Embed Size (px)
Citation preview

Surgical Treatment of Cardiac Tumors: A 25-Year Experience Michael C. Murphy, MD, Michael S. Sweeney, MD, J. B. Putnam, Jr, MD, William E. Walker, MD, 0. H. Frazier, MD, David A. Ott, MD, and Denton A. Cooley, MD Texas Heart Institute, The University of Texas Health Science Center, and M. D. Anderson Cancer Institute, Houston, Texas
From 1964 to 1989, we performed operations on 133 patients with cardiac tumors. There were 58 male and 75 female patients ranging in age from three days to 81 years; 101 were adults, and 32 were children (less than 12 years of age). Primary tumors (102 benign and 12 malig- nant) were found in 114 patients and metastatic tumors in 19. Symptoms included congestive heart failure, arrhyth- mias, emboli, and chest pain. Diagnosis was accom- plished through angiography, echocardiography, com- puted tomography, and magnetic resonance imaging. Operative treatment encompassed techniques ranging from biopsy to complete excision (including hypothermic circulatory arrest and cardiac autotransplantation) depend- ing on the site of disease and the extent of involvement. Overall operative survival was 91%. Twelve patients died
ardiac tumors are rare, with an incidence ranging C from 0.0017% to 0.03% at postmortem examination in different series [l-31. Much has changed since Hodgkin first distinguished tumor from thrombus in the early 19th century and since Crafoord first reported successful exci- sion of a cardiac tumor using cardiopulmonary bypass in 1955 [4].
In the 25-year period 1964 to 1989, we saw 133 patients with cardiac neoplasms. This report reviews our experi- ence with numerous cardiac tumors, both benign and malignant, and primary and metastatic. Our data suggest that an aggressive surgical approach is generally safe, usually efficacious, and appropriately considered as ther- apy for otherwise untreatable lesions.
Material and Methods We reviewed the hospital records and follow-up clinical charts of 133 patients with heart tumors who were treated at our institution. Of these patients, 114 had primary tumors (102 were benign, and 12 were malignant), and 19 had metastatic tumors. There were 101 adults and 32 children (less than 12 years old), and the age range was three days to 81 years. We analyzed our patients by placing them in groups according to the type of tumor and
Presented at the Thirty-sixth Annual Meeting of the Southern Thoracic Surgical Association, Scottsdale, AZ, Nov 9-11, 1989.
Address reprint requests to Dr Sweeney, University of Texas Medical School, 6431 Fannin, MSB 1.220, Houston, TX 77030.
early (within 30 days of operation), and follow-up was obtained for 110 (90.9%) of the remaining 121 survivors (total patient-years of follow-up, 572.8; mean follow-up, 5.2 years). Of the 20 patients who died late, 15 had malignant disease. Operative survival for patients with primary cardiac malignancies and for those with meta- static disease was 83% and 68.4%, respectively, with 3 and 5 patients, respectively, still living. We advocate an aggressive surgical approach, especially in patients with benign tumors, who can expect an excellent outcome. For patients with malignant or metastatic disease, palliation and cure are also possible if aggressive surgical actions are taken.
(Ann Thorac Surg 1990;49:612-8)
reviewed the presenting symptoms, diagnosis, and sur- gical treatment.
Benign Tumors MYXOMA. The most common benign tumor in this series was myxoma, affecting 55% of the patients, all of whom were adults (Table 1). Three patients had previously undergone resection of a myxoma, had local recurrences, and were referred to us for further treatment. Presenting symptoms included congestive heart failure (44 patients), palpitations (14), emboli (13), constitutional symptoms (ll), syncope (lo), and chest pain (8). Five patients had no symptoms.
Diagnosis was made preoperatively by angiography in 47 patients. It revealed intracavitary filling defects (fixed or mobile), neovascularity, and valvular obstruction or insufficiency. Pulmonary hypertension (mean pulmonary artery pressure greater than 20 mm Hg) was present in 27 of 39 patients in whom intracardiac pressures were re- corded. Echocardiography confirmed the diagnosis in 35 patients and was the sole method used in 4 of them. Diagnosis was made during operation for suspected mi- tral valve disease in 5 patients. Tumors were located in the left atrium in the majority of patients. There were no tumors in either ventricle.
Currently, we completely excise myxomas through a biatrial approach during total cardiopulmonary bypass support under moderate hypothermia (30°C) with bicaval cannulation for venous drainage. The full thickness of the septum is excised if the lesion is in the region of the fossa
0 1990 by The Society of Thoracic Surgeons 0003-4975/90/$3.50

Ann Thorac Surg 1990;49:612-8
MURPHY ET AL 613 CARDIAC TUMORS
Table 1. Profiles of Patients With Primary Benign Tumors
Follow-up Deaths
No. of Mean Sex Age No. of ~
Tumor Type Patients M F Range Mean Early” Late Patients Range ( Y 4 Myxoma 63 24 39 21-81 yr 51 yr 2 3 (2b) 50‘ 2 mc-25 yr 7.1 Purkinje cell 13 4 9 2-20 mo 12.6 mo 0 1 12 6 m0-8 yr 3.8 Rhabdomyoma 9 2 7 3 days-1 yr 5.3 mo 1 0 8 7 m0-8.5 yr 3.1
2-18 yr 7.3 Lipoma 4 2 2 2165 yr 49 yr 0 0 4 7-13 yr 8 Other 6 3 3 9-55 yr 39.1 yr 1 lb 5 2-22 yr 7.1
102 38 64 3days-81 yr 36.17yr 4 5 (3b) 86 2 mc-25 yr 6.5
Fibroma 7 3 4 lmc-12yr 3.3 yr 0 0 7
Total
a Early death is defined as death within the perioperative period or within 30 days of operation. the 61 patients who lived more than 30 days after operation, 50 were followed up and data were available.
These deaths were unrelated to the tumor. Of
ovalis. The atrial septa1 defect created is closed with a Dacron patch or, less commonly, by primary closure [5].
PURKINJE CELL. Purkinje cell tumors (also known as myo- cardial hamartomas) were the second most common type of tumor in our patients (see Table 1). As reported by Garson and associates [6, 71, all the patients in this group were children, and all had incessant ventricular tachycar- dia. In 12 patients, cardiovascular collapse, characterized by hypotension or cardiac arrest, was present. One pa- tient was asymptomatic.
All patients underwent echocardiographic studies, and then angiographic studies with electrophysiological map- ping were done to determine the focus of the tachycardia. Medical therapy had failed in every patient. All patients subsequently underwent operation in which intraopera- tive electrophysiological mapping was followed by exci- sion or cryoablation (or both) of the originating focus.
RHABDOMYOMA. All patients with rhabdomyomas were children (see Table 1). The most common presenting symptoms included intractable ventricular arrhythmias ( 4 patients) and heart murmurs (5). One of the patients with heart murmurs had accompanying cyanosis, which was caused by a pulmonary outflow tract obstruction as shown by echocardiography, and 1 had congestive heart failure. Three patients were known to have tuberous sclerosis, which has been noted in up to 50% of patients with rhabdomyomas (81. Five patients had single tumors, and 4 had multiple tumors.
After attempts to treat the arrhythmias with medication failed, those patients underwent cardiac catheterization and electrophysiological mapping to delineate the ar- rhythmogenic foci. Two patients were found to have single tumors, and 2 had multiple tumors. They subse- quently underwent operation during which intraopera- tive electrophysiological mapping was done, followed by excision of the tumor or tumors.
Four of the patients with heart murmurs underwent resection of the tumors. A palliative shunt was created in the patient with cyanosis because the large size of the tumor precluded resection.
FIBROMA. All patients who had a fibroma were children (see Table 1). Presenting symptoms included heart mur- murs in 3 and congestive heart failure from cardiac obstruction in 2. In 1 patient, the tumor was found during evaluation for cardiomegaly and in another, during oper- ation for pulmonary stenosis. All patients in this group had single tumors. Depending on individual conditions, operative procedures ranged from incision biopsy to com- plete resection.
LIPOMA. Among the 4 patients in whom lipomas were found, diagnosis was made on examination of chest roentgenograms in 2, during coronary artery bypass graft- ing in 1, and during aortic valve replacement in 1 (see Table 1). Despite their large sizes, these tumors caused no specific symptoms. In all patients, the tumors were com- pletely excised.
OTHER BENIGN TUMORS. One patient had excision of a right atrial hemangioma discovered during operation to repair the mitral valve. One patient had a spherical filling defect at the mitral valve, which was caused by a cyst attached to the anterior leaflet of that valve; the patient underwent operation to remove the cyst. A 1.7-cm mass was found in the right ventricular outflow tract of a patient with a loud heart murmur. The mass proved to be a cardiac venous malformation (varix) filled with organized thrombus and was easily removed. A right ventricular angiomatous hamartoma was found in 1 patient who had premature atrial contractions associated with a lesion seen on the chest roentgenogram; the tumor was subsequently ex- cised. One patient underwent removal of a granuloma involving the surface of the right ventricle. Finally, an intramyocardial cyst was located and removed in 1 pa- tient.
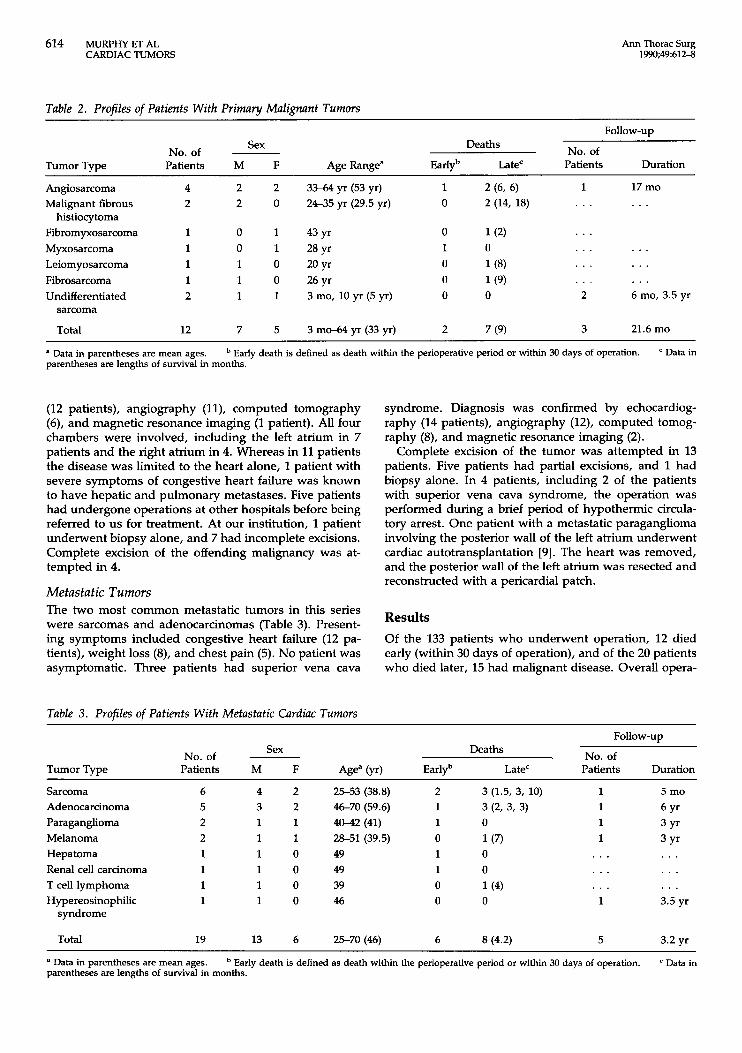
Primary Malignant Tumors All 12 patients had varieties of sarcoma (Table 2), and all had varying degrees of cardiac obstruction and resultant congestive heart failure. Presenting symptoms included chest pain (4 patients), weight loss (3), and arrhythmia (1 patient). Diagnosis was made through echocardiography
614 MURPHY ET AL CARDIAC TUMORS
Ann Thorac Surg 1990;49:612-8
Table 2. Profiles of Patients With Primary Malignant Tumors
Follow-up Deaths No. of Sex
NO. of - Tumor Type Patients M F Age Range“ Early” Late‘ Patients Duration
Angiosarcoma 4 2 2 3 M 4 yr (53 yr) 1 2 (6, 6 ) 1 17 mo Malignant fibrous 2 2 0 24-35 yr (29.5 yr) 0 2 (14, 18) . . . . . .
Fibromyxosarcoma 1 0 1 43 yr 0 1 (2) . . . Myxosarcoma 1 0 1 28 yr 1 0 . . . . . . Leiomyosarcoma 1 1 0 20yr 0 . . . . . . Fibrosarcoma 1 1 0 26yr 0 1(9) Undifferentiated 2 1 1 3 mo, 10 yr (5 yr) 0 0
histiocytoma
. . . . . . 2 6 mo, 3.5 yr
sarcoma
Total 12 7 5 3 mo-64 yr (33 yr) 2 7 (9) 3 21.6 mo
a Data in parentheses are mean ages. parentheses are lengths of survival in months.
Early death is defined as death within the perioperative period or within 30 days of operation. ‘ Data in
(12 patients), angiography (ll), computed tomography (6), and magnetic resonance imaging (1 patient). All four chambers were involved, including the left atrium in 7 patients and the right atrium in 4. Whereas in 11 patients the disease was limited to the heart alone, 1 patient with severe symptoms of congestive heart failure was known to have hepatic and pulmonary metastases. Five patients had undergone operations at other hospitals before being referred to us for treatment. At our institution, 1 patient underwent biopsy alone, and 7 had incomplete excisions. Complete excision of the offending malignancy was at- tempted in 4.
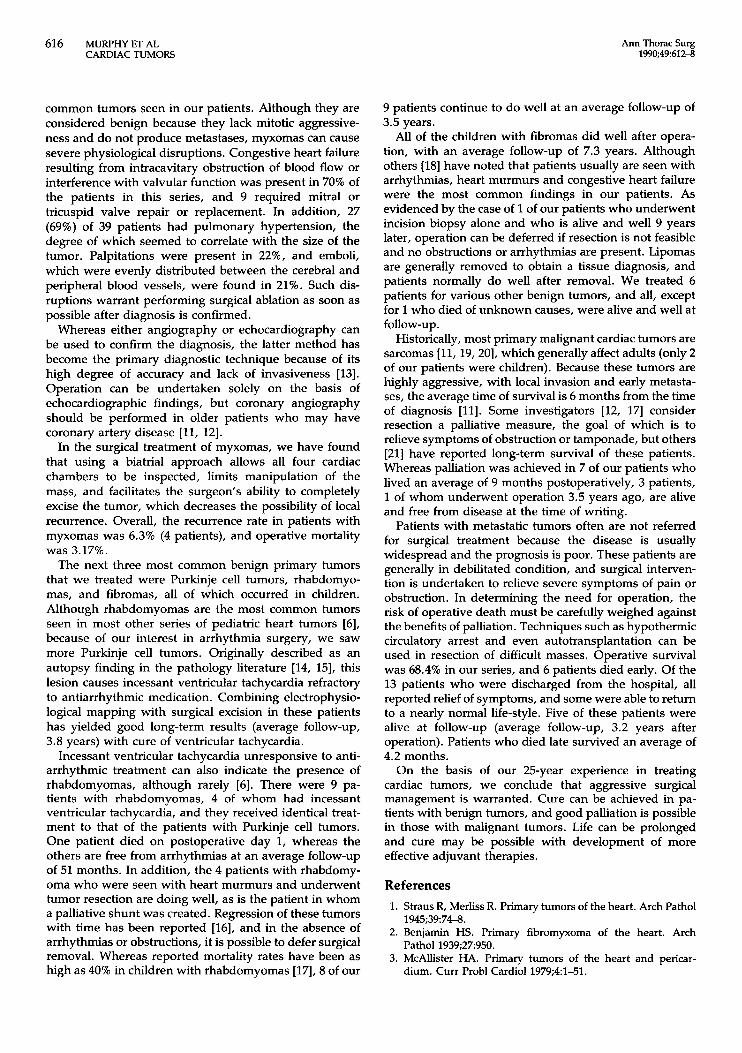
Metastatic Tumors The two most common metastatic tumors in this series were sarcomas and adenocarcinomas (Table 3). Present- ing symptoms included congestive heart failure (12 pa- tients), weight loss (€9, and chest pain (5). No patient was asymptomatic. Three patients had superior vena cava
syndrome. Diagnosis was confirmed by echocardiog- raphy (14 patients), angiography (12), computed tomog- raphy (8), and magnetic resonance imaging (2).
Complete excision of the tumor was attempted in 13 patients. Five patients had partial excisions, and 1 had biopsy alone. In 4 patients, including 2 of the patients with superior vena cava syndrome, the operation was performed during a brief period of hypothermic circula- tory arrest. One patient with a metastatic paraganglioma involving the posterior wall of the left atrium underwent cardiac autotransplantation [9]. The heart was removed, and the posterior wall of the left atrium was resected and reconstructed with a pericardial patch.
Results Of the 133 patients who underwent operation, 12 died early (within 30 days of operation), and of the 20 patients who died later, 15 had malignant disease. Overall opera-
Table 3. Profiles of Patients With Metastatic Cardiac Tumors
FOIIOW-UP
No. of Sex Deaths No. of
Tumor Type Patients M F Age” (Yr) Early” Late‘ Patients Duration
Sarcoma Adenocarcinoma Paraganglioma Melanoma Hepatoma Renal cell carcinoma T cell lymphoma Hypereosinophilic
syndrome
Total 19
4 2 3 2 1 1 1 1 1 0 1 0 1 0 1 0
13 6
25-53 (38.8) 46-70 (59.6) 4042 (41) 28-51 (39.5) 49 49 39 46
25-70 (46) 6
3 (1.5, 3, 10) 3 (2, 3, 3) 0 1(7) 0 0 1 (4) 0
8 (4.2)
1 1 1 1
. . .
. . .
. . . 1
5
5 mo 6 Y‘ 3Yr 3Yr . . . . . . . . . 3.5 yr
3.2 yr ~~ ~~~~
a Data in parentheses are mean ages. parentheses are lengths of survival in months.
Early death is defined as death within the perioperative period or within 30 days of operation. Data in

Ann Thorac Surg 1990;49:612-8
MURPHYETAL 615 CARDIAC TUMORS
tive survival was 91%. Total follow-up for this series is 572.8 patient-years (mean follow-up, 5.2 years).
Benign Tumors MYXOMA. Of the 63 myxomas, 57 (90.5%) were of left atrial origin and six (9.5%), of right atrial origin; none originated in either ventricle. The tumors ranged in size from 1.5 x 1.5 x 0.5 cm to 11 x 7 x 4 cm. The consistency of the tumors also varied from smooth and firm to friable and soft. Associated operative procedures included mitral (5 patients) or tricuspid (4) valve repair or replacement, aortocoronary bypass (3), atrial septa1 defect closure (2), and aortic valve replacement (1 patient).
Arrhythmias, usually transient supraventricular tachy- cardia, were the most common postoperative complica- tion (12 patients). Two patients had pulmonary emboli, 1 experienced bleeding, and 1 had a stroke. Only 1 patient, who had undergone treatment for a left atrial myxoma, had a recurrence of myxoma in the right atrium after operation.
Sixty-one patients lived more than 30 days after opera- tion, and follow-up information was available on 50 (see Table 1). For the 2 patients who died early, the cause of death was myocardial infarction on postoperative day 4 in 1 and multiorgan failure on postoperative day 28 in the other. This latter patient was 81 years old, the oldest in the series. There were three late deaths, and the only one related to myxoma occurred in a 32-year-old woman who had multiple recurrences and reoperations and died as a result of cardiomyopathy. All the other survivors are asymptomatic and free from disease.
PURKINJE CELL. Arrhythmias were successfully ablated in all 13 patients, and visible areas of gray-white myocar- dium were excised in 12. None had evidence of ventricu- lar tachycardia on leaving the operating room. Three patients experienced recurrent tachycardia within the first postoperative week and required reoperation; all reoper- ations were successful. Postoperative complications in- cluded ventricular premature contractions in 2 patients, which resolved with antiarrhythmic medication, and com- plete heart block in 1 patient in whom a pacemaker was subsequently implanted. The one death occurred 3.5 months after operation in a patient with diffuse endocar- dial lesions that required extensive subendocardial resec- tion and led to intractable congestive heart failure.
Twelve patients have been followed, all of whom are alive and well (see Table 1). They have neither experi- enced recurrent arrhythmias nor required antiarrhythmic medications.
RHABDOMYOMA. After operation, 3 of the 4 patients with arrhythmias had successful resolution of tachycardia and have not required antiarrhythmic medication. The other patient, a 4-month-old infant, died on postoperative day 1 of intractable congestive heart failure secondary to papil- lary muscle injury that occurred during operation. All of the patients seen with heart murmurs survived operation and were alive and well at follow-up.
FIBROMA. All patients survived operation and were alive and well at follow-up (see Table 1). One patient who was 7 months old at the time that an incision biopsy alone was performed on a left ventricular free wall tumor has been followed for 9 years and continues to do well.
LIPOMA. All 4 patients survived the operation without postoperative complications and were alive and well at follow-up (see Table 1).
OTHER BENIGN TUMORS. Each of the 6 patients survived operation, and 5 have remained asymptomatic without signs of recurrence (see Table 1). The patient with the intramyocardial cyst, however, died within two days of operation as a result of cardiac arrest. At postmortem examination, no evidence of myocardial infarction could be found.
Prima y Malignant Tumors Of the 12 patients with primary malignant tumors, 3 are alive at 6, 17, and 54 months (see Table 2). These patients all had complete excision and included both children with undifferentiated sarcoma and 1 adult with angiosarcoma. Two patients have undergone postoperative chemother- apy and 1 patient, radiotherapy.
The patients who died survived an average of 9 months postoperatively, and palliation of the obstructive symp- toms was good. One patient with angiosarcoma and the patient with myxosarcoma died in the immediate periop- erative period. Metastatic disease was the cause of death in all but 1 of these patients. In 2 of the patients with angiosarcoma, no evidence of residual cardiac tumor was found [lo]. The 2 patients who underwent resection of primary cardiac malignant fibrous histiocytomas survived 14 months and 18 months.
Metastatic Tumor Despite their debilitated condition, 17 of the 19 patients with cardiac metastases survived attempts at surgical resection. There were four additional early deaths, and 13 patients were discharged from the hospital with relief of symptoms. Of these, 8 died an average of 4.2 months after operation, and 5 are alive at an average follow-up of 3.2 years.
Among operative survivors, early complications in- cluded respiratory or congestive heart failure (2 patients each), arrhythmias (1 patient), and bacterial sepsis follow- ing chemotherapy (1). Except for 1 of the patients with congestive heart failure and the 1 with arrhythmias, early postoperative complications played a major role in the early deaths.
Comment Using modern techniques of myocardial protection, car- diopulmonary bypass, hypothermic circulatory arrest, and even cardiac autotransplantation, the cardiac surgeon can resect almost all tumors of the heart and great vessels. Patients with benign tumors have a low incidence of morbidity and mortality, and resection results in cure.
As in other series [ll, 121, myxomas were the most
616 MURPHY ET AL CARDIAC TUMORS
Ann Thorac Surg 1990;49612-8
common tumors seen in our patients. Although they are considered benign because they lack mitotic aggressive- ness and do not produce metastases, myxomas can cause severe physiological disruptions. Congestive heart failure resulting from intracavitary obstruction of blood flow or interference with valvular function was present in 70% of the patients in this series, and 9 required mitral or tricuspid valve repair or replacement. In addition, 27 (69%) of 39 patients had pulmonary hypertension, the degree of which seemed to correlate with the size of the tumor. Palpitations were present in 22%, and emboli, which were evenly distributed between the cerebral and peripheral blood vessels, were found in 21%. Such dis- ruptions warrant performing surgical ablation as soon as possible after diagnosis is confirmed.
Whereas either angiography or echocardiography can be used to confirm the diagnosis, the latter method has become the primary diagnostic technique because of its high degree of accuracy and lack of invasiveness [13]. Operation can be undertaken solely on the basis of echocardiographic findings, but coronary angiography should be performed in older patients who may have coronary artery disease [ l l , 121.
In the surgical treatment of myxomas, we have found that using a biatrial approach allows all four cardiac chambers to be inspected, limits manipulation of the mass, and facilitates the surgeon’s ability to completely excise the tumor, which decreases the possibility of local recurrence. Overall, the recurrence rate in patients with myxomas was 6.3% (4 patients), and operative mortality was 3.17%.
The next three most common benign primary tumors that we treated were Purkinje cell tumors, rhabdomyo- mas, and fibromas, all of which occurred in children. Although rhabdomyomas are the most common tumors seen in most other series of pediatric heart tumors [6], because of our interest in arrhythmia surgery, we saw more Purkinje cell tumors. Originally described as an autopsy finding in the pathology literature [14, 151, this lesion causes incessant ventricular tachycardia refractory to antiarrhythmic medication. Combining electrophysio- logical mapping with surgical excision in these patients has yielded good long-term results (average follow-up, 3.8 years) with cure of ventricular tachycardia.
Incessant ventricular tachycardia unresponsive to anti- arrhythmic treatment can also indicate the presence of rhabdomyomas, although rarely [6]. There were 9 pa- tients with rhabdomyomas, 4 of whom had incessant ventricular tachycardia, and they received identical treat- ment to that of the patients with Purkinje cell tumors. One patient died on postoperative day 1, whereas the others are free from arrhythmias at an average follow-up of 51 months. In addition, the 4 patients with rhabdomy- oma who were seen with heart murmurs and underwent tumor resection are doing well, as is the patient in whom a palliative shunt was created. Regression of these tumors with time has been reported [16], and in the absence of arrhythmias or obstructions, it is possible to defer surgical removal. Whereas reported mortality rates have been as high as 40% in children with rhabdomyomas [17], 8 of our
9 patients continue to do well at an average follow-up of 3.5 years.
All of the children with fibromas did well after opera- tion, with an average follow-up of 7.3 years. Although others [18] have noted that patients usually are seen with arrhythmias, heart murmurs and congestive heart failure were the most common findings in our patients. As evidenced by the case of 1 of our patients who underwent incision biopsy alone and who is alive and well 9 years later, operation can be deferred if resection is not feasible and no obstructions or arrhythmias are present. Lipomas are generally removed to obtain a tissue diagnosis, and patients normally do well after removal. We treated 6 patients for various other benign tumors, and all, except for 1 who died of unknown causes, were alive and well at
Historically, most primary malignant cardiac tumors are sarcomas [ll, 19,201, which generally affect adults (only 2 of our patients were children). Because these tumors are highly aggressive, with local invasion and early metasta- ses, the average time of survival is 6 months from the time of diagnosis [ l l ] . Some investigators [12, 171 consider resection a palliative measure, the goal of which is to relieve symptoms of obstruction or tamponade, but others [21] have reported long-term survival of these patients. Whereas palliation was achieved in 7 of our patients who lived an average of 9 months postoperatively, 3 patients, 1 of whom underwent operation 3.5 years ago, are alive and free from disease at the time of writing.
Patients with metastatic tumors often are not referred for surgical treatment because the disease is usually widespread and the prognosis is poor. These patients are generally in debilitated condition, and surgical interven- tion is undertaken to relieve severe symptoms of pain or obstruction. In determining the need for operation, the risk of operative death must be carefully weighed against the benefits of palliation. Techniques such as hypothermic circulatory arrest and even autotransplantation can be used in resection of difficult masses. Operative survival was 68.4% in our series, and 6 patients died early. Of the 13 patients who were discharged from the hospital, all reported relief of symptoms, and some were able to return to a nearly normal life-style. Five of these patients were alive at follow-up (average follow-up, 3.2 years after operation). Patients who died late survived an average of 4.2 months.
On the basis of our 25-year experience in treating cardiac tumors, we conclude that aggressive surgical management is warranted. Cure can be achieved in pa- tients with benign tumors, and good palliation is possible in those with malignant tumors. Life can be prolonged and cure may be possible with development of more effective adjuvant therapies.
follow-up.
References 1. Straus R, Merliss R. Primary tumors of the heart. Arch Pathol
2. Benjamin HS. Primary fibromyxoma of the heart. Arch
3. McAllister HA. Primary tumors of the heart and pericar-
1945;3974-8.
Pathol 1939;27950.
dium. Curr Probl Cardiol 1979;4:1-51.
Ann Thorac Surg 1990;49:612-8
MURPHY ET AL 617 CARDIAC TUMORS
4.
5.
6.
7.
8.
9.
10.
11.
12.
Cooley DA. Surgical management of cardiac tumors. In: Kapoor AS, ed. Cancer and the heart. New York Springer- Verlag, 1986:12&34. Kabbani SS, Cooley DA. Atrial myxoma. Surgical consider- ations. J Thorac Cardiovasc Surg 1973;65731-7. Garson A, Smith RT, Moack JP, et al. Incessant ventricular tachycardia in infants: myocardial hamartomas and surgical cure. J Am Coll Cardiol 1987;10:619-26. Garson A Jr, Gillette PC, Titus JL, et al. Surgical treatment of ventricular tachycardia in infants. N Engl J Med 1984; 310: 1443-5. Arciniegas E, Hakimi M, Farooki ZQ, Truccone NJ, Green EW. Primary cardiac tumors in children. J Thorac Cardiovasc Surg 1980;79:582-91. Cooley DA, Reardon MJ, Frazier OH, Angelini P. Human cardiac explanation and autotransplantation: application in a patient with a large cardiac pheochromocytoma. Tex Heart lnst J 1985;12171-6. Reece IJ, Cooley DA, Frazier OH, Hallman GL, Powers PL, Montero CG. Cardiac tumors: clinical spectrum and progno- sis of lesions other than classical benign myxoma in 20 patients. J Thorac Cardiovasc Surg 1984;88:43946. Dein JR, Frist WH, Stinson EB. Primary cardiac neoplasms: early and late results of surgical treatment in 42 patients. J Thorac Cardiovasc Surg 1987;93:502-11. Silverman NA. Primary cardiac tumors. Ann Surg 1980; 19L127-38.
13. Donahoo JS, Weiss JL, Gardner TJ, et al. Current manage- ment of atrial myxomas with emphasis on a new diagnostic technique. Ann Surg 1979;189:763-8.
14. Ferrans VJ, McAllister HA Jr, Haese WH. Infantile cardiomy- opathy with histiocytoid change in cardiac muscle cells: report of six patients. Circulation 1976;5370&19.
15. James TN, Beeson CW 11, Sherman EB, Mowry RW. De subitaneis mortibus. XIII. Multifocal Purkinje cell tumors of the heart. Circulation 1975;52:33M.
16. Foster ED, Spooner EW, Farina MA, Shaher RM, Alley RD. Cardiac rhabdomyoma in the neonate: surgical management. Ann Thorac Surg 1984;37249-53.
17. Chitwood WR Jr. Cardiac neoplasms: current diagnosis, pathology, and therapy. J Cardiac Surg 1988;3:119-54.
18. Kimura M, Fujino T, Kawachi Y, Kitazatok K. Successful excision of a right ventricular fibroma associated with ven- tricular tachycardia: report of a six year survival. Jpn Heart J 1988;29753-9.
19. Bear PA, Moodie DS. Malignant primary cardiac tumors: the Cleveland Clinic experience, 1956 to 1986. Chest 1987; 92:86&2.
20. McAllister HA Jr, Fenoglio JJ. Tumors of the cardiovascular system. In: Atlas of tumor pathology. Fasc. 15, second series. Washington, DC: Armed Forces Institute of Pathology, 1978.
21. Srlie D, Myhre ESP, Stalsberg H. Angiosarcoma of the heart. Unusual presentation and survival after treatment. Br Heart J 1984;51:9&7.
DISCUSSION
DR W. RANDOLPH CHITWOOD, JR (Greenville, NC): I con- gratulate Dr Murphy on an absolutely outstanding presentation, and Drs Cooley, Sweeney, and co-workers for what is most assuredly the largest series of patients with cardiac tumors treated surgically, that is, 133 patients. I am very supportive of your aggressive approach for the treatment of primary and metastatic malignant tumors with obstruction. Your survival of up to 4% years for patients with primary malignant tumors and the average survival of 3.2 years for 5 patients with metastatic tumors are excellent.
I thought that the use of autotransplantation in your series was a very ingenious approach. I know of only 2 patients in the literature who had transplantation, and they had cardiac fi- bromas.
Certainly this is the largest group of Purkinje tumors extant, displacing rhabdomyomas in your series as the second most frequent tumor. Three patients required reoperation for recurrent arrhythmias after a Purkinje tumor resection. Also, I noticed that 1 patient died of multiple Purkinje tumors in the endocardium. At reoperation in those patients with recurrent arrhythmias, did you find multiple tumors?
DR MURPHY The patients who had reoperation underwent a local reexcision of the Purkinje cell lesions. The mapping was done again and localized the earliest activation to the site where resection had previously been done. Resection involved a more extensive procedure, and that ultimately resulted in the death of the 1 patient who died 3.5 months after operation. She had extensive subendocardial tumor and required resection of both left and right ventricular endocardium. She died of refractory congestive heart failure.
DR CHITWOOD: The biatrial approach is certainly a very excellent method for both localization and mobilization of myx-
omas; however, my colleagues and I have found that the right atrial approach is satisfactory for most cardiac myxomas, includ- ing right atrial and left atrial myxomas. Even large ones can be excised through the septum. However, we do use transesoph- ageal echocardiography very liberally as well as epicardial echo- cardiography for children with rhabdomyomas. Have you used transesophageal echocardiography for definitive localization of the tumor stalk?
DR MURPHY We have not yet used intraoperative echocardiog- raphy in the evaluation of these patients with tumors. This technique appears to be becoming more popular at our institu- tion, but is still in its earliest stages of operative use.
DR IRVING L. KRON (Charlottesville, VA): I have two ques- tions. One, do you definitely need the biatrial approach to left atrial myxomas? Dr Nolan has demonstrated to me the technique of inverting the left atrium through the atrial appendage, and you can get excellent access to the septum.
My second question concerns Purkinje cell tumors. Consider the case of a child who has ventricular arrhythmias. Preoperative mapping is performed, and all that is demonstrated is ventricular tachycardia but no anatomical focus by echocardiography or computed tomographic scan. Do you think that alone is an indication for surgical intervention?
DR MURPHY The first question regarded the technique of removal of myxomas. We recommend the biatrial approach because it allows minimal handling of the tumor and complete examination of both atria and both ventricles. It allows en bloc removal of the tumor with minimal handling of the tumor itself, and has proved to be the technique that we use in most instances. Your approach, though we have not used it, sounds very effective.

618 MURPHY ET AL CARDIAC TUMORS
Ann Thorac Surg 1990;49612-8
As for failing to localize an actual tumor preoperatively in a child with a Purkinje cell lesion and ventricular tachycardia, there is actually no current methodology that can determine without a doubt that that child has a Purkinje cell tumor before operation. Neither angiography nor echocardiography identified any of these tumors before operation in our series. We believe that a child less than 2 years old with incessant ventricular tachycardia refractory to medication deserves operative exploration on that basis alone, after preoperative echocardiography and angiogra- phy with electrophysiological study.
DR SAFUH ATTAR (Baltimore, MD): Our experience has in- volved 20 primary cardiac tumors and innumerable metastatic cardiac tumors. I have a few points to stress and then a few questions to ask.
Among the benign tumors, there were seven fibromas. We had 1 child who at the age of 3 years had biopsy of a fibromyxoma. Pathological study revealed definite evidence of tumor. We followed this patient for 20 years; he is currently alive and has no evidence of recurrence. What is the follow-up for the patients with fibromas in your series?
Another point is that myxomas occur mostly in the cavities of the heart rather than in the valves. The valves are mostly involved either with fibroelastomas or with malignant tumors, and malignant tumors occur mostly in children, whereas adult cardiac tumors are mostly benign. We have had 1 case of recurrence of left atrial myxoma. The septum was excised, and yet recurrence occurred three times. What should be done when there are such repeat recurrences?
Finally, in our series, the prognosis for myxomas of the right
side was much worse than that for myxomas of the left, even if the tumor was resected, because of the need for removal of the valve.
My last question concerns the method for diagnosis. We have used exclusively two-dimensional echocardiography for the di- agnosis. Do you think that magnetic resonance imaging would be of any additional help? Is it necessary, considering its expense?
DR MURPHY Of myxomas?
DR ATTAR Of all cardiac tumors.
DR MURPHY The last question first. Echocardiography is probably the best screening device for cardiac tumors. Angiog- raphy is usually done in addition as a complementary study. As for computed tomography and magnetic resonance imaging, magnetic resonance imaging was used increasingly in the latter part of our series. It is particularly good for determining whether there is extracavitary involvement of the tumor and whether, in fact, the tumor originates in an intracavitary location or an extracavitary site.
The follow-up of the 7 children with fibromas averaged 7 years. All were doing well in follow-up, including the patient with the massive right ventricular fibroma.
Another question concerned patients with recurrent tumors. There were 4 patients with recurrent tumors in our series, 3 of whom were operated on initially at other institutions. As for operation for recurrence, we believe that wide excision of the septum with septa1 patch reconstruction with Dacron is the best way to prevent recurrence.





























