Embed Size (px)
Citation preview

ORIGINAL ARTICLE DOI:10.1111/j.1365-2303.2010.00761.x
Survey of medical training in cytopathology carried out by thejournal Cytopathology
Anshu1, A. Herbert2, B. Cochand-Priollet3, P. Cross4, M. Desai5, R. Dina6, J. Duskova7,
A. Evered8, A. Farnsworth9, W. Gray10, S. S. Gupta11, K. Kapila12, I. Kardum-Skelin13,
V. Kloboves-Prevodnik14, T. K. Kobayashi15, H. Koutselini16, W. Olszewski17, B. Onal18,
M. B. Pitman19, Z. Marinsek20, T. Sauer21, U. Schenck22, F. Schmitt23, I. Shabalova24,
J. H. F. Smith25, E. Tani26, L. Vass27, P. Vielh28 and H. Wiener29
1Mahatma Gandhi Institute of Medical Sciences, Sevagram, India, 2Department of Cellular Pathology, Guy�s & St Thomas NHS
Foundation Trust, St Thomas� Hospital, London, UK, 3Service d�Anatomie et Cytologie Pathologiques, Hopital Lariboisiere, Paris,
France, 4Department of Pathology, Queen Elizabeth Hospital, Gateshead, UK, 5Manchester Cytology Centre, Manchester Royal
Infirmary, Manchester, UK, 6Histopathology Department, Imperial College NHS Trust, Hammersmith Hospital, London, UK,7Institute of Pathology, 1st Faculty of Medicine, Charles University, Prague, Czech Republic, 8Cervical Screening Wales and
University of Wales Institute, Cardiff, Wales, 9Douglass Hanly Moir Pathology Cytology, Macquarie Park, New South Wales,
Australia, 10John Radcliffe Hospital, Oxford, England, 11Department of Community Medicine, Mahatma Gandhi Institute of
Medical Sciences, Sewagram, India, 12Cytopathology Unit, Department of Pathology, Faculty of Medicine, Kuwait University,
Kuwait, 13Laboratory for Cytology and Haematology, Merkur University Hospital, Zagreb, Croatia, 14Department of
Cytopathology, Institute of Oncology, Ljubljana, Slovenia, 15Pathology Department, Saiseikai Shiga Hospital, Imperial Gift
Foundation Inc, Shiga, Japan, 16Department of Cytopathology, Aretaieion University Hospital, University of Athens Medical
School, Athens, Greece, 17Department of Pathology, Institute of Oncology, Warsaw, Poland, 18Department of Cytology
&Pathology, Ankara Diskapi Training & Research Hospital, Ankara, Turkey, 19Department of Pathology, Massachusetts General
Hospital, Harvard Medical School, Boston, Massachusetts, USA, 20Department of Cytopathology, Institute of Oncology,
Ljubljana, Slovenia, 21Department of Pathology, Ulleval University Hospital, Oslo, Norway, 22Institute of Pathology, Technical
University of Munich, Germany, 23IPATIMUP and Medical Faculty of Porto University, Porto, Portugal, 24General Institute of
Advanced Medical Studies, Moscow, Russia, 25Department of Histopathology & Cytology, Royal Hallamshire Hospital, Sheffield,
UK, 26Department of Pathology and Cytology, Karolinska University Hospital, Solna, Stockholm, Sweden, 27Department of
Pathology ⁄ Cytopathology, Flor F. University Hospital of Pest County, Kistarcsa, Hungary, 28Department of Pathology, Institut
Gustave Roussy, Villejuif, France and 29Clinical Department of Pathology, Medical Unversity Vienna, Vienna, Austria
Accepted for publication 26 February 2010
Anshu, A. Herbert, B. Cochand-Priollet, P. Cross, M. Desai, R. Dina, J. Duskova, A. Evered, A. Farnsworth,
W. Gray, S. S. Gupta, K. Kapila, I. Kardum-Skelin, V. Kloboves-Prevodnik, T. K. Kobayashi,
H. Koutselini, W. Olszewski, B. Onal, M. B. Pitman, Z. Marinsek, T. Sauer, U. Schenck, F. Schmitt,
I. Shabalova, J. H. F. Smith, E. Tani, L. Vass, P. Vielh and H. Wiener
Survey of medical training in cytopathology carried out by the journal Cytopathology
This report of the Editorial Advisory Board of Cytopathology gives the results of a survey of medical practitioners
in cytopathology, which aimed to find out their views on the current situation in undergraduate and
postgraduate training in their institutions and countries. The results show that training in cytopathology and
histopathology are largely carried out at postgraduate level and tend to be organized nationally rather than
locally. Histopathology was regarded as essential for training in cytopathology by 89.5% of respondents and was
Correspondence:
Dr A. Herbert, Department of Cellular Pathology, Second
Floor North Wing, St Thomas� Hospital, London, UK
Tel: +44(0)20 7188 2926; Fax: +44(0)20 7401 3661;
E-mail: [email protected]
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd 147

mandatory according to 83.1%. Mandatory cytopathology sections of histopathology were reported by 67.3%
and specific examinations in cytopathology by 55.4%. The main deficiencies in training were due to its
variability; there were insufficient numbers of pathologists interested in cytology and a consequent lack of
training to a high level of competence. Pathologists without specific training in cytopathology signed out cytology
reports according to 54.7% of responses, more often in centres where training was 3–6 months or less duration.
Although 92.2% of respondents thought that specialist cytology should not be reported by pathologists without
experience in general cytopathology, that practice was reported by 30.9%, more often in centres with small
workloads. The survey report recommends that 6–12 months should be dedicated to cytopathology during
histopathology training, with optional additional training for those wanting to carry out independent practice in
cytopathology. Formal accreditation should be mandatory for independent practice in cytopathology. When
necessary, temporary placements to centres of good practice should be available for trainees intending to practise
independently in cytopathology. There should be adequate numbers of pathologists trained in cytopathology to a
high level of competence; some of their time could be released by training cytotechnologists and trainee
pathologists to prescreen cytology slides and assess adequacy of fine-needle aspiration samples when immediate
diagnosis was not required. The survey demonstrated a clear need for European and international guidelines for
training in cytopathology.
Keywords: medical training in cytopathology, international survey, accreditation, postgraduate training,
cytopathology examinations
Introduction
Members of the Editorial Advisory Board and many
of their colleagues were conscious that there might be
problems in training pathologists in the clinically
diverse speciality of cytopathology at a time when
fine-needle aspiration (FNA) cytology should be
developing rapidly to support new methods of spec-
imen procurement1 and exfoliative cytology contin-
ues to play an important role in patient management
and screening.2 In many places with active cervical
screening programmes time dedicated to �non-gynae-
cological� cytopathology may be compromized by
increasing demands from workload and quality con-
trol in cervical cytology.3 Now that cervical screening
is likely to be modified (especially in its volume) by
human papillomavirus testing4 and vaccination,5
non-gynaecological cytopathology should flourish,
but only if teaching and training are available to a
high standard. Our observations take account of the
Bologna principles6 for higher education and training
and should be considered by the European Union of
Medical Specialists (UEMS), with which the Euro-
pean Federation of Cytology Societies (EFCS) and
European Society of Pathology have both been
working.
The aims of this survey were directed at specialists
practising in cytopathology to elicit their views
on the current situation in undergraduate and
postgraduate teaching and training in cytopathology
in their countries and institutions. We aimed to find
out what they regarded as the essentials of good
training, what were thought to be examples of good
practice and what were deficiencies in training. We
also aimed to link these training practices to con-
sultant pratice and laboratory workloads in the insti-
tutions from which responses were received. Finally,
we aimed to publish the results of this survey as an
evidence-base for those wanting to improve cytopa-
thology training in Europe and elsewhere in the
world. Our aims are consistent with those of the
Bologna declaration for higher education and train-
ing, recognizing the need for common reforms and
coordinated action with comparable and compatible
criteria for education and practice.8
Methods
A draft questionnaire was discussed and validated at
the Cytopathology Editorial Advisory Board meeting
in June 2008. It included both closed- and open-
ended questions. The survey questionnaire was
uploaded onto an online survey site (http://www.
surveymonkey.com) and the link was circulated to
representatives of cytology societies by email with
an appeal to circulate it widely. Among other
medical practitioners in cytopathology, survey
respondents included members of the Advisory and
Anshu et al.148
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

Management Boards of Cytopathology, representatives
of societies affiliated to Cytopathology and officers of
member societies of the EFCS. The survey was
advertised on the EFCS website (http://www.
efcs.eu), which proved to be a useful site for this
type of communication.
The survey was divided into five parts: (1) curric-
ulum design, (2) undergraduate training, (3) post-
graduate training, (4) assessment of training and
(5) consultant workloads and practice in cytopathol-
ogy. All analyses were calculated for total respondents
and countries as a whole and where relevant both
analyses are presented.
Chi-square test was used as a test of significance
to compare difference between proportions. Statcalc
calculator in the EPI INFO 6 software was used for
calculation of Chi-square tests.
Results
We received responses from 76 individuals from 26
countries including: Australia, Canada, Chile, Croatia,
the Czech Republic, Denmark, France, Greece, India,
Italy, Kuwait, New Zealand, Norway, Portugal, Roma-
nia, Russia, Singapore, Slovenia, Spain, Sudan,
Sweden, Switzerland, Turkey, the United Kingdom
(UK), Uruguay and the USA (Figure 1). There was a
single respondent from each of 15 countries, two from
six countries, three from four and seven from one. As it
was not mandatory to reveal personal details in the
survey questionnaire, 27 respondents did not provide
details of position or place of work and not all
respondents answered all the questions. Respondents
had received training in cytology from 27 different
countries, all except one in the country where they
practised.
Curriculum design
Of 69 responses, 46 (66.7%) said that the medical
school curriculum was designed at national level. The
curriculum was designed at regional level according to
nine (13.0%), while according to 14 (20.3%) it was
designed at the level of the individual institution,
where schools had the freedom to tailor their curric-
ulum according to their needs. Conventional learning
was said to be used by 46 (66.7%) medical schools,
while 16 (23.2%) followed a horizontally or vertically
integrated curriculum. In 15 (21.7%) schools, prob-
lem-based learning was used. In six schools there was
a combination of conventional and problem-based
learning and two had all three forms of curricula.
Undergraduate training
Organization of undergraduate teaching Nine of 68
(13.2%) respondents said that cytopathology was
included as a defined course in the medical curricu-
lum while 59 (86.8%) said it was not a defined course.
Of the nine respondents who said that their schools
had cytopathology as a defined course, the duration of
that course was less than a year in six, 1–2 years in
two and more than 2 years in one school. Four
respondents who said that cytopathology was not a
defined course said that the subject was taught for less
than a year. On the other hand, histopathology was
included as a defined course in the medical curricula
of 53 of 70 (75.7%) respondents� countries. Of the 53
respondents who said that histopathology was a
defined course, 18 (33.9%) said that the modules
lasted less than a year. Nineteen (35.8%), six
(11.3%) and five (9.4%) respondents said that
courses lasted 1 year, 2 years and 3 or more years,
respectively, while five of them did not specify the
duration of the course. These percentages were
similar in replies for 26 named countries as a whole,
where cytopathology was not a defined course in
their undergraduate curriculum in 21 (80.8%), but
histopathology was a defined course in the curricu-
lum in 17 (65.4%). Responses varied among respon-
dents in 11 countries.
Histopathology was included as part of multi-
disciplinary clinical teaching sessions in 40 (59.7%)
of 67 respondents� medical schools. Of these 40,
histopathology was included in the teaching sessions
Figure 1. Map showing distribution of respondents across
the world.
Survey of medical training in cytopathology 149
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

after the third year in 22 (55.0%) of the respon-
dents� medical schools, in the third year in 13
(32.5%), in the second year in three (7.5%) and in
the first year in two (5.0%). Cytopathology was
used in the clinical teaching modules in 33 (49.3%)
of 67 respondents� medical schools. Respondents
reported including cytopathology training in several
other formats at the undergraduate level. Most
medical schools included cytopathology in lectures
but not in practical training.
Several respondents reported that cytopathology
was taught as part of the pathology-histopathology
course, eight respondents reported that it was
included as part of the gynaecology course and one
respondent each reported that it was taught during
the medical, surgical and radiation oncology or inter-
nal medicine course. In two schools cytopathology
was offered as an optional subject or taught only
when it came up as part of a systemic course or case
discussion.
Postgraduate training
Organization of postgraduate training Of 63 replies to
the question, 76.2% said that postgraduate training
was organized at a national level (in four of these it
was also regional, institutional or both), 1.6% said it
was at a regional level, 20.6% said it was institutional
and 1.6% said �other�. Cytopathology was integrated
into histopathology training according to 50 (79.4%),
of whom 58.0% said that exposure was continuous.
These percentages were similar in replies for 26
named countries, of which 76.9% said organization
was national (four of these recorded institutional
organization as well), 69.2% said that cytopathology
was integrated into routine histopathology training
and 50% of those had continuous exposure.
Time dedicated to cytopathology training Of 60 replies to
this question, 44 (73.3%) said there was a defined
time for cytopathology training. Twenty-four (40.0%)
said the defined time for cytopathology training was
6–12 months or more, 20 (33.3%) said training lasted
for 3–6 months or less while 16 (26.7%) said there
was no defined time dedicated to training. Defined
time varied when there was more than one response
from the same country, probably because trainees in
some centres were able to undertake specialist train-
ing. Thus, in 26 named countries responses were
variable in nine; five said the defined time for
cytopathology was 6–12 months or more, five said
3–6 months or less and six reported no defined time.
This contrasted with histopathology training, which
70.7% of 58 respondents said was for more than
3 years and 86.2% for at least 2–3 years; in 26 named
countries, 69.2% reported histopathology training for
more than 3 years and 88.5% for at least 2–3 years.
There were 51 individual responses concerning the
year of histopathology training during which cytopa-
thology started, but there was either no response or
they varied in 12 (46.3%) of 26 countries. Responses
were not significantly different between the first year
(15, 29.4%), second year (19, 37.3%) and final year
(17, 33.3%). Cytopathology training was separate
from histopathology training according to 58.9% of 56
replies.
Histopathology as a requirement for cytopathology
training Ten (16.9%) of 59 respondents said that it
was possible to train in cytopathology without histo-
pathology while 49 (83.1%) said it was not. Five of
those 10 answering �yes� to this question mentioned
non-medical degrees as criteria for entry into training.
An open question as to whether histopathology
training was essential for cytopathology elicited a
positive response in 89.5% of 57 replies. Two others
said it was essential �to a certain level, especially for
non-gynaecological cytology� and one said it was
�not essential but very, very useful�. Only one
response, from a laboratory with non-medical gradu-
ates training in cytopathology, said �unfortunately,
not�. Gynaecologists, haematologists, microbiologists,
oncologists and �doctors during specialist education�were able to train in cytopathology according to seven
free-text responses. In four of these they also trained
in histopathology. According to one response, limited
responsibility was given to peumonologists and
neurologists to report cytology.
Cytology practice during training Trainees were more
likely to screen unmarked gynaecological (87.7%) or
non-gynaecological (85.7%) slides and prepare their
own draft reports (89.1%) than they were to attend
rapid on-site evaluation of slides (71.7%), carry out
their own FNAs (67.9%) or sign out reports at a
defined stage of training (36.4%) (Table 1). The
trend was more pronounced in responses combined
for named countries as a whole. Non-medical cytol-
ogists contribute to cytology training of medical
trainees in 16 (61.5%) countries.
Examples of good practice given as free-text com-
ments focused on (1) additional specialist training
Anshu et al.150
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

(n = 10), (2) good local departments and enthusiasm
of cytopathologists (n = 9), (3) formal specialist
courses, examinations and accreditation (n = 8), (4)
interaction with clinical teams (n = 6), (5) practice
and hands-on experience under supervision (n = 5)
and (6) training along with histopathology (n = 5).
Others (n = 3) said what good training �should be� and
one mentioned improvement in gynaecological cyto-
pathology training after a national screening debacle.
There were no responses to this question from 30 of
76 respondents. Some respondents mentioned more
than one of these features as in the quotation in the
text box below. There was no correlation between
these broad groups of responses about good practice
and size of workload or time dedicated to cytopathol-
ogy training.
An example of good practice in training
• ‘‘Connection with other clinicians
(gynaecologists, haematologists, oncologists)
• active participation in FNA
• direct contact with patients
• participation in treatment planning
• training in histopathology.
All of these are contained in a 3-year programme
of independent training (specialisation) in clinical
cytology.’’
Examples of deficiency in training focused on (1)
lack of experienced cytopathologists in many centres
(several said that most pathologists were not inter-
ested in cytology) and variability of training (n = 9),
(2) lack of specific cytopathology training or time for
that training (n = 9), (3) lack of equipment, facilities
and time for overworked cytopathologists (n = 8), (4)
the need for better integration of cytopathology with
histopathology (n = 5), (5) lack of training to a high
level of competence (n = 4) and (6) neglect of gynae-
cological cytology (n = 2) or it being not available
when cervical cytology was centralized (n = 1). Single
respondents mentioned the problem of cyto-
pathology ⁄ histopathology subspecialization, the need
for standardized terminology, lack of government and
clinicians� awareness of biomedical scientist (cytotech-
nologist) ⁄ pathologist interaction. Four replies made
no specific points and 30 of 76 respondents did not
answer this question.
Lack of equipment, facilities and time for over-
worked cytopathologists were related to centres with
6–12 months or more of training in cytopathology
(seven of eight responses). Problems with integrating
cytopathology into histopathology and lack of training
to a high level of competence were related to centres
with no defined time or 3–6 months or less dedicated
to cytopathology training (four of four and five of five
comments in those categories, respectively). There
was no correlation between these responses and size
of workload.
Examples of deficiencies in training
• ‘‘Insufficient time to gain experience’’
• ‘‘Insufficient numbers of pathologists with an
interest in cytopathology to provide training’’
• ‘‘It is a �desert island� from where it ought to be
easy to go to Europe for homogenous
guidelines rather than aiming for local or even
national initiatives’’
Table 1. Trainee practice and examinations in cytopathology
Training practice
All responses
(maximum 77)
26 countries
(*one no response)
Yes No
Total Yes No Yes & noResponse rate 67.5–75.3%
Screen unmarked gyn slides 50 (87.7) 7 (12.3) 57 22 (84.6) 4 (15.4)
Screen unmarked non-gyn slides 48 (85.7) 8 (14.3) 56 19 (73.1) 3 (11.5) 4 (15.4)
Prepare draft reports 49 (89.1) 6 (10.9) 55 21 (80.8) 3 (11.5) 2 (7.7)
Attend rapid assessment FNAs 40 (71.7) 16 (28.6) 56 13 (50.0) 9 (34.6) 4 (15.4)
Carry out FNAs 38 (67.9) 18 (32.1) 56 14 (53.8) 9 (34.6) 3 (11.5)
Sign out reports at defined time
in training*
20 (36.4) 35 (63.6) 55 5 (19.2) 14 (53.8) 6 (23.1)
(n) = percentage.
gyn, gynaecology; non-gyn, non-gynaecological; FNA, fine needle aspirate.
Survey of medical training in cytopathology 151
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

Assessment of Training
Mandatory examinations in pathology exist in 45
(81.8%) of 55 respondents� countries. Cytopathology
is a mandatory section of the histopathology post-
graduate examination in 35 of 52 (67.3%) of the
respondents� settings. Of 55 respondents, 31 (56.4%)
said that there were no separate postgraduate examin-
ations in cytopathology. According to 32 (58.2%) of 55
responses a specialist cytopathology examination was
not required for independent practice in cytopathology.
A mandatory pathology qualification (histopathol-
ogy ⁄ cytopathology) exists in 49 (89.1%) of 55
respondents� countries. These degrees are awarded
by national, regional or institution-based agencies.
Certain overseas qualifications (such as MRCPath)
were not accepted in the work settings of 28 (51.9%)
of 54 respondents.
Cytopathology workloads and consultant reporting practice
Cytopathology workloads The variation in workloads
(defined by number of specimens received per year) of
gynaecological cytology, FNA and exfoliative cytology
handled by 42 and 46 respondents who gave infor-
mation about their laboratories is shown in Table 2.
For purposes of analysis, non-gynaecological cytology
workloads have been divided into small (< 1 000 tests
per year), medium (1 000–5 000 tests per year) and
large (> 5 000 tests per year). For analysis, gynaecol-
ogy laboratories have been divided into those above
and below 10 000 tests per year. Workloads for FNAs
and exfoliative cytology varied from below 100 to
25 000 requests per year. Cervical cytology workloads
varied from 100–500 to 200 000 requests per year;
those defined as �large� processed a range of 13 000–
200 000 with an average of 38 000 per year. The
balance in terms of large, medium and small labora-
tories is shown in Table 2.
Consultant reporting practice Of 55 respondents, 87.3%
said that cytopathologists attend multidisciplinary
meetings and contribute to clinical decisions on
patient management. Pathologists without specific
training in cytopathology sign out cytopathology
reports according to 54.7% of 53 responses. Patholo-
gists report specialized cytology for a particular system
without experience in general cytopathology accord-
ing to 30.9% of 55 responses. Medical practitioners
from other specialties report cytopathology according
to 15.1% of 53 responses and non-medical cytologists
report non-gynaecological cytology according to
16.3% of 49 responses. These percentages are shown
in Tables 3–5. According to 48.1% of 54 responses,
non-medical staff report cervical cytology.
According to 51 free-text replies, 92.2% thought
that experience in general cytopathology was essential
for specialist cytopathology reporting while three
thought it should be essential and only one thought
it should not. According to 61.5% of 53 free-text
replies, non-pathologists should not report cytopa-
thology. Nine respondents (17.3%) thought that
�trained and certified technicians� could report in areas
with many normal cases such as the cervix, sputum
and urine. Two (3.8%) gave an unqualified �yes� to
this question and four (7.6%) said �yes� if correctly
trained and with the supervision of a cytopathologist.
Two said that gynaecologists may report cervical
cytology. There was little mention of cervical screen-
ing cytology in these free-text responses, which did
not reflect the widespread practice of non-medical
staff reporting and signing out such cytology.
Who should report cytopathology?
• ‘‘I personally favour cytopathologists signing out,
particularly abnormal gynaecological cytology
and general cytology, because there is often
�value added� by a clinical perspective on the
cellular pattern.’’
• ‘‘Specially trained medical technicians do a very
good job as screeners in cytopathology and also
relieve the pathologists of a large load of
normal ⁄ negative smears and reporting.’’
Correlation between reporting practice, training and
workload Tables 3–5 show the reporting practice of
(1) specialists with no general cytopathology experi-
ence, (2) general pathologists with no specific training
in cytopathology, (3) non-pathologist medical practi-
Table 2. Workloads reported by respondents
Tests per year Gynaecology FNA
Exfoliative
cytology
< 1 000 2 11 10
1 000–5 000 8 19 17
5 000–10 000 6 14 15
10 000+ 26 2 4
Total responses to
the question
42 46 46
Anshu et al.152
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd
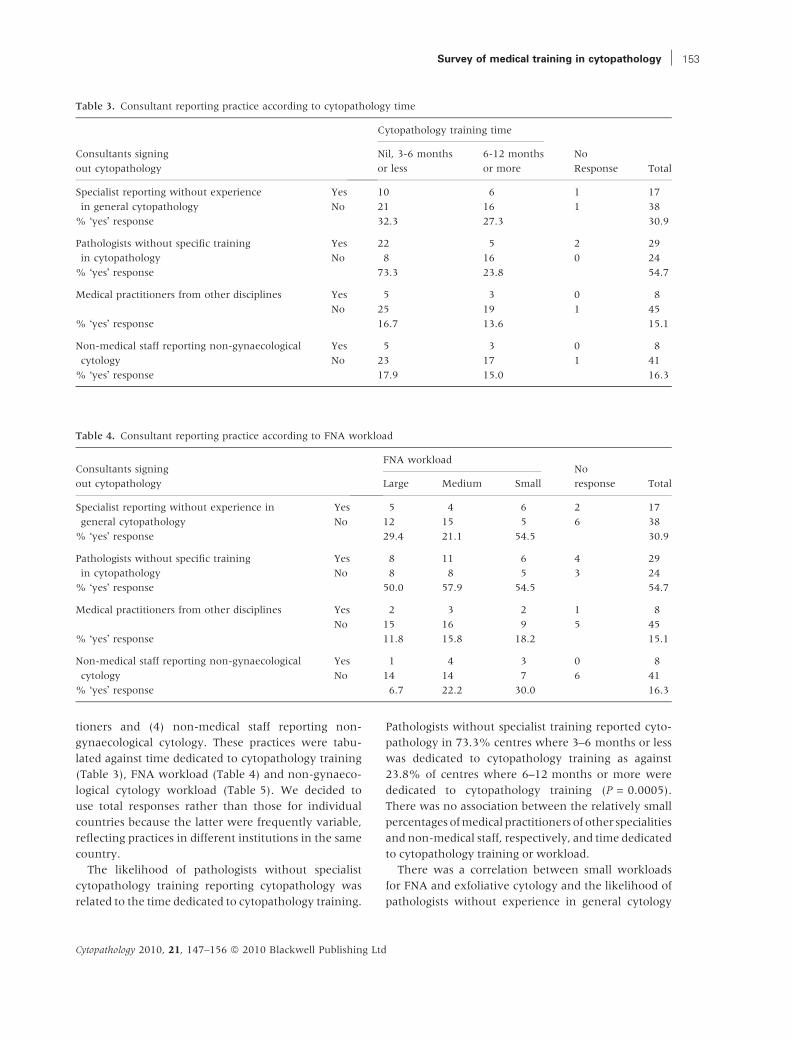
tioners and (4) non-medical staff reporting non-
gynaecological cytology. These practices were tabu-
lated against time dedicated to cytopathology training
(Table 3), FNA workload (Table 4) and non-gynaeco-
logical cytology workload (Table 5). We decided to
use total responses rather than those for individual
countries because the latter were frequently variable,
reflecting practices in different institutions in the same
country.
The likelihood of pathologists without specialist
cytopathology training reporting cytopathology was
related to the time dedicated to cytopathology training.
Pathologists without specialist training reported cyto-
pathology in 73.3% centres where 3–6 months or less
was dedicated to cytopathology training as against
23.8% of centres where 6–12 months or more were
dedicated to cytopathology training (P = 0.0005).
There was no association between the relatively small
percentages of medical practitioners of other specialities
and non-medical staff, respectively, and time dedicated
to cytopathology training or workload.
There was a correlation between small workloads
for FNA and exfoliative cytology and the likelihood of
pathologists without experience in general cytology
Table 4. Consultant reporting practice according to FNA workload
Consultants signing
out cytopathology
FNA workloadNo
response TotalLarge Medium Small
Specialist reporting without experience in
general cytopathology
Yes 5 4 6 2 17
No 12 15 5 6 38
% �yes� response 29.4 21.1 54.5 30.9
Pathologists without specific training
in cytopathology
Yes 8 11 6 4 29
No 8 8 5 3 24
% �yes� response 50.0 57.9 54.5 54.7
Medical practitioners from other disciplines Yes 2 3 2 1 8
No 15 16 9 5 45
% �yes� response 11.8 15.8 18.2 15.1
Non-medical staff reporting non-gynaecological
cytology
Yes 1 4 3 0 8
No 14 14 7 6 41
% �yes� response 6.7 22.2 30.0 16.3
Table 3. Consultant reporting practice according to cytopathology time
Consultants signing
out cytopathology
Cytopathology training time
No
Response Total
Nil, 3-6 months
or less
6-12 months
or more
Specialist reporting without experience
in general cytopathology
Yes 10 6 1 17
No 21 16 1 38
% �yes� response 32.3 27.3 30.9
Pathologists without specific training
in cytopathology
Yes 22 5 2 29
No 8 16 0 24
% �yes� response 73.3 23.8 54.7
Medical practitioners from other disciplines Yes 5 3 0 8
No 25 19 1 45
% �yes� response 16.7 13.6 15.1
Non-medical staff reporting non-gynaecological
cytology
Yes 5 3 0 8
No 23 17 1 41
% �yes� response 17.9 15.0 16.3
Survey of medical training in cytopathology 153
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

reporting specialized cytopathology. The percentage
answering �yes� to that question represented 25% of
those with medium and large workloads of exfoliative
and FNA cytology compared with 60% of those
with small exfoliative cytology workloads and
54.5% with small workloads of FNA cytology. The
difference was significant for exfoliative cytology
(P = 0.037) but not for FNA cytology (P = 0.066).
There was no correlation between likelihood of
gynaecological cytology being reported by non-med-
ical staff and time dedicated to training but there was
an association with workload. Among 16 respondents
with workloads below 10 000 per year, 31.3%
answered �yes� to non-medical staff reporting gynae-
cological cytology compared with 63.0% of 27 with
workloads of 10 000 or more (P = 0.04).
Discussion
This survey showed that the majority of undergrad-
uate and postgraduate training was organized at a
national level, suggesting that improvements to
training should be focused on governments rather
than individual institutions. Perhaps not surprisingly,
cytopathology was less likely than histopathology to
be a defined undergraduate course (13.2% compared
with 75.7%). Histopathology was only included in
59.7% of multidisciplinary clinical sessions and cyto-
pathlogy in 49.3% of these clinical teaching modules,
reflecting a relatively low level of exposure to
pathology in general. However, in some medical
schools cytopathology was taught as part of histopa-
thology, gynaecology, oncology, surgery and internal
medicine, demonstrating its wide clinical relevance as
a discipline.
As with histopathology, the low level of cytopathol-
ogy teaching at undergraduate level means that
training must almost entirely be carried out at
postgraduate level. One of the most consistent findings
in this survey was the importance of histopathology as
a basis for cytopathology training. Histopathology
training was mandatory for training in cytopathology
in 83.1% of respondents� countries and an over-
whelming majority of respondents (89.5%) regarded
it as essential. Qualifications and examinations
for histopathology and cytopathology were usually
combined (more than 80%). Although 67.3% of
respondents reported mandatory cytopathology
sections of examinations, mandatory cytopathology
courses and separate examinations were less common,
which was identified as a deficiency in training. �InEurope, we only know of a postgraduate diploma in
France (7) and the Royal College of Pathologists
Diploma in Cytopathology, which is available but no
Table 5. Consultant reporting practice according to exfoliative cytology workload
Consultants signing
out cytopathology
Exfoliative cytology
workloadNo
response TotalLarge Medium Small
Specialist reporting
without experience in
general cytopathology
Yes 5 4 6 2 17
No 14 13 4 7 38
% �yes� response 26.3 23.5 60.0 30.9
Pathologists without
specific training
in cytopathology
Yes 10 8 7 4 29
No 8 9 3 4 24
% �yes� response 55.6 47.1 70.0 54.7
Medical practitioners
from other disciplines
Yes 4 1 2 1 8
No 15 16 8 6 45
% �yes� response 21.1 5.9 20.0 15.1
Non-medical staff
reporting non-
gynaecological
cytology
Yes 3 2 3 0 8
No 15 12 6 6 41
% �yes� response 16.7 14.3 33.3 16.3
Anshu et al.154
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

longer used in the UK (8).� The lack of integration of
cytopathology into histopathology was also cited as
a deficiency. However, the main deficiencies in cyto-
pathology training were the variability of training,
the lack of specifically trained cytopathologists in
many centres, the lack of training to a high level of
competence and the overwork and shortage of training
facilities in those centres that did have trained cytop-
athologists and potentially good training programmes.
The over-riding problem is that while histopathology is
essential for training in cytopathology, �most pathol-
ogists have no interest in cytology�.One of the problems identified in the survey was
the lack of training to a level of competence, which
must be a serious problem when so many posts
include cytopathology in their job description and
87.3% attend multidisciplinary meetings and con-
tribute to decisions on management of patients.
Furthermore, cytopathologists in centres of good
practice carry out FNAs themselves, provide imme-
diate diagnoses and contribute to image-guided
biopsy sessions.
Training in cytopathology was more likely to
involve screening slides than gaining hands-on expe-
rience with FNA and rapid assessment and less than a
third of trainees gained sufficient experience to be
allowed to sign out reports. Examples of good practice
in cytopathology cited �connection with other clini-
cians (gynaecologists, haematologists, oncologists),
active participation in FNA, direct contact with
patients, participation in planning of therapeutic
approach (along with) training in histopathology�,demonstrating the added clinical perspective that a
training in cytopathology requires; it is not a training
that should be confined to the examination of slides.
It was unusual for non-medical degrees to be
acceptable for entry into cytopathology training and
medical graduates from other specialties were usually
(but not always) required to train in histopathology as
well. Although non-medical staff sign out negative
cervical cytology according to 48.1% of responses,
particularly in laboratories with larger workloads,
they rarely sign out non-gynaecological cytology,
except in some instances negative sputum and urine.
Nevertheless, non-medical staff contributed to cyto-
pathology training according to more than half of
responses, supporting the comment that there are
�insufficient numbers of pathologists with an interest
in cytopathology to provide the training�. In view of
the important role that well-trained cytotechnologists
play in cervical screening cytology, their role could
usefully be expanded by formally training them to
pre-screen non-gynaecological cytology specimens
and perhaps to assess cytology sample adequacy in
situations where a cytopathologist was not needed to
provide a diagnosis on site.
The length of time dedicated to training in cytopa-
thology was highly variable and frequently depended
on the local enthusiasm of cytopathologists, often
with insufficient time and resources. There was at
least 6–12 months for cytopathology in 40% of
responses compared with at least 2–3 years for histo-
pathology in 88.5%. The brief time dedicated to
cytopathology was frequently cited as a deficiency in
training. Although this survey provides information
about opinion and practice of cytopathology, the
importance of who reports what and how much
training is required depends on clinical audit, corre-
lation with histopathology and outcome, none of
which is available in this survey. However, we
thought that variations in reporting practice should
be correlated with time dedicated to cytopathology
training and workload to see whether any patterns
emerged. There was a correlation between training
times of 3–6 months or less and likelihood of pathol-
ogists without specific training in cytopathology sign-
ing out reports, and this practice was reported in
54.7% of responses. Furthermore, there was a
correlation between centres where training was 3-6
months or less and respondents saying that there was
insufficient integration of cytopathology into histo-
pathology training and a lack of training to a high
level of competence. Although 92.2% of respondents
thought that specialist cytology should not be reported
by pathologists without experience in general cytopa-
thology, that practice was reported in 30.9% of
responses and correlated with laboratories with
smaller workloads.
We have demonstrated serious deficiencies in cyto-
pathology training as well as insufficiencies in man-
power and resources in places with potentially
adequate programmes. What is the way forward and
what can be gained from this survey? It is clear that
cytopathology training is overly dependent on local
centres of excellence and that training is variable,
often concentrating on microscopy alone rather than
the clinical aspects of the speciality. A vicious cycle of
inadequate training and insufficient trainers can only
be broken by increasing the amount of time dedicated
to cytopathology training, if necessary by seconding
trainees (as temporary placements) to centres
where adequate training is available, and providing
Survey of medical training in cytopathology 155
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd

mandatory requirements for independent practice. As
this is unlikely to be achieved at a local or even
national level it should be taken at least to the level of
the EFCS and perhaps the European Union, for
example through UEMS, so that guidelines can be
produced that overcome the unfortunate but unac-
ceptable fact that �most pathologists have no interest
in cytology�. The overwhelming opinion that (1) a
medical qualification and (2) training in histopathol-
ogy are essential for practice in cytopathology and the
growing importance of direct involvement with
patient care and attendance at multidisciplinary
meetings and biopsy procedures make it necessary to
regard cytopathology as a �superspeciality� rather than
a �subspeciality� and grant it the level of training it
deserves.
Recommendations
• 6-12 months should be dedicated to cytopathol-
ogy during histopathology training with optional
additional training for those wanting to carry out
independent practice in cytopathology.
• Formal accreditation (preferably with specialist
examinations) in all types of cytopathology should
be mandatory for independent practice in cytopa-
thology, including specialist cytopathology.
• When necessary, temporary attachments (sec-
ondments) to centres of good practice should be
available to trainees intending to practise inde-
pendently in cytopathology.
• There should be adequate numbers of patholo-
gists trained in cytopathology to a high level of
competence; some of their time could be released
by training cytotechnologists and trainee pathol-
ogists to pre-screen non-gynaecological cytology
slides and assess adequacy of FNAs when imme-
diate diagnosis is not required.
• European and international guidelines for train-
ing and accreditation in cytopathology should be
developed with some urgency.
References
1. Kocjan G, Chandra A, Cross P et al. BSCC Code of Practice –
fine needle aspiration cytology. Cytopathology 2009;20:283–
96.
2. Chandra A, Cross P, Denton K et al. The BSCC code of
practice – exfoliative cytopathology (excluding gynae-
cological cytopathology). Cytopathology 2009;20:211–23.
3. Wiener HG, Klinkhamer P, Schenck U et al. European
guidelines for quality assurance in cervical cancer screen-
ing: recommendations for cytology laboratories. Cytopa-
thology 2007;18:67–78.
4. Gray W, Bayer-Pietsch E, Chieco P et al. The future of
cytopathology in Europe. Will the wider use of HPV
testing have an impact on the provision of cervical
screening?. Cytopathology 2007;18:278–82.
5. Lynge E, Antilla A, Arbyn M, Segnan N, Ronco G. What�snext? Perspectives and future needs of cervical screening
in Europe in the era of molecular testing and vaccination.
Eur J Cancer. 2009 Oct;45:2714.
6. Confederation of EU Rectors� Conferences and the Associ-
ation of European Universities (CRE). The Bologna decla-
ration on the European space for higher education: and
explanation. Available at http://ec.europa.eu/education/
policies/educ/bologna.pdf (accessed 29 January 2010).
7. Cochand-Priollet B, Vincent S, Vielh P. Cytopathology in
France. Cytopathology 2004;15:163–6.
8. College examinations for fellowship and diplomas. Regula-
tions and guidelines for 2009. Available at http://www.
rcpath.org/resource/pdf/regs_and_guide_2009.pdf (accessed
25 March 2010).
Anshu et al.156
Cytopathology 2010, 21, 147–156 ª 2010 Blackwell Publishing Ltd





























