Embed Size (px)
Citation preview

The Copenhagen Soccer Test: PhysiologicalResponse and Fatigue Development
MADS BENDIKSEN1, RASMUS BISCHOFF1, MORTEN B. RANDERS1, MAGNI MOHR1,2, IAN ROLLO1,3,CHARLOTTE SUETTA4, JENS BANGSBO1, and PETER KRUSTRUP1,2
1Section of Human Physiology, Department of Exercise and Sport Sciences, University of Copenhagen, Copenhagen,DENMARK; 2Sport and Health Sciences, College of Life and Environmental Sciences, St. Luke’s Campus,University of Exeter, Exeter, UNITED KINGDOM; 3Loughborough University, Leicestershire, UNITED KINGDOM;and 4Institute of Sports Medicine Copenhagen, Bispebjerg Hospital, Copenhagen, DENMARK
ABSTRACT
BENDIKSEN, M., R. BISCHOFF, M. B. RANDERS, M. MOHR, I. ROLLO, C. SUETTA, J. BANGSBO, and P. KRUSTRUP. The
Copenhagen Soccer Test: Physiological Response and Fatigue Development. Med. Sci. Sports Exerc., Vol. 44, No. 8, pp. 1595–1603,
2012. Introduction: The aims of the study were 1) to evaluate whether a multifaceted simulated soccer game protocol, entitled the
Copenhagen Soccer Test (CST), elicited a similar physiological loading as a competitive game (CG) and 2) to determine muscle
metabolites, blood variables, and sprint performance in various phases of CST. Methods: Twelve Danish Second- and Third-Division
soccer players participated in the study. On separate days, HR measurements, frequent blood sampling, and physical/technical tests were
performed during 60- and 90-min versions of the CST during which repeated musculus vastus lateralis biopsies were collected. A CG
was also played, where HR was recorded and pre- and post-game muscle biopsies and blood samples were collected. Results: No differences
were observed between CST and CG in average HR (85% T 1% and 86% T 1% HRmax, P 9 0.05) or recovery plasma creatine kinase
(24 h: 312 T 57 and 324 T 76 UILj1, P 9 0.05). Muscle glycogen decreased (P G 0.05) from 459 T 15 to 232 T 30 mmolIkgj1 dry weight
(d.w.) during CST, which was not different from CG (P 9 0.05). The rate of glycogen utilization was 4 T 1 mmolIkgj1 d.w.Iminj1 during
the warm-up and the first 15 min of CST and 1 T 1 mmolIkgj1 d.w.Iminj1 (P G 0.05) from 60 to 90 min of CST. After 15 min of CST,
muscle lactate was elevated (P G 0.05) approximately fivefold (24 T 3 mmolIkgj1 d.w.), and creatine phosphate was lowered (P G 0.05) by
È60% (28 T 4 mmolIkgj1 d.w.). Sprint velocity (2 � 20 m) decreased (P G 0.05) by 7% during CST (5.2 T 0.6 to 4.9 T 0.7 mIsj1).
Conclusions: The physiological response to the CST was reproducible and comparable to that of high-level CG. The CST allowed for rapid
muscle sampling and revealed high creatine phosphate degradation throughout the test and a lowered glycogen utilization toward the end
of the simulated game. Key Words: MUSCLE GLYCOGEN UTILIZATION, MUSCLE CRP, LACTATE, PLASMA CK, SPRINT
PERFORMANCE, ASSOCIATION FOOTBALL
During the last three decades, numerous studies haveinvestigated the activity profile of elite soccergames, and some studies have also examined the
HR and blood lactate response, although this has mostlybeen done during friendly games (4,6,10,24,30). Few stud-ies have determined the muscle and blood metabolites invarious phases of soccer games or during soccer-specificexercise (13,16,17,23,37,39) because of the inherent diffi-culties in obtaining such measurements. Exercise intensitychanges dramatically throughout a soccer game (24,26),which has an effect on the physiological response to differ-
ent game periods. Thus, the response is to a great extentdependent upon the activities immediately before sampling.Moreover, the amount of high-intensity running and sprint-ing is highly variable from game to game in elite soccer (12).Therefore, protocols in which soccer games are simulatedcan be a useful tool that allows for controlled and repro-ducible evaluations of the effect of various interventionssuch as strength and conditioning regimens, dietary effectson recovery, effect of playing on different surfaces, and theinfluence of the temperature and altitude on the physicalperformance.
Some studies have attempted to simulate the intermittentworkload of soccer by the use of intermittent treadmill run-ning with similar HR responses as in elite soccer (9,35).However, these protocols lack many soccer-specific move-ments such as backward and sideways running and directionchanges along with technical skills including passing, drib-bling, and heading. A few studies have included soccer-specific skills and investigate the effect of soccer-relatedexercise on technical performance (11,28,32), but these testsare shorter than the full game, and the physiological re-sponse and performance development during the tests have
Address for correspondence: Professor Peter Krustrup, PhD, Section ofHuman Physiology, Department of Exercise and Sport Sciences, Universityof Copenhagen, August Krogh Building, Universitetsparken 13, Copenhagen2100, Denmark; E-mail: [email protected] for publication September 2011.Accepted for publication January 2012.
0195-9131/12/4408-1595/0MEDICINE & SCIENCE IN SPORTS & EXERCISE�Copyright � 2012 by the American College of Sports Medicine
DOI: 10.1249/MSS.0b013e31824cc23b
1595
APPLIED
SCIEN
CES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

not been compared with similar measures during competi-tive soccer games.
Thus, the purpose of the present study was to develop andvalidate a test that simulates the work and physiological re-sponse of players during a soccer game. The test shouldresult in fatigue development comparable to competitivegames (CG) and allow for instantaneous and frequent mea-surements of muscle and blood metabolites, making it pos-sible to study the contribution of anaerobic energy turnoverand the rate of glycogen utilization in various phases of a90-min simulated soccer game.
METHODS
Subjects
Twelve Second- and Third-Division Danish soccer play-ers, with a mean T SD age, height, body mass, fat percent-age, and VO2max of 24.2 T 4.5 yr, 181.2 T 6.5 cm, 80.0 T7.5 kg, 15.8 T 3.4, and 4.93 T 0.33 LIminj1, correspondingto 61.5 T 5.1 mLIkgj1Iminj1, respectively, participated inthe study. The players had a Yo-Yo Intermittent Recoverylevel 2 test performance of 761 T 89 m. All players werefully informed of experimental procedures and possiblediscomforts associated with the study before giving theirwritten informed consent to participate. The study was ap-proved by the ethics committee of the Copenhagen andFrederiksberg communities (KF-01-307803).
Experimental Design
All players (n = 12) carried out the Copenhagen SoccerTest (CST) consisting of 2 � 45 min of soccer-specificmovements interspersed with a 15-min half-time break (seebelow). HR was measured continuously during the CST, andblood samples were collected every 5 min throughout theCST and during the first 15 min of recovery (Fig. 1). Sevenplayers had a quadriceps muscle biopsy collected for me-tabolite measurements at rest and after the test (90 min ofactivity, CST90). To evaluate the reproducibility of thephysiological response to CST, the 12 players also carriedout a 60-min version of the CST (CST60) with HR meas-urements and blood sampling as in CST90. The CST60 wasalso used for intermediate muscle metabolite measurementsas quadriceps muscle biopsies were collected for the sameseven players after 15 min of activity as well as after the test(60 min) (Fig. 1). To compare the physiological response ofCST to CG, the same seven players had muscle biopsiesand blood samples collected immediately after a CG and HRrecorded throughout the game. The CG was played in theafternoon, whereas the CST was conducted in the morning(9 a.m. to 12 noon) or afternoon (1–4 p.m.). The score of theinvestigated matches was 2–1, 1–1, and 1–3, and all matchesinfluenced the league ranking. The time of day was heldconstant between the two CST tests for each player.
CST. The CST is designed as a 2 � 45-min field test, inwhich the players meet the physical demands equivalent to
what has been previously reported during CG (24). To meetthe physical demands of elite soccer games, the movementpatterns, the amount of high-intensity running, the time withthe ball, and the number of headers, shots, and passes wereall put into the design. The activity pattern was based on thestudy of Mohr et al. (24), which described 42 soccer playersat a high competitive level, on the basis of individual time–motion analysis (6,15,24). From the time–motion analysis,the study presented the mean duration of the eight differentlocomotive categories, and on the basis of those, the meandistance of one movement in each of the locomotive cate-gories was calculated. Furthermore, the simulated test wasdivided into 18 periods of 5 min because it has been shownthat an individual’s exercise intensity varies throughout a soccergame (8, 24), and this subdivision of the test would allow forlow-, medium-, and high-intensity periods throughout the test(Fig. 2). The final version of the CST consisted of repeated5-min bouts each representing 152, 171, 69, 41, 55, 40, 30,and 23 m of walking (È6 kmIhj1); jogging (È8 kmIhj1);low- (È12 kmIhj1), moderate- (È15 kmIhj1), and high-speed running (È18 kmIhj1); sprinting (925 kmIhj1);backward running (È10 kmIhj1); and backward/sidewaysrunning (È8 kmIhj1), respectively. The 40 m of sprintingwas performed as a 20-m shuttle sprint. The 5-min bouts
FIGURE 1—Schematic representation of the CST, including multiplerepetitions of forward, backward, and sideways running at variousspeeds (sprinting and HS, MS, and LS, i.e., high-, moderate-, and low-speed running) as well as jump, shots, dribbles, and turns with andwithout the ball. A 2 � 20-m sprinting test and technical free-kick andpassing tests are also shown. The players run one full circuit every5 min, and the intensity is varied between low-intensity, medium-intensity,and the high-intensity 5-min segments by adjusting the amount of moder-ate speed and high-intensity running performed at the end of each circuit,i.e., the penalty area triple shuttle.
http://www.acsm-msse.org1596 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

were categorized as a low- (L), moderate- (M), or high-intensity(H) bout where the medium- and high-intensity bouts includedan additional 20 and 60 m of moderate-speed running, respec-tively, and 22 and 65 m of high-speed running, respectively.Both the CST90 and the CST60 consisted of two halves,interspersed by a 15-min break with no activities. The firsthalf consisted of 9 � 5-min periods carried out in the orderL-M-H-L-M-M-L-M-H (Fig. 2), which was repeated in thesecond half of the CST90, whereas the second half of theCST60 consisted of 3 � 5-min bouts performed in the orderL-M-H. The total distance covered during CST60 andCST90 was 7.55 and 11.29 km, respectively, of which 2.12and 3.28 km, respectively, was covered with high-intensityrunning. Furthermore, 0.48 and 0.72 km was covered with
sprinting in CST60 and CST90, respectively. At the end ofeach 5-min period, 15- to 20-s rest periods were incorpo-rated for collection of blood samples or other physiologicalmeasurements. The test was also designed to allow moredetailed measurements of the player’s technical abilities andphysical performance during a game. This was done by in-corporating a sprint test and a technical shooting–passingperformance test into each 5-min segment of the protocol(Fig. 1). The players had individual water bottles preparedand were allowed to drink 1 L of water during the test. Theplayers were supervised during the test by experienced testpersonnel. Before the CST as well as the CG, the playersrefrained from strenuous exercise and intake of alcohol for48 h and from tobacco and caffeine for 12 h. All subjectswere instructed to follow their habitual diet before all testingsessions and theCG.TheCSTwas carried out on a 60� 106-mnatural grass soccer field.
Sprint Tests
After the 15-min warm-up before the CST90 and CST60,the players performed a repeated sprint test consisting of five2 � 20-m shuttle sprints with 30 s of rest between the sprints(Fig. 1). At the end of every 5-min segment of the 90- and60-min CST protocols, the players performed single 2 �20-m shuttle sprints. The sprints were initiated from a stand-ing position, 30 cm behind the first timing gate, and splittimes were recorded at 15, 25, and the full 40 m. Sprint timeswere recorded by photocell gates with a precision of 0.001 splaced 1.0 m above the ground (Newtest Powertimer System;Oulu, Finland).
Technical Performance Test
The technical testing included in the CST90 and CST60was composed of free-kick shooting and passing (Fig. 1).The shooting test allowed the player to shoot once every5 min throughout CST at a standard 11-a-side goal (2.44 �7.32 m). The goal was divided into six areas by two vertical6-cm-wide nylon strings placed 1.20 m from the goalpostsand one horizontal string placed at a height of 1.14 m. Oneand a half minutes into each 5-min segment, the players had10 s to make a shot at the goal from a distance of 20.15 m.The players were awarded points as to how accurate they hitthe goal, i.e., five points for shots in the top corners; threepoints for shots in the bottom corner, at the corner posts, andin the top middle part of the goal; one point for shots in thebottom middle part of the goal, at the lowest part of theposts, and at the top middle part of the bar; and zero pointsfor shots wide of the goal. The passing test was carried outas previously described (32) allowing the player to make onelong, high pass every 5 min throughout the test. Three and ahalf minutes into each 5-min segment, after running 30 m at15 kmIhj1, the players had one touch on the ball beforemaking a 30-m long airborne pass in the running directionaiming at hitting a 50-m2 area close to the goal line (Fig. 1).
FIGURE 2—Schematic presentation of a 90-min trial of the CST, in-cluding physiological measures performed before, during, and after thetest (A) and sprint velocity (mIsj1) for the 2 � 20-m sprint tests duringthe CST (B). Data are means T SEM. *Significantly different from thelast sprint.
THE COPENHAGEN SOCCER TEST Medicine & Science in Sports & Exercised 1597
APPLIED
SCIEN
CES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

The accuracy of the 30-m pass was awarded with points asfollows: five points if the ball landed in the inner area (6 � 3m), three points if it landed in the middle area (8� 4 m), andone point if it landed in the outer area (10 � 5 m) with zeropoints if the ball missed the target. The points from theshooting and passing were summed in six 15-min intervals.
Muscle and Blood Sampling
The muscle biopsies (È70–120 mg wet weight [w.w.])were obtained from musculus vastus lateralis in the right legusing the Bergstrom needle biopsy technique with suction.All biopsies, including the biopsies taken during the CST,were obtained with the subjects lying in the supine positionon a portable bed. Muscle biopsies during the CST werecollected 5–15 s after a high-intensity run with the portablebed standing 1–2 m from the cone that marked the end of therunning bout. Five to 15 mins after the CG, muscle biopsiesand blood samples were collected in the dressing room sit-uated right next to the stadium. Blood samples were takenfrom an antecubital vein in the right arm using flexi-ble venflon cannulas (18 gauge, 32 mm). Samples were col-lected in 5-mL syringes, and the cannula was flushed withsaline after each blood draw. Within 10 s of sampling, 100 KLof blood was hemolyzed in an ice-cold 100-KL Triton X-100buffer solution (Sigma-Aldrich, Brondby, Denmark) andwas later analyzed for lactate and glucose using a YSI 2300lactate analyzer (Yellow Springs Instruments, Yellow Springs,OH). The rest of the sample was rapidly centrifuged for 30 s.From this, plasma was collected and stored at j20-C until asubsequent analysis could be performed. Plasma free fattyacid (FFA) concentration was measured fluorometrically usingan enzymatic kit (Wako Chemical, Neuss, Germany). Plasmacreatine kinase (CK) was analyzed by the use of Roche kits on aHitashi 912 Automatic Analyzer (Roche Diagnostics, Indian-apolis, IN) (34).
HR Measurements
HR was recorded in 5-s intervals during CST and the CGusing Polar Team 1 HR monitors (Polar Electro, Kempele,Finland). The data were subsequently stored on a computerusing a Team 1 interface (Polar Electro, Kempele, Finland).
Laboratory Treadmill Test
The laboratory treadmill test consisted of a submaximaltest before completion of an incremental test to exhaustion.The submaximal test consisted of 6-min runs at runningspeeds of 10, 12, 14, and 16 kmIhj1 interspersed by 2-minbreaks. Fifteen minutes after the submaximal test, the in-cremental test to exhaustion was conducted. After running14 kmIhj1 for 4 min, the velocity increased with a stepwise1-kmIhj1 speed inclination every 30 s until volitional ex-haustion. During each submaximal running bout and duringthe exhaustive test, HR was continuously measured usingthe Polar Team 1 belts (Polar Electro, Kempele, Finland),and pulmonary oxygen uptake was measured using a breath-
by-breath gas analyzer (Jaeger MasterScreen CPX; ViasysHealthcare, GmbH, Hoechberg, Germany). This system wascalibrated before each trial with two gases of known con-centrations. Individual values for VO2max and HRmax weredetermined as the peak values reached in 15- and 5-s peri-ods, respectively.
Yo-Yo Intermittent Recovery Testing
All players performed the Yo-Yo Intermittent RecoveryTest level 2 (8,17). After a 10-min warm-up, the playersperformed the test, which consists of repeated 2� 20-m runsback and forth between the start and finish line at a pro-gressively increased speed controlled by audio bleeps from atape recorder. Between the running bouts, the participantshad a 10-s active recovery period where they jogged arounda cone placed 5 m behind the finish line. When the par-ticipants twice failed to reach the finish line in time, thedistance covered was recorded and was used as the test re-sult. Performance in this test has been shown to be a goodindicator of physical fitness for high-level soccer players(5,16,19,29).
Muscle Analysis
The muscle tissue was immediately frozen in liquid N2
and stored at j80-C. The frozen sample was weighed be-fore and after freeze drying to determine water content. Afterfreeze drying, the muscle samples were dissected free ofblood, fat, and connective tissue, and about 1-mg dry weight(d.w.) tissue was extracted in a solution of 0.6-M perchloricacid and 1-mM EDTA, neutralized to pH 7.0 with 2.2-MKHCO3 and stored at 80-C until analyzed fluorometricallyfor lactate and creatine phosphate (CrP) (22). About 2-mgd.w. muscle tissue was extracted in 1-M HCl and hydrolyzedat 100-C for 3 h, after which the glycogen content was de-termined by the hexokinase method (22). For the biopsiesweighing more than 60 mg w.w., about 20 mg w.w. was usedfor histochemical analyses (n = 7 for rest and CST60, n = 4for CST90 and CG). This process included mounting of thesample in an embedding medium (OCT Compound Tissue-Tek; Sakura Finetek, Zoeterwoude, The Netherlands) andfreezing in isopentane. After storage atj80-C, these sampleswere cut in serial 10-Km-thick slices for adenosine triphos-phatase staining of fiber type distribution (18) and in 16-Km-thick slices for the periodic acid–Schiff analyses of glycogencontent. The individual fibers were analyzed by a researcherwho was blinded as to when the biopsies were collected.Each slow-twitch (ST) and fast-twitch (FT) fiber was ratedas full of glycogen (80%–100%), partly full (60%–79%),half full (40%–59%), almost empty (20%–39%), or empty(0%–19%) using the computer-based software Tema95 (Temaversion 1.04; CheckVision ApS, Hadsund, Denmark) (18).
Statistical Analysis
Changes in muscle and blood variables as well as sprintperformance during CST90 were evaluated using a one-way
http://www.acsm-msse.org1598 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

ANOVA with repeated measures. Differences in the HRduring the CST and the CG as well as differences in HR andblood metabolites during CST60 and the first 60 min ofCST90 were evaluated using a two-way ANOVA with re-peated measures. When a significant interaction was detected,data were subsequently analyzed using a Newman–Keuls posthoc test. Differences in the muscle glycogen concentrationafter the CST and the CG were evaluated by a Student’spaired t-test. The coefficient of variance was calculated asthe SD of the individual differences in the test–retest re-sult divided by the mean test result and multiplied by 100.A significance level of 0.05 was chosen. Data are presentedas means T SEM unless otherwise stated.
RESULTS
Comparison between CST and CG. Mean HR was85% T 1% and 86% T 1% HRmax (P 9 0.05) during the CSTand the CG, with corresponding values for peak HR of 96% T1% and 97% T 1% HRmax (P 9 0.05). The HR during CST
was G70%, 70%–80%, 80%–90%, and 990% of individualHRmax for 5% T 2%, 29% T 6%, 47% T 4%, and 18% T 5% oftotal time, respectively, which was not different from the CG(5% T 3%, 22% T 3%, 46% T 8%, and 27% T 8% of totaltime).
Muscle glycogen was 235 T 27 mmolIkgj1 d.w. at the endof CST, which was not significantly different from the CG(188 T 19 mmolIkgj1 d.w.; Fig. 3A). The difference inpostgame glycogen content between CST and CG was lessthan 35 mmolIkgj1 d.w. for all players, except for one(Fig. 3A). At rest, 83% and 85% of all ST and FT fibers,respectively, were full of glycogen with no individual fibersbeing half full, partly full, or empty of glycogen (Fig. 4).After 90 min of CST, 80% and 84% of the ST and FT fibers,respectively, were empty or partly empty of glycogen, withcorresponding values of 98% and 100% for the CG (Fig. 4).
The plasma CK was 229 T 48 UILj1 immediately afterand 312 T 57 UILj1 24 h after CST, which was not signif-icantly different from the corresponding values after theCG (200 T 21 and 324 T 76 UILj1, respectively).
Sprint performance and physiological responseto CST. Sprint velocity in the first four 2 � 20-m sprintsin CST (5–20 min) was 5.2 T 0.6, 5.2 T 0.4, 5.1 T 0.4, and5.1 T 0.4 mIsj1, which was 5%–7% higher (P G 0.05) than inthe last sprint carried out after 90 min of CST (4.9 T0.7 mIsj1; Fig. 2B).
Muscle glycogen at rest was 459 T 15 mmolIkgj1 d.w.and decreased (P G 0.05) by 26%, 43%, and 50% after 15,60, and 90 min of CST (Fig. 3B). The mean net rate ofmuscle glycogen utilization was 4.0 T 1.2 mmolIkgj1
d.w.Iminj1 during the warm-up and the first 15 min of CSTand was lowered (P G 0.05) to 1.8 T 0.5 mmolIkgj1
d.w.Iminj1 from 15 to 60 min and 0.9 T 1.2 mmolIkgj1
d.w.Iminj1 from 60 to 90 min.
FIGURE 4—Relative glycogen content in ST and FT fibers at rest, after60 and 90 min of the CST, and after a CG. Mean values are presentedfor n = 7 (rest, CST60) and n = 4 (CST90 and CG).
FIGURE 3—Muscle glycogen, expressed as percent of peak individualglycogen level, after 90 min of the CST and a CG (A), as well as inabsolute muscle glycogen content (mmolIkgj1 d.w.) at rest and after 15,60, and 90 min of CST (B). Mean and individual values are presented.*Significant difference from rest; #Significant difference from 15 min.
THE COPENHAGEN SOCCER TEST Medicine & Science in Sports & Exercised 1599
APPLIED
SCIEN
CES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
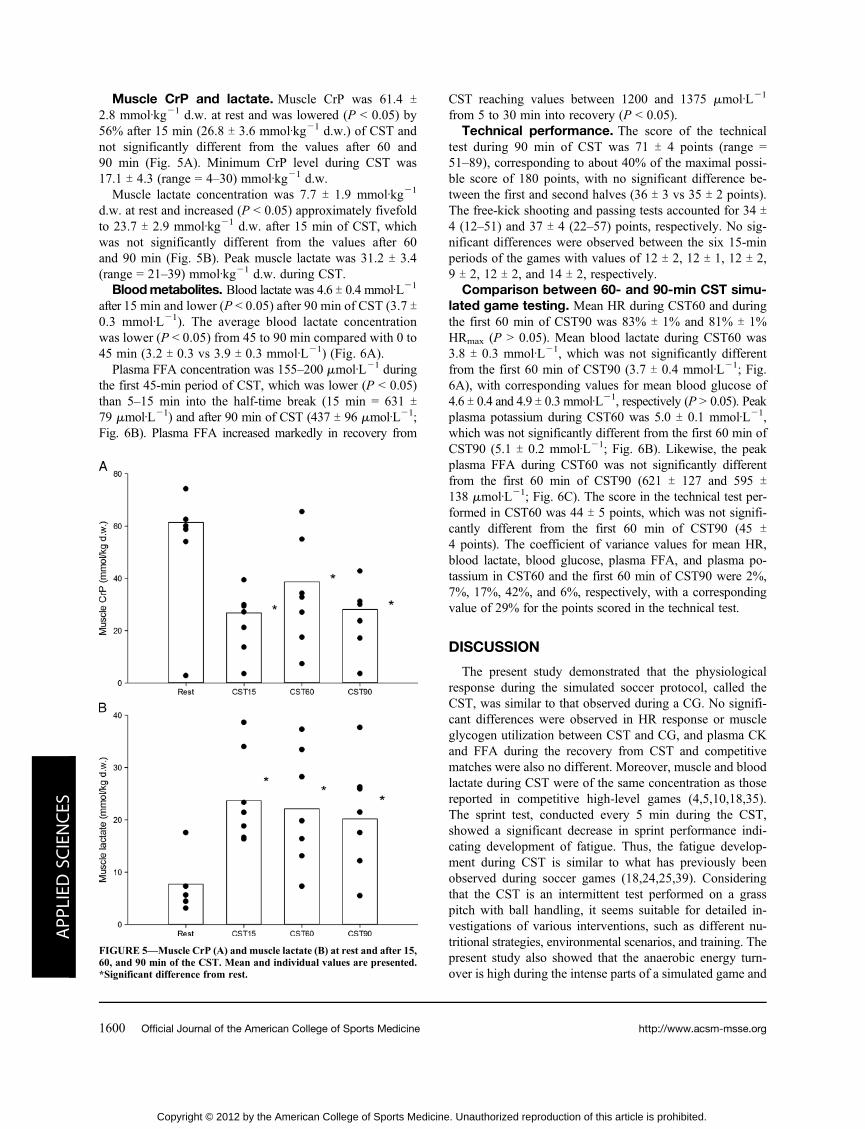
Muscle CrP and lactate. Muscle CrP was 61.4 T2.8 mmolIkgj1 d.w. at rest and was lowered (P G 0.05) by56% after 15 min (26.8 T 3.6 mmolIkgj1 d.w.) of CST andnot significantly different from the values after 60 and90 min (Fig. 5A). Minimum CrP level during CST was17.1 T 4.3 (range = 4–30) mmolIkgj1 d.w.
Muscle lactate concentration was 7.7 T 1.9 mmolIkgj1
d.w. at rest and increased (P G 0.05) approximately fivefoldto 23.7 T 2.9 mmolIkgj1 d.w. after 15 min of CST, whichwas not significantly different from the values after 60and 90 min (Fig. 5B). Peak muscle lactate was 31.2 T 3.4(range = 21–39) mmolIkgj1 d.w. during CST.
Bloodmetabolites. Blood lactate was 4.6 T 0.4 mmolILj1
after 15 min and lower (P G 0.05) after 90 min of CST (3.7 T0.3 mmolILj1). The average blood lactate concentrationwas lower (P G 0.05) from 45 to 90 min compared with 0 to45 min (3.2 T 0.3 vs 3.9 T 0.3 mmolILj1) (Fig. 6A).
Plasma FFA concentration was 155–200 KmolILj1 duringthe first 45-min period of CST, which was lower (P G 0.05)than 5–15 min into the half-time break (15 min = 631 T79 KmolILj1) and after 90 min of CST (437 T 96 KmolILj1;Fig. 6B). Plasma FFA increased markedly in recovery from
CST reaching values between 1200 and 1375 KmolILj1
from 5 to 30 min into recovery (P G 0.05).Technical performance. The score of the technical
test during 90 min of CST was 71 T 4 points (range =51–89), corresponding to about 40% of the maximal possi-ble score of 180 points, with no significant difference be-tween the first and second halves (36 T 3 vs 35 T 2 points).The free-kick shooting and passing tests accounted for 34 T4 (12–51) and 37 T 4 (22–57) points, respectively. No sig-nificant differences were observed between the six 15-minperiods of the games with values of 12 T 2, 12 T 1, 12 T 2,9 T 2, 12 T 2, and 14 T 2, respectively.
Comparison between 60- and 90-min CST simu-lated game testing. Mean HR during CST60 and duringthe first 60 min of CST90 was 83% T 1% and 81% T 1%HRmax (P 9 0.05). Mean blood lactate during CST60 was3.8 T 0.3 mmolILj1, which was not significantly differentfrom the first 60 min of CST90 (3.7 T 0.4 mmolILj1; Fig.6A), with corresponding values for mean blood glucose of4.6 T 0.4 and 4.9 T 0.3 mmolILj1, respectively (P 9 0.05). Peakplasma potassium during CST60 was 5.0 T 0.1 mmolILj1,which was not significantly different from the first 60 min ofCST90 (5.1 T 0.2 mmolILj1; Fig. 6B). Likewise, the peakplasma FFA during CST60 was not significantly differentfrom the first 60 min of CST90 (621 T 127 and 595 T138 KmolILj1; Fig. 6C). The score in the technical test per-formed in CST60 was 44 T 5 points, which was not signifi-cantly different from the first 60 min of CST90 (45 T4 points). The coefficient of variance values for mean HR,blood lactate, blood glucose, plasma FFA, and plasma po-tassium in CST60 and the first 60 min of CST90 were 2%,7%, 17%, 42%, and 6%, respectively, with a correspondingvalue of 29% for the points scored in the technical test.
DISCUSSION
The present study demonstrated that the physiologicalresponse during the simulated soccer protocol, called theCST, was similar to that observed during a CG. No signifi-cant differences were observed in HR response or muscleglycogen utilization between CST and CG, and plasma CKand FFA during the recovery from CST and competitivematches were also no different. Moreover, muscle and bloodlactate during CST were of the same concentration as thosereported in competitive high-level games (4,5,10,18,35).The sprint test, conducted every 5 min during the CST,showed a significant decrease in sprint performance indi-cating development of fatigue. Thus, the fatigue develop-ment during CST is similar to what has previously beenobserved during soccer games (18,24,25,39). Consideringthat the CST is an intermittent test performed on a grasspitch with ball handling, it seems suitable for detailed in-vestigations of various interventions, such as different nu-tritional strategies, environmental scenarios, and training. Thepresent study also showed that the anaerobic energy turn-over is high during the intense parts of a simulated game and
FIGURE 5—Muscle CrP (A) and muscle lactate (B) at rest and after 15,60, and 90 min of the CST. Mean and individual values are presented.*Significant difference from rest.
http://www.acsm-msse.org1600 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

that the rate of muscle glycogen utilization decreases pro-gressively during a 90-min soccer simulation.
The mean rate of glycogen utilization in the CST was ofthe same magnitude as that during the CG and at a level alsoobserved in other games (4,5,14,18,20,21,35). Furthermore,the average HR and HR distribution were similar in the CSTand the CG and also consistent with values reported duringgames in other studies (4,20,24,27,28,29). Likewise, theplasma CK levels were similar during the first 24 h after theCST and the CG, which may indicate that the soccer-specificmovements in the CST caused a degree of muscle damagecomparable to that of CG. Muscle and blood lactate duringthe CST were also of the same magnitude as those observedin competitive and friendly games (4,6,10,18). However,it should be emphasized that a comparison is difficult be-cause both blood and muscle lactate are dependent on theactivities just before the sampling. This observation is rein-forced by the results of the present study where blood lactatewas the highest 5 min after the most intense exercise period(Fig. 6A). Thus, the physiological response to the CST is toa large degree similar to that observed during CG.
Several simulated soccer protocols have been performedusing a motorized treadmill (9,13). Although treadmill pro-tocols simulate the intermittent running of competitive soc-cer games, average HR for high-level soccer players areapproximately 20 bpm lower when running on a treadmill atthe speeds observed during games (4,9,13). This may wellbe explained by the fact that the players in competitivesoccer games are doing multiple specific intense activi-ties that elevate the energy demand, such as fast sidewaysmovement, handling the ball, stopping, and tackling. In thestudy by Drust et al. (9), the treadmill running speeds wereelevated so that the average HR was similar to elite footballgames (162 T 10 bpm). Nonetheless, protocols conducted onmotorized treadmills have severe limitations. For example, itis difficult to obtain maximal running speeds, and frequentmotion changes (every 3–4 s, including backward and side-ways running) and other soccer-specific movements cannotbe performed. Another well-known soccer simulation test isthe Loughborough Intermittent Shuttle Test (LIST) (23,38),which is performed as a 20-m shuttle run test. It representsmore frequent changes in running speeds, and it allows formaximal accelerations and decelerations. HR response to theLIST reveals differences in HR equivalent to those observedin the simulations on a treadmill (23,38) but lower lactatevalues than during competitive soccer matches. Despite al-lowing for frequent changes in running speeds and maximalaccelerations and decelerations, the LIST does not simulateother soccer-specific movements, nor does the protocol allowfor handling the ball. Pilot CST results reproducing the ac-tivities and running speeds observed during CG (8,24,27) also
FIGURE 6—Blood lactate (A), plasma potassium (B), and plasma FFA(C) before, during, and after 60 min (open circles) and 90 min (closedcircles) of the CST. L, M, and H represent low-, moderate-, and high-intensity 5-min segments, respectively. ST represents the shooting test.HT stands for half time. Data are means T SEM.
THE COPENHAGEN SOCCER TEST Medicine & Science in Sports & Exercised 1601
APPLIED
SCIEN
CES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

resulted in lower HR and blood lactate. Therefore, it wasdecided to increase the amount of high-intensity work and thenumber of sprints. The final version of the CST has the ad-vantage that it includes soccer-specific movements, ballhandling, and frequent and marked alterations in exerciseintensity as has been substantiated in real soccer games(1,8,24,26,29) and that it is performed on the same surface(1). Moreover, it evaluates both physical and technical per-formance throughout the test, in a similar manner as was donein Rugby (36), which allows for a detailed examination offatigue development.
The CST was used to examine the muscle metabolic re-sponse during a soccer game. The rate of muscle glyco-gen utilization during the first part of the game wassignificantly higher than that during the rest of the game.Even when taking into account a possible resynthesis ofmuscle glycogen at half time, corresponding to about0.9 mmolIkgj1 d.w.Iminj1 (at a muscle glycogen concen-tration of 300 mmolIkgj1 d.w. [7]), the net rate of glyco-genolysis during the warm-up and the first 15 min of thegame was at the least twofold higher than from 15 to 60 minand fourfold higher than during the last part of the game(Fig. 3). It would be expected that the differences are evengreater during CG because the amount of high-intensitywork is the highest in the initial 15 min (24,26,27), whichwas not the case during the CST. Therefore, a novel findingof the present study is that the rate of glycogenolysis ismarkedly reduced in the middle of the game and even moreso toward the end of the simulated soccer game (Fig. 3). Itmay be related to a progressive increase in fat oxidation asthe game progresses. The potential for fat oxidation is ele-vated because plasma FFA increased with exercise time asalso observed in CG (4,18), an observation that may be re-lated to lowered insulin levels and elevated levels of cat-echolamines leading to an increased lipolysis in the adiposetissue and, thus, a more pronounced release of fatty acidsinto the circulation (2,4).
Sprint performance decreased toward the end of CST asalso demonstrated in CG (18,19,25,27). It has been sug-gested that fatigue under these conditions occur because of adepletion of glycogen in some muscle fibers toward the endof a game (3,7,14,18,20,21,33). The present study showedthat the muscle glycogen level after both the CST and theCG was È50% of the resting state. This may have influ-enced the sprint performance because it is shown that a
muscle glycogen level of less than È200 mmolIkgj1 d.w.decreases the rate of glycolysis noticeably (4). Moreover, thedepletion pattern of the individual fibers was examined, andit was demonstrated that all fiber types had a marked de-crease in glycogen with more than 80% of the fibers beingempty or almost empty of glycogen after both the CST andthe CG (Fig. 4). In addition, the histochemical analysisrevealed low glycogen levels after 60 min of the CST withÈ55% of all fibers being empty or almost empty.
Muscle CrP has been determined in biopsies obtainedduring a soccer game (18) and a short-term simulated soccerprotocol (32). However, because of the delay in collectingthe muscle sample and a high rate of CrP resynthesis afterexercise, these values probably do not represent the levelimmediately after an intense action during a game. In thepresent study, muscle samples were obtained within 10 safter a sprint, and the muscle CrP values were significantlylower than observed previously (18). The values were, how-ever, not as low as observed after intense continuous work,and it is doubtful whether lowered muscle CrP played a rolein the fatigue development. This notion was also supportedby the findings that sprint performance was not impaired af-ter 15 min of CST where muscle CrP concentrations were aslow as those recorded at end of CST.
In summary, the physiological response and the fatiguedevelopment during the CST represent those observed dur-ing a competitive soccer game. Therefore, the test can beconsidered a valid test when investigating the effect of en-vironmental temperature, nutritional supplementation, andtraining on the physiological response to and physical per-formance in soccer. The present study also showed that therate of muscle glycogen utilization decreases progressivelyduring a game and that the impaired sprint performance to-ward the end of game may be related to lowered muscleglycogen levels.
The study was supported by Team Denmark and the DanishMinistry of Culture (Kulturministeriets Udvalg for Idr&tsforskning).There is no conflict of interest for any of the article authors.
The authors thank the players and their elite soccer clubs for theparticipation. They also thank the Danish Football Association(Dansk Boldspil-Union) for their cooperation. The technical assistanceby Jens Jung Nielsen, Bengt Saltin, Lars Nybo, Niels H. Secher,Joshua Horton, Sarah R. Jackman, Per Hansen, Christoffer Krustrup,and Christian Hasson is appreciated.
The results of the present study do not constitute endorsement bythe American College of Sports Medicine.
REFERENCES
1. Andersson H, Ekblom B, Krustrup P. Elite football on artificial turfversus natural grass: movement patterns, technical standards, andplayer impressions. J Sports Sci. 2008;26(2):113–22.
2. Arner P, Kriegholm E, Engfeldt P. In situ studies of catechol-amine-induced lipolysis in human adipose tissue using micro-dialysis. J Pharmacol Exp Ther. 1990;254(1):284–8.
3. Balsom PD, Gaitanos GC, Soderlund K, Ekblom B. High-intensityexercise and muscle glycogen availability in humans. Acta PhysiolScand. 1999;165:337–45.
4. Bangsbo J. Energy demands in competitive soccer. J Sports Sci.1994;12:S5–12.
5. Bangsbo J, Mohr M, Krustrup P. Physical and metabolic demandsof training and match-play in the elite football player. J Sports Sci.2006;24:665–74.
6. Bangsbo J, Norregaard L, Thorsoe F. Activity profile of competi-tion soccer. Can J Sport Sci. 1991;16:110–6.
7. Bangsbo J, Norregaard L, Thorsoe F. The effect of carbohydratediet on intermittent exercise performance. Int J Sports Med. 1992;13:152–7.
8. Bradley PS, Sheldon W, Wooster B, et al. High-intensity runningin English FA Premier League soccer matches. J Sports Sci. 2009;27(2):159–68.
http://www.acsm-msse.org1602 Official Journal of the American College of Sports Medicine
APP
LIED
SCIENCES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.

9. Drust B, Reilly T, Cable NT. Physiological response to laboratory-based soccer-specific intermittent and continuous exercise. J SportsSci. 2000;18:885–92.
10. Ekblom B. Applied physiology of soccer. Sports Med. 1986;3:50–60.
11. Foskett A, Ali A, Gant N. Caffeine enhances cognitive functionand skill performance during simulated soccer activity. Int J SportNutr Exerc Metab. 2009;19(4):410–23.
12. Gregson W, Drust B, Atkinson G, Salvo VD. Match-to-matchvariability of high-speed activities in Premier League soccer. Int JSports Med. 2010;31(4):237–42.
13. Greig MP, McNaughton LR, Lovell RJ. Physiological and me-chanical response to soccer-specific intermittent activity andsteady-state activity. Res Sports Med. 2006;14(1):29–52.
14. Jacobs I, Westlin N, Karlsson J, et al. Muscle glycogen and diet inelite soccer players. Eur J Appl Physiol Occup Physiol. 1982;48:297–302.
15. Krustrup P, Bangsbo J. Physiological demands of top-class soccerrefereeing in relation to physical capacity: effect of intense inter-mittent exercise training. J Sports Sci. 2001;19(11):881–91.
16. Krustrup P, Mohr M, Amstrup T, et al. The Yo-Yo IntermittentRecovery Test: physiological response, reliability, and validity.Med Sci Sports Exerc. 2003;35(4):697–705.
17. Krustrup P, Mohr M, Nybo L, et al. The Yo-Yo IR2 test: physio-logical response, reliability, and application to elite soccer. MedSci Sports Exerc. 2006;38(9):1666–73.
18. Krustrup P, Mohr M, Steensberg A, et al. Muscle and bloodmetabolites during a soccer game: implications for sprint perfor-mance. Med Sci Sports Exerc. 2006;38(6):1165–74.
19. Krustrup P, Zebis M, Jensen JM, Mohr M. Game-induced fa-tigue patterns in elite female soccer. J Strength Cond Res. 2010;24:437–41.
20. Krustrup P, Ortenblad N, Nielsen J, et al. Maximal voluntarycontraction force, SR function and glycogen resynthesis during thefirst 72 h after a high-level competitive soccer game. Eur J ApplPhysiol. 2011;111(12):2987–95.
21. Leatt PB, Jacobs I. Effect of glucose polymer ingestion on glyco-gen depletion during a soccer match. Can J Sport Sci. 1989;14(2):112–6.
22. Lowry OH, Passoneau JV. A Flexible System of Enzymatic Anal-ysis. New York (NY): Academic; 1972. p. 237–49.
23. Magalhaes J, Rebelo A, Oliveira E, Silva JR, Marques F, AscensaoA. Impact of Loughborough Intermittent Shuttle Test versus soccermatch on physiological, biochemical and neuromuscular parame-ters. Eur J Appl Physiol. 2010;108:39–48.
24. Mohr M, Krustrup P, Bangsbo J. Match performance of high-standard soccer players with special reference to development offatigue. J Sports Sci. 2003;21:519–28.
25. Mohr M, Krustrup P, Nybo L, Nielsen JJ, Bangsbo J. Muscletemperature and sprint performance during soccer matches—effectof a re–warm-up at half-time. Scand J Med Sci Sports. 2004;14(3):156–62.
26. Mohr M, Krustrup P, Andersson H, Kirkendal D, Bangsbo J.Match activities of elite women soccer players at different perfor-mance levels. J Strength Cond Res. 2008;22(2):341–9.
27. Mohr M, Mujika I, Santisteban J, et al. Examination of fatigue de-velopment in elite soccer in a hot environment: a multi-experimentalapproach. Scand J Med Sci Sports. 2010;20(suppl 3):125–32.
28. Rampinini E, Impellizzeri FM, Castagna C, et al. Effect of match-related fatigue on short-passing ability in young soccer players.Med Sci Sports Exerc. 2008;40(5):934–42.
29. Randers MB, Jensen JM, Bangsbo J, Krustrup P. Match Perfor-mance and Yo-Yo IR2 Test Performance of Players from Suc-cessful and Unsuccessful Professional Soccer Teams. Science andSoccer VI. Routedge, Oxon, UK; 2009. p. 147–8.
30. Reilly T, Thomas V. Estimated energy expenditures of profes-sional association footballers. Ergonomics. 1979;22:541–8.
31. Rohde E, Espersen T. Work intensity during soccer training andmatch-play. In: Lees TA, Davids K, Murphy WJ, editors. Scienceand Football. London: E & FN Spon; 1988. p. 68–75.
32. Rostgaard T, Iaia FM, Simonsen DS, Bangsbo J. A test to evaluatethe physical impact on technical performance in soccer. J StrengthCond Res. 2008;22(1):283–92.
33. Schertzer JD, Green HJ, Fowles JR, et al. Effects of prolongedexercise and recovery on sarcoplasmic reticulum Ca2+ cycling prop-erties in rat muscle homogenates. Acta Physiol Scand. 2004;180:195–208.
34. Schumann G, Bonora R, Ceriotti F, et al. IFCC primary referenceprocedures for the measurement of catalytic activity concentrationsof enzymes at 37 degrees C. Part 2. Reference procedure for themeasurement of catalytic concentration of creatine kinase. ClinChem Lab Med. 2002;40:635–42.
35. Smaros G. Energy usage during a football match. In: Vecchiet L,editor. Proceedingsofthe1stInternationalCongressonSportsMedicineAppliedtoFootball. Rome, Italy: D. Guanello; 1980. p.795–801.
36. Stuart GR, Hopkins WG, Cook C, Cairnes SP. Multiple effects ofcaffeine on simulated high-intensity team-sport performance. MedSci Sports Exerc. 2005;37(11):1998–2005.
37. Thatcher R, Batterham AM. Development and validation of asport-specific exercise protocol for elite youth soccer players. JSports Med Phys Fitness. 2004;44:15–22.
38. Thompson D, Nicholas CW, Williams C. Muscular soreness fol-lowing prolonged intermittent high-intensity shuttle running. JSports Sci. 1999;17:387–95.
39. Thorlund JB, Aagaard P, Madsen K. Rapid muscle force capacitychanges after soccer match play. Int J Sports Med. 2009;30:273–8.
THE COPENHAGEN SOCCER TEST Medicine & Science in Sports & Exercised 1603
APPLIED
SCIEN
CES
Copyright © 2012 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.





























