Embed Size (px)
Citation preview

Systems Collaboration with Schools andTreatment of Severely Emotionally Disturbed
Children or AdolescentsMo Yee Lee, Barbra Teater, Kai Shyang Hsu, Gilbert J. Greene, J. Scott Fraser, Andrew D. Solovey,
and David Grove
This study explored the relationship between the level of systems collaboration with schoolsand outcomes for children diagnosed with serious emotional disorder and their familiesinvolved in integrative family and systems treatment, a home-based treatment program.Using data collected from 38 clients and their families, this study used a structural equationmodel to explore how systems collaboration with schools influenced children’s behavioraloutcomes, parental competence, and family functioning. The squared multiple correlationsfrom endogenous variables of the final model accounted for 31 percent of the variance inproblem severity in children, 38 percent of the variance in level of functioning in children,30 percent of the variance in parental competence with children, and 41 percent of the vari-ance in family functioning. The final model indicated the following: Systems collaborationwith schools positively influenced parental competence with children, which positively pre-dicted level of functioning in children and negatively predicted problem severity in children.Although the limited sample size of the study precludes any definitive conclusions, implica-tions of the study on the potential role of systems collaboration with schools in treating fam-ilies with at-risk children or adolescents are explored and discussed.
KEYWORDS: home-based treatment; I-FAST; serious emotional disorder; severely emotionally disturbed; systemscollaboration with schools
An estimated 5 percent to 26 percent ofchildren and adolescents in the UnitedStates have experienced a mental health
difficulty (Brauner & Stephens, 2006) and an esti-mated 9 percent to 13 percent have experienced aserious emotional disorder (SED) (Mark & Buck,2006). The Center for Mental Health Servicesdefines a child (birth to 18 years) as having an SEDif that child currently has, or at any time during thelast year has had, a diagnosable mental, behavioral,or emotional disorder of sufficient duration to meetdiagnostic criteria in the Diagnostic and Statistical Man-ual of Mental Disorders (DSM-IV-TR) (SubstanceAbuse and Mental Health Services Administration,1993). Children with SEDs may exhibit emotionsor behaviors, such as hyperactivity, aggression, self-injurious behaviors, social withdrawal, poor copingskills, temper tantrums, or extreme mood swings(National Dissemination Center for Children withDisabilities, or NICHCY, 2010) within the home,community or school environment. Within theschool system, children with a SED are at a striking
disadvantage. They tend to experience the following:lower grades, higher grade retention, higher likeli-hood of dropping out of high school, higher absen-tee rates, and higher likelihood of receiving schoolsuspensions and expulsions (Armstrong, Dedrick, &Greenbaum, 2003; Rapport, Denney, Chung, &Hustace, 2001; U.S. Department of Education,Office of Special Education Programs, 2001;Wagneret al., 2006). In addition, children with SEDs arefound to externalize their emotional difficulties,which results in disruptive behaviors in the classroomsetting (Mottram, Bray, Kehle, Broudy, & Jenson,2002; Passaro, Moon, Wiest, &Wong, 2004).
Children and adolescents with SEDs are often-times referred to a specialist for treatment when par-ents and schools are unable to successfully addressproblems or difficulties (Foltz, 2004;Mears, Yaffe, &Harris, 2009). If the problems persist, the child canbe at a greater risk of out-of-home placement(Lakin, Brambila, & Sigda, 2005).Community-basedor home-based treatments are widely used modelsfor treating families with a child or adolescent who
doi: 10.1093/cs/cdt013 © 2013 National Association of Social Workers 1
Children & Schools Advance Access published July 19, 2013
has been diagnosed with a SED and is at risk ofout-of-home placement (for example, integrativefamily and systems treatment [I-FAST], multisyste-mic therapy, family-directed structural therapy). Yetin order to be effective, these treatment modelsrequire systems collaboration among the multipleinstitutions serving the family (Borduin et al., 1995;Lee et al., 2009; Radohl, 2011). Many, if not most,of the families with a child who has a SED areinvolved with several different agencies and theirrepresentatives, such as mental health workers, socialservices, schools, juvenile courts, and psychiatrichospitals. Furthermore, these families desire a treat-ment approach based on consistency in servicedelivery and structured coordination and collabora-tion among service providers (Ditrano & Silverstein,2006; McLendon, 2008). Although systems collabo-ration promises coordinated, effective, and efficientservices for families (Bronstein, 2003; Johnson,Wistow, Schulz, & Hardy, 2003), such a collabora-tive process involving diverse disciplines, profession-als, and systems is not without struggles and barriers.
Systems collaboration can exist along a contin-uum from a low level of communication, such as aconsultation, to a more in-depth, shared work basedaround a single client system (Darlington, Feeney, &Rixon, 2005; Walter & Petr, 2000). Challenges tothe collaborative effort can stem from a diverseknowledge base; conflicting mandates, goals forclients, or intervention priorities; differences in poli-cies and procedures; and the working practices of thecollaborators (Bronstein, 2003; Huxham & Vangen,2000;Milbourne, Macrae, &Maguire, 2003;Riddell& Tett, 2001). Despite the good intentions of thecollaborating institutions and professionals, discon-nection and disruption between systems can send aconfusing message to clients and counteract thepotential benefits of treatment (Bronstein, 2003;Huxham & Vangen, 2000). For instance, a schoolmight suspend a child with a SED from school or thecourt might send the child to a residential treatmentfacility for the behavior, while a home-based casemanager or therapist would attempt to work withthe parents and the child to control the problembehaviors. Therefore, systems collaboration amongthe various service providers (that is, mental health,social services, schools, juvenile courts, psychiatrichospitals) and the client systems (that is, child, adoles-cent, family) may play a crucial role in achievingpositive outcomes for the child and family (Chuang&Wells, 2010;Milbourne, 2005).
Using data collected from a larger evaluation ofI-FAST, a home-based, family-centered treatmentprogram for families with a child or adolescent whohas a SED and is at risk of out-of-home placement(Fraser, Solovey, Grove, Lee, & Greene, 2012; Leeet al., 2009), this study used a structural equationmodel to explore the potential effects of systems col-laboration with schools in influencing a child’s behav-ioral outcome, as mediated by other familial variableslike parental competence and family functioning.
LITERATURE REVIEW
Systems CollaborationIn their 1998 work, Berg-Weger and Schneiderdefined systems collaboration as an interpersonal pro-cess through which members of different disciplinescontribute to a common product or goal (p. 698).Bronstein (2003) extended this definition by statingthat interdisciplinary collaboration, or systems col-laboration, aims to achieve the goals “that cannot bereached when individual professionals act on theirown” (p. 299). This extended definition highlightsthe complexities of systems collaboration andthe distinction from cooperation, communication,coordination, and partnership (Bronstein, 2003;Bruner, 1991). Successful systems collaborationincorporates factors such as mutual trust, powersharing, a commitment to collaboration among thepartners, and the ability to adjust previously definedboundaries (Torres & Margolin, 2003)—alongsidekey interpersonal skills, attitudes, professional quali-ties and contextual factors (Lee et al., 2011). Despitethese factors, the extent of collaboration is influ-enced by professional roles, structural characteristics,personal characteristics, and a history of collabora-tion (Bronstein, 2003). The existing literature onsystems collaboration consistently cites the impor-tance of collaborative efforts, particularly whenworking with children and families (Anderson-Butcher & Ashton, 2004; Brandes & Cheung, 2009;Darlington & Feeney, 2008; Darlington, Healy, &Feeney, 2010; Spath, Werrbach, & Pine, 2008).However, empirical evidence illustrating the bene-fits or effects of systems collaboration on outcomeswith children and families remains scarce.
CHILDRENWITH SEDsWITHIN SCHOOLSETTINGSSchools serve as a critical environment in whichsystems collaboration can occur, particularly as they
2 Children & Schools
are a place where children use, demonstrate, anddevelop their academic and social skills (Repie,2005). Children and adolescents with SEDs areoften considered at-risk within the educational sys-tems for several reasons. First, children with SEDstend to experience more complex academic issuesand mental health difficulties as compared withchildren with or without disabilities (Reddy &Richardson, 2006) and are often targeted for inter-ventions to improve academic and social success(Reddy, De Thomas, Newman, & Chun, 2009).Second, research has shown that children with aSED are more likely to have lower grades, fail oneor more courses, receive school suspensions andexpulsions, and have greater rates of absenteeismthan other children (Armstrong et al., 2003;Wagner, Kutash, Duchnowski, Epstein, & Sumi,2005). Finally, research has found that there is astigma attached to children with SEDs, as teachersperceive them as less competent and academicallycapable than their counterparts without SEDs, evenwhen scores for academic performance are equiva-lent (Lane, Carter, Pierson, & Glaeser, 2006).
Schools tend to take an individualized approachwhen providing interventions to children and ado-lescents with SEDs. In 2009, Reddy and colleaguesconducted a review of school-based preventionand intervention programs for children with SEDsand found that the majority of the interventionsdo not embrace a biopsychosocial or person-in-environment-based approach. Instead, individuallyfocused interventions that address behaviors thatoccur within the school setting alone are used.These programs typically focus on behavioral orcognitive–behavioral treatment (that is, social skillstraining, token economies, group contingencies);classroom-based treatment; parent-training treat-ment; or multimodal treatment approaches such asindividualized psychodynamic therapy, medication,social skills training, or psychodrama, art, play, orpet therapies in the classroom, home, or commu-nity. For example, the program with the largesteffect size consisted of a classroom-based interven-tion where classroom behavior rules are placed oneach student’s desk and students are able to receiveone sticker for following all the rules for 30 minutes.The intervention consists of positive reinforcementand verbal redirection (De Martini-Scully, Bray, &Kehle, 2000;Musser, Bray, Kehle, & Jenson, 2001).However, collaboration with other systems is notincluded in the design of any of these programs.
SYSTEMS COLLABORATION AND IMPACTON CHILD AND FAMILY’S OUTCOMESBarriers to collaboration with school-based interven-tions, as described by Reddy et al. (2009), often occurand can include a lack of communication betweenservice providers and parents. For example, parentsmay be unsure of what their child is doing within theschool, and school personnel might perceive the par-ents to be disengaged (Ouellette, Briscoe, & Tyson,2004). When families are involved and empoweredin interventions, such as the Intensive Mental HealthProgram (IMHP), there is a noted improvement inthe child’s thought processes, overall functioning,and the ability of the family to provide social andemotional supports (Richards, Bowers, Lazicki, Krall,& Jacobs, 2008). An additional barrier to school-based interventions is the mere lack of systems collab-oration as a treatment component when providinginterventions specifically designed for children withSEDs and their families. A qualitative study examin-ing the overall satisfaction of youths, caregivers, andproviders with the IMHP concluded that teachersdesired more consistent communication with care-givers. Caregivers, although satisfied with the level oftherapeutic alliance, felt that there were too manyprofessionals involved and desired a more collabora-tive relationship between themselves and serviceproviders (Lazicki, Vernberg, Roberts, & Benson,2008). Although collaboration was identified as adesire by the caregivers, systems collaboration is notlisted as an essential treatment component withinthe IMHP treatment model (see Vernberg, Roberts,& Nyre, 2008).
Despite the common use of individualizedinterventions and the potential barriers to systemscollaboration within schools, there is a growingbody of research that illustrates the benefits ofcommunity-based and home-based treatment pro-grams that include systems collaboration in work-ing with children and adolescents with SEDs.Research indicates that treatment models are moreeffective when they are tailored across settings,such as home and school. For example, KutashDuchnowski, Sumi, Rudo, and Harris (2002) eval-uated a school-based program, the School, Familyand Community Partnership, implemented withmiddle-school-age children (N= 23) who were inspecial education. The goal was to determine theextent to which participation in the program con-tributed to the child’s emotional, social, behavioral,and academic functioning. The pretest–posttest
Lee et al. / Systems Collaboration with Schools and Treatment of Severely Emotionally Disturbed Children or Adolescents 3

evaluation found a statistically significant decrease indiscipline rates over time and an improvement onmeasures of emotionality and impairment overtime. However, these improvements were not sig-nificant, and no significant changes in levels ofachievement in math and reading, number of daysabsent, or percentage of time spent in the specialeducation environment were found. Anothercommunity-based prevention program, the HelpingFamilies Initiative, found that among 147 families,school outcomes (for example, school problems,school grades) were predicted by family functioningas mediated by child well-being. The results of theprogram confirm that family relationships are impor-tant in influencing a child’s development andbehavior (Turner, Powell, Langhinrichsen-Rohling,& Carson, 2009).
Collaboration is also considered a critical treat-ment component to the “wraparound practicemodel” (Bruns et al., 2010; Kernan & Morilus-Black, 2010), which is the largest community-basedtreatment model for children and adolescents.Nearly 98,000 youths receive services in over 800wraparound initiatives in the United States (Bruns,Leverentz-Brady, & Sute, 2008). Evaluations of thewraparound approach show fewer missed schooldays and suspensions; fewer attempts to run awayfrom home; fewer assaults, days in detention, andstops by the police for youths receiving wraparoundservices when compared with youths who did notreceive wraparound treatment (Carney & Buttell,2003); as well as lower recidivism rates (Pullmanet al., 2006). In addition, an evaluation of the wrap-around service for children involved in the childwelfare system illustrated a statistically significantincrease in residential stability, decreased reliance onout-of-community placements, and an improve-ment in behavior, functioning, and school out-comes (Bruns, Rast, Walker, Bosworth, & Peterson,2006). A critical component of these programs isthe team or partnership of individuals who work inconjunction with immediate and extended familymembers, child-serving agencies, community repre-sentatives, and school personnel to foster a coopera-tive, child-focused environment. Although each ofthese treatment approaches emphasize collaborationbetween the individuals and agencies involved withthe child and family, the evaluations of such pro-grams do not consider the extent to which the levelof systems collaboration contributes to the outcomesfor the child and family.
The existing literature highlights that systems col-laboration, which includes schools, can serve as acritical factor for a child or adolescent with a SEDand their families when working to overcome prob-lems and difficulties that clearly span beyond thehome environment. In addition, the literature sug-gests that the impact of systems collaboration on achild’s outcomes could be mediated by family vari-ables (Richards et al., 2008; Turner et al., 2009).However, while there are evaluations of existingcommunity-based or home-based treatment modelson child and family outcomes, the studies did notexamine the extent to which systems collaborationwith schools can contribute to child and family out-comes and the pathways of influence. Research ofhome-based treatment models that promote systemscollaboration as a core treatment component, suchas I-FAST, can address this gap in the literature byexamining the relationship between systems collab-oration with schools and behavioral outcomes asmediated by family variables in terms of parentalcompetence and level of family functioning.
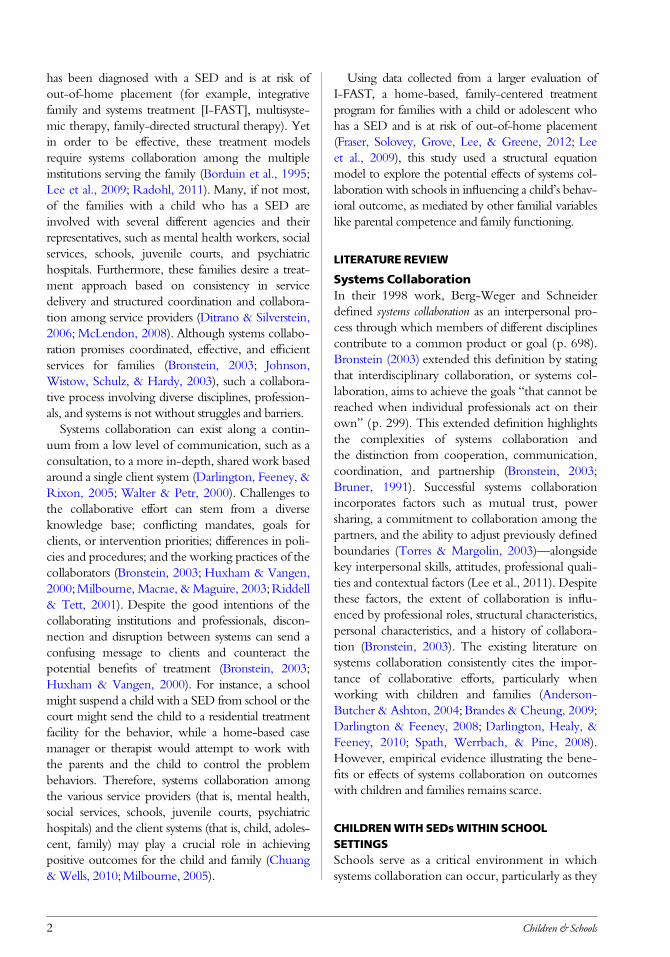
MethodThis is an exploratory study that used a posttestdesign to explore the role of systems collaborationwith schools in influencing child and family out-comes when the family had child with a SED atrisk of out-of-home placement. The study analysesdata from a larger outcome study that evaluated theeffectiveness of I-FAST (Lee et al., 2009) a home-based treatment program that consists of three corecomponents: therapeutic alliance, change in inter-actional patterns, and systems collaboration (Fraseret al., 2012; Lee et al., 2009). Based on existing lit-erature regarding the effect of community-basedprograms on child and family outcomes, thisstudy’s three hypotheses were as follows: (1)Greater collaboration with schools would lead toincreased parental competence with children andimproved level of family functioning; (2) increasedparental competence with children and improvedlevel of family functioning would lead to adecrease in problem severity and an increase in thelevel of functioning in children; and (3) systemscollaboration with schools would predict a child’soutcomes (problem severity; functioning in chil-dren) as mediated by family variables (parentalcompetence with children; family functioning)(Figure 1). In addition, therapeutic alliance is acore I-FAST treatment component. Research has
4 Children & Schools
repeatedly revealed the important role of therapeu-tic alliance in facilitating positive outcomes in cli-ents and families (Asay & Lambert, 1999; Diamondet al., 2006; Johnson, Wright, & Ketring, 2002). Inthe larger outcome study, therapeutic alliance wassignificantly associated with child outcomes. Tocontrol for the potential impact of therapeutic alli-ance on the model, this variable was entered as apredictor variable in the model (Lee et al., 2009).
Research ParticipantsParticipants of the study included families with chil-dren who were at risk of out-of-home placement.The courts, children’s services, hospitals, or othermental health agencies referred families to theI-FAST program at two large community mentalhealth agencies in a midwestern state. Both the par-ents and the child who is at risk of placement wereinvited to participate in the study. Participation inthe study was voluntary and formal written consentwas obtained from all participants. Participants wereclearly told that neither participation nor refusalwould affect their legal situation. The study wasreviewed for institutional review board approval.
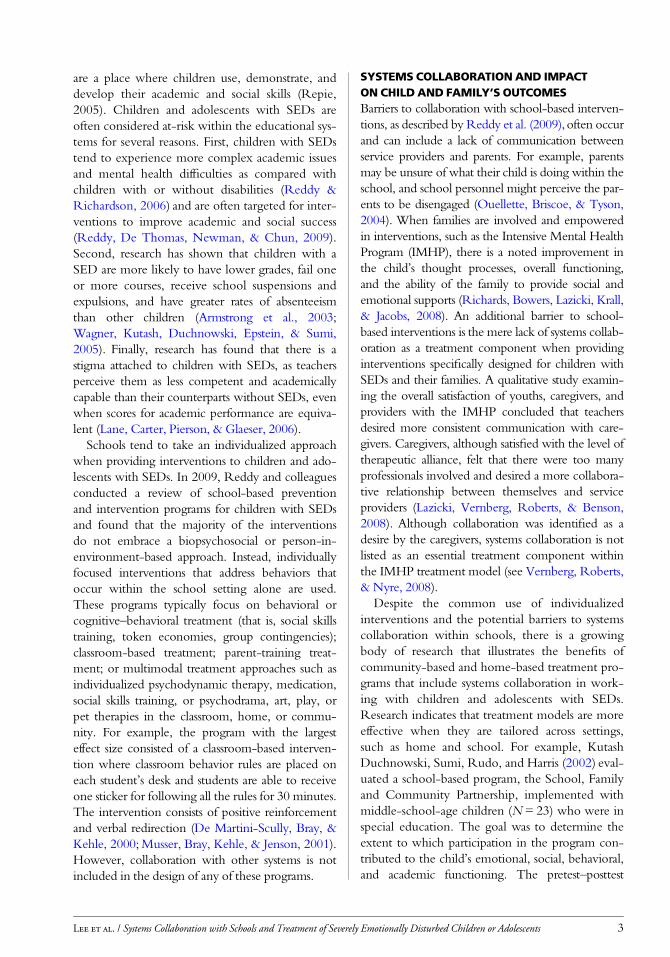
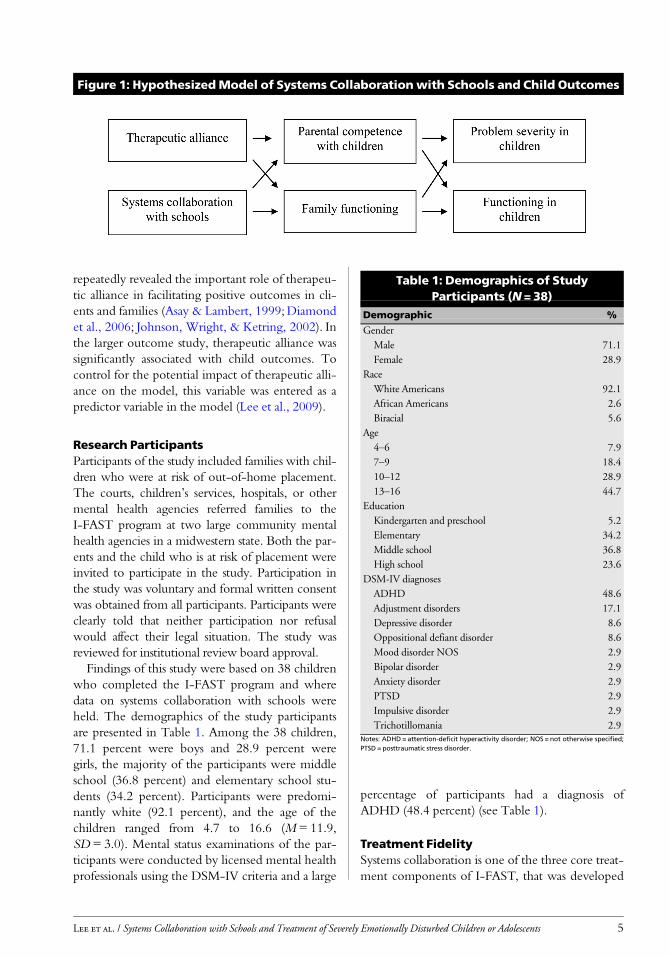
Findings of this study were based on 38 childrenwho completed the I-FAST program and wheredata on systems collaboration with schools wereheld. The demographics of the study participantsare presented in Table 1. Among the 38 children,71.1 percent were boys and 28.9 percent weregirls, the majority of the participants were middleschool (36.8 percent) and elementary school stu-dents (34.2 percent). Participants were predomi-nantly white (92.1 percent), and the age of thechildren ranged from 4.7 to 16.6 (M = 11.9,SD= 3.0). Mental status examinations of the par-ticipants were conducted by licensed mental healthprofessionals using the DSM-IV criteria and a large
percentage of participants had a diagnosis ofADHD (48.4 percent) (see Table 1).
Treatment FidelitySystems collaboration is one of the three core treat-ment components of I-FAST, that was developed
Figure 1: HypothesizedModel of Systems Collaborationwith Schools and Child Outcomes
Table 1: Demographics of StudyParticipants (N = 38)
Demographic %
Gender
Male 71.1
Female 28.9
Race
White Americans 92.1
African Americans 2.6
Biracial 5.6
Age
4–6 7.9
7–9 18.4
10–12 28.9
13–16 44.7
Education
Kindergarten and preschool 5.2
Elementary 34.2
Middle school 36.8
High school 23.6
DSM-IV diagnoses
ADHD 48.6
Adjustment disorders 17.1
Depressive disorder 8.6
Oppositional defiant disorder 8.6
Mood disorder NOS 2.9
Bipolar disorder 2.9
Anxiety disorder 2.9
PTSD 2.9
Impulsive disorder 2.9
Trichotillomania 2.9Notes: ADHD = attention-deficit hyperactivity disorder; NOS = not otherwise specified;PTSD = posttraumatic stress disorder.
Lee et al. / Systems Collaboration with Schools and Treatment of Severely Emotionally Disturbed Children or Adolescents 5
based on existing evidence-based approaches forworking with at-risk children, adolescents, andfamilies and a strengths perspective (Fraser et al.,2011; Lee et al., 2009). The study collected audioor videotapes on 35 initial family sessions, 17 six-week family sessions, and nine consultation sessionswhere I-FAST case managers participated in super-vision with I-FAST consultants. Model fidelitywas measured by the 31-item I-FAST Checklist,which assesses core treatment components ofI-FAST: therapeutic alliance (items 1 through 20);second-order change strategies (items 21 through25); and systems collaboration (items 26 through31) (Lee et al., 2003; Lee et al., 2009). Independentraters viewed each video or audio tape and usedthe I-FAST Checklist to rate specific interventionsof each core treatment component used by casemanagers and the clinical consultants in the treat-ment process or the consultation process. Thestudy used intraclass correlation (ICC) to assessinterrater reliability of I-FAST and found a satisfac-tory level of interrater reliability. In regard to thefamily sessions, the ICC for therapeutic alliancewas .84, for second-order change was .86, and forsystems collaboration was .88. In regard to the con-sultation sessions, the ICC for therapeutic alliancewas .82, for second-order change was .88, and forsystems collaboration was .80. The ICC for theoverall I-FAST was .88 (Lee et al., 2009).
Variables: Measurement andModelData collected from the various instrumentsdescribed as follows were checked and coded fordata processing and statistical analyses using the Stat-istical Package for Social Sciences (SPSS). Structuralequation modeling (SEM) was used in the data anal-ysis to examine a causal model (see Figure 1) thataccounted for outcomes in children. The modelincluded treatment variables of systems collaborationwith schools and therapeutic alliance, families’ pro-files of parental competence with children and fam-ily functioning, and child’s outcomes of problemseverity and functioning. The study uses AMOS19.0 from SPSS to conduct the analysis of SEM.
PREDICTING VARIABLES
Systems Collaborationwith SchoolsSystems collaboration with schools is understood asrelational and interpersonal activities that ensurethe coordination of services between the I-FASTcase managers and school personnel to accomplish
the treatment goals on behalf of the client and thefamily (Lee et al., 2012). These activities include,but are not limited to, personal meetings, phonecalls, or sharing information. Systems collaborationwas operationally defined as the scores of the Sys-tems Collaboration Scale as completed by I-FASTcase managers at termination of the treatment. TheSystems Collaboration Scale is a self-constructedscale developed by Lee and Greene (2002) to assessthe degree of cooperation and helpfulness whenservice systems collaborate with each other in thetreatment process. The extent of collaborationwith other service systems is rated on a three-pointLikert-type scale (ranging from 1 = positive collab-oration to 3 = negative collaboration). A total scorefor each subscale was obtained by adding the scorefor each individual system contacted and thendividing by the number of systems contacted.
Therapeutic AllianceTherapeutic alliance was operationally defined bythe scores of the Family Alliance Scale (Pinsof, 2003)as completed by the parents at termination of theI-FAST treatment. The Family Therapy AllianceScale, which is a 40-item scale was adapted andexpanded from the original 29-item Family TherapyAlliance Scale (Pinsof & Catherall, 1986) to assess thequality of therapeutic alliance between the therapistand the family. The Family Therapy Alliance Scaleconsists of the following three subscales with exam-ples of statements from each: Bonds—“The therapistcares about my family”; Tasks—“The therapist hasthe skills and ability to help my family”; and Goals—“The therapist is in agreement with my family’sgoals for this therapy.” Statements are rated on aseven-point Likert-type scale (ranging from 1 =completely disagree to 7 = completely agree). One-half of the items on each subscale are reverse scored.The three subscale scores can be summed to a totalscore. Pinsof and Catherall (1986) reported a satisfac-tory reliability coefficient of .83 of the original scale.Heatherington and Friedlander (1990) examined theinternal consistency of the original scale and reportedsatisfactory Cronbach’s alphas of .94 for the totalscale, .81 for the Bonds subscale, .90 for the Taskssubscale, and .80 for the Goals subscale.
MEDIATING VARIABLES
Parental Competencewith ChildrenParental competence with children was operation-ally defined by the scores on the Parental Efficacy
6 Children & Schools
Scale based on parents’ report. This is a 10-itemscale adapted and modified from the Parental Locusof Control Scale (Campis, Lyman, & Prentice-Dunn, 1986). Examples of items are “When mychild gets angry I can usually deal with him/her if Istay calm”; “What I do has little effect on my child’sbehavior” (reverse scored item). Parents are asked torate their responses on a five-point Likert scale(ranging from 1 = strongly disagree to 5 = stronglyagree). The Parental Efficacy subscale is scored bysumming individual items with six items reverse-scored. The scores range from 5 to 50 with higherscore indicating greater parental competence in rela-tion to children. Norms for the original ParentalEfficacy subscale are not reported, although meansfor parents who did not report difficulties in the par-enting role (17.62) are distinguished from means ofparents who had requested counseling services forparental problems (19.27), and a reliability coeffi-cient of .62 of the Parental Efficacy subscale wasreported (Campis et al., 1986).
Family FunctioningFamily functioning refers to the cohesion and adapt-ability of the family and was operationally defined asthe scores on Family Types of FACES II as com-pleted by parents at termination. FACES II is30-item scale developed by Olson, Portner, andBell (1982) based on the circumplex model of familyas formulated by David H. Olson, Candyce Russell,and Douglas Sprenkle. FACES II contains 16 cohe-sion items and 14 adaptability items. Respondentsare requested to rate how frequently the describedbehavior occurs in their family on a five-pointLikert-type scale (ranging from 1 = almost never to5 = almost always). Examples are as follows: “Familymembers are supportive of each other during diffi-cult times” (Cohesion item); “Our family tries newways of dealing with problems” (adaptability item).Detailed scoring procedures are described in theFamily Inventories Manual (Olson, 1992). Based oncohesion scores and adaptability scores, FACES IIprovides Family Types scores in terms of balanced(scores 7 to 8), moderately balanced (5 to 6), mid-range (3 to 4), and extreme (1 to 2).
Olson (1992) reported satisfactory Cronbach’salphas of .90 for the total scale, .87 for cohesion,and .78 for adaptability. Test–retest reliability over aperiod of four to five weeks was .83 for cohesionand .80 for adaptability. Good concurrent validitywas also established for FACES II. Hampson, Hulgus,
and Beavers (1991) compared the Dallas Self-ReportFamily Inventory (SFI) with FACES II and reportedstrong and significant correlations between SFI globalmeasure of family health and FACES II (.93 forcohesion and .79 for adaptability).
DEPENDENT VARIABLES
Problem Severity in ChildrenProblem severity refers to the level of commonproblems associated with children who receive men-tal health services and is operationally defined as thescores the child obtains on the Problem Severitysubscales of the Ohio Scale as reported by parents attermination. The Ohio Scales were developed toprovide multisource, multicontent measures of clini-cal outcomes of youths ages five to 18 years (Ogles,Lambert, & Masters, 1996). The Problem SeverityScale comprises 20 items, and raters are asked to ratethe degree to which the child has experienced theproblem in the past 30 days on a six-point Likertscale (ranging from 0 = not at all to 5 = all the time).The scores range from 0 to 100, with a higher scoreindicating a more severe problem (Ohio Depart-ment of Mental Health [ODMH], 2006).
Functioning in ChildrenFunctioning refers to the level of emotional andbehavioral functioning of the child and is opera-tionally defined as the scores the child obtains onthe Functioning subscales of the Ohio Scale asreported by parents at termination. The Function-ing Scale comprises 20 items designed to rate thechild’s level of functioning in a variety of areas ofdaily activity. Raters are asked to rate the currentlevel of functioning using a five-point Likert-typescale (ranging from 0 = extreme troubles to 4 =doing very well). The scores range from 0 to 80with a higher score indicating a higher level offunctioning (ODMH, 2006).
Ogles, Melendez, Davis, and Lunnen (2001)reported satisfactory reliability coefficients of theOhio Scale across multiple reporting sources thatrange from .65 to .97 and test–retest reliabilities thatare adequate and range from .43 to .88. In addition,the Ohio Scale ratings were significantly correlatedwith other established measures including, but notlimited to, the Progress Evaluation Scales (Ihilevich& Gleser, 1982), Child and Adolescent FunctionalAssessment Scales (Hodges & Wong, 1996), Child-ren’s Global Assessment Scale (Shaffer et al., 1983),Child Behavior Checklist (Achenbach, 1991), and
Lee et al. / Systems Collaboration with Schools and Treatment of Severely Emotionally Disturbed Children or Adolescents 7
Vanderbilt Functioning Index (Bickman, Lambert,Karver, & Andrade, 1998).
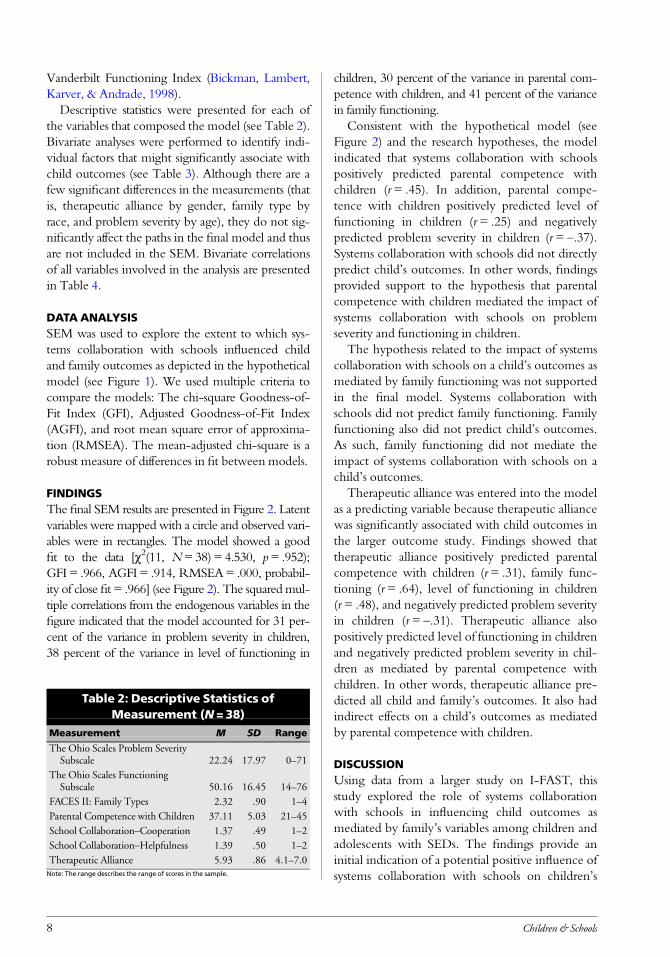
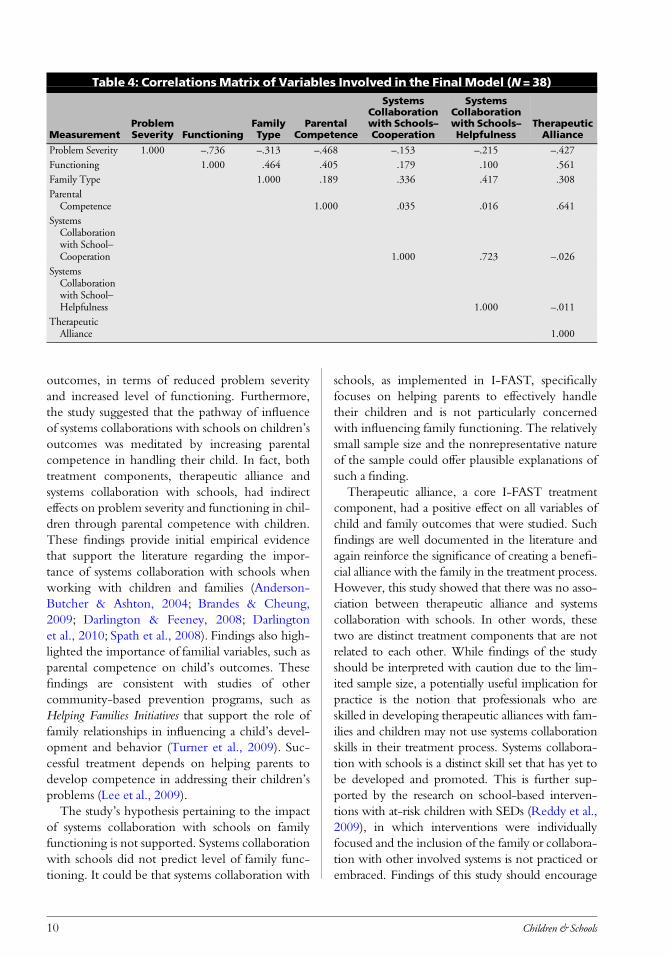
Descriptive statistics were presented for each ofthe variables that composed the model (see Table 2).Bivariate analyses were performed to identify indi-vidual factors that might significantly associate withchild outcomes (see Table 3). Although there are afew significant differences in the measurements (thatis, therapeutic alliance by gender, family type byrace, and problem severity by age), they do not sig-nificantly affect the paths in the final model and thusare not included in the SEM. Bivariate correlationsof all variables involved in the analysis are presentedin Table 4.
DATA ANALYSISSEM was used to explore the extent to which sys-tems collaboration with schools influenced childand family outcomes as depicted in the hypotheticalmodel (see Figure 1). We used multiple criteria tocompare the models: The chi-square Goodness-of-Fit Index (GFI), Adjusted Goodness-of-Fit Index(AGFI), and root mean square error of approxima-tion (RMSEA). The mean-adjusted chi-square is arobust measure of differences in fit between models.
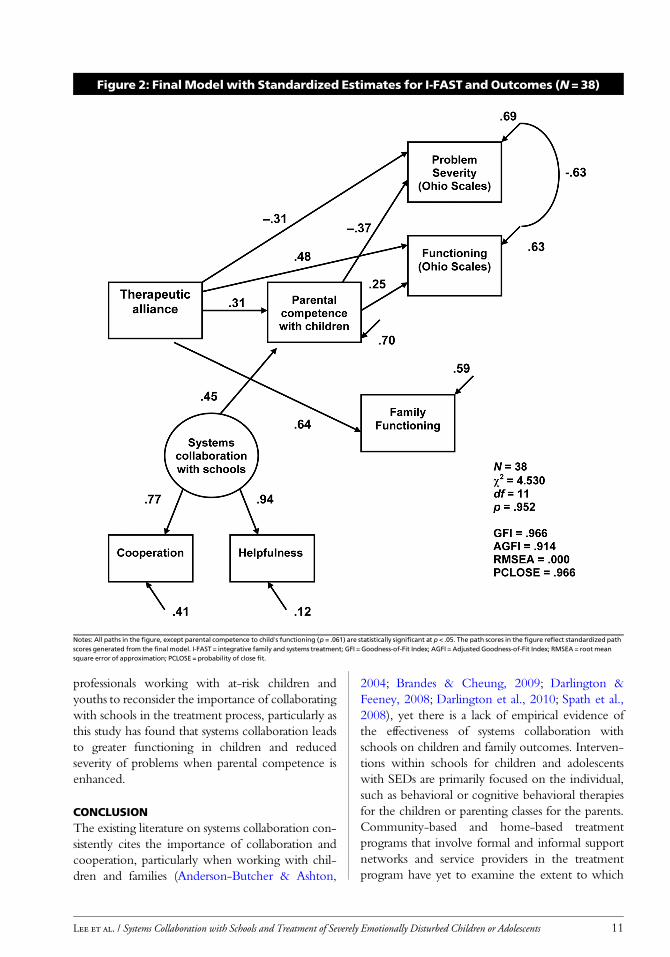
FINDINGSThe final SEM results are presented in Figure 2. Latentvariables were mapped with a circle and observed vari-ables were in rectangles. The model showed a goodfit to the data [χ2(11, N=38) = 4.530, p= .952);GFI = .966, AGFI = .914, RMSEA= .000, probabil-ity of close fit = .966] (see Figure 2). The squaredmul-tiple correlations from the endogenous variables in thefigure indicated that the model accounted for 31 per-cent of the variance in problem severity in children,38 percent of the variance in level of functioning in
children, 30 percent of the variance in parental com-petence with children, and 41 percent of the variancein family functioning.
Consistent with the hypothetical model (seeFigure 2) and the research hypotheses, the modelindicated that systems collaboration with schoolspositively predicted parental competence withchildren (r = .45). In addition, parental compe-tence with children positively predicted level offunctioning in children (r = .25) and negativelypredicted problem severity in children (r = –.37).Systems collaboration with schools did not directlypredict child’s outcomes. In other words, findingsprovided support to the hypothesis that parentalcompetence with children mediated the impact ofsystems collaboration with schools on problemseverity and functioning in children.
The hypothesis related to the impact of systemscollaboration with schools on a child’s outcomes asmediated by family functioning was not supportedin the final model. Systems collaboration withschools did not predict family functioning. Familyfunctioning also did not predict child’s outcomes.As such, family functioning did not mediate theimpact of systems collaboration with schools on achild’s outcomes.
Therapeutic alliance was entered into the modelas a predicting variable because therapeutic alliancewas significantly associated with child outcomes inthe larger outcome study. Findings showed thattherapeutic alliance positively predicted parentalcompetence with children (r = .31), family func-tioning (r = .64), level of functioning in children(r = .48), and negatively predicted problem severityin children (r= –.31). Therapeutic alliance alsopositively predicted level of functioning in childrenand negatively predicted problem severity in chil-dren as mediated by parental competence withchildren. In other words, therapeutic alliance pre-dicted all child and family’s outcomes. It also hadindirect effects on a child’s outcomes as mediatedby parental competence with children.
DISCUSSIONUsing data from a larger study on I-FAST, thisstudy explored the role of systems collaborationwith schools in influencing child outcomes asmediated by family’s variables among children andadolescents with SEDs. The findings provide aninitial indication of a potential positive influence ofsystems collaboration with schools on children’s
Table 2: Descriptive Statistics ofMeasurement (N = 38)
Measurement M SD Range
The Ohio Scales Problem SeveritySubscale 22.24 17.97 0–71
The Ohio Scales FunctioningSubscale 50.16 16.45 14–76
FACES II: Family Types 2.32 .90 1–4
Parental Competence with Children 37.11 5.03 21–45
School Collaboration–Cooperation 1.37 .49 1–2
School Collaboration–Helpfulness 1.39 .50 1–2
Therapeutic Alliance 5.93 .86 4.1–7.0Note: The range describes the range of scores in the sample.
8 Children & Schools
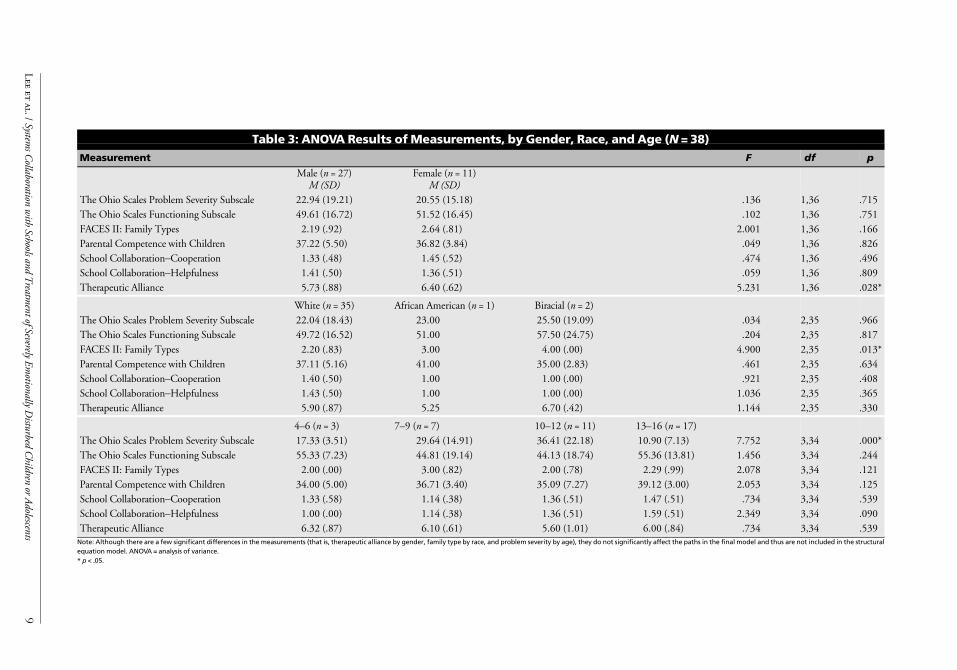
Table 3: ANOVA Results of Measurements, by Gender, Race, and Age (N = 38)
Measurement F df p
Male (n = 27)M (SD)
Female (n = 11)M (SD)
The Ohio Scales Problem Severity Subscale 22.94 (19.21) 20.55 (15.18) .136 1,36 .715
The Ohio Scales Functioning Subscale 49.61 (16.72) 51.52 (16.45) .102 1,36 .751
FACES II: Family Types 2.19 (.92) 2.64 (.81) 2.001 1,36 .166
Parental Competence with Children 37.22 (5.50) 36.82 (3.84) .049 1,36 .826
School Collaboration–Cooperation 1.33 (.48) 1.45 (.52) .474 1,36 .496
School Collaboration–Helpfulness 1.41 (.50) 1.36 (.51) .059 1,36 .809
Therapeutic Alliance 5.73 (.88) 6.40 (.62) 5.231 1,36 .028*
White (n = 35) African American (n = 1) Biracial (n = 2)The Ohio Scales Problem Severity Subscale 22.04 (18.43) 23.00 25.50 (19.09) .034 2,35 .966
The Ohio Scales Functioning Subscale 49.72 (16.52) 51.00 57.50 (24.75) .204 2,35 .817
FACES II: Family Types 2.20 (.83) 3.00 4.00 (.00) 4.900 2,35 .013*
Parental Competence with Children 37.11 (5.16) 41.00 35.00 (2.83) .461 2,35 .634
School Collaboration–Cooperation 1.40 (.50) 1.00 1.00 (.00) .921 2,35 .408
School Collaboration–Helpfulness 1.43 (.50) 1.00 1.00 (.00) 1.036 2,35 .365
Therapeutic Alliance 5.90 (.87) 5.25 6.70 (.42) 1.144 2,35 .330
4–6 (n = 3) 7–9 (n = 7) 10–12 (n = 11) 13–16 (n = 17)The Ohio Scales Problem Severity Subscale 17.33 (3.51) 29.64 (14.91) 36.41 (22.18) 10.90 (7.13) 7.752 3,34 .000*
The Ohio Scales Functioning Subscale 55.33 (7.23) 44.81 (19.14) 44.13 (18.74) 55.36 (13.81) 1.456 3,34 .244
FACES II: Family Types 2.00 (.00) 3.00 (.82) 2.00 (.78) 2.29 (.99) 2.078 3,34 .121
Parental Competence with Children 34.00 (5.00) 36.71 (3.40) 35.09 (7.27) 39.12 (3.00) 2.053 3,34 .125
School Collaboration–Cooperation 1.33 (.58) 1.14 (.38) 1.36 (.51) 1.47 (.51) .734 3,34 .539
School Collaboration–Helpfulness 1.00 (.00) 1.14 (.38) 1.36 (.51) 1.59 (.51) 2.349 3,34 .090
Therapeutic Alliance 6.32 (.87) 6.10 (.61) 5.60 (1.01) 6.00 (.84) .734 3,34 .539Note: Although there are a few significant differences in the measurements (that is, therapeutic alliance by gender, family type by race, and problem severity by age), they do not significantly affect the paths in the final model and thus are not included in the structuralequation model. ANOVA = analysis of variance.* p < .05.
Lee
etal./System
sCollaboration
with
SchoolsandTreatm
entofSeverelyEmotionally
Disturbed
Children
orAdolescents
9
outcomes, in terms of reduced problem severityand increased level of functioning. Furthermore,the study suggested that the pathway of influenceof systems collaborations with schools on children’soutcomes was meditated by increasing parentalcompetence in handling their child. In fact, bothtreatment components, therapeutic alliance andsystems collaboration with schools, had indirecteffects on problem severity and functioning in chil-dren through parental competence with children.These findings provide initial empirical evidencethat support the literature regarding the impor-tance of systems collaboration with schools whenworking with children and families (Anderson-Butcher & Ashton, 2004; Brandes & Cheung,2009; Darlington & Feeney, 2008; Darlingtonet al., 2010; Spath et al., 2008). Findings also high-lighted the importance of familial variables, such asparental competence on child’s outcomes. Thesefindings are consistent with studies of othercommunity-based prevention programs, such asHelping Families Initiatives that support the role offamily relationships in influencing a child’s devel-opment and behavior (Turner et al., 2009). Suc-cessful treatment depends on helping parents todevelop competence in addressing their children’sproblems (Lee et al., 2009).
The study’s hypothesis pertaining to the impactof systems collaboration with schools on familyfunctioning is not supported. Systems collaborationwith schools did not predict level of family func-tioning. It could be that systems collaboration with
schools, as implemented in I-FAST, specificallyfocuses on helping parents to effectively handletheir children and is not particularly concernedwith influencing family functioning. The relativelysmall sample size and the nonrepresentative natureof the sample could offer plausible explanations ofsuch a finding.
Therapeutic alliance, a core I-FAST treatmentcomponent, had a positive effect on all variables ofchild and family outcomes that were studied. Suchfindings are well documented in the literature andagain reinforce the significance of creating a benefi-cial alliance with the family in the treatment process.However, this study showed that there was no asso-ciation between therapeutic alliance and systemscollaboration with schools. In other words, thesetwo are distinct treatment components that are notrelated to each other. While findings of the studyshould be interpreted with caution due to the lim-ited sample size, a potentially useful implication forpractice is the notion that professionals who areskilled in developing therapeutic alliances with fam-ilies and children may not use systems collaborationskills in their treatment process. Systems collabora-tion with schools is a distinct skill set that has yet tobe developed and promoted. This is further sup-ported by the research on school-based interven-tions with at-risk children with SEDs (Reddy et al.,2009), in which interventions were individuallyfocused and the inclusion of the family or collabora-tion with other involved systems is not practiced orembraced. Findings of this study should encourage
Table 4: CorrelationsMatrix of Variables Involved in the Final Model (N = 38)
MeasurementProblemSeverity Functioning
FamilyType
ParentalCompetence
SystemsCollaborationwith Schools–Cooperation
SystemsCollaborationwith Schools–Helpfulness
TherapeuticAlliance
Problem Severity 1.000 –.736 –.313 –.468 –.153 –.215 –.427
Functioning 1.000 .464 .405 .179 .100 .561
Family Type 1.000 .189 .336 .417 .308
ParentalCompetence 1.000 .035 .016 .641
SystemsCollaborationwith School–Cooperation 1.000 .723 –.026
SystemsCollaborationwith School–Helpfulness 1.000 –.011
TherapeuticAlliance 1.000
10 Children & Schools
professionals working with at-risk children andyouths to reconsider the importance of collaboratingwith schools in the treatment process, particularly asthis study has found that systems collaboration leadsto greater functioning in children and reducedseverity of problems when parental competence isenhanced.
CONCLUSIONThe existing literature on systems collaboration con-sistently cites the importance of collaboration andcooperation, particularly when working with chil-dren and families (Anderson-Butcher & Ashton,
2004; Brandes & Cheung, 2009; Darlington &Feeney, 2008; Darlington et al., 2010; Spath et al.,2008), yet there is a lack of empirical evidence ofthe effectiveness of systems collaboration withschools on children and family outcomes. Interven-tions within schools for children and adolescentswith SEDs are primarily focused on the individual,such as behavioral or cognitive behavioral therapiesfor the children or parenting classes for the parents.Community-based and home-based treatmentprograms that involve formal and informal supportnetworks and service providers in the treatmentprogram have yet to examine the extent to which
Figure 2: Final Model with Standardized Estimates for I-FAST and Outcomes (N = 38)
Notes: All paths in the figure, except parental competence to child’s functioning (p = .061) are statistically significant at p < .05. The path scores in the figure reflect standardized pathscores generated from the final model. I-FAST = integrative family and systems treatment; GFI = Goodness-of-Fit Index; AGFI = Adjusted Goodness-of-Fit Index; RMSEA = root meansquare error of approximation; PCLOSE = probability of close fit.
Lee et al. / Systems Collaboration with Schools and Treatment of Severely Emotionally Disturbed Children or Adolescents 11

such systems collaboration has influenced the out-comes for children and families. The present studyshould be viewed as a preliminary effort to explorethe effect of systems collaboration on treatment out-comes through the use of empirical data.
Limitations of the study must be acknowledged.First, due to the exploratory nature of this researchand also practical limitations of subject recruitmentin intervention field research, the study sample sizewas relatively small. Bentler and Chou (1987) sug-gested that the ratio of sample size to free parame-ters can go as low as 5 to 1 in structural modeling.Still, the sample size of this study did not meet therecommended guideline. As such, findings of thestudy should be interpreted with caution. Anotherlimitation of the present study was the use of self-reports from I-FAST case managers and not theteachers or other school personnel to measure sys-tems collaboration with schools. As such, data onsystems collaboration with schools only repre-sented the perceptions of the case manager andcould be biased. In addition, the Systems Collabo-ration Scale assesses the degree of cooperation andhelpfulness of collaboration with other service sys-tems by a single-item, three-level Likert-type scalemeasures. The use of single-item measures wouldpotentially increase the likelihood of measurementerrors. Finally, participating families were mostlywhite Americans; other ethnic and racial groups,including African-, Asian-, Hispanic-, and Native-American populations, were largely underrepre-sented. Although limitations of the study clearlypreclude any definitive conclusions, findings of thestudy do provide initial indication of the potentialpositive influences of systems collaboration withschools on a child’s outcomes in terms of reducedproblem severity and increased level of functioning.
Although the present study provided preliminaryevidence as to the benefits of systems collaborationwith schools on family and child outcomes, findingsof the study should be interpreted with cautionbecause of the small sample size. Future research isneeded to fully examine the effectiveness of systemscollaboration as an intervention, as well as to refinethe mechanisms of change related to it. Seven spe-cific recommendations for future investigations are asfollows: (1) Use a larger sample size that uses repre-sentative samples; (2) include control or comparisongroups using randomized assignment procedures; (3)use more refined, multiple-item, or standardizedinstruments to measure studied variables that would
decrease the likelihood of measurement errors; (4)use multiple reporting sources to avoid reportingbias; (5) include research sites that serve more ethni-cally and racially diverse populations; (6) examinesystems collaboration with other systems, in additionto schools for a broader understanding of the phe-nomenon; and (7) use multiple research methods,both quantitative and qualitative, to identify themechanisms of change associated with systems col-laboration as part of the treatment process.
REFERENCESAchenbach, T. M. (1991).Manual for the Child Behavior
Checklist and 1991 profile. Burlington: University ofVermont, Department of Psychiatry.
Anderson-Butcher, D., & Ashton, D. (2004). Innovativemodels of collaboration to serve children, youths, fam-ilies, and communities. Children & Schools, 26, 39–53.
Armstrong, K. H., Dedrick, R. F., & Greenbaum, P. E.(2003). Factors associated with community adjustmentof young adults with serious emotional disturbance: Alongitudinal analysis. Journal of Emotional and BehavioralDisorders, 11, 66–76.
Asay, T. P., & Lambert, M. J. (1999). The empirical case forthe common factors in therapy: Quantitative findings.In M. A. Hubble, B. L. Duncan, & S. Miller (Eds.),The heart and soul of change: What works in therapy (pp.23–55). Washington, DC: American PsychologicalAssociation.
Bentler, P. M., & Chou, C. P. (1987). Practical issues instructural modeling. Sociological Methods and Research,16, 78–117.
Berg-Weger, M., & Schneider, F. D. (1998). Interdisciplin-ary collaboration in social work education. Journal ofSocial Work Education, 34, 97–107.
Bickman, L., Lambert, E. W., Karver, M., & Andrade, A. R.(1998). Two low-cost measures of child and adolescentfunctioning for services research. Evaluation and ProgramPlanning, 21, 263–275.
Borduin, C., Mann, B., Cone, L., Henggeler, S., Fucci, B.,Blaske, D., et al. (1995). Multisystemic treatment ofserious juvenile offenders: Long term prevention ofcriminality and violence. Journal of Consulting and Clin-ical Psychology, 63, 569–578.
Brandes, B. J., & Cheung, M. (2009). Supervision and treat-ment of juveniles with sexual behavior problems.Child and Adolescent Social Work Journal, 26, 179–196.
Brauner, C. B., & Stephens, C. B. (2006). Estimating theprevalence of early childhood serious emotional/behavioral disorders: Challenges and recommenda-tions. Public Health Reports, 121, 303–310.
Bronstein, L. R. (2003). A model for interdisciplinary col-laboration. Social Work, 48, 297–306.
Bruner, C. (1991). Ten questions and answers to help policymakers improve children’s services. Washington, DC: Edu-cation and Human Services Consortium.
Bruns, E. J., Leverentz-Brady, K. M., & Suter, J. C. (2008).Is it wraparound yet? Setting quality standards forimplementation of the wraparound process. Journal ofBehavioral Health Services and Research, 35, 240–252.
Bruns, E. J., Rast, J., Walker, J. S., Bosworth, J., & Peterson,C. (2006). Spreadsheets, service providers, and thestatehouse: Using data and the wraparound process toreform systems for children and families. American Jour-nal of Community Psychology, 38, 201–212.
Bruns, E. J., Walker, J. S., Zabel, M., Matarese, M., Estep,K., Harburger, D., & Pires, S. A. (2010). Intervening
12 Children & Schools

in the lives of youth with complex behavioral healthchallenges and their families: The role of the wrap-around process. American Journal of Community Psychol-ogy, 46, 314–331.
Campis, L. K., Lyman, R. D., & Prentice-Dunn, S. (1986).The Parental Locus of Control Scale: Developmentand validation. Journal of Clinical Child Psychiatry, 15,260–267.
Carney, M. M., & Buttell, F. (2003). Reducing juvenilerecidivism: Evaluating the wraparound services model.Research on Social Work Practice, 13, 551–568.
Chuang, E., & Wells, R. (2010). The role of inter-agencycollaboration in facilitating receipt of behaviouralhealth services for youth involved with child welfareand juvenile justice. Children and Youth Services Review,32, 1814–1822.
Darlington, Y., & Feeney, J. A. (2008). Collaborationbetween mental health and child protection services:Professionals’ perceptions of best practice. Children andYouth Services Review, 30, 187–198.
Darlington, Y., Feeney, J. A., & Rixon, K. (2005). Inter-agency collaboration between child protection andmental health services: Practices, attitudes and barriers.Child Abuse & Neglect, 29, 1085–1098.
Darlington, Y., Healy, K., & Feeney, J. A. (2010).Approaches to assessment and intervention across fourtypes of child and family welfare services. Children andYouth Services Review, 32, 356–364.
De Martini-Scully, D., Bray, M. A., & Kehle, T. J. (2000).A packaged intervention to reduce disruptive behav-iors in general education students. Psychology in theSchools, 37, 149–156.
Diamond, G. S., Liddle, H. A., Wintersteen, M. B., Dennis,M. L., Godley, S. H., & Tims, F. (2006). Early thera-peutic alliance as a predictor of treatment outcome foradolescent cannabis users in outpatient treatment.American Journal of Addictions, 15, 26–33.
Ditrano, C. J., & Silverstein, L. B. (2006). Listening to par-ents’ voices: Participatory action research in theschools. Professional Psychology, Research and Practice, 37,359–366.
Foltz, R. (2004). The efficacy of residential treatment: Anoverview of the evidence. Residential Treatment forChildren & Youth, 22(2), 1–19.
Fraser, J. S., Solovey, A. D., Grove, D., Lee, M. Y., &Greene, G. J. (2012). Integrative families in systemstreatment: A middle path towards integratingcommon and specific factors in evidence based familytherapy. Journal of Marital and Family Therapy, 38,515–528.
Hampson, R. B., Hulgus, Y. F., & Beavers, W. R. (1991).Comparisons of self-report measures of the Beaverssystems model and Olson’s circumplex model. Journalof Family Psychology, 4, 326–340.
Heatherington, L., & Friedlander, M. L. (1990). Coupleand family therapy alliance scales: Empirical consider-ations. Journal of Marital and Family Therapy, 16,299–306.
Hodges, K., & Wong, M. M. (1996). Psychometric charac-teristics of a multidimensional measure to assessimpairment: The Child and Adolescent FunctionalAssessment Scale. Journal of Child and Family Studies, 5,445–467.
Huxham, C., & Vangen, S. (2000). What makes partner-ships work? In S. Osborne (Ed.), Public private partner-ships (pp. 202–216). London: Routledge.
Ihilevich, D., & Gleser, G. C. (1982). Evaluating mentalhealth programs: The Progress Evaluation Scale. Lexington,MA: Lexington Books.
Johnson, L. N., Wright, D. W., & Ketring, S. A. (2002).The therapeutic alliance in home-based family
therapy: Is it predictive of outcome? Journal of Maritaland Family Therapy, 28, 93–102.
Johnson, P., Wistow, G., Schultz, R., & Hardy, B. (2003).Interagency and interprofessional collaboration incommunity care: The interdependence of structuresand values. Journal of Interprofessional Care, 17, 69–83.
Kernan, J. B., & Morilus-Black, M. (2010). Social supportsfor youth and families. Community Mental Health Jour-nal, 46, 258–264.
Kutash, K., Duchnowski, A. J., Sumi, C. W., Rudo, Z., &Harris, K. M. (2002). A school, family, and commu-nity collaborative program for children who haveemotional disturbances. Journal of Emotional and Behav-ioral Disorders, 10, 99–107.
Lakin, B. L., Brambila, A. D., & Sigda, K. B. (2005). Behav-ioral managed care and its effects in the readmission toa children’s residential treatment center. ResidentialTreatment for Children & Youth, 24, 315–326.
Lane, K. L., Carter, E. W., Pierson, M. R., & Glaeser, B. C.(2006). Academic, social, and behavioral characteristicsof high school students with emotional disturbances orlearning disabilities. Journal of Emotional and BehavioralDisorders, 14, 108–117.
Lazicki, T. A., Vernberg, E. M., Roberts, M. C., & Benson,E. R. (2008). Satisfaction with components of thetherapeutic model: Perspectives of consumers and pro-fessionals. Journal of Child Family Studies, 17, 264–276.
Lee, M. Y., & Greene, G. J. (2002). Systems CollaborationScale. Columbus, OH: Authors.
Lee, M. Y., Greene, G. J., Hsu, K. S., Solovey, A., Grove,D., Fraser, J. S., et al. (2009). Utilizing familystrengths and resilience: Integrative family and systemstreatment with children and adolescents with severeemotional and behavioral problems. Family Process, 48,395–416.
Lee, M. Y., Greene, G. J., Solovey, A., Grove, D., & Fraser,S. (2003). The Integrative Family and Systems TreatmentChecklist. Columbus, OH: Authors.
Lee, M. Y., Teater, B., Greene, G. J., Solovey, A., Grove,D., Fraser, J. S., & Hsu, K. S. (2012). Key processes,ingredients and components of successful systems col-laboration: Working with severely emotionally orbehaviorally disturbed children and their families.Administration and Policy in Mental Health and MentalHealth Services Research, 39, 394–405.
Mark, T. L., & Buck, J. A. (2006). Characteristics of U.S.youth with serious emotional disturbance: Data fromthe National Health Interview Survey. Psychiatric Ser-vices, 57, 1573–1578.
McLendon, T. (2008). Best practices to engage parents ofchildren receiving mental health services. In C. G. Petr(Ed.),Multidimensional evidence-based practice: Synthesizingknowledge, research and values (pp. 108–131). New York:Routledge.
Mears, S. L., Yaffe, J., & Harris, N. J. (2009). Evaluation ofwraparound services for severely emotionally disturbedyouths. Research on Social Work Practice, 19, 678–685.
Milbourne, L. (2005). Children, families and inter-agencywork: Experiences of partnership work in primaryeducation settings. British Education Research Journal,31, 681–701.
Milbourne, L., Macrae, S., & Maguire, M. (2003). Collabo-rative solutions or new policy problems: Exploringmulti-agency partnerships in education and healthwork. Journal of Education Policy, 18, 19–35.
Mottram, L. M., Bray, M. A., Kehle, T. J., Broudy, M., &Jenson, W. R. (2002). A classroom-based interventionto reduce disruptive behaviors. Journal of Applied SchoolPsychology, 19, 65–74.
Musser, E. H., Bray, M. A., Kehle, T. J., & Jenson, W. R.(2001). Reducing disruptive behaviors in students
Lee et al. / Systems Collaboration with Schools and Treatment of Severely Emotionally Disturbed Children or Adolescents 13

with serious emotional disturbance. School PsychologyReview, 30, 294–304.
National Dissemination Center for Children with Disabili-ties (NICHCY). (2010). Disability fact sheet #5.Retrieved from http://nichcy.org/wp-content/uploads/docs/fs5.pdf
Ogles, B. M., Lambert, M. J., & Masters, K. S. (1996).Assessing outcome in clinical practice. Boston: Allyn &Bacon.
Ogles, B. M., Melendez, G., Davis, D., & Lunnen, K. M.(2001). The Ohio Scales: Practical outcome assess-ment. Journal of Child and Family Studies, 10, 199–212.
Ohio Department of Mental Health. (2006). The statewidereport, Vol. 12. Columbus: Author.
Olson, D. H. (1992). Family inventories manual.Minneapolis:Life Innovations.
Olson, D. H., Portner, J., & Bell, R. Q. (1982). FACES II:Family adaptability and cohesion evaluation scales. St. Paul:Family Social Sciences, University of Minnesota.
Ouellette, P. M., Briscoe, R., & Tyson, C. (2004). Parent-school and community partnerships in children’s mentalhealth: networking challenges, dilemmas, and solutions.Journal of Child and Family Studies, 13, 295–308.
Passaro, P. D., Moon, M., Wiest, D. J., & Wong, E. H.(2004). A model for school psychology practice:Addressing the needs of students with emotional andbehavioral challenges through the use of an in-schoolsupport room and reality therapy. Adolescence, 39,503–517.
Pinsof, W. M. (2003). Family Therapy Alliance Scale. Evans-ton, IL: The Family Institute.
Pinsof, W. M., & Catherall, D. R. (1986). The integrativepsychotherapy alliance: Family, couple, and individualtherapy scales. Journal of Marital and Family Therapy, 12,137–151.
Pullman, M. A., Kerbs, J., Koroloff, N., Veach-White, E.,Gaylore, R., & Sieler, D. D. (2006). Juvenile offenderswith mental health needs: Reducing recidivism usingwraparound. Crime and Delinquency, 52, 375–397.
Radohl, T. (2011). Incorporating family into the formula:Family-directed structural therapy for children withserious emotional disturbance. Child & Family SocialWork, 16, 127–137.
Rapport, M. D., Denney, C. B., Chung, K. M., & Hustace,K. (2001). Internalizing behavior problems and scho-lastic achievement in children: Cognitive and behavio-ral pathways as mediators of outcome. Journal ofClinical Child Psychology, 30, 536–551.
Reddy, L. A., De Thomas, C. A., Newman, E., & Chun,V. (2009). School-based prevention and interventionprograms for children with emotional disturbance: Areview of treatment components and methodology.Psychology in the Schools, 46, 132–153.
Reddy, L. A., & Richardson, L. (2006). School-based pre-vention and intervention programs for children withemotional disturbance. Education and Treatment ofChildren, 29, 1–26.
Richards, M. M., Bowers, M. J., Lazicki, T., Krall, D., &Jacobs, A. K. (2008). Caregiver involvement in theIntensive Mental Health Program: Influence onchanges in child functioning. Journal of Child and Fam-ily Studies, 17, 241–252.
Riddell, S., & Tett, L. (2001). Education, social justiceand inter-agency working: Joined up or fractured policy?London: Routledge.
Shaffer, D., Gould, M. S., Brasic, J., Ambrosini, P., Fisher,P., Hector, B., et al. (1983). Children’s Global Assess-ment Scale (CGAS). Archives of General Psychiatry, 40,1228–1231.
Spath, R., Werrbach, G. B., & Pine, B. A. (2008). Sharingthe baton, not passing it: Collaboration between
public and private child welfare agencies to reunifyfamilies. Journal of Community Practice, 16, 481–507.
Substance Abuse and Mental Health Administration.(1993). Definition of mental illness and emotional dis-turbance in children. Federal Register, 58,29422–29425.
Torres, G.W., & Margolin, F. S. (2003). The collaborationprimer: Proven strategies, considerations and tools to get youstarted. Chicago: Health Research and EducationalTrust.
Turner, L. A., Powell, A. E., Langhinrichsen-Rohling, J., &Carson, J. (2009). Helping families initiative: Interven-ing with high-risk students through a community,school, and district attorney partnership. Child Adoles-cent Social Work Journal, 26, 209–223.
U.S. Department of Education, Office of Special EducationPrograms. (2001). Twenty-third annual report to Congresson the implementation of the Individuals with DisabilitiesEducation Act: Results.Washington, DC: Author.
Vernberg, E. M., Roberts, M. C., & Nyre, J. E. (2008). TheIntensive Mental Health Program: Developmentstructure of the model of intervention for childrenwith serious emotional disturbances. Journal of Childand Family Studies, 17, 169–177.
Wagner, M., Friend, M., Bursuck, W. D., Kutash, K.,Duchnowski, A. J., Sumi, W. C., et al. (2006). Educat-ing students with emotional disturbance: A nationalperspective on school programs and services. Journal ofEmotional and Behavioral Disorders, 14, 12–30.
Wagner, M., Kutash, K., Duchnowski, A. J., Epstein, M. H.,& Sumi, W. C. (2005). The children and youth weserve: A national picture of the characteristics of studentswith emotional disturbances receiving special educa-tion. Journal of Emotional and Behavioral Disorders, 13,79–96.
Walter, J. M., & Petr, C. (2000). A template for family-centered interagency collaboration. Families in Society,8, 494–503.
Mo Yee Lee, PhD, RSW, is professor, College of Social Work,Ohio State University–Columbus, 340A Stillman Hall, 1947College Road, Columbus, OH 43210; e-mail: [email protected]. Barbra Teater, PhD, is senior lecturer, School for PolicyStudies, University of Bristol, United Kingdom. Kai ShyangHsu, PhD, is assistant professor, Fu Jen Catholic University ofSocial Work, New Taipei City, Taiwan. Gilbert J. Greene,PhD, LISW, ACSW, is professor, College of Social Work,Ohio State University–Columbus. J. Scott Fraser, PhD,ABPP, is professor, School of Professional Psychology, WrightState University, Dayton, OH. Andrew D. Solovey, MA,ACSW, is therapist/consultant, Solution Counseling, Dubin,OH. David Grove, MSW, LISW, is therapist/consultant andcodirector, Family Therapy Institute of Columbus, Westerville,OH. This study was supported by the Ohio Department ofMental Health, Grant #744832.
Original manuscript received October 3, 2011Final revision received February 1, 2012Accepted February 29, 2012
14 Children & Schools





























