Embed Size (px)
Citation preview

Hernia (2008) 12:395–400
DOI 10.1007/s10029-008-0352-6ORIGINAL ARTICLE
The accuracy of ultrasonography in classiWcation of groin hernias according to the criteria of the uniWed classiWcation system
A. Djuric-Stefanovic · D. Saranovic · A. Ivanovic · D. Masulovic · M. Zuvela · M. Bjelovic · P. Pesko
Received: 16 October 2007 / Accepted: 25 January 2008 / Published online: 22 February 2008© Springer-Verlag 2008
AbstractBackground The modern concept of type-related indi-vidualized groin hernia surgery imposes a demand for preciseand accurate preoperative determination of the type ofgroin hernia. The aim of this prospective study was to eval-uate the accuracy of ultrasonography in classiWcation ofgroin hernias, according to the criteria of the uniWed classi-Wcation system. UniWed classiWcation divides groin hernias
into nine types (grades): type I (indirect, small), II (indirect,medium), III (indirect, large), IV (direct, small), V (direct,medium), VI (direct, large), VII (combined-pantaloon),VIII (femoral), and O (other).Patients and methods One hundred and twenty-Wve adultpatients with clinically diagnosed or suspected groin her-nias were examined. Ultrasonography of both groins wasperformed with a 5 to 10-MHz linear-array transducer. Pre-operative ultrasonographic Wndings of type of groin herniawere compared with the intraoperative Wndings, whichwere considered the gold standard.Results Total accuracy of ultrasonography in determina-tion of type of groin hernia was 96% (119 of 124 correctpredictions of type of groin hernia compared with surgicalexplorations). All hernias of types I, IV, V, VII, and VIIIwere correctly identiWed with ultrasonography (sensitivityand speciWcity 100%). In the remaining Wve cases ofthe 124 (4%), hernia was incorrectly classiWed with ultra-sonography: type VI (direct, large) was misdiagnosed astype III (indirect, large) in three cases, type III as type VIin one case, and type III as type II (indirect, medium) inone case. The sensitivity and the speciWcity of ultraso-nography in classifying type II were 100 and 99%, respec-tively, for type III, 85 and 97%, and for type VI, 90 and99%.Conclusion Ultrasonography of the groin regions couldbe used with great accuracy for precise classiWcation ofgroin hernias in adults. Each type of groin hernia, accordingto the uniWed classiWcation system that we used for classiW-cation, has a characteristic ultrasonographic presentation,which is demonstrated in this study.
Keywords Ultrasound · Hernia · Groin · ClassiWcation
A. Djuric-Stefanovic (&) · D. Saranovic · A. Ivanovic · D. MasulovicDepartment of Digestive Radiology (First Surgical Clinic), Institute of Radiology, Clinical Center of Serbia, Koste Todorovica 6, 11000 Belgrade, Serbiae-mail: [email protected]
D. Saranovice-mail: [email protected]
A. Ivanovice-mail: [email protected]
D. Masulovice-mail: [email protected]
M. Zuvela · M. Bjelovic · P. PeskoFirst Surgical Clinic, Institute for Diseases of Digestive System, Clinical Center of Serbia, Koste Todorovica 6, 11000 Belgrade, Serbiae-mail: [email protected]
M. Bjelovice-mail: [email protected]
P. Peskoe-mail: [email protected]
A. Djuric-Stefanovic · D. Saranovic · D. Masulovic · M. Zuvela · M. Bjelovic · P. PeskoSchool of Medicine, University of Belgrade, Belgrade, Serbia
123

396 Hernia (2008) 12:395–400
Introduction
The surgical concept of individualized groin hernia repairimposes a demand for more precise and detailed preopera-tive evaluation of the type of groin hernia [1–4]. Thisassessment should enable the surgeon to choose the mostappropriate therapeutic approach for each type of groin her-nia, for every individual patient [1–4]. According to theoldest traditional classiWcation system, which is still widelyused, groin hernias are divided into three types: direct(medial) and indirect (lateral) inguinal, and femoral hernias[3–5]. As diVerent operative techniques for open or laparo-scopic repair of groin hernias were introduced and developed,more complex and precise systems of classiWcations werecreated [3–5]. Recently, the uniWed classiWcation systemwas proposed [3, 4] and modiWed by Zollinger [5]. Accord-ing to the uniWed classiWcation system groin hernias aredivided into nine types (grades), considering the anatomicalsite of the hernia, the approximate size of the hernia, andthe presence or loss of functional integrity—the compe-tence of the internal inguinal ring and the integrity of thedirect Xoor (see “Patients and methods” section) [3–5].
Surgeons still usually diagnose and classify the groinhernias by clinical examination, although imaging tech-niques such as herniography, ultrasonography, CT, andMRI, enable visualization and certain diagnosis [6–21].Ultrasonography, a non-invasive method and the mostavailable imaging method in all radiology departments, hasbeen used for detection and classiWcation of groin herniasin adults [9–21]. However, in all studies that are availablein literature, groin hernias were classiWed according to thetraditional classiWcation system [13–15, 17–21]. The objec-tive of this prospective study was to evaluate the accuracyof ultrasonography in typing the groin hernias in adults ifthe criteria of the uniWed classiWcation system were applied.
Patients and methods
A consecutive series of 125 adult patients with clinicallydiagnosed (116 patients) or suspected (groin pain, but nopalpable hernia; nine patients) groin hernias were enrolledin this prospective study (111 male and 14 female, meanage of 48 years, range 19–82 years). After clinical exami-nation, patients were referred to the radiology departmentfor ultrasonography. The radiologist was blind to clinicaldiagnosis and both groins were examined. The presence/absence of hernia for each groin and the type of detectedgroin hernia were recorded. In addition, ultrasonographicvisualization of the spermatic cord (or the round ligament)and the inferior epigastric artery, as two anatomical land-marks for diVerentiation between indirect and direct ingui-nal hernias, was recorded for both groins of every patient
examined. Patients in whom hernia was diagnosed withclinical examination, or detected with ultrasound, or both,were operated on. Ultrasonographic Wndings of the type ofgroin hernia were compared with the surgical Wndings,which were considered the gold standard. Ethical approvalfor the study was obtained, and informed oral consent forthe preoperative ultrasound examination was obtained fromeach patient.
Ultrasonography was performed with a 5 to 10-MHz lin-ear-array transducer (Diagnostic Ultrasound System SDU-2200; Shimadzu, Japan). After a learning period while weexamined 20 patients and compared ultrasonographic appear-ances of hernias with anatomical description and surgicalWndings, we created the following scanning technique andultrasonographic criteria for classiWcation of groin hernias.
Scanning technique
All the patients were initially scanned in a lying supineposition with relaxed and then contracted abdominal mus-cles (at rest and during straining). In equivocal cases,patients were also examined in the standing position.
We examined the inguinal regions with transversalscans. The scanning area included the region from thelower segments of the rectus muscle and the lateralabdominal muscles cranially to the level of the pubic bonecaudally, and from the middle line medially to the iliaccrest laterally.
Hernia was diagnosed when bowel loops or fat, whichsigniWcantly protrude during straining, were seen withultrasound in the inguinal region.
Ultrasonographic diVerentiation between indirect inguinal, direct inguinal, and femoral hernia
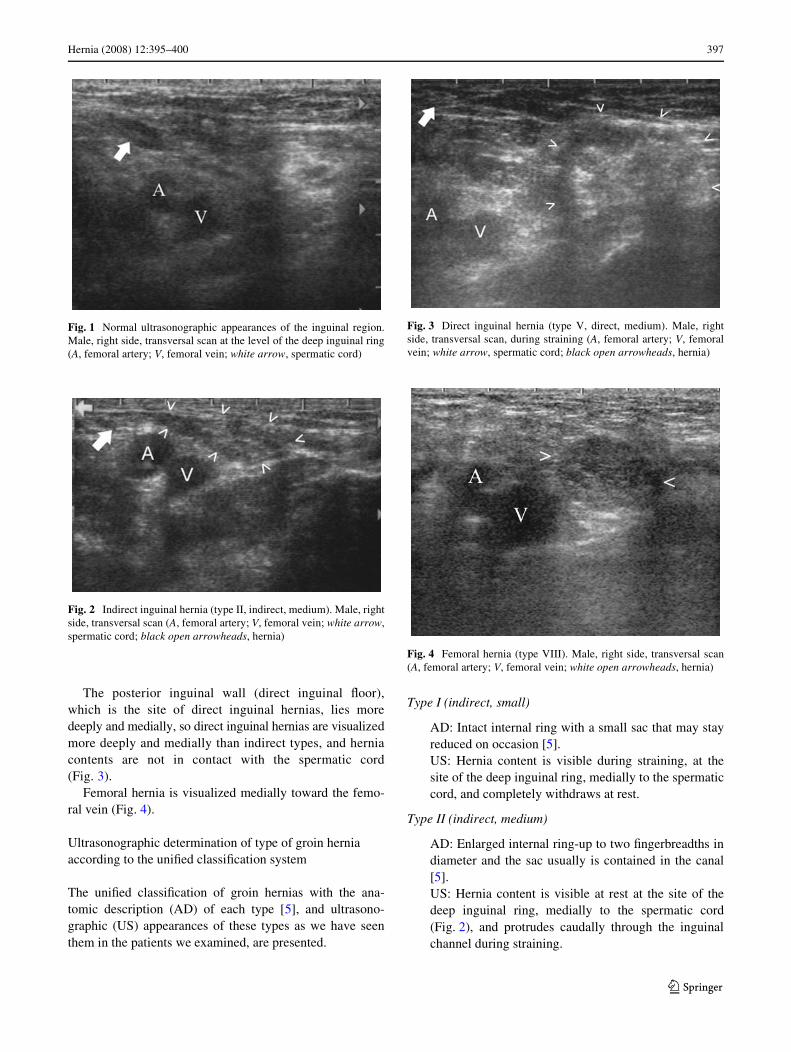
According to our experience during the learning period, theessential fact that we used for sonographic diVerentiationbetween indirect and direct inguinal hernia was the rela-tionship of the hernia contents to the spermatic cord (or theround ligament). The spermatic cord is clearly visible withshort-axis scans as a hypoechoic ovoid structure with ahyperechoic center, which lies in the subcutaneous adiposetissue superWcially to the femoral vessels (Fig. 1). Trans-versal section of the round ligament is visualized at thesame position in the subcutaneous fatty tissue, as a homo-geneously hypoechoic round structure. When the trans-ducer is moved in cranial–caudal direction, the point wherethe spermatic cord (or the round ligament) appears in thesubcutaneous fatty tissue of the inguinal region is the site ofthe deep inguinal ring.
Indirect inguinal hernias are visualized medially towardthe spermatic cord and always are in contact with it(Fig. 2).
123
Hernia (2008) 12:395–400 397
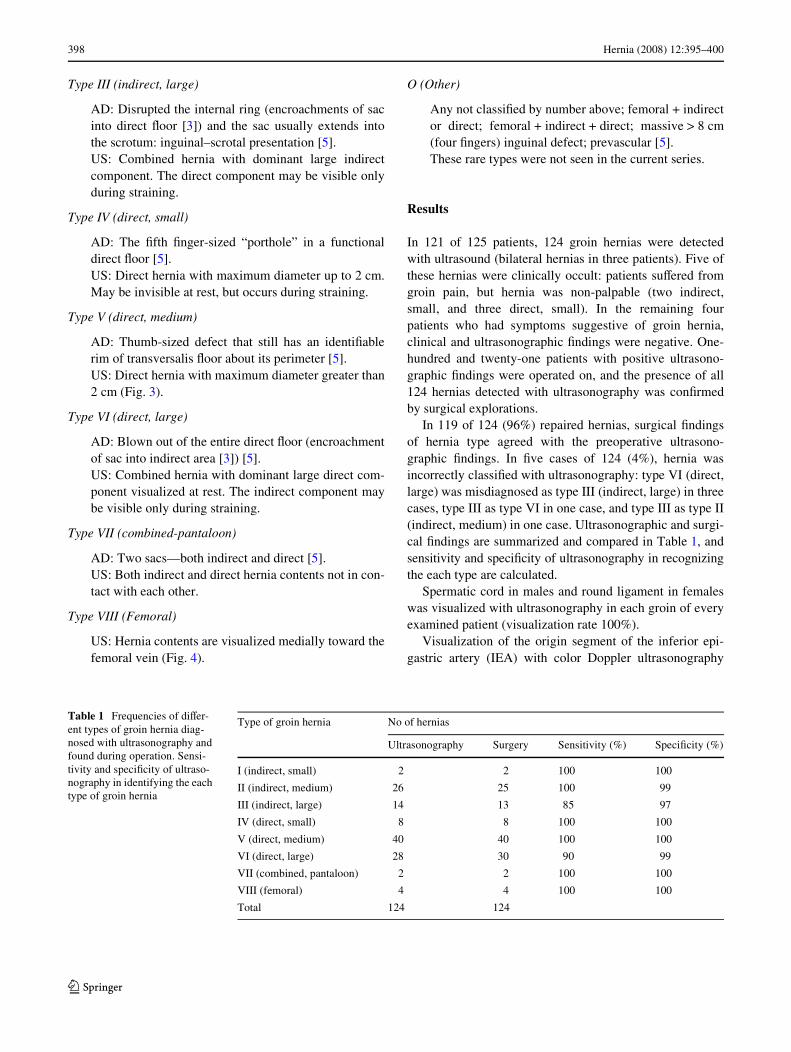
The posterior inguinal wall (direct inguinal Xoor),which is the site of direct inguinal hernias, lies moredeeply and medially, so direct inguinal hernias are visualizedmore deeply and medially than indirect types, and herniacontents are not in contact with the spermatic cord(Fig. 3).
Femoral hernia is visualized medially toward the femo-ral vein (Fig. 4).
Ultrasonographic determination of type of groin hernia according to the uniWed classiWcation system
The uniWed classiWcation of groin hernias with the ana-tomic description (AD) of each type [5], and ultrasono-graphic (US) appearances of these types as we have seenthem in the patients we examined, are presented.
Type I (indirect, small)
AD: Intact internal ring with a small sac that may stayreduced on occasion [5].US: Hernia content is visible during straining, at thesite of the deep inguinal ring, medially to the spermaticcord, and completely withdraws at rest.
Type II (indirect, medium)
AD: Enlarged internal ring-up to two Wngerbreadths indiameter and the sac usually is contained in the canal[5].US: Hernia content is visible at rest at the site of thedeep inguinal ring, medially to the spermatic cord(Fig. 2), and protrudes caudally through the inguinalchannel during straining.
Fig. 1 Normal ultrasonographic appearances of the inguinal region.Male, right side, transversal scan at the level of the deep inguinal ring(A, femoral artery; V, femoral vein; white arrow, spermatic cord)
Fig. 2 Indirect inguinal hernia (type II, indirect, medium). Male, rightside, transversal scan (A, femoral artery; V, femoral vein; white arrow,spermatic cord; black open arrowheads, hernia)
Fig. 3 Direct inguinal hernia (type V, direct, medium). Male, rightside, transversal scan, during straining (A, femoral artery; V, femoralvein; white arrow, spermatic cord; black open arrowheads, hernia)
Fig. 4 Femoral hernia (type VIII). Male, right side, transversal scan(A, femoral artery; V, femoral vein; white open arrowheads, hernia)
123
398 Hernia (2008) 12:395–400
Type III (indirect, large)
AD: Disrupted the internal ring (encroachments of sacinto direct Xoor [3]) and the sac usually extends intothe scrotum: inguinal–scrotal presentation [5].US: Combined hernia with dominant large indirectcomponent. The direct component may be visible onlyduring straining.
Type IV (direct, small)
AD: The Wfth Wnger-sized “porthole” in a functionaldirect Xoor [5].US: Direct hernia with maximum diameter up to 2 cm.May be invisible at rest, but occurs during straining.
Type V (direct, medium)
AD: Thumb-sized defect that still has an identiWablerim of transversalis Xoor about its perimeter [5].US: Direct hernia with maximum diameter greater than2 cm (Fig. 3).
Type VI (direct, large)
AD: Blown out of the entire direct Xoor (encroachmentof sac into indirect area [3]) [5].US: Combined hernia with dominant large direct com-ponent visualized at rest. The indirect component maybe visible only during straining.
Type VII (combined-pantaloon)
AD: Two sacs––both indirect and direct [5].US: Both indirect and direct hernia contents not in con-tact with each other.
Type VIII (Femoral)
US: Hernia contents are visualized medially toward thefemoral vein (Fig. 4).
O (Other)
Any not classiWed by number above; femoral + indirector direct; femoral + indirect + direct; massive > 8 cm(four Wngers) inguinal defect; prevascular [5].These rare types were not seen in the current series.
Results
In 121 of 125 patients, 124 groin hernias were detectedwith ultrasound (bilateral hernias in three patients). Five ofthese hernias were clinically occult: patients suVered fromgroin pain, but hernia was non-palpable (two indirect,small, and three direct, small). In the remaining fourpatients who had symptoms suggestive of groin hernia,clinical and ultrasonographic Wndings were negative. One-hundred and twenty-one patients with positive ultrasono-graphic Wndings were operated on, and the presence of all124 hernias detected with ultrasonography was conWrmedby surgical explorations.
In 119 of 124 (96%) repaired hernias, surgical Wndingsof hernia type agreed with the preoperative ultrasono-graphic Wndings. In Wve cases of 124 (4%), hernia wasincorrectly classiWed with ultrasonography: type VI (direct,large) was misdiagnosed as type III (indirect, large) in threecases, type III as type VI in one case, and type III as type II(indirect, medium) in one case. Ultrasonographic and surgi-cal Wndings are summarized and compared in Table 1, andsensitivity and speciWcity of ultrasonography in recognizingthe each type are calculated.
Spermatic cord in males and round ligament in femaleswas visualized with ultrasonography in each groin of everyexamined patient (visualization rate 100%).
Visualization of the origin segment of the inferior epi-gastric artery (IEA) with color Doppler ultrasonography
Table 1 Frequencies of diVer-ent types of groin hernia diag-nosed with ultrasonography and found during operation. Sensi-tivity and speciWcity of ultraso-nography in identifying the each type of groin hernia
Type of groin hernia No of hernias
Ultrasonography Surgery Sensitivity (%) SpeciWcity (%)
I (indirect, small) 2 2 100 100
II (indirect, medium) 26 25 100 99
III (indirect, large) 14 13 85 97
IV (direct, small) 8 8 100 100
V (direct, medium) 40 40 100 100
VI (direct, large) 28 30 90 99
VII (combined, pantaloon) 2 2 100 100
VIII (femoral) 4 4 100 100
Total 124 124
123

Hernia (2008) 12:395–400 399
was achieved in 205 of 250 examined groins (total visuali-zation rate 82%). IEA was visible in 114 of 126 normalgroins (90%) and in 91 of 124 groins with hernia (73%)(X2 = 12.365, p < 0.01). In the remaining 45 groins (12normal and 33 with detected groin hernias) we could notidentify the origin segment of IEA with color Dopplerultrasonography.
Discussion
The high accuracy of ultrasonography in detecting groinhernias is reported in many studies [9, 11, 16–19]. CorrectclassiWcation of groin hernias with ultrasonography wasusually less successful than detection the presence of thehernia [3–15, 17–19]. Total accuracy (percentages of cor-rect ultrasonographic diagnoses of type of groin herniascompared with surgical Wndings) reported in literaturewere: 78% for direct and 89% for indirect type in study ofKorenkov et al. [13], 71.1% for direct and 84.3% for indi-rect type in study of Babkova and Bozhko [14], 86% fordirect and 97% for indirect type in study of Bradley et al.[17], 45% for all types in study of Zhang et al. [15], 85% instudy of Lilly and Arregui [18], 62% in study of Kraft et al.[19], and 100% in study of Robinson et al. [20]. In all thesestudies, the traditional classiWcation system was applied.Combined hernias were not correctly recognized with ultra-sonography in the majority of cases in the series reported[13, 19]. For clinical examination as a tool for typing thegroin hernias, lower accuracy rates compared with ultraso-nography were reported in studies available in the literature[9, 19, 22]. Direct inguinal and femoral hernias, especially,were reported as diYcult to diagnose by clinical exam [22].
The traditional anatomical concept of classiWcation ofinguinal hernias as medial (direct) and lateral (indirect) isbased at the relationship of the hernia sac toward the infe-rior epigastric artery (IEA) [10, 21, 23, 24]. Although manystudies have reported that the IEA had been used as alandmark for classiWcation of inguinal hernias with ultraso-nography, two studies were particularly focused on visuali-zation of the IEA and its relation to the hernia, andsubsequent determination of hernia type [13, 15]. Visuali-zation rate of the IEA with color Doppler ultrasonographyin the present study was 82%, for all 250 examined groins.Visualization rate was signiWcantly lower for groins withhernia compared with normal groins (73%: 90%). Koren-kov et al. reported in their study that visualization rate ofthe IEA was 100%, but accuracy in determination of thetype of inguinal hernia was lower—78% for direct and 89%for indirect—in a group of patients with small inguinal her-nias [13]. In the study of Zhang et al. visualization rate ofthe root segment of the IEA was 55% and the overall accu-racy in classiWcation of inguinal hernias was 45% [15]. In
the recent study of Robinson et al., the authors reported thatthe IEA was visible with ultrasonography in all examinedgroins and all of 18 inguinal hernias were correctly classi-Wed as direct or indirect [20]. DiVerences in the scanningtechnique and in selection of patients (size of hernias) maybe explanations of the discrepancies among the cited studiesand the current study. Two series in which 100% visualizationof the IEA was reported consisted of patients with small[13] and occult [20] inguinal hernias, but in the cohorts ofZhang et al. [15] and in the current study, patients withlarger hernias were included. One-third of all hernias in ourseries were large inguinal hernias (types III and VI) (Table 1).Larger inguinal hernias may compress the root segment ofthe IEA, so it becomes invisible with color Doppler ultraso-nography [15].
Some authors have proposed the spermatic cord or theround ligament as alternative landmarks for diVerentiationbetween indirect and direct inguinal hernias [8, 10, 15]. Asthe spermatic cord (or the round ligament) was clearly visi-ble with sonography in all examined groins, we used thosestructures as the main landmarks for location of the internalinguinal ring and the inguinal channel, and for subsequentdiVerentiation between indirect and direct inguinal hernias(Figs. 1, 2, 3). With the previously described methodologyof ultrasonographic examination, we correctly classiWed all“pure” (small and medium) indirect and direct inguinal her-nias (Table 1).
To the best of our knowledge this is the Wrst study inwhich groin hernias have been classiWed by use of ultraso-nography according to the criteria proposed by the morecomplex uniWed classiWcation system [5]. In the currentstudy, total accuracy rate of ultrasonography for determina-tion of groin hernia type was 96% (119 of 124 correct pre-dictions of type of groin hernia compared with surgicalexplorations). Sensitivity and speciWcity of sonography inidentifying the each of eight types of groin hernia are pre-sented in Table 1. For types I (indirect, small), IV (direct,small), V (direct, medium), VII (combined, pantaloon), andVIII (femoral), sensitivity and speciWcity were 100%. Fortype II (indirect, medium), one false positive Wndingdecreased speciWcity to 99% (type III was found by surgicalexploration). The remaining four cases of misdiagnosedhernia types were large mixed indirect and direct hernias(types III and VI) (Table 1). The explanation for suchcross-diagnosis between types III and VI might be theextensiveness of those large hernias, in which the posterioringuinal wall with the internal inguinal ring is completelydisrupted. Therefore, the dominant component (indirect ordirect) of such large hernias could not be recognized insome cases. Otherwise, recommended surgical strategy isthe same for both types of large inguinal hernia [2].
Provoking maneuvers during the ultrasonographic examfacilitates the examiner making a correct diagnosis of groin
123

400 Hernia (2008) 12:395–400
hernia, which was emphasized in all studies [8–21]. Thesize of hernia increases, and peritoneal contents protrudeinto the hernia sac during straining of patient, which isclearly visible by real-time ultrasonography. Dynamicultrasound examination was particularly useful for diagnos-ing the small inguinal hernias in the present series, whichwere clinically occult. In cases of large, mixed inguinal her-nias (types III and VI), the dominant hernia component(indirect or direct) is sonographically obvious at rest, butencroachment of hernia contents into the neighboring area(direct Xoor or the inguinal channel) often becomes visibleonly during straining. Thus, applying the provoking maneu-vers may help the examiner to avoid misdiagnosing largeinguinal hernias as medium ones.
Considering the concept of type-related individualizedgroin hernia repair, maximally accurate and precise pre-operative assessment of type, size, and extensiveness ofhernia is necessary [1–5, 19, 22, 25]. This should allow thesurgeon to choose the most appropriate surgical approachand technique to repair the each type of groin hernia.According to the recommendations of the authorities ingroin hernia surgery, the strategy “one-operation-Wts-all”should be rejected and particular surgical strategies forevery type of groin hernia are proposed in the literature [1,2, 4, 22, 25]. Following this concept, we believed that eachtype of groin hernia should be recognized and describedprecisely with ultrasound prior to operation, and for thispurpose, we applied the uniWed classiWcation system.
In summary, according to the results presented in thisstudy, we may conclude that ultrasonography of the groinregions with a high-frequency linear-array transducer is anaccurate imaging method for precise classiWcation of groinhernias. Each type of groin hernia, according to the uniWedclassiWcation system that we used for classiWcation in ourclinical practice, has a characteristic ultrasonographicappearance, which is demonstrated in this study.
References
1. Nyhus LM (1993) Individualization of hernia repair; a new era.Surgery 114:1–2
2. Nyhus LM (2004) ClassiWcation of groin hernia: milestones. Her-nia 8:87–88. doi:10.1007/s10029-003-0173-6
3. Zollinger RM Jr (1999) A uniWed classiWcation for inguinal her-nias. Hernia 4:195–200
4. Kingsnorth A, LeBlanc KA (2003) Anterior open repair of ingui-nal hernia in adults. In: Kingsnorth A, LeBlanc KA (eds) Manage-ment of abdominal hernias, 3rd edn. Arnold, London, pp 167–170
5. Zollinger RM Jr (2002) ClassiWcation of ventral and groin hernias.In: Fitzgibbons RJ, Greenburg AG (eds) Nyhus and Condon’shernia, 5th edn. Lippincott Willliams and Wilkins, Philadelphia,pp 71–79
6. van den Berg JC, Strijk SP (1992) Groin hernia: role of herniogra-phy. Radiology 184:191–194
7. Aquirre DA, Santosa AC, Casola G, Sirlin CB (2005) Abdominalwall hernias: imaging features, complications, and diagnostic pit-falls at Multi-Detector Row CT. RadioGraphics 25:1501–1520
8. van den Berg JC, de Valois JC, Go PM, Rosenbusch G (1997) Dy-namic magnetic resonance imaging in the diagnosis of groin her-nia. Invest Radiol 32:644–647
9. van den Berg JC, de Valois JC, Go PM, Rosenbusch G (1999)Detection of groin hernia with physical examination, ultrasound,and MRI compared with laparoscopic Wndings. Invest Radiol34:739–743
10. van den Berg JC (2002) Inguinal hernias: MRI and ultrasound. Se-min Ultrasound CT MRI 23:156–173. doi:10.1053/sult.2002.31191
11. Truong SN, Jansen M (2002) Diagnostic imaging in the evaluationand management of abdominal wall hernia. In: Fitzgibbons RJ,Greenburg AG (eds) Nyhus and Condon’s hernia, 5th edn. Lippin-cott Willliams and Wilkins, Philadelphia, pp 81–94
12. Truong S, PWngsten FP, Dreuw B, Schumpelick V (1993) Value ofsonography in diagnosis of uncertain lesions of the abdominal walland inguinal region. Chirurg 64:468–475
13. Korenkov M, Paul A, Troidl H (1999) Color duplex sonography:diagnostic tool in the diVerentiation of inguinal hernias. J Ultra-sound Med 18:565–568
14. Babkova IV, Bozhko VV (1999) Ultrasound assessment in diagno-sis of uncomplicated inguinal hernia. Khirurgiia (Mosk) 2:46–50
15. Zhang GQ, Sugiyama M, Hagi H, Urata T, Shimamori N, AtomiY (2001) Groin hernias in adults: value of color Doppler sonogra-phy in their classiWcation. J Clin Ultrasound 29:429–434
16. Dattola P, Alberti A, Dattola A, Giannetto G, Basile G, Basile M(2002) Inguino-crural hernias: preoperative diagnosis and post-operative follow-up by high-resolution ultrasonography. A per-sonal experience. Ann Ital Chir 73:65–68
17. Bradley M, Morgan D, Pentlow B, Roe A (2003) The groin her-nia––an ultrasound diagnosis? Ann R Coll Surg Engl 85:178–180
18. Lilly MC, Arregui ME (2002) Ultrasound of the inguinal Xoor forevaluation of hernias. Surg Endosc 16:659–662
19. Kraft BM, Kolb H, Kuckuk B, Haaga S, Leibl BJ, Kraft K, BittnerR (2003) Diagnosis and classiWcation of inguinal hernias: accu-racy of clinical, ultrasonographic, and laparoscopic Wndings. SurgEndosc 17:2021–2024. doi:10.1007/s00464-002-9283-y
20. Robinson P, Hensor E, Lansdown MJ, Ambrose S, Chapman AH(2006) Inguinofemoral hernia: accuracy of sonography in patientswith indeterminate clinical features. AJR 187:1168–1178
21. Jamadar DA, Jacobson JA, Morag Y, Girish G, Ebrahim F, Gest T,Franz M (2006) Sonography of inguinal region hernias. AJR187:185–190
22. Moreno-Egea A, Girela E, Canteras M, Martinez D, Aguayo L(2000) Accuracy of clinical diagnosis of inguinal and femoral her-nia and its usefulness for indicating laparoscopic surgery. Hernia4:23–27
23. Shadbolt C, Heinze S, Dietrich R (2001) Imaging of groin masses:inguinal anatomy and pathologic conditions revisited. Radio-Graphics 21:261–271
24. van den Berg JC, de Valois JC, Go PM, Rosenbusch G (2000)Radiological anatomy of the groin region. Eur Radiol 10:661–670
25. Renzulli P, Frei E, Schafer M, Werlen S, Wegmuller H,Krahenbuhl L (1997) Preoperative Nyhus classiWcation of inguinalhernias and type-related individual hernia repair. A case for diag-nostic laparoscopy. Surg Laparosc Endosc 7:373–377
123





























