Embed Size (px)
Citation preview

THEORET ICAL STUD IES doi: 10.1111/j.1471-6712.2008.00645.x
The needs of carers of people with multiple sclerosis: aliterature review
Margarita Corry BNS, BSc, MSc, RNT, RGN (Lecturer)1 and Alison While PhD, Cert Ed, RGN, RHV (Professor)2
1Lecturer, School of Nursing & Midwifery, Trinity College, Dublin, Ireland, and 2Professor Community Nursing, King’s College London,
Florence Nightingale School of Nursing & Midwifery, London, UK
Scand J Caring Sci; 2009; 23; 569–588
The needs of carers of people with multiple sclerosis: a
literature review
People with multiple sclerosis depend heavily upon their
families and other informal carers as they receive limited
support from health-care professionals or health-care ser-
vices. Adopting the carer role results in a life-changing
experience, which may bring rewards and challenges to
the carer. This paper reviews the research addressing the
experiences of carers of people with multiple sclerosis
published between 2002 and 2007 building upon an earlier
review. The literature suggests that carers have needs
across various domains and that spouses/partners have
particular needs. Much of the evidence has limited
generalizibility although the geographical spread of the
evidence indicates considerable consistency of need. The
review describes ongoing carer needs which require sup-
portive care and provides the basis for the development
and testing of carer interventions for use by health-care
professionals.
Keywords: literature review, informal carers, multiple
sclerosis, spouses, needs, experiences.
Submitted 1 February 2008, Accepted 21 May 2008
Introduction
Multiple sclerosis (MS) is a progressive degenerative
neurological disease of unknown cause with a variety of
neurologically distressing symptoms (1), which results in
life-changing experiences for both the person with MS
(PwMS) and his carer. Carers provide much of the every-
day support for the PwMS contributing substantially to
their on-going care and well being (2). Since the 1990s, the
needs of the carers has been identified as requiring support
(3); however, resources are frequently limited reflecting
the low prevalence of the disorder, the low profile of carer
support within health-care provision and the increasing
pressure on health and social care budgets.
Informal carers are carers: ‘who are not financially
compensated for their services’ (4: 946) and may be cate-
gorized as primary or secondary carers although there is
inconsistency in the use of these terms. For example, pri-
mary carers may be spouses (5) or those (not necessarily
spouses) dedicating a minimum of 1 hour each day to the
care of a PwMS (6). Secondary carers are those with whom
the primary carer would feel comfortable leaving the per-
son with for short periods of time (5). Generally, the pri-
mary carer is someone who spends a substantial amount of
time providing care, while a secondary carer provides short
periods of relief for the primary carer. In this review, the
term carer is used to denote informal carers and spousal
carer to denote informal carers who are spouses/partners.
A number of factors have been identified as contributing
to the care burden, including: the severity of impairment
of the PwMS; age and health of the carer; availability of
support; and perceived uncertainty (7–10). In a systematic
review of the needs and experiences of carers of PwMS,
McKeown et al. (3) highlighted that carers experience a
decrease in their quality of life (QOL), deficits in their
physical health, impaired psychological well being and
social life, and an adverse effect upon their financial situ-
ation. Decreased QOL was found to be associated with age
(between 50 and 59 years), having a low family income,
being a spouse, the duration and daily frequency of caring,
increased severity of MS symptoms and having an unstable
disease course. Although a causal link could not be
established between caring and physical health deficits
owing to the impact of the normal ageing process and pre-
existing health problems, the most commonly reported
physical deficit was arthritis. However, carer health was
found to be a critical factor in enabling them to continue
providing care. The psychological effect of caring was de-
scribed as ‘chronic sorrow’ and stress was a major factor
with carers reporting more stress symptoms than the
Correspondence to:
Magarita Corry, School of Nursing & Midwifery, Trinity College
Dublin, 24 D’Olier Street, Dublin 2, Ireland.
E-mail: [email protected]
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science 569

general population. Restrictions on carers’ ability to attend
recreational and social activities, holidays, telephone
contacts, and visit friends, all impacted negatively on their
social lives. The financial situation of carers was found to
worsen with the number of years of caring.
Informal caring has gradually received greater recogni-
tion as a major component of community care (11). The
growing dependence upon carers for care delivery in the
wake of budgetary constraints requires that health-care
professionals recognize the negative impact of caring and
provide interventions to sustain carer well being. This re-
view builds upon McKeown et al.’s (3) earlier work to
provide a comprehensive synthesis of current knowledge
to inform professional practice.
Method
Search strategy
A computer-based literature search was conducted using
the following search terms:
‘Multiple sclerosis and needs assessment’; ‘Multiple
sclerosis and needs assessment and carer’; ‘Multiple scle-
rosis and carer’; ‘Multiple sclerosis and carers’; ‘Multiple
sclerosis and caregiver’; ‘Multiple sclerosis and caregivers’;
‘Multiple sclerosis and informal caregivers’; ‘Multiple
sclerosis and informal caregiver’; ‘Multiple sclerosis and
support systems’; ‘Multiple sclerosis and carers’ needs’;
‘Multiple sclerosis and caregiver burden’; ‘Multiple scle-
rosis and caregiver burden and needs assessment’; ‘Multi-
ple sclerosis and caregiver support’; ‘Multiple sclerosis and
caregiver support and needs assessment’ and ‘Multiple
Sclerosis and caring’. Amed, British Nursing Index, CI-
NAHL (thesaurus and exploded), Psychlit, Pubmed (MeSH
database) and Social Science index databases limited to
English language and peer-reviewed articles from May
2002 to November 2007 were searched yielding 412 hits,
including duplicates.
Selection criteria
The inclusion criteria were: primary research which fo-
cussed on adult carers and/or included and reported findings
on the experiences of adult carers’ of PwMS written in
English, published in peer-reviewed journals between May
2002 and November 2007. Papers not meeting these criteria
were excluded from the review. Full texts of all identified
studies were reviewed against the inclusion critera. Thirty-
three papers were identified as relevant for inclusion in the
review. (Not relevant n = 169; duplicates n = 210.) The
quality of the quantitative papers varied with sample sizes
ranging from 13 to 445 and response rates from 19% to
100% or unreported (n = 8 papers). However, owing to the
limited number of studies available, all quantitative papers
that fulfilled the inclusion criteria were included. The
qualitative papers included had sample sizes ranging from 2
to 17. The studies were of varying rigour.
Data analysis
Data were extracted from all the studies and a thematic
content analysis conducted in light of the diversity of the
study foci and measures which precluded any quantitative
analysis. The themes were not imposed but allowed to
emerge from the study findings. They were identified by
the first author initially and validated by the second author.
Results
Tables 1 and 2 provide a summary of the papers; 21 papers
focussed upon carers generally, while 12 focussed upon
spouses as carers. The term spouse is used interchangeably
with partner; the term spouse will be used in this paper.
The research was conducted in 11 countries (Australia
n = 10; England n = 6; United States n = 4; Canada n = 2;
Italy n = 2; Netherlands n = 4; Norway n = 1; Spain n = 1;
Sweden n = 1; Ireland n = 1; Netherlands and Belgium
n = 1). Although there are areas of consistency between
nonspousal and spousal carers, marital satisfaction was
unique to the studies relating to spouses
Carer studies
The carer studies examined the following areas: utilization
of health-care resources by PwMS and their carers and
satisfaction with those resources (11–15); caring activities,
burden and coping strategies (6, 14, 16–21); psycho-social
and physical health and QOL (14, 17, 21–29) and the po-
tential rewards of caring to PwMS (30). All the studies had
a descriptive design (19 surveys and two qualitative stud-
ies) and revealed consistent evidence of the need for re-
sources and services to relieve carer burden. Three themes
emerged from the studies, namely the impact of caring, the
services available and gender differences.
The impact of caring
Four sub-themes emerged regarding the impact of caring:
the psychological and emotional impact of caring, the
impact of disease characteristics on carers, carer burden
and the benefits of caring.
Psychological and emotional impact of caring. The impact of
caring was evident in the carers’ psychological needs, their
levels of stress and distress together with the high level of
activities undertaken and the burden experienced. Psycho-
logical needs constituted the highest number of needs in
the survey of carers of PwMS conducted by Benbow and
Koopman (23), where the sample reported the need to be
listened to and heard by others together with the need for
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
570 M. Corry, A. While
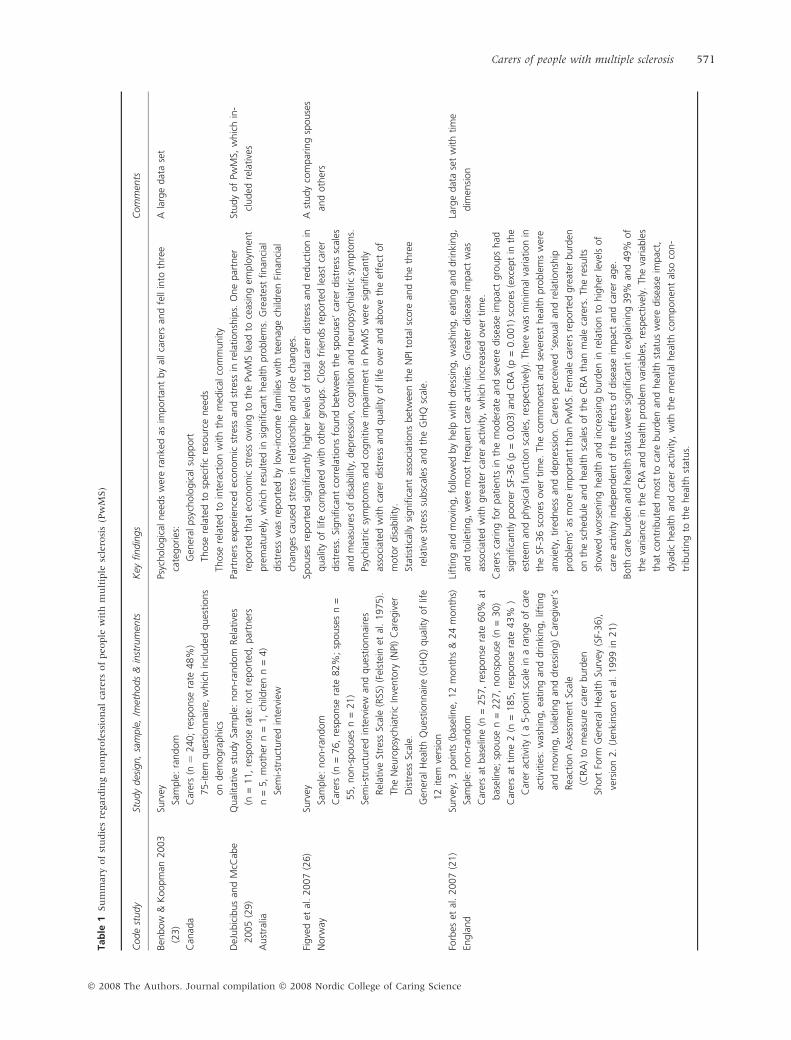
Tab
le1
Su
mm
ary
of
stu
die
sre
gard
ing
non
pro
fess
ion
al
care
rsof
people
wit
hm
ult
iple
scle
rosi
s(P
wM
S)
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Ben
bow
&K
oopm
an2003
(23)
Can
ada
Surv
ey
Sam
ple
:ra
ndom
Car
ers
(n¼
240;
resp
onse
rate
48%
)
75-ite
mques
tionnai
re,w
hic
hin
cluded
ques
tions
on
dem
ogra
phic
s
Psyc
holo
gic
alnee
ds
wer
era
nke
das
import
ant
by
allca
rers
and
fell
into
thre
e
cate
gories
:
Gen
eral
psy
cholo
gic
alsu
pport
Those
rela
ted
tosp
ecifi
cre
sourc
enee
ds
Those
rela
ted
toin
tera
ctio
nw
ith
the
med
ical
com
munity
Ala
rge
dat
ase
t
DeJ
ubic
ibus
and
McC
abe
2005
(29)
Aust
ralia
Qual
itat
ive
study
Sam
ple
:non-r
andom
Rel
ativ
es
(n=
11,
resp
onse
rate
:not
report
ed,
par
tner
s
n=
5,
moth
ern
=1,
child
ren
n=
4)
Sem
i-st
ruct
ure
din
terv
iew
Part
ner
sex
per
ience
dec
onom
icst
ress
and
stre
ssin
rela
tionsh
ips.
One
par
tner
report
edth
atec
onom
icst
ress
ow
ing
toth
ePw
MS
lead
toce
asin
gem
plo
ymen
t
pre
mat
ure
ly,
whic
hre
sulted
insi
gnifi
cant
hea
lth
pro
ble
ms.
Gre
ates
tfinan
cial
dis
tres
sw
asre
port
edby
low
-inco
me
fam
ilies
with
teen
age
child
ren
Finan
cial
chan
ges
cause
dst
ress
inre
lationsh
ipan
dro
lech
anges
.
Study
of
PwM
S,w
hic
hin
-
cluded
rela
tive
s
Figve
det
al.
2007
(26)
Norw
ay
Surv
ey
Sam
ple
:non-r
andom
Car
ers
(n=
76,
resp
onse
rate
82%
;sp
ouse
sn
=
55,
non-s
pouse
sn
=21)
Sem
i-st
ruct
ure
din
terv
iew
and
ques
tionnai
res
Rel
ativ
eSt
ress
Scal
e(R
SS)
(Fel
stei
net
al.
1975).
The
Neu
ropsy
chia
tric
Inve
nto
ry(N
PI)
Car
egiv
er
Dis
tres
sSc
ale.
Gen
eral
Hea
lth
Ques
tionnai
re(G
HQ
)qual
ity
of
life
12
item
vers
ion
Spouse
sre
port
edsi
gnifi
cantly
hig
her
leve
lsof
tota
lca
rer
dis
tres
san
dre
duct
ion
in
qual
ity
of
life
com
par
edw
ith
oth
ergro
ups.
Clo
sefr
iends
report
edle
ast
care
r
dis
tres
s.Si
gnifi
cant
corr
elat
ions
found
bet
wee
nth
esp
ouse
s’ca
rer
dis
tres
ssc
ales
and
mea
sure
sof
dis
abili
ty,dep
ress
ion,co
gnitio
nan
dneu
ropsy
chia
tric
sym
pto
ms.
Psyc
hia
tric
sym
pto
ms
and
cognitiv
eim
pai
rmen
tin
PwM
Sw
ere
signifi
cantly
asso
ciat
edw
ith
care
rdis
tres
san
dqual
ity
of
life
ove
ran
dab
ove
the
effe
ctof
moto
rdis
abili
ty.
Stat
istica
llysi
gnifi
cant
asso
ciat
ions
bet
wee
nth
eN
PIto
talsc
ore
and
the
thre
e
rela
tive
stre
sssu
bsc
ales
and
the
GH
Qsc
ale.
Ast
udy
com
par
ing
spouse
s
and
oth
ers
Forb
eset
al.
2007
(21)
Engla
nd
Surv
ey,
3poin
ts(b
asel
ine,
12
month
s&
24
month
s)
Sam
ple
:non-r
andom
Car
ers
atbas
elin
e(n
=257,
resp
onse
rate
60%
at
bas
elin
e;sp
ouse
n=
227,
nonsp
ouse
(n=
30)
Car
ers
attim
e2
(n=
185,
resp
onse
rate
43%
)
Car
erac
tivi
ty(
a5-p
oin
tsc
ale
ina
range
of
care
activi
ties
:w
ashin
g,
eating
and
drinki
ng,
lifting
and
movi
ng,
toile
ting
and
dre
ssin
g)
Car
egiv
er’s
Rea
ctio
nA
sses
smen
tSc
ale
(CRA
)to
mea
sure
care
rburd
en
Short
Form
Gen
eral
Hea
lth
Surv
ey(S
F-36),
vers
ion
2.
(Jen
kinso
net
al.
1999
in21)
Lift
ing
and
movi
ng,
follo
wed
by
hel
pw
ith
dre
ssin
g,
was
hin
g,
eating
and
drinki
ng,
and
toile
ting,
wer
em
ost
freq
uen
tca
reac
tivi
ties
.G
reat
erdis
ease
impac
tw
as
asso
ciat
edw
ith
gre
ater
care
rac
tivi
ty,
whic
hin
crea
sed
ove
rtim
e.
Car
ers
caring
for
pat
ients
inth
em
oder
ate
and
seve
redis
ease
impac
tgro
ups
had
signifi
cantly
poore
rSF
-36
(p=
0.0
03)
and
CRA
(p=
0.0
01)
score
s(e
xcep
tin
the
este
eman
dphys
ical
funct
ion
scal
es,
resp
ective
ly).
Ther
ew
asm
inim
alva
riat
ion
in
the
SF-3
6sc
ore
sove
rtim
e.Th
eco
mm
ones
tan
dse
vere
sthea
lth
pro
ble
ms
wer
e
anxi
ety,
tire
dnes
san
ddep
ress
ion.
Car
ers
per
ceiv
ed‘s
exual
and
rela
tionsh
ip
pro
ble
ms’
asm
ore
import
ant
than
PwM
S.Fe
mal
eca
rers
report
edgre
ater
burd
en
on
the
sched
ule
and
hea
lth
scal
esof
the
CRA
than
mal
eca
rers
.Th
ere
sults
show
edw
ors
enin
ghea
lth
and
incr
easi
ng
burd
enin
rela
tion
tohig
her
leve
lsof
care
activi
tyin
dep
enden
tof
the
effe
cts
of
dis
ease
impac
tan
dca
rer
age.
Both
care
burd
enan
dhea
lth
stat
us
wer
esi
gnifi
cant
inex
pla
inin
g39%
and
49%
of
the
varian
cein
the
CRA
and
hea
lth
pro
ble
mva
riab
les,
resp
ective
ly.
The
variab
les
that
contr
ibute
dm
ost
toca
reburd
enan
dhea
lth
stat
us
wer
edis
ease
impac
t,
dya
dic
hea
lth
and
care
rac
tivi
ty,
with
the
men
talhea
lth
com
ponen
tal
soco
n-
trib
uting
toth
ehea
lth
stat
us.
Larg
edat
ase
tw
ith
tim
e
dim
ensi
on
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 571
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
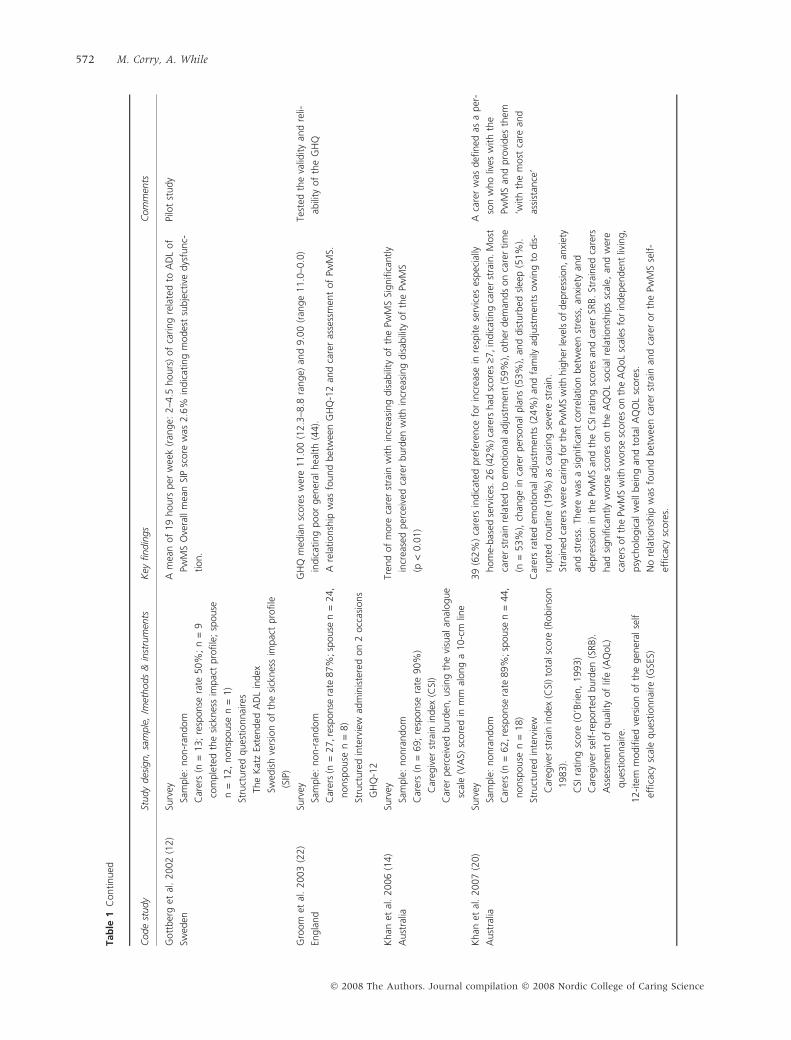
Gott
ber
get
al.
2002
(12)
Swed
en
Surv
ey
Sam
ple
:non-r
andom
Car
ers
(n=
13;
resp
onse
rate
50%
;n
=9
com
ple
ted
the
sick
nes
sim
pac
tpro
file
;sp
ouse
n=
12,
nonsp
ouse
n=
1)
Stru
cture
dques
tionnai
res
The
Kat
zEx
tended
AD
Lin
dex
Swed
ish
vers
ion
of
the
sick
nes
sim
pac
tpro
file
(SIP
)
Am
ean
of
19
hours
per
wee
k(r
ange:
2–4
.5hours
)of
caring
rela
ted
toA
DL
of
PwM
SO
vera
llm
ean
SIP
score
was
2.6
%in
dic
atin
gm
odes
tsu
bje
ctiv
edys
func-
tion.
Pilo
tst
udy
Gro
om
etal
.2003
(22)
Engla
nd
Surv
ey
Sam
ple
:non-r
andom
Car
ers
(n=
27,re
sponse
rate
87%
;sp
ouse
n=
24,
nonsp
ouse
n=
8)
Stru
cture
din
terv
iew
adm
inis
tere
don
2occ
asio
ns
GH
Q-1
2
GH
Qm
edia
nsc
ore
sw
ere
11.0
0(1
2.3
–8.8
range)
and
9.0
0(r
ange
11.0
–0.0
)
indic
atin
gpoor
gen
eral
hea
lth
(44).
Are
lationsh
ipw
asfo
und
bet
wee
nG
HQ
-12
and
care
ras
sess
men
tof
PwM
S.
Test
edth
eva
lidity
and
reli-
abili
tyof
the
GH
Q
Khan
etal
.2006
(14)
Aust
ralia
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
69;
resp
onse
rate
90%
)
Car
egiv
erst
rain
index
(CSI
)
Car
erper
ceiv
edburd
en,
usi
ng
the
visu
alan
alogue
scal
e(V
AS)
score
din
mm
along
a10-c
mlin
e
Tren
dof
more
care
rst
rain
with
incr
easi
ng
dis
abili
tyof
the
PwM
SSi
gnifi
cantly
incr
ease
dper
ceiv
edca
rer
burd
enw
ith
incr
easi
ng
dis
abili
tyof
the
PwM
S
(p<
0.0
1)
Khan
etal
.2007
(20)
Aust
ralia
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
62,re
sponse
rate
89%
;sp
ouse
n=
44,
nonsp
ouse
n=
18)
Stru
cture
din
terv
iew
Car
egiv
erst
rain
index
(CSI
)to
tals
core
(Robin
son
1983).
CSI
rating
score
(O’B
rien
,1993)
Car
egiv
erse
lf-r
eport
edburd
en(S
RB).
Ass
essm
ent
of
qual
ity
of
life
(AQ
oL)
ques
tionnai
re.
12-ite
mm
odifi
edve
rsio
nof
the
gen
eral
self
effica
cysc
ale
ques
tionnai
re(G
SES)
39
(62%
)ca
rers
indic
ated
pre
fere
nce
for
incr
ease
inre
spite
serv
ices
espec
ially
hom
e-bas
edse
rvic
es.26
(42%
)ca
rers
had
score
s‡7
,in
dic
atin
gca
rer
stra
in.M
ost
care
rst
rain
rela
ted
toem
otional
adju
stm
ent
(59%
),oth
erdem
ands
on
care
rtim
e
(n=
53%
),ch
ange
inca
rer
per
sonal
pla
ns
(53%
),an
ddis
turb
edsl
eep
(51%
).
Car
ers
rate
dem
otional
adju
stm
ents
(24%
)an
dfa
mily
adju
stm
ents
ow
ing
todis
-
rupte
dro
utine
(19%
)as
causi
ng
seve
rest
rain
.
Stra
ined
care
rsw
ere
caring
for
the
PwM
Sw
ith
hig
her
leve
lsof
dep
ress
ion,an
xiet
y
and
stre
ss.
Ther
ew
asa
signifi
cant
corr
elat
ion
bet
wee
nst
ress
,an
xiet
yan
d
dep
ress
ion
inth
ePw
MS
and
the
CSI
rating
score
san
dca
rer
SRB.
Stra
ined
care
rs
had
signifi
cantly
wors
esc
ore
son
the
AQ
OL
soci
alre
lationsh
ips
scal
e,an
dw
ere
care
rsof
the
PwM
Sw
ith
wors
esc
ore
son
the
AQ
oL
scal
esfo
rin
dep
enden
tliv
ing,
psy
cholo
gic
alw
ellbei
ng
and
tota
lA
QO
Lsc
ore
s.
No
rela
tionsh
ipw
asfo
und
bet
wee
nca
rer
stra
inan
dca
rer
or
the
PwM
Sse
lf-
effica
cysc
ore
s.
Aca
rer
was
defi
ned
asa
per
-
son
who
lives
with
the
PwM
San
dpro
vides
them
‘with
the
most
care
and
assi
stan
ce’
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
572 M. Corry, A. While
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
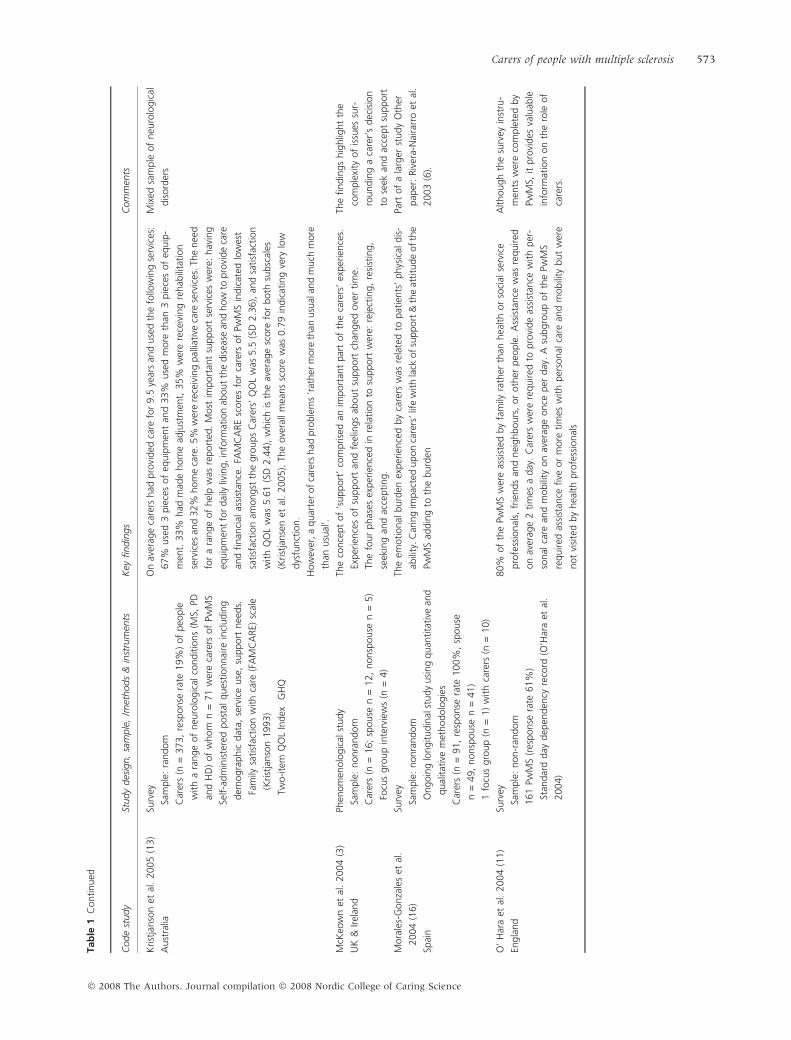
Krist
janso
net
al.
2005
(13)
Aust
ralia
Surv
ey
Sam
ple
:ra
ndom
Car
ers
(n=
373,
resp
onse
rate
19%
)of
peo
ple
with
ara
nge
of
neu
rolo
gic
alco
nditio
ns
(MS,
PD
and
HD
)of
whom
n=
71
wer
eca
rers
of
PwM
S
Self-a
dm
inis
tere
dpost
alques
tionnai
rein
cludin
g
dem
ogra
phic
dat
a,se
rvic
euse
,su
pport
nee
ds.
Fam
ilysa
tisf
action
with
care
(FA
MC
ARE)
scal
e
(Krist
janso
n1993)
Two-ite
mQ
OL
Index
GH
Q
On
aver
age
care
rshad
pro
vided
care
for
9.5
year
san
duse
dth
efo
llow
ing
serv
ices
:
67%
use
d3
pie
ces
of
equip
men
tan
d33%
use
dm
ore
than
3pie
ces
of
equip
-
men
t.33%
had
mad
ehom
ead
just
men
t,35%
wer
ere
ceiv
ing
rehab
ilita
tion
serv
ices
and
32%
hom
eca
re.5%
wer
ere
ceiv
ing
pal
liative
care
serv
ices
.Th
enee
d
for
ara
nge
of
hel
pw
asre
port
ed.
Most
import
ant
support
serv
ices
wer
e:hav
ing
equip
men
tfo
rdai
lyliv
ing,in
form
atio
nab
out
the
dis
ease
and
how
topro
vide
care
and
finan
cial
assi
stan
ce.
FAM
CA
RE
score
sfo
rca
rers
of
PwM
Sin
dic
ated
low
est
satisf
action
amongst
the
gro
ups
Car
ers’
QO
Lw
as5.5
(SD
2.3
6),
and
satisf
action
with
QO
Lw
as5.6
1(S
D2.4
4),
whic
his
the
aver
age
score
for
both
subsc
ales
(Krist
janse
net
al.
2005).
The
ove
rall
mea
ns
score
was
0.7
9in
dic
atin
gve
rylo
w
dys
funct
ion.
How
ever
,a
quar
ter
of
care
rshad
pro
ble
ms
‘rat
her
more
than
usu
alan
dm
uch
more
than
usu
al’.
Mix
edsa
mple
of
neu
rolo
gic
al
dis
ord
ers
McK
eow
net
al.
2004
(3)
UK
&Irel
and
Phen
om
enolo
gic
alst
udy
Sam
ple
:nonra
ndom
Car
ers
(n=
16;
spouse
n=
12,
nonsp
ouse
n=
5)
Focu
sgro
up
inte
rvie
ws
(n=
4)
The
conce
pt
of
‘support
’co
mprise
dan
import
ant
par
tof
the
care
rs’
exper
ience
s.
Exper
ience
sof
support
and
feel
ings
about
support
chan
ged
ove
rtim
e.
The
four
phas
esex
per
ience
din
rela
tion
tosu
pport
wer
e:re
ject
ing,
resi
stin
g,
seek
ing
and
acce
pting.
The
findin
gs
hig
hlig
ht
the
com
ple
xity
of
issu
essu
r-
roundin
ga
care
r’s
dec
isio
n
tose
ekan
dac
cept
support
Mora
les-
Gonza
les
etal
.
2004
(16)
Spai
n
Surv
ey
Sam
ple
:nonra
ndom
Ongoin
glo
ngitudin
alst
udy
usi
ng
quan
tita
tive
and
qual
itat
ive
met
hodolo
gie
s
Car
ers
(n=
91,
resp
onse
rate
100%
,sp
ouse
n=
49,
nonsp
ouse
n=
41)
1fo
cus
gro
up
(n=
1)
with
care
rs(n
=10)
The
emotional
burd
enex
per
ience
dby
care
rsw
asre
late
dto
pat
ients
’phys
ical
dis
-
abili
ty.C
arin
gim
pac
ted
upon
care
rs’lif
ew
ith
lack
of
support
&th
eat
titu
de
of
the
PwM
Sad
din
gto
the
burd
en
Part
of
ala
rger
study
Oth
er
pap
er:
Riv
era-
Nai
rarr
oet
al.
2003
(6).
O’
Har
aet
al.
2004
(11)
Engla
nd
Surv
ey
Sam
ple
:non-r
andom
161
PwM
S(r
esponse
rate
61%
)
Stan
dar
dday
dep
enden
cyre
cord
(O’H
ara
etal
.
2004)
80%
of
the
PwM
Sw
ere
assi
sted
by
fam
ilyra
ther
than
hea
lth
or
soci
alse
rvic
e
pro
fess
ional
s,fr
iends
and
nei
ghbours
,or
oth
erpeo
ple
.A
ssis
tance
was
required
on
aver
age
2tim
esa
day
.C
arer
sw
ere
required
topro
vide
assi
stan
cew
ith
per
-
sonal
care
and
mobili
tyon
aver
age
once
per
day
.A
subgro
up
of
the
PwM
S
required
assi
stan
cefive
or
more
tim
esw
ith
per
sonal
care
and
mobili
tybut
wer
e
not
visi
ted
by
hea
lth
pro
fess
ional
s
Although
the
surv
eyin
stru
-
men
tsw
ere
com
ple
ted
by
PwM
S,it
pro
vides
valu
able
info
rmat
ion
on
the
role
of
care
rs.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 573
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
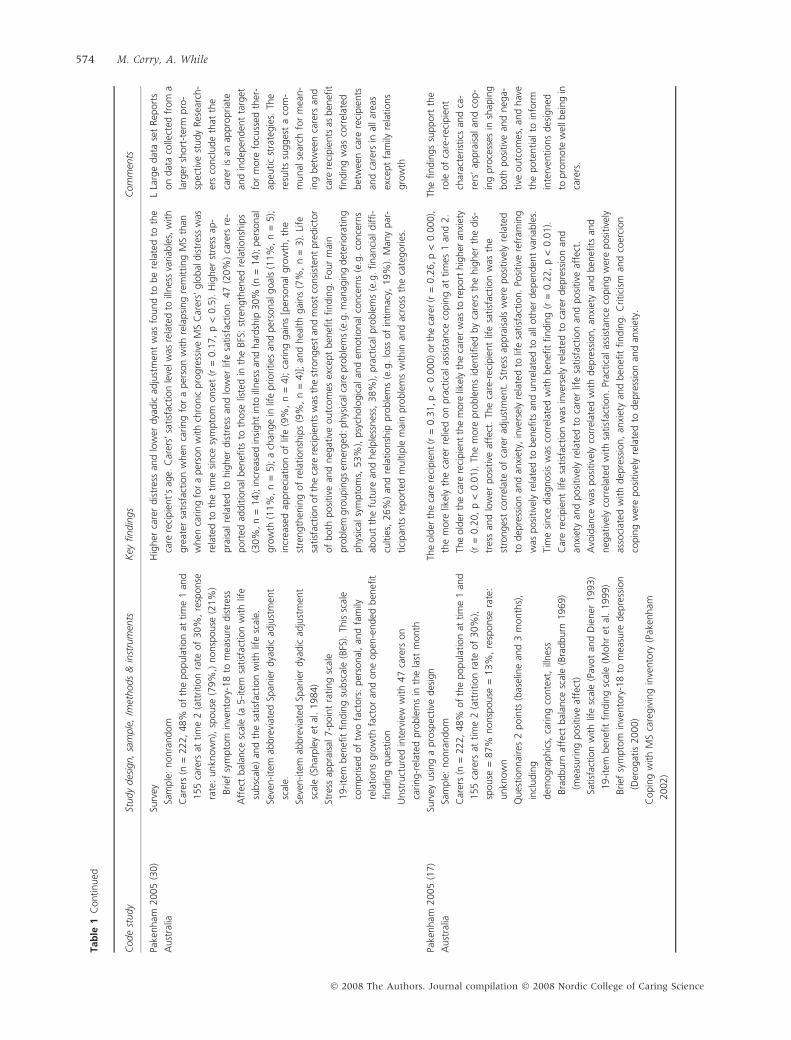
Pake
nham
2005
(30)
Aust
ralia
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
222,
48%
of
the
popula
tion
attim
e1
and
155
care
rsat
tim
e2
(att
rition
rate
of
30%
,re
sponse
rate
:unkn
ow
n),
spouse
(79%
,)nonsp
ouse
(21%
)
Brief
sym
pto
min
vento
ry-1
8to
mea
sure
dis
tres
s
Aff
ect
bal
ance
scal
e(a
5-ite
msa
tisf
action
with
life
subsc
ale)
and
the
satisf
action
with
life
scal
e.
Seve
n-ite
mab
bre
viat
edSp
anie
rdya
dic
adju
stm
ent
scal
e.
Seve
n-ite
mab
bre
viat
edSp
anie
rdya
dic
adju
stm
ent
scal
e(S
har
ple
yet
al.
1984)
Stre
ssap
pra
isal
7-p
oin
tra
ting
scal
e
19-ite
mben
efit
findin
gsu
bsc
ale
(BFS
).Th
issc
ale
com
prise
dof
two
fact
ors
:per
sonal
,an
dfa
mily
rela
tions
gro
wth
fact
or
and
one
open
-ended
ben
efit
findin
gques
tion
Unst
ruct
ure
din
terv
iew
with
47
care
rson
caring-r
elat
edpro
ble
ms
inth
ela
stm
onth
Hig
her
care
rdis
tres
san
dlo
wer
dya
dic
adju
stm
ent
was
found
tobe
rela
ted
toth
e
care
reci
pie
nt’
sag
e.C
arer
s’sa
tisf
action
leve
lwas
rela
ted
toill
nes
sva
riab
les,
with
gre
ater
satisf
action
when
caring
for
aper
son
with
rela
psi
ng
rem
itting
MS
than
when
caring
for
aper
son
with
chro
nic
pro
gre
ssiv
eM
SC
arer
s’glo
bal
dis
tres
sw
as
rela
ted
toth
etim
esi
nce
sym
pto
monse
t(r
=0.1
7,
p<
0.5
).H
igher
stre
ssap
-
pra
isal
rela
ted
tohig
her
dis
tres
san
dlo
wer
life
satisf
action.
47
(20%
)ca
rers
re-
port
edad
ditio
nal
ben
efits
toth
ose
liste
din
the
BFS
:st
rength
ened
rela
tionsh
ips
(30%
,n
=14);
incr
ease
din
sight
into
illnes
san
dhar
dsh
ip30%
(n=
14);
per
sonal
gro
wth
(11%
,n
=5);
ach
ange
inlif
epriorities
and
per
sonal
goal
s(1
1%
,n
=5);
incr
ease
dap
pre
ciat
ion
of
life
(9%
,n
=4);
caring
gai
ns
[per
sonal
gro
wth
,th
e
stre
ngth
enin
gof
rela
tionsh
ips
(9%
,n
=4)]
;an
dhea
lth
gai
ns
(7%
,n
=3).
Life
satisf
action
of
the
care
reci
pie
nts
was
the
stro
nges
tan
dm
ost
consi
sten
tpre
dic
tor
of
both
posi
tive
and
neg
ativ
eoutc
om
esex
cept
ben
efit
findin
g.
Four
mai
n
pro
ble
mgro
upin
gs
emer
ged
:phys
ical
care
pro
ble
ms
(e.g
.m
anag
ing
det
erio
rating
phys
ical
sym
pto
ms,
53%
),psy
cholo
gic
alan
dem
otional
conce
rns
(e.g
.co
nce
rns
about
the
futu
rean
dhel
ple
ssnes
s,38%
),pra
ctic
alpro
ble
ms
(e.g
.finan
cial
diffi-
cultie
s,26%
)an
dre
lationsh
ippro
ble
ms
(e.g
.lo
ssof
intim
acy,
19%
).M
any
par
-
tici
pan
tsre
port
edm
ultip
lem
ain
pro
ble
ms
within
and
acro
ssth
eca
tegories
.
LLa
rge
dat
ase
tRep
ort
s
on
dat
aco
llect
edfr
om
a
larg
ersh
ort
-ter
mpro
-
spec
tive
study
Res
earc
h-
ers
concl
ude
that
the
care
ris
anap
pro
priat
e
and
indep
enden
tta
rget
for
more
focu
ssed
ther
-
apeu
tic
stra
tegie
s.Th
e
resu
lts
sugges
ta
com
-
munal
sear
chfo
rm
ean-
ing
bet
wee
nca
rers
and
care
reci
pie
nts
asben
efit
findin
gw
asco
rrel
ated
bet
wee
nca
rere
cipie
nts
and
care
rsin
allar
eas
exce
pt
fam
ilyre
lations
gro
wth
Pake
nham
2005
(17)
Aust
ralia
Surv
eyusi
ng
apro
spec
tive
des
ign
Sam
ple
:nonra
ndom
Car
ers
(n=
222,
48%
of
the
popula
tion
attim
e1
and
155
care
rsat
tim
e2
(att
rition
rate
of
30%
),
spouse
=87%
nonsp
ouse
=13%
,re
sponse
rate
:
unkn
ow
n
Ques
tionnai
res
2poin
ts(b
asel
ine
and
3m
onth
s),
incl
udin
g
dem
ogra
phic
s,ca
ring
conte
xt,
illnes
s
Bra
dburn
affe
ctbal
ance
scal
e(B
radburn
1969)
(mea
suring
posi
tive
affe
ct)
Satisf
action
with
life
scal
e(P
avot
and
Die
ner
1993)
19-ite
mben
efit
findin
gsc
ale
(Mohr
etal
.1999)
Brief
sym
pto
min
vento
ry-1
8to
mea
sure
dep
ress
ion
(Der
ogat
is2000)
Copin
gw
ith
MS
care
giv
ing
inve
nto
ry(P
aken
ham
2002)
The
old
erth
eca
rere
cipie
nt
(r=
0.3
1,p
<0.0
00)or
the
care
r(r
=0.2
6,p
<0.0
00),
the
more
likel
yth
eca
rer
relie
don
pra
ctic
alas
sist
ance
copin
gat
tim
es1
and
2.
The
old
erth
eca
rere
cipie
nt
the
more
likel
yth
eca
rer
was
tore
port
hig
her
anxi
ety
(r=
0.2
0,
p<
0.0
1).
The
more
pro
ble
ms
iden
tified
by
care
rsth
ehig
her
the
dis
-
tres
san
dlo
wer
posi
tive
affe
ct.
The
care
-rec
ipie
nt
life
satisf
action
was
the
stro
nges
tco
rrel
ate
of
care
rad
just
men
t.St
ress
appra
isal
sw
ere
posi
tive
lyre
late
d
todep
ress
ion
and
anxi
ety,
inve
rsel
yre
late
dto
life
satisf
action.
Posi
tive
refr
amin
g
was
posi
tive
lyre
late
dto
ben
efits
and
unre
late
dto
alloth
erdep
enden
tva
riab
les.
Tim
esi
nce
dia
gnosi
sw
asco
rrel
ated
with
ben
efit
findin
g(r
=0.2
2,
p<
0.0
1).
Car
ere
cipie
nt
life
satisf
action
was
inve
rsel
yre
late
dto
care
rdep
ress
ion
and
anxi
ety
and
posi
tive
lyre
late
dto
care
rlif
esa
tisf
action
and
posi
tive
affe
ct.
Avo
idan
cew
asposi
tive
lyco
rrel
ated
with
dep
ress
ion,
anxi
ety
and
ben
efits
and
neg
ativ
ely
corr
elat
edw
ith
satisf
action.
Prac
tica
las
sist
ance
copin
gw
ere
posi
tive
ly
asso
ciat
edw
ith
dep
ress
ion,
anxi
ety
and
ben
efit
findin
g.
Critici
sman
dco
erci
on
copin
gw
ere
posi
tive
lyre
late
dto
dep
ress
ion
and
anxi
ety.
The
findin
gs
support
the
role
of
care
-rec
ipie
nt
char
acte
rist
ics
and
ca-
rers
’ap
pra
isal
and
cop-
ing
pro
cess
esin
shap
ing
both
posi
tive
and
neg
a-
tive
outc
om
es,
and
hav
e
the
pote
ntial
toin
form
inte
rven
tions
des
igned
topro
mote
wel
lbei
ng
in
care
rs.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
574 M. Corry, A. While
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
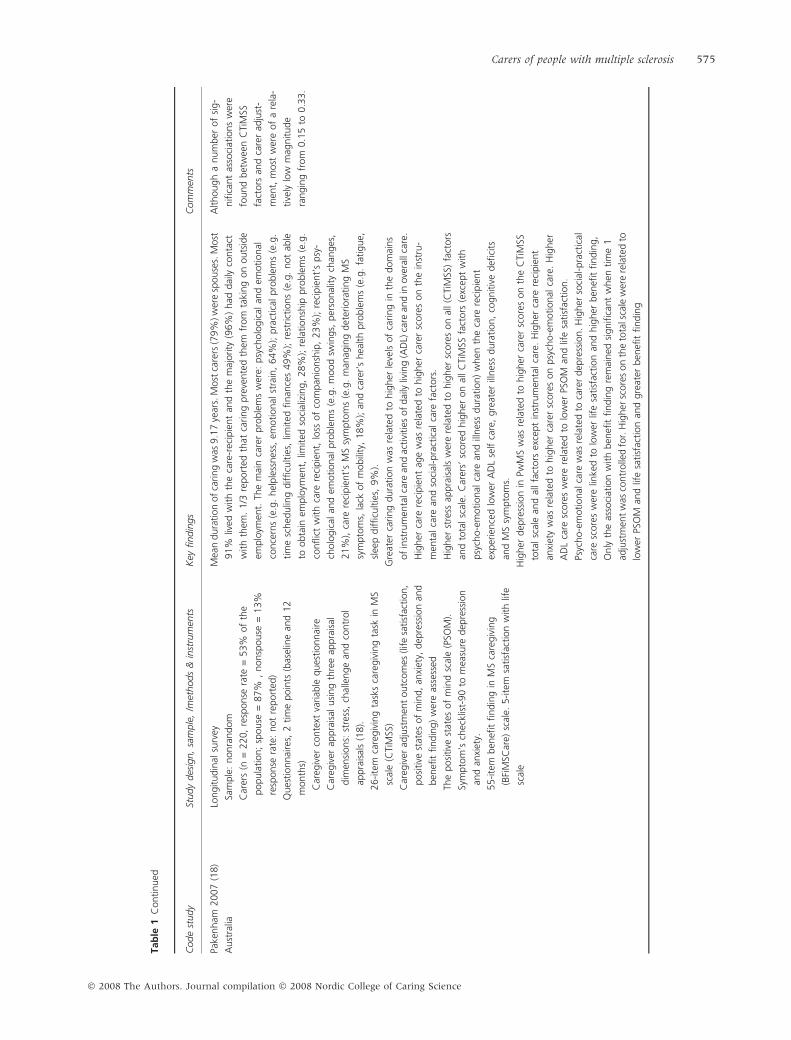
Pake
nham
2007
(18)
Aust
ralia
Longitudin
alsu
rvey
Sam
ple
:nonra
ndom
Car
ers
(n=
220,
resp
onse
rate
=53%
of
the
popula
tion;
spouse
=87%
,nonsp
ouse
=13%
resp
onse
rate
:not
report
ed)
Ques
tionnai
res,
2tim
epoin
ts(b
asel
ine
and
12
month
s)
Car
egiv
erco
nte
xtva
riab
leques
tionnai
re
Car
egiv
erap
pra
isal
usi
ng
thre
eap
pra
isal
dim
ensi
ons:
stre
ss,
chal
lenge
and
contr
ol
appra
isal
s(1
8).
26-ite
mca
regiv
ing
task
sca
regiv
ing
task
inM
S
scal
e(C
TiM
SS)
Car
egiv
erad
just
men
toutc
om
es(li
fesa
tisf
action,
posi
tive
stat
esof
min
d,
anxi
ety,
dep
ress
ion
and
ben
efit
findin
g)
wer
eas
sess
ed
The
posi
tive
stat
esof
min
dsc
ale
(PSO
M).
Sym
pto
m’s
chec
klis
t-90
tom
easu
redep
ress
ion
and
anxi
ety.
55-ite
mben
efit
findin
gin
MS
care
giv
ing
(BFi
MSC
are)
scal
e.5-ite
msa
tisf
action
with
life
scal
e
Mea
ndura
tion
of
caring
was
9.1
7ye
ars.
Most
care
rs(7
9%
)w
ere
spouse
s.M
ost
91%
lived
with
the
care
-rec
ipie
nt
and
the
maj
ority
(96%
)had
dai
lyco
nta
ct
with
them
.1/3
report
edth
atca
ring
pre
vente
dth
emfr
om
taki
ng
on
outs
ide
emplo
ymen
t.Th
em
ain
care
rpro
ble
ms
wer
e:psy
cholo
gic
alan
dem
otional
conce
rns
(e.g
.hel
ple
ssnes
s,em
otional
stra
in,
64%
);pra
ctic
alpro
ble
ms
(e.g
.
tim
esc
hed
ulin
gdifficu
ltie
s,lim
ited
finan
ces
49%
);re
strict
ions
(e.g
.not
able
toobta
inem
plo
ymen
t,lim
ited
soci
aliz
ing,
28%
);re
lationsh
ippro
ble
ms
(e.g
.
conflic
tw
ith
care
reci
pie
nt,
loss
of
com
pan
ionsh
ip,
23%
);re
cipie
nt’
spsy
-
cholo
gic
alan
dem
otional
pro
ble
ms
(e.g
.m
ood
swin
gs,
per
sonal
ity
chan
ges
,
21%
),ca
rere
cipie
nt’
sM
Ssy
mpto
ms
(e.g
.m
anag
ing
det
erio
rating
MS
sym
pto
ms,
lack
of
mobili
ty,
18%
);an
dca
rer’
shea
lth
pro
ble
ms
(e.g
.fa
tigue,
slee
pdifficu
ltie
s,9%
).
Gre
ater
caring
dura
tion
was
rela
ted
tohig
her
leve
lsof
caring
inth
edom
ains
of
inst
rum
enta
lcar
ean
dac
tivi
ties
of
dai
lyliv
ing
(AD
L)ca
rean
din
ove
rall
care
.
Hig
her
care
reci
pie
nt
age
was
rela
ted
tohig
her
care
rsc
ore
son
the
inst
ru-
men
talca
rean
dso
cial
-pra
ctic
alca
refa
ctors
.
Hig
her
stre
ssap
pra
isal
sw
ere
rela
ted
tohig
her
score
son
all(C
TiM
SS)
fact
ors
and
tota
lsc
ale.
Car
ers’
score
dhig
her
on
allC
TiM
SSfa
ctors
(exc
ept
with
psy
cho-e
motional
care
and
illnes
sdura
tion)
when
the
care
reci
pie
nt
exper
ience
dlo
wer
AD
Lse
lfca
re,
gre
ater
illnes
sdura
tion,
cognitiv
edefi
cits
and
MS
sym
pto
ms.
Hig
her
dep
ress
ion
inPw
MS
was
rela
ted
tohig
her
care
rsc
ore
son
the
CTi
MSS
tota
lsc
ale
and
allfa
ctors
exce
pt
inst
rum
enta
lca
re.
Hig
her
care
reci
pie
nt
anxi
ety
was
rela
ted
tohig
her
care
rsc
ore
son
psy
cho-e
motional
care
.H
igher
AD
Lca
resc
ore
sw
ere
rela
ted
tolo
wer
PSO
Man
dlif
esa
tisf
action.
Psyc
ho-e
motional
care
was
rela
ted
toca
rer
dep
ress
ion.
Hig
her
soci
al-p
ract
ical
care
score
sw
ere
linke
dto
low
erlif
esa
tisf
action
and
hig
her
ben
efit
findin
g,
Only
the
asso
ciat
ion
with
ben
efit
findin
gre
mai
ned
signifi
cant
when
tim
e1
adju
stm
ent
was
contr
olle
dfo
r.H
igher
score
son
the
tota
lsca
lew
ere
rela
ted
to
low
erPS
OM
and
life
satisf
action
and
gre
ater
ben
efit
findin
g
Although
anum
ber
of
sig-
nifi
cant
asso
ciat
ions
wer
e
found
bet
wee
nC
TiM
SS
fact
ors
and
care
rad
just
-
men
t,m
ost
wer
eof
are
la-
tive
lylo
wm
agnitude
rangin
gfr
om
0.1
5to
0.3
3.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 575
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
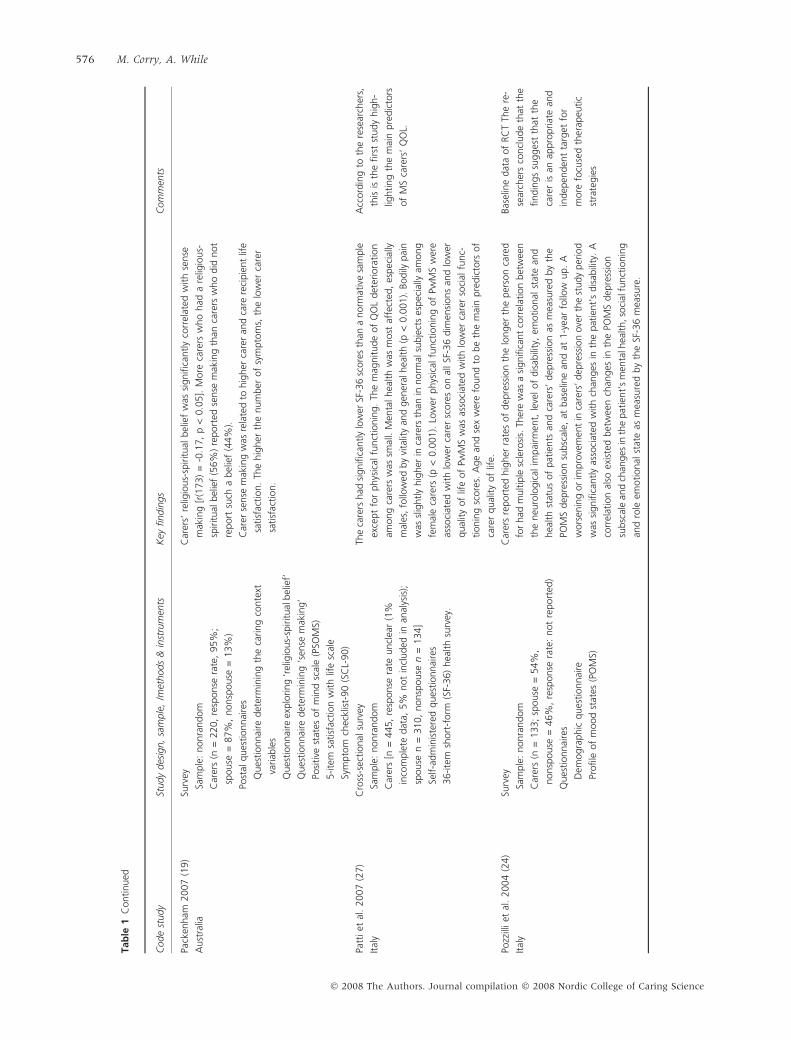
Pack
enham
2007
(19)
Aust
ralia
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
220,
resp
onse
rate
,95%
;
spouse
=87%
,nonsp
ouse
=13%
)
Post
alques
tionnai
res
Ques
tionnai
redet
erm
inin
gth
eca
ring
conte
xt
variab
les
Ques
tionnai
reex
plo
ring
‘rel
igio
us-
spiritual
bel
ief’
Ques
tionnai
redet
erm
inin
g‘s
ense
mak
ing’
Posi
tive
stat
esof
min
dsc
ale
(PSO
MS)
5-ite
msa
tisf
action
with
life
scal
e
Sym
pto
mch
eckl
ist-
90
(SC
L-90)
Car
ers’
relig
ious-
spiritual
bel
ief
was
signifi
cantly
corr
elat
edw
ith
sense
mak
ing
[r(1
73)
=-0
.17,
p<
0.0
5].
More
care
rsw
ho
had
are
ligio
us-
spiritual
bel
ief
(56%
)re
port
edse
nse
mak
ing
than
care
rsw
ho
did
not
report
such
abel
ief
(44%
).
Car
erse
nse
mak
ing
was
rela
ted
tohig
her
care
ran
dca
rere
cipie
nt
life
satisf
action.
The
hig
her
the
num
ber
of
sym
pto
ms,
the
low
erca
rer
satisf
action.
Patt
iet
al.
2007
(27)
Ital
y
Cro
ss-s
ectional
surv
ey
Sam
ple
:nonra
ndom
Car
ers
[n=
445,
resp
onse
rate
uncl
ear
(1%
inco
mple
tedat
a,5%
not
incl
uded
inan
alys
is);
spouse
n=
310,
nonsp
ouse
n=
134]
Self-a
dm
inis
tere
dques
tionnai
res
36-ite
msh
ort
-form
(SF-
36)
hea
lth
surv
ey.
The
care
rshad
signifi
cantly
low
erSF
-36
score
sth
ana
norm
ativ
esa
mple
exce
pt
for
phys
ical
funct
ionin
g.
The
mag
nitude
of
QO
Ldet
erio
ration
among
care
rsw
assm
all.
Men
talhea
lth
was
most
affe
cted
,es
pec
ially
mal
es,
follo
wed
by
vita
lity
and
gen
eral
hea
lth
(p<
0.0
01).
Bodily
pai
n
was
slig
htly
hig
her
inca
rers
than
innorm
alsu
bje
cts
espec
ially
among
fem
ale
care
rs(p
<0.0
01).
Low
erphys
ical
funct
ionin
gof
PwM
Sw
ere
asso
ciat
edw
ith
low
erca
rer
score
son
allSF
-36
dim
ensi
ons
and
low
er
qual
ity
of
life
of
PwM
Sw
asas
soci
ated
with
low
erca
rer
soci
alfu
nc-
tionin
gsc
ore
s.A
ge
and
sex
wer
efo
und
tobe
the
mai
npre
dic
tors
of
care
rqual
ity
of
life.
Acc
ord
ing
toth
ere
sear
cher
s,
this
isth
efirs
tst
udy
hig
h-
lighting
the
mai
npre
dic
tors
of
MS
care
rs’
QO
L.
Pozz
illiet
al.
2004
(24)
Ital
y
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
133;
spouse
=54%
,
nonsp
ouse
=46%
,re
sponse
rate
:not
report
ed)
Ques
tionnai
res
Dem
ogra
phic
ques
tionnai
re
Profile
of
mood
stat
es(P
OM
S)
Car
ers
report
edhig
her
rate
sof
dep
ress
ion
the
longer
the
per
son
care
d
for
had
multip
lesc
lero
sis.
Ther
ew
asa
signifi
cant
corr
elat
ion
bet
wee
n
the
neu
rolo
gic
alim
pai
rmen
t,le
velof
dis
abili
ty,
emotional
stat
ean
d
hea
lth
stat
us
of
pat
ients
and
care
rs’
dep
ress
ion
asm
easu
red
by
the
POM
Sdep
ress
ion
subsc
ale,
atbas
elin
ean
dat
1-y
ear
follo
wup.
A
wors
enin
gor
impro
vem
ent
inca
rers
’dep
ress
ion
ove
rth
est
udy
per
iod
was
signifi
cantly
asso
ciat
edw
ith
chan
ges
inth
epat
ient’
sdis
abili
ty.
A
corr
elat
ion
also
exis
ted
bet
wee
nch
anges
inth
ePO
MS
dep
ress
ion
subsc
ale
and
chan
ges
inth
epat
ient’
sm
enta
lhea
lth,so
cial
funct
ionin
g
and
role
emotional
stat
eas
mea
sure
dby
the
SF-3
6m
easu
re.
Bas
elin
edat
aof
RC
TTh
ere
-
sear
cher
sco
ncl
ude
that
the
findin
gs
sugges
tth
atth
e
care
ris
anap
pro
priat
ean
d
indep
enden
tta
rget
for
more
focu
sed
ther
apeu
tic
stra
tegie
s
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
576 M. Corry, A. While
Tab
le1
Continued
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
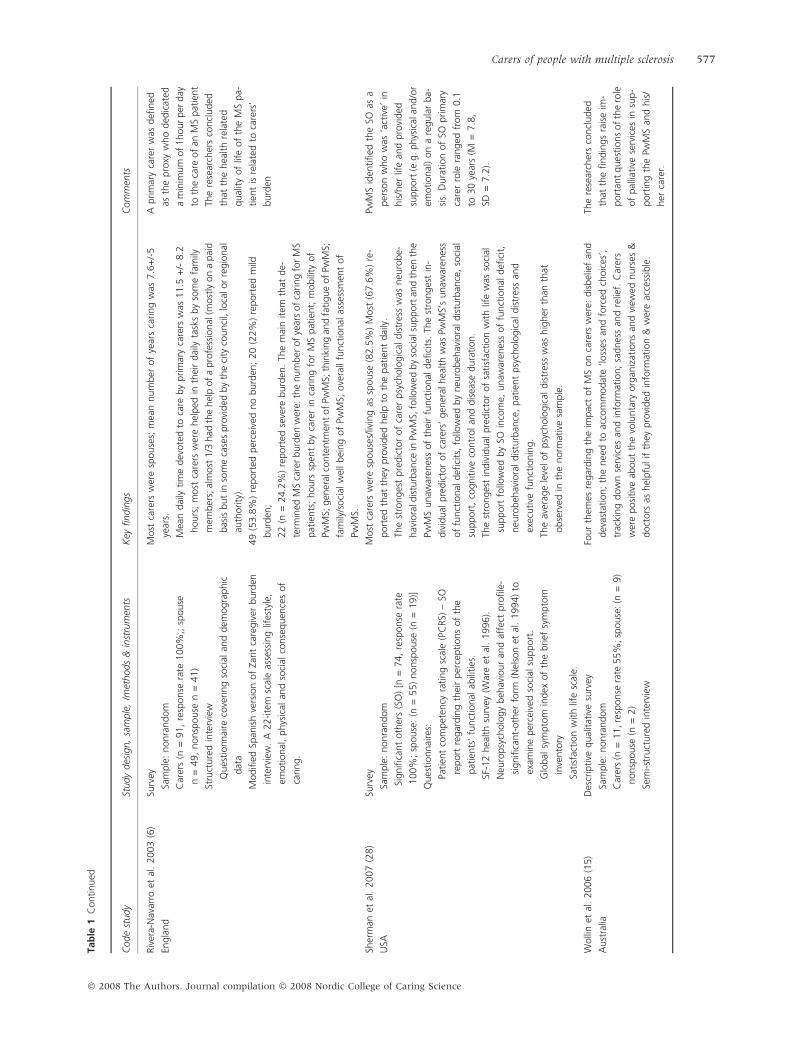
Riv
era-
Nav
arro
etal
.2003
(6)
Engla
nd
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
91,
resp
onse
rate
100%
,;sp
ouse
n=
49,
nonsp
ouse
n=
41)
Stru
cture
din
terv
iew
Ques
tionnai
reco
vering
soci
alan
ddem
ogra
phic
dat
a
Modifi
edSp
anis
hve
rsio
nof
Zarit
care
giv
erburd
en
inte
rvie
w.
A22-ite
msc
ale
asse
ssin
glif
esty
le,
emotional
,phys
ical
and
soci
alco
nse
quen
ces
of
caring.
Most
care
rsw
ere
spouse
s;m
ean
num
ber
of
year
sca
ring
was
7.6
+/-
5
year
s.
Mea
ndai
lytim
edev
ote
dto
care
by
prim
ary
care
rsw
as11.5
+/-
8.2
hours
;m
ost
care
rsw
ere
hel
ped
inth
eir
dai
lyta
sks
by
som
efa
mily
mem
ber
s;al
most
1/3
had
the
hel
pof
apro
fess
ional
(most
lyon
apai
d
bas
isbut
inso
me
case
spro
vided
by
the
city
counci
l,lo
calo
rre
gio
nal
auth
ority
).
49
(53.8
%)
report
edper
ceiv
edno
burd
en;
20
(22%
)re
port
edm
ild
burd
en;
22
(n=
24.2
%)
report
edse
vere
burd
en.
The
mai
nitem
that
de-
term
ined
MS
care
rburd
enw
ere:
the
num
ber
of
year
sof
caring
for
MS
pat
ients
;hours
spen
tby
care
rin
caring
for
MS
pat
ient;
mobili
tyof
PwM
S;gen
eral
conte
ntm
ent
of
PwM
S;th
inki
ng
and
fatigue
of
PwM
S;
fam
ily/s
oci
alw
ellbei
ng
of
PwM
S;ove
rall
funct
ional
asse
ssm
ent
of
PwM
S.
Aprim
ary
care
rw
asdefi
ned
asth
epro
xyw
ho
ded
icat
ed
am
inim
um
of
1hour
per
day
toth
eca
reof
anM
Spat
ient
The
rese
arch
ers
concl
uded
that
the
hea
lth
rela
ted
qual
ity
of
life
of
the
MS
pa-
tien
tis
rela
ted
toca
rers
’
burd
en
Sher
man
etal
.2007
(28)
USA
Surv
ey
Sam
ple
:nonra
ndom
Signifi
cant
oth
ers
(SO
)[n
=74,
resp
onse
rate
100%
;sp
ouse
:(n
=55)
nonsp
ouse
(n=
19)]
Ques
tionnai
res:
Patien
tco
mpet
ency
rating
scal
e(P
CRS)
–SO
report
regar
din
gth
eir
per
ceptions
of
the
pat
ients
’fu
nct
ional
abili
ties
.
SF-1
2hea
lth
surv
ey(W
are
etal
.1996).
Neu
ropsy
cholo
gy
beh
avio
ur
and
affe
ctpro
file
-
signifi
cant-
oth
erfo
rm(N
elso
net
al.
1994)
to
exam
ine
per
ceiv
edso
cial
support
.
Glo
bal
sym
pto
min
dex
of
the
brief
sym
pto
m
inve
nto
ry
Satisf
action
with
life
scal
e.
Most
care
rsw
ere
spouse
s/liv
ing
assp
ouse
(82.5
%)
Most
(67.6
%)
re-
port
edth
atth
eypro
vided
hel
pto
the
pat
ient
dai
ly.
The
stro
nges
tpre
dic
tor
of
care
rpsy
cholo
gic
aldis
tres
sw
asneu
robe-
hav
iora
ldis
turb
ance
inPw
MS,
follo
wed
by
soci
alsu
pport
and
then
the
PwM
Sunaw
aren
ess
of
thei
rfu
nct
ional
defi
cits
.Th
est
ronges
tin
-
div
idual
pre
dic
tor
of
care
rs’
gen
eral
hea
lth
was
PwM
S’s
unaw
aren
ess
of
funct
ional
defi
cits
,fo
llow
edby
neu
robeh
avio
raldis
turb
ance
,so
cial
support
,co
gnitiv
eco
ntr
olan
ddis
ease
dura
tion.
The
stro
nges
tin
div
idual
pre
dic
tor
of
satisf
action
with
life
was
soci
al
support
follo
wed
by
SOin
com
e,unaw
aren
ess
of
funct
ional
defi
cit,
neu
robeh
avio
ral
dis
turb
ance
,pat
ient
psy
cholo
gic
aldis
tres
san
d
exec
utive
funct
ionin
g.
The
aver
age
leve
lof
psy
cholo
gic
aldis
tres
sw
ashig
her
than
that
obse
rved
inth
enorm
ativ
esa
mple
.
PwM
Sid
entified
the
SOas
a
per
son
who
was
‘act
ive’
in
his
/her
life
and
pro
vided
support
(e.g
.phys
ical
and/o
r
emotional
)on
are
gula
rba-
sis.
Dura
tion
of
SOprim
ary
care
rro
lera
nged
from
0.1
to30
year
s(M
=7.8
,
SD=
7.2
).
Wolli
net
al.
2006
(15)
Aust
ralia
Des
crip
tive
qual
itat
ive
surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
11,re
sponse
rate
55%
;sp
ouse
:(n
=9)
nonsp
ouse
(n=
2)
Sem
i-st
ruct
ure
din
terv
iew
Four
them
esre
gar
din
gth
eim
pac
tof
MS
on
care
rsw
ere:
dis
bel
ief
and
dev
asta
tion;
the
nee
dto
acco
mm
odat
e‘lo
sses
and
forc
edch
oic
es’;
trac
king
dow
nse
rvic
esan
din
form
atio
n;
sadnes
san
dre
lief.
Car
ers
wer
eposi
tive
about
the
volu
nta
ryorg
aniz
atio
ns
and
view
ednurs
es&
doct
ors
ashel
pfu
lif
they
pro
vided
info
rmat
ion
&w
ere
acce
ssib
le.
The
rese
arch
ers
concl
uded
that
the
findin
gs
rais
eim
-
port
ant
ques
tions
of
the
role
of
pal
liative
serv
ices
insu
p-
port
ing
the
PwM
San
dhis
/
her
care
r.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 577
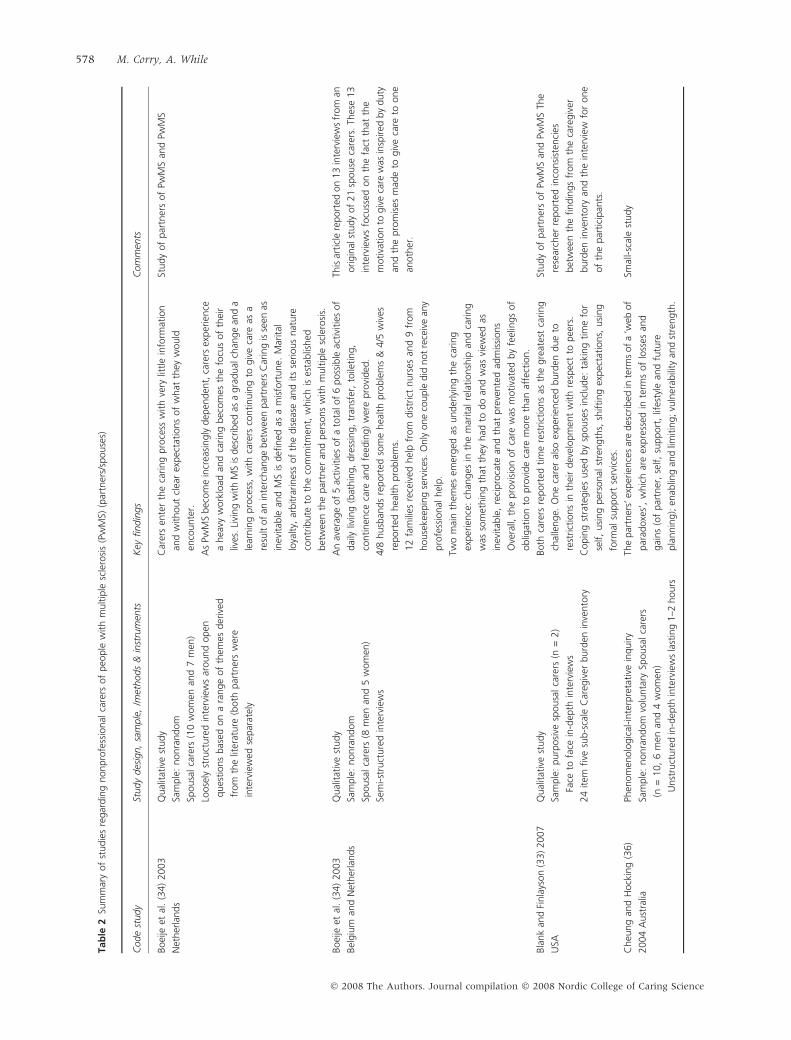
Tab
le2
Sum
mar
yof
studie
sre
gar
din
gnonpro
fess
ional
care
rsof
peo
ple
with
multip
lesc
lero
sis
(Pw
MS)
(par
tner
s/sp
ouse
s)
Code
study
Study
des
ign,
sam
ple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Boei
jeet
al.
(34)
2003
Net
her
lands
Qual
itat
ive
study
Sam
ple
:nonra
ndom
Spousa
lca
rers
(10
wom
enan
d7
men
)
Loose
lyst
ruct
ure
din
terv
iew
sar
ound
open
ques
tions
bas
edon
ara
nge
of
them
esder
ived
from
the
liter
ature
(both
par
tner
sw
ere
inte
rvie
wed
separ
atel
y
Car
ers
ente
rth
eca
ring
pro
cess
with
very
little
info
rmat
ion
and
without
clea
rex
pec
tations
of
what
they
would
enco
unte
r.
As
PwM
Sbec
om
ein
crea
singly
dep
enden
t,ca
rers
exper
ience
ahea
vyw
ork
load
and
caring
bec
om
esth
efo
cus
of
thei
r
lives
.Li
ving
with
MS
isdes
crib
edas
agra
dual
chan
ge
and
a
lear
nin
gpro
cess
,w
ith
care
rsco
ntinuin
gto
giv
eca
reas
a
resu
ltof
anin
terc
han
ge
bet
wee
npar
tner
sC
arin
gis
seen
as
inev
itab
lean
dM
Sis
defi
ned
asa
mis
fort
une.
Mar
ital
loya
lty,
arbitra
rines
sof
the
dis
ease
and
its
serious
nat
ure
contr
ibute
toth
eco
mm
itm
ent,
whic
his
esta
blis
hed
bet
wee
nth
epar
tner
and
per
sons
with
multip
lesc
lero
sis.
Study
of
par
tner
sof
PwM
San
dPw
MS
Boei
jeet
al.
(34)
2003
Bel
giu
man
dN
ether
lands
Qual
itat
ive
study
Sam
ple
:nonra
ndom
Spousa
lca
rers
(8m
enan
d5
wom
en)
Sem
i-st
ruct
ure
din
terv
iew
s
An
aver
age
of
5ac
tivi
ties
of
ato
talof
6poss
ible
activi
ties
of
dai
lyliv
ing
(bat
hin
g,
dre
ssin
g,
tran
sfer
,to
ileting,
continen
ceca
rean
dfe
edin
g)
wer
epro
vided
.
4/8
husb
ands
report
edso
me
hea
lth
pro
ble
ms
&4/5
wiv
es
report
edhea
lth
pro
ble
ms.
12
fam
ilies
rece
ived
hel
pfr
om
dis
tric
tnurs
esan
d9
from
house
keep
ing
serv
ices
.O
nly
one
couple
did
not
rece
ive
any
pro
fess
ional
hel
p.
Two
mai
nth
emes
emer
ged
asunder
lyin
gth
eca
ring
exper
ience
:ch
anges
inth
em
arital
rela
tionsh
ipan
dca
ring
was
som
ethin
gth
atth
eyhad
todo
and
was
view
edas
inev
itab
le,
reci
pro
cate
and
that
pre
vente
dad
mis
sions
Ove
rall,
the
pro
visi
on
of
care
was
motiva
ted
by
feel
ings
of
oblig
atio
nto
pro
vide
care
more
than
affe
ctio
n.
This
articl
ere
port
edon
13
inte
rvie
ws
from
an
origin
alst
udy
of
21
spouse
care
rs.
Thes
e13
inte
rvie
ws
focu
ssed
on
the
fact
that
the
motiva
tion
togiv
eca
rew
asin
spired
by
duty
and
the
pro
mis
esm
ade
togiv
eca
reto
one
anoth
er.
Bla
nk
and
Finla
yson
(33)
2007
USA
Qual
itat
ive
study
Sam
ple
:purp
osi
vesp
ousa
lca
rers
(n=
2)
Face
tofa
cein
-dep
thin
terv
iew
s
24
item
five
sub-s
cale
Car
egiv
erburd
enin
vento
ry
Both
care
rsre
port
edtim
ere
strict
ions
asth
egre
ates
tca
ring
chal
lenge.
One
care
ral
soex
per
ience
dburd
endue
to
rest
rict
ions
inth
eir
dev
elopm
ent
with
resp
ect
topee
rs.
Copin
gst
rate
gie
suse
dby
spouse
sin
clude:
taki
ng
tim
efo
r
self,
usi
ng
per
sonal
stre
ngth
s,sh
ifting
expec
tations,
usi
ng
form
alsu
pport
serv
ices
.
Study
of
par
tner
sof
PwM
San
dPw
MS
The
rese
arch
erre
port
edin
consi
sten
cies
bet
wee
nth
efindin
gs
from
the
care
giv
er
burd
enin
vento
ryan
dth
ein
terv
iew
for
one
of
the
par
tici
pan
ts.
Cheu
ng
and
Hock
ing
(36)
2004
Aust
ralia
Phen
om
enolo
gic
al-inte
rpre
tative
inquiry
Sam
ple
:nonra
ndom
volu
nta
rySp
ousa
lca
rers
(n=
10,
6m
enan
d4
wom
en)
Unst
ruct
ure
din
-dep
thin
terv
iew
sla
stin
g1–2
hours
The
par
tner
s’ex
per
ience
sar
edes
crib
edin
term
sof
a‘w
ebof
par
adoxe
s’,
whic
har
eex
pre
ssed
inte
rms
of
loss
esan
d
gai
ns
(of
par
tner
,se
lf,
support
,lif
esty
lean
dfu
ture
pla
nnin
g);
enab
ling
and
limitin
g;vu
lner
abili
tyan
dst
rength
.
Smal
l-sc
ale
study
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
578 M. Corry, A. While
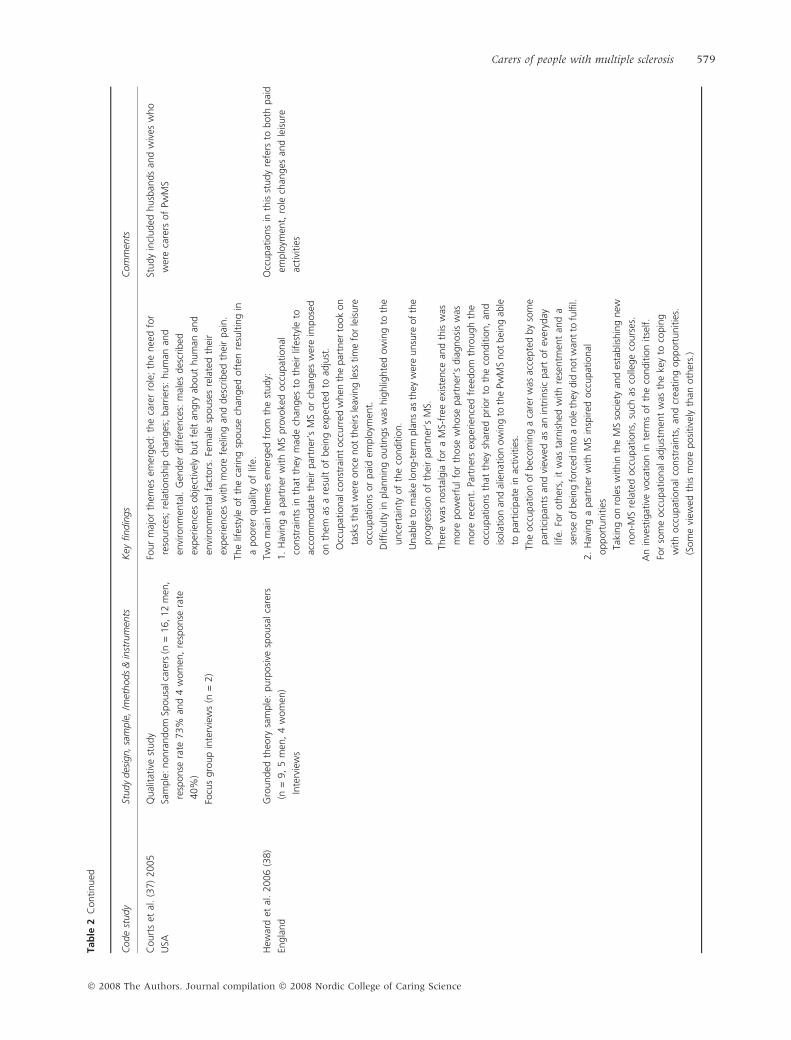
Tab
le2
Continued
Code
study
Study
des
ign,sa
mple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Court
set
al.
(37)
2005
USA
Qual
itat
ive
study
Sam
ple
:nonra
ndom
Spousa
lcar
ers
(n=
16,12
men
,
resp
onse
rate
73%
and
4w
om
en,
resp
onse
rate
40%
)
Focu
sgro
up
inte
rvie
ws
(n=
2)
Four
maj
or
them
esem
erged
:th
eca
rer
role
;th
enee
dfo
r
reso
urc
es;
rela
tionsh
ipch
anges
;bar
rier
s:hum
anan
d
envi
ronm
enta
l.G
ender
diffe
rence
s:m
ales
des
crib
ed
exper
ience
sobje
ctiv
ely
but
felt
angry
about
hum
anan
d
envi
ronm
enta
lfa
ctors
.Fe
mal
esp
ouse
sre
late
dth
eir
exper
ience
sw
ith
more
feel
ing
and
des
crib
edth
eir
pai
n.
The
lifes
tyle
of
the
caring
spouse
chan
ged
oft
enre
sultin
gin
apoore
rqual
ity
of
life.
Study
incl
uded
husb
ands
and
wiv
esw
ho
wer
eca
rers
of
PwM
S
Hew
ard
etal
.2006
(38)
Engla
nd
Gro
unded
theo
rysa
mple
:purp
osi
vesp
ousa
lca
rers
(n=
9,
5m
en,
4w
om
en)
Inte
rvie
ws
Two
mai
nth
emes
emer
ged
from
the
study:
1.
Hav
ing
apar
tner
with
MS
pro
voke
docc
upat
ional
const
rain
tsin
that
they
mad
ech
anges
toth
eir
lifes
tyle
to
acco
mm
odat
eth
eir
par
tner
’sM
Sor
chan
ges
wer
eim
pose
d
on
them
asa
resu
ltof
bei
ng
expec
ted
toad
just
.
Occ
upat
ional
const
rain
tocc
urr
edw
hen
the
par
tner
took
on
task
sth
atw
ere
once
not
thei
rsle
avin
gle
sstim
efo
rle
isure
occ
upat
ions
or
pai
dem
plo
ymen
t.
Difficu
lty
inpla
nnin
goutings
was
hig
hlig
hte
dow
ing
toth
e
unce
rtai
nty
of
the
conditio
n.
Unab
leto
mak
elo
ng-t
erm
pla
ns
asth
eyw
ere
unsu
reof
the
pro
gre
ssio
nof
thei
rpar
tner
’sM
S.
Ther
ew
asnost
algia
for
aM
S-fr
eeex
iste
nce
and
this
was
more
pow
erfu
lfo
rth
ose
whose
par
tner
’sdia
gnosi
sw
as
more
rece
nt.
Part
ner
sex
per
ience
dfr
eedom
thro
ugh
the
occ
upat
ions
that
they
shar
edprior
toth
eco
nditio
n,
and
isola
tion
and
alie
nat
ion
ow
ing
toth
ePw
MS
not
bei
ng
able
topar
tici
pat
ein
activi
ties
.
The
occ
upat
ion
of
bec
om
ing
aca
rer
was
acce
pte
dby
som
e
par
tici
pan
tsan
dvi
ewed
asan
intr
insi
cpar
tof
ever
yday
life.
For
oth
ers,
itw
asta
rnis
hed
with
rese
ntm
ent
and
a
sense
of
bei
ng
forc
edin
toa
role
they
did
not
wan
tto
fulfi
l.
2.
Hav
ing
apar
tner
with
MS
insp
ired
occ
upat
ional
opport
unitie
s
Taki
ng
on
role
sw
ithin
the
MS
soci
ety
and
esta
blis
hin
gnew
non-M
Sre
late
docc
upat
ions,
such
asco
llege
cours
es.
An
inve
stig
ativ
evo
cation
inte
rms
of
the
conditio
nitse
lf.
For
som
eocc
upat
ional
adju
stm
ent
was
the
key
toco
pin
g
with
occ
upat
ional
const
rain
ts,
and
crea
ting
opport
unitie
s.
(Som
evi
ewed
this
more
posi
tive
lyth
anoth
ers.
)
Occ
upat
ions
inth
isst
udy
refe
rsto
both
pai
d
emplo
ymen
t,ro
lech
anges
and
leis
ure
activi
ties
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 579
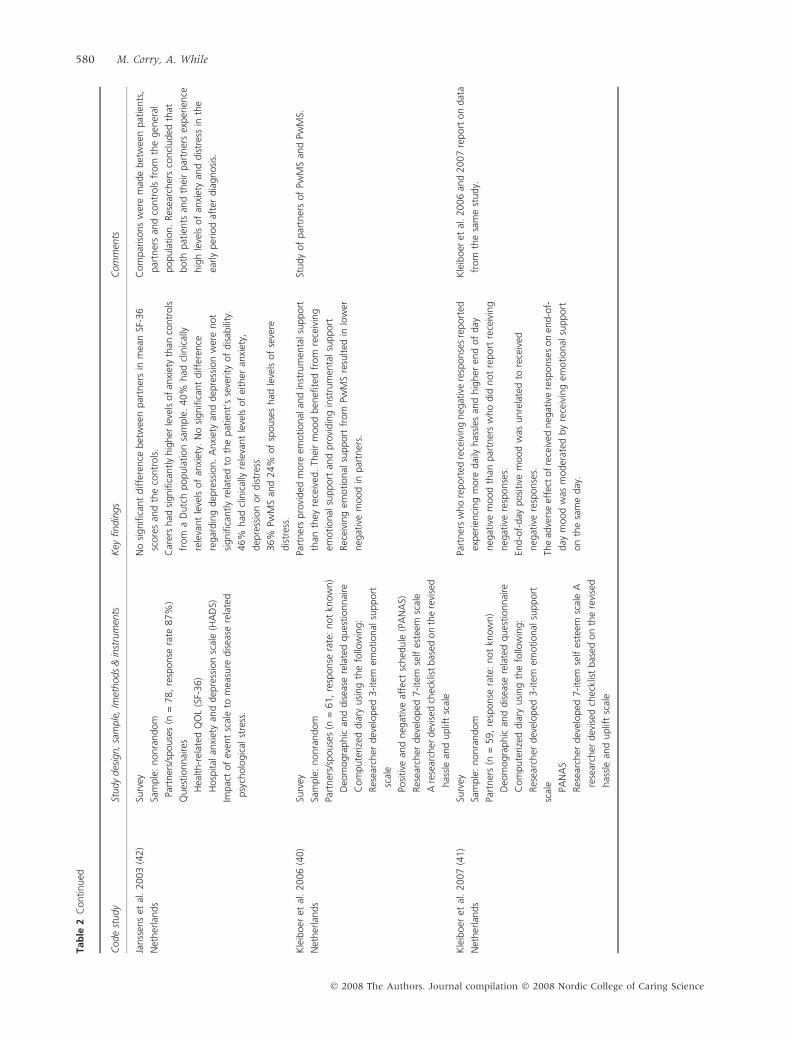
Tab
le2
Continued
Code
study
Study
des
ign,sa
mple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Janss
ens
etal
.2003
(42)
Net
her
lands
Surv
ey
Sam
ple
:nonra
ndom
Part
ner
s/sp
ouse
s(n
=78,
resp
onse
rate
87%
)
Ques
tionnai
res
Hea
lth-r
elat
edQ
OL
(SF-
36)
Hosp
ital
anxi
ety
and
dep
ress
ion
scal
e(H
AD
S)
Impac
tof
even
tsc
ale
tom
easu
redis
ease
rela
ted
psy
cholo
gic
alst
ress
.
No
signifi
cant
diffe
rence
bet
wee
npar
tner
sin
mea
nSF
-36
score
san
dth
eco
ntr
ols
.
Car
ers
had
signifi
cantly
hig
her
leve
lsof
anxi
ety
than
contr
ols
from
aD
utc
hpopula
tion
sam
ple
.40%
had
clin
ical
ly
rele
vant
leve
lsof
anxi
ety.
No
signifi
cant
diffe
rence
regar
din
gdep
ress
ion.
Anxi
ety
and
dep
ress
ion
wer
enot
signifi
cantly
rela
ted
toth
epat
ient’
sse
verity
of
dis
abili
ty.
46%
had
clin
ical
lyre
leva
nt
leve
lsof
eith
eran
xiet
y,
dep
ress
ion
or
dis
tres
s.
36%
PwM
San
d24%
of
spouse
shad
leve
lsof
seve
re
dis
tres
s.
Com
par
isons
wer
em
ade
bet
wee
npat
ients
,
par
tner
san
dco
ntr
ols
from
the
gen
eral
popula
tion.
Res
earc
her
sco
ncl
uded
that
both
pat
ients
and
thei
rpar
tner
sex
per
ience
hig
hle
vels
of
anxi
ety
and
dis
tres
sin
the
early
per
iod
afte
rdia
gnosi
s.
Kle
iboer
etal
.2006
(40)
Net
her
lands
Surv
ey
Sam
ple
:nonra
ndom
Part
ner
s/sp
ouse
s(n
=61,
resp
onse
rate
:not
know
n)
Deo
mogra
phic
and
dis
ease
rela
ted
ques
tionnai
re
Com
pute
rize
ddia
ryusi
ng
the
follo
win
g:
Res
earc
her
dev
eloped
3-ite
mem
otional
support
scal
e
Posi
tive
and
neg
ativ
eaf
fect
sched
ule
(PA
NA
S)
Res
earc
her
dev
eloped
7-ite
mse
lfes
teem
scal
e
Are
sear
cher
dev
ised
chec
klis
tbas
edon
the
revi
sed
has
sle
and
uplif
tsc
ale
Part
ner
spro
vided
more
emotional
and
inst
rum
enta
lsu
pport
than
they
rece
ived
.Th
eir
mood
ben
efite
dfr
om
rece
ivin
g
emotional
support
and
pro
vidin
gin
stru
men
talsu
pport
Rec
eivi
ng
emotional
support
from
PwM
Sre
sulted
inlo
wer
neg
ativ
em
ood
inpar
tner
s.
Study
of
par
tner
sof
PwM
San
dPw
MS.
Kle
iboer
etal
.2007
(41)
Net
her
lands
Surv
ey
Sam
ple
:nonra
ndom
Part
ner
s(n
=59,
resp
onse
rate
:not
know
n)
Deo
mogra
phic
and
dis
ease
rela
ted
ques
tionnai
re
Com
pute
rize
ddia
ryusi
ng
the
follo
win
g:
Res
earc
her
dev
eloped
3-ite
mem
otional
support
scal
e
PAN
AS
Res
earc
her
dev
eloped
7-ite
mse
lfes
teem
scal
eA
rese
arch
erdev
ised
chec
klis
tbas
edon
the
revi
sed
has
sle
and
uplif
tsc
ale
Part
ner
sw
ho
report
edre
ceiv
ing
neg
ativ
ere
sponse
sre
port
ed
exper
ienci
ng
more
dai
lyhas
sles
and
hig
her
end
of
day
neg
ativ
em
ood
than
par
tner
sw
ho
did
not
report
rece
ivin
g
neg
ativ
ere
sponse
s.
End-o
f-day
posi
tive
mood
was
unre
late
dto
rece
ived
neg
ativ
ere
sponse
s.
The
adve
rse
effe
ctof
rece
ived
neg
ativ
ere
sponse
son
end-o
f-
day
mood
was
moder
ated
by
rece
ivin
gem
otional
support
on
the
sam
eday
.
Kle
iboer
etal
.2006
and
2007
report
on
dat
a
from
the
sam
est
udy.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
580 M. Corry, A. While
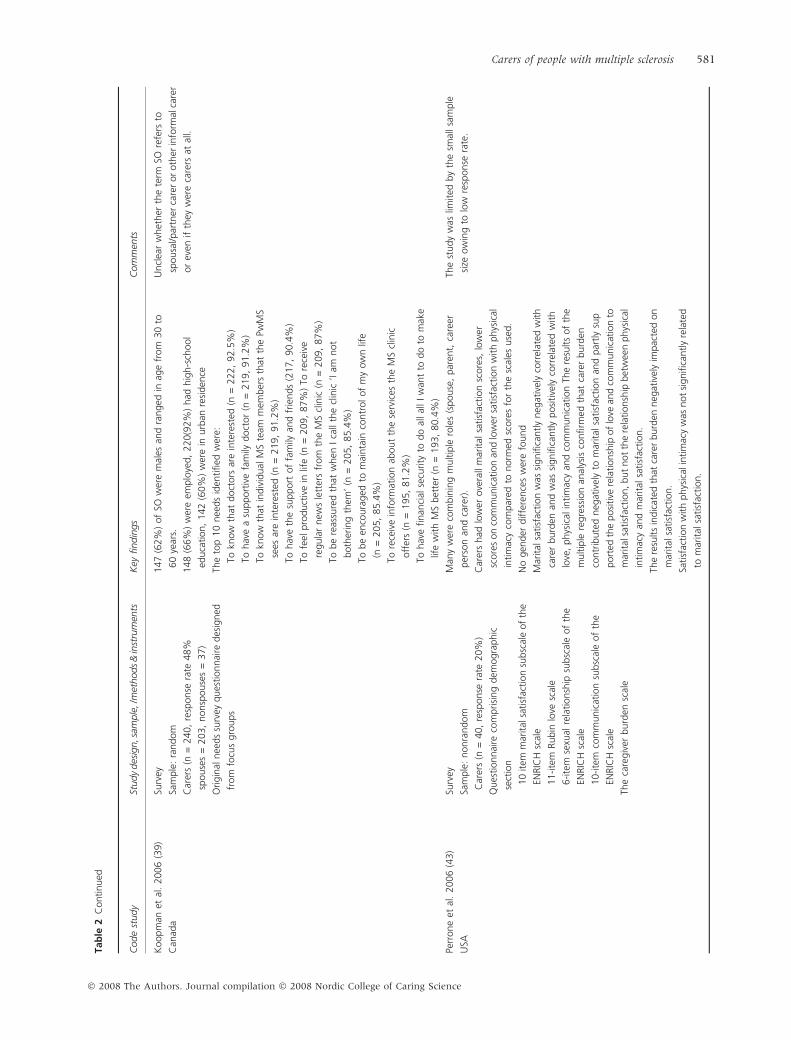
Tab
le2
Continued
Code
study
Study
des
ign,s
ample
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Koopm
anet
al.
2006
(39)
Can
ada
Surv
ey
Sam
ple
:ra
ndom
Car
ers
(n=
240,
resp
onse
rate
48%
spouse
s=
203,
nonsp
ouse
s=
37)
Origin
alnee
ds
surv
eyques
tionnai
redes
igned
from
focu
sgro
ups
147
(62%
)of
SOw
ere
mal
esan
dra
nged
inag
efr
om
30
to
60
year
s.
148
(66%
)w
ere
emplo
yed,
220(9
2%
)had
hig
h-s
chool
educa
tion,
142
(60%
)w
ere
inurb
anre
siden
ce
The
top
10
nee
ds
iden
tified
wer
e:
Tokn
ow
that
doct
ors
are
inte
rest
ed(n
=222,
92.5
%)
Tohav
ea
support
ive
fam
ilydoct
or
(n=
219,
91.2
%)
Tokn
ow
that
indiv
idual
MS
team
mem
ber
sth
atth
ePw
MS
sees
are
inte
rest
ed(n
=219,
91.2
%)
Tohav
eth
esu
pport
of
fam
ilyan
dfr
iends
(217,
90.4
%)
Tofe
elpro
duct
ive
inlif
e(n
=209,
87%
)To
rece
ive
regula
rnew
sle
tter
sfr
om
the
MS
clin
ic(n
=209,
87%
)
Tobe
reas
sure
dth
atw
hen
Ica
llth
ecl
inic
‘Iam
not
both
erin
gth
em’
(n=
205,
85.4
%)
Tobe
enco
ura
ged
tom
ainta
inco
ntr
ol
of
my
ow
nlif
e
(n=
205,
85.4
%)
Tore
ceiv
ein
form
atio
nab
out
the
serv
ices
the
MS
clin
ic
off
ers
(n=
195,
81.2
%)
Tohav
efinan
cial
secu
rity
todo
allal
lIw
ant
todo
tom
ake
life
with
MS
bet
ter
(n=
193,
80.4
%)
Uncl
ear
whet
her
the
term
SOre
fers
to
spousa
l/par
tner
care
ror
oth
erin
form
alca
rer
or
even
ifth
eyw
ere
care
rsat
all.
Perr
one
etal
.2006
(43)
USA
Surv
ey
Sam
ple
:nonra
ndom
Car
ers
(n=
40,
resp
onse
rate
20%
)
Ques
tionnai
reco
mprisi
ng
dem
ogra
phic
sect
ion
10
item
mar
ital
satisf
action
subsc
ale
of
the
ENRIC
Hsc
ale
11-ite
mRubin
love
scal
e
6-ite
mse
xual
rela
tionsh
ipsu
bsc
ale
of
the
ENRIC
Hsc
ale
10-ite
mco
mm
unic
atio
nsu
bsc
ale
of
the
ENRIC
Hsc
ale
The
care
giv
erburd
ensc
ale
Man
yw
ere
com
bin
ing
multip
lero
les
(spouse
,par
ent,
care
er
per
son
and
care
r).
Car
ers
had
low
erove
rall
mar
ital
satisf
action
score
s,lo
wer
score
son
com
munic
atio
nan
dlo
wer
satisf
action
with
phys
ical
intim
acy
com
par
edto
norm
edsc
ore
sfo
rth
esc
ales
use
d.
No
gen
der
diffe
rence
sw
ere
found
Mar
ital
satisf
action
was
signifi
cantly
neg
ativ
ely
corr
elat
edw
ith
care
rburd
enan
dw
assi
gnifi
cantly
posi
tive
lyco
rrel
ated
with
love
,phys
ical
intim
acy
and
com
munic
atio
nTh
ere
sults
of
the
multip
lere
gre
ssio
nan
alys
isco
nfirm
edth
atca
rer
burd
en
contr
ibute
dneg
ativ
ely
tom
arital
satisf
action
and
par
tly
sup
port
edth
eposi
tive
rela
tionsh
ipof
love
and
com
munic
atio
nto
mar
ital
satisf
action,but
not
the
rela
tionsh
ipbet
wee
nphys
ical
intim
acy
and
mar
ital
satisf
action.
The
resu
lts
indic
ated
that
care
rburd
enneg
ativ
ely
impac
ted
on
mar
ital
satisf
action.
Satisf
action
with
phys
ical
intim
acy
was
not
signifi
cantly
rela
ted
tom
arital
satisf
action.
The
study
was
limited
by
the
smal
lsa
mple
size
ow
ing
tolo
wre
sponse
rate
.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 581

access to appropriate support and information so that they
could feel productive and maintain control of their lives.
Wollin et al.’s (15) study illuminated the challenge of
becoming a carer by describing the experience of disbelief
and devastation, the need to accommodate ‘losses and
forced choices’ and sadness and relief. This study reiterated
the importance of information and access to support. More
recently, psychological and emotional concerns, such as
helplessness and emotional strain, comprised one of seven
carer problems reported in Pakenham’s study (18),
emphasizing the importance of emotional support to carers.
Psychological distress and emotional strain were con-
sistently associated with reduced QOL, life satisfaction and
depression. Pakenham (17) examined the relationship
between stress and coping predictors and negative and
positive outcomes in MS caring. He found that higher
stress appraisals were related to higher distress, lower sat-
isfaction and negative affect, and that carers experienced
higher distress when they relied on avoidance coping
strategies and placed less reliance on meaning-based cop-
ing (positive reframing). In a more recent study (18), high
carer activity was related to lower positive states of mind
scale (PSOM) scores and lower life satisfaction and greater
personal reward, including strengthened relationships and
increased insight. Indeed, high care activity levels and care
burden have been consistently related to poorer psycho-
logical health in carers (21, 30).
Impact of disease characteristics on carers. The particular dis-
ease characteristics of MS appear to add an extra dimen-
sion to the caring experience. For example, depression,
cognitive and neuropsychiatric symptoms, including
delusion, disinhibition, agitation and anxiety in the PwMS
have been found to be significantly correlated with carer
distress over and above the effect of motor disability (26).
Khan et al. (20) also found a significant correlation be-
tween stress, anxiety and depression in the PwMS and the
caregiver strain index (CSI) total score, reflecting the
emotional adjustment, demands on carer time, change in
carer personal plans and disturbed sleep. Carers in Khan
et al.’s study rated emotional adjustments and family
adjustments owing to disrupted routine as causing severe
strain with disrupted schedule having a major impact upon
carers (21). Strained carers consistently report significantly
worse QOL scores (17, 20, 30). Sherman et al. (28) con-
firmed others’ findings but noted that the strongest
individual predictor of psychological distress was neuro-
behavioural disturbance in the PwMS, followed by the
adequacy of social support, followed by the PwMS’s lack of
awareness of their functional deficits.
Carer burden. Carer burden, which refers to the physical,
psychological, emotional, social and financial difficulties
experienced by carers (18), has been associated with
negative outcomes for carers, including: carers’ mood andTab
le2
Continued
Code
study
Study
des
ign,sa
mple
,/m
ethods
&in
stru
men
tsK
eyfindin
gs
Com
men
ts
Ved
har
aet
al.
2002
(32)
Engla
nd
Surv
ey,
com
par
ativ
edes
ign
Sam
ple
:nonra
ndom
Spousa
lca
rers
(n=
41;
14
wom
en,
27
men
,
resp
onse
rate
:uncl
ear)
62
nonca
rers
(44
wom
en,
18
men
)
Psyc
holo
gic
alques
tionnai
res
for
psy
choso
cial
asse
ssm
ent
usi
ng
the
follo
win
g:
14-ite
mglo
bal
mea
sure
of
per
ceiv
edst
ress
scal
e
5-ite
man
xiet
yan
ddep
ress
ion
subsc
ales
from
the
sava
ge
aged
per
sonal
ity
Scre
enin
gsc
ale
Leve
lof
care
rburd
envi
ath
eBurd
enin
terv
iew
Horm
onal
asse
ssm
ent
via
saliv
asa
mple
s.
Imm
une
asse
ssm
ent
via
blo
od
sam
ple
s.
Giv
enan
influen
zava
ccin
atio
n
Car
ers’
report
edsi
gnifi
cantly
hig
her
leve
lsof
stre
ssth
an
non
care
rs.
No
signifi
cant
diffe
rence
sw
ere
found
bet
wee
nca
rers
and
nonca
rers
inle
vels
of
anxi
ety
or
dep
ress
ion.
MS
care
rsre
port
edm
oder
atel
yhig
hnum
ber
sof
care
r
difficu
ltie
s.
Saliv
ary
cort
isola
nd
deh
ydro
epia
dro
ster
on
esu
lphat
e(D
HEA
)
leve
lsw
ere
signifi
cantly
hig
her
innonca
rers
than
care
rs,but
the
ratios
did
not
diffe
rbet
wee
nth
etw
ogro
ups.
No
signifi
cant
diffe
rence
sw
asfo
und
bet
wee
nM
Sca
rers
and
non
care
rsin
thei
rim
mune
resp
onse
sto
influen
za
vacc
inat
ion
Study
of
the
spouse
sof
PwM
S.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
582 M. Corry, A. While

mental health (6, 13, 14, 16, 18, 21, 22, 26) and QOL
(21, 29) with levels of psychological distress being signifi-
cantly higher than the normative population (28). Al-
though Kristjanson et al. (13) found little dysfunction
among carers using the general health questionnaire
(GHQ), they noted that over a quarter of carers had
problems with the response category ‘rather more than
usual and much more than usual’ (p. 373). This contrasts
with Gottberg et al.’s (12) pilot study testing the adequacy
of the sickness impact profile (SIP), which reported that
carers experienced modest subjective dysfunction, while
other studies reported mental and physical health prob-
lems among carers of PwMS (21, 26) and high GHQ scores
(poor health) (22). The commonest and most severe health
problems reported were anxiety, tiredness and depression,
and although less frequent, sexual and relationship prob-
lems were also regarded as severe (21). Pakenham (17)
reported an inverse relationship between depression and
anxiety and carer life satisfaction.
In a study by Forbes et al. (21), the variables that con-
tributed most to care burden and health status were disease
impact, dyadic health and carer activity, with the mental
health component also contributing to the health status.
Both care burden and health status were significant in
explaining 39% and 49% of the variance in the Caregivers
reaction assessment scale (CRA) and health problem vari-
ables, respectively. Carers’ needs and burden were found to
increase with increased carer activity (21) and care recipient
disability (13, 14, 27). Forbes et al. (21) found that greater
disease impact in the PwMS was related to more carer
activity, and that over time, the level of carer activity
increased in relation to all care activities. They also dem-
onstrated worsening health and increasing burden in rela-
tion to higher levels of carer activity, and this finding was
independent of the effects of disease impact and carer age.
Pakenham (19) has reported an association between
high care recipient symptoms and lower carer satisfaction.
Indeed, the strongest individual predictor of carer satis-
faction with life in Sherman et al.’s study (28) was social
support followed by significant other income, unawareness
of functional deficit, neurobehavioural disturbance,
psychological distress and executive functioning in the
PwMS. The impact of financial distress owing to loss of a
PwMS’s earnings was also highlighted by DeJubicibus and
McCabe (29), and was found to have greatest impact on
low-income families with teenage children. Patti et al. (27)
reported that lower physical functioning of the PwMS was
associated with lower carer scores on all SF-36 dimensions
and that lower QOL of the PwMS was associated with
lower carer social functioning scores. The disease trajectory
was recognized by Kristjanson et al.’s (13) carer sample
who reported anticipating the ‘bumpy road ahead of them’
(p. 375). This small-scale study noted that, where the
PwMS received more tailored services and more palliative
care services, carers were the most satisfied. However,
Krisjanson et al.’s study must be interpreted in the context
of the participants included in the study, who, for ethical
reasons, were in the early stages of the disease and thus may
not have experienced unmet needs or used services (13).
The increased need for more help as the disease pro-
gresses was a consistent finding (14, 21), and Khan et al.
(14) reported that many of their participants were not in
contact with a nurse or therapist with the burden of care
falling exclusively on the family and unpaid carer with all
its negative consequences upon the carers themselves.
They also noted Freeman et al.’s (1999) assertion that
carer strain is partly predictable and may be amenable to
prevention or reduction with appropriately directed
health-care resources.
Pozilli et al. (25) re-analysed data from a randomized
controlled trial with a 1-year follow up comparing the
effectiveness and the cost of multidisciplinary home care in
MS with traditional hospital care. They found that
depression in carers was related to the physical, emotional
and health status of the PwMS both at the start of the study
and at 12-month follow up. They also found that, when
carers’ depression worsened or improved over time, there
was a significant associated change in the PwMS’s dis-
ability. Pozilli et al. (25) argued that their findings sup-
ported a previously reported relationship between
depression in carers and longer disease duration and
higher severity of MS although they acknowledged a lack
of a control group and cautioned against concluding that
the association between carer psychological state, and
disability and emotional problems of PwMS implies that
carer depression is caused by these factors.
Benefits of caring. Only Pakenham (30) has examined the
nature of benefit finding in carers of PwMS using both
qualitative and quantitative methods with a large sample
of carers (n = 267). The qualitative data revealed that ca-
rers experienced seven benefits, including: greater insights
into illness and hardship; interpersonal benefits, such as
companionship gains; personal growth, such as becoming
more patient; the strengthening of relationships; increased
appreciation of life; health gains; and a change in life pri-
orities and personal goals. The findings derived from the
Carer Benefit Finding Scale which has two main compo-
nents – ‘Personal Growth’ and ‘Family Relations Growth’ –
showed differential relationships with illness and adjust-
ment domains. The benefit finding from the PwMS and
carer perspective correlated on all items except in the area
of ‘Family Relations Growth’, which showed the large
differences between the carers and the PwMS. Pakenham
(30) suggested that the PwMS was more likely to perceive
and value growth from family relations because of their
dependency on family caring. He also argued that the high
number of item correlations was the result of ‘… the no-
tion of a ‘communal search for meaning within carer-care
recipient dyads’ (p. 994). The Carer Benefit Finding Scale
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 583

factors were found to be positively related to carer and the
PwMS dyadic adjustment; however, the PwMS benefit
finding was unrelated to the carer adjustment domains.
Further, the carer benefit finding was related to carer po-
sitive adjustment domains and unrelated to carer negative
adjustment domains, suggesting that carer benefit finding
has a positive impact on carer adjustment. Interestingly,
greater benefit finding was also found to be related to high
carer activity (18).
Despite the limitations of the research, it is clear that,
while there are some benefits to carers in relation to caring
for PwMS, carers also experience stress, high care burden
and inadequate professional support. Holland and Nor-
throp (31), in a discussion paper exploring the benefits of
home services and coordination of care for the PwMS,
emphasized how carers of the PwMS differ from other
carers as they are more likely to be young or middle-aged
adults, to have children at home and to be employed full
time. They highlighted that carer strain for family mem-
bers caring for the PwMS is related to several contributing
factors with memory problems, needs in relation to activ-
ities of living and bowel dysfunction being particularly
stressful for carers.
Services available to carers
Four studies highlighted the inadequacy of the support
services available (11, 15, 20, 24). A study carried out in
the United Kingdom (11) investigating the nature of
informal and professional care in a community population
of PwMS found that respondents were most likely to be
assisted by their family rather than health or social-care
professionals and that the help which they received was
considered essential by approximately 70% of the
respondents. Another UK study (24) reported that many
carers were very unhappy with the formal support services
in place as they did not meet their needs or those of the
PwMS and were ‘… of such poor quality that they caused
both carer and care recipient much distress and angst’ (p.
227). An Australian study (15) comparing support for
people with motor neurone disease, Huntingdon’s disease,
Parkinson’s disease and MS identified that PwMS and their
families had difficulties accessing services and information
and noted the positive role played by the disease voluntary
organization and health-care professionals who provided
useful information and were accessible to PwMS and their
families. Another Australian study (20) reported a desire
for more respite services and a preference for home-based
provision.
However, the provision of professional support services
may not be just a matter of providing the service but of
educating carers regarding what they should ask for and
accepting the support services when offered. McKeown
et al. (24) found that carers may go through four stages in
their acceptance of support with caring; initially, they may
reject support but with time and as the PwMS becomes
more dependent, they may resist asking for support until
they reach a crisis when they seek out support progressing
to finally accepting the support given. The initial rejection
may be related to the carer’s desire to protect themselves
and the PwMS from the reality of MS reflecting a strong
desire to care for their loved one alone without assistance
from informal/formal services (24). They emphasized that
a carer’s view of or acceptance of support is not static and
that a carer may experience more than one phase at any
one time. This sample of carers reported that the formal
support services frequently did not meet their needs or
those of the PwMS as they were inconsistent, inflexible
and of poor quality causing much distress and angst to the
carer to the point that the carer rejected the support
completely (24).
Gender differences. Two studies (21, 27) provide some in-
sight into the differences between male and female carers.
While Forbes et al. (21) reported greater burden on the
disrupted schedule and health scales of the Caregiver’s
Reaction Assessment Scale among female carers compared
with male carers, Pattie et al. (27) found that the magni-
tude of QOL deterioration among carers was small. Mental
health was the dimension most affected in the carers,
especially males, followed by vitality and general health
(p < 0.001). Bodily pain was slightly higher in carers than
in normal subjects, especially among the female carers
(p < 0.001). Although the physical functioning of PwMS
impacted on carers, the age and gender of the carer were
found to be the main predictors of carer QOL.
While these studies provide some knowledge regarding
the impact of caring for PwMS, they provide limited
information in relation to how the well being of carers
impact upon the well being of PwMS or how the use of and
availability of support services impact on the psychological
well being of carers. Furthermore, the literature (31)
highlights that, if partners have to take on responsibilities
for personal care without any support from others, they
may be at risk for burnout. As a result, the PwMS may
experience neglect as the carer tries to juggle work, child
care and house work while providing necessary care for a
loved one. However, these assertions were not confirmed
by the studies exploring caring from the perspective of
spouses.
Spouse studies
The spouse studies examined the following areas: immune
response (32); experience of care giving (33–37); psycho-
logical outcomes and QOL, including marital satisfaction
(38–43). Both qualitative (n = 6) and quantitative (n = 6)
approaches were utilized, and together, they provide in-
sight regarding the spousal dimension of care-giving and
suggest that spouse carers have particular needs. Two
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
584 M. Corry, A. While

themes emerged in relation to spouses of PwMS, namely
the impact of caring and gender differences in caring.
Impact of caring
Four sub-themes emerged under the impact of caring: the
psychological and emotional impact of caring, carer bur-
den, losses and gains and marital satisfaction. Losses and
gains and marital satisfaction had both a positive and
negative impact on spouses.
The psychological and emotional impact of caring. Both the
PwMS and their spouse experience high levels of anxiety
and distress in the early period after diagnosis (42). Janssen
et al. (42) found that, on average, at 8 months after diag-
nosis (0–24 months), 40% of spouses reported high levels
of anxiety with 24% reporting severe stress. This echoes
the findings from an earlier study (32) which noted that
stress levels were higher in partner carers of PwMS com-
pared with noncarers. Courts et al. (37) has also reported
how friends and family were a source of stress for carers
because they did not understand MS and tended to
disappear as they felt unable to face the demands of the
illness.
Spouses’ end-of-day mood benefited from giving
instrumental support to and receiving emotional support
from the PwMS (40). More daily hassles and higher
end-of-day negative mood were reported by spouses who
received negative responses from the PwMS than those
who did not receive negative responses (41). However, the
adverse effects of the received negative responses on
end-of-day mood were moderated by receiving emotional
support on the same day (41).
Carer burden. Only one small-scale qualitative study (33)
(n = 2) explored spousal care burden, and therefore, the
transferability of the findings is limited. Time restrictions
and restrictions in development with respect to peers were
highlight as issues of concern. Similar findings were also
identified by Heward et al. (38) in the themes that
emerged from a grounded theory study on the way MS
affects the occupations of partners of PwMS.
Losses and gains. Cheung and Hocking (36) described how
spouses of PwMS responded to non-death-related losses.
They highlighted carers’ experiences of loss and gain and
their feelings of vulnerability and strength through pre-
senting some of the paradoxes found in the qualitative
data. Spouses experienced both loss and gain as they had:
‘… lost the person they once knew and gained a changed
person to look after’ (p. 157). They also lost the compan-
ionship of their spouse while simultaneously losing aspects
of themselves as a person with paid employment which is
valued by society and gaining the role of an unpaid carer.
Some of the carers also reported losing support from family
members, while others reported gaining this support. In-
come and lifestyle changes were experienced by all carers
in the study with lack of money resulting in the loss of
holidays and restrictions regarding family outings. Addi-
tionally, giving up full-time employment to look after their
spouse meant that their future employment opportunities
were limited. While for some, the carer role exposed their
vulnerability, it also helped them to develop strength.
Similar findings were reported by Heward et al. (38) in
terms of occupational constraints and opportunities expe-
rienced as a result of becoming a carer.
Court et al. (37) also noted the experience of loss with
participants reporting the loss of their partner together
with the loss of a fulfilling sexual relationship. Women
reported finding the role reversals challenging and de-
scribed MS as: ‘the third person in a marriage’ (p. 20). This
study highlighted the need for spouses to find a safe place
to discuss what Courts et al. (37) described as: ‘the dark
side of their feelings’ (p. 24). In addition to the losses
experienced, the reported relationship changes included
more arguments and disagreement in what was described
as a harmonious marriage prior to the illness (37) and
changes in overall marital satisfaction (43).
Marital satisfaction. One study explicitly explored the con-
cept of marital satisfaction. Perrone et al. (43) compared
carers of PwMS with scores from a normative group and
found that carers of PwMS had lower overall marital sat-
isfaction, lower scores on communication and lower sat-
isfaction with physical intimacy than the normed samples
for the measurement scales. However, carers of PwMS
reported greater amounts of love for their spouses than the
normed sample, and they did not indicate high levels of
perceived burden. Further, there were no gender differ-
ences in this study. Nonetheless, marital satisfaction was
negatively correlated with carer burden and was positively
correlated with love, physical intimacy and communica-
tion. Perrone et al. concluded that the findings suggested
that carer burden negatively impacts on marital satisfac-
tion, but that satisfaction with physical intimacy is not
significantly related to marital satisfaction. Positive aspects
of relationship changes were also highlighted by Courts
et al. (37). Some of the participants in Perrone et al.’s (43)
study reported having a stronger marriage, while others
reported ambivalence about their marriage. Indeed, one
respondent described how they also had the disease, not
just the PwMS reflecting the consequences upon a spousal
relationship.
Gender differences
Two studies (35, 37) provided some insight regarding the
differences between male and female carers. Boeije et al.
(35) reported how male and female carers developed
different perspectives of care-giving. While the male
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 585

carer’s perspective was characterized as: ‘you have to be
satisfied with it, feel obliged to give care and then be-
come resigned to it’ (p. 238), the female care-giving was
depicted as: ‘I have to become harder and less self-sac-
rificing’ (p. 238).
Men and women also differed in how they protected
themselves and their own lives; men were more likely to
set limits and protect their own lives, while women tended
to feel guilty if they did this, and reported feeling less
compensated for their caring efforts and overall suffered
more from the burden of caring. This gender difference
was also reported by Courts et al. (37), who found that,
while women tended to describe the lifestyle changes and
role reversals with great feeling, men tended to describe
their experiences more objectively. Thus, while women
became advocates to help their husbands maintain inde-
pendence and existing roles, men tended to feel angry and
take on a protective role. Men expressed anger about hu-
man and environmental barriers and became protectors of
their wives’ time, energy and employment opportunities
and were particularly angry with those who did not appear
to understand the effects of MS on the PwMS. Men dem-
onstrated their support by taking on more household
management, participating in giving injections and going
with their spouses to see their physicians.
Male and female carers also differed in relation to the
stress experienced with female carers reporting more stress
than male carers (35).
In addition to the aforementioned themes, one study
(39) was found that identified the top 10 needs of spouses
of PwMS. These included: the need for support from
health-care professionals, family and friends; to know that
health-care professionals are interested and to feel com-
fortable in communicating with them; to get information
about the condition and services on offer; and encour-
agement to maintain control over their own lives.
Discussion
All the studies had descriptive designs and many had sig-
nificant methodological weaknesses, including small sam-
ple sizes, nonrandom sampling, recruitment from small
geographical areas and use of unvalidated instruments.
Only studies reported in English language were included,
which may have excluded a number of European studies;
however, while McKeown et al.’s (3) review included only
three European studies, this review included 16. Addi-
tionally, there may be a publication bias as studies were
only included if they had been published in peer-reviewed
journals catalogued in the databases used to identify the
papers for inclusion. It is hoped that the review provides a
comprehensive extension to the earlier review of McKe-
own et al. (3).
The papers included in this review confirmed the
findings of McKeown et al.’s (3) review, namely the
major impact that caring has upon many aspects of ca-
rers’ lives and other dimensions of health. In particular,
the negative impact upon carers’ psychological well
being and the impact of increasing disability of the
PwMS was well demonstrated across a number of stud-
ies. In this review, the increased burden owing to the
advancing age of the PwMS was also highlighted.
Additionally, the particular characteristics of MS as a
disease appear to increase the carer burden, highlighting
the need for professionals to recognize the unique and
additional needs of carers of PwMS in comparison with
those caring for others.
Resource constraints are increasing the reliance upon
carers to provide ongoing support for PwMS emphasizing
the importance of maintaining the well being of carers, if
PwMS are to be sustained at optimal levels of functioning
and independence in their homes. Health-care profes-
sionals need to prioritize health promotion among carers of
PwMS if the deleterious effects of care giving are to be
minimized and poor health avoided.
This review, like the earlier review, found continued
poor support provision for carers of PwMS despite the
evidence that it is helpful and a source of satisfaction. It
seems that access to information and services remains a
challenge for carers with the reluctance of carers to accept
offered support playing a part. Much work needs to be
done by health-care professionals to both improve access
to services and to encourage carers to accept available
support.
However, unlike the earlier review, two additional
themes emerged from the papers, namely, that some carers
gain personal reward from their caring, although this was
by no means universal, and that the needs of spouses are
distinct and in addition to those of other carers. While both
groups of carers experienced both negative and positive
aspects to caring, the nature of the spousal relationship
meant that the experience was described in a more per-
sonal and intense manner in terms of a ‘web of paradoxes’
and expressed in terms of losses and gains (36). Although
both groups also experienced gender differences, carers in
general experienced this in terms of mental and physical
health. However, for spousal carers, the difference was in
the giving of care and the emotional aspect of caring. The
differences between carers and spousal carers was echoed
in Figved et al.’s study (26), where spouses reported sig-
nificantly higher levels of total carer distress and reduction
in QOL compared with other groups, and close friends
reporting least carer distress. Carers were reported to gain
benefit where there was carer adjustment within the car-
er–PwMS dyad (30), which echoes an assertion of Forbes
et al. (21) that health-care professionals should consider
the carer–PwMS dyad in the assessment of need. The
particular needs of spouses warrant especial attention by
health-care professionals if marriages are to be sustained in
the changed circumstances.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
586 M. Corry, A. While

Conclusion
Thirty-three studies from 11 countries were reviewed
which addressed a wide range of foci reflecting the breadth
of issues facing carers of PwMS. The studies revealed
consistent evidence of the need for resources and services
to relieve carer burden. However, as in the earlier review,
all the studies were descriptive, some with significant
methodological flaws so that descriptive evidence contin-
ues to be accumulated to the neglect of the development
and testing of interventions to support carers continuing in
their essential role.
This review highlights that, while all carers of PwMS
need professional support, spouses/partners who are carers
have additional and different needs to other carers. The
findings suggest that carers of PwMS face similar issues
internationally and that much remains to be done to limit
the negative impact of caring. As carers of PwMS are a
small group within the larger carer population, there is a
danger that their unique needs will be overlooked when
allocating scarce resources.
A national needs analysis incorporating the views of all
stakeholders is required to determine appropriate support
structures for carers of PwMS. Such support structures
should be uniquely tailored to the specific needs of carers
of PwMS and include the following: access to information
and education, professional counselling services, support
group facilitation and advocacy. In providing holistic care
to PwMS, health-care providers should also consider the
needs and well being of carers. There is also a need for
research to move beyond descriptive studies and to vali-
date instruments to assess carers of PwMS to permit
comparisons across studies internationally and to enable
the measurement of outcome of new interventions to
support carers of PwMS.
Author contributions
Margarita Corry performed literature search, analysis of
the literature and drafting of the review. Alison While gave
literature search advice, analysed the literature and gave
critical review of drafts and advice.
References
1 Swan J. Understanding multiple sclerosis. Nurs Resid Care
2006; 8: 358–60.
2 Carton H, Loos R, Pacolet J, Versieck K, Vlietinck R. A
quantitative study of unpaid caregiving in multiple sclerosis.
Mult Scler 2000; 6: 274–79.
3 McKeown LP, Porter-Armstrong AP, Baxter GD. The needs
and experiences of caregivers of individuals with multiple
sclerosis: a systematic review. Clin Rehabil 2003; 17: 234–48.
4 Vitaliano PP, Zhang J, Scanlan JM. Is caregiving hazardous to
one’s physical health? A meta-analysis Psychol Bull 2003;
129: 946–72.
5 Bourgeois MS, Burgio LD. When primary and secondary
caregivers disagree: predictors and psychosocial conse-
quences. Psychol Aging 1996; 11: 527–37.
6 Rivera-Nairarro J, Morales-Gonzales JM, Benito-Leon J.
Informal caregiving in multiple sclerosis patients; data from
the Madrid demyelinating disease group study. Disabil
Rehabil 2003; 25: 1057–64.
7 Chipchase SY, Lincoln NB. Factors associated with carer
strain in carers of people with multiple sclerosis. Disabil
Rehabil 2001; 23: 768–76.
8 Cohen S, Gottlieb BH, Underwood LG. Social relationships
and health: challenges for measurement and intervention.
Adv Mind-Body Med 2001; 17: 129–42.
9 Good DM, Bower DA, Einsporn RL. Social support: gender
differences in multiple sclerosis spousal caregivers. J Neurosci
Nurs 1995; 27: 305–11.
10 O’ Brien RA, Wineman NM, Nealon NR. Correlates of the
caregiving process in multiple sclerosis. Sch Inq Nurs Pract
1995; 9: 323–42.
11 O’ Hara L, De Souza L, Ide L. The nature of care giving in a
community sample of people with multiple sclerosis. Disabil
Rehabil 2004; 26: 1401–10.
12 Gottberg K, Einarsson U, Fredrikson S, Von Koch L,
Holmqvist LW. Multiple sclerosis in Stockholm county. A
pilot study of utilisation of health-care resources, patient
satisfaction with care and impact on family caregivers. Acta
Neurol Scand 2002; 106: 241–47.
13 Kristjanson LJ, Aoun SM, Oldham L. Palliative care and
support for people with neurodegenerative conditions and
their carers. Int J Palliat Nurs 2005; 12: 368–77.
14 Khan F, McPhail T, Brand C, Turner-Stokes L, Kilpatrick T.
Multiple sclerosis: disability profile and quality of life in Aus-
tralian community report. Int J Rehabil Res 2006; 29: 87–96.
15 Wollin JA, Yates PM, Kristjanson L. Supportive and palliative
care needs identified by multiple sclerosis patients and their
families. Int J Palliat Nurs 2006; 12: 20–26.
16 Morales-Gonzales JM, Benito-Leon J, Rivera-Navarro J,
Mitchell AJ. GEDMA study group: a systematic approach to
analyse health-related quality of life in multiple sclerosis: the
GEDMA study. Mult Scler 2004; 10: 47–54.
17 Pakenham KI. Relations between coping and positive and
negative outcomes in carers of persons with multiple scle-
rosis. J Clin Psychol Med Settings 2005; 12: 25–38.
18 Pakenham KI. The nature of caregiving in multiple sclerosis:
development of the caregiving tasks in multiple sclerosis
scale. Mult Scler 2007; 12: 929–38.
19 Pakenham KI. The nature of sense making in caregiving for
personswithmultiplesclerosis.DisabilRehabil2007;Sept24:1–
11.
20 Khan F, Pallant J, Brand C. Caregiver strain and factors
associated with caregiver self-efficacy and quality of life in a
community cohort with multiple sclerosis. Disabil Rehabil
2007; 29: 1241–50.
21 Forbes A, While A, Mathes L. Informal carer activities, carer
burden and health status in multiple sclerosis. Clin Rehabil
2007; 21: 563–75.
22 Groom MJ, Lincoln NB, Francis VM, Stephan TF. Assessing
mood in patients with multiple sclerosis. Clin Rehabil 2003;
17: 847–57.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
Carers of people with multiple sclerosis 587
23 Benbow C-L, Koopman WJ. Clinic-based needs assessment
of individuals with multiple sclerosis and significant others:
implications for program planning – psychological needs.
Rehabil Nurs 2003; 28: 109–16.
24 McKeown LP, Porter-Armstrong AP, Baxter GD. Caregivers
of people with multiple sclerosis: experiences of support. Mult
Scler 2004; 10: 219–30.
25 Pozzilli C, Palmisano L, Mainero C, Tomassini V, Marinelli F,
Risori G, Gasperini C, Fabiani M, Battagia MA. Relationship
between emotional distress in caregivers and health status in
persons with multiple sclerosis. Mult Scler 2004; 10: 442–46.
26 Figved N, Myhr KM, Larsen J-P, Aarsland D. Caregiver burden
in multiple sclerosis: the impact of neuropsychiatric symp-
toms. J Neuroogyl Neurosurg Psychiatry 2007; 78: 1097–102.
27 Patti F, Amato MP, Battaglia MA, Pitaro M, Russo P, Solaro
C, Trojano M. Caregiver quality of life in multiple sclerosis: a
multicentre Italian study. Mult Scler 2007; 13: 412–19.
28 Sherman TE, Rapport LJ, Hanks RA, Ryan KA, Keenan PA,
Khan O, Lisak RP. Predictors of well-being among significant
others of persons with multiple sclerosis. Mult Scler 2007; 13:
238–49.
29 DeJubicibus MA, McCabe M. Economic deprivation and its
effects on subjective wellbeing in families of people with
multiple sclerosis. J Ment Health 2005; 14: 49–59.
30 Pakenham IK. The positive impact of multiple sclerosis (MS)
on carers: associations between carer benefit finding and
positive and negative adjustment domains. Disabil Rehabil
2005; 27: 985–97.
31 Holland NJ, Northrop DE. Young adults with multiple scle-
rosis: management in the home. Home Health Care Manag
Pract 2006; 18: 186–95.
32 Vedhara K, McDermott MP, Evans TG, Treanor JJ, Plummer
S, Tallon D, Cruttenden KA, Schiftto G. Chronic stress in
non-elderly caregivers psychological, endocrine and immune
implications. J Psychosom Res 2002; 53: 1153–61.
33 Blank CW, Finlayson M. Exploring the impact of multiple
sclerosis on couples: a pilot study. Can J Occup Ther 2007; 74:
134–42.
34 Boeije HR, Duijnstee MSH, Grypdonck MHF. Continuation
of caregiving among partners who give total care to spouses
with multiple sclerosis. Health Soc Care Community 2003; 11:
242–52.
35 Boeije HR, Van Doorne- Huiskes A. Fulfilling a sense of duty:
how men and women giving care to spouses with multiple
sclerosis interpret this role. Community Work Fam 2003; 6:
222–44.
36 Cheung J, Hocking P. The experience of spousal carers of
people with multiple sclerosis. Qual Health Res 2004; 14: 153–
66.
37 Courts NF, Newton AN, McNeal LJ. Husbands and
wives living with multiple sclerosis. J Neurosci Nurs 2005; 37:
20–27.
38 Heward K, Molineux M, Gough B. A grounded theory
analysis of the occupational impact of caring for a partner
who has multiple sclerosis. J Occup Sci 2006; 13: 188–97.
39 Koopman WJ, Benbow C, Vandervoort M. Top 10 needs of
people with multiple sclerosis and their significant others.
J Neurosci Nurs 2006; 38: 369–73.
40 Kleiboer AM, Kuijer RG, Hox JJ, Schreurs KMG, Bensing
JM. Receiving and providing support in couples dealing with
multiple sclerosis: a diary study using an equity perspective.
Personal Relationships 2006; 13: 485–501.
41 Kleiboer AM, Kuijer RG, Hox JJ, Jongen PJH, Frequin STFM,
Bensing JM. Daily negative interactions and mood among
patients and partners dealing with multiple sclerosis (MS):
the moderating effects of emotional support. Soc Sci Med
2007; 64: 389–400.
42 Janssens AC, van Doorn PA, de Boer JB, van der Meche
FGA, Passchier J, Hintzen RQ. Impact of recently diagnosed
multiple sclerosis on quality of life, anxiety, depression and
distress of patients and partners. Acta Neurol Scand 2003; 108:
389–95.
43 Perrone KM, Gordon PA, Tschopp MK. Caregiver marital
satisfaction when a spouse has multiple sclerosis. J Appl
Rehabil Counsel 2006; 37: 26–32.
44 Mart́ı́nez-Ortega JA, Jurado D, Mart́ı́nez-Gonzalez MA,
Gurpegui M. Nicotine dependence, use of illegal drugs and
psychiatric morbidity. Addictive Behaviors 2006; 31: 1722–29.
� 2008 The Authors. Journal compilation � 2008 Nordic College of Caring Science
588 M. Corry, A. While





























