in major or completerelief from tremors. DBS, initially considered an alternative tostereotactic thalamotomy, gradually became the surgical proce-dure of choice for the treatment of essential tremor, as itdemonstrated similar efficacy rates and lower risks (174, 275,316, 343). A direct comparison between thalamotomy and thal-amic stimulation was reported by Schuurman et al. (316).Seventy patients with PD, essential tremor, or tremor from mul-tiple sclerosis were randomized to stimulation or ablative sur-gery groups. Patients with unilateral symptoms underwent asingle intervention contralateral to the symptoms. Patients withbilateral tremors underwent either bilateral thalamic stimula-tion or a unilateral thalamotomy with contralateral stimula-tion. Patients with PD and essential tremor who had undergonethalamic stimulation performed significantly better in ADLsthan those undergoing ablation. Sixteen adverse effectsoccurred among the patients randomized to the thalamotomygroup. In comparison, only six patients with thalamic stimula-tion experienced adverse effects, which were successfullyresolved with stimulation cessation. Pahwa et al. (275) reportedsimilar results when comparing the outcomes of 17 patients
undergoing thalamic stimulation to the outcomes of 17 patientswho had previously undergone thalamotomy. Although theeffects from tremor suppression were very similar in bothgroups, complications, particularly intracerebral hemorrhages,were more common among patients with thalamotomies (35versus 0%). Likewise, cognitive deterioration and hemiparesisoccurred, respectively, in 29 and 12% of patients who hadundergone thalamotomies but in none of those with thalamicstimulation. Although thalamic stimulation is chronically effec-tive for most patients (37, 57, 186, 213, 222, 228, 293, 316), reduc-tions in efficacy during longer-term follow-up periods havebeen reported (32, 173).
The vast majority of thalamic DBS procedures have been tar-geted at the upper extremity function. However, lower extrem-ity, head/neck, and axial tremor are also common problemsthat negatively impact quality of life for patients with essentialtremor. Putzke et al. (293) reported on the outcomes of 22patients with head, voice, or trunk tremor undergoing bilateral,staged, DBS thalamic implants. Bilateral stimulation was moreeffective than unilateral stimulation in alleviating axial tremors;however, as for bilateral thalamotomies, the rate of neurologi-cal complications was higher in patients who underwent bilat-eral stimulation. Dysarthria was observed in 27% of patientswith bilateral stimulation, whereas none of those undergoingunilateral stimulation experienced the same problem. Likewise,disequilibrium was more common during bilateral stimulation.Although unilateral stimulation was comparatively less effec-tive, it still demonstrated a significant reduction in axialtremors when compared with the preoperative baseline andstimulation-off periods. These findings are supported by thework of Koller et al. (172) in a prospective assessment of 38patients with head tremor undergoing unilateral thalamic stim-ulation. In this study, 71% of patients presented with tremoralleviation at 3 months. The effects remained generally stableover the long-term (1 yr) follow-up period. Stimulation set-tings varied minimally during this period, further corroborat-ing the stability of the effects. Although staged bilateral proce-dures are often preferred for axial symptoms, they may not besafer than simultaneous implantation procedures (337).
GPi DBS for DystoniaStereotactic ablative surgery of the GPi (pallidotomy) has
been attempted in the past in patients with generalized dysto-nia. Encouraging results have been reported (91, 92, 150, 371)but, unlike reports of thalamotomies for treating tremor, thebest results are not observed immediately, but rather, after sev-eral weeks or months (218, 224). Unilateral and, in particular,bilateral pallidotomies may carry a higher risk of neurologicalmorbidity, including lethargy and hemiparesis (270, 345), evenin the absence of hemorrhagic complications. Excellent resultsfrom bilateral stimulation of the GPi were initially reported foran 8-year-old child with severe dystonia (75). In this age group,bilateral pallidotomies were considered by the authors to beparticularly risky (74), and DBS was attempted as a compas-sionate, last-resort alternative. The results encouraged formalassessment of this technique with prospective cohorts. In most
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC823

of the literature, treatment outcomes for generalized dystoniaare measured using the Burke-Fahn-Marsden Dystonia RatingScale (BFMDRS), whereas treatment outcomes for torticollisare assessed using the Toronto West Spasmodic TorticollisRating Scale. The former has a total of 120 points (higher isworse) and takes into account the severity at each segment aswell as the provoking factors. The latter scale, which is specificfor torticollis, takes into account severity, disability, and pain.
In 2004, Coubes et al. (74) reported on the long-term resultsof 31 patients with primary generalized dystonia, 14 of whomwere positive for the DYT-1 gene mutation. There was an over-all mean improvement of 50% in the BFMDRS at 3 months,with additional gains observed at the 2-year follow-up evalua-tion, reaching a mean improvement of 65%. DYT-1-positivepatients had improved more (74%) than patients with DYT-1-negative disease (58%). Subsequent series also found betteroutcomes among primary dystonia patients (92), with mostdramatic improvements observed in patients with disease ofearly onset (184). Gradual improvement (or maintenance) ofresults after 3 years has been demonstrated (364), further vali-dating DBS for treatment of generalized dystonia. Significantand sustained long-term improvements have been reported inpatients with spasmodic torticollis (49).
Pallidal stimulation for dystonia has been formally assessedin prospective, controlled, multicenter studies. Results from aseries of 22 patients with primary generalized dystonia (sevenof whom were DYT-1 positive) were described by Vidailhetand the French Stimulation du Pallidum Interne dans laDystonie Study Group (363). At the 3-month follow-up, inves-tigators who were blind to the status of stimulation assesseddystonia severity through video recordings. At 12 months, thedystonia-movement scores had decreased to a mean of 21, com-pared with a baseline preoperative mean score of 46.3. Similarblinding methodologies were used by Kupsch and the DBS forDystonia Study Group (194) to assess patients with primarygeneralized or segmental dystonia. Greater reductions in thedystonia-movement scores were evident in the stimulationgroup (15.8 points, 39.3%) than in the sham stimulation group(1.4 points, 4.9%). Surprisingly, there were no significant differ-ences in the degree of amelioration of patients who were posi-tive for the DYT-1 mutation versus those who were negative forthe mutation. Significant differences were also not apparentwhen the outcomes of patients with generalized dystonia werecompared with those with segmental dystonia.
In summary, GPi or STN DBS has been demonstrated to beeffective in alleviating the symptoms of medically refractoryPD in multiple reports in the literature. These results were con-firmed by prospective series with double-blinded assessmentsand were largely sustained at 5-year follow-up evaluations. Atrend exists in favor of STN versus GPi DBS that must be ver-ified once the outcome of additional studies comparing GPiand STN is available.
Chronic stimulation of the VIM thalamus has become theprocedure of choice for the treatment of tremors because of itsassociated high efficacy rates and low risks. VIM DBS is alsohighly effective for PD tremor, but it is rarely performed today
for PD because both STN and GPi DBS significantly improvetremor as well as other manifestations of PD. Patients withaxial tremors tend to benefit from bilateral stimulation, whichcarries a higher risk of adverse neurological effects.
Bilateral pallidal (GPi) DBS is safe and effective for alleviat-ing primary generalized and segmental dystonia, but theresults may not be evident until after several weeks or monthsof stimulation. Patients who are positive for the DYT-1 muta-tion and those with disease of early onset may experiencegreater benefits.
In reviewing the outcomes of movement-disorder surgery, itis important to emphasize that there should be more random-ized, prospective, and controlled studies in the future. In addi-tion, systematic and standardized assessment, reporting, andpublication of outcome and complications are necessary. Thisincludes the use of published and accepted standardized ratingscales for tremor, PD, and dystonia, with evaluations per-formed by a blinded observer who is unaware of the stimula-tion status (on versus off). The implementation and publicationof standard and rigorous study designs and outcome reportingwill facilitate the acceptance and development of DBS surgeryas a standard therapeutic modality for movement disorders.
Cognitive and Neurobehavioral Outcome andComplications with DBS
The vast majority of data documenting neurobehavioral out-comes after DBS involve patients who underwent surgery inthe STN. The most common neuropsychiatric side effect in theimmediate postoperative period after STN DBS is transientconfusion, with an incidence that ranges between 1 and 36%(5, 18, 61, 72, 95, 107, 131, 138, 177, 244, 250, 281, 285, 286, 303,352, 380, 389, 390). Evidence of greater neuropsychologicaldeficits before surgery is significantly associated withincreased confusion after surgery (284). In general, the datasuggest that the most frequently observed long-term neu-ropsychological change after STN DBS is a decline in word flu-ency. A recent meta-analysis of the available data confirmedthis finding (281). The meta-analysis revealed much smaller,yet significant, declines on measures assessing executive func-tion, verbal learning, and memory. These findings are consis-tent with those reviewed elsewhere in the literature (380, 390).However, it is critical to recall that the majority of availableneuropsychological outcome studies have not included controlgroups, did not statistically control for potential practiceeffects, and generally consisted of small groups, resulting inreduced power; this makes it very difficult to ascertain signif-icant cognitive effects unless the related effect sizes were verylarge. Virtually no studies have clearly identified potential riskfactors for increased cognitive decline after STN DBS. Aybeket al. (18) recently reported that the incidence of conversion todementia in PD patients who underwent STN DBS over a 3-year follow-up period was similar to the incidence reportedfor medically treated patients. Furthermore, risk factors forthe development of dementia in surgical patients were similarto those identified in non-surgical PD patients and includedincreased age, presence of hallucinations, and reduced scores
REZAI ET AL.
SHC824 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com

on measures of executive cognitive function. The preliminarydata suggest that DBS in the STN may result in greater cogni-tive and neurobehavioral changes than GPi DBS in patientswith PD (15, 303, 378). This observation might reflect the rela-tively smaller size of the STN with the increased proximity ofassociative (cognitive), limbic, and motor circuits, and the sub-sequent increased likelihood of misplaced electrodes and/orcurrent spread to non-motor circuits. More detailed, prospec-tive studies are necessary to ascertain the relative neurobe-havioral risks associated with STN versus GPi DBS for thetreatment of PD. Despite the methodological concerns and rel-atively limited data, it appears that STN DBS is a relativelysafe procedure from a neuropsychological perspective in well-selected patients.
Neuropsychiatric symptoms have also been reported afterSTN DBS, and several studies have reported hypomania,depression, apathy, and suicidality (380). Postoperative hypo-mania was reported in 4 to 15% of STN patients in four studies(79, 147, 177, 306), and postoperative depression has beenreported to occur in up to 1.5 to 25% of patients (147, 156, 177,236, 245, 272, 302, 306, 348, 358, 379). The extent to which med-ication changes after surgery contributed to the reportedchanges in mood state is not well known. Overall groupdepression scores have been reported to improve at 3 and 12months after surgery in multiple studies (79, 89, 285, 379); how-ever, most studies relied on reporting group mean depressionscores, which may be misleading. A more accurate indication ofthe number of patients who met criteria for depression beforeand after surgery is a more clinically relevant variable. Someuncontrolled series have documented suicide attempts and/orsuicides after placement of DBS electrodes in the STN (45, 177),but, once again, there are no data to indicate a clear relationshipto stimulation. Within the first 3 postoperative months, apathy,which can respond to administration of dopaminergic medica-tion, can occur, although the incidence is unknown. In con-trast, more permanent apathy was identified in 12% of patients,in whom 80% had associated decreases on executive cognitivemeasures (177). It is important to recognize that all of the neu-ropsychiatric symptoms previously described are evident inmedically managed nonsurgical patients with PD. Conse-quently, it is very difficult to ascertain, on the basis of the cur-rent literature, the extent to which STN DBS is truly associatedwith increased neuropsychiatric symptoms versus the role ofunderlying ongoing disease progression.
The neurobehavioral outcome literature after DBS in theGPi and VIM is much more limited than that pertaining toSTN DBS. Many studies examining cognitive and neuropsy-chiatric outcomes after GPi DBS documented no significantdeclines. Isolated studies identified mild declines on measuresof word fluency and visuoconstructional skills (380). Thereare very few studies examining neurobehavioral outcomesafter VIM stimulation, and interpretation of the available datais confounded by small samples of patients with mixed diag-noses. In general, most of the data revealed no significantcognitive or neuropsychiatric declines. Improvements in ver-bal memory were documented in two studies, whereas
declines in word fluency were documented after left-sidedVIM stimulation in one study (380).
In summary, the neurobehavioral outcome literature suggestthat the cognitive effects associated with DBS in the STN, GPi,and VIM are relatively minor in well-selected patients. Theneuropsychiatric outcome data are more limited, and surgeonsshould be alert to the possibility of neuropsychiatric symptomsafter surgery, particularly STN DBS, but it is still unknownwhether these symptoms reflect neurosurgical/neurostimula-tion effects or ongoing disease progression.
Complications of DBS Surgery
Understanding the complications of any surgical procedurehelps in anticipating, preventing, recognizing, and promptlyintervening on such occasions. The complications of DBS sur-gery can be mainly classified into four categories. These includeintracranial hemorrhages, infections, hardware-related issues,and stimulation-related complications. The incidence ofreported complications is variable among centers and has beenchanging over the past few years as a result of the increasedexperience of the surgical team, advancement in techniques,and improvement in devices. Another factor contributing tothe observed variability in complication reporting is the lack ofa systemic and consistent process for complication definition,recording, and assessment. For example, not all centers report-ing outcomes obtain postoperative imaging to evaluate for ahemorrhage that is nonsymptomatic. Instead, imaging is onlyperformed if there is clinical change in the patients. Similarly,the reporting of infections is inconsistent because the definitionof “infection” varies (i.e., an infection that requires hardwareexplantation versus a superficial wound infection).
Intracranial HemorrhageIntracranial hemorrhage is one of the most important compli-
cations of movement-disorder surgery. Intraoperative hemor-rhages are reported to occur in 0.2 to 12.5% of all STN DBScases (43, 46, 47, 50, 84, 121, 139, 161, 171, 173, 175, 177, 211, 212,229, 347, 356, 361). The correlation of hemorrhage with the typeof procedure is an area of controversy. According to Blomstedtand Hariz (50), there is no significant difference between thehemorrhage risk in lesioning (1.6%) versus DBS surgeries.Terao et al. (347), however, reported a lesion surgery bleedingrate of 15.8% (thalamotomy, 21.7%; pallidotomy, 11.8%) versusa hemorrhage rate in DBS operations of 3.4% (347). Hemor-rhages can be extradural, subdural, and intraparenchymal.Intraparenchymal hemorrhages are the most common and typ-ically occur in the tract of the electrode or in the periventricu-lar region in close proximity to vessels associated with the ven-tricles (Fig. 17). The size of the hemorrhages is generally small.There is little agreement on the predictors of intraoperativehemorrhages in patients who undergo DBS. The common fac-tors identified include:1) High blood pressure: the practices of carefully controlling
blood pressure and painstakingly planning the trajectory,avoiding vasculature seen on the contrast-enhanced preop-
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC825
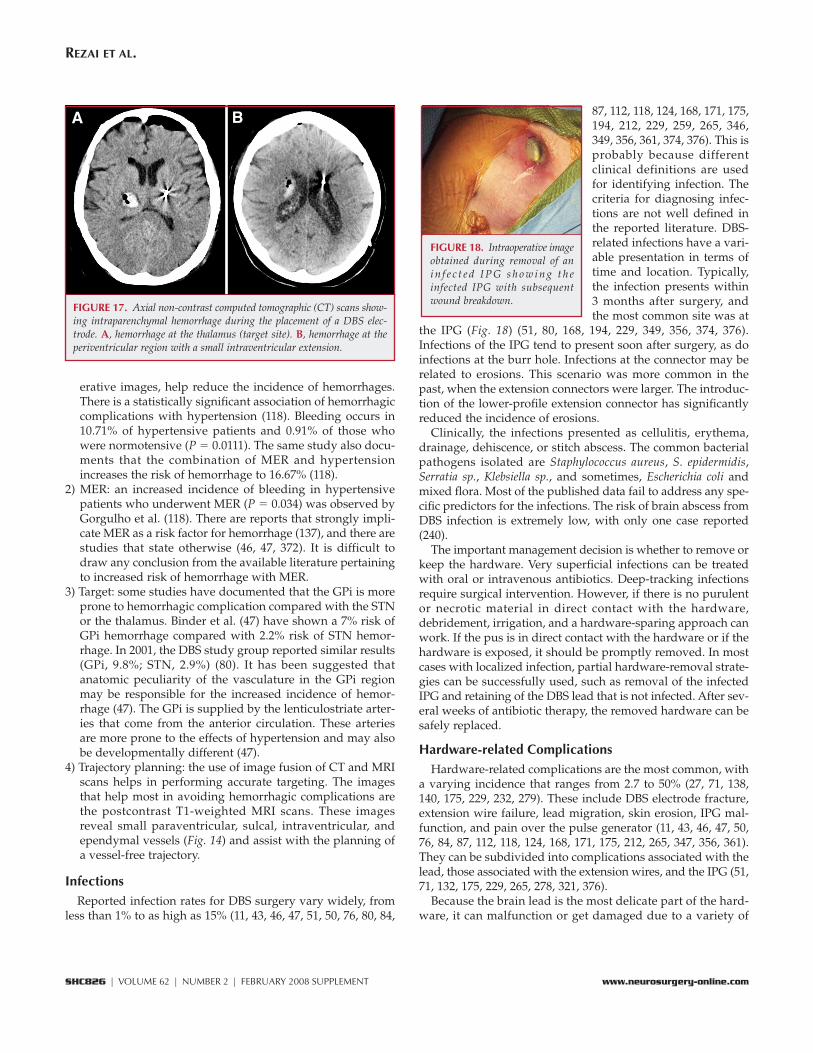
erative images, help reduce the incidence of hemorrhages.There is a statistically significant association of hemorrhagiccomplications with hypertension (118). Bleeding occurs in10.71% of hypertensive patients and 0.91% of those whowere normotensive (P � 0.0111). The same study also docu-ments that the combination of MER and hypertensionincreases the risk of hemorrhage to 16.67% (118).
2) MER: an increased incidence of bleeding in hypertensivepatients who underwent MER (P � 0.034) was observed byGorgulho et al. (118). There are reports that strongly impli-cate MER as a risk factor for hemorrhage (137), and there arestudies that state otherwise (46, 47, 372). It is difficult todraw any conclusion from the available literature pertainingto increased risk of hemorrhage with MER.
3) Target: some studies have documented that the GPi is moreprone to hemorrhagic complication compared with the STNor the thalamus. Binder et al. (47) have shown a 7% risk ofGPi hemorrhage compared with 2.2% risk of STN hemor-rhage. In 2001, the DBS study group reported similar results(GPi, 9.8%; STN, 2.9%) (80). It has been suggested thatanatomic peculiarity of the vasculature in the GPi regionmay be responsible for the increased incidence of hemor-rhage (47). The GPi is supplied by the lenticulostriate arter-ies that come from the anterior circulation. These arteriesare more prone to the effects of hypertension and may alsobe developmentally different (47).
4) Trajectory planning: the use of image fusion of CT and MRIscans helps in performing accurate targeting. The imagesthat help most in avoiding hemorrhagic complications arethe postcontrast T1-weighted MRI scans. These imagesreveal small paraventricular, sulcal, intraventricular, andependymal vessels (Fig. 14) and assist with the planning ofa vessel-free trajectory.
InfectionsReported infection rates for DBS surgery vary widely, from
less than 1% to as high as 15% (11, 43, 46, 47, 51, 50, 76, 80, 84,
87, 112, 118, 124, 168, 171, 175,194, 212, 229, 259, 265, 346,349, 356, 361, 374, 376). This isprobably because differentclinical definitions are usedfor identifying infection. Thecriteria for diagnosing infec-tions are not well defined inthe reported literature. DBS-related infections have a vari-able presentation in terms oftime and location. Typically,the infection presents within3 months after surgery, andthe most common site was at
the IPG (Fig. 18) (51, 80, 168, 194, 229, 349, 356, 374, 376).Infections of the IPG tend to present soon after surgery, as doinfections at the burr hole. Infections at the connector may berelated to erosions. This scenario was more common in thepast, when the extension connectors were larger. The introduc-tion of the lower-profile extension connector has significantlyreduced the incidence of erosions.
Clinically, the infections presented as cellulitis, erythema,drainage, dehiscence, or stitch abscess. The common bacterialpathogens isolated are Staphylococcus aureus, S. epidermidis,Serratia sp., Klebsiella sp., and sometimes, Escherichia coli andmixed flora. Most of the published data fail to address any spe-cific predictors for the infections. The risk of brain abscess fromDBS infection is extremely low, with only one case reported(240).
The important management decision is whether to remove orkeep the hardware. Very superficial infections can be treatedwith oral or intravenous antibiotics. Deep-tracking infectionsrequire surgical intervention. However, if there is no purulentor necrotic material in direct contact with the hardware,debridement, irrigation, and a hardware-sparing approach canwork. If the pus is in direct contact with the hardware or if thehardware is exposed, it should be promptly removed. In mostcases with localized infection, partial hardware-removal strate-gies can be successfully used, such as removal of the infectedIPG and retaining of the DBS lead that is not infected. After sev-eral weeks of antibiotic therapy, the removed hardware can besafely replaced.
Hardware-related ComplicationsHardware-related complications are the most common, with
a varying incidence that ranges from 2.7 to 50% (27, 71, 138,140, 175, 229, 232, 279). These include DBS electrode fracture,extension wire failure, lead migration, skin erosion, IPG mal-function, and pain over the pulse generator (11, 43, 46, 47, 50,76, 84, 87, 112, 118, 124, 168, 171, 175, 212, 265, 347, 356, 361).They can be subdivided into complications associated with thelead, those associated with the extension wires, and the IPG (51,71, 132, 175, 229, 265, 278, 321, 376).
Because the brain lead is the most delicate part of the hard-ware, it can malfunction or get damaged due to a variety of
REZAI ET AL.
SHC826 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
FIGURE 17. Axial non-contrast computed tomographic (CT) scans show-ing intraparenchymal hemorrhage during the placement of a DBS elec-trode. A, hemorrhage at the thalamus (target site). B, hemorrhage at theperiventricular region with a small intraventricular extension.
BA
FIGURE 18. Intraoperative imageobtained during removal of ani n f e c t e d I P G s h o w i n g t h einfected IPG with subsequentwound breakdown.

causes. These include leadfracture, lead erosion, andlead malfunction. The frac-tures are most often the resultof a fall or trauma (Fig. 19).However, fractures can occursecondary to migration of theconnector to the neck (296) oreven with unusual condi-tions, such as compulsivetwisting (232). Lead erosion isnot commonly observed andis usually caused by superfi-cial placement of the lead.Lead malfunctions are gener-ally related to connector mi-gration in the cervical regionthat causes stress on the leadand results in multiple open
or short circuits. Complications associated with extensionwires are more uncommon than of the DBS lead because theextension material is more robust. Extension wire complica-tions include erosions (if placed superficially), fractures, andpain and/or tightness that result from superficial placement(51, 71, 132, 175, 229, 265, 278, 321, 376). Complications asso-ciated with the IPG include erosion, caudal migration of IPGs,and shocking sensations at the IPG site (51, 71, 87, 132, 175,265, 278, 321, 376). Subfascial implantation of the IPG is analternative to subcutaneous implantation and may be advan-tageous in very thin patients.
Stimulation-related ComplicationsThese are complications associated with programming of the
DBS system after surgery. For the most part, these complica-tions are reversible and require vigilance of the programmer.However, if a DBS lead is placed suboptimally, even the mostexpert programming cannot help, and the patient may requirerevision surgery.
The most common stimulation-induced complications aredyskinesias, worsening of axial symptoms, speech dysfunc-tion, capsular stimulation, and ocular symptoms. Stimulation-induced dyskinesias can be a good sign of accurate placementand are generally self-limiting (179, 217). They are observedafter STN DBS and may require adjustment in stimulationparameters or change of dosage of dopaminergic medications(87, 217). Worsening of axial symptoms such as freezing andbalance and gait disturbance have been reported in some stud-ies (59, 87, 104, 127, 170, 271, 394). It has been suggested thatchanging the active contact and adjusting the stimulationparameters are generally helpful (87, 127). Dysarthria or hypo-phonia as a side effect of STN stimulation is observed in 4 to17% of patients (59, 87, 104, 127, 170, 271, 394). The etiology isconsidered to be the spread of current to the capsule. Movingthe active contact away from the capsule or reducing the ampli-tude may help reduce this side effect (87). Capsular stimulationcan also cause muscle contraction that can be focal or general-
ized on the side contralateral to the stimulation. The treatmentfor this is steering the current away from the capsule by adjust-ing the stimulation-field parameters (87). Stimulation can alsoinduce side effects in ocular movements causing either monoc-ular deviation (spread to oculomotor nucleus), conjugate gazedeviation (spread to capsule) or eyelid apraxia (87, 179).Overall, the stimulation-induced complications must be moni-tored with the neurologist and the programming team.
In summary, as the number of DBS surgeries increases, therewill be more complications. The hypervigilance of the team isnecessary to avoid, recognize, and manage complications asso-ciated with DBS implants.
Neurorestorative Surgical Approaches for PDDBS is currently the best surgical approach for movement
disorders with respect to safety, efficacy, and proven trackrecord. However, DBS is an implantable device, with its asso-ciated complications, and it treats the symptoms of the patientand not the underlying disease. In this context, restorativestrategies aimed at treating the underlying disease pathophys-iology are important.
A variety of surgical neurorestorative approaches have beendeveloped in an attempt to prevent the loss of nigral neuronsand stimulate the regeneration of nigrostriatal projections.These include the delivery of protein trophic factors, the deliv-ery of therapeutic genes, and the transplantation of a variety ofpotentially restorative cell types.
Delivery of Therapeutic Growth FactorsTranslational research on growth factors for PD has focused
on the glial-derived neurotrophic factor (GDNF), family lig-ands, and neurturin. Much of the literature supports the abilityof these proteins to protect dopaminergic neurons from a vari-ety of toxic insults in cell culture and rodent and primate mod-els (3). These observations led to two separate open-label stud-ies of GDNF infusions into the human parkinsonian putamen(114, 324). Both open-label studies demonstrated significantimprovements in UPDRS scores in the recipients. The secondstudy demonstrated a gradual return to baseline in the firstyear after cessation of GDNF delivery. Enthusiasm generatedby these open-label trials led to an international, multicenter,randomized placebo-controlled trial sponsored by Amgen(Thousand Oaks, CA) and Medtronic. In this study, patientswere randomized to receive either GDNF or vehicle throughbilateral putamenal catheters. The approach was abandonedby the sponsors after the safety and efficacy data werereviewed, including the development of anti-GDNF antibodiesin some of the patients, and the observation that some monkeyshad developed cerebellar lesions attributed to putamenalGDNF therapy. Results of the study at the time of terminationrevealed no significant difference between the placebo andtreatment groups, although positron-emission tomographicimaging revealed increased dopamine production in the treat-ment group in the region immediately adjacent to the cannulatip (199). Proponents of intraparenchymal GDNF infusion ther-apy cite potential problems with catheter design and drug dis-
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC827
FIGURE 19. Lateral cranial x-ray showing two DBS leads, oneof which is broken with a curvedend (arrow). This patient pre-sented with loss of efficacy andlocal pain due to the hook-like partof the electrode pressing on thescalp.

tribution as possible reasons for the trial’s failure (317).Ongoing research with a naturally-occurring structural andfunctional analog of GDNF, neurturin, suggest that this growthfactor may also offer a potential means of dopamine neuronprotection via intraparenchymal delivery.
Delivery of Therapeutic GenesTwo separate restorative gene-therapy strategies have entered
clinical trials: trophic factor gene delivery and dopaminereplacement. Ceregene (San Diego, CA) has taken the lead onstereotactic growth factor gene therapy with its product CERE-120, an adeno-associated viral vector for the delivery of thegene for neurturin. The basis for the Ceregene trial can befound in the primate studies of striatal GDNF gene deliverywith viral vectors, which demonstrated protection of striataldopamine delivery with tyrosine hydroxylase staining,positron-emission tomography, and behavior studies in twodifferent monkey models. Preclinical studies by Ceregenedemonstrated that CERE-120 could similarly protect dopamineneurons in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridinemonkey model (176), as well as enhance dopamine markersand activity in aged primates. The Phase I CERE-120 trial testedthe safety and tolerability of putamenal CERE-120 injection in12 patients. Surgery consisted of four injections targeting theputamen on each side, with two deposits at each injection site.Open-label follow-up of this initial cohort for 6 months hasrevealed no serious adverse events or decline in neurologicalcondition. UPDRS off scores were reported to improve byroughly 40% in these Phase I patients at 12 months postdosingcompared with each patient’s own baseline (P � 0.001) (333).On the basis of these results, a Phase II sham-surgery, con-trolled, multicenter trial was initated in December 2006.
The next strategy, alteration of neurotransmitter production,has been pursued by three groups. The first trial (Genzyme,Westborough, MA) uses an adeno-associated viral vector todeliver the gene for aromatic amino acid L-dopa decarboxylase(AADC). Initial experiments demonstrated that AADC expres-sion in the putamen could restore striatal dopamine when L-dopa was administered in animal models of PD (21). This strat-egy provides a potential means to control the amount ofdopamine produced through the amount of L-dopa adminis-tered. The investigators hypothesized that this approach wouldprevent the development of runaway dyskinesias such as thosethat complicated fetal mesencephalic transplants. This team(21) conducted extensive preclinical studies, including anexamination of the role of convection-enhanced delivery inviral injection as well as testing of a silicon tubing injectioncannula. The issue of ideal cannula design has emerged asimportant to prevent vector-cannula binding with a resultingdecrease in the titer delivered. The ongoing Phase I trial hasincluded patients at the University of California, San Franciscowith bilateral intrastriatal adeno-associated viral-AADC injec-tions. To date, there have been no serious adverse events.Positron-emission tomography studies in initial patientsdemonstrated a 15% increase in striatal AADC activity 6months after injection.
A second trial has been pursued by Oxford Biomedica(Oxford, England) for stereotactic injection of a lentiviral vectorcarrying three separate transgenes: tyrosine hydroxylase,AADC, and guanosine triphosphate cyclohydrolase I. Together,these gene products are capable of driving autonomous pro-duction of L-dopa with subsequent dopamine production.Thus, unlike the Genzyme strategy, the Biomedica vector,named Prosavin, will drive dopamine production independentof L-dopa administration (388). The company plans a Prosavintrial in either England or France.
A third gene-therapy approach has been advanced byNeurologix (Fort Lee, NJ). This approach induces subthalamicand pallidal inhibition through the expression of glutamatedecarboxylase in the STN. Glutamate decarboxylase is theenzyme that changes glutamate to GABA. Thus, inhibition isaffected by the production of GABA in the STN, and a reductionin efferent glutamate. Twelve patients received unilateral STNinjection at three escalating doses (n � 4 patients per group) tominimize risk. Investigators reported sustained improvementsin UPDRS motor scores at 12 months (24% off state and 27% onstate), with no serious adverse events related to gene therapy.Positron-emission tomographic studies confirmed reduction inthalamic metabolism (163). As the Neurologix project was thefirst PD gene therapy trial to pass through regulation, particu-lar care was required in addressing safety over efficacy (asreflected in the decision to inject unilaterally). The authors notethat effects were proportionally larger on the side contralateralto infusion, which lends weight to the hypothesis that gene-based STN inhibition can provide a benefit beyond placebo.
Cell Transplantation DeliveryThe approach of cell transplantation has the longest history,
and perhaps, the most complex landscape. A wide variety ofcells have been studied as potential means to provide neuro-protection and potentially replace lost dopamine neurons.Initial efforts used autografts of adrenal medullary cells as apotential source of dopamine but failed to show consistentimprovements (97). Subsequent efforts involved the transplan-tation of fetal mesencephalic tissue containing nigral dopaminecells transplanted into the putamen. Results in this studyproved inconsistent as well, with some patients showingimprovements. However, a subset of patients developed anexacerbation of dyskinesias thought to be a result of heteroge-neous and uncontrolled production of dopamine throughoutthe putamen (106, 305). Contemporary efforts at neural trans-plantation have involved putamenal implantation of retinalpigment epithelial cells grown in a bead matrix calledSpheramine (Titan, San Francisco, CA). Retinal pigment epithe-lial cells can produce L-dopa, but also appear to havetrophic/protective effects on adjoining neurons (305, 335). Anongoing Phase II, controlled, multicenter trial is under way toassess the safety and efficacy of Spheramine implants.
Advances in stem cell technology have made it possible tomanufacture dopaminergic neurons. A wide variety of proto-cols have been developed for the production of dopamine cellsfrom embryonic stem cells, fetal-derived uncommitted and
REZAI ET AL.
SHC828 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com

committed progenitors, and even adult progenitors harvestedfrom the subventricular zone. Parallel strategies have beendeveloped to purify the dopaminergic cells from nondopamin-ergic cells in these preparations with the hope of creating asustainable, practical source for pure, differentiated, humandopaminergic cells. Finally, a fusion of gene-delivery technol-ogy with transplantation (ex vivo gene transfer) provides apotential means to control these cells, hence reducing thepotential for the runaway dyskinesias to occur that wereobserved in the fetal transplant.
Surgery for Movement Disorders: Future DirectionsThe field of functional neurosurgery has witnessed a renais-
sance over the past 20 years. This development has been fueledby progress in the neurobiology of movement disorders, surgi-cal technical advancements, therapeutic device developments,and innovative approaches. The growth in our understandingof the neural circuitry of the disease has determined andrefined our surgical targets. This increased understanding ofthe neurobiology of movement disorders will guide the discov-ery of additional targets for surgical exploration and transla-tional clinical research.
The evolution of stereotactic surgical tools and techniques isfacilitating safe and minimally invasive approaches that enableneurosurgeons to target various brain structures with reliableaccuracy. This, coupled with rapid advances in imaging tech-nology and capabilities, will play an important role in improv-ing our capability to visualize brain structures and functionwith unparalleled resolution.
At present, DBS is the standard therapy of choice formovement-disorder patients who are medication intractableand who meet the surgical selection criteria. DBS has a provensafety and efficacy profile and long-term outcomes have beendemonstrated by prospective, randomized studies. Technologi-cal advances in DBS systems have already resulted in improve-ments and will continue to do so. The next-generation DBSsystems will be smaller and rechargeable, with current steeringfeatures and built-in sensing capabilities.
A number of clinical trials are under way to explore the util-ity of gene therapy and cell transplantation and stem cellapproaches with promising preliminary outcomes. In the nearfuture, these technologies will provide additional options forneurosurgical management of movement disorders.
Functional neurosurgery is one of the most exciting and rap-idly growing areas in neurosurgery. Despite significantadvances, this arena of neurosurgery is still in its infancy. Themovement-disorder surgery evolution can be argued to be amodel approach for development of neurosurgical therapies.The lessons learned from movement-disorder surgical experi-ence are already being applied to surgical treatment of psychi-atric and other chronic neurological disorders.
REFERENCES
1. Abosch A, Lozano A: Stereotactic neurosurgery for movement disorders.Can J Neurol Sci 30 [Suppl 1]:S72–S82, 2003.
2. Agid Y: Parkinson’s disease: Pathophysiology. Lancet 337:1321–1324, 1991.3. Airaksinen MS, Saarma M: The GDNF family: Signalling, biological func-
tions and therapeutic value. Nat Rev Neurosci 3:383–394, 2002.4. Akert K, Koella WP, Hess R Jr: Sleep produced by electrical stimulation of
the thalamus. Am J Physiol 168:260–267, 1952.5. Alegret M, Junque C, Valldeoriola F, Vendrell P, Pilleri M, Rumia J, Tolosa E:
Effects of bilateral subthalamic stimulation on cognitive function inParkinson disease. Arch Neurol 58:1223–1227, 2001.
6. Alesch F, Pinter MM, Helscher RJ, Fertl L, Benabid AL, Koos WT:Stimulation of the ventral intermediate thalamic nucleus in tremor domi-nated Parkinson’s disease and essential tremor. Acta Neurochir (Wien)136:75–81, 1995.
7. Alexander GE, DeLong MR, Strick PL: Parallel organization of functionallysegregated circuits linking basal ganglia and cortex. Annu Rev Neurosci9:357–381, 1986.
8. Alterman RL, Kall BA, Cohen H, Kelly PJ: Stereotactic ventrolateral thalam-otomy: Is ventriculography necessary? Neurosurgery 37:717–722, 1995.
9. Alterman RL, Shils JL, Miravite J, Tagliati M: Lower stimulation frequencycan enhance tolerability and efficacy of pallidal deep brain stimulation fordystonia. Mov Disord 22:366–368, 2007.
10. Alterman RL, Sterio D, Beric A, Kelly PJ: Microelectrode recording duringposteroventral pallidotomy: Impact on target selection and complications.Neurosurgery 44:315–323, 1999.
11. Amirnovin R, Williams ZM, Cosgrove GR, Eskandar EN: Experience withmicroelectrode guided subthalamic nucleus deep brain stimulation.Neurosurgery 58 [Suppl]:ONS96–ONS102, 2006.
12. Anca MH, Zaccai TF, Badarna S, Lozano AM, Lang AE, Giladi N: Naturalhistory of Oppenheim’s dystonia (DYT1) in Israel. J Child Neurol18:325–330, 2003.
13. Anderson T, Hu B, Pittman Q, Kiss ZH: Mechanisms of deep brain stimula-tion: An intracellular study in rat thalamus. J Physiol 559:301–313, 2004.
14. Anderson TR, Hu B, Iremonger K, Kiss ZH: Selective attenuation of afferentsynaptic transmission as a mechanism of thalamic deep brain stimulation-induced tremor arrest. J Neurosci 26:841–850, 2006.
15. Anderson VC, Burchiel KJ, Hogarth P, Favre J, Hammerstad JP: Pallidal vssubthalamic nucleus deep brain stimulation in Parkinson disease. ArchNeurol 62:554–560, 2005.
16. Andrade-Souza YM, Schwalb JM, Hamani C, Eltahawy H, Hoque T, Saint-Cyr J, Lozano AM: Comparison of three methods of targeting the subthala-mic nucleus for chronic stimulation in Parkinson’s disease. Neurosurgery56:360–368, 2005.
17. Andrade-Souza YM, Schwalb JM, Hamani C, Hoque T, Saint-Cyr J, LozanoAM: Comparison of 2-dimensional magnetic resonance imaging and 3-pla-nar reconstruction methods for targeting the subthalamic nucleus inParkinson disease. Surg Neurol 63:357–363, 2005.
18. Aybek S, Gronchi-Perrin A, Verney A, Chiuvé SC, Villemure JG, Bukhard PR,Vingerhoets FJ: Long-term cognitive profile and incidence of dementia afterSTN-DBS in Parkinson’s disease. Mov Disord 22:974–981, 2007.
19. Aziz TZ, Nandi D, Parkin S, Liu X, Giladi N, Bain P, Gregory RG, Joint C,Scott RB, Stein JF: Targeting the subthalamic nucleus. Stereotact FunctNeurosurg 77:87–90, 2001.
20. Baev KV, Greene KA, Marciano FF, Samanta JE, Shetter AG, Smith KA, StacyMA, Spetzler RF: Physiology and pathophysiology of cortico-basal ganglia-thalamocortical loops: Theoretical and practical aspects. Prog Neuro-psychopharmacol Biol Psychiatry 26:771–804, 2002.
21. Bankiewicz KS, Forsayeth J, Eberling JL, Sanchez-Pernaute R, Pivirotto P,Bringas J, Herscovitch P, Carson RE, Eckelman W, Reutter B, Cunningham J:Long-term clinical improvement in MPTP-lesioned primates after gene ther-apy with AAV-hAADC. Mol Ther 14:564–570, 2006.
22. Bechtereva NP, Bondartchuk AN, Smirnov VM, Meliutcheva LA,Shandurina AN: Method of electrostimulation of the deep brain structuresin treatment of some chronic diseases. Confin Neurol 37:136–140, 1975.
23. Bejjani B, Damier P, Arnulf I, Bonnet AM, Vidailhet M, Dormont D, PidouxB, Cornu P, Marsault C, Agid Y: Pallidal stimulation for Parkinson’s disease.Two targets? Neurology 49:1564–1569, 1997.
24. Bejjani BP, Dormont D, Pidoux B, Yelnik J, Damier P, Arnulf I, Bonnet AM,Marsault C, Agid Y, Philippon J, Cornu P: Bilateral subthalamic stimulationfor Parkinson’s disease by using three-dimensional stereotactic magnetic
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC829
resonance imaging and electrophysiological guidance. J Neurosurg92:615–625, 2000.
25. Benabid AL, Benazzouz A, Hoffmann D, Limousin P, Krack P, Pollak P:Long-term electrical inhibition of deep brain targets in movement disor-ders. Mov Disord 13 [Suppl 3]:119–125, 1998.
26. Benabid AL, Benazzouz A, Limousin P, Koudsie A, Krack P, Piallat B, PollakP: Dyskinesias and the subthalamic nucleus. Ann Neurol 47 [Suppl1]:S189–S192, 2000.
27. Benabid AL, Chabardes S, Seigneuret E: Deep-brain stimulation inParkinson’s disease: Long-term efficacy and safety—What happened thisyear? Curr Opin Neurol 18:623–630, 2005.
28. Benabid AL, Deuschl G, Lang AE, Lyons KE, Rezai AR: Deep brain stimula-tion for Parkinson’s disease. Mov Disord 21 [Suppl 14]:S168–S170, 2006.
29. Benabid AL, Koudsie A, Benazzouz A, Fraix V, Ashraf A, Le Bas JF,Chabardes S, Pollak P: Subthalamic stimulation for Parkinson’s disease.Arch Med Res 31:282–289, 2000.
30. Benabid AL, Koudsie A, Benazzouz A, Le Bas JF, Pollak P: Imaging of sub-thalamic nucleus and ventralis intermedius of the thalamus. Mov Disord 17[Suppl 3]:S123–S129, 2002.
31. Benabid AL, Krack PP, Benazzouz A, Limousin P, Koudsie A, Pollak P:Deep brain stimulation of the subthalamic nucleus for Parkinson’s dis-ease: Methodologic aspects and clinical criteria. Neurology 55 [Suppl6]:S40–S44, 2000.
32. Benabid AL, Pollak P, Gao D, Hoffmann D, Limousin P, Gay E, Payen I,Benazzouz A: Chronic electrical stimulation of the ventralis intermediusnucleus of the thalamus as a treatment of movement disorders. J Neurosurg84:203–214, 1996.
33. Benabid AL, Pollak P, Gervason C, Hoffmann D, Gao DM, Hommel M,Perret JE, de Rougemont J: Long-term suppression of tremor by chronicstimulation of the ventral intermediate thalamic nucleus. Lancet 337:403–406, 1991.
34. Benabid AL, Pollak P, Gross C, Hoffmann D, Benazzouz A, Gao DM, LaurentA, Gentil M, Perret J: Acute and long-term effects of subthalamic nucleus stim-ulation in Parkinson’s disease. Stereotact Funct Neurosurg 62:76–84, 1994.
35. Benabid AL, Pollak P, Hommel M, Gaio JM, de Rougemont J, Perret J:Treatment of Parkinson tremor by chronic stimulation of the ventral inter-mediate nucleus of the thalamus [in French]. Rev Neurol (Paris) 145:320–323, 1989.
36. Benabid AL, Pollak P, Louveau A, Henry S, de Rougemont J: Combined (thal-amotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus forbilateral Parkinson disease. Appl Neurophysiol 50:344–346, 1987.
37. Benabid AL, Pollak P, Seigneuret E, Hoffmann D, Gay E, Perret J: ChronicVIM thalamic stimulation in Parkinson’s disease, essential tremor and extra-pyramidal dyskinesias. Acta Neurochir Suppl (Wien) 58:39–44, 1993.
38. Benabid AL, Wallace B, Mitrofanis J, Xia R, Piallat B, Chabardes S, Berger F:A putative generalized model of the effects and mechanism of action ofhigh frequency electrical stimulation of the central nervous system. ActaNeurol Belg 105:149–157, 2005.
39. Benazzouz A, Hallett M: Mechanism of action of deep brain stimulation.Neurology 55 [Suppl 6]:S13–S16, 2000.
40. Benazzouz A, Piallat B, Ni ZG, Koudsie A, Pollak P, Benabid AL: Implicationof the subthalamic nucleus in the pathophysiology and pathogenesis ofParkinson’s disease. Cell Transplant 9:215–221, 2000.
41. Bergman H, Deuschl G: Pathophysiology of Parkinson’s disease: From clin-ical neurology to basic neuroscience and back. Mov Disord 17 [Suppl3]:S28–S40, 2002.
42. Bergman H, Wichmann T, DeLong MR: Reversal of experimental parkinson-ism by lesions of the subthalamic nucleus. Science 249:1436–1438, 1990.
43. Beric A, Kelly PJ, Rezai A, Sterio D, Mogilner A, Zonenshayn M, Kopell B:Complications of deep brain stimulation surgery. Stereotact FunctNeurosurg 77:73–78, 2001.
44. Berk C, Carr J, Sinden M, Martzke J, Honey CR: Thalamic deep brain stim-ulation for the treatment of tremor due to multiple sclerosis: A prospectivestudy of tremor and quality of life. J Neurosurg 97:815–820, 2002.
45. Berney A, Vingerhoets F, Perrin A, Guex P, Villemure JG, Burkhard PR,Benkelfat C, Ghika J: Effect on mood of subthalamic DBS for Parkinson’s dis-ease: A consecutive series of 24 patients. Neurology 59:1427–1429, 2002.
46. Binder DK, Rau G, Starr PA: Hemorrhagic complications of microelectrode-guided deep brain stimulation. Stereotact Funct Neurosurg 80:28–31, 2003.
47. Binder DK, Rau GM, Starr PA: Risk factors for hemorrhage during micro-electrode-guided deep brain stimulator implantation for movement disor-ders. Neurosurgery 56:722–732, 2005.
48. Bittar RG, Kar-Purkayastha I, Owen SL, Bear RE, Green A, Wang S, Aziz TZ:Deep brain stimulation for pain relief: A meta-analysis. J Clin Neurosci12:515–519, 2005.
49. Bittar RG, Yianni J, Wang S, Liu X, Nandi D, Joint C, Scott R, Bain PG,Gregory R, Stein J, Aziz TZ: Stereotactic and Functional NeurosurgeryResident Award: Deep brain stimulation for generalized dystonia and spas-modic torticollis: Rate and extent of postoperative improvement. ClinNeurosurg 52:379–383, 2005.
50. Blomstedt P, Hariz MI: Are complications less common in deep brain stim-ulation than in ablative procedures for movement disorders? StereotactFunct Neurosurg 84:72–81, 2006.
51. Blomstedt P, Hariz MI: Hardware-related complications of deep brain stim-ulation: A ten year experience. Acta Neurochir (Wien) 147:1061–1064, 2005.
52. Blond S, Siegfried J: Thalamic stimulation for the treatment of tremor andother movement disorders. Acta Neurochir Suppl (Wien) 52:109–111, 1991.
53. Bonnet AM, Houeto JL: Pathophysiology of Parkinson’s disease. BiomedPharmacother 53:117–121, 1999.
54. Brice J, McLellan L: Suppression of intention tremor by contingent deep-brain stimulation. Lancet 1:1221–1222, 1980.
55. Brown P: Bad oscillations in Parkinson’s disease. J Neural Transm Suppl70:27–30, 2006.
56. Brown P: Oscillatory nature of human basal ganglia activity: Relationship tothe pathophysiology of Parkinson’s disease. Mov Disord 18:357–363, 2003.
57. Bryant JA, De Salles A, Cabatan C, Frysinger R, Behnke E, Bronstein J: Theimpact of thalamic stimulation on activities of daily living for essentialtremor. Surg Neurol 59:479–485, 2003.
58. Bucher SF, Seelos KC, Dodel RC, Reiser M, Oertel WH: Activation mappingin essential tremor with functional magnetic resonance imaging. AnnNeurol 41:32–40, 1997.
59. Burchiel KJ, Anderson VC, Favre J, Hammerstad JP: Comparison of pallidaland subthalamic nucleus deep brain stimulation for advanced Parkinson’sdisease: Results of a randomized, blinded pilot study. Neurosurgery45:1375–1384, 1999.
60. Carpenter LL: Neurostimulation in resistant depression. J Psychopharmacol20 [Suppl]:35–40, 2006.
61. Castelli L, Perozzo P, Zibetti M, Crivelli B, Morabito U, Lanotte M, Cossa F,Bergamasco B, Lopiano L: Chronic deep brain stimulation of the subthalamicnucleus for Parkinson’s disease: Effects on cognition, mood, anxiety andpersonality traits. Eur Neurol 55:136–144, 2006.
62. Ceballos-Baumann AO: Functional imaging in Parkinson’s disease: activa-tion studies with PET, fMRI and SPECT. J Neurol 250 [Suppl 1]:I15–I23,2003.
63. Ceballos-Baumann AO, Boecker H, Fogel W, Alesch F, Bartenstein P, ConradB, Diederich N, von Falkenhayn I, Moringlane JR, Schwaiger M, TronnierVM: Thalamic stimulation for essential tremor activates motor and deacti-vates vestibular cortex. Neurology 56:1347–1354, 2001.
64. Chapman WP, Livingston KE, Poppen JL: Effect upon blood pressure ofelectrical stimulation of tips of temporal lobes in man. J Neurophysiol13:65–71, 1950.
65. Chapman WP, Livingston RB, Livingston KE: Frontal lobotomy and electri-cal stimulation of orbital surface of frontal lobes; effect on respiration and onblood pressure in man. Arch Neurol Psychiatry 62:701–716, 1949.
66. Chen CC, Kuhn AA, Trottenberg T, Kupsch A, Schneider GH, Brown P:Neuronal activity in globus pallidus interna can be synchronized to localfield potential activity over 3–12 Hz in patients with dystonia. Exp Neurol202:480–486, 2006.
67. Cintas P, Simonetta-Moreau M, Ory F, Brefel-Courbon C, Fabre N, ChaynesP, Sabatier J, Sol JC, Rascol O, Berry I, Lazorthes Y: Deep brain stimulationfor parkinson’s disease: Correlation between intraoperative subthalamicnucleus neurophysiology and most effective contacts. Stereotact FunctNeurosurg 80:108–113, 2003.
68. Cobb S, Pool JL, Scarff J, Schwab RS, Walker AE, White JC: Section of U fibersof motor cortex in cases of paralysis agitans (Parkinson’s disease); report of9 cases. Arch Neurol Psychiatry 64:57–59, 1950.
REZAI ET AL.
SHC830 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
69. Coffey RJ, Lozano AM: Neurostimulation for chronic noncancer pain: Anevaluation of the clinical evidence and recommendations for future trialdesigns. J Neurosurg 105:175–189, 2006.
70. Cohen OS, Hassin-Baer S, Spiegelmann R: Deep brain stimulation of theinternal globus pallidus for refractory tardive dystonia. Parkinsonism RelatDisord 13:541–544, 2007.
71. Constantoyannis C, Berk C, Honey CR, Mendez I, Brownstone RM:Reducing hardware-related complications of deep brain stimulation. Can JNeurol Sci 32:194–200, 2005.
72. Contarino MF, Daniele A, Sibilia AH, Romito LM, Bentivoglio AR, GainottiG, Albanese A: Cognitive outcome 5 years after bilateral chronic stimulationof subthalamic nucleus in patients with Parkinson’s disease. J NeurolNeurosurg Psychiatry 78:248–252, 2007.
72a. Cooper IS: Ligation of the anterior choroidal artery for involuntary move-ments; parkinsonism. Psychiatr Q 27:317–319, 1953.
73. Cosyns P, Gabriels L, Nuttin B: Deep brain stimulation in treatment refrac-tory obsessive compulsive disorder. Verh K Acad Geneeskd Belg 65:385–400, 2003.
74. Coubes P, Cif L, El Fertit H, Hemm S, Vayssiere N, Serrat S, Picot MC,Tuffery S, Claustres M, Echenne B, Frerebeau P: Electrical stimulation of theglobus pallidus internus in patients with primary generalized dystonia:Long-term results. J Neurosurg 101:189–194, 2004.
75. Coubes P, Echenne B, Roubertie A, Vayssiere N, Tuffery S, HumbertclaudeV, Cambonie G, Claustres M, Frerebeau P: Treatment of early-onset general-ized dystonia by chronic bilateral stimulation of the internal globus pal-lidus. Apropos of a case [in French]. Neurochirurgie 45:139–144, 1999.
76. Coubes P, Vayssiere N, El Fertit H, Hemm S, Cif L, Kienlen J, Bonafe A,Frerebeau P: Deep brain stimulation for dystonia. Surgical technique.Stereotact Funct Neurosurg 78:183–191, 2002.
77. Crevier PH: Various considerations on pallidotomy for relief of abnormalmovements [in French]. Union Med Can 86:734–750, 1957.
78. Cuny E, Guehl D, Burbaud P, Gross C, Dousset V, Rougier A: Lack of agree-ment between direct magnetic resonance imaging and statistical determina-tion of a subthalamic target: The role of electrophysiological guidance. JNeurosurg 97:591–597, 2002.
79. Daniele A, Albanese A, Contarino MF, Zinzi P, Barbier A, Gasparini F,Romito LM, Bentivoglio AR, Scerrati M: Cognitive and behavioural effects ofchronic stimulation of the subthalamic nucleus in patients with Parkinson’sdisease. J Neurol Neurosurg Psychiatry 74:175–182, 2003.
80. Deep-Brain Stimulation for Parkinson’s Disease Study Group: Deep-brainstimulation of the subthalamic nucleus or the pars interna of the globus pal-lidus in Parkinson’s disease. N Engl J Med 345:956–963, 2001.
81. DeLong MR, Crutcher MD, Georgopoulos AP: Primate globus pallidusand subthalamic nucleus: Functional organization. J Neurophysiol53:530–543, 1985.
82. Delong MR, Georgopoulos AP, Crutcher MD, Mitchell SJ, Richardson RT,Alexander GE: Functional organization of the basal ganglia: Contributions ofsingle-cell recording studies. Ciba Found Symp 107:64–82, 1984.
83. Deogaonkar M, Subramanian T: Pathophysiological basis of drug-induceddyskinesias in Parkinson’s disease. Brain Res Brain Res Rev 50:156–168, 2005.
84. De Salles AA, Frighetto L, Behnke E, Sinha S, Tseng L, Torres R, Lee M,Cabatan-Awang C, Frysinger R: Functional neurosurgery in the MRI envi-ronment. Minim Invasive Neurosurg 47:284–289, 2004.
85. Deuschl G, Bain P: Deep brain stimulation for tremor [correction of trauma]:Patient selection and evaluation. Mov Disord 17 [Suppl 3]:S102–S111, 2002.
86. Deuschl G, Fogel W, Hahne M, Kupsch A, Müller D, Oechsner M, SommerU, Ulm G, Vogt T, Volkmann J: Deep-brain stimulation for Parkinson’s dis-ease. J Neurol 249 [Suppl 3]:36–39, 2002.
87. Deuschl G, Herzog J, Kleiner-Fisman G, Kubu C, Lozano AM, Lyons KE,Rodriguez-Oroz MC, Tamma F, Tröster AI, Vitek JL, Volkmann J, Voon V:Deep brain stimulation: Postoperative issues. Mov Disord 21 [Suppl14]:S219–S237, 2006.
88. Diallo R, Welter ML, Mallet L: Therapeutic management of tics in Tourette’ssyndrome [in French]. Rev Neurol (Paris) 163:375–386, 2007.
89. Dujardin K, Defebvre L, Krystkowiak P, Blond S, Destee A: Influence ofchronic bilateral stimulation of the subthalamic nucleus on cognitive func-tion in Parkinson’s disease. J Neurol 248:603–611, 2001.
90. Eljamel MS, Tulley M, Spillane K: A simple stereotactic method for framelessdeep brain stimulation. Stereotact Funct Neurosurg 85:6–10, 2007.
91. Eltahawy HA, Feinstein A, Khan F, Saint-Cyr J, Lang AE, Lozano AM:Bilateral globus pallidus internus deep brain stimulation in tardive dyskine-sia: A case report. Mov Disord 19:969–972, 2004.
92. Eltahawy HA, Saint-Cyr J, Giladi N, Lang AE, Lozano AM: Primary dysto-nia is more responsive than secondary dystonia to pallidal interventions:Outcome after pallidotomy or pallidal deep brain stimulation. Neurosurgery54:613–621, 2004.
93. Eriksen SK, Tuite PJ, Maxwell RE, Sullivan M, Low WC, Ebner TJ: Bilateralsubthalamic nucleus stimulation for the treatment of Parkinson’s disease:Results of six patients. J Neurosci Nurs 35:223–231, 2003.
94. Erola T, Heikkinen ER, Haapaniemi T, Tuominen J, Juolasmaa A, Myllylä VV:Efficacy of bilateral subthalamic nucleus (STN) stimulation in Parkinson’sdisease. Acta Neurochir (Wien) 148:389–394, 2006.
95. Fields JA, Troster AI: Cognitive outcomes after deep brain stimulation forParkinson’s disease: A review of initial studies and recommendations forfuture research. Brain Cogn 42:268–293, 2000.
96. Filali M, Hutchison WD, Palter VN, Lozano AM, Dostrovsky JO:Stimulation-induced inhibition of neuronal firing in human subthalamicnucleus. Exp Brain Res 156:274–281, 2004.
97. Fine A: Transplantation of adrenal tissue into the central nervous system.Brain Res Brain Res Rev 15:121–133, 1990.
98 Finger S: Origins of Neuroscience. New York, Oxford University Press, 1994,p 39.
99. Foffani G, Ardolino G, Meda B, Egidi M, Rampini P, Caputo E, Baselli G,Priori A: Altered subthalamo-pallidal synchronisation in parkinsonian dysk-inesias. J Neurol Neurosurg Psychiatry 76:426–428, 2005.
100. Foncke EM, Bour LJ, Speelman JD, Koelman JH, Tijssen MA: Local fieldpotentials and oscillatory activity of the internal globus pallidus inmyoclonus-dystonia. Mov Disord 22:369–376, 2007.
101. Foote KD, Okun MS: Ventralis intermedius plus ventralis oralis anterior andposterior deep brain stimulation for posttraumatic Holmes tremor: Twoleads may be better than one: Technical note. Neurosurgery 56 [Suppl]:E445, 2005.
102. Ford B, Winfield L, Pullman SL, Frucht SJ, Du Y, Greene P, Cheringal JH, YuQ, Cote LJ, Fahn S, McKhann GM 2nd, Goodman RR: Subthalamic nucleusstimulation in advanced Parkinson’s disease: Blinded assessments at oneyear follow up. J Neurol Neurosurg Psychiatry 75:1255–1259, 2004.
103. Fox MW, Ahlskog JE, Kelly PJ: Stereotactic ventrolateralis thalamotomy formedically refractory tremor in post-levodopa era Parkinson’s diseasepatients. J Neurosurg 75:723–730, 1991.
104. Fraix V, Pollak P, Moro E, Chabardes S, Xie J, Ardouin C, Benabid AL:Subthalamic nucleus stimulation in tremor dominant parkinsonian patients withprevious thalamic surgery. J Neurol Neurosurg Psychiatry 76:246–248, 2005.
105. Franzini A, Marras C, Ferroli P, Zorzi G, Bugiani O, Romito L, Broggi G: Long-term high-frequency bilateral pallidal stimulation for neuroleptic-induced tar-dive dystonia. Report of two cases. J Neurosurg 102:721–725, 2005.
106. Freed CR, Greene PE, Breeze RE, Tsai WY, DuMouchel W, Kao R, Dillon S,Winfield H, Culver S, Trojanowski JQ, Eidelberg D, Fahn S: Transplantationof embryonic dopamine neurons for severe Parkinson’s disease. N Engl JMed 344:710–719, 2001.
107. Funkiewiez A, Ardouin C, Caputo E, Krack P, Fraix V, Klinger H, ChabardesS, Foote K, Benabid AL, Pollak P: Long term effects of bilateral subthalamicnucleus stimulation on cognitive function, mood, and behaviour inParkinson’s disease. J Neurol Neurosurg Psychiatry 75:834–839, 2004.
108. Garonzik IM, Hua SE, Ohara S, Lenz FA: Intraoperative microelectrode andsemi-microelectrode recording during the physiological localization of the thal-amic nucleus ventral intermediate. Mov Disord 17 [Suppl 3]:S135–S144, 2002.
109. George MS, Nahas Z, Borckardt JJ, Anderson B, Foust MJ, Burns C, Kose S,Short EB: Brain stimulation for the treatment of psychiatric disorders. CurrOpin Psychiatry 20:250–254, 2007.
110. Gerfen CR, Engber TM, Mahan LC, Susel Z, Chase TN, Monsma FJ Jr, SibleyDR: D1 and D2 dopamine receptor-regulated gene expression of striatonigraland striatopallidal neurons. Science 250:1429–1432, 1990.
111. Gilbert DL, Lipps TD: Tourette’s Syndrome. Curr Treat Options Neurol7:211–219, 2005.
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC831
112. Gill CE, Konrad PE, Davis TL, Charles D: Deep brain stimulation forParkinson’s disease: The Vanderbilt University Medical Center experience,1998–2004. Tenn Med 100:45–47, 2007.
113. Giller CA, Dewey RB Jr: Ventralis intermedius thalamotomy can succeedwhen ventralis intermedius thalamic stimulation fails: Report of 2 cases fortremor. Stereotact Funct Neurosurg 79:51–56, 2002.
114. Gill SS, Patel NK, Hotton GR, O’Sullivan K, McCarter R, Bunnage M, BrooksDJ, Svendsen CN, Heywood P: Direct brain infusion of glial cell line-derivedneurotrophic factor in Parkinson disease. Nat Med 9:589–595, 2003.
115. Goldman MS, Ahlskog JE, Kelly PJ: The symptomatic and functional out-come of stereotactic thalamotomy for medically intractable essential tremor.J Neurosurg 76:924–928, 1992.
116. Goldman MS, Kelly PJ: Stereotactic thalamotomy for medically intractableessential tremor. Stereotact Funct Neurosurg 58:22–25, 1992.
117. Goldman MS, Kelly PJ: Symptomatic and functional outcome of stereotac-tic ventralis lateralis thalamotomy for intention tremor. J Neurosurg77:223–229, 1992.
118. Gorgulho A, De Salles AA, Frighetto L, Behnke E: Incidence of hemorrhageassociated with electrophysiological studies performed using macroelec-trodes and microelectrodes in functional neurosurgery. J Neurosurg102:888–896, 2005.
119. Green AL, Nandi D, Armstrong G, Carter H, Aziz T: Post-herpetic trigemi-nal neuralgia treated with deep brain stimulation. J Clin Neurosci 10:512–514, 2003.
120. Greenamyre JT: “Ottorino Rossi” Award 2000. New targets for therapy inParkinson’s disease: Pathogenesis and pathophysiology. Funct Neurol15:67–80, 2000.
121. Greenberg BD, Malone DA, Friehs GM, Rezai AR, Kubu CS, Malloy PF,Salloway SP, Okun MS, Goodman WK, Rasmussen SA: Three-year outcomesin deep brain stimulation for highly resistant obsessive-compulsive disorder.Neuropsychopharmacology 31:2384–2393, 2006.
122. Greenberg BD, Rezai AR: Mechanisms and the current state of deep brainstimulation in neuropsychiatry. CNS Spectr 8:522–526, 2003.
123. Gross CE, Boraud T, Guehl D, Bioulac B, Bezard E: From experimentation tothe surgical treatment of Parkinson’s disease: Prelude or suite in basal gan-glia research? Prog Neurobiol 59:509–532, 1999.
124. Gross RE, Krack P, Rodriguez-Oroz MC, Rezai AR, Benabid AL:Electrophysiological mapping for the implantation of deep brain stimulatorsfor Parkinson’s disease and tremor. Mov Disord 21 [Suppl 14]:S259–S283, 2006.
125. Gross RE, Lombardi WJ, Hutchison WD, Narula S, Saint-Cyr JA, DostrovskyJO, Tasker RR, Lang AE, Lozano AM: Variability in lesion location aftermicroelectrode-guided pallidotomy for Parkinson’s disease: Anatomical,physiological, and technical factors that determine lesion distribution. JNeurosurg 90:468–477, 1999.
126. Gross RE, Lozano AM: Advances in neurostimulation for movement disor-ders. Neurol Res 22:247–258, 2000.
127. Guehl D, Cuny E, Benazzouz A, Rougier A, Tison F, Machado S, Grabot D,Gross C, Bioulac B, Burbaud P: Side-effects of subthalamic stimulation inParkinson’s disease: Clinical evolution and predictive factors. Eur J Neurol13:963–971, 2006.
128. Guiot G, Arfel G, Derome P, Kahn A: Neurophysiologic control proceduresfor sterotaxic thalamotomy [in French]. Neurochirurgie 14:553–566, 1968.
129. Guiot G, Derome P, Trigo JC: Intention tremor: The best indication for stereo-taxic surgery [in French]. Presse Med 75:2513–2518, 1967.
130. Guridi J, Rodriguez-Oroz MC, Lozano AM, Moro E, Albanese A, Nuttin B,Gybels J, Ramos E, Obeso JA: Targeting the basal ganglia for deep brainstimulation in Parkinson’s disease. Neurology 55 [Suppl 6]:S21–S28, 2000.
131. Halbig TD, Gruber D, Kopp UA, Schneider GH, Trottenberg T, Kupsch A:Pallidal stimulation in dystonia: Effects on cognition, mood, and quality oflife. J Neurol Neurosurg Psychiatry 76:1713–1716, 2005.
132. Hamani C, Lozano AM: Hardware-related complications of deep brain stim-ulation: A review of the published literature. Stereotact Funct Neurosurg84:248–251, 2006.
133. Hamani C, Lozano AM: Physiology and pathophysiology of Parkinson’sdisease. Ann N Y Acad Sci 991:15–21, 2003.
134. Hamani C, Richter E, Schwalb JM, Lozano AM: Bilateral subthalamicnucleus stimulation for Parkinson’s disease: A systematic review of the clin-ical literature. Neurosurgery 56:1313–1324, 2005.
135. Hamani C, Saint-Cyr JA, Fraser J, Kaplitt M, Lozano AM: The subthalamicnucleus in the context of movement disorders. Brain 127:4–20, 2004.
136. Hamid NA, Mitchell RD, Mocroft P, Westby GW, Milner J, Pall H: Targetingthe subthalamic nucleus for deep brain stimulation: Technical approach andfusion of pre- and postoperative MR images to define accuracy of lead place-ment. J Neurol Neurosurg Psychiatry 76:409–414, 2005.
137. Hariz M, Fodstad H: Do microelectrode techniques increase accuracy ordecrease risks in pallidotomy and deep brain stimulation? A critical reviewof the literature. Stereotact Funct Neurosurg 72:157–169, 1999.
138. Hariz MI: Complications of deep brain stimulation surgery. Mov Disord 17[Suppl 3]:S162–S166, 2002.
139. Hariz MI, Fodstad H: Do microelectrode techniques increase accuracy ordecrease risks in pallidotomy and deep brain stimulation? A critical reviewof the literature. Stereotact Funct Neurosurg 72:157–169, 1999.
140. Hariz MI, Johansson F: Hardware failure in parkinsonian patients withchronic subthalamic nucleus stimulation is a medical emergency. MovDisord 16:166–168, 2001.
141. Hashimoto T, Elder CM, Okun MS, Patrick SK, Vitek JL: Stimulation of thesubthalamic nucleus changes the firing pattern of pallidal neurons. JNeurosci 23:1916–1923, 2003.
142. Hassler R: Anatomy of the thalamus [in German]. Arch Psychiatr Nervenkr184:249–256, 1950.
143. Hassler R, Riechert T, Mundinger F, Umbach W, Ganglberger JA:Physiological observations in stereotaxic operations in extrapyramidal motordisturbances. Brain 83:337–350, 1960.
144. Heimer G, Rivlin M, Israel Z, Bergman H: Synchronizing activity of basalganglia and pathophysiology of Parkinson’s disease. J Neural TransmSuppl:17–20, 2006.
145. Hertel F, Züchner M, Weimar I, Gemmar P, Noll B, Bettag M, Decker C:Implantation of electrodes for deep brain stimulation of the subthalamicnucleus in advanced Parkinson’s disease with the aid of intraoperativemicrorecording under general anesthesia. Neurosurgery 59:E1138, 2006.
146. Herzog J, Fietzek U, Hamel W, Morsnowski A, Steigerwald F, Schrader B,Weinert D, Pfister G, Müller D, Mehdorn HM, Deuschl G, Volkmann J: Mosteffective stimulation site in subthalamic deep brain stimulation forParkinson’s disease. Mov Disord 19:1050–1054, 2004.
147. Herzog J, Reiff J, Krack P, Witt K, Schrader B, Müller D, Deuschl G: Manicepisode with psychotic symptoms induced by subthalamic nucleus stimula-tion in a patient with Parkinson’s disease. Mov Disord 18:1382–1384, 2003.
148. Herzog J, Volkmann J, Krack P, Kopper F, Pötter M, Lorenz D, Steinbach M,Klebe S, Hamel W, Schrader B, Weinert D, Müller D, Mehdorn HM, DeuschlG: Two-year follow-up of subthalamic deep brain stimulation in Parkinson’sdisease. Mov Disord 18:1332–1337, 2003.
149. Hitchcock E, Flint GA, Gutowski NJ: Thalamotomy for movement disorders:A critical appraisal. Acta Neurochir Suppl (Wien) 39:61–65, 1987.
150. Holloway KL, Gaede SE, Starr PA, Rosenow JM, Ramakrishnan V,Henderson JM: Frameless stereotaxy using bone fiducial markers for deepbrain stimulation. J Neurosurg 103:404–413, 2005.
151. Hooper J, Taylor R, Pentland B, Whittle IR: Rater reliability of Fahn’s tremorrating scale in patients with multiple sclerosis. Arch Phys Med Rehabil79:1076–1079, 1998.
152. Hornykiewicz O, Kish SJ: Biochemical pathophysiology of Parkinson’s dis-ease. Adv Neurol 45:19–34, 1987.
153. Hosobuchi Y: Chronic brain stimulation for the treatment of intractable pain.Res Clin Stud Headache 5:122–126, 1978.
154. Hosobuchi Y: Subcortical electrical stimulation for control of intractable painin humans. Report of 122 cases (1970–1984). J Neurosurg 64:543–553, 1986.
155. Houeto JL, Karachi C, Mallet L, Pillon B, Yelnik J, Mesnage V, Welter ML,Navarro S, Pelissolo A, Damier P, Pidoux B, Dormont D, Cornu P, Agid Y:Tourette’s syndrome and deep brain stimulation. J Neurol NeurosurgPsychiatry 76:992–995, 2005.
156. Houeto JL, Mesnage V, Mallet L, Pillon B, Gargiulo M, du Moncel ST, BonnetAM, Pidoux B, Dormont D, Cornu P, Agid Y: Behavioural disorders,Parkinson’s disease and subthalamic stimulation. J Neurol NeurosurgPsychiatry 72:701–707, 2002 (comment).
157. Houeto JL, Mesnage V, Welter ML, Mallet L, Agid Y, Bejjani BP: SubthalamicDBS replaces levodopa in Parkinson’s disease: Two-year follow-up.Neurology 60:154–155, 2003.
REZAI ET AL.
SHC832 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
158. Hubel D: Tungsten microelectrode from recording from single units. Science125:549–550, 1957.
159. Hung SW, Hamani C, Lozano AM, Poon YY, Piboolnurak P, Miyasaki JM,Lang AE, Dostrovsky JO, Hutchison WD, Moro E: Long-term outcome ofbilateral pallidal deep brain stimulation for primary cervical dystonia.Neurology 68:457–459, 2007.
160. Iansek R, Rosenfeld JV, Huxham FE: Deep brain stimulation of the subthal-amic nucleus in Parkinson’s disease. Med J Aust 177:142–146, 2002.
161. Jeon SW, Shure MA, Baker KB, Huang D, Rollins AM, Chahlavi A, Rezai AR:A feasibility study of optical coherence tomography for guiding deep brainprobes. J Neurosci Methods 154:96–101, 2006.
162. Kahilogullari G, Ugur HC, Savas A, Dirik EB, Akbostanci MC, Elibol B,Kanpolat Y: Management of a hemidystonic patient with thalamotomy, cam-potomy and cervical dorsal root entry zone operation. Stereotact FunctNeurosurg 83:180–183, 2005.
163. Kaplitt MG, Feigin A, Tang C, Fitzsimons HL, Mattis P, Lawlor PA, Bland RJ,Young D, Strybing K, Eidelberg D, During MJ: Safety and tolerability ofgene therapy with an adeno-associated virus (AAV) borne GAD gene forParkinson’s disease: An open label, phase I trial. Lancet 369:2097–2105, 2007.
164. Katayama Y, Kano T, Kobayashi K, Oshima H, Fukaya C, Yamamoto T:Difference in surgical strategies between thalamotomy and thalamic deepbrain stimulation for tremor control. J Neurol 252 [Suppl 4]:IV17-IV22, 2005.
165. Katayama Y, Oshima H, Kano T, Kobayashi K, Fukaya C, Yamamoto T:Direct effect of subthalamic nucleus stimulation on levodopa-induced peak-dose dyskinesia in patients with Parkinson’s disease. Stereotact FunctNeurosurg 84:176–179, 2006.
166. Kelly PJ: Microelectrode recording for the somatotopic placement of stereo-tactic thalamic lesions in the treatment of parkinsonian and cerebellar inten-tion tremor. Appl Neurophysiol 43:262–266, 1980.
167. Kelly PJ, Ahlskog JE, Goerss SJ, Daube JR, Duffy JR, Kall BA: Computer-assisted stereotactic ventralis lateralis thalamotomy with microelectroderecording control in patients with Parkinson’s disease. Mayo Clin Proc62:655–664, 1987.
168. Kenney C, Simpson R, Hunter C, Ondo W, Almaguer M, Davidson A,Jankovic J: Short-term and long-term safety of deep brain stimulation in thetreatment of movement disorders. J Neurosurg 106:621–625, 2007.
169. Kitagawa M, Murata J, Kikuchi S, Sawamura Y, Saito H, Sasaki H, Tashiro K:Deep brain stimulation of subthalamic area for severe proximal tremor.Neurology 55:114–116, 2000.
170. Kleiner-Fisman G, Fisman DN, Sime E, Saint-Cyr JA, Lozano AM, Lang AE:Long-term follow up of bilateral deep brain stimulation of the subthalamicnucleus in patients with advanced Parkinson disease. J Neurosurg99:489–495, 2003.
171. Kleiner-Fisman G, Herzog J, Fisman DN, Tamma F, Lyons KE, Pahwa R,Lang AE, Deuschl G: Subthalamic nucleus deep brain stimulation: Summaryand meta-analysis of outcomes. Mov Disord 21 [Suppl 14]:S290–S304, 2006.
172. Koller WC, Lyons KE, Wilkinson SB, Pahwa R: Efficacy of unilateral deepbrain stimulation of the VIM nucleus of the thalamus for essential headtremor. Mov Disord 14:847–850, 1999.
173. Koller WC, Lyons KE, Wilkinson SB, Troster AI, Pahwa R: Long-term safetyand efficacy of unilateral deep brain stimulation of the thalamus in essentialtremor. Mov Disord 16:464–468, 2001.
174. Koller WC, Pahwa PR, Lyons KE, Wilkinson SB: Deep brain stimulation ofthe Vim nucleus of the thalamus for the treatment of tremor. Neurology 55[Suppl 6]:S29–S33, 2000.
175. Kondziolka D, Whiting D, Germanwala A, Oh M: Hardware-related compli-cations after placement of thalamic deep brain stimulator systems. StereotactFunct Neurosurg 79:228–233, 2002.
176. Kordower JH: In vivo gene delivery of glial cell line-derived neurotrophicfactor for Parkinson’s disease. Ann Neurol 53 [Suppl 3]:S120–S134, 2003.
177. Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, KoudsieA, Limousin PD, Benazzouz A, LeBas JF, Benabid AL, Pollak P: Five-year fol-low-up of bilateral stimulation of the subthalamic nucleus in advancedParkinson’s disease. N Engl J Med 349:1925–1934, 2003.
178. Krack P, Dostrovsky J, Ilinsky I, Kultas-Ilinsky K, Lenz F, Lozano AM, VitekJ: Surgery of the motor thalamus: Problems with the present nomenclatures.Mov Disord 17 [Suppl 3]:S2–S8, 2002.
179. Krack P, Fraix V, Mendes A, Benabid AL, Pollak P: Postoperative manage-ment of subthalamic nucleus stimulation for Parkinson’s disease. MovDisord 17 [Suppl 3 ]:S188–S197, 2002.
180. Krack P, Limousin P, Benabid AL, Pollak P: Chronic stimulation of subthal-amic nucleus improves levodopa-induced dyskinesias in Parkinson’s dis-ease. Lancet 350:1676, 1997.
181. Krack P, Pollak P, Limousin P, Hoffmann D, Xie J, Benazzouz A, Benabid AL:Subthalamic nucleus or internal pallidal stimulation in young onsetParkinson’s disease. Brain 121:451–457, 1998.
182. Kraft SP, Lang AE: Cranial dystonia, blepharospasm and hemifacial spasm:Clinical features and treatment, including the use of botulinum toxin. CMAJ139:837–844, 1988.
183. Krause M, Fogel W, Heck A, Hacke W, Bonsanto M, Trenkwalder C, TronnierV: Deep brain stimulation for the treatment of Parkinson’s disease:Subthalamic nucleus versus globus pallidus internus. J Neurol NeurosurgPsychiatry 70:464–470, 2001.
184. Krause M, Fogel W, Kloss M, Rasche D, Volkmann J, Tronnier V: Pallidalstimulation for dystonia. Neurosurgery 55:1361–1370, 2004.
185. Krause M, Fogel W, Tronnier V, Pohle S, Hörtnagel K, Thyen U, VolkmannJ: Long-term benefit to pallidal deep brain stimulation in a case of dystoniasecondary to pantothenate kinase-associated neurodegeneration. MovDisord 21:2255–2257, 2006.
186. Krauss JK, Simpson RK Jr, Ondo WG, Pohle T, Burgunder JM, Jankovic J:Concepts and methods in chronic thalamic stimulation for treatment oftremor: Technique and application. Neurosurgery 48:535–543, 2001.
187. Krauss JK, Yianni J, Loher TJ, Aziz TZ: Deep brain stimulation for dystonia.J Clin Neurophysiol 21:18–30, 2004.
188. Kringelbach ML, Jenkinson N, Green AL, Owen SL, Hansen PC, CornelissenPL, Holliday IE, Stein J, Aziz TZ: Deep brain stimulation for chronic paininvestigated with magnetoencephalography. Neuroreport 18:223–228, 2007.
189. Kühn AA, Kupsch A, Schneider GH, Brown P: Reduction in subthalamic8–35 Hz oscillatory activity correlates with clinical improvement inParkinson’s disease. Eur J Neurosci 23:1956–1960, 2006.
190. Deleted in proof.191. Kumar K, Kelly M, Toth C: Deep brain stimulation of the ventral intermedi-
ate nucleus of the thalamus for control of tremors in Parkinson’s disease andessential tremor. Stereotact Funct Neurosurg 72:47–61, 1999.
192. Kumar K, Wyant GM: Deep brain stimulation for alleviating chronicintractable pain. Can J Surg 28:20–22, 1985.
193. Kumar R, Lozano AM, Sime E, Lang AE: Long-term follow-up of thalamicdeep brain stimulation for essential and parkinsonian tremor. Neurology61:1601–1604, 2003.
194. Kupsch A, Benecke R, Müller J, Trottenberg T, Schneider GH, Poewe W,Eisner W, Wolters A, Müller JU, Deuschl G, Pinsker MO, Skogseid IM,Roeste GK, Vollmer-Haase J, Brentrup A, Krause M, Tronnier V, Schnitzler A,Voges J, Nikkhah G, Vesper J, Naumann M, Volkmann J; Deep BrainStimulation for Dystonia Study Group: Pallidal deep-brain stimulation inprimary generalized or segmental dystonia. N Engl J Med 355:1978–1990,2006.
195. Kupsch A, Klaffke S, Kühn AA, Meissner W, Arnold G, Schneider GH,Maier-Hauff K, Trottenberg T: The effects of frequency in pallidal deep brainstimulation for primary dystonia. J Neurol 250:1201–1205, 2003.
196. Laitinen LV, Bergenheim AT, Hariz MI: Leksell’s posteroventral pallidotomyin the treatment of Parkinson’s disease. J Neurosurg 76:53–61, 1992.
197. Laitinen LV, Bergenheim AT, Hariz MI: Ventroposterolateral pallidotomycan abolish all parkinsonian symptoms. Stereotact Funct Neurosurg58:14–21, 1992.
198. Lambert D, Waters CH: Essential Tremor. Curr Treat Options Neurol1:6–13, 1999.
199. Lang AE, Gill S, Patel NK, Lozano AM, Nutt JG, Penn R, Brooks DJ, HottonG, Moro E, Heywood P, Brodsky MA, Burchiel K, Kelly P, Dalvi A, Scott B,Stacy M, Turner D, Wooten VG, Elias WJ, Laws ER, Dhawan V, Stoessl AJ,Matcham J, Coffey RJ, Traub M: Randomized controlled trial of intraputame-nal glial cell line-derived neurotrophic factor infusion in Parkinson disease.Ann Neurol 59:459–466, 2006.
200. Lang AE, Kleiner-Fisman G, Saint-Cyr JA, Miyasaki J, Lozano A:Subthalamic DBS replaces levodopa in Parkinson’s disease: Two-year follow-up. Neurology 60:154–155, 2003.
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC833
201. Lee JY, Deogaonkar M, Rezai A: Deep brain stimulation of globus pallidusinternus for dystonia. Parkinsonism Relat Disord 13:261–265, 2006.
202. Lee JY, Kondziolka D: Thalamic deep brain stimulation for management ofessential tremor. J Neurosurg 103:400–403, 2005.
203. Lee KH, Chang SY, Roberts DW, Kim U: Neurotransmitter release fromhigh-frequency stimulation of the subthalamic nucleus. J Neurosurg101:511–517, 2004.
204. Lee M, Epstein FJ, Rezai AR, Zagzag D: Nonneoplastic intramedullary spinalcord lesions mimicking tumors. Neurosurgery 43:788–795, 1998.
205. Lee RG: Physiology of the basal ganglia and pathophysiology of Parkinson’sdisease. Can J Neurol Sci 14 [Suppl 3]:373–380, 1987.
206. Leksell L: A stereotactic apparatus for intracerebral surgery. Acta Chir Scand99:229–233, 1949.
207. Lenz FA, Dostrovsky JO, Kwan HC, Tasker RR, Yamashiro K, Murphy JT:Methods for microstimulation and recording of single neurons and evokedpotentials in the human central nervous system. J Neurosurg 68:630–634, 1988.
208. Lévesque MF, Taylor S, Rogers R, Le MT, Swope D: Subthalamic stimulationin Parkinson’s disease. Preliminary results. Stereotact Funct Neurosurg72:170–173, 1999.
209. Levy R, Ashby P, Hutchison WD, Lang AE, Lozano AM, Dostrovsky JO:Dependence of subthalamic nucleus oscillations on movement anddopamine in Parkinson’s disease. Brain 125:1196–1209, 2002.
210. Levy RM: Deep brain stimulation for the treatment of intractable pain.Neurosurg Clin N Am 14:389–399, 2003.
211. Levy RM, Lamb S, Adams JE: Treatment of chronic pain by deep brain stim-ulation: Long term follow-up and review of the literature. Neurosurgery21:885–893, 1987.
212. Liang GS, Chou KL, Baltuch GH, Jaggi JL, Loveland-Jones C, Leng L,Maccarone H, Hurtig HI, Colcher A, Stern MB, Kleiner-Fisman G, Simuni T,Siderowf AD: Long-term outcomes of bilateral subthalamic nucleus stimu-lation in patients with advanced Parkinson’s disease. Stereotact FunctNeurosurg 84:221–227, 2006.
213. Limousin-Dowsey P: Thalamic stimulation in essential tremor. LancetNeurol 3:80, 2004.
214. Limousin P, Krack P, Pollak P, Benazzouz A, Ardouin C, Hoffmann D,Benabid AL: Electrical stimulation of the subthalamic nucleus in advancedParkinson’s disease. N Engl J Med 339:1105–1111, 1998.
215. Limousin P, Pollak P, Benazzouz A, Hoffmann D, Broussolle E, Perret JE,Benabid AL: Bilateral subthalamic nucleus stimulation for severeParkinson’s disease. Mov Disord 10:672–674, 1995.
216. Limousin P, Pollak P, Benazzouz A, Hoffmann D, Le Bas JF, Broussolle E,Perret JE, Benabid AL: Effect of parkinsonian signs and symptoms of bilat-eral subthalamic nucleus stimulation. Lancet 345:91–95, 1995.
217. Limousin P, Pollak P, Hoffmann D, Benazzouz A, Perret JE, Benabid AL:Abnormal involuntary movements induced by subthalamic nucleus stimu-lation in parkinsonian patients. Mov Disord 11:231–235, 1996.
218. Lin JJ, Lin SZ, Lin GY, Chang DC, Lee CC: Treatment of intractable general-ized dystonia by bilateral posteroventral pallidotomy—one-year results.Zhonghua Yi Xue Za Zhi (Taipei) 64:231–238, 2001.
219. Lipp A, Tank J, Trottenberg T, Kupsch A, Arnold G, Jordan J: Sympatheticactivation due to deep brain stimulation in the region of the STN. Neurology65:774–775, 2005.
220. Liu X, Rowe J, Nandi D, Hayward G, Parkin S, Stein J, Aziz T: Localisationof the subthalamic nucleus using Radionics Image Fusion and Stereoplancombined with field potential recording. A technical note. Stereotact FunctNeurosurg 76:63–73, 2001.
221. Loher TJ, Gutbrod K, Fravi NL, Pohle T, Burgunder JM, Krauss JK: Thalamicstimulation for tremor. Subtle changes in episodic memory are related tostimulation per se and not to a microthalamotomy effect. J Neurol 250:707–713, 2003.
222. Lozano AM: Vim thalamic stimulation for tremor. Arch Med Res31:266–269, 2000.
223. Lozano AM, Carella F: Physiologic studies in the human brain in move-ment disorders. Parkinsonism Relat Disord 8:455–458, 2002.
224. Lozano AM, Kumar R, Gross RE, Giladi N, Hutchison WD, Dostrovsky JO,Lang AE: Globus pallidus internus pallidotomy for generalized dystonia.Mov Disord 12:865–870, 1997.
225. Lyons KE, Davis JT, Pahwa R: Subthalamic nucleus stimulation inParkinson’s disease patients intolerant to levodopa. Stereotact FunctNeurosurg 85:169–174, 2007.
226. Lyons KE, Pahwa R: Deep brain stimulation and essential tremor. J ClinNeurophysiol 21:2–5, 2004.
227. Lyons KE, Pahwa R: Deep brain stimulation in Parkinson’s disease. CurrNeurol Neurosci Rep 4:290–295, 2004.
228. Lyons KE, Pahwa R: Long-term benefits in quality of life provided by bilat-eral subthalamic stimulation in patients with Parkinson disease. J Neurosurg103:252–255, 2005.
229. Lyons KE, Wilkinson SB, Overman J, Pahwa R: Surgical and hardware com-plications of subthalamic stimulation: A series of 160 procedures. Neurology63:612–616, 2004.
230. Macchi G, Jones EG: Toward an agreement on terminology of nuclear andsubnuclear divisions of the motor thalamus. J Neurosurg 86:670–685, 1997.
231. Machado A, Rezai AR, Kopell BH, Gross RE, Sharan AD, Benabid AL: Deepbrain stimulation for Parkinson’s disease: Surgical technique and perioper-ative management. Mov Disord 21 [Suppl 14]:S247–S258, 2006.
232. Machado AG, Hiremath GK, Salazar F, Rezai AR: Fracture of subthalamicnucleus deep brain stimulation hardware as a result of compulsive manip-ulation: Case report. Neurosurgery 57:E1318, 2005.
233. Maciunas RJ, Galloway RL Jr, Latimer JW: The application accuracy ofstereotactic frames. Neurosurgery 35:682–695, 1994.
234. Marceglia S, Foffani G, Bianchi AM, Baselli G, Tamma F, Egidi M, Priori A:Dopamine-dependent non-linear correlation between subthalamic rhythmsin Parkinson’s disease. J Physiol 571:579–591, 2006.
235. Martin AJ, Larson PS, Ostrem JL, Keith Sootsman W, Talke P, Weber OM,Levesque N, Myers J, Starr PA: Placement of deep brain stimulator elec-trodes using real-time high-field interventional magnetic resonance imaging.Magn Reson Med 54:1107–1114, 2005.
236. Martínez-Martín P, Valldeoriola F, Tolosa E, Pilleri M, Molinuevo JL, RumiàJ, Ferrer E: Bilateral subthalamic nucleus stimulation and quality of life inadvanced Parkinson’s disease. Mov Disord 17:372–377, 2002.
237. Matsumoto K, Asano T, Baba T, Miyamoto T, Ohmoto T: Long-term follow-up results of bilateral thalamotomy for parkinsonism. Appl Neurophysiol39:257–260, 1976.
238. Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C,Schwalb JM, Kennedy SH: Deep brain stimulation for treatment-resistantdepression. Neuron 45:651–660, 2005.
239. McLeod JG: Pathophysiology of Parkinson’s disease. Aust N Z J Med 1[Suppl 1]:19–23, 1971.
240. Merello M, Cammarota A, Leiguarda R, Pikielny R: Delayed intracerebralelectrode infection after bilateral STN implantation for Parkinson’s disease.Case report. Mov Disord 16:168–170, 2001.
241. Meyer JS, Magee KR: Current views concerning the etiology, pathophysiol-ogy, and treatment of Parkinson’s disease. J Neuropsychiatr 5:284–290, 1964.
242. Millet B, Jaafari N: Treatment of obsessive-compulsive disorder [in French].Rev Prat 57:53–57, 2007.
243. Mink JW, Walkup J, Frey KA, Como P, Cath D, Delong MR, Erenberg G,Jankovic J, Juncos J, Leckman JF, Swerdlow N, Visser-Vandewalle V, Vitek JL;Tourette Syndrome Association, Inc.: Patient selection and assessment rec-ommendations for deep brain stimulation in Tourette syndrome. MovDisord 21:1831–1838, 2006.
244. Miyawaki E, Perlmutter JS, Tröster AI, Videen TO, Koller WC: The behav-ioral complications of pallidal stimulation: A case report. Brain Cogn42:417–434, 2000.
245. Molinuevo JL, Valldeoriola F, Tolosa E, Rumia J, Valls-Sole J, Roldan H,Ferrer E: Levodopa withdrawal after bilateral subthalamic nucleus stimula-tion in advanced Parkinson disease. Arch Neurol 57:983–988, 2000.
246. Molnar GF, Pilliar A, Lozano AM, Dostrovsky JO: Differences in neuronal fir-ing rates in pallidal and cerebellar receiving areas of thalamus in patientswith Parkinson’s disease, essential tremor, and pain. J Neurophysiol93:3094–3101, 2005.
247. Molnar GF, Sailer A, Gunraj CA, Lang AE, Lozano AM, Chen R: Thalamicdeep brain stimulation activates the cerebellothalamocortical pathway.Neurology 63:907–909, 2004.
248. Moore DJ, West AB, Dawson VL, Dawson TM: Molecular pathophysiologyof Parkinson’s disease. Annu Rev Neurosci 28:57–87, 2005.
REZAI ET AL.
SHC834 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com

249. Moore RY: Organization of midbrain dopamine systems and the pathophys-iology of Parkinson’s disease. Parkinsonism Relat Disord 9 [Suppl2]:S65–S71, 2003.
250. Morrison CE, Borod JC, Perrine K, Beric A, Brin MF, Rezai A, Kelly P, SterioD, Germano I, Weisz D, Olanow CW: Neuropsychological functioning fol-lowing bilateral subthalamic nucleus stimulation in Parkinson’s disease.Arch Clin Neuropsychol 19:165–181, 2004.
251. Mouradian MM, Heuser IJ, Baronti F, Fabbrini G, Juncos JL, Chase TN:Pathogenesis of dyskinesias in Parkinson’s disease. Ann Neurol25:523–526, 1989.
252. Murata J, Kitagawa M, Uesugi H, Saito H, Iwasaki Y, Kikuchi S, Tashiro K,Sawamura Y: Electrical stimulation of the posterior subthalamic area for thetreatment of intractable proximal tremor. J Neurosurg 99:708–715, 2003.
253. Narabayashi H: Neurophysiological ideas on pallidotomy and ventrolateralthalamotomy for hyperkinesis. Confin Neurol 22:291–303, 1962.
254. Narabayashi H, Maeda T, Yokochi F: Long-term follow-up study of nucleusventralis intermedius and ventrolateralis thalamotomy using a microelec-trode technique in parkinsonism. Appl Neurophysiol 50:330–337, 1987.
255. Narabayashi H, Ohye C: Nucleus ventralis intermedius of human thala-mus. Trans Am Neurol Assoc 99:232–233, 1974.
256. Narabayashi H, Shimazu H, Fujita Y, Shikiba S, Nagao T, Nagahata M:Procaine-oil-wax pallidotomy for double athetosis and spastic states ininfantile cerebral palsy: Report of 80 cases. Neurology 10:61–69, 1960.
257. Niemann K, Naujokat C, Pohl G, Wollner C, von Keyserlingk D: Verificationof the Schaltenbrand and Wahren stereotactic atlas. Acta Neurochir (Wien)129:72–81, 1994.
258. Nilsson MH, Törnqvist AL, Rehncrona S: Deep-brain stimulation in the sub-thalamic nuclei improves balance performance in patients with Parkinson’sdisease, when tested without anti-parkinsonian medication. Acta NeurolScand 111:301–308, 2005.
259. Novak KE, Nenonene EK, Bernstein LP, Vergenz S, Medalle G, Prager JM,Eller TW, Cozzens JW, Rezak M: Two cases of ischemia associated with sub-thalamic nucleus stimulator implantation for advanced Parkinson’s disease.Mov Disord 21:1477–1483, 2006.
260. Obeso JA, Grandas F, Vaamonde J, Luquin MR, Artieda J, Lera G, RodriguezME, Martinez-Lage JM: Motor complications associated with chronic lev-odopa therapy in Parkinson’s disease. Neurology 39 [Suppl 2]:11–19, 1989.
261. Obeso JA, Rodriguez-Oroz MC, Rodriguez M, DeLong MR, Olanow CW:Pathophysiology of levodopa-induced dyskinesias in Parkinson’s disease:Problems with the current model. Ann Neurol 47 [Suppl 1]:S22–S34, 2000.
262. Obeso JA, Rodríguez-Oroz MC, Rodríguez M, Lanciego JL, Artieda J,Gonzalo N, Olanow CW: Pathophysiology of the basal ganglia in Parkin-son’s disease. Trends Neurosci 23 [Suppl 10]:S8–S19, 2000.
263. Obeso JA, Rodriguez-Oroz MC, Rodriguez M, Macias R, Alvarez L, GuridiJ, Vitek J, DeLong MR: Pathophysiologic basis of surgery for Parkinson’s dis-ease. Neurology 55 [Suppl 6]:S7–S12, 2000.
264. Obeso JA, Rodríguez MC, Gorospe A, Guridi J, Alvarez L, Macias R: Surgicaltreatment of Parkinson’s disease. Baillieres Clin Neurol 6:125–145, 1997.
265. Oh MY, Abosch A, Kim SH, Lang AE, Lozano AM: Long-term hardware-related complications of deep brain stimulation. Neurosurgery 50:1268–1276, 2002.
266. Okun MS, Rodriguez RL, Mikos A, Miller K, Kellison I, Kirsch-Darrow L,Wint DP, Springer U, Fernandez HH, Foote KD, Crucian G, Bowers D: Deepbrain stimulation and the role of the neuropsychologist. Clin Neuropsychol21:162–189, 2007.
267. Ondo W, Dat Vuong K, Almaguer M, Jankovic J, Simpson RK: Thalamicdeep brain stimulation: Effects on the nontarget limbs. Mov Disord16:1137–1142, 2001.
268. Ondo WG: Essential tremor: Treatment options. Curr Treat Options Neurol8:256–267, 2006.
269. Ondo WG, Bronte-Stewart H: The North American survey of placement andadjustment strategies for deep brain stimulation. Stereotact FunctNeurosurg 83:142–147, 2005.
270. Ondo WG, Desaloms JM, Jankovic J, Grossman RG: Pallidotomy for gener-alized dystonia. Mov Disord 13:693–698, 1998.
271. Østergaard K, Aa Sunde N: Evolution of Parkinson’s disease during 4 yearsof bilateral deep brain stimulation of the subthalamic nucleus. Mov Disord21:624–631, 2006.
272. Østergaard K, Sunde N, Dupont E: Effects of bilateral stimulation of the sub-thalamic nucleus in patients with severe Parkinson’s disease and motor fluc-tuations. Mov Disord 17:693–700, 2002.
273. Pahapill PA, Lozano AM: The pedunculopontine nucleus and Parkinson’sdisease. Brain 123:1767–1783, 2000.
274. Pahwa R, Lyons KE, Wilkinson SB, Simpson RK Jr, Ondo WG, Tarsy D,Norregaard T, Hubble JP, Smith DA, Hauser RA, Jankovic J: Long-termevaluation of deep brain stimulation of the thalamus. J Neurosurg104:506–512, 2006.
275. Pahwa R, Lyons KE, Wilkinson SB, Tröster AI, Overman J, Kieltyka J, KollerWC: Comparison of thalamotomy to deep brain stimulation of the thalamusin essential tremor. Mov Disord 16:140–143, 2001.
276. Pahwa R, Wilkinson SB, Overman J, Lyons KE: Preoperative clinical predic-tors of response to bilateral subthalamic stimulation in patients withParkinson’s disease. Stereotact Funct Neurosurg 83:80–83, 2005.
277. Pahwa R, Wilkinson S, Smith D, Lyons K, Miyawaki E, Koller WC: High-fre-quency stimulation of the globus pallidus for the treatment of Parkinson’sdisease. Neurology 49:249–253, 1997.
278. Paluzzi A, Bain PG, Liu X, Yianni J, Kumarendran K, Aziz TZ: Pregnancy indystonic women with in situ deep brain stimulators. Mov Disord21:695–698, 2006.
279. Paluzzi A, Belli A, Bain P, Liu X, Aziz TM: Operative and hardware compli-cations of deep brain stimulation for movement disorders. Br J Neurosurg20:290–295, 2006.
280. Parr JR, Green AL, Joint C, Andrew M, Gregory RP, Scott RB, McShane MA,Aziz TZ: Deep brain stimulation in childhood: An effective treatment forearly onset generalised idiopathic dystonia. Arch Dis Child 92:708-711, 2007.
281. Parsons TD, Rogers SA, Braaten AJ, Woods SP, Tröster AI: Cognitive seque-lae of subthalamic nucleus deep brain stimulation in Parkinson’s disease: Ameta-analysis. Lancet Neurol 5:578–588, 2006.
282. Peppe A, Pierantozzi M, Bassi A, Altibrandi MG, Brusa L, Stefani A,Stanzione P, Mazzone P: Stimulation of the subthalamic nucleus comparedwith the globus pallidus internus in patients with Parkinson disease. J Neurosurg 101:195–200, 2004.
283. Perlmutter JS: New insights into the pathophysiology of Parkinson’s disease:The challenge of positron emission tomography. Trends Neurosci11:203–208, 1988.
284. Pilitsis JG, Rezai AR, Boulis NM, Henderson JM, Busch RM, Kubu CS: Apreliminary study of transient confusional states following bilateral sub-thalamic stimulation for Parkinson’s disease. Stereotact Funct Neurosurg83:67–70, 2005.
285. Pillon B, Ardouin C, Damier P, Krack P, Houeto JL, Klinger H, Bonnet AM,Pollak P, Benabid AL, Agid Y: Neuropsychological changes between “off”and “on” STN or GPi stimulation in Parkinson’s disease. Neurology55:411–418, 2000.
286. Pillon B, Ardouin C, Dujardin K, Vittini P, Pelissolo A, Cottencin O, VercueilL, Houeto JL, Krystkowiak P, Agid Y, Destée A, Pollak P, Vidailhet M:Preservation of cognitive function in dystonia treated by pallidal stimula-tion. Neurology 66:1556–1558, 2006.
287. Pogosyan A, Kühn AA, Trottenberg T, Schneider GH, Kupsch A, Brown P:Elevations in local gamma activity are accompanied by changes in the firingrate and information coding capacity of neurons in the region of the subthal-amic nucleus in Parkinson’s disease. Exp Neurol 202:271–279, 2006.
288. Pollak P, Benabid AL, Gervason CL, Hoffmann D, Seigneuret E, Perret J:Long-term effects of chronic stimulation of the ventral intermediate thalamicnucleus in different types of tremor. Adv Neurol 60:408–413, 1993.
289. Pollak P, Benabid AL, Gross C, Gao DM, Laurent A, Benazzouz A, HoffmannD, Gentil M, Perret J: Effects of the stimulation of the subthalamic nucleus inParkinson disease [in French]. Rev Neurol (Paris) 149:175–176, 1993.
290. Pollak P, Krack P, Fraix V, Mendes A, Moro E, Chabardes S, Benabid AL:Intraoperative micro- and macrostimulation of the subthalamic nucleus inParkinson’s disease. Mov Disord 17 [Suppl 3]:S155–S161, 2002.
291. Pool JL, Ransohoff J: Autonomic effects on stimulating rostral portion ofcingulate gyri in man. J Neurophysiol 12:385–392, 1949.
292. Priori A, Foffani G, Pesenti A, Tamma F, Bianchi AM, Pellegrini M, LocatelliM, Moxon KA, Villani RM: Rhythm-specific pharmacological modulation ofsubthalamic activity in Parkinson’s disease. Exp Neurol 189:369–379, 2004.
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC835
293. Putzke JD, Uitti RJ, Obwegeser AA, Wszolek ZK, Wharen RE: Bilateral thal-amic deep brain stimulation: Midline tremor control. J Neurol NeurosurgPsychiatry 76:684–690, 2005.
294. Putzke JD, Wharen RE Jr, Obwegeser AA, Wszolek ZK, Lucas JA, Turk MF,Uitti RJ: Thalamic deep brain stimulation for essential tremor: Recommen-dations for long-term outcome analysis. Can J Neurol Sci 31:333–342, 2004.
295. Rasche D, Rinaldi PC, Young RF, Tronnier VM: Deep brain stimulation for thetreatment of various chronic pain syndromes. Neurosurg Focus 21:E8, 2006.
296. Rezai AR, Kopell BH, Gross RE, Vitek JL, Sharan AD, Limousin P, BenabidAL: Deep brain stimulation for Parkinson’s disease: Surgical issues. MovDisord 21 [Suppl 14]:S197–S218, 2006.
297. Rezai AR, Lozano AM, Crawley AP, Joy ML, Davis KD, Kwan CL,Dostrovsky JO, Tasker RR, Mikulis DJ: Thalamic stimulation and func-tional magnetic resonance imaging: Localization of cortical and subcorti-cal activation with implanted electrodes. Technical note. J Neurosurg90:583–590, 1999.
298. Richardson DE: Brain stimulation for pain control. IEEE Trans Biomed Eng23:304–306, 1976.
299. Richardson DE: Thalamic stimulation in the control of pain. South Med J 73:283–285, 1980.
300. Richardson DE, Akil H: Pain reduction by electrical brain stimulation inman. Part 1: Acute administration in periaqueductal and periventricularsites. J Neurosurg 47:178–183, 1977.
301. Richter EO, Hoque T, Halliday W, Lozano AM, Saint-Cyr JA: Determiningthe position and size of the subthalamic nucleus based on magnetic reso-nance imaging results in patients with advanced Parkinson disease. J Neurosurg 100:541–546, 2004.
302. Rodriguez-Oroz MC, Gorospe A, Guridi J, Ramos E, Linazasoro G,Rodriguez-Palmero M, Obeso JA: Bilateral deep brain stimulation of thesubthalamic nucleus in Parkinson’s disease. Neurology 55 [Suppl6]:S45–S51, 2000.
303. Rodriguez-Oroz MC, Obeso JA, Lang AE, Houeto JL, Pollak P, Rehncrona S,Kulisevsky J, Albanese A, Volkmann J, Hariz MI, Quinn NP, Speelman JD,Guridi J, Zamarbide I, Gironell A, Molet J, Pascual-Sedano B, Pidoux B,Bonnet AM, Agid Y, Xie J, Benabid AL, Lozano AM, Saint-Cyr J, Romito L,Contarino MF, Scerrati M, Fraix V, Van Blercom N: Bilateral deep brain stim-ulation in Parkinson’s disease: A multicentre study with 4 years follow-up.Brain 128:2240–2249, 2005.
304. Rodriguez-Oroz MC, Zamarbide I, Guridi J, Palmero MR, Obeso JA: Efficacyof deep brain stimulation of the subthalamic nucleus in Parkinson’s disease4 years after surgery: Double blind and open label evaluation. J NeurolNeurosurg Psychiatry 75:1382–1385, 2004.
305. Roitberg B, Urbaniak K, Emborg M: Cell transplantation for Parkinson’sdisease. Neurol Res 26:355–362, 2004.
306. Romito LM, Raja M, Daniele A, Contarino MF, Bentivoglio AR, Barbier A,Scerrati M, Albanese A: Transient mania with hypersexuality after surgeryfor high frequency stimulation of the subthalamic nucleus in Parkinson’sdisease. Mov Disord 17:1371–1374, 2002.
307. Romito LM, Scerrati M, Contarino MF, Iacoangeli M, Bentivoglio AR,Albanese A: Bilateral high frequency subthalamic stimulation inParkinson’s disease: Long-term neurological follow-up. J Neurosurg Sci47:119–128, 2003.
308. Saint-Cyr JA, Hoque T, Pereira LC, Dostrovsky JO, Hutchison WD, MikulisDJ, Abosch A, Sime E, Lang AE, Lozano AM: Localization of clinically effec-tive stimulating electrodes in the human subthalamic nucleus on magneticresonance imaging. J Neurosurg 97:1152–1166, 2002.
309. Santens P, Boon P, Van Roost D, Caemaert J: The pathophysiology of motorsymptoms in Parkinson’s disease. Acta Neurol Belg 103:129–134, 2003.
310. Sartorius A, Henn FA: Deep brain stimulation of the lateral habenula intreatment resistant major depression. Med Hypotheses 69:1305–1308, 2007.
311. Schad LR, Boesecke R, Schlegel W, Hartmann GH, Sturm V, Strauss LG,Lorenz WJ: Three dimensional image correlation of CT, MR, and PET stud-ies in radiotherapy treatment planning of brain tumors. J Comput AssistTomogr 11:948–954, 1987.
312. Schadt CR, Charles PD, Davis TL, Konrad PE: Thalamotomy, DBS-Vim, andDBS-GPi for generalized dystonia: A case report. Tenn Med 100:38–39, 2007.
313. Schaltenbrand G, Wahren W: Atlas for Stereotaxy of the Human Brain. Stuttgart,Thieme Medical Publishers, 1977, pp 41–47.
314. Schlaepfer TE, Cohen MX, Frick C, Kosel M, Brodesser D, Axmacher N, JoeAY, Kreft M, Lenartz D, Sturm V: Deep brain stimulation to reward circuitryalleviates anhedonia in refractory major depression. Neuropsycho-pharmacology, 2007.
315. Schüpbach WM, Chastan N, Welter ML, Houeto JL, Mesnage V, Bonnet AM,Czernecki V, Maltête D, Hartmann A, Mallet L, Pidoux B, Dormont D,Navarro S, Cornu P, Mallet A, Agid Y: Stimulation of the subthalamicnucleus in Parkinson’s disease: A 5 year follow up. J Neurol NeurosurgPsychiatry 76:1640–1644, 2005.
316. Schuurman PR, Bosch DA, Bossuyt PM, Bonsel GJ, van Someren EJ, de BieRM, Merkus MP, Speelman JD: A comparison of continuous thalamic stim-ulation and thalamotomy for suppression of severe tremor. N Engl J Med342:461–468, 2000.
317. Sherer TB, Fiske BK, Svendsen CN, Lang AE, Langston JW: Crossroads inGDNF therapy for Parkinson’s disease. Mov Disord 21:136–141, 2006.
318. Siderowf A, Jaggi JL, Xie SX, Loveland-Jones C, Leng L, Hurtig H, Colcher A,Stern M, Chou KL, Liang G, Maccarone H, Simuni T, Baltuch G: Long-termeffects of bilateral subthalamic nucleus stimulation on health-related quality oflife in advanced Parkinson’s disease. Mov Disord 21:746–753, 2006.
319. Siegfried J, Shulman J: Deep brain stimulation. Pacing Clin Electrophysiol10:271–272, 1987.
320. Silberstein P, Pogosyan A, Kühn AA, Hotton G, Tisch S, Kupsch A, Dowsey-Limousin P, Hariz MI, Brown P: Cortico-cortical coupling in Parkinson’sdisease and its modulation by therapy. Brain 128:1277–1291, 2005.
321. Sixel-Döring F, Trenkwalder C, Kappus C, Hellwig D: Abscess at the implantsite following apical parodontitis. Hardware-related complications of deepbrain stimulation [in German]. Nervenarzt 77:946–947, 2006.
322. Skidmore FM, Rodriguez RL, Fernandez HH, Goodman WK, Foote KD,Okun MS: Lessons learned in deep brain stimulation for movement andneuropsychiatric disorders. CNS Spectr 11:521–536, 2006.
323. Slavin KV, Thulborn KR, Wess C, Nersesyan H: Direct visualization of thehuman subthalamic nucleus with 3T MR imaging. AJNR Am J Neuroradiol27:80–84, 2006.
324. Slevin JT, Gash DM, Smith CD, Gerhardt GA, Kryscio R, Chebrolu H, WaltonA, Wagner R, Young AB: Unilateral intraputaminal glial cell line-derivedneurotrophic factor in patients with Parkinson disease: Response to 1 yeareach of treatment and withdrawal. Neurosurg Focus 20:E1, 2006.
325. Snyder SH, D’Amato RJ: MPTP: A neurotoxin relevant to the pathophysiol-ogy of Parkinson’s disease. The 1985 George C. Cotzias lecture. Neurology36:250–258, 1986.
326. Spiegel EA, Wycis HT: Effect of thalamic and pallidal lesions upon invol-untary movements in choreoathetosis. Trans Am Neurol Assoc51:234–237, 1950.
327. Spiegel EA, Wycis HT, Baird HW 3rd: Pallidotomy and pallido-amygdalo-tomy in certain types of convulsive disorders. Trans Am Neurol Assoc82:51–54, 1957.
328. Spiegel EA, Wycis HT, Marks M, Lee AJ: Stereotaxic apparatus for operationson the human brain. Science 106:349–350, 1947.
329. Stacy MA, Elble RJ, Ondo WG, Wu SC, Hulihan J: Assessment of interraterand intrarater reliability of the Fahn-Tolosa-Marin Tremor Rating Scale inessential tremor. Mov Disord 22:833–838, 2007.
330. Starr PA: Placement of deep brain stimulators into the subthalamic nucleusor Globus pallidus internus: Technical approach. Stereotact FunctNeurosurg 79:118–145, 2002.
331. Starr PA, Turner RS, Rau G, Lindsey N, Heath S, Volz M, Ostrem JL, MarksWJ Jr: Microelectrode-guided implantation of deep brain stimulators into theglobus pallidus internus for dystonia: Techniques, electrode locations, andoutcomes. J Neurosurg 104:488–501, 2006.
332. Starr PA, Vitek JL, Bakay RA: Ablative surgery and deep brain stimulationfor Parkinson’s disease. Neurosurgery 43:989–1015, 1998.
333. Starr P, Verhagen L, Larson P, Bakay E, Taylor R, Cahn-Weiner D, Bartus R,Ostrem J, Marks W: Intrastriatal gene transfer with AAV-neurturin forParkinson’s disease: Results of a phase I trial. Presented at the 75th AnnualMeeting of the American Association of Neurological Surgeons, Washington,D.C., April 16, 2007.
334. Sterio D, Zonenshayn M, Mogilner AY, Rezai AR, Kiprovski K, Kelly PJ,Beric A: Neurophysiological refinement of subthalamic nucleus targeting.Neurosurgery 50:58–69, 2002.
REZAI ET AL.
SHC836 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
335. Stover NP, Bakay RAE, Subramanian T, Raiser CD, Cornfeldt ML,Schweikert AW, Allen RC, Watts RL: Intrastriatal implantation of human reti-nal pigment epithelial cells attached to microcarriers in advanced Parkinsondisease. Arch Neurol 62:1833–1837, 2005.
336. Svennilson E, Torvik A, Lowe R, Leksell L: Treatment of parkinsonism bystereotatic thermolesions in the pallidal region. A clinical evaluation of 81cases. Acta Psychiatr Scand 35:358–377, 1960.
337. Taha JM, Janszen MA, Favre J: Thalamic deep brain stimulation for the treat-ment of head, voice, and bilateral limb tremor. J Neurosurg 91:68–72, 1999.
338. Tai CH, Boraud T, Bezard E, Bioulac B, Gross C, Benazzouz A:Electrophysiological and metabolic evidence that high-frequency stimulationof the subthalamic nucleus bridles neuronal activity in the subthalamicnucleus and the substantia nigra reticulata. FASEB J 17:1820–1830, 2003.
339. Talairach J, Tournoux P: Co-planar Stereotactic Atlas of the Human Brain.Stuttgart, Thieme Verlag, 1988, pp 5–9.
340. Tapper VJ: Pathophysiology, assessment, and treatment of Parkinson’s dis-ease. Nurse Pract 22:76–78, 1997.
341. Tasker RR: Deep brain stimulation is preferable to thalamotomy for tremorsuppression. Surg Neurol 49:145–154, 1998.
342. Tasker RR: Tremor of parkinsonism and stereotactic thalamotomy. MayoClin Proc 62:736–739, 1987.
343. Tasker RR, Munz M, Junn FS, Kiss ZH, Davis K, Dostrovsky JO, Lozano AM:Deep brain stimulation and thalamotomy for tremor compared. ActaNeurochir Suppl 68:49–53, 1997.
344. Tavella A, Bergamasco B, Bosticco E, Lanotte M, Perozzo P, Rizzone M, TorreE, Lopiano L: Deep brain stimulation of the subthalamic nucleus inParkinson’s disease: Long-term follow-up. Neurol Sci 23 [Suppl 2]:S111–S112, 2002.
345. Teive HA, Sá DS, Grande CV, Antoniuk A, Werneck LC: Bilateral pallido-tomy for generalized dystonia. Arq Neuropsiquiatr 59:353–357, 2001.
346. Terao T, Okiyama R, Takahashi H, Yokochi F, Taniguchi M, Hamada I,Hasegawa N: Comparison and examination of stereotactic surgical complica-tions in movement disorders [in Japanese]. No Shinkei Geka 31:629–636, 2003.
347. Terao T, Takahashi H, Yokochi F, Taniguchi M, Okiyama R, Hamada I:Hemorrhagic complication of stereotactic surgery in patients with move-ment disorders. J Neurosurg 98:1241–1246, 2003.
348. Thobois S, Mertens P, Guenot M, Hermier M, Mollion H, Bouvard M, ChazotG, Broussolle E, Sindou M: Subthalamic nucleus stimulation in Parkinson’sdisease: Clinical evaluation of 18 patients. J Neurol 249:529–534, 2002.
349. Tir M, Devos D, Blond S, Touzet G, Reyns N, Duhamel A, Cottencin O,Dujardin K, Cassim F, Destée A, Defebvre L, Krystkowiak P: Exhaustive,one-year follow-up of subthalamic nucleus deep brain stimulation in alarge, single-center cohort of parkinsonian patients. Neurosurgery61:297–305, 2007.
350. Tisch S, Rothwell JC, Bhatia KP, Quinn N, Zrinzo L, Jahanshahi M, AshkanK, Hariz M, Limousin P: Pallidal stimulation modifies after-effects of pairedassociative stimulation on motor cortex excitability in primary generaliseddystonia. Exp Neurol 206:80–85, 2007.
351. Tisch S, Zrinzo L, Limousin P, Bhatia KP, Quinn N, Ashkan K, Hariz M: Theeffect of electrode contact location on clinical efficacy of pallidal deep brainstimulation in primary generalised dystonia. J Neurol NeurosurgPsychiatry, 2007.
352. Trépanier LL, Kumar R, Lozano AM, Lang AE, Saint-Cyr JA: Neuropsycho-logical outcome of GPi pallidotomy and GPi or STN deep brain stimulationin Parkinson’s disease. Brain Cogn 42:324–347, 2000.
353. Trottenberg T, Fogelson N, Kühn AA, Kivi A, Kupsch A, Schneider GH,Brown P: Subthalamic gamma activity in patients with Parkinson’s disease.Exp Neurol 200:56–65, 2006.
354. Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T: Deafferentation painand stimulation of the thalamic sensory relay nucleus: Clinical and experi-mental study. Appl Neurophysiol 48:166–171, 1985.
355. Uc EY, Follett KA: Deep brain stimulation in movement disorders. SeminNeurol 27:170–182, 2007.
356. Umemura A, Jaggi JL, Hurtig HI, Siderowf AD, Colcher A, Stern MB,Baltuch GH: Deep brain stimulation for movement disorders: Morbidityand mortality in 109 patients. J Neurosurg 98:779–784, 2003.
357. Ushe M, Mink JW, Revilla FJ, Wernle A, Schneider Gibson P, McGee-MinnichL, Hong M, Rich KM, Lyons KE, Pahwa R, Perlmutter JS: Effect of stimula-
tion frequency on tremor suppression in essential tremor. Mov Disord19:1163–1168, 2004.
358. Valldeoriola F, Pilleri M, Tolosa E, Molinuevo JL, Rumià J, Ferrer E: Bilateralsubthalamic stimulation monotherapy in advanced Parkinson’s disease:Long-term follow-up of patients. Mov Disord 17:125–132, 2002.
359. Varma TR, Fox SH, Eldridge PR, Littlechild P, Byrne P, Forster A, MarshallA, Cameron H, McIver K, Fletcher N, Steiger M: Deep brain stimulation ofthe subthalamic nucleus: Effectiveness in advanced Parkinson’s diseasepatients previously reliant on apomorphine. J Neurol Neurosurg Psychiatry74:170–174, 2003.
360. Vergani F, Landi A, Antonini A, Sganzerla EP: Bilateral subthalamic deepbrain stimulation in a patient with Parkinson’s disease who had previouslyundergone thalamotomy and autologous adrenal grafting in the caudatenucleus: Case report. Neurosurgery 59:E1140, 2006.
361. Vesper J, Haak S, Ostertag C, Nikkhah G: Subthalamic nucleus deep brainstimulation in elderly patients—Analysis of outcome and complications.BMC Neurol 7:7, 2007.
362. Vesper J, Klostermann F, Stockhammer F, Funk T, Brock M: Results of chronicsubthalamic nucleus stimulation for Parkinson’s disease: A 1-year follow-upstudy. Surg Neurol 57:306–313, 2002.
363. Vidailhet M, Vercueil L, Houeto JL, Krystkowiak P, Benabid AL, Cornu P,Lagrange C, Tézenas du Montcel S, Dormont D, Grand S, Blond S, DetanteO, Pillon B, Ardouin C, Agid Y, Destée A, Pollak P: Bilateral deep-brainstimulation of the globus pallidus in primary generalized dystonia. N EnglJ Med 352:459–467, 2005.
364. Vidailhet M, Vercueil L, Houeto JL, Krystkowiak P, Lagrange C, Yelnik J,Bardinet E, Benabid AL, Navarro S, Dormont D, Grand S, Blond S, ArdouinC, Pillon B, Dujardin K, Hahn-Barma V, Agid Y, Destée A, Pollak P; FrenchSPIDY Study Group: Bilateral, pallidal, deep-brain stimulation in primarygeneralised dystonia: A prospective 3 year follow-up study. Lancet Neurol6:223–229, 2007.
365. Vingerhoets FJ, Villemure JG, Temperli P, Pollo C, Pralong E, Ghika J:Subthalamic DBS replaces levodopa in Parkinson’s disease: Two-year follow-up. Neurology 58:396–401, 2002.
366. Visser-Vandewalle V, Ackermans L, van der Linden C, Temel Y, Tijssen MA,Schruers KR, Nederveen P, Kleijer M, Boon P, Weber W, Cath D: Deep brainstimulation in Gilles de la Tourette’s syndrome. Neurosurgery 58:E590, 2006.
367. Visser-Vandewalle V, van der Linden C, Temel Y, Celik H, Ackermans L,Spincemaille G, Caemaert J: Long-term effects of bilateral subthalamicnucleus stimulation in advanced Parkinson disease: A four year follow-upstudy. Parkinsonism Relat Disord 11:157–165, 2005.
368. Vitek JL: Deep brain stimulation for Parkinson’s disease. A critical re-evalu-ation of STN versus GPi DBS. Stereotact Funct Neurosurg 78:119–131, 2002.
369. Vitek JL: Mechanisms of deep brain stimulation: Excitation or inhibition.Mov Disord 17 [Suppl 3]:S69–S72, 2002.
370. Vitek JL: Pathophysiology of dystonia: A neuronal model. Mov Disord 17[Suppl 3]:S49–S62, 2002.
371. Vitek JL, Bakay RA: The role of pallidotomy in Parkinson’s disease and dys-tonia. Curr Opin Neurol 10:332–339, 1997.
372. Vitek JL, Bakay RA, Hashimoto T, Kaneoke Y, Mewes K, Zhang JY, Rye D,Starr P, Baron M, Turner R, DeLong MR: Microelectrode-guided pallido-tomy: Technical approach and its application in medically intractableParkinson’s disease. J Neurosurg 88:1027–1043, 1998.
373. Vitek JL, Zhang J, Evatt M, Mewes K, DeLong MR, Hashimoto T, Triche S,Bakay RA: GPi pallidotomy for dystonia: Clinical outcome and neuronalactivity. Adv Neurol 78:211–219, 1998.
374. Voges J, Hilker R, Bötzel K, Kiening KL, Kloss M, Kupsch A, Schnitzler A,Schneider GH, Steude U, Deuschl G, Pinsker MO: Thirty days complica-tion rate following surgery performed for deep-brain-stimulation. MovDisord, 22:1486–1489, 2007.
375. Voges J, Volkmann J, Allert N, Lehrke R, Koulousakis A, Freund HJ, SturmV: Bilateral high-frequency stimulation in the subthalamic nucleus for thetreatment of Parkinson disease: Correlation of therapeutic effect withanatomical electrode position. J Neurosurg 96:269–279, 2002.
376. Voges J, Waerzeggers Y, Maarouf M, Lehrke R, Koulousakis A, Lenartz D,Sturm V: Deep-brain stimulation: Long-term analysis of complicationscaused by hardware and surgery—experiences from a single centre. J NeurolNeurosurg Psychiatry 77:868–872, 2006.
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC837

377. Volkmann J: Deep brain stimulation for the treatment of Parkinson’s disease.J Clin Neurophysiol 21:6–17, 2004.
378. Volkmann J, Allert N, Voges J, Sturm V, Schnitzler A, Freund HJ: Long-termresults of bilateral pallidal stimulation in Parkinson’s disease. Ann Neurol55:871–875, 2004.
379. Volkmann J, Allert N, Voges J, Weiss PH, Freund HJ, Sturm V: Safety andefficacy of pallidal or subthalamic nucleus stimulation in advanced PD.Neurology 56:548–551, 2001.
380. Voon V, Kubu C, Krack P, Houeto JL, Troster AI: Deep brain stimulation:Neuropsychological and neuropsychiatric issues. Mov Disord 21 [Suppl14]:S305–S327, 2006.
381. Walker AE: Cerebral pedunculotomy for the relief of involuntary move-ments; hemiballismus. Acta Psychiatr Neurol 24:723–729, 1949.
382. Walker AE: Cerebral pedunculotomy for the relief of involuntary move-ments. II. Parkinsonian tremor. J Nerv Ment Dis 116:766–775, 1952.
383. Weetman J, Anderson IM, Gregory RP, Gill SS: Bilateral posteroventral pal-lidotomy for severe antipsychotic induced tardive dyskinesia and dystonia.J Neurol Neurosurg Psychiatry 63:554–556, 1997.
384. Welter ML, Houeto JL, Tezenas du Montcel S, Mesnage V, Bonnet AM,Pillon B, Arnulf I, Pidoux B, Dormont D, Cornu P, Agid Y: Clinical predic-tive factors of subthalamic stimulation in Parkinson’s disease. Brain125:575–583, 2002.
385. Wichmann T, DeLong MR: Pathophysiology of Parkinson’s disease: TheMPTP primate model of the human disorder. Ann N Y Acad Sci 991:199–213, 2003.
386. Wichmann T, Delong MR: Deep brain stimulation for neurologic and neu-ropsychiatric disorders. Neuron 52:197–204, 2006.
387. Wills AJ, Jenkins IH, Thompson PD, Findley LJ, Brooks DJ: A positron emis-sion tomography study of cerebral activation associated with essential andwriting tremor. Arch Neurol 52:299–305, 1995.
388. Wong LF, Goodhead L, Prat C, Mitrophanous KA, Kingsman SM, MazarakisND: Lentivirus-mediated gene transfer to the central nervous system:Therapeutic and research applications. Hum Gene Ther 17:1–9, 2006.
389. Woods SP, Fields JA, Lyons KE, Koller WC, Wilkinson SB, Pahwa R, TrosterAI: Neuropsychological and quality of life changes following unilateral thal-amic deep brain stimulation in Parkinson’s disease: A one-year follow-up.Acta Neurochir (Wien) 143:1273–1278, 2001.
390. Woods SP, Fields JA, Troster AI: Neuropsychological sequelae of subthalamicnucleus deep brain stimulation in Parkinson’s disease: A critical review.Neuropsychol Rev 12:111–126, 2002.
391. Wooten GF: Progress in understanding the pathophysiology of treatment-related fluctuations in Parkinson’s disease. Ann Neurol 24:363–365, 1988.
392. Wycis HT, Baird HW, Spiegel EA: Pallidotomy and pallido-amygdalotomyin certain types of convulsive disorders. Confin Neurol 17:67–68, 1957.
393. Yokoyama T, Sugiyama K, Nishizawa S, Yokota N, Ohta S, Uemura K:Subthalamic nucleus stimulation for gait disturbance in Parkinson’s dis-ease. Neurosurgery 45:41–49, 1999.
394. Zhang JG, Zhang K, Ma Y, Hu WH, Yang AC, Chu JS, Wu ST, Ge M, ZhangY, Wang ZC: Follow-up of bilateral subthalamic deep brain stimulation forParkinson’s disease. Acta Neurochir Suppl 99:43–47, 2006.
395. Zhang JG, Zhang K, Wang ZC: Deep brain stimulation in the treatment oftardive dystonia. Chin Med J (Engl) 119:789–792, 2006.
396. Zhang JG, Zhang K, Wang ZC, Ge M, Ma Y: Deep brain stimulation in thetreatment of secondary dystonia. Chin Med J (Engl) 119:2069–2074, 2006.
AcknowledgmentsWe thank Charles Steiner, M.E., Martha Tobin, M.A., and Christine Moore,
A.A., for their expert technical assistance in the preparation of this manuscript.
COMMENTS
This ambitious article shows what a privilege it is to participate in theextraordinary world of movement disorder surgery. This narrow
subspecialty is paradigmatic of the “golden age” of neurosurgery, com-bining so many of the elements that fascinate and inspire us: Its rise hasbeen fueled by seminal discoveries in basal ganglia physiology, the
technical approaches are rapidly evolving, and it represents a comingera where elective neurosurgery can greatly enhance quality of life fora prolonged period in serious neurological diseases.
Philip A. StarrSan Francisco, California
Deep brain stimulation for movement disorders joined the main-stream of neurosurgical practice only in the last 10 years, yet as
noted by Rezai et al. (who have played no small role in increasingaccess to this procedure for patients with movement disorders as wellas other more novel indications), more than 1000 articles have beenpublished on this topic. A detailed, comprehensive review of this com-plex field would require a whole supplement (1), but the authors pro-vide a review that nevertheless addresses all of the major issues and isin a very readable form.
Certain aspects of surgical technique tend to inspire extensive debateamong functional neurosurgeons, such as the use of framed vs. frame-less devices, or the use of microelectrode recording techniques. Rezai etal. provide balanced views of these areas, correctly pointing out thatthese and other issues can only be resolved with prospective, random-ized, blinded trials. However, it is not feasible to subject every nuanceof functional neurosurgical procedures to such a metric. Ten years later,we still do not know from prospective randomized trials (Class 1 evi-dence) whether the subthalamic nucleus (STN) truly is a “superior” tar-get to the globus pallidus internus, and what the relative risks andbenefits are (although two such trials will be arriving soon, one fromEmory and the Cleveland Clinic, and the other from the multicenterNational Institutes of Health/Veteran’s Administration trial). Ten yearslater, we must still suffer the endless debate about the utility of micro-electrode recording, now obfuscating the pioneering work on newpotential targets for Parkinson’s disease (2, 3). As new indications, e.g.,depression (7), and new targets, e.g., pedunculopontine nucleus (PPN),arrive on the landscape, new and old issues will arise, providing morefodder for prospective, randomized, clinical trials: Which is better, STN,PPN, STN + PPN, or STN then PPN (4, 5)? Which is better, gene ther-apy or cell therapy or deep brain stimulation? If gene therapy is better,then which gene therapy? Anterior internal capsule or Area 25 fordepression? Medtronic (Minneapolis, MN) or Advanced Neuromodu-lation Systems (Plano, TX)? Which method is better: yours, or mine, orboth, or neither? And has anyone yet subjected prospective, random-ized, double-blind, sham/placebo-controlled trials to a prospective,randomized, clinical trial? Two such trials seemingly eliminated fetalcell transplantation for Parkinson’s disease, but were the trials fair?Perhaps we will even see this subject revisited in the years to come (6).If Rezai et al. reflects the state of the art for movement disorders alone10 years later and approximately a century after surgery for move-ment disorders began, I suspect functional neurosurgeons will be welloccupied for the next century too.
Robert E. GrossAtlanta, Georgia
1. Benabid AL, Deuschl G, Lang AE, Rezai AR: Deep brain stimulation forParkinson’s disease. Mov Disord 21 [Suppl 14]:S168–S170, 2006.
2. Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C,Schwalb JM, Kennedy SH: Deep brain stimulation for treatment-resistantdepression. Neuron 45:651–660, 2005.
3. Mazzone P, Stanzione P, Lozano A, Scarnati E, Peppe A, Galati S, Stefani A:Reply: The peripeduncular and pedunculopontine nuclei: A putative disputenot discouraging the effort to define a clinically relevant target. Brain 130:E74,2007 (comment).
REZAI ET AL.
SHC838 | VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT www.neurosurgery-online.com
4. Plaha P, Gill SS: Bilateral deep brain stimulation of the pedunculopontinenucleus for Parkinson’s disease. Neuroreport 16:1883–1887, 2005.
5. Stefani A, Lozano AM, Peppe A, Stanzione P, Galati S, Tropepi D, PierantozziM, Brusa L, Scarnati E, Mazzone P: Bilateral deep brain stimulation of thepedunculopontine and subthalamic nuclei in severe Parkinson’s disease. Brain130:1596–1607, 2007.
6. Tuszynski M: Rebuilding the brain: Resurgence of fetal grafting. Nat Neurosci10:1229–1230, 2007.
7. Zrinzo L, Zrinzo LV, Hariz M: The pedunculopontine and peripeduncularnuclei: A tale of two structures. Brain 130:E73, 2007.
In this article, Rezai et al. provide an excellent overview of the currentstatus of movement disorder neurosurgery. The information is pro-
vided in a well-organized manner and the literature review is exten-sive. The conclusions presented are based on the available literature,gray areas in our knowledge are appropriately highlighted, and profes-sional biases are minimized. This is a comprehensive first read for any-one interested in participating in this exciting field of neurosurgery.
Ron L. AltermanBronx, New York
Rezai et al. provide an outstanding review of the history, presentstatus, and possible future of movement disorder surgery that has
progressed from gross ablations to precise lesioning to neuroaugmen-tation and neuromodulation. Initially based on empiricism and a crudeunderstanding of the neural circuitry of the motor system, functionalneurosurgery has been ever more refined by better understanding ofextrapyramidal neurophysiology and cellular neurochemistry. As aresult of modern advances in basic science, future procedures may gobeyond simple manipulation of large cellular populations for the con-trol of symptoms (as we do now with deep brain stimulation neu-roaugmentation) to neurochemically target-specific cellular groupswithin these populations. In addition, genetically programmed stemcells may be used to repopulate central nervous system regions whosecells have been decimated by the underlying disease process. However,the ultimate therapy may focus on identifying and reversing the neu-rotoxic triggers that result in selective loss of neuromelanin-containingdopaminergic neurons in the substantia nigra.
Patrick J. KellyNew York, New York
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC839
Dissection of the brain, (engraving, after A. Vesalius, Fabrica, 1543), T. Geminus, Compendiosa totius anatomie delineatio. London, J. Herford, 1545. (From:Roberts KB, Tomlinson JDW: The Fabric of the Body: European Traditions of Anatomical Illustration. Oxford, Clarendon Press, 1992).





























