Embed Size (px)
Citation preview

Psychology of Women Quarterly, 18 (1994), 509-537. Printed in the United States of America.
THE GLOBAL HEALTH BURDEN OF RAPE
Mary P. Koss University of Arizona
Lori Heise Pacific Institute far Women's Heafth, Western Consortium for Public Health, Washington, DC
Nancy Felipe Russo Arizona State University
Women's rights to be free from male violence are now recognized by the United Nations as fundamental human rights. Two parallel transfor- mations in the understanding of rape have been central to the interna- tional effort to achieve this declaration. The first i s increased recognition of the extent to which rape typically involves intimates. The second is the shift from regarding rape as a criminal justice matter towards an appreciation of its implications for women's health. The focus of this paper i s the health burden of rape, which is addressed from the global perspective and includes discussion of its prevalence and psychological, sociocultural, somatic, and reproductive health consequences. Quantita- tive efforts to capture the relative economic impact of rape compared to other threats to women's health are also discussed. The paper concludes with an agenda for future research on rape that could enrich activists' efforts on behalf of women's health and development.
Almost everywhere in the world, the popular mythology surrounding rape is the same. Rape is perceived as a rare event, perpetrated by unknown assailants who are either unbalanced or who lose control of themselves in
The first author gratefully acknowledges support for the preparation of this article from a Research Scientist Career Development Award from the National Institute of Mental Health and supplemental funds from the Office of Research on Women's Health of the National Institute of Health.
Address correspondence and reprint requests to: Mary P. Koss, Department of Family and Community Medicine, University of Arizona, 2223 E. Speedway Blvd., Tucson, AZ 85719.
Published by Cambridge University Press 0361-6843104 $5.00 + .OO 509

510 KOSS ET AL.
the face of female enticement. Over the past two decades, feminist schol- ars and activists have challenged this perception using research and wom- en’s experience to replace myth. The result has been a transformation in our understanding of the notion of rape. Research has helped reveal the alarming frequency of sexual coercion in women’s lives and the various guises in which rape occurs. Research has likewise debunked the public’s preoccupation with “stranger danger” by documenting the frequency of rape by acquaintances, intimates, and spouses. Feminist legal scholars have in turn won many changes in how rape is treated in law. Legal reforms have altered the very acts that are defined as rape, broadening the scope of the crime to include oral and anal penetration and a greater range of perpetrators (Estrich, 1987). They have also sought to shift the burden of proof from the woman to the man, reducing the demand for evidence of physical injury to prove nonconsent. As these changes filter into the culture at large, women increasingly realize the applicability of the term rape to incidents that they have experienced.
Feminist scholarship has also helped transform rape from merely a so- cial or criminal justice issue to an issue of health and human rights (Bunch, 1991). Recent work conceptualizes rape as a violation of women’s bodily integrity and therefore an abuse of their fundamental human rights. Other work has successfully reframed rape as a woman’s health issue with long-term consequences for women’s physical, psychological, and social health. Rape is now recognized as a risk factor for a range of diseases and reproductive health consequences. These consequences play a predominant role in determining women’s quality of life. Today it is widely believed that multiple forms of men’s violence against women have common roots and ultimately have to be understood as interrelated dimen- sions of women’s experience ( KOSS, Goodman, Browne, Fitzgerald, Keita, & RUSSO, 1994). This perspective is reflected in the United Nations (UN) recent “Declaration of the Eradication of Violence against Women,” which characterizes rape as one of many forms of gender-based abuse (UN Resolution 48/104, December, 1993). According to this declaration, violence against women includes, “Any act of gender-based violence that results in, or is likely to result in, physical, sexual, or psychological harm or suffering to women, including threats of such acts, coercion, or arbi- trary deprivations of liberty, whether occurring in public or private life” (Economic and Social Council, 1992, p. 5). The declaration specifically lists marital rape, sexual abuse of female children, sexual harassment, trafficking in women, forced prostitution, and violence perpetrated by the State among the many acts explicitly covered by the definition.
Although it is artificial to separate the forms of male-perpetrated vio- lence that women cumulatively encounter across their lifespans, it is some- times necessary. To give adequate consideration to existing scholarship within space limitations, we reluctantly limit the focus of this paper to rape of adolescent and adult women globally. We have tried to avoid

Health Burden of Rape 511
reiterating conclusions based on U.S. research that are available in reviews published elsewhere (see Foa, Rothbaum, & Steketee, 1993; Koss et al., 1994; KOSS, 1993; Resick, 1993). In addition to duplication, reliance on research findings from the United States risks inappropriate generalization to a global context. Instead, we have tried to emphasize the universality of the issues by using documentation from as many different nations as possi- ble. This effort has required us to use information collected under the auspices of nongovernmental organizations that often lack the resources and training in methodology characteristic of academic researchers. The critical reader will notice multiple instances where documentation is sparse or weak. Each of these instances should be viewed as an idea for future research. We sincerely hope that this article will stimulate interest in the study of the health effects of rape beyond the boundaries of the United States.
RAPE IN SOCIOCULTURAL CONTEXT
The defining characteristic of rape is lack of choice or consent by the woman to engage in sexual intercourse (Minturn, Grosse, & Haider, 1969; RozCe, 1993; Sanday, 1981). RozCe ( 1993) prefers the word choice to the word consent, because it avoids implicit acceptance of a male prerogative to initiate sexual intercourse. This prerogative is evident in most North American jurisdictions where rape is defined as penetration (oral, anal, or vaginal), against consent, through force, threat of bodily harm, or when the woman is unable to consent (Searles & Berger, 1987).
The critical role that sociocultural supports play in defining and pro- moting rape as well as shaping its consequences is reflected in the categori- zation of rape into two major types: normative and non-normative ( Roz&, 1993). These distinctions mirror Heise’s (1993a) conceptual dis- tinction between tolerated and transgressive rape. Whatever rape’s form every society has mechanisms that “legitimize, obfuscate, deny, and thereby perpetuate violence” (Heise, Pitanguy, & Germain, 1993, p. 1; also see LaFree, 1989). These social processes prompted one feminist legal scholar to write that, “Rape, from a woman’s point of view, is not prohib- ited, it is regulated’ (MacKinnon, 1983, p. 651).
Non-normative Rape
Rape that is non-normative is defined as, “illicit, uncondoned genital con- tact that is both against the will of the woman and in violation of social norms for expected behavior” (RozCe, 1993, p. 504). This definition de- picts the stereotypical rape that consists of a surprise attack on a virtuous woman. In fact, the wrongness of rape is often determined not by the nature of the act committed but by the marital or moral status of the

512 KOSS ET AL.
woman. Cultural responses to rape reflect the attitude that only women of good character deserve protection from rape. This notion is codified in certain Latin American countries - including Costa Rica, Ecuador, and Guatemala- whose laws recognize rape of only honest and chaste women (Heise et al., 1993). The distinction between types of women may also be implied. In Pakistan, courts have ruled that testimony of women of easy virtue has less weight. To assess a woman’s virtue, that court uses, among other things, a finger test to see if her vagina accommodates two fingers easily. If so, sex is said to be habitual, and a woman’s testimony loses weight (Jahangi & Jalani, 1990). In Sri Lanka, class and caste are addi- tional considerations. Thus, virgins under 18 years of age who are raped by a man of lesser class or caste are assured of a conviction. “But if you are an independent lower class woman, of middle age, raped by an acquain- tance, then it is better that you nurse your wounds at home” (Coomaras- wamy, 1992, p. 51).
Such attitudes hearken back to the days when rape was first conceived of as a crime. For the first few thousand years in the development of Western civilization, the crime of rape appears to have consisted of defile- ment of a virgin. The legal recourse was to demand that the perpetrator compensate the girl’s father for her lost value in the marriage market (Brownmiller, 1975). Still in Peru, the penalty for rape decreases as the victim gets older and drops to virtually no punishment for raping a mature woman (Human Rights Watch, 1992a). In Guatemala, Peru, and Chile, the law specifically exonerates a man who rapes a minor if he agrees to marry her and thus legitimizes the union (Heise et al., 1993). In the United States as well, criminal justice officials often fail to prosecute cases that fall outside their stereotypical notions of real rape, which in general involve a stranger brutally raping a respectable woman (Estrich, 1987). Women who are sexually experienced, have been drinking, or who other- wise violate traditional gender norms find the justice system very reluctant to address their rapes.
Pakistan, however, earns the dubious distinction of having the legal system most biased against the victim. As part of a fundamentalist wave of reform in 1979, Pakistan passed the Zina Ordinance, which made all forms of sex outside of marriage - including rape, fornication, and adul- tery- crimes against the state. A new law of evidence also made women’s testimony worth only half that of a man’s, making it even more difficult for rape victims to prove their cases. Women who fail to meet Pakistan’s high standard of proof for rape can be thrown in jail for adultery or fornication based on their own admission of intercourse. Others who be- come pregnant due to unreported rapes have likewise been charged, the pregnancy itself serving as evidence of illicit sex. Human rights activists estimate that upwards of 1,500 Pakistani women are in prison awaiting trial for zina (Human Rights Watch, 1992b).
Health Burden of Rape
Normative Rape
513
Normative rape is defined as, “ , . . genital contacts that the female does not choose, but that are supported by social norms” (Rozke, 1993, p. 503). It can be said that there are sociocultural supports for rape when, “ . . . there is no punishment of the male or the female only is punished; if the rape itself is condoned as a punishment of the female; if the genital contact is embedded in a cultural ritual such as an initiation ceremony; or when re- fusal is disapproved or punished by the community” ( RozBe, 1993, p. 503).
The naming of forced genital contact by intimates, particularly spouses, as rape is a revo- lutionary transformation of the concept. Rapes in which the parties are friends, romantic partners, or spouses are still unlikely to be treated the same as rapes by total strangers, even in settings where the law makes no distinctions among rapes according to relationships. Women are least likely to have legal protection from marital rape. Outside North America there is no widely accepted legal concept of marital rape; only last year did the United Kingdom move to outlaw it (Human Rights Watch, 1992a).
But many women worldwide are beginning to question the traditional notion that marriage represents tacit agreement to provide sexual services to the husband upon demand (Russell, 1990). For example, Indian re- searcher Annie George (1993) speculates whether the notion of consent by virtue of marriage has any validity among lower caste Indian women who are married off at a very young age, have no say in whom they will marry, and have been given virtually no information about sex prior to their wedding night. Algerian gynecologist, Malika Ben Baraka ( 1993) likewise observes that the consummation of marriage itself can constitute rape in her country, where very young girls are physically restrained and forced to submit to intercourse on their wedding night without any prior instruc- tion in sexuality. The trauma of defloration can be even more excruciating in those countries where young girls are infibulated to preserve their vir- ginity until marriage. Not infrequently, infibulated women must be cut open on their wedding nights so that intercourse can occur (Toubia, 1993).
Punitive rape is a category of normative rape that in- volves “any genital contact that is used in a disciplinary or punitive man- ner . . . occurs generally as a masculine response to women behaving in a way that is considered solely the prerogative of males . . . ” (Rozk, 1993, pp. 507-508). In Latin America, for example, feminists contend that the aim of rape is to change women from “Madonna to whore” and to warn them that they must retreat to their traditional sphere (Bunster, 1986, p. 307; quoted in Lykes, Brabeck, Ferns, & Radan, 1993, p. 535). Rape as punishment often involves the violation of one woman by a series of men.
Acquaintance rape including date and marital rape.
Punitive rape.

514 KOSS ET AL.
Rape as a mechanism of intentional social control of women leaders has been documented in Peru and in India (Human Rights Watch, 1992a; Mathur, 1992). In Rajasthan, India, for example, a woman leader of the highly successful Women’s Development Programme was gang raped by male community members because they disapproved of her organizing effort against child marriage. The woman was raped in front of her hus- band, who was warned, “Keep your wife in line or we’ll rape her again.”
Another form of punitive rape is sexual torture of women by state secu- rity forces in their villages or while in detention (Blatt, 1992; Lunde & Ortmann, 1990). Sexual torture is a form of psychological manipulation that has the aim of depriving “the victim of his or her identity” (Agger, 1989, p. 307). Amnesty International (1992) describes the ill-treatment of women in detention and documents hundreds of women worldwide who have been victims of state-sanctioned rapes. Human Rights Watch (1992a, 1992b) has recorded state-tolerated rape of women in detention both in Peru and Pakistan.
Throughout history, rape has co-occurred with warfare and has involved the capture of women as slaves, prostitutes, concubines, and raiding for wives (Brownmiller, 1975; RozBe, 1993). In January, 1993, the United Nations Commission on Human Rights passed a resolution that for the first time identified rape as a war crime (United Nations, 1993). Rape in war is designed to destroy the bonds of family and society and demoralize the enemy. Where there is ethnic conflict, rape is used to accomplish goals of both war and nationalism (Asia Watch, 1992; United Nations, 1993). Documented incidents of rape during wartime include:
Rape as a weapon of war.
1. Massive raping of women during recent conflicts in Liberia, Uganda, Peru, Cambodia, Somalia, and Bosnia (Goldfeld, Mollica, Pesavento, & Farone, 1988; Human Rights Watch, 1993a, 1993b; Swiss & Giller, 1993).
2. An international team sent by the UN to investigate the former Yugoslavia in January 1993 estimated rapes on the basis of data on abortions, deliveries, pregnancies known to be due to rape, and sexually transmitted diseases. During their short 10-day mission, they documented 119 pregnancies at six hospitals in Bosnia, Croatia, and Serbia. Using estimates of a single act of intercourse resulting in pregnancy 1 to 4 % of the time, they estimated that the 119 pregnancies alone represented 11,900 rapes (Swiss & Giller, 1993; United Nations, 1993). The use of rape appeared to be part of an “ethnic- cleansing strategy” because it was used with the expressed intent to impreg- nate (Thomas, 1993).
3. In Bangladesh, estimates are that the 9-month war for independence in 1971 resulted in the rape of between 250,000-400,000 women and led to an esti- mated 25,000 pregnancies according to International Planned Parenthood (attributed to Brownmiller, 1975; cited in Swiss & Giller, 1993).
4. The Japanese government recently acknowledged that during World War 11, it forcibly conscripted 100,000-200,000 women (mostly Korean) into sexual
Health Burden of Rape 515 slavery to serve as “comfort women” for the Japanese Army (Hearings before the United Nations Secretary-General, February 25, 1992, cited in Swiss & Giller, 1993).
5. Recent reports indicate that Burmese government agents have been raping Muslim women to get them to move out of contested areas and over the border into Bangladesh (Human Rights Watch, 1993~).
6. Among women who lived in Cambodia under the Pol Pot reign who later immigrated to the United States and sought treatment for trauma, at least 53% had been raped or sexually assaulted in addition to other heinous tor- tures (Van Boemel & RozBe, 1992). Other practitioners working with this group have reported rates of rape as high as 95 % (Mollica, 1986).
Other forms of normative rape in- clude exchange rape, ceremonial rape, and status rape. “Exchange rape” involves the “male use of female genital contact as a bargaining tool, gesture of solidarity, or conciliation” ( RozBe, 1993, p. 507). Wyatt ( 1993) has suggested that the world community must address a form of exchange rape that she calls “survival rape.” Here, young women living under eco- nomic deprivation involve themselves with older men to obtain goods or services that they need for survival. “Ceremonial rape” is a category of unchosen genital contact that occurs within the context of ceremonies including defloration rituals or virginity tests, where sexual intercourse is part of the ceremony and females are expected to participate whether they want to or not (Rozke, 1993). “Status rape” occurs because of acknowl- edged differences in rank including master and slave, chief and clans- woman, nobleman and commoner, or priest and parishioner (RozBe, 1993). Recent examples of status rapes include the treatment of Asian maids in Kuwait, where cultural expectations dictate that domestic ser- vants be sexually available for their employers (Human Rights Watch, 1992~).
Other forms of normative rape.
THE PREVALENCE OF RAPE WORLDWIDE
Accurate estimates of the global health burden of sexual victimization are hampered by lack of data on the incidence and prevalence of rape in its various forms. Unfortunately, conclusions drawn from crime statistics are virtually useless for estimating the incidence of sexual assault because women are universally reluctant to report rape to authorities. Thus, com- munity-based surveys reveal that less than 2% of rape victims informed the police in Korea (Shim, 1992) and 12% did so in the United States (National Victims Center, 1992). Crime statistics are also of limited utility in estimating the health burden of rape because they generally reflect only those rapes that occurred within the previous year, whereas the afteref- fects of rape may extend for many years beyond the incident or series of incidences.
Measurement of rape prevalence faces a central methodological chal-

516 KOSS ET AL.
lenge- to overcome women’s historic tendency to keep silent about rape. In addition, other compelling social forces complicate the collection of valid and reliable data, including: norms about discussing sexual matters, distrust of authorities, distrust of fellow citizens under conditions of social stress, and difficulty creating privacy and confidentiality in small, close- knit societies. Currently, there exists a small database on the prevalence of rape, most of which was developed in the United States. Koss (1993) recently reviewed and critiqued these studies. She concluded that esti- mates of rape or sexual assault prevalence among adult women range between 14% and 25% in the majority of sources. The major problem identified in this literature is that lack of comparability across studies in definitions and methodologies has precluded the accumulation of a cohe- sive database.
To begin constructing a global database on rape prevalence, we will review information drawn from three main sources: ethnographic records collected and catalogued by anthropologists, international crime survey data, and cross-national studies of rape prevalence among college-aged women.
Ethnographic Studies
Rape is found in 42% to 90% of nonindustrial societies, depending on how it is defined and on the cultural and geographic representativeness of sample of societies examined (Bart, Blumberg, Tombs, & Behan, 1975; Broude & Green, 1976; Levinson, 1989; Minturn et al., 1969; Sanday, 1981). Note that these figures refer to the proportion of societies in which rape occurs at some level, not to the magnitude of rape within any one society. Thus, Minturn and associates defined rapes as “sexual relations without the consent of the woman involved” (p. 303) and reported its occurrence in 90% of the societies studied. Sanday (1981) coded 156 world societies on the basis of a similar definition. She included as rape unchosen sexual intercourse that occurred in the context of ceremonies and as part of warfare, but she excluded “sleepcrawling” (that is, surreptitious sex with a woman who is asleep in the same room as the remainder of her family; RozBe, 1993, p. 509). Sanday reported rape in 53 % of her sample of nonindustrial societies, partly because she classified as rape-free those societies where rape did occur but was extremely rare. Roz6e (1993) like- wise defined rape as lack of female choice and examined a sample of 35 nonindustrial societies. One or more forms of rape were found in all of the 35 societies she examined. Nearly all of the societies (97 % ) had normative rape, that is, structured ways of sexually abusing women that did not violate social norms, including marital rape (40% of societies), exchange rape (71 % ), punitive rape ( 14 % ), theft rape (63 % ) , ceremonial rape (49 % ), and status rape (29 % ). Non-normative rape was found in 63 % of the societies studied.

Health Burden of Rape 517
It would be incorrect to conclude on the basis of these studies that the ethnographic record documents a universal male predilection, perhaps biologically based, to rape women (Sanday, 1993). Rather, the data force the conclusions that rape takes multiple forms depending on the sociocul- tural context, and that in some societies, rape is far less common than in others. These societies warrant study so that the rest of the world may learn from them. Knowledge that can be gained from examination of relatively rape-free societies include how social organizations and customs minimize rape and how to socialize boys so that they learn to control aggressive tendencies and behave in nonaggressive ways (Miedzian, 1993; Sanday, 1993).
international Crime Survey Data
A question about sexual victimization was included in the International Crime Survey (van Dijk & Mayhew, 1993). The text of the question was the following, “Firstly, a rather personal question. People sometimes grab, touch or assault others for sexual reasons in a really offensive way. This can happen either inside one’s house or elsewhere, for instance in a pub, the street, at school, on public transport, in cinemas, on the beach, or at one’s work place. Over the past five years has anyone done this to you?” (van Dijk & Mayhew, 1993, p. 21). The results revealed that among industrial countries included in the sample, Australia ranked number one in affirmative responses (5.6% ), Canada second (4.1% ), and the United States third (3.7% ). Data from nonindustrial nations are not yet publicly available.
Given the extensive sample included in the International Crime Survey and the expense of data collection, it is very unfortunate that the screening for sexual assault is both minimal and ambiguous. Although disaggregated figures are presented in the report for rape and molestation, this distinc- tion cannot be made on the basis of the screening item alone, and the authors do not discuss their follow-up questioning. Use of a global screen- ing item for all forms of sexual assault from which cases of rape can later be culled by further questioning has been shown in the United States to result in serious underestimation of rape (Koss, 1993). More successful in obtaining disclosure of rape are multiple, behaviorally specific, culturally sensitive questions to jog respondents’ recollection about the variety of guises in which rape may appear. A further problem with the approach toward rape in this survey is the unfortunate wording of the screening item. The use of the expression “in a really offensive way” describes an appropriate reaction to sexual crimes such as unwanted groping, pinching, or rubbing up against the victim. It clearly understates the typical reaction to rape. Coming as it does after questions about crimes such as pickpocket- ing, the item intended to identify the range of sexual assaults may instead
518 KOSS ET AL.
favor recall of minor public molestations. Also suggestive of problems with the rape item are the ratings of severity that respondents ascribed to the sexual assault item. From country to country they varied greatly: some societies considered that the item described a serious violation, whereas others considered it a minor one. If the international crime survey screen- ing for rape referred unambiguously to forcible rape, it would be difficult to find a society that considered the violation minor.
Cross-national Studies of College Students
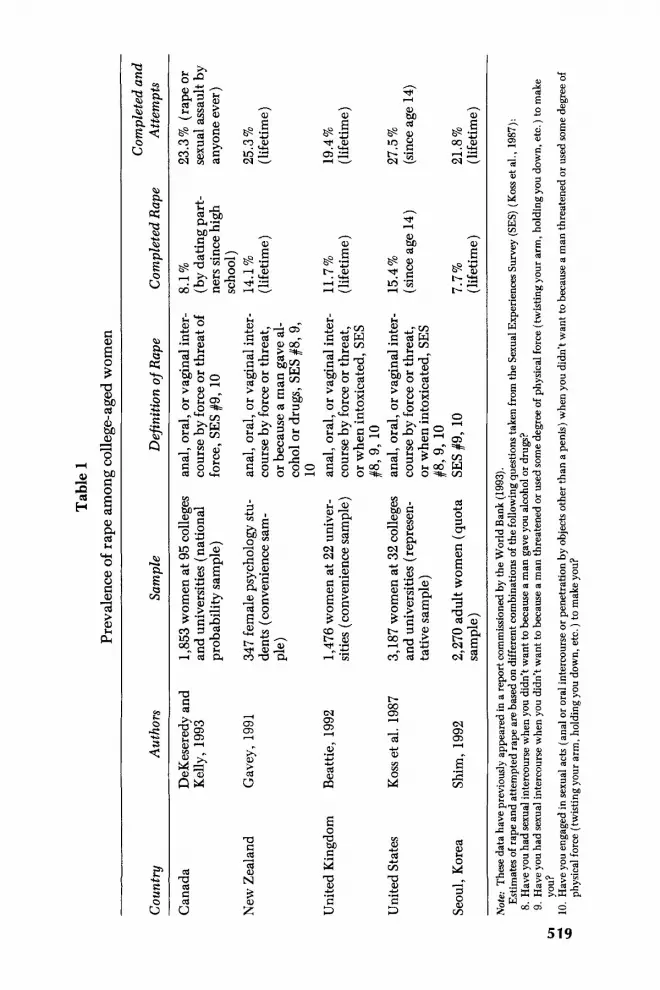
More or less directly comparable cross-national figures on rape prevalence come from a small number of studies that have administered the Sexual Experiences Survey (Koss, Gidycz, & Wisniewski, 1987) to college stu- dents in several countries. This survey consists of 10 items to screen for a continuum of unwanted sexual behavior, including three items designed to measure rape as it is defined in most North American jurisdictions. Administrations of the survey to students in Canada, New Zealand, United Kingdom, United States, and Korea are summarized in Table 1. Individ- ual authors have assembled their rape prevalence figures differently, de- pending on whether they wished to include or exclude unwanted sex while intoxicated as rape (item 8). In addition to differences in definition, other sources of variation include the researcher’s choice of the age at which recall is to begin and whether focus is on all experiences or is limited to those incidents involving dating partners. Even with these sources of varia- tion in mind, however, the data point to an impressive consistency in prevalence of rape among college students cross-nationally. Lifetime prev- alence of completed and attempted rape combined among college women is universally above 20 % .
Also consistent are cross-national findings on the typical victims and perpetrators of rape. Table 2 contains figures from selected cities and countries that point to a sad global reality. The majority of perpetrators are people known to the victim, and a substantial subset of victims are very young girls. Across diverse continents and hemispheres, between one and two thirds of the victims are 15 years and younger.
High-risk groups.
THE EFFECTS OF RAPE
The effects of rape include psychological distress, sociocultural impacts, and somatic consequences. A large body of empirical literature exists to document these effects. (For reviews of psychological effects see Good- man, KOSS, & RUSSO, 1993a, 1993b; Hanson, 1990; Lurigio & Resick, 1990; McCann, Sakheim, & Abrahamson, 1988; Resick, 1987, 1990; Roth & Lebowitz, 1988. For reviews of somatic effects see Council on Scientific
Tab
le 1
Pr
eval
ence
of
rape
am
ong
coll
ege-
aged
wom
en
Cou
ntry
A
utho
rs
Sam
ple
Com
plet
ed a
nd
Def
initi
on o
f R
ape
Com
plet
ed R
ape
Atte
mpt
s
Can
ada
New
Zea
land
Uni
ted
Kin
gdom
Uni
ted
Stat
es
Seou
l, K
orea
DeK
eser
edy
and
Kel
ly, 1
993
Gav
ey, 1
991
Bea
ttie,
199
2
Kos
s et a
l. 19
87
Shim
, 199
2
1,85
3 wom
en a
t 95
colle
ges
and
univ
ersi
ties (
nati
onal
pr
obab
ility
sam
ple)
347
fem
ale
psyc
holo
gy st
u-
dent
s (c
onve
nien
ce sa
m-
ple)
1,47
6 w
omen
at 2
2 un
iver
- si
ties (
conv
enie
nce
sam
ple)
3,18
7 w
omen
at 3
2 co
llege
s an
d un
iver
sitie
s (re
pres
en-
tativ
e sa
mpl
e)
2,27
0 ad
ult w
omen
(qu
ota
sam
ple)
anal
, ora
l, or
vag
inal
inte
r-
cour
se b
y fo
rce
or th
reat
of
forc
e, S
ES #
9, 1
0
anal
, ora
l, or
vag
inal
inte
r-
cour
se b
y fo
rce
or th
reat
, or
bec
ause
a m
an g
ave
al-
coho
l or
drug
s, S
ES #
8,9,
10
an
al, o
ral,
or v
agin
al in
ter-
co
urse
by
forc
e or
thre
at,
or w
hen
into
xica
ted,
SES
#8
,9, 1
0 an
al, o
ral,
or v
agin
al in
ter-
co
urse
by
forc
e or
thre
at,
or w
hen
into
xica
ted,
SES
#&
9, 10
SE
S #9
, 10
8.1 %
(b
y da
ting
par
t-
ners
sinc
e hi
gh
scho
ol)
14.1
%
(lif
etim
e)
11.7
%
(lif
etim
e)
15.4
%
(sin
ce a
ge 1
4)
7.7%
(l
ifet
ime)
23.3
% (
rape
or
sexu
al a
ssau
lt by
an
yone
eve
r)
25.3
%
(lif
etim
e)
19.4
%
(lif
etim
e)
27.5
%
(sin
ce ag
e 14
)
21.8
%
(lif
etim
e)
Not
e: Th
ese d
ata
have
pre
viou
sly
appe
ared
in a
repo
rt c
omm
issi
oned
by
the
Wor
ld B
ank
(199
3).
Est
imat
es of
rap
e an
d at
tem
pted
rap
e ar
e ba
sed
on d
iffe
rent
com
bina
tions
of t
he fo
llow
ing q
uest
ions
take
n fr
om th
e Se
xual
Exp
erie
nces
Sur
vey
(SES
) (Koss et
al.,
198
7):
8. H
ave
you
had
sexu
al in
terc
ours
e whe
n yo
u di
dn’t
wan
t to
beca
use
a m
an g
ave y
ou a
lcoh
ol or
dru
gs?
9. H
ave
you
had
sexu
al in
terc
ours
e whe
n yo
u di
dn’t
wan
t to
beca
use a
man
thre
aten
ed o
r use
d so
me d
egre
e of
phy
sica
l for
ce (t
wis
ting y
our a
rm, h
oldi
ng y
ou d
own,
etc
. ) to
mak
e
10. H
ave
you
enga
ged
in s
exua
l act
s (a
nal o
r ora
l int
erco
urse
or p
enet
ratio
n by
obj
ects
oth
er th
an a
pen
is) w
hen
you
didn
’t w
ant t
o be
caus
e a m
an th
reat
ened
or u
sed
som
e deg
ree o
f Gl
you?
3;
phys
ical
forc
e (tw
istin
g you
r arm
, hol
ding
you
dow
n, e
tc. )
to m
ake y
ou?

520 KOSS ET AL.
Table 2 Statistics on sexual crimes, selected countries a
Percent of Percent of
City or country to victim 15 years and under and under perpetrators known Percent of victims victims 10 years
Lima, Peru 60 - 18'
Mexico City 67 36 23
Papua New Guinea - 47 13d Santiago, Chilee 72 58 32' United States 78 62 29
Malaysia 68 58 1Sb
Panama City 63 40 -
Note: Data are from the following sources: Malaysia data (Consumer's Association, 1988); Mexico City data (COVAC, 1990 & Carpeta Basica, 1991. Mexico City: Procurador de Justicia del Distrito Federal de Mexico); Panama City data (Perez, 1990); Peru data (Portugal, 1988); Papua New Guinea data (Riley, 1985, as cited in Bradley, 1990); Chile data (Avendano & Vergara, 1992); United States data (National Victims Center, 1992). These data have appeared previously in a report commissioned by the World Bank (1993). "Studies include rape and sexual assaults such as attempted rape and molestation except for U.S. data which includes only completed rapes. bPercentage of survivors age 6 and younger. 'Percentage of survivors age 9 and younger. dPercentage of survivors age 7 and younger. 'Based on 5-year averages derived from crimes reported to the Legal Medical Service, 1987-1991; Anuario Estadistico del Servicio Medico Legal de Chile. 'Percentage of survivors age 17 and younger.
Affairs, 1992; Dunn & Gilchrist, 1993; Hendricks-Mathews, 1993; Koss & Heslet, 1992.) However, most of the studies are based on Western women in peacetime, many of whom may have experienced a single episode of rape (Swiss & Giller, 1993). Studies generally have not taken into account the cumulative impact of multiple traumas as commonly experienced by women in war and conflict situations, including death of loved ones, loss of home and community, dislocation, untreated illness, deprivation, and war-related injury (for exceptions see Bowen, Carscadden, Beighle, & Fleming, 1992; Friedman, 1992; Mollica & Son, 1989; Mollica, Wyshak, & Lavelle, 1987; RozCe & Van Boemel, 1989; Sheperd, 1992; Van Boemel & RozCe, 1992).
Psychological Distress
Given the nature of rape, it is not surprising that some symptoms are experienced by almost everyone in the immediate aftermath. However, approximately one quarter of women continue to experience negative ef- fects several years after rape (Hanson, 1990). Even when evaluated many years after sexual assault, survivors in the United States and New Zealand were more likely to have received several psychiatric diagnoses during their adult life, including major depression, alcohol abuse/dependence, drug abuse/dependence, generalized anxiety, obsessive-compulsive disor-

Health Burden of Rape 521
der, and post-traumatic stress disorder (Burnam et al. , 1988; Kilpatrick, Saunders, Veronen, Best, & Von, 1987; Winfield, George, Schwartz, & Blazer, 1990; Mullen, Romans-Clarkson, Walton, & Herbison, 1988). These effects may be more severe for younger victims. For example, Bur- nam et al. (1988) found that those who were sexually abused as children were more likely (59% vs. 24%) than those not abused to have at least one psychiatric diagnosis. Rape and other sexual abuse in childhood also creates a legacy of increased vulnerability to revictimization. Thus, child abuse victims are 2.4 times more likely to be raped as adults (Wyatt, Guthrie, & Notgrass, 1992).
Many of the psychological effects of rape - including intrusive memo- ries, attempts to avoid reminders of the trauma, depression, and anxiety- are conceptualized as post-traumatic stress disorder (PTSD ) in North America (American Psychiatric Association, 1994). Most rape victims who are evaluated at a trauma center in the immediate aftermath of rape meet symptom criteria for PTSD. For example, an average of 12 days following assault, 94 % of rape victims met PTSD symptom criteria; 46% still met the criteria 3 months later (Rothbaum, Foa, Riggs, Murdock, & Walsh, 1992). Rape is more likely to induce PTSD than a range of traumatic events affecting civilians, including robbery, tragic death of a close friend or family member, or natural disaster (Norris, 1992).
However, the PTSD conceptualization has been severely critiqued, espe- cially by Latin-American feminist psychologists (Becker, Lira, Castillo, Ganez, & Kovalskys, 1990; Marth-Barb, 1988; RozCe & Van Boemel, 1989). Critics see the PTSD diagnosis as a conceptualization rooted in the medical model that ignores the gendered, structural, and social aspects of male violence against women. It also deflects attention from traumatized social relations and social systems by overemphasizing individual responses to male violence. These comments are well founded because none of the current models of PTSD address characteristics of the victim that may shape her response to rape, including ethnicity, class, and sexual orienta- tion. Nor do they address the fact that the cultural context that spawned the violence may itself present an obstacle to recovery (Goodman, Koss, & RUSSO, 1993a, 1993b).
Promising to ameliorate some of the shortcomings in conceptual models of PTSD are new developments linking specific aspects of the environment with emotions ( Lazarus, 1991). In this conceptualization a person’s emo- tional response to an event is neither determined by the actual event nor by intrapsychic processes, but rather by a cognitive appraisal of the experi- ence that arises out of a person-event interaction (Lazarus, 1991). Cogni- tive appraisals are substantially influenced by both individual and socio- cultural variables including family history, existence of prior trauma, personality, coping style, ethnicity, class, sexual orientation, community attitudes, and gender-based norms. The notion of cognitive appraisal sug-

522 KOSS ET AL.
gests that understanding psychological responses to rape requires looking at both the trauma and the recovery process from the woman’s point of view - in the context of her personal meanings.
Sociocultural I rn pacts
One rape can affect many women when it leads nonvictimized women to change their behavior and to restrict their movements to avoid being raped. A range of findings suggest that women develop distrust of men and live their lives under the threat of sexual violation. For example:
1. Women in Seoul, Korea identified rape as the major stress in their lives (Korean Sexual Violence Relief Center, 1991). A second survey of over 2,000 women found that 40% felt “extremely uneasy” about sexual violence and restricted their activities because of these fears (Shim, 1992).
2. In Ethiopia, women refugees reduced the number of cooked meals they fed their children because they feared being raped while collecting firewood (Lapin, 1992).
3. Female health workers in Gujurat, India report being reluctant to travel alone between villages for fear of being raped (Khanna, 1992, cited in Heise et al., 1993).
4. In a national telephone survey of 12,300 Canadian women conducted by Statistics Canada, 60% of women reported that they feared walking alone after dark, 81% feared using public transportation after dark, and 83% feared walking alone to their cars in a parking garage. Women who actually had been victims of violence were only slightly more likely to be fearful than women who had never been personally affected by violence (The DaiZy Statistics Canada, November 18,1993, pp. 8-9).
5. For urban U.S. women younger than 35, rape is feared even more than murder (Warr, 1985). In response to their fear about rape, over half of the women surveyed reacted with self-isolation, forgoing certain activities such as evening entertainment. In contrast, most men (90% ) living in some neigh- borhoods denied taking steps to reduce their vulnerability to crime, even though statistics suggest that they are more likely to be victims of every violent crime with the exception of rape (Gordon & Riger, 1989).
More dire social effects of rape occur in societies where the stigma of rape is pronounced. In parts of Asia and the Middle East, for example, these include being divorced by one’s husband, being ostracized by one’s family, and even being killed by family members to cleanse the family honor (Ben Baraka, 1993). In Cambodian culture women are likened to cotton. “Once cotton has fallen in the soil, it can never be washed com- pletely clean” (Van Boemel 81 RozBe, 1992, p. 239; taken from Mollica, 1986). In contrast, men are likened to diamonds, which can be washed if soiled. Whereas monks perform purification rituals for men, none are available for women who have been raped. These women must carry their sense of impurity for the remainder of their lives (Mollica, 1986).

Health Burden of Rape 523
Somatic Effects
The somatic effects of rape can include injuries such as suicide and homi- cide, chronic illness, and range of reproductive health consequences.
Rape is associated with physical injury caused by the perpetrator (Beebe, 1991; KOSS, Wood- ruff, & KOSS, 1991; National Victims Center, 1992). But in societies where victim-blaming is strong and the stain of sexual violation is considered permanent, rape also can become a significant risk factor for both suicide and murder. Although the majority of honor killings are against women suspected of adultery or fornication, one study of 72 honor murders among Arab Israelis notes that 5 were against women who had been raped (Kres- sel, 1981). Likewise, in a study of women murdered in Alexandria, Egypt, 47 % were victims of rape who had been killed by a relative (Graitcer 81 Youssef, 1993). Some cultures place so much emphasis on virginity that the greatest preoccupation of victims in the aftermath of rape is seeking surgical reconstruction of their hymen. According to Eman Kandaloof, Palestinian Outreach Coordinator of Israel’s Haifa Rape Crisis Center, “Women tend to fixate on getting their hymens reconstructed instead of dealing with the psychological aftermath of the rape (Kandaloof, 1991).
A number of chronic conditions are diagnosed disproportion- ately among rape victims, including chronic pelvic pain, arthritis, gastro- intestinal disorders, headaches, chronic pain disorders, psychogenic sei- zures, premenstrual symptoms, and substance use (Golding, 1994; Koss & Heslet, 1992). A number of potential mechanisms exist to account for the links between victimization and illness, and somatic symptoms may be multiply determined. Examples of somatic consequences of rape reported in various nations include:
Intentional injuries including suicide and murder.
Illnesses.
1. In Bangladesh 84% of victims suffered injuries or unconsciousness, mental illness, or death following rape (Shamim, 1985).
2. Among Ugandan rape victims, 53% described headaches, chest pain, and rashes, and 57 % described gynecological symptoms including vaginal dis- charge or pelvic pain (Giller, 1992).
3. U.S. women with a history of victimization by rape (and other crimes) report more symptoms of illness across virtually all body systems and perceive their health less favorably than nonvictimized women ( Kimerling & Calhoun, 1994; Koss, Koss, &Woodruff, 1991).
4. Victimized women, compared to those free from male violence, are more likely to report negative health behaviors, including smoking, alcohol use, and failure to use seat belts (Koss, Koss, & Woodruff, 1991).
Reproductive Health Consequences
It is on the battleground of reproductive health that some of the fiercest struggles to realize women’s rights are being waged. In the context of women’s freedom to control their own bodies, “Rape is undoubtedly the

524 KOSS ET AL.
most direct breach of choice that a woman can face” (Heise, 1993a, p. 77). In the material that follows we address not only the direct conse- quences of rape on reproductive health but also the barriers to change in reproductive health behavior posed by women’s fears of rape.
Between 15 and 18 % of rape victims who visited Mexican rape crisis centers reported they became pregnant as a result of rape (CAMVAC, 1985; COVAC, 1990), figures consistent with data from Thailand and Korea ( Archavanitkui & Pramualratana, 1990; Shim, 1992). In the United States, pregnancy results from rape in approximately 5% of the cases (Beebe, 1991; KOSS, Woodruff, & KOSS, 1991). Forced impregnation takes on an additional horror where abortion is illegal, and the victim faces the prospect of bearing the rapist’s child.
Rape also plays a causal role in pregnancy among teenagers (Boyer & Fine, 1992). For example:
Pregnancy.
1. A study conducted in the maternity hospital of Lima, Peru revealed that 90% of young mothers 12-16 years of age delivered a child that resulted from rape (Rosas, 1992). The vast majority were impregnated by their father, stepfather, or other close relative. An organization for adolescent mothers in Costa Rica reported similar findings: 95 % of their clients under age 15 were victims of incest (Treguear & Carro, 1991).
2. In Peru, where abortion is illegal even in the case of rape, a high percentage of abortions are performed on rape victims, many of whom are minors abused by fathers or other family members (Human Rights Watch, 1992a). According to Peru’s Health Ministry, 43 % of all maternal hospitalizations in 1990 were due to botched abortions.
3. In the United States, women survivors of sexual assault in childhood were found to be three times more likely to become pregnant before age 18 com- pared to nonvictimized women (Zierler et al., 1991; also see Wyatt, 1988).
In Barbados, a probability survey of 407 women and men revealed that sexual abuse was the single most powerful predictor of high-risk sexual activity during adolescence for both women and men (Handwerker, 1991). After controlling for SES factors and home environment variables, sexual abuse remained linked to the age at first intercourse and the number of sexual partners. These effects remained significant until respondents reached their mid-30s. In the United States, a background of childhood or adolescent sexual abuse or rape is associated with a range of high-risk sexual behaviors (Boyer & Fine, 1992; Finkelhor, 1987; Paone, Chavkin, Willets, Friedman, & Des Jarlais, 1992; Zierler et al., 1991). For example, abused girls began sex earlier, were more likely to use alcohol and drugs, were less likely to use birth control at first intercourse, and were more likely to be battered or to have traded sex for food, money, shelter, or drugs (Boyer & Fine, 1992). Early sexual abuse raised the risk of entering prostitution (Finkelhor, 1987; Meyerding, 1977). In the United States, the chance of working in prostitution was four
High-risk sexual behaviors.

Health Burden of Rape 525
times greater among those forced to have sex in childhood or adolescence compared to nonabused (Zierler et al., 1991 ) . Among crack cocaine users those sexually abused as children were more likely to engage in sex for drugs transactions (Paone et al., 1992).
In many parts of the world there appears to be a trend for men to seek younger and younger partners based on the belief that this behavior will protect them from exposure to HIV. Among women, sexual experience at very young ages is just as important as multiple sex partners in raising the risk for sexually transmitted diseases. It is well established that women have a much greater chance of being infected per coital act and have particularly vul- nerable reproductive tracts at young ages (Ericksen, 1994). Some exam- ples of the severity of the problem include:
Sexually transmitted disease including AIDS.
1. Ten percent of clients contact STD from rape in Thailand (Archavanitkui & Pramualratana, 1990).
2. In studies in Nigeria and Uganda, 16% of female patients seeking treatment for STDs were under 5 years of age and another 6% were between 6 and 15 years (Kisekka & Otesanya, 1988).
3. Twenty-two percent of female patients attending an STD clinic in Nigeria were under 10 years of age (Sogbetun, Alausa, & Osoba, 1977).
4. Children in Nicaragua identified sexual abuse as the number one health priority facing children in their country (Rompiendo el Silencio, 1992).
In the United States, sexually transmitted diseases occur as a result of rape in 4 to 30 % of victims (Koss & Heslet, 1992). In addition to pain and stigmatization, untreated STDs can lead to pelvic inflammatory disease, which is a major cause of infertility. In societies where the role of women is closely identified with her ability to bear children, this rape-related consequence is psychologically and socially devastating.
In many countries, such as Mexico, wives’ bargain- ing power in marriage is lowest in decisions about when and if sexual intercourse will occur (Beneria & Roldan, 1987; Worth, 1989). A major determinant of birth control use is partner approval in countries as diverse as Mexico, South Africa, and Bangladesh (Banwell, 1990; Kincaid, 1991). Fear of male reprisal limits the use of birth control (Dixon-Mueller, 1992). In Mexico and Peru, women feared violence, desertion, or accusations of infidelity if they suggested birth control (Folch-Lyon, Macorra, & Schearer, 1981; Fort, 1989). Natural family planning in the Philippines, Peru, and Sri Lanka is undermined by the husband arriving home drunk and forcing his wife to have sex (Liskin, 1981). Victimization can lower self-esteem and confidence and impede the ability to protect the self. Therefore, the ability to enforce condom use is influenced both by the aftereffects of earlier victimization and by direct threats of violence.
Birth control use.

526 KOSS ET AL.
THE CUMULATIVE HEALTH BURDEN
The burden of sexual violence on health can be calculated in terms of the additional costs to the health care systems to care for victimization-related health aftereffects and in terms of women’s quality of life by examining the healthy years of life lost because of violence.
Economic Costs
Victimized women in the United States receive significantly more medical care than nonvictimized women (Colding et al., 1988; Kimerling & Cal- houn, 1994; Koss, KOSS, & Woodruff, 1991). Thus, adult women who had been physically and sexually assaulted in their past visited their physician twice as often in an index year-an average of 6.9 visits per year, com- pared to 3.5 visits for nonvictimized women ( KOSS, KOSS, & Woodruff, 1991). Utilization data across 5 years preceding and following victimiza- tion ruled out the possibility that victims had been high utilizers of services from some earlier point preceding their victimization. The costs of provid- ing a year of healthcare for the severely victimized women are 2.5 times higher than nonvictimized women.
Healthy Years of Life Lost
Estimates of the health burden of rape must take into account both its prevalence and the extent of disability that it creates. Perhaps the best attempt to quantify the health consequences appears in the World Deuel- opment Report 1993: Investing in Health, the policy annual of the World Bank. For this exercise, Bank staff and outside experts attempted to esti- mate the healthy years of life lost to women and men from a variety of causes. The exercise counted every year lost due to premature death as one disability-adjusted life year or DALY and every year spent sick or incapacitated as a fraction of a DALY, depending on the severity of the disability. Neither rape nor domestic violence are diseases in and of them- selves but they are risk factors that lead to a range of diseases including mental disorders such as PTSD, physical illnesses such as irritable bowel syndrome, and reproductive consequences such as sexually transmitted diseases, exposure to HIV, and pregnancy-related health consequences.
According to this analysis, rape and domestic violence both emerge as a significant cause of disability and death among women of reproductive age in both the industrialized and developing world. The estimates suggest that gender-based victimization accounts for almost 1 in every 5 healthy years of life lost to women ages 15 to 44 in established market economies. The health burden for rape and domestic violence is roughly the same in developing countries, but because of a greater overall burden of disease,

Health Burden of Rape 527 the percentage attributable to gender-based victimization is smaller. Among demographically developing countries, estimates are that rape and domestic violence account for 5 % of the healthy years of life lost to women of reproductive age. In developing countries where maternal mortality and poverty-related diseases have been brought under relative control, rape and domestic violence again account for a larger percentage, 16 % of the total burden. On a global basis, the health burden from gender-based victimization (9.5 million DALY) is comparable to that posed by other diseases or risk factors already high on the world agenda such as HIV (10.6 million DALY), tuberculosis (10.9 million DALY), sepsis during childbirth (10 million DALY), all cancers (9.0 million DALY), and car- diovascular disease ( 10.5 million DALY ).
CONCLUSIONS AND RECOMMENDATIONS
The studies reviewed here reveal that rape is manifested in a variety of forms, supported by sociocultural norms, and is widespread around the globe. Although current data are sparse, they confirm that rape plays a significant role in women’s physical and mental health. In addition, they substantiate the assertion made at the outset that women’s rights with regard to their bodies do involve survival issues with widespread public impact. However, more and better research is needed to spur political action globally and to influence the ways in which physical, mental, and reproductive healthcare are delivered to women. In the following material we focus on applied research. We also consider intervention and preven- tion strategies of utmost importance but do not wish to duplicate Schuler’s numerous recommendations for understanding, responding to, and pre- venting gender-based violence, including rape (1992, pp. 22-23).
Assembling a Global Database
Reliable and valid cross-national data on rape prevalence are an impor- tant priority because these numbers help raise awareness of the problem of sexual violence and justify allocation of resources for services and preven- tion. The reverse may also be true. That is, the minimal existing database may reflect the current priority placed on documenting this threat to women’s health and quality of life. It is particularly pressing that changes be made in international crime surveys so that the rape is detected more fully. Emerging evidence from credible sources such as Statistics Canada ( The Daily Statistics Canada, November 18,1993, pp. 1-10) reaffirm that the male violence against women is there if the lessons that have been learned about its measurement are applied. In contrast, publication of flawed sexual assault estimates by international agencies are a cruel hoax for women. The low numbers invalidate women’s experience, indicate a

528 KOSS El AL.
lack of commitment and concern for women’s well-being, and fuel illu- sions that rape is a minor issue on which feminists are overly focused. As a result, rape activists are less able to speak authoritatively about the need for social changes or to command financial resources for intervention and prevention services.
However, it is very unlikely that a single large data collection can ad- dress the multiple questions that exist about rape prevalence among di- verse groups. It is more reasonable to develop a strategy to allow smaller scale, specialized data gathering efforts to be cumulated into a comprehen- sive literature on rape prevalence cross-nationally. Achievement of such a goal rests on developing professional consensus around the following issues:
How will rape and consent be defined? Clearly, a single definition of rape with global currency is lacking. For example, the world is not of a single mind on the validity of the concept of marital rape. One solution to this dilemma is to use multiple items that query about experiences under various consent circumstances. Then individual items can be included or excluded as necessary to calculate local rates or to permit comparison across nations.
Much is already known about the kinds of questions that result in underdetection of rape, includ- ing single omnibus abuse items, items expressed in professional terms such as sexual assault, and items that are vague for the purpose of avoiding offense. Successful detection of rape depends on the use of multiple ques- tions expressed in the most concrete and behaviorally specific language possible. However, the forms of rape that are commonly seen may vary across societies. Therefore, individual research teams may need to use qualitative methods to determine the forms of rape that are most charac- teristic in a given society and guide their choice of screening items accord- ingly. A common core of screening items that was standard across studies would allow accumulation into a coherent body of literature, while still permitting individual investigators the flexibility to add on specialized items of local relevance.
Methods that are feasible in industrialized countries such as mailed or telephone surveys lack appropriateness in other settings. In-person data collection is an obvious alternative, but prevalence research demands large and representative samples. The assembly of such samples will require attention to sample planning as well as the commit- ment of financial resources.
Data collection must be completely confidential and conducted in total privacy. Other- wise, women may hesitate to reveal rape, particularly in societies where severe stigma attaches to the rape victim, and can even result in her being
What questions will be used to identify rape?
How will data be collected?
How will confidentiality and rapport be established?

Health Burden of Rape 529
incarcerated or put to death. In addition, given the large proportion of rapes that are perpetrated by family members, questioning in front of others may place the woman who reveals rape at risk of retaliatory vio- lence. Careful thought must be given to the selection of the culturally appropriate people to serve as interviewers, while at the same time devel- oping procedures to ensure that interviewers can avoid work with kin or acquaintances.
There is no evidence that women inflate their reports of minor victimizations. Indeed, respondents are more likely to take a conservative approach in which only obvious incidents are labeled as abuse (Mullen et al. , 1988). Some observ- ers consider underdetection of rape to be a more serious problem than false reporting ( KOSS, 1993). However, it is prudent to include reliability and validity checks into survey protocols to bolster the credibility of the data. This step is important because any data on rape are a powerful challenge to the patriarchal status quo and are likely to be received with scrutiny and skepticism.
How will the validity of the responses be demonstrated?
Describing the Context and Impact of Rape
Participants at a recent meeting of the Population Council and the Pacific Institute for Women’s Health concluded that a research agenda on sexual violence globally should be guided by several general principles: It should be across cultures, across continents, across the life span, and free from heterosexist bias. Currently, there are almost no scientific studies of rape prevalence or consequences in the nonindustrialized world. In redressing this deficit, it is necessary for world organizations to develop strategies to bring academics and activists together. Alone, activists may lack the train- ing and support to carry out scientifically valid research; and academics may use sophisticated methods to ask the wrong questions. Collaborative research models are needed, models that may require researchers to re- spond to realities of sexual oppression that lie outside of their previous, perhaps privileged experience (e. g. , Lykes, 1989). Guided by their conclu- sions and principles, and recognizing the importance of credible research findings to the international women’s movement to conceptualize women’s rights as human rights, we emphasize the following areas of investigation for future research:
1 . Context of Violence Studies are needed to address the sociocultural context that shapes and supports gender-based sexual violence, including studies of sexual values, attitudes and scripts, and gender-linked sexual roles; influential sociocul- tural institutions and organizations and their mechanisms for influencing sexual violence; and economic and cultural practices that engender vio-

530 KOSS ET AL.
lence. Such studies are particularly needed to document the public nature of this issue.
2. Basic Epidemiologic Research To document the societal impact of rape on health, prevalence estimates based in different healthcare settings are needed. Links between rape, other forms of violence, and other social problems (e.g., unwanted preg- nancy), must be explored. Questions on gender-linked violence should be integrated into health and social surveys and ongoing research on AIDS, sexuality, and family planning.
3. Interpretations and Meanings Popular myths about rape, its perpetrators and victims, and how such myths limit understanding of the destructive consequences of violence, must be documented cross-culturally. Although physical and emotional symptoms seen in the aftermath of rape may be similar across cultures, groups differ in the meanings attached to these symptoms and in the preferred methods for healing. Urgently needed are culturally sensitive portraits of violence and its effects from the point of view of its victims ( RUSSO, KOSS, & Goodman, in press).
4 . Consequences of Rape Studies of the consequences of rape need to be extended into settings where multiple sources of trauma are occurring, as well as studies of the cultural attitudes toward rape that shape the form of recovery and influence the extent to which recovery is even believed to be possible. Studies are needed on the psychological, social, somatic, and economic consequences of vari- ous forms of rape in diverse sociocultural contexts.
5. Processes that Maintain Violence The major systems of criminal justice, law, media, and medical care play a role in maintaining rape by procedures that deny victimization, create obstacles to obtaining validation or care, and decontextualize injury and illness. Studies that delineate these processes are needed, including how laws are enforced, how victims are handled in systems (e.g., in the courts or in emergency rooms), how rape is reported by the media, and biases held by key decision-makers (e. g., police, judges, editors, physicians).
6. Zntervention Little is known about the social networks through which people are now dealing with sexual violence. This information is essential to formulate responses to sexual violence that are culturally appropriate. Undesirable medicalizing of the response to sexual violence can be avoided by under- standing cultural patterns in healing the victim and addressing the perpe- trator. In many countries, sexual violence is viewed as a community prob- lem for which there must be a political response.

Health Burden of Rape 531
7. Prevention/Education Informed approaches to intervention rest upon developing a theoretical and empirical understanding of the context of violence and the social processes that maintain violence. But in addition to developing a relevant knowledge base, it is necessary to disseminate that knowledge to women’s groups, as well as others, so that the findings can be used to take effective action.
Many of these research avenues will pose formidable methodological and practical challenges. Yet, credible research on rape is urgently needed that explores its multiple forms in criminal context and documents its health consequences and public impact. Feminist psychologists who blend the identities of academic and activist have special roles to play in building bridges across disciplines, communities, and cultures so that the outcome of our efforts will reflect the reality of women’s lives around the world, and will address real survival threats to women.
First draft received: January 12,1994 Final draft received: June 27, 1994
REFERENCES
Agger, I. (1989). Sexual torture of political prisoners: An overview. Iournal of Traumatic Stress, 2, 305-318.
American Psychiatric Association. ( 1994). Diagnostic and statistical manual of mental disor- ders (4th ed.). Washington, DC: Author.
Amnesty International. (1992). Rape and sexual abuse: Torture and ill-treatment of women in detention. New York: Author.
Archavanitkui, K., & Pramualratana, A. (1990, October). Factors affecting women’s health in Thailand. Paper presented at the Population Council Workshop on Women’s Health in Southeast Asia, Jakarta.
Asia Watch. (1992). Burma: Rape, forced labor, and religious persecution in Northern Ara- kan. Washington, DC: Asia Watch, 1992.
Avendano, C., & Vergara, J. (1992). La violencia sexual en Chile, dimensiones: Colectiva, cultural y pola‘tica. Santiago, Chile: Servicio Nacional de la Mujer.
Banwell, S. S. (1990). Law, status of women, and family planning in sub-saharan Africa: A suggestion for action. Nairobi: The Pathfinder Fund.
Bart, P. B., Blumberg, R. L., Tombs, T., & Behan, F. (1975). The cross-societal study of rape: Some methodological problems and results. Paper presented at the Groves Confer- ence International Workshop on Changing Sex Roles in Family and Society, Dubrovnik, Yugoslavia .
Beattie, V. (1992). Analysis of the results of a survey on sexual violence in the UK. Cam- bridge, UK: Women’s Forum (unpublished manuscript).
Becker, D., Lira, E., Castillo, M. I., Ganez, E., & Kovalskys, J. (1990). Therapy with victims of political repression in Chile: The challenge of social reparation. Journal of Social Issues, 46,133-149.
Beebe, D. K. (1991). Emergency management of the adult female rape victim. American Family Physician, 43,2041-2046.
Ben Baraka, M. (1993, November). DejZoration in Algeria: A case study of force during sexual initiation. Paper presented at the United Nations Population Council meeting,
532 KOSS ET AL.
Sexual Coercion and Women’s Reproductive Health, jointly sponsored by the Population Council and the Pacific Institute for Women’s Health, New York.
Beneria, L., & Roldan, M. (1987). The crossroads of class and gender. Chicago: University of Chicago Press.
Blatt, D. (1993). Recognizing rape as a method of torture. New York University Review of Law and Social Change, 19,821.
Bowen, D. J., Carscadden, L., Beighle, K . , & Fleming, I. (1992). Post-traumatic stress disorder among Salvadoran women: Empirical evidence and description of treatment. Women b Therapy, 13,267-280.
Boyer, D., & Fine, D. (1992). Sexual abuse as a factor in adolescent pregnancy and child maltreatment. Family Planning Perspectives, 24, 4-10.
Bradley, C. (1990). W h y male violence against women is a development issue: Reflections f rom Papua, New Guinea. UNIFEM Occasional Paper. New York: United Nations Fund for Women.
Broude, G. J., & Green, S. J. (1976). Cross-cultural codes on twenty sexual practices. Ethnology, 15,409-429.
Brownmiller, S. (1975). Against our will: Men, women and rape. New York: Simon & Schuster.
Bunch, C. (1991). Women’s rights as human rights: Toward a re-vision of human rights. In Gender violence: A development and human rights issue. Rutgers, NJ: Center for Wom- en’s Global Leadership.
Bunster, X. (1986). Surviving beyond fear: Women and torture in Latin America. In J. Nash & H. Safa (Eds. ), Women and change in Latin America (pp. 297-325). South Hadley, MA: Bergin & Gamey.
Burnam, M. A., Stein, J. A., Golding, J. M., Siegel, J. M., Sorenson, S. B., Forsythe, A. B., & Telles, C. A. (1988). Sexual assault and mental disorders in a community population. Journal of Conszrlting and Clinical Psychology, 56, 843-850.
CAMVAC. (1985). Carpeta de informacidn bdsica para la atencidn solidaria y feminista a mujeres violadas. Mexico City: Centro de Apoyo a Mujeres Violadas.
Carpeta Basica. (1991). Mexico City: Procurador de Justicia del Distrito Federal de MBxico. Consumers Association of Penang. (1988). Rape in Malaysia. Penang, Malaysia. Coomaraswamy, R. (1992). Sri Lanka-Of Kali born: Women, violence, and the law. In M.
Schuler (Ed. ), Freedom from violence: Women’s strategiesfrom around the world (pp. 49-61). New York: UNIFEM WIDBOOKS.
Council on Scientific Affairs. (1992). Violence against women: Relevance for medical prac- titioners. Journal of the American Medical Association, 267, 3184-3189.
COVAC. (1990). Evaluacidn de proyecto para educacidn, capacitacidn, y atencidn a mujeres y menores de edad en materia de violencia sexual, enero a diciembre, 1990. Mexico City: Asociacion Mexicana contra la Violencia a las Mujeres.
DeKeseredy, W., & Kelly, K. (1993). The incidence and prevalence of woman abuse in Canadian university and college dating relationships. The Canadian Journal of Sociol- ogy, 18, 137-159.
Dixon-Mueller, R. (1992, November 29). Pais conta 337 mulheres agredidas por dia. Folha de San Paulo.
Dunn, S. F . , & Gilchrist, V. J. (1993). Sexual assault. Primary Care, 20, 359-373. Economic and Social Council. (1992). Report to the Working Group on Violence Against
Women. Vienna: United Nations, E/CN.6/WG.21/1992/L.3. Ericksen, K. P. (1994, May). Recommendations to the Women’s Health Advisoy Committee
on Women’s Reproductive Health and Disease. Paper prepared for the American Psycho- logical Association conference Psychosocial and Behavioral Factors in Women’s Health, Washington, DC.
Estrich, S. (1987). Real rape. Cambridge, MA: Harvard University Press. Finkelhor, D. (1987). The sexual abuse of children: Current research reviewed. Psychiatric
Annals, 17,233-241.

Health Burden of Rape 533 Fauveau, V., & Blanchet, T. (1989). Epidemiology and cause of deaths among women in
rural Bangladesh. International Journal of Epidemiology, 18, 139-145. Foa, E. B., Rothbaum, B. O., & Steketee, G. S. (1993). Treatment of rape victims. Journal
of Interpersonal Violence, 8, 256-276. Folch-Lyon, E., Macorra, L., & Schearer, S . B. (1981). Focus group and survey research on
family planning in Mexico. Studies in Family Planning, 12, 409-432. Fort, A. (1989). Investigating the social context of fertility and family planning: A qualitative
study in Peru. International Family Planning Perspectives, 15, 88-94. Friedman, A. R. (1992). Rape and domestic violence: The experience of refugee women.
Women rlz Therapy, 13,65-78. Gavey, N. (1991). Sexual victimization prevalence among New Zealand university students.
lournal of Consulting and Clinical Psychology, 59, 464-466. George, A. (1993, November). Coerciue sex within consensual unions: A case study fTom
Bombay. Paper presented at the United Nations Population Council meeting, Sexual Coercion and Women’s Reproductive Health, jointly sponsored by the Population Coun- cil and the Pacific Institute for Women’s Health, New York.
Giller, J. E. (1992). War, women and rape. Thesis presented to the School of Oriental and African Studies, University of London, London, England.
Goldfeld, A. E., Mollica, R. F., Pesavento, B. H., & Farone, S. V. (1988). The physical and psychological sequelae of torture. Journal of the American Medical Association, 259,
Golding, J. M. (1994). Sexual assault history and physical health in randomly selected Los Angeles women. Health Psychology, 13, 130-138.
Goodman, L. A., Koss, M. P., & Russo, N. F. (1993a). Violence against women: Physical and mental health effects. Part I. Research findings. Applied 6 Preventive Psychology: Current Scientific Perspectives, 2, 79-89.
Goodman, L. A., Koss, M. P., & Russo, N. F. (1993b). Violence against women: Physical and mental health effects. Part 11. Conceptualizing post-traumatic stress. AppZied rlz Preventive Psychology: Current Scientific Perspectives, 2, 123-130.
Gordon, M. T., & Riger, S . (1989). Thefemalefear. New York: Free Press. Graitcer, P. L., & Youssef, Z. (Eds.). (1993). Injury in Egypt: An analysis of injuries as a
health problem. Jointly published by USAID and the Ministry of Health Cairo, Egypt. Handwerker, W. P. (1991, November). Gender power difference may be STD risk factors
for the next generation. Paper presented at the 90th annual meeting of the American Anthropological Association, Chicago, IL.
Hanson, R. K. (1990). The psychological impact of sexual assault on women and children: A review. Annals of Sex Research, 3 , 187-232.
Heise, L. (1991, December 13). When women are prey. Washington Post. pp. Cl-C3. Heise, L. (1993a). Violence against women and reproductive health: Where are the intersec-
tions? Journal of Law, Medicine, and Ethics, 21, 76-86. Heise, L. (1993b, November). Status of existing knowledge. Paper presented at the Popula-
tion Council meeting, Sexual Coercion and Women’s Reproductive Health, jointly spon- sored by the Population Council and the Pacific Institute for Women’s Health, New York.
Heise, L., Pitanguy, J., & Germain, A. (1993). Violence against women: The hidden health burden. Washington, DC: The World Bank.
Hendricks-Mathews, M. K. (1993). Survivors of abuse: Health care issues. Primary Care, 20, 391-406.
Human Rights Watch. (1992a). Untold terror: Violence against women [in Peru]. New York: Author.
Human Rights Watch. (199213). Double jeopardy: Police abuse of women in Pakistan. New York: Author.
Human Rights Watch. (1992~). Rape and mistreatment of Asian maids[Kuwait]. New York: Author.
2725-2729.

534 KOSS ET AL.
Human Rights Watch. (1993a). War crimes in Bosnia-Hercegovina: Volume I I . New York:
Human Rights Watch. (1993b). Widespread rape of Somali women refugees in NE Kenya.
Human Rights Watch. (1993~). Rape in Kashmir. New York: Author. Jahangi, A., & Jalani, H. (1990). The Hudood Ordinances: A divine sanction? Lahore,
Pakistan: Rhotas Books. Kandaloof, E. (1991, May). Services at Haifa Rape Crisis Center. Paper presented at the
conference, Leading the Way Out: A Global Conference to End Violence Against Women sponsored by the Global Fund for Women, Menlo Park, CA.
Kilpatrick, D. G., Saunders, B. E., Veronen, L. J., Best, C. L., & Von, J . M. (1987). Criminal victimization: Lifetime prevalence, reporting to police, and psychological im- pact, Crime and Delinquency, 33,479-489.
Kimerling, R., & Calhoun, K. S. (1994). Somatic symptoms, social support, and treatment seeking among sexual assault victims. Journal of Cowl t ing and Clinical Psychology, 62, 333-340.
Kincaid, D. L. (1991, November 13). Family planning and the empowerment of women in Bangladesh. Paper presented at the annual meeting of the American Public Health Association, Atlanta, GA.
Kisekka, M., & Otesanya, B. (1988, August). Sexually transmitted disease as a gender issue: Examplesfrom Nigeria and Uganda. Paper given at the AFARDlAAWORD Third Gen- eral Assembly on the African Crisis and the Women’s Vision of the Way Out, Dakar, Senegal.
Korean Sexual Violence Relief Center. (1991). information booklet of the Korean Sexual Violence Relief Center. Seoul, Korea: Author.
Koss, M. P. (1993). Detecting the scope of rape: A review of prevalence research methods. Journal of Interpersonal Violence, 8,98-122.
Koss, M. P., Gidycz, C. A., & Wisniewski, N. (1987). The scope of rape: Incidence and prevalence of sexual aggression and victimization in a national sample of higher educa- tion students. Journal of Consulting and Clinical Psychology, 55, 162-170.
Koss, M. P., Goodman, L. A,, Browne, A., Fitzgerald, L., Keita, G. P., & Russo, N. F. (1994). No safe haven: Male violence against women at home, at work, and in the community. Washington, DC: American Psychological Association.
Koss, M. P., & Heslet, L. (1992). Somatic consequences of violence against women. Archives of Family Medicine, 1, 53-59.
Koss, M. P., Koss, P. G., &Woodruff, W. J. (1991). Deleterious effects of criminal victimiza- tion on women’s health and medical utilization. Archives of Internal Medicine, 151, 342-357.
Koss, M. P., Woodruff, W. J., & Koss, P. G. (1991). Criminal victimization among primary care medical patients: Prevalence, incidence, and physician usage. Behavioral Sciences and the Law, 9,85-96.
Kressel, G. (1981 ). Sororicide/filiacide: Homicide for family honour. Current Anthropology,
LaFree, G. (1989). Rape and criminal justice: The social construction of assault. Belmont, CA: Wadsworth.
Lapin, D. (1992, November). Assessing psychosocial needs of refugee women and children using rapidfield techniques. Paper presented at the 120th Annual Meeting of the Ameri- can Public Health Association, Washington, DC.
Lazarus, R. S. (1991). Cognition and motivation in emotion. American PsychoZogist, 46, 352-367.
Levinson, D. ( 1989). Violence in cross-cultural perspective. Newbury Park, CA: Sage. Liskin, L. (1981). Periodic abstinence: How well do new approaches work? Population
Reports, Series 1, No. 3. Baltimore, MD: Population Information Program, Johns Hop- kins University.
Author.
New York: Author.
22, 141-158.

Health Burden of Rape 535
Lunde, I., & Ortmann, J. (1990). Prevalence and sequelae of sexual torture. Lancet, 336,
Lurigio, A. J., & Resick, P. A. (1990). Healing the psychological wounds of criminal victim- ization: Predicting postcrime distress and recovery. In A. J. Lurigio, W. G. Skogan, & R. C. Davis (Eds.), Victims of crime: Problem, policies, and programs (pp. 51-67). Newbury Park, CA: Sage.
Lykes, M. B. (1989). Dialogue with Guatemalan Indian women: Critical perspectives on constructing collaborative research. In R. Unger (Ed. ), Representations: Social construc- tions of gender (pp. 167-185). Amityville, NY: Baywood.
Lykes, M. B., Brabeck, M. M., Ferns, T., & Radan, A. (1993). Human rights and mental health among Latin American women in situations of state-sponsored violence. Psychol- ogy of Women Quarterly, 17,525-544.
MacKinnon, C. A. (1983). Feminism, Marxism, method and the State: Toward feminist jurisprudence. Signs: Journal of Women in Culture and Society, 8,635-658.
Martin-Barb, I. (1988). La violencia politica y la guerra como causa del trauma psicosocial en El Salvador [Political violence and war as causes of psychosocial trauma in El Salva- dor]. Revista de Psicologia de El Salvador, 28, 123-141.
Mathur, K. (1992, October 10). Bhateri rape case: Backlash and protest. Economic and Political Weekly, pp. 2221-2224.
McCann, I. L., Sakheim, D. K., & Abrahamson, D. J. (1988). Trauma and victimization: A model of psychological adaptation. The Counseling Psychologist, 6,531-594.
Meyerding, J. (1977). Early sexual experience and prostitution. American Journal of Psychia-
Miedzian, M. (1993, November). An overview of sex and aggression in popular discourse. Paper presented at the Population Council meeting, Sexual Coercion and Women’s Re- productive Health, jointly sponsored by the Population Council and the Pacific Institute for Women’s Health, New York.
Minturn, L., Grosse, M., & Haider, S. (1969). Cultural patterning of sexual beliefs and behavior. Ethnology, 8, 301-318.
Mollica, R. (1986, August). Cambodian refugee women at risk. Paper presented at the annual meeting of the American Psychological Association, Washington, DC.
Mollica, R., & Son, L. (1989). Cultural dimensions in the evaluation and treatment of sexual trauma: An overview. Psychiatric Clinics of North America, 12,363-379.
Mollica, R., Wyshak, G., & Lavelle, J. (1987). The psychological impact of war trauma and torture on Southeast Asian refugees. American Journal of Psychiatry, 144,1557-1571.
Mullen, P. E., Romans-Clarkson, S. E., Walton, V. A., & Herbison, P. G. (1988). Impact of sexual and physical abuse on women’s mental health. Lancet, 1 , 841.
National Victims Center. (1992, April 23). Rape in America: A report to the nation. Arling- ton, VA: Author.
Norris, F. H. (1992). Epidemiology of trauma: Frequency and impact of different potentially traumatic events on different demographic groups. Journal of Consulting and Clinical
Paone, D., Chavkin, W., Willets, I., Friedman, P., & Des Jarlais, D. (1992). The impact of sexual abuse: Implications for drug treatment. Journal of Women’s Health, 1 , 149- 153.
Perez, A. M. (1990). Aproximacion diagndstica a las violaciones de mujeres en 10s distritos de Panamci y Sun Miguelito. Centro Para el Desarrollo de la Mujer, Universidad de Panam&
Portugal, A. M. (1988). Crbnica de una violacibn provocada? Revisa Mujer/Fempress Con- traviolencia. Santiago, Chile: FEMPRESS-ILET.
Resick, P. A. (1987). Psychological effects of victimization: Implications for the criminal justice system. Crime and Delinquency, 33,468-478.
Resick, P. A. (1990). Victims of sexual assault. In A. J. Lurigio, W. G. Skogan, & R. C. Davis (Eds.), Victims of crime: Problems, policies, and programs (pp. 69-85). Newbury Park, CA: Sage.
289-291.
try, 134,1381-1385.
Psychology, 60,4409-4418.

536 KOSS ET AL.
Resick, P. A. (1993). The psychological impact of rape. Journal of Interpersonal Violence, 8 , 223-256.
Rompiendo el Silencio. (1992). La Boletina, OctlNov, 9. Managua, Nicaragua: Puntos de Encuentro.
Rosas, M. I. (1992). Violencia sexual y pofitica criminal. CLADEM lnformrativo No. 6, Lima, Peru.
Roth, S., & Lebowitz, L. (1988). The experience of sexual trauma. Journal of Traumatic Stress, 1 , 79-107.
Rothbaum, B. O., Foa, E. B., Riggs, D. S., Murdock, T., & Walsh, W. (1992). A prospective examination of post-traumatic stress disorder in rape victims. Journal of Traumatic Stress, 5 , 455-475.
RozBe, P. D. (1993). Forbidden or forgiven? Rape in cross-cultural perspective. Psychology of Women Quarterly, 17, 499-514.
RozBe, P. D., & Van Boemel, G . B. (1989). The psychological effects of war trauma and abuse on older Cambodian refugee women. Women dr Therapy, 8, 23-50.
Russell, D. (1990). Rape in marriage (revised edition). Bloomington, IN: Indiana University Press.
Russo, N. F., Koss, M. P., & Goodman, L. (in press). Male violence against women: A global health and development issue. In L. L. Adler & F. L. Denmark (Eds.), Violence and the prevention of violence. New York: Greenwood.
Sanday, P. R. (1981). The socio-cultural context of rape: A cross-cultural study. Journal of Social Issues, 37, 5-27.
Sanday, P. R. (1993, November). Men in groups: A cross-cultural look at gang rape. Paper presented at the Population Council meeting, Sexual Coercion and Women’s Reproduc- tive Health, jointly sponsored by the Population Council and the Pacific Institute for Women’s Health, New York.
Schuler, M. (1992). Violence against women: An international perspective. In M. Schuler (Ed.) , Freedom from violence? Women’s strategiesfrom around the world (pp. 1-48). New York: UNIFEM WIDBOOKS.
Searles, P., & Berger, R. J. (1987). The current status of rape reform legislation: An examina- tion of state statutes. Women’s Rights Law Reporter, 10, 25-43.
Shamim, I. (1985, December). Kidnapped, raped, killed: Recent trends in Bangladesh. Paper presented at the International conference on Families in the Face of Urbanization, New Delhi.
Sheperd, J. (1992). Post-traumatic stress disorder in Vietnamese women. Women 6 Therapy,
Shim, Y. (1992). Sexual violence against women in Korea: A victimization survey of Seoul women. Paper presented at the conference on International Perspectives: Crime, Justice and Public Order, St. Petersburg, Russia, June 21-27.
Sogbetun, A. O., Alausa, K . O., & Osoba, A. 0. (1977). Sexually transmitted disease in Ibadan, Nigeria. British Journal of Venereal Disease, 53, 158.
Statistics Canada. (1993, November 18). The Violence Against Women Survey highlights. The Daily Statistics Canada, pp. 1-10.
Swiss, S., & Giller, J. E. (1993). Rape as a crime of war: A medical perspective. Journal of the American Medical Association, 270( 5), 612-615.
Thomas, D. (1993, November). Rape in refugee and conflict situations. Paper presented at the United Nations Population Council meeting, Sexual Coercion and Women’s Repro- ductive Health, jointly sponsored by the Population Council and the Pacific Institute for Women’s Health, New York.
Toubia, N. (1993). Female genital mutilation: A call for global action. New York: Women, Ink.
Treguear, T. L., & Carro, C. (1991). Nifias madres: Recuento de una experiencia. San Jose, Costa Rica: PROCAL.
13, 281-296.

Health Burden of Rape 537 United Nations. (1993). Rape and the abuse of women in the territory of former Yugoslauia
(UN document E/CN.4/1993/L.21). Geneva, Switzerland: Author. Van Boemel, G. B., & RozBe, P. D. (1992). Treatment for psychosomatic blindness among
Cambodian refugee women. Women &- Therapy, 13, 239-266. van Dijk, J., & Mayhew, P. (1993). Criminal victimization in the industrial world: Key
findings of the 1989 and 1992 International Crime Surveys. In A. Alvassi del Frate, U. Zvekic, & J. van Dijk (Eds.), Understanding crime: Experiences of crime and crime control (U.N. publication E-93.III.N.2). Rome, Italy: United Nations International Crime and Justice Institute.
Warr, M. (1985). Fear of rape among urban women. Social Problems, 32,239-250. Winfield, I., George, L. K., Schwartz, M., & Blazer, D. G. (1990). Sexual assault and
psychiatric disorders among a community sample of women. American Journal of Psy- chiatry, 147,335341.
World Bank. (1993). World Development Report 1993: Inuesting in Health. New York: Oxford University Press.
Worth, D. (1989). Sexual decision-making and AIDS: Why condom promotion among vul- nerable women is likely to fail. Studies in Family Planning, 20, 297-307.
Wyatt, 6. E. (1988). The relationship between child sexual abuse and adolescent sexual functioning in Afro-American and White American women. Annals of the New York Academy of Sciences, 528,111-122.
Wyatt, G. E. (1993, November). Lessonsfiom Jamaica. Paper presented at the Population Council meeting, Sexual Coercion and Women’s Reproductive Health, jointly sponsored by the Population Council and the Pacific Institute for Women’s Health, New York.
Wyatt, 6. E., Guthrie, D., & Notgrass, C. M. (1992). Differential effects of women’s child sexual abuse and subsequent sexual revictimization. Journal of Consulting and Clinical
Zierler, S., Feingold, L., Laufer, D., Velentgas, P., Kantorwitz-Gordon, S. B., & Mayer, K. (1991). Adult survivors of childhood sexual abuse and subsequent risk of HIV infection. American Journal of Public Health, 81,572-575.
PSyChology, 60,167-173.





























