Embed Size (px)
Citation preview

1 23
Surgical and Radiologic Anatomy ISSN 0930-1038 Surg Radiol AnatDOI 10.1007/s00276-013-1194-1
What is the dorsal median sulcus of thespinal cord? Interest for surgical approachof intramedullary tumors
Timothée Jacquesson, NathalieStreichenberger, Marc Sindou, PatrickMertens & Emile Simon

1 23
Your article is protected by copyright and
all rights are held exclusively by European
Union. This e-offprint is for personal use only
and shall not be self-archived in electronic
repositories. If you wish to self-archive your
article, please use the accepted manuscript
version for posting on your own website. You
may further deposit the accepted manuscript
version in any repository, provided it is only
made publicly available 12 months after
official publication or later and provided
acknowledgement is given to the original
source of publication and a link is inserted
to the published article on Springer's
website. The link must be accompanied by
the following text: "The final publication is
available at link.springer.com”.
ORIGINAL ARTICLE
What is the dorsal median sulcus of the spinal cord? Interestfor surgical approach of intramedullary tumors
Timothee Jacquesson • Nathalie Streichenberger •
Marc Sindou • Patrick Mertens • Emile Simon
Received: 6 March 2013 / Accepted: 19 August 2013
� European Union 2013
Abstract
Purpose For intramedullary tumor (IMT) surgery, a bal-
ance has to be found between aggressively resecting the
tumor and respecting all the sensory and motor pathways.
The most common surgical approach is through the dorsal
median sulcus (DMS) of the spinal cord. However, the
precise organization of the meningeal sheats in the DMS
remains obscure in the otherwise well-described anatomy
of the spinal cord. A better understanding of this archi-
tecture may be of benefit to IMT surgeon to spare the spinal
cord.
Methods Three spinal cords were studied. The organiza-
tion of the spinal cord meninges in the DMS was described
via macroscopic, microsurgical and optical microscopic
views. A micro dissection of the DMS was also performed.
Results No macroscopic morphological abnormalities
were observed. With the operative magnifying lens, the
dura was opened, the arachnoid was removed and the pia
mater was cut to access the DMS. The histological study
showed that the DMS was composed of a thin rim of
capillary-carrying connective tissue extending from the pia
mater and covering the entire DMS. There was no true
space between the dorsal columns, no arachnoid or cross-
ing axons either.
Conclusion Our work indicates that the DMS is not a
sulcus but a thin blade of collagen extending from the pia
mater. Its location is given by tiny vessels coming from the
surface towards the deep. Thus, the surgical corridor has to
follow the DMS as closely as possible to prevent damage to
the spinal cord during midline IMT removal.
Keywords Spinal cord � Meninges � Dorsal media
sulcus � Intramedullary tumors
Introduction
The earliest example of spinal cord surgery may date to
1,549, when the French army surgeon Ambroise Pare
excised bony splinters compressing a spinal cord and
applied traction for spinal dislocations. Later, in 1887,
Horsley described the first removal of a spinal meningioma
[7]. Then, at the beginning of the twentieth century,
Cushing reported the first myelotomy to expose an inop-
erable intramedullary tumor (IMT) [3], and this was
quickly followed by the first cases of IMT removal [4, 10].
Today, IMT surgery, although still delicate, is performed
daily in neurosurgical centers. Excepting lateral or exo-
phitic tumors, the surgical approach of IMT is generally
done via the dorsal median sulcus (DMS), situated between
the two dorsal columns [5, 6]. IMT surgery often neces-
sitates a careful balance between aggressive resection of
the complete tumor and the respect of sensory-motor
pathways.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00276-013-1194-1) contains supplementarymaterial, which is available to authorized users.
T. Jacquesson (&) � M. Sindou � P. Mertens � E. Simon
Department of Neurosurgery, Hopital Neurologique Pierre
Wertheimer, 59 Bd Pinel, 69677 Bron, Cedex, France
e-mail: [email protected]
T. Jacquesson � P. Mertens � E. Simon
Department of Anatomy, University of Lyon1,
8 Avenue Rockefeller, 69003 Lyon, France
N. Streichenberger
Department of Pathology, Groupement Hospitalier Est,
59 Bd Pinel, 69677 Bron, Cedex, France
123
Surg Radiol Anat
DOI 10.1007/s00276-013-1194-1
Author's personal copy

Human spinal cord anatomy has long been well estab-
lished [2, 8, 21, 24]. The spinal meninges are quite similar
to those of the brain. Indeed, they include three main layers
enclosing the spinal central nervous system from the
foramen magnum to the sacrum. The outermost layer is the
dura mater, a single cylindrical sleeve enclosing the spinal
cord and its roots all along the spinal canal. Next is the
outer parietal arachnoid mater, which projects a series of
highly perforated intermediate sheets that envelope nerve
roots and vessels. These sheets are impermeable to cere-
brospinal fluid (CSF) and form the subarachnoid space.
The innermost layer is the pia mater, which covers the
entire spinal cord surface and supports arteries and nerves.
The term leptomeninges refers to the arachnoid and the pia
mater together, but excludes the dura mater [16, 23].
Despite the fact that spinal cord anatomy is generally
well known, and that IMT surgery has existed for quite a
long time, the precise architecture of the leptomeninges in
the DMS is currently poorly understood. The brain men-
ingeal barrier has been studied to understand blood-CSF
exchanges or tumor growth [13]. Furthermore, the ultra-
structure of cranial or spinal meninges has also been
recently studied, but the DMS or the anterior median sulcus
(AMS) has never been described at a histological scale [14,
15, 22, 23].
The DMS has been described differently in different
ways by different authors: a partition made of pia mater
[21]; a small intermediate sulcus that may be detectable on
the posterior surface [17]; a distinct median raphe, over
which the very tortuous posterior spinal vein runs [1]; or a
thin fibrous structure that dorsally separates the spinal cord
in two halves [19]. Also, the existence of a true deep sulcus
with meninges or a virtual space crossed by axons between
the dorsal columns is not formally established. In the
present study, we thus specifically studied the meninges in
the DMS to clarify knowledge of this anatomical feature
and to provide useful information for IMT removal.
Materials and methods
Samples
Three fresh cadavers were used in the Laboratory of
Anatomy of Lyon. One cervical spinal cord was used for
preliminary tests. Red latex was injected in the arteries of
another cervical spinal cord to provide a more complete
macroscopic view. Finally, an entire spinal cord was
sampled. The delay after death was inferior to 30 days and
formalin preparation was done on all bodies. To access the
spinal cord, the bodies were placed in a prone position and
posterior midline skin incisions from the occipital protu-
berance to the sacrum were done. Then, the paravertebral
muscles were retracted to expose the posterior arches and
to allow complete wide laminectomy. After sharp section
of the dural sac from C1 to S1 levels, the meninges were
carefully released from the posterior longitudinal ligament.
Then, the spinal cord with all the meninges and roots were
removed ‘‘en bloc’’. The samples were placed in a 4 %
formaldehyde bath for 15 days at room temperature to
obtain additional formalin fixation.
Macroscopic and operative study
First, orthogonal transversal sections were performed with
ultra fine razor blades at the cervical, thoracic and lumbar
levels, corresponding to the C2, C6, T4, T8 and L1 nerve
root exits. Using micro-surgical instruments, the dura
mater and parietal arachnoid layer were opened and fixed
with pins on a rigid plate. Then, under a 109 magnification
operating microscope, the microsurgical dissection of the
meninges and the DMS was performed, using scissors,
tweezers and spatulas to carefully separate the anatomic
structures. Secondly, another transversal section was per-
formed to precisely include the DMS opening site.
Histological study
Eight mm thick samples were included in a 30 9 25 9
10 mm box for a 4 % formaldehyde bath at room tem-
perature. After paraffin embedding and microtome sec-
tioning 10 microns thin, the samples were spread on a slide
and stained with Luxol Fast Blue—PAS. Analyses were
then performed by the pathologist using an optical micro-
scope at high magnification (209, 409 and 1009).
Latex injection
One cadaver head was cut at the C7 level, irrigated with
warm water to remove blood and fixed with formalin via
the neck vessels. Red latex was then injected in the internal
carotid and vertebral arteries (Aerographe Magenta acrylic
Fig. 1 Macroscopic view of the C7 spinal cord. Note the butterfly-
shaped gray matter
Surg Radiol Anat
123
Author's personal copy

ink pb15.2 Pebeo). After formalin fixation, the cervical
spinal cord was removed, thus providing a better view of
arterial supply.
Results
Macroscopic views
No macroscopic morphological abnormalities such as root
duplications, tumors or vascular malformations were
observed. Comfortable access to the posterior face of the
spinal cord was attained by pinning the dura open. Rootlets
and roots merged regularly on both sides. The spinal cord
measured 1 cm diameter in average and presented the
typical cervical and lumbar enlargements. The roots of the
cauda equina emerged normally from the terminal conus.
The denticulate ligament was stretched between the lateral
columns and the dura mater. The arachnoid mater covered
the entire spinal cord and hid the pia mater and vessels. The
tortuous posterior spinal vein was discernable along the
posterior midline surface and two dorsolateral arteries sent
Fig. 2 Microsurgical views. a Dissection of the arachnoid and the pia
maters using microsurgical scissors. b Presence of fibrous septa
between dorsal columns. c Separation of the posterior columns to
open the DMS. d Presence of multiple tiny vessels coming from the
surface and going deeply along the DMS. They could lead the surgeon
to find the DMS
Surg Radiol Anat
123
Author's personal copy

small perforating arteries laterally and toward the midline.
The gray matter, with its characteristic butterfly shape, was
visible at the inferior end of the sample, surrounded by the
white matter (Fig. 1).
Operative views
Using the operating microscope, the arachnoid bridging
tissues were cut to release the dura mater from the pia
mater. The deep arachnoid layer covering the pia mater
was then gently removed to preserve the underlying
structures. These later comprised a large number of very
small vessels covering the surface of the spinal cord. After
switching the spinal vein, a small trench, more or less
visible according to the location, was exposed exactly in
the middle of the posterior face of the spinal cord. Formalin
fixation maintains tissue consistency very close to those
in vivo. The pia mater, which carries all the vessels, was
then cut, thus allowing the spontaneous separation of the
two dorsal columns (Fig. 2a).
If it is not clearly seen, the pia mater may be incised
longitudinally and medially using the emergence of the
posterior roots, the two dorsolateral arteries or the bulging
of the dorsal columns as reference points. In our samples,
no true septum could be identified in the DMS, but there
were many small fibrous bridges connecting the two dorsal
columns (Fig. 2b). The dissection was conducted smoothly
to spare the white matter laterally (Fig. 2c). A deep vas-
cularized area, the ependyma, was ultimately reached.
Sulco commissural vessels from the anterior spinal artery
at the bottom of this last area were also visible. Tiny
arteries or veins on the walls of the DMS plunged deeply
coming from the surface (Fig. 2d). This meningeal archi-
tecture in the DMS was consistent throughout the spinal
cord, but less evident at the thoracic level. Indeed, DMS
dissection seemed easier at the cervical and lumbar
enlargements, where we found more landmarks or vessels.
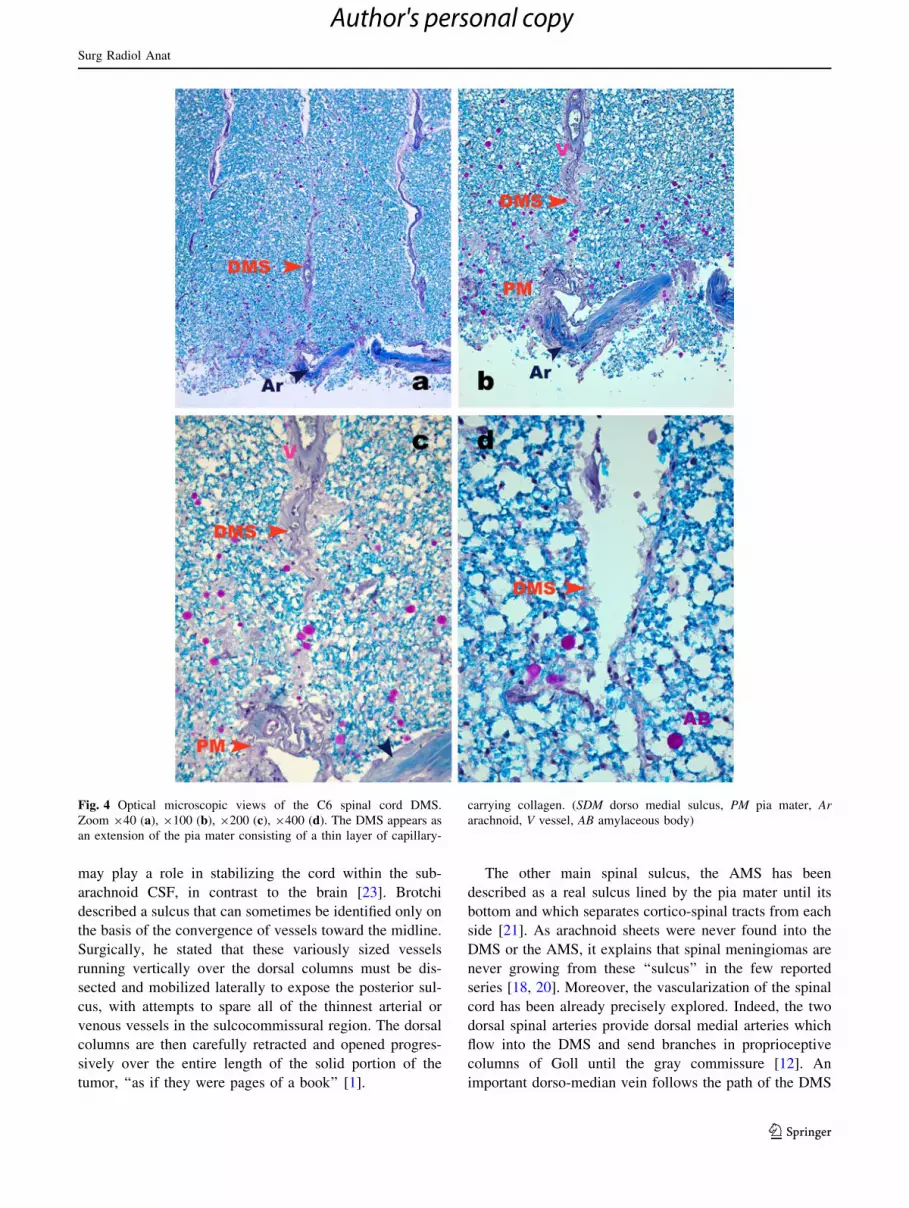
Histological study
Via histological examination with an optical microscope,
we found that the DMS presented as a single layer between
the dorsal columns (Fig. 3). In the AMS by contrast, there
was a real open space surrounded by pia and arachnoid
maters. Under higher magnification, we identified a thin
rim of conjunctive tissue that covered the columns
throughout the DMS, but did not cover the ependyma. No
arachnoid or subarachnoid space was found. In our sam-
ples, the DMS appeared to be an extension of the pia mater
comprising a narrow layer of collagen and small capillaries
(Fig. 4). Laterally, the white matter contained axons for
sensory pathways but none crossed the DMS. There were
no neuronal cell bodies, but oligodendrocytes and
astrocytes were present. There were also degenerative,
amylaceous bodies (stained red). The ‘‘dorsal intermedio-
lateral sulci’’ appeared as empty spaces also covered by pia
like the DMS.
The surgical pathway followed the DMS, but some
white fibers were damaged and, in several samples, the
dissection exceeded the ependyma, reaching the AMS.
The histological architecture of the DMS was preserved,
albeit with slight variations, along the entire spinal cord.
At the cervical and lumbosacral levels, we noted that in
some samples, a layer of pia mater entered partially into
the DMS. At the thoracic level, the DMS was less rec-
ognizable and there were several dorsolateral sulci with
septa formed from the pia mater as in the DMS (Fig. 5).
The septa at this last level could not be followed
throughout the DMS, which suggests that they were
discontinuous.
Discussion
The history of spinal meninges studies starts at end of the
nineteenth century with the works of Key and Retzius [9].
Different authors have referred to the DMS as ‘‘the septum
arachnoidale’’, ‘‘septum intermedium’’, or ‘‘septum lep-
tomeningeum dorsale’’. Samii described the DMS as a
septum along the posterior midline, attached to the pia
mater of the spinal cord. For the author, the DMS runs from
the cervical to the lower thoracic region [19]. Weller
described a substantial layer of subpial collagen separating
the pia mater from the glia limitans on the surface of the
spinal cord. He went on to say that this layer of subpial
collagen attaches to the dura via the dentate ligament and
Fig. 3 Optical Microscopic view of C6 spinal cord axial section.
Zoom 920. An example of spinal cord sample as it was embedded
with its dura sleeve, rootlets and arachnoid sheets. (DMS dorso medial
sulcus, Ar arachnoid, DM dura mater, R rootlet)
Surg Radiol Anat
123
Author's personal copy
may play a role in stabilizing the cord within the sub-
arachnoid CSF, in contrast to the brain [23]. Brotchi
described a sulcus that can sometimes be identified only on
the basis of the convergence of vessels toward the midline.
Surgically, he stated that these variously sized vessels
running vertically over the dorsal columns must be dis-
sected and mobilized laterally to expose the posterior sul-
cus, with attempts to spare all of the thinnest arterial or
venous vessels in the sulcocommissural region. The dorsal
columns are then carefully retracted and opened progres-
sively over the entire length of the solid portion of the
tumor, ‘‘as if they were pages of a book’’ [1].
The other main spinal sulcus, the AMS has been
described as a real sulcus lined by the pia mater until its
bottom and which separates cortico-spinal tracts from each
side [21]. As arachnoid sheets were never found into the
DMS or the AMS, it explains that spinal meningiomas are
never growing from these ‘‘sulcus’’ in the few reported
series [18, 20]. Moreover, the vascularization of the spinal
cord has been already precisely explored. Indeed, the two
dorsal spinal arteries provide dorsal medial arteries which
flow into the DMS and send branches in proprioceptive
columns of Goll until the gray commissure [12]. An
important dorso-median vein follows the path of the DMS
Fig. 4 Optical microscopic views of the C6 spinal cord DMS.
Zoom 940 (a), 9100 (b), 9200 (c), 9400 (d). The DMS appears as
an extension of the pia mater consisting of a thin layer of capillary-
carrying collagen. (SDM dorso medial sulcus, PM pia mater, Ar
arachnoid, V vessel, AB amylaceous body)
Surg Radiol Anat
123
Author's personal copy

but appears often sinuous or discontinuous. So, this dorsal
vein is not a fiable landmark of the dorsal midline. Finally,
because of the somatotopic organization inside the dorsal
column described by Kahler, the sensory fibers coming
from the lumbosacral area are the more medial fibers in the
funiculus. Also, they are preferentially exposed to vessel
damages during the surgical approach through the DMS.
Thus, this vascular lesion could be responsible for the
lumbosacral proprioceptive symptoms.
In the present work, we shed new light on the anatomy
of the spinal meninges and provide potentially useful
information for preoperative planning in IMT removal. Our
macroscopic, operative and histological study was
designed to mimic the point of view of the surgeon and the
pathologist. We performed micro-dissection of the DMS
with visual and tactile information close to that encoun-
tered in the most frequent approach to IMT surgery.
Indeed, our findings suggest that the surgical path has to be
precisely through the DMS; the gentle spacing of the dorsal
columns is vital to sparing the white matter and nerve
functions. Our assessment of the entire spinal cord con-
firmed that the architecture of the DMS is quite similar at
the cervical and lumbosacral levels. Some authors report
that the anterior spinal artery is not continuous and there
exists a critical narrow zone for the vascularization in the
midthoracic region [11]. We noticed that, at this last level,
the organization of the meninges was less homogeneous.
This may be due to poorer blood supply in the DMS. In
contrast, the cervical and lumbosacral levels had the same
meninges anatomy. In a few samples, we found that the pia
mater even fed the DMS superficially.
Cut artifacts can affect the analysis of histological
samples. To best manage this issue, we used ultra fine razor
blades to achieve the most orthogonal cutting plane as
possible. Luxol Fast Blue was used in our study to differ-
entiate white matter, gray matter, leptomeninges or blood
vessels. We also tried staining with silver or periodic acid-
Schiff but these provided no additional information.
Fig. 5 Optical microscopic views. a, b A small piece of pia mater
extending into the DMS in D12 spinal cord (orange narrow);
Zoom 920 and 9100. c The DMS is not homogeneous. The ‘‘dorsal
intermediolateral sulci’’ between dorsal columns have ‘‘DMS like’’
structures in D8 spinal cord (orange narrow); Zoom 940. d C6 spinal
cord after DMS dissection showing that the adjacent white fibers of
the dorsal columns can be endangered by surgical opening of the
DMS (orange narrow); Zoom 912 (color figure online)
Surg Radiol Anat
123
Author's personal copy

Obviously, the conditions encountered during surgery will
be more complex than those of our research setting. Indeed,
the anatomical changes induced by the IMT itself may
make its surgical removal more complex. Micro-surgical
dissection is furthermore surgeon-dependent; the ability to
save white fibers grows with the surgeon’s experience.
Finally, we do wish to underline that our study was per-
formed on only a few samples and thus the significance of
our conclusions is limited. Our protocol will need to be
repeated in larger studies to confirm the present findings.
Conclusions
Unlike the variable organization of the meninges in the
DMS described in the literature, our work indicates that the
DMS is not a sulcus but a septum or a raphe which appears
as a thin blade of capillary-carrying collagen that extends
from the pia mater, tightly separates the dorsal columns
and goes deeply to—but excludes—the ependyma. Fur-
thermore, we found no arachnoid, no true space between
the dorsal columns and no crossing axons. The tiny vessels
coming from the surface has to be considered as Ariane’s
threads finding the way for the surgeon to the ‘‘dorsal
median septum’’. Thus, the surgical corridor in midline
IMT removal has to follow the DMS as closely as possible
to prevent damage to the spinal cord.
Acknowledgments We thank Prof Sindou who was at the origin of
this work. We thank the technical staff of the pathology laboratory for
their preparation of samples prior to histological analyses. We thank
K. Erwin for proofreading the English article.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Brotchi J (2002) Intrinsic spinal cord tumor resection. Neuro-
surgery 50:1059–1063
2. Cajal SR (1894) Les nouvelles idees sur la structure du systeme
nerveux chez l’homme et chez les vertebres. Paris
3. Cushing H (1905) The special field of neurosurgery. Bulletin of
the Johns Hopkins Hospital, Baltimore, pp 77–87
4. Elsberg CA (1912) Surgery of intramedullary affections of the
spinal cord: anatomical basis and technique. JAMA 59:1532–
1536
5. Fischer G, Brotchi J (1994) Les tumeurs intramedullaires. Societe
de Neuro-Chirurgie de Langue Francaise, 45eme Congres Ann-
uel. Angers, 12-15 juin 1994. Neurochirurgie 40(Suppl 1):1–108
6. Fischer G, Mansuy L (1980) Total removal of intramedullary
ependymomas: follow-up study of 16 cases. Surg Neurol 14:243–249
7. Gowers R, Horsley V (1888) A case of tumour of the spinal cord.
Removal; recovery. Med Chir Trans 53:377–428
8. Hirschfeld L (1865) Traite et iconographie du systeme nerveux et
des organes des sens de l’homme. Paris Masson
9. Key EAH, Retzius MG (1876) Studien der Anatomie des
Nervensystems und des Bindegewebes. Stockholm Samson
Wallin, Stockholm
10. Krause F (1908) Erfahrungen bei 26 operativen Fallen von
Ruckenmarkstumoren mit Projektionen. Dtsch Z Nervenheilkd
36:106–113
11. Lazorthes (1973) Vascularisation et circulation de la moelle
epiniere. Paris Masson
12. Lazorthes G, Gouaze A, Zadeh JO, Santini JJ, Lazorthes Y,
Burdin P (1971) Arterial vascularization of the spinal cord.
Recent studies of the anastomotic substitution pathways. J Neu-
rosurg 35:253–262
13. Lescanne E, Velut S, Lefrancq T, Destrieux C (2002) The internal
acoustic meatus and its meningeal layers: a microanatomical
study. J Neurosurg 97:1191–1197
14. Mertens P, Guenot M, Hermier M, Jouvet A, Tournut P, Froment
JL, Sindou M, Carret JP (2000) Radiologic anatomy of the spinal
dorsal horn at the cervical level (anatomic-MRI correlations).
Surg Radiol Anat 22:81–88
15. Nauta HJ, Dolan E, Yasargil MG (1983) Microsurgical anatomy
of spinal subarachnoid space. Surg Neurol 19:431–437
16. Nicholas DS, Weller RO (1988) The fine anatomy of the human
spinal meninges. A light and scanning electron microscopy study.
J Neurosurg 69:276–282
17. Nieuwenhuys R (1978) The human central nervous system.
A Synopsis and Atlas. Springer, Heidelberg
18. Roux FX, Nataf F, Pinaudeau M, Borne G, Devaux B, Meder JF
(1996) Intraspinal meningiomas: review of 54 cases with dis-
cussion of poor prognosis factors and modern therapeutic man-
agement. Surg Neurol 46:458–463
19. Samii M, Keklamp J (2007) Surgery of spinal tumors. Springer,
Baltimore, p 526
20. Sandalcioglu IE, Hunold A, Muller O, Bassiouni H, Stolke D,
Asgari S (2008) Spinal meningiomas: critical review of 131
surgically treated patients. Eur Spine J 17:1035–1041
21. Testut L (1911) Traite d’Anatomie Humaine. Systeme nerveux
central. Octove Doin, Paris
22. Vandenabeele F, Creemers J, Lambrichts I (1996) Ultrastructure
of the human spinal arachnoid mater and dura mater. J Anat
189(Pt 2):417–430
23. Weller RO (2005) Microscopic morphology and histology of the
human meninges. Morphologie 89:22–34
24. Dejerine J (1980) Anatomie des centres nerveux. Paris Masson
Surg Radiol Anat
123
Author's personal copy





























