Embed Size (px)
Citation preview

�9 1995 by Humana Press Inc. All rights of any nature whatsoever reserved. 1044-7393/95/2603--0231 $07.00
tau Protein in Cerebrospinal Fluid
A Biochemical Marker for Axonal Degeneration in Alzheimer Disease?
K. BLENNOW, "'1 A. WALLIN, 2 H. AGREN, 2 C . S P E N G E R , 3 a . SIEGFRIED, 4 AND E . VANME C HE L E N 5
Department of Clinical Neuroscience, 1 Unit of Neurochemistry, 2Unit of Psychiatry, University of GOteborg, Molndal Hospital,
S-431 80 MOlndal, Sweden; 3Department of Neurosurgery, University of Bern, Switzerland; 4Klinik im Park, Zhrich, Switzerland;
and 51nnogenetics N. V., Ghent, Belgium
Received April 10, 1995; Accepted April 27, 1995
ABSTRACT
Cerebrospinal fluid (CSF) biochemical markers for Alzheimer disease (AD) would be of great value to improve the clinical diagnostic accuracy of the disorder. As abnormally phosphorylated forms of the microtubule-associated protein tau have been consistently found in the brains of AD patients, and since tau can be detected in CSF, two assays based on several well-defined monoclonal tau antibodies were used to study these proteins in CSF. One assay detects most normal and abnormal forms of tau (CSF-tau), while the other is highly specific for phosphorylated tau (CSF-PHFtau). A marked increase in CSF- PHFtau was found in AD (2230 + 930 pg/mL), as compared with controls (640 + 230 pg/mL; p < 0.0001), vascular dementia, VAD (1610 + 840 pg/mL; p < 0.05), frontal lobe dementia, FLD (1530 + 1000 pg/mL; p < 0.05), Parkinson disease, PD (720 + 590 pg/mL; p < 0.0001), and patients with major depression (230 + 130 pg/mL; p < 0.0001). Parallel results were obtained for CSF-tau. No less than 35/40 (88%) of AD patients had a CSF-PHFtau value higher than the cutoff level of 1140 pg/mL in controls. The present study demonstrates that elevated tau/PHFtau levels are consistently found in CSF of AD patients.
*Author to whom all correspondence and reprint requests should be addressed.
Molecular and Chemical Neuropathology 231 VoL 26, 1995

232 B l e n n o w et al.
However, a considerable overlap is still present with other forms of dementia, both VAD and FLD. CSF-tau and CSF-PHFtau may there- fore be useful as a positive biochemical marker, to discriminate AD from normal aging, PD, and depressive pseudodementia. Further stud- ies are needed to clarify the sensitivity and specificity of these assays, including follow-up studies with neuropathological examinations.
Index Entries: Alzheimer disease (AD); biochemical markers; cerebrospinal fluid (CSF); tau protein.
INTRODUCTION
Alzheimer disease (AD) is the most common form of dementia. Some relatively rare genetic forms of AD do exist, but the majority of patients have no obvious family history and are classified as suffering from spor- adic AD. Although new research criteria for the clinical diagnosis of pure AD have been proposed (Wallin et al., 1994), the clinical diagnosis of spor- adic AD continues to be made by way of exclusion (McKhann et al., 1984), without the support of any positive diagnostic criteria. Therefore, bio- chemical markers for AD would be of great use, both to improve the clini- cal diagnostic accuracy in scientific studies and treatment trials, and to increase our knowledge concerning the underlying pathogenesis of the disorder. These markers should reflect the pathological changes in the brain, i.e., the degeneration of neurones and their synapses (Coleman and Flood, 1987; Davies et al., 1987; Hamos et al., 1989), as well as the in- creased number of senile plaques (SPs) and neurofibrillary tangles (NFTs) compared with those found in nondemented individuals of similar age (Tomlinson and Corsellis, 1984).
The normal tau protein is a human brain phosphoprotein with six iso- forms ranging in size from 352-441 amino acids (Goedert et al., 1988; Harrington et al., 1991), which binds to tubulin in the microtubules, thereby promoting microtubule assembly and stability (for a review, see Goedert, 1993). In AD, however, the principal component of the paired helical fila- ments (PHFs), which make up the characteristic NFTs, neuropil threads, and senile plaque neurites, is probably an abnormally hyperphosphory- lated form of tau protein (PHFtau) (Grundke-Iqbal et al., 1986; Ihara et al., 1986). PHFtau is also called A68 (Wolozin and Davies, 1987), Alzheimer disease associated proteins (ADAP) (Ghanbari et al., 1990), and tau 64/69 (Delacourte et al., 1990).
The concentration of PHF-tau, is increased in cortical AD brain homog- enates (Wolozin and Davies, 1987; Bissette et al., 1991; Harrington et al., 1991; Mukaetova-Ladinska et al., 1992; Bramblett et al., 1992; Khatoon et al., 1992; Mercken et al., 1992; Harrington et al., 1994), whereas the con- centration of normal tau is reduced (Bramblett et al., 1992; Mukaetova- Ladinska et al., 1992; Harrington et al., 1994). These findings are con- sistent with studies reporting that the tau mRNA level is unchanged in
Molecular and Chemical Neuropathology Vol. 26, 199_5

Tau Protein in CSF in AD 233
AD (Goedert et al., 1988; Oyama et al., 1991), suggesting a hyperphos- phorylation of normal tau rather than an increased synthesis of tau protein.
Since the extracellular space in the brain is continuous with the cere- brospinal fluid (CSF), analysis of CSF may reflect biochemical changes in the brain. Although PHF-tau in NFTs has low solubility (Delacourte et al., 1990; Harrington et al., 1991), antibodies against tau stain not only NFTs but also the cytoplasm in neurons devoid of NFTs (Wolozin and Davies, 1987; Hyman et al., 1988; Bancher et al., 1989). PHFtau may also be ex- tracted from AD brain tissue in buffers without detergents, suggesting that phosphorylation of tau protein to PHFtau is an early event in the for- mation of PHFs and NFTs, preceding its aggregation and incorporation into insoluble PHFs (Hyman et al., 1988; Bancher et al., 1989; Greenberg and Davies, 1990). Therefore, soluble PHF-tau may also be present in CSF. Several researchers have also attempted to measure PHF-tau in CSF. Usin~ the monoclonal antibody (MAb) 5-25 against PHFs, Mehta and coworkers (1985) found high levels of "paired helical filaments antigen" in CSF from AD patients. However, further studies have revealed that the epitope recognized by MAb 5-25 consists of ubiquitin residues 64-76 (Perry et al., 1987), and that MAb 5-25 recognizes a variety of proteins conjugated to ubiquitin in CSF (Wang et al., 1991). Another study reported an increase of A68 in a small series of AD patients (Wolozin and Davies, 1987), but this finding has not been confirmed in a large series of patients and controls.
In the present study, we report data on tau protein in CSF as a poten- tial biochemical marker for AD, using two different enzyme-linked immu- nosorbent assays (ELISAs) for determination of total tau (both normal tau and PHF-tau) and PHFtau in unconcentrated CSF.
MATERIALS AND METHODS
Pat ien t s a nd Controls
All patients underwent a thorough clinical investigation that included a medical history, physical, neurological, and psychiatric examination, screening laboratory tests, ECG, X-ray of the chest, EEG, and computer- ized tomography (CT) of the brain. In demented patients, the severity of dementia was evaluated according to the DSM-[[I-R criteria (APA, 1987). All clinical diagnoses were made without knowledge of the results from the biochemical analyses and vice versa.
The AD group included 44 patients, 20 men and 24 women, mean age + SD 72.4 + 7.3 yr. The diagnosis of "probable AD" was made by exclu- sion, in accordance with the NINCDS-ADRDA criteria (McKhann et al., 1984). In short, "'probable AD" was diagnosed in cases with:
1. Progressive dementia with deficits in two or more areas of cognition,
2. No disturbance of consciousness;
Molecular and Chemical Neuropathology Vol. 26, I 995

234 B l e n n o w et al.
3. Onset between ages 40 and 90; and 4. Absence of systemic disorders or other brain diseases that alone
could account for the progressive deficits in memory and cog- nition, such as depression, normal-pressure hydrocephalus, and metabolic disturbances.
The vascular dementia (VAD) group composed 17 patients, eight men and nine women, mean age + SD 69.8 + 6.4 yr. VAD was diagnosed in patients with transitory ischemic attacks and/or stroke episodes in relation to the evolution of dementia and/or CT findings of large infarcts and/or multiple lacunas (Wallin and Blennow, 1991). The frontal lobe dementia (FLD) group included 11 patients, five men and six women, mean age + SD 66.9 + 6.6 yr. FLD was diagnosed in cases with marked frontal lobe symptoms early in the course of the disease, without predominant parietal lobe symptoms, and with no signs of cerebrovascular damage, according to recommendat ions by Gustafson (1987). The Parkinson disease (PD) without dementia group was composed of 15 patients, 12 men and three women, mean age + SD 63.8 + 9.2 yr. The diagnosis of PD was made according to recommendat ions by Langston et al. (1992). Briefly, all PD patients showed at least two out of three features of bradykinesia, rigid- ity, or resting tremor, and all PD patients were responsive to L-dopa treatment. The major depression without dementia group, diagnosed according to the DSM-III-R criteria (APA, 1987), included 10 patients, five men and five women, mean age + SD 54.8 + 8.4 yr.
The control group consisted of individuals without histories, symp- toms, or signs of psychiatric or neurological disease, malignant disease, or systemic disorders (e.g., rheumatoid arthritis, infectious disease). This group included 31 individuals, 19 men and 12 women, mean age + SD 64.7 • 6.4 yr. In those individuals over 60 yr of age, the cognitive status was examined using the Mini-Mental State examination (Folstein et al., 1975). Individuals with scores below 28 were excluded.
The study was approved by the Ethics Committee, University of Goteborg. All patients (or their nearest relatives) and the controls gave their informed consent to participate in the study, which was conducted in accordance with the provisions of the Helsinki Declaration.
Cerebrosplnal Fluid Analyses In the AD, VAD, FLD, depression, and control groups, CfiF samples
were obtained by lumbar puncture in the L3/L4 or L4/L5 interspace. The first 12 mL of CfiF was collected and gently mixed to avoid gradient effects (Blennow et al., 1993). In the PD group, CSF samples were obtained during therapeutic stereotactic intracerebral neurosurgery. A serum sample was taken at the same time. All CSF samples with more than 500 erythrocytes per microliter were excluded. The CSF and serum samples were centri- fuged in 2000g for 10 min to eliminate cells and other insoluble material and was then stored at - 80~ until biochemical analyses.
Molecular and Chemical Neuropathology Vol. 26. 1995

Tau Protein in CSF in AD 235
Quantitative determination of albumin in serum and CSF was performed using the Behring Nephelometer Analyzer (Behringwerke AG, Marburg, Germany). The CSF/S albumin ratio (Tibbling et al., 1977) was calculated as: [CSF-albumin (mg/L)/S-albumin (g/L)], and was used as the measure of the blood-brain barrier (BBB) function. The CSF/S albumin ratio was determined in the AD, VAD, FLD, and controls groups.
Tau protein in CSF was measured using two different sandwich ELISAs. Both tests are based on the same principle. Monoclonal anti- bodies used to capture the antigen are coated at a final antibody concen- tration of 5 #g/mL in 10 rnM NaC1, 10 mM Na-azide, 10 mM Tris, pH 8.6, overnight at 4~ in high-binding microtiter plates (Nunc, Gibco, Paisley, UK). After blocking with 1% BSA in PBS for I h at 37~ the plates were incubated with an appropriately diluted tau standard or with CSF samples (25/~L for the CSF-tau assay and 100 #L for the PHF-tau assay) for 2 h at 37~ The plates were then washed four times with PBS, 0.05% Tween 20 (v/v), and 100/~L of highly purified biotinylated antibodies were added at 20 ng/mL and incubated for I h at 37~ Following washing with PBS/ Tween 20, 100 #L of streptavidin horseradish peroxidase complex (Jack- son Laboratories, Westgrove, PA, 1/10000) was added for 30' at room temperature. After a final washing 100 /~L of 0.42 mM 3,5,3',5'-tetra- methylbenzidine, 0.003% (v/v) H~O2 in 100 mM citric acid, and Na2HPO~ pH 4.3 were added as peroxidase substrate. The reaction was stopped with 100 #L of a 1M H2SO 4 solution. Absorbance was read in a Titertek Multiscan (Flow Laboratories, Eflab Oy, Finland) at 450 nm. Optical den- sity values obtained from the CSF samples were compared with standard curves generated from known quantities of purified tau material.
In the first ELISA, constructed to measure total tau (normal tau and PHFtau), the MAb AT120 was used as capturing antibody and two bio- tinylated MAbs (HT7 and BT2) were used as detection antibodies. MAb AT120 reacts equally well with both normal and hyperphosphorylated human tau protein (Vandermeeren et al., 1993), MAb HT7 also reacts equally well with both normal and hyperphosphorylated human tau pro- tein, whereas MAb BT2 preferentially recognizes normal tau (Goedert et al., 1994). Affinity purified tau protein was used as standard, prepared as described previously (Mercken et al., 1992). Tau protein concentration of the standard was determined by amino acid composition on a 420 A/H amino acid analyzer (Applied Bio-systems B.V., Maarssen, the Netherlands).
In the second ELISA, constructed to measure PHFtau specifically, the MAbs AT180 and AT270 were used as capturing antibodies, and two bio- tinylated MAbs (HT7 and AT120) were used as detection antibodies. MAbs AT180 and AT270 have been shown to recognize specifically phosphory- lated threonine 18 and threonine 231, respectively, on human tau (Goedert et al., 1994). Hyperphosphorylated recombinant tau protein was used as standard, prepared as described previously (Goedert et al., 1991), and the concentration of recombinant tau was determined prior to phosphoryla- tion by amino acid analysis as described. In vitro phosphorylated tau was
Molecular and Chemical Neuropathology Vol. 26, 1995

236 Blennow et al.
used as standard, because these tau form gave consistently the same results in ELISA, whereas PHF-tau isolated from Alzheimer brains gave small but statistically significant differences in the assays (unpublished results). On immunoblot t ing of human brain tissue, MAbs AT180 and AT270 recognized all three PHFtau bands, but also some of the six non- phosphorylated human brain tau isoforms (Goedert et al., 1994).
S t a t i s t i c a l Analysis A fully factorial multiple ANOVA was performed with CSF-tau and
CSF-PHFtau respectively as dependent variables, age, duration, and severity of dementia as covariates, and diagnostic category (AD, VAD, FLD, PD, depression, and healthy controls) as factor. For comparisions between groups, the Mann-Whitney U-test was used when comparing two groups, and the Kruskal-Wallis test was used when comparing more than two groups. The Spearman correlation coefficient was used for cor- relations. The upper reference limit was estimated as the 0.95 fractile of the control values using a rank-based method (IFCC, 1987).
RESULTS
Tau and PHFtau levels were not only determined in CSF samples, but also in a series of serum samples, but both tau and PHF-tau were below the detection limit in all serum samples. Due to technical difficulties, PHF- tau could not be run in four CSF samples, all belonging to the AD group.
The CSF/S albumin ratio was significantly higher in the AD group (7.3 + 3.5; p < 0.01), in the VAD group (8.3 + 4.0; p < 0.001), and in the FLD group (6.8 + 1.8; p < 0.05), than in the control group (5.3 + 1.7), al though it did not significantly differ between the different patient groups. Within the group of healthy controls, there were no significant correlations between the CSF/S albumin ratio and CSF-tau (r = 0.19), or CSF-PHFtau (r = 0.25). Within the group of healthy controls, no signifi- cant correlations emerged between age and either CSF-tau (r = 0.11), or CSF-PHFtau (r = 0.16).
CSF-tau was significantly higher in the AD (524 + 280 pg/mL; p < 0.0001), VAD (445 + 195 pg/mL; p < 0.0001), and FLD (275 + 131 pg/mL; p < 0.05) groups as compared with controls (185 + 50 pg/mL). CSF-tau was also significantly higher in the AD group as compared with the FLD (p < 0.001), PD (p < 0.0001), and depression (p < 0.0001) groups, al though it did not significantly differ between the AD and the VAD groups. By contrast, CSF-tau did not significantly differ between the PD (216 + 105 pg/mL) or the depression (108 + 13 pg/mL) groups and controls.
The individual values are given in Fig. 1. A total of 37/44 (84%) of AD patients had CSF-tau values higher than the cutoff level of 258 pg/mL in
Molecular and Chemical Neuropathology Vol. 26, 1995

Tau Protein in CSF in A D 237
1600
1400-
t200-
1000-
800- pg/mL
600.
400 -
200 -
0
o �9 0
~ o 0 0 0 0
0 0 o
0 0 0 �9 e O e o
0 e �9 �9
eee �9 o o
o o e ~ �9 �9 �9 0 �9 o00o 00~
o.o~ e " o " ~ o ~176
0 0 0 0 0
0
0 0 0
00 u~ r~ o o~ o
~OoO o~%oo% oow167176176 o
AD FLD VAD PD Depr Controls
Fig. 1. Individual cerebrospinal fluid (CSF) tau protein values in different brain disorders. AD = Alzheimer disease; FLD = frontal lobe dementia; VAD = vascular dementia; PD = Parkinson disease; Depr = major depression without dementia. Filled circles = mildly demented patients. Line represents the upper reference limit in controls, estimated as the 0.95 fractile of the control values using a rank-based method (258 pg/mL).
controls, as compared with 13/17 (76%) of VAD patients, 4/11 (36%) FLD patients, 4/15 (27%) PD patients, and none of the depressed patients (Fig. 1).
CSF-PHFtau concentrations were significantly higher in the AD group (2230 + 930 pg/mL; p < 0.0001), in the VAD group (1610 + 840 pg/mL; p < 0.01), and in the FLD group (1530 + 1000 pg/mL; p < 0.01), than in the control group (640 + 320 pg/mL), whereas it did not significantly dif- fer be tween the PD group (720 + 590 pg/mL) or the depression group (230 + 130 pg/mL) and the control group. CSF-PHFtau was also signifi- cantly higher in the AD group as compared with all off the VAD (p < 0.005), FLD (p < 0.05), PD (p < 0.0001), and the depression (p < 0.0001) groups.
Individual values are given in Fig. 2. No less than 35/40 (88%) of AD patients had a CSF-PHFtau protein value higher than the cutoff level of 1140 pg/mL in controls as compared with 11/17 (65%) of VAD patients, 6/11 (55%) FLD patients, 4/15 (27%) PD patients, and none of the depressed patients (Fig. 2).
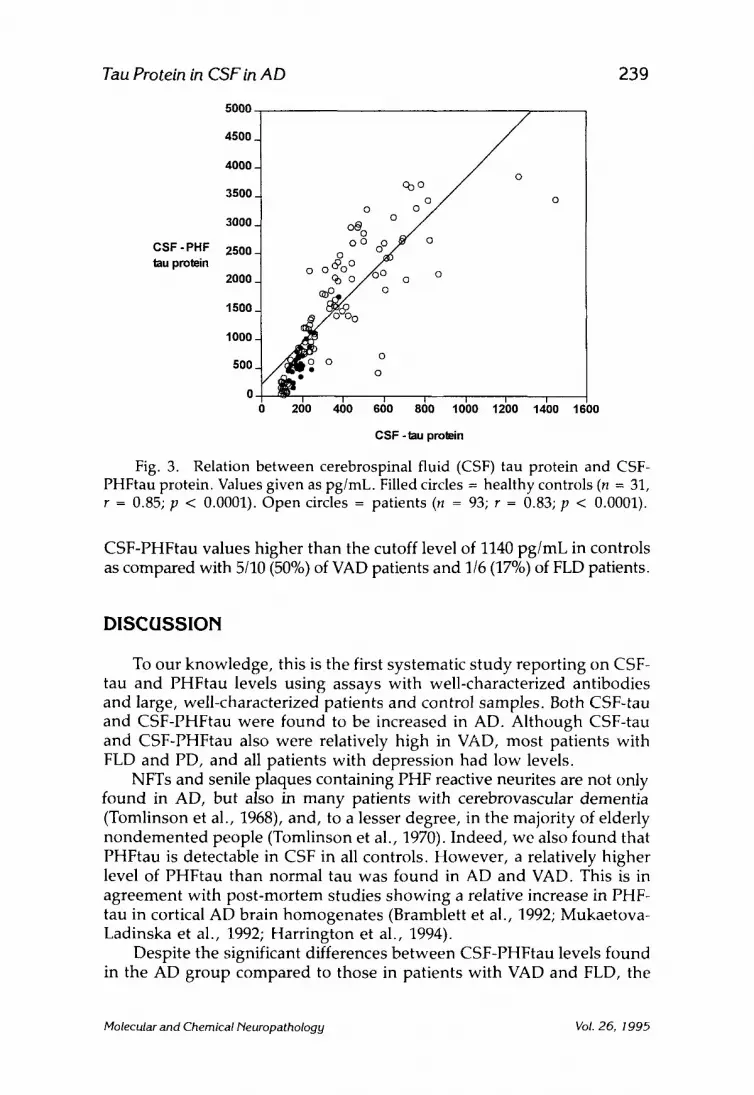
Thus, CSF-PHFtau levels generally paralleled those of CSF-tau. There were also significant correlations between CSF-tau and CSF-PHFtau levels, both in healthy controls (r = 0.83; p < 0.0001), and in patients (r = 0.83;
Molecular and Chemical Neuropathology Vol. 26, 1995

238 Blennow et al.
pg/mL
4000-
3500.
3000-
2500-
2000-
1500-
1000-
500
0
0 O0
�9 0 �9 0
0
moO00 �9
O 0 o
0~0 0
0 �9 �9 ~
0~ �9
0 ~176 �9 0 0
eeeo o o
0 o o o
." o �9 O 0
0 0 o 0 0 o
o 0 0 0 0
0
U 0
0 0 O 0 0 0
0
o o
00OO0o 0 0o0O0
0 0 0 0 o ~ ~ 0 o O0 O0
0000o O0 o
AD FLD VAD PD Depr Controls
Fig. 2. Individual cerebrospinal fluid (CSF) PHFtau protein values in dif- ferent brain disorders. AD = Alzheimer disease; FLD = frontal lobe dementia; VAD = vascular dementia; PD = Parkinson disease; Depr = major depression without dementia. Filled circles = mildly demented patients. Line represents the upper reference limit in controls, estimated as the 0.95 fractile of the control values using a rank-based method (1140 pg/mL).
p < 0.0001) (Fig. 3). The main difference when comparing results between CSF-tau and CSF-PHFtau was that CSF-PHFtau was significantly higher in AD than in VAD, although this difference was not found for CSF-tau.
A fully factorial multiple ANOVA showed that neither of age, dura- tion, or severity of dementia covaried with CSF-tau or CSF-PHFtau. How- ever, within the VAD and FLD groups, there was a tendency for higher CSF-tau and CSF-PHFtau values to be found in mildly demented patients, whereas within the AD group, there was a tendency for higher values to emerge in moderately and severely demented patients. Since clinical dif- ferentiation between AD, VAD, and FLD is difficult to make, we also analyzed the results excluding mildly demented patients in the AD, VAD, and FLD groups. After such exclusion, CSF-tau was significantly higher in the AD group (593 + 313 pg/mL), than in the VAD group (382 + 176 pg/mL; p < 0.05), and the FLD group (200 + 86 pg/mL; p < 0.001). Regard- ing individual values, 24/28 (86%) of AD patients had a CSF-tau protein value higher than the cutoff level of 258 pg/mL in controls, as compared with 6/10 (60%) of VAD patients and 1/6 (17%) of FLD patients. CSF- PHFtau was also significantly higher in the AD group (2390 + 970 pg/mL), than in the VAD group (1400 + 860 pg/mL; p < 0.01), and the FLD group (860 + 620 pg/mL; p < 0.005). We found 22/24 (92%) of AD patients with
Molecular and Chemical Neuropatho!ogy Vol. 26, 1995
Tau Protein in CSF in AD 239
C S F - P H F ~upmtein
5O0O
4500_
4000-
3500
3000
2500-
2000_
1500
1000
500
0 0 1600
~ o ~
oo~o ~ / Z ~ , o / O O o o
/ # - ; - o
- 4 ' 0 ' ' ' ' 2 0 400 6 0 800 1000 1200 1400
CSF - tau protein
Fig. 3. Relation between cerebrospinal fluid (CSF) tau protein and CSF- PHFtau protein. Values given as pg/mL. Filled circles = healthy controls (n -- 31, r = 0.85; p < 0.0001). Open circles = patients (n = 93; r = 0.83; p < 0.0001).
CSF-PHFtau values higher than the cutoff level of 1140 pg/mL in controls as compared with 5/10 (50%) of VAD patients and 1/6 (17%) of FLD patients.
DISCUSSION
To our knowledge, this is the first systematic study reporting on CSF- tau and PHFtau levels using assays with well-characterized antibodies and large, well-characterized patients and control samples. Both CSF-tau and CSF-PHFtau were found to be increased in AD. Although CSF-tau and CSF-PHFtau also were relatively high in VAD, most patients with FLD and PD, and all patients with depression had low levels.
NFTs and senile plaques containing PHF reactive neurites are not only found in AD, but also in many patients with cerebrovascular dementia (Tomlinson et al., 1968), and, to a lesser degree, in the majority of elderly nondemented people (Tomlinson et al., 1970). Indeed, we also found that PHFtau is detectable in CSF in all controls. However , a relatively higher level of PHFtau than normal tau was found in AD and VAD. This is in agreement with post-mortem studies showing a relative increase in PHF- tau in cortical AD brain homogenates (Bramblett et al., 1992; Mukaetova- Ladinska et al., 1992; Harrington et al., 1994).
Despite the significant differences between CSF-PHFtau levels found in the AD group compared to those in patients with VAD and FLD, the
Molecular and Chemical Neuropathology Vol. 26, 1995

240 Blennow et al.
overlap between the groups are considerable. This overlap may be caused by several factors.
First, the typical AD (Blennow et al., 1991) and FLD (Gustafson, 1987) symptomatology is not fully developed early in the course of the disorders. Thus, based on clinical criteria, it is difficult to discriminate Alzheimer from VAD and FLD patients. In addition, it is well-known that clinically diagnosed VAD patients may have concomitant Alzheimer-type pathol- ogy, i.e., have "mixed" AD/VAD. It is known that clinical differentiation between AD and other dementias is more difficult early in the course of the disease (Blennow and Wallin, 1992). Indeed, upon reanalysis of the results after excluding the mildly demented patients, differences between groups were more pronounced.
Second, although MAbs AT180 and AT270 are highly dependent on phosphorylated residues (Goedert et al., 1994) they also recognize normal human tau to some extent. The finding that PHFtau is present in all CSF samples from healthy individuals indicates that these sites are at least partially phosphorylated under normal conditions. The difference between the degree of phosphorylation in AD as compared with that in control brains has not yet been quantified. These CSF results, if truly reflecting an ongoing neurodegenerative process, would thereby indicate that these hypothetical differences in phosphorylation might not be so great as orig- inally assumed. Tau protein isolated rapidly from normal human brain (Garver et al., 1994), as well as tau isolated from biopsy brain tissue (Matsuo et al., 1994), has a high degree of phosphorylation, findings that seem to confirm this observation. Quantification of the degree of phosphorylation of tau isolated from normal brains and a comparison with Alzheimer brains, preferentially from biopsy tissue, may help resolve this issue.
Third, both assays may reflect similar processes in the brain. Normal tau is an intraneuronal protein, preferentially located in the axons, and also PHFtau is intraneuronal. Thus, both CSF-tau and CSF-PHFtau may both identify a pathological biochemical process that is common to both VAD and AD, such as the axonal degeneration (Wallin et al., 1989). NFTs are found in a variety of disorders (Wisniewski et al., 1979). PHFtau (Alz- 50) immunoreactivity has been found to be induced after experimental focal cerebral ischemia in cats (Dewar et al., 1994), which may explain the increase in CSF-PHFtau in VAD.
We unexpectedly found large differences in the amount of CSF-tau compared to CSF-PHFtau. This is most likely owing to the fact that differ- ent antibodies were used to recognize their respective epitopes on the tau molecule. The antigen-antibody reaction, especially for the tau molecule, is to some extent dependent on the conformation of the epitope, as has been shown for Alz50 and tau-1 (Goedert et al., 1991; Szendrei et al., 1993). The epitopes of the antibodies used in this study map in the proline- rich region of tau, which is heavily phosphorylated in AD (Morishima- Kawashima et al., 1995) and therefore may also be dependent on the con- firmation of the epitope.
Molecular and Chemical Neuropathology Vol. 26, 1995

Tau Protein in CSF in A D 241
In addition there is a large difference between tau levels reported in Vandermeeren et al. (1993) and this work. This is probably related to the sole used of MAbs for tau detection in the present investigation as com- pared to the use of a polyclonal antibody in the previous study. Second, the limited amount of highly purified tau used in the earlier study to deter- mine tau concentrations via amino acid analysis caused an extensive loss of material during one of the dialysis steps prior to analysis. Thereafter, tau was isolated from several different sources (Baculovirus expression, E. coli expression, and normal human brain), and tau isolated from normal human brain consistently gave the best results in several types of ELISAs (unpublished results).
In conclusion elevated tau/PHFtau levels are consistently found in CSF of AD patients. However, a considerable overlap is still present with other forms of dementia, both VAD and FLD. CSF-tau and CSF-PHFtau there- fore may be useful as a positive biochemical marker, to discriminate AD from normal aging, PD, and depressive pseudodementia. Further studies are needed to clarify the sensitivity and specificity of these assays, includ- ing follow-up studies with neuropathological examinations. We are pres- ently attempting to gain a clear understanding of the difference between "normal tau" and "Alzhe imer" tau in brains and CSF.
ACKNOWLEDGMENTS
This work was supported by grants from The Swedish Medical Research Council (Grant #B96-12X), AlzheimerfOreningen, Lund, Sweden; Stiftel- telsen for Gamla Tj/inarinnor, Stockholm, Sweden; Tore Nilssons Fond for Medicinsk Forskning, Stockholm, Sweden; Svenska L~kares~illskapet, Stockholm, Sweden; and Ake Wibergs Stiftelse, Stockholm, Sweden.
REFERENCES
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd ed., American Psychiatric Association, Washington, DC.
Bancher C., Brunner C., Lassman H., Budka H., Jellinger K., Wiche G., Seitel- berger F., Grundke-Iqbal I., iqbal K., and Wisniewski H. M. (1989) Accumu- lation of abornmally phosphorylated T precedes the formation of neurofibril- lary tangles in Alzheimer disease. Brain Res. 477, 90-99.
Bissette G., Smith W. H., Dole K. C., Crain B., Ghanbari H., Miller B., and Nemeroff C. B. (1991) Alterations in Alzheimer's disease-associated protein in Alzheimer's disease frontal and temporal cortex. Arch. Gen. Psychiat. 48, 1009-1012.
Blennow K., WaUin A., and Gottfries C. G. (1991) Presence of parietal lobe symptomatology distinguishes early and late onset Alzheimer's disease. Int. J. Geriatr. Psychiat. 6, 147-154.
Molecular and Chemical Neuropathology Vol. 26, 1995

242 B l e n n o w et al.
Blennow K. and Wallin A. (1992) Clinical heterogeneity of probable Alzheimer's disease. J. Geriatr. Psychiatry Neurol. 5, 106-113.
Blennow K., Fredman P., Wallin A., Gottfries C. G., Langstrom L., and Svenner- holm L. (1993) Protein analyses in cerebrospinal fluid: I. Influence of con- centration gradients for proteins on cerebrospinal fluid/serum albumin ratio. Eur. Neurol. 33, 126-128.
Bramblett G. T., Trojanowski J. Q., and Lee V. M. Y. (1992) Regions with abun- dant neurofibrillary pathology in human brain exhibit a selective reduction in levels of binding-competent r and accumulation of abnormal T-isoforms (A68 proteins). Lab Invest. 66, 212-222.
Coleman P. D. and Flood D. G. (1987) Neuron numbers and dendrite extent in normal aging and Alzheimer's disease. Neurobiol. Aging 8, 521-545.
Davies C. A., Mann D. M. A., Sumpter P. Q., and Yates P. O. (1987) A quantita- tive morphometric analysis of the neuronal and synaptic content of the fron- tal and temporal cortex in patients with Alzheimer's disease. J. Neurol. Sci. 78, 151-164.
Delacourte A., Flament S., Dibe E. M., Hublau P., Sablonniere B., Hemon B., Sherrer V., and D6fossez A. (1990) Pathological proteins tau 64 and 69 are specifically expressed in the somatodendritic domain of the degenerating cortical neurons during Alzheimer's disease. Acta Neuropathol. 80, 111-117.
Dewar D., Graham D. I., Teasdale G. M., and McCulloch J. (1994) Cerebral ischemia induces alterations in tau and ubiquitin proteins. Dementia 5, 168-173.
Folstein M., Folstein S., and McHugh P. (1975) "Mini-Mental State" A practical method for grading the cognitive state of patients for the clinician. ]. Psychiatr. Res. 12, 189-198.
Garver T. D., Harris K. A., Lehman R. A. W., Lee V. M. Y., Trojanowski J. Q., and Billingsley M. L. (1994) ~ phosphorylation in human, primate, and rat brain: evidence that a pool of ~ is highly phosphorylated in vivo and is rapidly dephosphorylated in vitro. J. Neurochem. 63, 2279-2287.
Ghanbari H. A., Kozuk T., Miller B. E., and Riesing S. (1990) A sandwich enzyme immunoassay for detecting and measuring Alzheimer's disease- associated proteins in human brain tissue. ]. Clin. Lab. Anal. 4, 189-192.
Goedert M., Wischik C. M., Crowther R. A., Walker J. E., and Klug A. (1988) Cloning and sequencing of the cDNA encoding a core protein of the paired helical filament of Alzheimer disease: identification as the microtubule- associated protein tau. Proc. Natl. Acad. Sci. USA 85, 4051-4055.
Goedert M., Spillantini M., and Jakes R. (1991) Localization of the Alz-50 epi- tope in recombinant human microtubule-associated protein tau. Neurosci. Lett. 126, 149-154.
Goedert M. (1993) Tau protein and the neurofibrillary pathology of Alzheimer's disease. Trends Neurosci. 16, 460-465.
Goedert M., Jakes R., Crowther A., Cohen P., Vanmechelen E., Vandermeeren M., and Cras P. (1994) Epitope mapping of monoclonal antibodies to the paired helical filaments of Alzheimer's disease: identification of phosphory- lation sites in tau protein. Biochem. J. 301, 871-877.
Molecular and Chemical Neuropathology Vol. 26, 1995

Tau Protein in CSF in A D 243
Greenberg S. G. and Davies P. (1990) A preparation of Alzheimer paired helical filaments that displays distinct T proteins by polyacrylamide gel electro- phoresis. Proc. Natl. Acad. Sci. USA 87, 5827-5831.
Grundke-lqbal I., Iqbal K., Tung Y. C., Quinlan M., Wisniewski H. M., and Binder L. I. (1986) Abnormal phosphorylation of the microtubule-associated protein T (tau) in Alzheimer cytoskeletal pathology. Proc. Natl. Acad. Sci. USA 83, 4913-4917.
Gustafson L. (1987) Frontal lobe degeneration of non-Alzheimer type. 2. Clinical picture and differential diagnosis. Arch. Gerontol. Geriatr. 6, 209-223.
Hamos J. E., DeGennaro L. J., and Drachman D. A. (1989) Synaptic loss in Alz- heimer's disease and other dementias. Neurology 39, 355-361.
Harrington C. R., Mukeatova-Ladinska E. B., Hills R., Edwards P. C., de Garcini E. M., Novak M., and Wischik C. M. (1991) Measurement of distinct immu- nochemical presentations of tau protein in Alzheimer disease. Proc. Natl. Acad. Sci. USA 88, 5842-5846.
Harrington C. R., Perry R. H., Per D, E. K., Hurt J., McKeith I. G., Roth M., and Wischik C. M. (1994) Senile dementia of Lewy Body-type and Alzheimer type are biochemically distinct in terms of paired helical filaments and hyperphosphorylated tau protein. Dementia 5, 215-218.
Hyman B. T., van Hoesen G. W., Wolozin B. L., Davies P., Kromer L. J., and Damasio A. R., (1988) Alz-50 antibody recognizes Alzheimer-related neu- ronal changes. Ann. Neurol. 23, 371-379.
lhara Y., Nukina N., Miura R., and Ogawara M. (1986) Phosphorylated tau pro- tein is integrated into paired helical filaments in Alzheimer's disease. ]. Bio- chem. 99, 1807-1810.
International Federation of Clinical Chemistry (IFCC) (1987) Approved recom- mendation on the theory of reference values. Part 5. Statistical treatment of collected reference values. Determination of reference limits. Clin. Chim. Acta 170, 13-32.
Katzman R. (1986) Alzheimer's disease. N. Engl. J. Med. 314, 964-973. Khatoon S., Grundkeqqbal I., and Iqbal K. (1992) Brain levels of microtubule-
associated protein r are elevated in Alzheimer's disease: a radioimmuno- slot-blot assay for nanograms of the protein. J. Neurochem. 59, 750-753.
Langston J. W., Widner H., Goetz C. G., Brooks D., Fahn S., Freeman T., and Watts R. (1992) Core assessment program for intracerebral transplantations (CAPIT). Mov. Disord. 7, 2-13.
Lishman W. A. (1987) Organic Psychiatry: the Psychological Consequences of Cerebral Disorder. 2nd ed. Chicago, Year Book Medical Publishers.
Matsuo E., Shin R.-W., Billingsley M. L., Van de Voorde A., O'Connor M., Trojanowski J., and Lee V.-M. (1994) Biopsy~derived adult human brain tau is phosphorylated at many of the same sites as Alzheimer's disease paired helical filament tau. Neuron 13, 989-1002.
McKhann G., Drachman D., Folstein M., Katzman R., Price D., and Stadlan E. M. (1984) Clinical diagnosis of Alzheimer's disease: report of the NINCDS- ADRDA Work Group under the auspices of department of health and human services task force on Alzheimer's disease. Neurology 34, 939-944.
Molecular and Chemical Neuropathology Vol. 26, 1995

244 B l e n n o w et al.
Mehta P. H., Thal L., and Wisniewski H. M., et al. (1985) Paired helical filaments antigen in CSF. (letter) Lancet II 35.
Mercken M., Vandermeeren M., Ltibke U., Six J., Boons J., van der Voorde A., Martin J. J., and Gheuens J. (1992) Monoclonal antibodies with selective spe- cificity for Alzheimer tau are directed against phosphatase-sensitive epitopes. Acta Neuropathol. 84, 265-272.
Mori H., Kondo J., and Ihara Y. (1987) Ubiquitin is a component of paired helical filaments in Alzheimer's disease. Science 235, 1641-1644.
Morishima-Kawashima M., Hasegawa M., Takio K., Suzuki M., Yoshida H., Titani K., and Ihara Y. (1995) Proline-directed and non-proline-directed phos- phorylation of PHF-tau. J. Biol. Chem. 270, 823-829.
Mukaetova-Ladinska E. B., Harrington C. R., Hills R., O'Sullivan A., Roth M., and Wischik C. M. (1992) Regional distribution of paired helical filaments and normal tau proteins in aging and in Alzheimer's disease with and without temporal lobe involvement. Dementia 3, 61-69.
Oyama F., Shimada H., Oyama R., Titani K., and Ihara Y. (1991) Differential ex- pression of B amyloid protein precursor (APP) and tau mRNA in the aged human brain: individual variability and correlation between APP-751 and four-repeat tau. J. Neuropathol. Exp. Neurol. 50, 560-578.
Perry G., Friedman R., Shaw G., and Chau V. (1987) Ubiquitin is detected in neurofibrillary tangles and senile plaque neurites of Alzheimer disease brains. Proc. Natl. Acad. Sci. USA 84, 3033-3036.
Scheltens P., Vermersch P., and Leys D. (1993) Het6rog6n6it6 de la maladie d'Alzheimer. Rev. Neurol. (Paris) 149, 14-25.
SjOgren T., Sjt~gren H., and Lindgren ,i.. (1952) Morbus Alzheimer and morbus Pick: A genetic, clinical and patho-anatomical study. Acta Psych. Neurol. Scand. (Suppl 82) 66-115.
Szendrei G., Lee V.-M., and Otvos L. (1993) Recognition of the minimal epitope of monoclonol antibody Tau-1 depends upon the presence of a phosphate group but not its localization. J. Neurosci. Res. 34, 243-249.
Thompson E. J. (1988) The CSF Proteins: A Biomedical Approach. Elsevier, Amster- dam; pp. 9-26.
Tibbling G., Link H., and Ohman S. (1977) Principles of albumin and IgG analysis in neurological disorders. I. Establishment of reference values. Scand. ]. Clin. Lab. Invest. 37, 385-390.
Tomlinson B. E., Blessed G., and Roth M. (1968) Observations of the brains of non-demented old people. J. Neurol. Sci. 7, 331-356.
Tomlinson B. E., Blessed G., and Roth M. (1968) Observations of the brains of demented old people. J. Neurol. Sci. 11, 205-242.
Tomlinson B. E. and Corsellis J. A. N. (1984) Ageing and the dementias, in Green- field's Neuropathology (Hume Adams J., Corsellis J. A. N., and Duchen L. W., eds., Edward Arnold, London, pp. 951-1025.
Vandermeeren M., Mercken M., Vanmechelen E., Six J., Van de Voorde A., Martin J. J., and Cras P. (1993) Detection of T proteins in normal and Alz- heimer's disease cerebrospinal fluid with a sensitive sandwich enzyme- linked immunosorbent assay. J. Neurochem. 61, 1828-1834.
Molecular and Chemical Neuropathology Vol. 26, 1995

Tau Protein in CSF in A D 245
Wallin A., Gottfries C. G., Karlsson I., and Svennerholm L. (1989) Decreased myelin lipids in Alzheimer's disease and vascular dementia. Acta Neurol. Scand. 80, 319-323.
Wallin A. and Blennow K. (1991) The pathogenetic basis of vascular dementia. Alzheimer Dis. Assoc. Disord. 5, 91-102.
Wallin A., Blennow K., and Scheltens P. (1994) Research criteria for clinical diag- nosis of "pure" Alzheimer's disease. Drugs Today 30, 265-273.
Wang G. P., Iqbal K., Bucht G., Winblad B., Wisniewski H. M., and Grundke- Iqbal I. (1991) Alzheimer's disease: paired helical filament immunoreactivity in cerebrospinal fluid. Acta Neuropathol. (Bed.) 82, 6-12.
Wisniewski K., George A. J., Moretz R. C., and Wisniewski H. M. (1979) Alz- heimer neurofibrillary tangles in diseases other than senile and presenile dementia. Ann. Neurol. 5, 288-294.
Wolozin B. and Davies P. (1987) Alzheimer-related neuronal protein A68: specif- icity and distribution. Ann. Neurol. 22, 521-526.
Molecular and Chemical Neuropathology Vol. 26, 1995





























