Embed Size (px)
Citation preview

Research ArticleTopically Applied Connective Tissue Growth FactorCCN2Improves Diabetic Preclinical Cutaneous WoundHealing Potential Role for CTGF in Human DiabeticFoot Ulcer Healing
F R Henshaw1 P Boughton2 L Lo1 S V McLennan13 and S M Twigg13
1Sydney Medical School and Charles Perkins Centre University of Sydney Sydney NSW 2006 Australia2Department of Biomedical Engineering School of Aerospace Mechanical and Mechatronic Engineering University of SydneySydney NSW 2006 Australia3Department of Endocrinology Royal Prince Alfred Hospital Camperdown NSW 2050 Australia
Correspondence should be addressed to S M Twigg stephentwiggsydneyeduau
Received 27 September 2014 Revised 23 January 2015 Accepted 2 February 2015
Academic Editor Solomon Tesfaye
Copyright copy 2015 F R Henshaw et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
AimsHypothesis Topical application of CTGFCCN2 to rodent diabetic and control wounds was examined In parallel researchcorrelation of CTGF wound fluid levels with healing rate in human diabetic foot ulcers was undertaken Methods Full thicknesscutaneous wounds in diabetic and nondiabetic control rats were treated topically with 1 120583g rhCTGF or vehicle alone on 2consecutive daysWound healing rate was observed on day 14 andwound sites were examined for breaking strength and granulationtissue In the human study across 32 subjects serial CTGF regulation was analyzed longitudinally in postdebridement diabeticwound fluidResults CTGF treated diabetic wounds had an accelerated closure rate compared with vehicle treated diabetic woundsHealed skin withstood more strain before breaking in CTGF treated rat wounds Granulation tissue from CTGF treatment indiabetic wounds showed collagen IV accumulation compared with nondiabetic animals Wound 120572-smooth muscle actin wasincreased inCTGF treated diabetic wounds comparedwith untreated diabetic wounds as wasmacrophage infiltration Endogenouswound fluidCTGFprotein rate of increase in human diabetic foot ulcers correlated positively with foot ulcer healing rate (119903 = 0406119875 lt 0001) ConclusionsInterpretation These data collectively increasingly substantiate a functional role for CTGF in humandiabetic foot ulcers
1 Introduction
Foot ulceration secondary to diabetes occurs in up to one-quarter of people with diabetes [1] and is the commonestcause of lower limb amputation accounting for 50ndash70 ofnontraumatic cases [2] Diabetes increases the risk of lowerextremity amputation by 10 to 20 times [3 4] The estimatedcost to the US healthcare system of diabetic foot ulcerationand related amputations is more than $10sdot9 billion [5] Thusdiabetic foot ulceration is a cause of significantmorbidity andfinancial burden
Wounds in diabetic patients typically show abnormalhealing characterized by chronicity persistent inflammationcopious exudate hypergranulation increased bacterial load
and reduced ability to heal [6] This delayed healing isthought to be due to a combination of factors includingmacro- and microvascular disease neuropathy bacterialinfection local pressure due to foot deformity and theadverse local metabolic environment caused by diabetesFurthermore pathogenic factors lead to suboptimal extracel-lular matrix (ECM) composition it has been hypothesizedthat a cytokinechemokine mediated imbalance betweensynthetic and degradative matrix pathways is responsiblefor the reduced amount and quality of ECM [7] Indeedhumandiabeticwounds exhibit an excess of proinflammatorycytokines such as TNF-120572 which contribute to an envi-ronment of increased protease activity in diabetic wounds[7]
Hindawi Publishing CorporationJournal of Diabetes ResearchVolume 2015 Article ID 236238 10 pageshttpdxdoiorg1011552015236238
2 Journal of Diabetes Research
CTGF is a 32ndash38 kDamember of the CCN family a groupof proteins which share a common modular structure [8]Also known as CCN2 CTGF is able to stimulate fibroblastproliferation and differentiation in sites including in skinthus enhancing ECM production [9] CTGF is overexpressedin many profibrotic conditions such as scleroderma [10]CTGF is able to promote cell adhesion and is chemotacticfor inflammatory cells especiallymacrophages it ismitogenicand also assists in cell differentiation [11 12] In vivo CTGFapplication accelerated wound healing in a monkey burnsmodel [13]
Changes in CTGF gene expression and protein levelshave been reported in some tissues and biological fluids ofdiabetic subjects especially where fibrosis occurs to relativeexcess [14] This includes diabetic nephropathy [15] diabeticcardiomyopathy [16] and retinopathy [17] where CTGF iselevated In contrast in skin in nonhuman primate (Baboon)studies we have recently shown that intact CTGF proteinis deficient in diabetic wound tissue compared with woundtissue in nondiabetic animals [18] In that study the woundinflammatory and protease environment was also increasedin diabetes and CTGF protein accumulation in woundswas delayed To date however CTGF regulation in humandiabetic wounds has not yet been reported and the effect oftopical application of CTGF to diabetic wounds has not beendescribed in any animalmodelThe aims of this study were to(i) examine if topical rhCTGF improves wound healing in awell defined model of diabetic rodent cutaneous woundingand (ii) determine whether CTGF increase in wound fluidfrom human diabetic foot ulcers demonstrates a relationshipwith wound healing rate
2 Methods and Materials
21 Connective Tissue Growth Factor (CTGF) and Its Applica-tion Recombinant human CTGF (rhCTGF) was expressedutilizing adenovirus in 911 cells and purified and quantitatedin house exactly as previously described with confirmationof its ECM inducing bioactivity [19]
22 Induction of Diabetes and Creation of SkinWounds MaleSprague-Dawley rats (119899 = 52) purchased from AustralianLaboratory Supply (Perth Australia) aged between 6 and7 weeks were used in these studies Ethics approval forinduction of diabetes in animals and creation of woundswas obtained from the Animal Research Ethics CommitteeSydney SouthWestern Area Health Service (SSWAHS) Type1 diabetes was induced in 23 animals using streptozotocin(STZ 65mgkg Calbiochem Sydney Australia) and animalswere maintained on 2ndash4 IU of insulin (Mixtard Novo-Nordisk) every second day to preventweight loss and ketoaci-dosis After 7 weeks diabetic (119899 = 23) and control (119899 = 29)animals were anesthetized using Ketamine (85mgkg PfizerSydney Australia) and Xylazine (5mgkg Bayer LeverkusenGermany) The dorsal skin was prepared for wounding byshaving with clippers and depilation (Nads Baulkham HillsAustralia) and swabbing with antiseptic (Betadine SymbionMelbourne Australia) As we previously described [20] 4
full thickness dorsally placed excisional wounds per rat werethen created using an 8mm punch biopsy (Stieffel Laborato-ries NSW Australia) The wounds included the panniculuscarnosus and exposed the underlying dorsolateral skeletalmuscle fascia At the time of wounding all animals weretreated with a single dose of parenteral antibiotic (Ampicillin50mgkg)
23 Topical RhCTGF Treatment of Skin Wounds RhCTGFas 1 120583g in 20120583L of sterile phosphate buffered saline (PBS)was applied topically to two of the ulcers in each animaland 20 120583L PBS was applied topically to the remaining twowounds Ulcers were each occluded using a transparentdressing (Tegaderm 3M NSW Australia) which was securedperipherally usingHypafix tape (Smith andNephewVictoriaAustralia) At an interval of 24 h animals were anaesthetizedin the manner already described and treated with a seconddose of rhCTGF or PBS to the same wounds as beforeWounds were again occluded using Tegaderm and Hypafix
In one series of experiments the effect of rhCTGF onwound closure was determined by tracing the circumferenceof the wounds onto transparencies on the day of woundingand then at regular intervals thereafter (Tegaderm dressingpackaging) In a parallel series rats from each group wereterminated at days 7 and 14 and the tissue containing thewound was excised and either (i) fixed in paraformaldehyde(4 in PBS) for later immunohistochemical analysis or (ii)snap-frozen in liquid nitrogen for determination of woundbreaking strength
24 Analysis of Wound Closure Wound circumference trac-ings were translated into computer images using pen-tablet software (Bamboo Wacom USA) for quantification ofwound area using Image J (Research Services Branch NIMHUSA) [20]Wound closure was then calculated and results areexpressed as a percentage of original wound size
25 Analysis of Wound Breaking Strength Wound breakingstrength was determined using our published methods [18]adapted for rodents Wounds that had been excised on day14 were removed from frozen storage and cut into shapeusing an aluminum template Width length and thicknessof skin pieces were measured using calipers The tissue wasallowed to thaw and tensile strength was determined atroom temperature Tissue ends were securely mounted ona 2mm balsa wood sandwich coupling using cyanoacrylateand placed in the jaws of an Elf3400 Tensiometer (BOSEEnduraTec Minnetonka MN USA) Load and displacementuntil the time of skin rupture at the healed wound sitewere obtained using a 45N load at a cross-head speedof 10mmmin Cross-sectional area was determined fromoriginal skin thickness measurements and values were usedto calculate stress and strain and Youngrsquos modulus (tensilestrength)
26 Analysis of Wound Cellular Content and ExtracellularMatrix The excised paraformaldehyde embedded woundswere sectioned (5 120583msection) perpendicular to the wound
Journal of Diabetes Research 3
Table 1 Wound closure data in diabetic and nondiabetic (control) rats each treated with topical rhCTGF or PBS alone
Wound closure ( of initial wound size)Group Day 1 Day 3 Day 7 Day 10 Day 14C + PBS alone 857 plusmn 15 577 plusmn 21 252 plusmn 09lowast 180 plusmn 06 130 plusmn 04DM + PBS alone 928 plusmn 16 617 plusmn 17 310 plusmn 11 207 plusmn 08 159 plusmn 05C + CTGF 817 plusmn 14lowast 522 plusmn 18lowast 256 plusmn 09lowast 165 plusmn 04 132 plusmn 03lowast
DM + CTGF 854 plusmn 14 575 plusmn 22 284 plusmn 12lowast 161 plusmn 07lowast 136 plusmn 04lowast
Results are shown as mean plusmn SEM lowast119875 lt 005 versus the same day diabetic wounds + PBS (DM + PBS alone) by ANOVA The main finding was that ulcerarea was significantly reduced on days 7 10 and 14 in the CTGF treated diabetic group (D + CTGF) compared with the non-rhCTGF treated diabetic group(D + PBS alone)
surface Macrophages from sections obtained at days 7 and14 were identified by immunohistochemical staining withCD68 (Abcam Cambridge MA) as described previously[20] In brief following antigen retrieval nonspecific bindingwas blocked by incubation in 10 vv goat serum andafter washing with PBS the sections were incubated for60min in CD68 (1 200) mouse IgG1 A further PBS washwas carried out before incubation with 1 400 dilution ofsecondary antibody (Biotinylated anti-mouse) Cells werevisualized using peroxidase-conjugated secondary antibodiesand 331015840-diaminobenzidine chromogen (Vector LaboratoriesBurlingame CA)The number of macrophages in 20 sequen-tial fields was determined (attimes1000magnification) by a singleobserver blinded to animal grouping and treatment status
Fibroblast and endothelial cells from sections obtainedat days 7 and 14 were identified by immunohistochemicalstaining using anti-120572-smoothmuscle actin (120572-SMA) primaryantibody 1 200 (120572-SMA Abcam Burlingame CA) andtheir characteristic morphology Detection then involvedsecondary antibody and the ABC method as described forCD68 staining above and as per [20] Cells were stained andvisualized as described formacrophagesThe 120572-SMApositivefibroblasts and endothelial staining intensity within eachwound section was scored by two independent observerseach blinded to animal grouping and treatment status Aspreviously described the scoring was based on a grade of0ndash3 where zero was for no staining up to three for intensestaining and any background staining in the isotype controlsectionwas subtracted from the overall staining score [18 21]
Immunohistochemical staining for collagen IV was per-formed as previously described using the goat generatedanti-collagen IV polyclonal antibody Abcam (Ab86042) at1 200 titer as the primary antibody The subsequent stainingand detection method was that previously used in diabeticpreclinical studies [18 21] with the same scoring method asdescribed for 120572-SMA quantitation above
27 Human Diabetic Foot Ulcer Wound Fluid Analysis Ina separate series of experiments relative CTGF levels inpostdebridement wound fluid in diabetic wounds were deter-mined in patients managed at the multidisciplinary high riskfoot service where all aspects of diabetic foot care had beenoptimized [22 23] (Table 3)Therewere 32 serial subjectswithtype 2 diabetes and each had dense peripheral neuropathyand some were also ischemic ulcers (Table 1) Ethics approval
for this study was obtained from the Human Research EthicsCommittee Sydney South Western Area Health Service
Wound fluid was obtained following debridement usinga sterile 1 cm2 Whatman 4mm filter paper as previouslydescribed [22 23] The protein concentration of the woundfluid was determined using the BioRad protein assay (Bio-Rad Sydney Australia) and a sample containing a standardamount of total protein (30 120583g) was applied to a 125 SDS-PAGEunder reducing conditions as previously described [1824] Western immunoblot analysis using an in-house gener-ated anti-CTGF polyclonal primary antibody (196) at 1 1000titer and subsequent goat anti-rabbit secondary antibody wasundertaken using standardmethods [18]Data determined bydensitometry was then analyzed and presented as changein immunoreactive CTGF in the wound fluid compared with ulcer healing rate across the same time interval In mostcases each wound had 3CTGF measures spread in totalacross 45 or more days
28 Statistical Analysis Wound data is expressed as mean plusmnSD or mean plusmn SEM each as indicated Analysis was per-formed by one way ANOVA with post hoc correction byBonferonirsquos multiple comparison test or by unpaired 119905-testeach as indicated A119875 valuelt 005was considered statisticallysignificant Simple linear correlation analysis was performedfor the human CTGF change in postdebridement woundfluid data in relation to time
3 Results
31 Effect of CTGF on Wound Closure Group data formacroscopic wound closure measurement expressed as apercentage change from the initial wound area at respectivetime points is shown in Table 1 Diabetic animals (D + PBS)were found to have wound closure rates that were slowerthan those in control (nondiabetic) animals (C + PBS) withthis being significant on day 7 In addition macroscopicwound closure was significantly enhanced on days 7 10 and14 in the CTGF treated diabetic group compared with thenonactively treated diabetic group with vehicle alone (D +PBS) Table 1 In contrast to CTGF effects in diabetic woundsnondiabetic wounds treated with CTGF (C + CTGF) did notshow improved closure rates relative to controls alone (C +PBS)
4 Journal of Diabetes Research
Table 2 Wound breaking strength data in all groups
Youngrsquos modulus Tear strength Tear strain Ultimate strength Final strainC + PBS alone 093 plusmn 009 056 plusmn 006 117 plusmn 010 106 plusmn 001 345 plusmn 022lowast
DM + PBS alone 087 plusmn 013 046 plusmn 005 071 plusmn 006 081 plusmn 013 220 plusmn 016C + CTGF 121 plusmn 011 053 plusmn 005 104 plusmn 010 089 plusmn 006 308 plusmn 027lowast
DM + CTGF 101 plusmn 017 053 plusmn 005 087 plusmn 018 086 plusmn 010 232 plusmn 022Data are mean plusmn SD each lowast119875 lt 005 versus DM + PBS by ANOVA
0
50
100
150
200
250
300
C C + CTGF D D + CTGF
lowast
lowast
Mac
roph
ages
(n) p
er20
sect
ions
(a) Day 7
0
50
100
150
200
250
300
C C + CTGF D D + CTGFM
acro
phag
es (n
) per
20
sect
ions
(b) Day 14
Figure 1 Wound macrophage counts (a) CTGF treated (control and diabetic groups combined) is different to CTGF untreated (control anddiabetic groups combined) lowast119875 lt 005 by unpaired 119905-test at day 7 No statistical difference was observed between groups at day 14 (b) Resultsare expressed as mean plusmn SEM
Table 3 Demographics of patients with diabetes who had postde-bridement foot ulcer fluid analyzed
Patient demographicsStudy subject number (119899) 32Age (years)lowast 641 plusmn 18Diabetes duration (years) 176 plusmn 19Gender ( male) 75Ulcer type
Neuropathic only 29Neuroischemic 3
lowastAll data are mean plusmn SD
32 CTGFTherapy and Wound Breaking Strength The effectof CTGF on the wound breaking strength at the woundsite was also measured Analysis by ANOVA showed thatuntreated diabetic wounds elongate less well before breakingthan either treated or untreated control wounds (119875 lt 005)(average 220MPa compared with 308 and 345MPa resp)indicating that diabetic wounds are functionally less flexible(Table 2) CTGF treated diabetic wounds had a slightly highermean final strain (232MPa) than the untreated diabeticwounds (220MPa) however this did not reach statisticalsignificance Youngrsquos modulus which measures stress in rela-tion to strain and thus wound elasticity was not significantlydifferent between groups in this model
33 Effect of CTGF Treatment onWound Cellular Content andMatrix Macrophage cell counts in CD68 stained sections
(Figure 1) were lower in PBS alone treated animals comparedwith CTGF treated animals at day 7 Macrophage cell countdeclined in both treated and untreated groups by day 14comparedwith day 7 Interestingly themacrophages appearedto persist in the CTGF treated diabetic animals (119899 =107 macrophages20 fields) compared with the nontreateddiabetic animals (119899 = 73 macrophages20 fields) at day 14although this did not reach statistical significance
Intensity of staining by 120572-SMA a marker of activatedfibroblasts and mature vascular blood vessel cells was mea-sured at days 7 and 14 The fibroblast 120572-SMA in the nondi-abetic rat wounds was higher (Figures 2(a) and 2(b)) thanboth the treated and untreated diabetic animals indicating arelative lack of activated fibroblasts in the diabetic wounds byANOVA (119875 lt 005) Increased120572-SMA staining in endothelialcells was observed at day 7 in control compared with diabeticanimals regardless of treatment (119875 lt 005) (Figures 2(c)and 2(d)) The CTGF topical treatment of diabetic micetrended at day 7 to higher 120572-SMA staining score in fibroblasts(Figure 2(a)) and endothelial cells (Figure 2(c)) comparedwith scores in untreated diabetic mouse although on eachoccasion this did not reach statistical significance Represen-tative images of 120572-SMA staining are shown in Figure 2(e)
Collagen IV staining was lower in untreated diabeticwounds at day 7 and was increased by rhCTGF (119875 lt005) (Figure 3(a)) At day 14 CTGF treated diabetic woundsshowed significant increases in wound collagen IV comparedwith untreated diabetic wounds (119875 lt 0005) (Figure 3(b))Representative collagen IV images for days 7 and 14 from ratswithin respective groups are shown in Figure 4
Journal of Diabetes Research 5
0
05
1
15
2In
tens
ity
C C + CTGF D D + CTGFlowast
lowast
lowastDifferent to C each P lt 005 by ANOVA
(a) Day 7 fibroblasts
0
05
1
15
2
Inte
nsity
C C + CTGF D D + CTGF
(b) Day 14 fibroblasts
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
lowast
by unpaired t-testlowastDifferent to C and C + CTGF combined P lt 005
(c) Day 7 endothelial cells
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
(d) Day 14 endothelial cells
Control Control + rhCTGF Diabetes + PBS Diabetes + rhCTGF
200120583m200120583m 200120583m200120583m
(e) Day 7
Figure 2 Wound 120572-smooth muscle actin staining in fibroblasts and endothelial cells (a) shows 120572-SMA staining intensity scoring infibroblasts in treated control animals compared with the two diabetic animal groups at day 7 lowast119875 lt 005 by ANOVA for each of the groupsmarked versus Control + CTGF No such differences were observed at day 14 in (b) In (c) increased 120572-SMA staining in endothelial cells wasobserved at day 7 in control animals (treated and untreated combined) compared with diabetic animals (treated and untreated combined)lowast
119875 lt 005 by unpaired 119905-test No such differences were observed at day 14 (d) Results are expressed as mean plusmn SEM Representative imagesat day 7 are shown in (e)
34 Endogenous CTGF Changes in Human Diabetic FootUlcer Wound Fluid Postdebridement wound fluid samplesobtained from people with type 2 diabetes who had footulcers were analyzed for CTGF byWestern immunoblot anal-ysis and wound area was determined at each visit based onacetate tracings Figure 5(a) shows a typical cutaneouswoundarea profile in a patient with a neuropathic hallux plantarulcer with times (arrows) when ulcer fluid was collectedand then analyzed the following serial debridements Therespective Western immunoblot analysis for CTGF in theulcer fluid is shown in Figure 5(b) CTGF was detected asa predominant intact sim36ndash38 kDa series of molecular mass
bands typical of known intact CTGF glycoforms [24] Insome immunoblots there was also lower molecular masssignal at sim26 kDa (Figure 5(b)) as previously observed inbiological fluids [18]
The group data (119899 = 32 study subjects) relating ulcerhealing rate to rate of change in CTGF in ulcer fluid acrossan average time period of 10 days showed that an increasein CTGF levels correlates highly significantly with woundhealing rate indicated as percentage reduction in ulcer areaper 10 days (Figure 5(c)) 119903 = 0406 119875 lt 0001 Whilethere was quite marked interindividual variation in the dataon average a 10 increase in CTGF levels in wound fluid
6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Journal of Diabetes Research
CTGF is a 32ndash38 kDamember of the CCN family a groupof proteins which share a common modular structure [8]Also known as CCN2 CTGF is able to stimulate fibroblastproliferation and differentiation in sites including in skinthus enhancing ECM production [9] CTGF is overexpressedin many profibrotic conditions such as scleroderma [10]CTGF is able to promote cell adhesion and is chemotacticfor inflammatory cells especiallymacrophages it ismitogenicand also assists in cell differentiation [11 12] In vivo CTGFapplication accelerated wound healing in a monkey burnsmodel [13]
Changes in CTGF gene expression and protein levelshave been reported in some tissues and biological fluids ofdiabetic subjects especially where fibrosis occurs to relativeexcess [14] This includes diabetic nephropathy [15] diabeticcardiomyopathy [16] and retinopathy [17] where CTGF iselevated In contrast in skin in nonhuman primate (Baboon)studies we have recently shown that intact CTGF proteinis deficient in diabetic wound tissue compared with woundtissue in nondiabetic animals [18] In that study the woundinflammatory and protease environment was also increasedin diabetes and CTGF protein accumulation in woundswas delayed To date however CTGF regulation in humandiabetic wounds has not yet been reported and the effect oftopical application of CTGF to diabetic wounds has not beendescribed in any animalmodelThe aims of this study were to(i) examine if topical rhCTGF improves wound healing in awell defined model of diabetic rodent cutaneous woundingand (ii) determine whether CTGF increase in wound fluidfrom human diabetic foot ulcers demonstrates a relationshipwith wound healing rate
2 Methods and Materials
21 Connective Tissue Growth Factor (CTGF) and Its Applica-tion Recombinant human CTGF (rhCTGF) was expressedutilizing adenovirus in 911 cells and purified and quantitatedin house exactly as previously described with confirmationof its ECM inducing bioactivity [19]
22 Induction of Diabetes and Creation of SkinWounds MaleSprague-Dawley rats (119899 = 52) purchased from AustralianLaboratory Supply (Perth Australia) aged between 6 and7 weeks were used in these studies Ethics approval forinduction of diabetes in animals and creation of woundswas obtained from the Animal Research Ethics CommitteeSydney SouthWestern Area Health Service (SSWAHS) Type1 diabetes was induced in 23 animals using streptozotocin(STZ 65mgkg Calbiochem Sydney Australia) and animalswere maintained on 2ndash4 IU of insulin (Mixtard Novo-Nordisk) every second day to preventweight loss and ketoaci-dosis After 7 weeks diabetic (119899 = 23) and control (119899 = 29)animals were anesthetized using Ketamine (85mgkg PfizerSydney Australia) and Xylazine (5mgkg Bayer LeverkusenGermany) The dorsal skin was prepared for wounding byshaving with clippers and depilation (Nads Baulkham HillsAustralia) and swabbing with antiseptic (Betadine SymbionMelbourne Australia) As we previously described [20] 4
full thickness dorsally placed excisional wounds per rat werethen created using an 8mm punch biopsy (Stieffel Laborato-ries NSW Australia) The wounds included the panniculuscarnosus and exposed the underlying dorsolateral skeletalmuscle fascia At the time of wounding all animals weretreated with a single dose of parenteral antibiotic (Ampicillin50mgkg)
23 Topical RhCTGF Treatment of Skin Wounds RhCTGFas 1 120583g in 20120583L of sterile phosphate buffered saline (PBS)was applied topically to two of the ulcers in each animaland 20 120583L PBS was applied topically to the remaining twowounds Ulcers were each occluded using a transparentdressing (Tegaderm 3M NSW Australia) which was securedperipherally usingHypafix tape (Smith andNephewVictoriaAustralia) At an interval of 24 h animals were anaesthetizedin the manner already described and treated with a seconddose of rhCTGF or PBS to the same wounds as beforeWounds were again occluded using Tegaderm and Hypafix
In one series of experiments the effect of rhCTGF onwound closure was determined by tracing the circumferenceof the wounds onto transparencies on the day of woundingand then at regular intervals thereafter (Tegaderm dressingpackaging) In a parallel series rats from each group wereterminated at days 7 and 14 and the tissue containing thewound was excised and either (i) fixed in paraformaldehyde(4 in PBS) for later immunohistochemical analysis or (ii)snap-frozen in liquid nitrogen for determination of woundbreaking strength
24 Analysis of Wound Closure Wound circumference trac-ings were translated into computer images using pen-tablet software (Bamboo Wacom USA) for quantification ofwound area using Image J (Research Services Branch NIMHUSA) [20]Wound closure was then calculated and results areexpressed as a percentage of original wound size
25 Analysis of Wound Breaking Strength Wound breakingstrength was determined using our published methods [18]adapted for rodents Wounds that had been excised on day14 were removed from frozen storage and cut into shapeusing an aluminum template Width length and thicknessof skin pieces were measured using calipers The tissue wasallowed to thaw and tensile strength was determined atroom temperature Tissue ends were securely mounted ona 2mm balsa wood sandwich coupling using cyanoacrylateand placed in the jaws of an Elf3400 Tensiometer (BOSEEnduraTec Minnetonka MN USA) Load and displacementuntil the time of skin rupture at the healed wound sitewere obtained using a 45N load at a cross-head speedof 10mmmin Cross-sectional area was determined fromoriginal skin thickness measurements and values were usedto calculate stress and strain and Youngrsquos modulus (tensilestrength)
26 Analysis of Wound Cellular Content and ExtracellularMatrix The excised paraformaldehyde embedded woundswere sectioned (5 120583msection) perpendicular to the wound
Journal of Diabetes Research 3
Table 1 Wound closure data in diabetic and nondiabetic (control) rats each treated with topical rhCTGF or PBS alone
Wound closure ( of initial wound size)Group Day 1 Day 3 Day 7 Day 10 Day 14C + PBS alone 857 plusmn 15 577 plusmn 21 252 plusmn 09lowast 180 plusmn 06 130 plusmn 04DM + PBS alone 928 plusmn 16 617 plusmn 17 310 plusmn 11 207 plusmn 08 159 plusmn 05C + CTGF 817 plusmn 14lowast 522 plusmn 18lowast 256 plusmn 09lowast 165 plusmn 04 132 plusmn 03lowast
DM + CTGF 854 plusmn 14 575 plusmn 22 284 plusmn 12lowast 161 plusmn 07lowast 136 plusmn 04lowast
Results are shown as mean plusmn SEM lowast119875 lt 005 versus the same day diabetic wounds + PBS (DM + PBS alone) by ANOVA The main finding was that ulcerarea was significantly reduced on days 7 10 and 14 in the CTGF treated diabetic group (D + CTGF) compared with the non-rhCTGF treated diabetic group(D + PBS alone)
surface Macrophages from sections obtained at days 7 and14 were identified by immunohistochemical staining withCD68 (Abcam Cambridge MA) as described previously[20] In brief following antigen retrieval nonspecific bindingwas blocked by incubation in 10 vv goat serum andafter washing with PBS the sections were incubated for60min in CD68 (1 200) mouse IgG1 A further PBS washwas carried out before incubation with 1 400 dilution ofsecondary antibody (Biotinylated anti-mouse) Cells werevisualized using peroxidase-conjugated secondary antibodiesand 331015840-diaminobenzidine chromogen (Vector LaboratoriesBurlingame CA)The number of macrophages in 20 sequen-tial fields was determined (attimes1000magnification) by a singleobserver blinded to animal grouping and treatment status
Fibroblast and endothelial cells from sections obtainedat days 7 and 14 were identified by immunohistochemicalstaining using anti-120572-smoothmuscle actin (120572-SMA) primaryantibody 1 200 (120572-SMA Abcam Burlingame CA) andtheir characteristic morphology Detection then involvedsecondary antibody and the ABC method as described forCD68 staining above and as per [20] Cells were stained andvisualized as described formacrophagesThe 120572-SMApositivefibroblasts and endothelial staining intensity within eachwound section was scored by two independent observerseach blinded to animal grouping and treatment status Aspreviously described the scoring was based on a grade of0ndash3 where zero was for no staining up to three for intensestaining and any background staining in the isotype controlsectionwas subtracted from the overall staining score [18 21]
Immunohistochemical staining for collagen IV was per-formed as previously described using the goat generatedanti-collagen IV polyclonal antibody Abcam (Ab86042) at1 200 titer as the primary antibody The subsequent stainingand detection method was that previously used in diabeticpreclinical studies [18 21] with the same scoring method asdescribed for 120572-SMA quantitation above
27 Human Diabetic Foot Ulcer Wound Fluid Analysis Ina separate series of experiments relative CTGF levels inpostdebridement wound fluid in diabetic wounds were deter-mined in patients managed at the multidisciplinary high riskfoot service where all aspects of diabetic foot care had beenoptimized [22 23] (Table 3)Therewere 32 serial subjectswithtype 2 diabetes and each had dense peripheral neuropathyand some were also ischemic ulcers (Table 1) Ethics approval
for this study was obtained from the Human Research EthicsCommittee Sydney South Western Area Health Service
Wound fluid was obtained following debridement usinga sterile 1 cm2 Whatman 4mm filter paper as previouslydescribed [22 23] The protein concentration of the woundfluid was determined using the BioRad protein assay (Bio-Rad Sydney Australia) and a sample containing a standardamount of total protein (30 120583g) was applied to a 125 SDS-PAGEunder reducing conditions as previously described [1824] Western immunoblot analysis using an in-house gener-ated anti-CTGF polyclonal primary antibody (196) at 1 1000titer and subsequent goat anti-rabbit secondary antibody wasundertaken using standardmethods [18]Data determined bydensitometry was then analyzed and presented as changein immunoreactive CTGF in the wound fluid compared with ulcer healing rate across the same time interval In mostcases each wound had 3CTGF measures spread in totalacross 45 or more days
28 Statistical Analysis Wound data is expressed as mean plusmnSD or mean plusmn SEM each as indicated Analysis was per-formed by one way ANOVA with post hoc correction byBonferonirsquos multiple comparison test or by unpaired 119905-testeach as indicated A119875 valuelt 005was considered statisticallysignificant Simple linear correlation analysis was performedfor the human CTGF change in postdebridement woundfluid data in relation to time
3 Results
31 Effect of CTGF on Wound Closure Group data formacroscopic wound closure measurement expressed as apercentage change from the initial wound area at respectivetime points is shown in Table 1 Diabetic animals (D + PBS)were found to have wound closure rates that were slowerthan those in control (nondiabetic) animals (C + PBS) withthis being significant on day 7 In addition macroscopicwound closure was significantly enhanced on days 7 10 and14 in the CTGF treated diabetic group compared with thenonactively treated diabetic group with vehicle alone (D +PBS) Table 1 In contrast to CTGF effects in diabetic woundsnondiabetic wounds treated with CTGF (C + CTGF) did notshow improved closure rates relative to controls alone (C +PBS)
4 Journal of Diabetes Research
Table 2 Wound breaking strength data in all groups
Youngrsquos modulus Tear strength Tear strain Ultimate strength Final strainC + PBS alone 093 plusmn 009 056 plusmn 006 117 plusmn 010 106 plusmn 001 345 plusmn 022lowast
DM + PBS alone 087 plusmn 013 046 plusmn 005 071 plusmn 006 081 plusmn 013 220 plusmn 016C + CTGF 121 plusmn 011 053 plusmn 005 104 plusmn 010 089 plusmn 006 308 plusmn 027lowast
DM + CTGF 101 plusmn 017 053 plusmn 005 087 plusmn 018 086 plusmn 010 232 plusmn 022Data are mean plusmn SD each lowast119875 lt 005 versus DM + PBS by ANOVA
0
50
100
150
200
250
300
C C + CTGF D D + CTGF
lowast
lowast
Mac
roph
ages
(n) p
er20
sect
ions
(a) Day 7
0
50
100
150
200
250
300
C C + CTGF D D + CTGFM
acro
phag
es (n
) per
20
sect
ions
(b) Day 14
Figure 1 Wound macrophage counts (a) CTGF treated (control and diabetic groups combined) is different to CTGF untreated (control anddiabetic groups combined) lowast119875 lt 005 by unpaired 119905-test at day 7 No statistical difference was observed between groups at day 14 (b) Resultsare expressed as mean plusmn SEM
Table 3 Demographics of patients with diabetes who had postde-bridement foot ulcer fluid analyzed
Patient demographicsStudy subject number (119899) 32Age (years)lowast 641 plusmn 18Diabetes duration (years) 176 plusmn 19Gender ( male) 75Ulcer type
Neuropathic only 29Neuroischemic 3
lowastAll data are mean plusmn SD
32 CTGFTherapy and Wound Breaking Strength The effectof CTGF on the wound breaking strength at the woundsite was also measured Analysis by ANOVA showed thatuntreated diabetic wounds elongate less well before breakingthan either treated or untreated control wounds (119875 lt 005)(average 220MPa compared with 308 and 345MPa resp)indicating that diabetic wounds are functionally less flexible(Table 2) CTGF treated diabetic wounds had a slightly highermean final strain (232MPa) than the untreated diabeticwounds (220MPa) however this did not reach statisticalsignificance Youngrsquos modulus which measures stress in rela-tion to strain and thus wound elasticity was not significantlydifferent between groups in this model
33 Effect of CTGF Treatment onWound Cellular Content andMatrix Macrophage cell counts in CD68 stained sections
(Figure 1) were lower in PBS alone treated animals comparedwith CTGF treated animals at day 7 Macrophage cell countdeclined in both treated and untreated groups by day 14comparedwith day 7 Interestingly themacrophages appearedto persist in the CTGF treated diabetic animals (119899 =107 macrophages20 fields) compared with the nontreateddiabetic animals (119899 = 73 macrophages20 fields) at day 14although this did not reach statistical significance
Intensity of staining by 120572-SMA a marker of activatedfibroblasts and mature vascular blood vessel cells was mea-sured at days 7 and 14 The fibroblast 120572-SMA in the nondi-abetic rat wounds was higher (Figures 2(a) and 2(b)) thanboth the treated and untreated diabetic animals indicating arelative lack of activated fibroblasts in the diabetic wounds byANOVA (119875 lt 005) Increased120572-SMA staining in endothelialcells was observed at day 7 in control compared with diabeticanimals regardless of treatment (119875 lt 005) (Figures 2(c)and 2(d)) The CTGF topical treatment of diabetic micetrended at day 7 to higher 120572-SMA staining score in fibroblasts(Figure 2(a)) and endothelial cells (Figure 2(c)) comparedwith scores in untreated diabetic mouse although on eachoccasion this did not reach statistical significance Represen-tative images of 120572-SMA staining are shown in Figure 2(e)
Collagen IV staining was lower in untreated diabeticwounds at day 7 and was increased by rhCTGF (119875 lt005) (Figure 3(a)) At day 14 CTGF treated diabetic woundsshowed significant increases in wound collagen IV comparedwith untreated diabetic wounds (119875 lt 0005) (Figure 3(b))Representative collagen IV images for days 7 and 14 from ratswithin respective groups are shown in Figure 4
Journal of Diabetes Research 5
0
05
1
15
2In
tens
ity
C C + CTGF D D + CTGFlowast
lowast
lowastDifferent to C each P lt 005 by ANOVA
(a) Day 7 fibroblasts
0
05
1
15
2
Inte
nsity
C C + CTGF D D + CTGF
(b) Day 14 fibroblasts
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
lowast
by unpaired t-testlowastDifferent to C and C + CTGF combined P lt 005
(c) Day 7 endothelial cells
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
(d) Day 14 endothelial cells
Control Control + rhCTGF Diabetes + PBS Diabetes + rhCTGF
200120583m200120583m 200120583m200120583m
(e) Day 7
Figure 2 Wound 120572-smooth muscle actin staining in fibroblasts and endothelial cells (a) shows 120572-SMA staining intensity scoring infibroblasts in treated control animals compared with the two diabetic animal groups at day 7 lowast119875 lt 005 by ANOVA for each of the groupsmarked versus Control + CTGF No such differences were observed at day 14 in (b) In (c) increased 120572-SMA staining in endothelial cells wasobserved at day 7 in control animals (treated and untreated combined) compared with diabetic animals (treated and untreated combined)lowast
119875 lt 005 by unpaired 119905-test No such differences were observed at day 14 (d) Results are expressed as mean plusmn SEM Representative imagesat day 7 are shown in (e)
34 Endogenous CTGF Changes in Human Diabetic FootUlcer Wound Fluid Postdebridement wound fluid samplesobtained from people with type 2 diabetes who had footulcers were analyzed for CTGF byWestern immunoblot anal-ysis and wound area was determined at each visit based onacetate tracings Figure 5(a) shows a typical cutaneouswoundarea profile in a patient with a neuropathic hallux plantarulcer with times (arrows) when ulcer fluid was collectedand then analyzed the following serial debridements Therespective Western immunoblot analysis for CTGF in theulcer fluid is shown in Figure 5(b) CTGF was detected asa predominant intact sim36ndash38 kDa series of molecular mass
bands typical of known intact CTGF glycoforms [24] Insome immunoblots there was also lower molecular masssignal at sim26 kDa (Figure 5(b)) as previously observed inbiological fluids [18]
The group data (119899 = 32 study subjects) relating ulcerhealing rate to rate of change in CTGF in ulcer fluid acrossan average time period of 10 days showed that an increasein CTGF levels correlates highly significantly with woundhealing rate indicated as percentage reduction in ulcer areaper 10 days (Figure 5(c)) 119903 = 0406 119875 lt 0001 Whilethere was quite marked interindividual variation in the dataon average a 10 increase in CTGF levels in wound fluid
6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Journal of Diabetes Research 3
Table 1 Wound closure data in diabetic and nondiabetic (control) rats each treated with topical rhCTGF or PBS alone
Wound closure ( of initial wound size)Group Day 1 Day 3 Day 7 Day 10 Day 14C + PBS alone 857 plusmn 15 577 plusmn 21 252 plusmn 09lowast 180 plusmn 06 130 plusmn 04DM + PBS alone 928 plusmn 16 617 plusmn 17 310 plusmn 11 207 plusmn 08 159 plusmn 05C + CTGF 817 plusmn 14lowast 522 plusmn 18lowast 256 plusmn 09lowast 165 plusmn 04 132 plusmn 03lowast
DM + CTGF 854 plusmn 14 575 plusmn 22 284 plusmn 12lowast 161 plusmn 07lowast 136 plusmn 04lowast
Results are shown as mean plusmn SEM lowast119875 lt 005 versus the same day diabetic wounds + PBS (DM + PBS alone) by ANOVA The main finding was that ulcerarea was significantly reduced on days 7 10 and 14 in the CTGF treated diabetic group (D + CTGF) compared with the non-rhCTGF treated diabetic group(D + PBS alone)
surface Macrophages from sections obtained at days 7 and14 were identified by immunohistochemical staining withCD68 (Abcam Cambridge MA) as described previously[20] In brief following antigen retrieval nonspecific bindingwas blocked by incubation in 10 vv goat serum andafter washing with PBS the sections were incubated for60min in CD68 (1 200) mouse IgG1 A further PBS washwas carried out before incubation with 1 400 dilution ofsecondary antibody (Biotinylated anti-mouse) Cells werevisualized using peroxidase-conjugated secondary antibodiesand 331015840-diaminobenzidine chromogen (Vector LaboratoriesBurlingame CA)The number of macrophages in 20 sequen-tial fields was determined (attimes1000magnification) by a singleobserver blinded to animal grouping and treatment status
Fibroblast and endothelial cells from sections obtainedat days 7 and 14 were identified by immunohistochemicalstaining using anti-120572-smoothmuscle actin (120572-SMA) primaryantibody 1 200 (120572-SMA Abcam Burlingame CA) andtheir characteristic morphology Detection then involvedsecondary antibody and the ABC method as described forCD68 staining above and as per [20] Cells were stained andvisualized as described formacrophagesThe 120572-SMApositivefibroblasts and endothelial staining intensity within eachwound section was scored by two independent observerseach blinded to animal grouping and treatment status Aspreviously described the scoring was based on a grade of0ndash3 where zero was for no staining up to three for intensestaining and any background staining in the isotype controlsectionwas subtracted from the overall staining score [18 21]
Immunohistochemical staining for collagen IV was per-formed as previously described using the goat generatedanti-collagen IV polyclonal antibody Abcam (Ab86042) at1 200 titer as the primary antibody The subsequent stainingand detection method was that previously used in diabeticpreclinical studies [18 21] with the same scoring method asdescribed for 120572-SMA quantitation above
27 Human Diabetic Foot Ulcer Wound Fluid Analysis Ina separate series of experiments relative CTGF levels inpostdebridement wound fluid in diabetic wounds were deter-mined in patients managed at the multidisciplinary high riskfoot service where all aspects of diabetic foot care had beenoptimized [22 23] (Table 3)Therewere 32 serial subjectswithtype 2 diabetes and each had dense peripheral neuropathyand some were also ischemic ulcers (Table 1) Ethics approval
for this study was obtained from the Human Research EthicsCommittee Sydney South Western Area Health Service
Wound fluid was obtained following debridement usinga sterile 1 cm2 Whatman 4mm filter paper as previouslydescribed [22 23] The protein concentration of the woundfluid was determined using the BioRad protein assay (Bio-Rad Sydney Australia) and a sample containing a standardamount of total protein (30 120583g) was applied to a 125 SDS-PAGEunder reducing conditions as previously described [1824] Western immunoblot analysis using an in-house gener-ated anti-CTGF polyclonal primary antibody (196) at 1 1000titer and subsequent goat anti-rabbit secondary antibody wasundertaken using standardmethods [18]Data determined bydensitometry was then analyzed and presented as changein immunoreactive CTGF in the wound fluid compared with ulcer healing rate across the same time interval In mostcases each wound had 3CTGF measures spread in totalacross 45 or more days
28 Statistical Analysis Wound data is expressed as mean plusmnSD or mean plusmn SEM each as indicated Analysis was per-formed by one way ANOVA with post hoc correction byBonferonirsquos multiple comparison test or by unpaired 119905-testeach as indicated A119875 valuelt 005was considered statisticallysignificant Simple linear correlation analysis was performedfor the human CTGF change in postdebridement woundfluid data in relation to time
3 Results
31 Effect of CTGF on Wound Closure Group data formacroscopic wound closure measurement expressed as apercentage change from the initial wound area at respectivetime points is shown in Table 1 Diabetic animals (D + PBS)were found to have wound closure rates that were slowerthan those in control (nondiabetic) animals (C + PBS) withthis being significant on day 7 In addition macroscopicwound closure was significantly enhanced on days 7 10 and14 in the CTGF treated diabetic group compared with thenonactively treated diabetic group with vehicle alone (D +PBS) Table 1 In contrast to CTGF effects in diabetic woundsnondiabetic wounds treated with CTGF (C + CTGF) did notshow improved closure rates relative to controls alone (C +PBS)
4 Journal of Diabetes Research
Table 2 Wound breaking strength data in all groups
Youngrsquos modulus Tear strength Tear strain Ultimate strength Final strainC + PBS alone 093 plusmn 009 056 plusmn 006 117 plusmn 010 106 plusmn 001 345 plusmn 022lowast
DM + PBS alone 087 plusmn 013 046 plusmn 005 071 plusmn 006 081 plusmn 013 220 plusmn 016C + CTGF 121 plusmn 011 053 plusmn 005 104 plusmn 010 089 plusmn 006 308 plusmn 027lowast
DM + CTGF 101 plusmn 017 053 plusmn 005 087 plusmn 018 086 plusmn 010 232 plusmn 022Data are mean plusmn SD each lowast119875 lt 005 versus DM + PBS by ANOVA
0
50
100
150
200
250
300
C C + CTGF D D + CTGF
lowast
lowast
Mac
roph
ages
(n) p
er20
sect
ions
(a) Day 7
0
50
100
150
200
250
300
C C + CTGF D D + CTGFM
acro
phag
es (n
) per
20
sect
ions
(b) Day 14
Figure 1 Wound macrophage counts (a) CTGF treated (control and diabetic groups combined) is different to CTGF untreated (control anddiabetic groups combined) lowast119875 lt 005 by unpaired 119905-test at day 7 No statistical difference was observed between groups at day 14 (b) Resultsare expressed as mean plusmn SEM
Table 3 Demographics of patients with diabetes who had postde-bridement foot ulcer fluid analyzed
Patient demographicsStudy subject number (119899) 32Age (years)lowast 641 plusmn 18Diabetes duration (years) 176 plusmn 19Gender ( male) 75Ulcer type
Neuropathic only 29Neuroischemic 3
lowastAll data are mean plusmn SD
32 CTGFTherapy and Wound Breaking Strength The effectof CTGF on the wound breaking strength at the woundsite was also measured Analysis by ANOVA showed thatuntreated diabetic wounds elongate less well before breakingthan either treated or untreated control wounds (119875 lt 005)(average 220MPa compared with 308 and 345MPa resp)indicating that diabetic wounds are functionally less flexible(Table 2) CTGF treated diabetic wounds had a slightly highermean final strain (232MPa) than the untreated diabeticwounds (220MPa) however this did not reach statisticalsignificance Youngrsquos modulus which measures stress in rela-tion to strain and thus wound elasticity was not significantlydifferent between groups in this model
33 Effect of CTGF Treatment onWound Cellular Content andMatrix Macrophage cell counts in CD68 stained sections
(Figure 1) were lower in PBS alone treated animals comparedwith CTGF treated animals at day 7 Macrophage cell countdeclined in both treated and untreated groups by day 14comparedwith day 7 Interestingly themacrophages appearedto persist in the CTGF treated diabetic animals (119899 =107 macrophages20 fields) compared with the nontreateddiabetic animals (119899 = 73 macrophages20 fields) at day 14although this did not reach statistical significance
Intensity of staining by 120572-SMA a marker of activatedfibroblasts and mature vascular blood vessel cells was mea-sured at days 7 and 14 The fibroblast 120572-SMA in the nondi-abetic rat wounds was higher (Figures 2(a) and 2(b)) thanboth the treated and untreated diabetic animals indicating arelative lack of activated fibroblasts in the diabetic wounds byANOVA (119875 lt 005) Increased120572-SMA staining in endothelialcells was observed at day 7 in control compared with diabeticanimals regardless of treatment (119875 lt 005) (Figures 2(c)and 2(d)) The CTGF topical treatment of diabetic micetrended at day 7 to higher 120572-SMA staining score in fibroblasts(Figure 2(a)) and endothelial cells (Figure 2(c)) comparedwith scores in untreated diabetic mouse although on eachoccasion this did not reach statistical significance Represen-tative images of 120572-SMA staining are shown in Figure 2(e)
Collagen IV staining was lower in untreated diabeticwounds at day 7 and was increased by rhCTGF (119875 lt005) (Figure 3(a)) At day 14 CTGF treated diabetic woundsshowed significant increases in wound collagen IV comparedwith untreated diabetic wounds (119875 lt 0005) (Figure 3(b))Representative collagen IV images for days 7 and 14 from ratswithin respective groups are shown in Figure 4
Journal of Diabetes Research 5
0
05
1
15
2In
tens
ity
C C + CTGF D D + CTGFlowast
lowast
lowastDifferent to C each P lt 005 by ANOVA
(a) Day 7 fibroblasts
0
05
1
15
2
Inte
nsity
C C + CTGF D D + CTGF
(b) Day 14 fibroblasts
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
lowast
by unpaired t-testlowastDifferent to C and C + CTGF combined P lt 005
(c) Day 7 endothelial cells
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
(d) Day 14 endothelial cells
Control Control + rhCTGF Diabetes + PBS Diabetes + rhCTGF
200120583m200120583m 200120583m200120583m
(e) Day 7
Figure 2 Wound 120572-smooth muscle actin staining in fibroblasts and endothelial cells (a) shows 120572-SMA staining intensity scoring infibroblasts in treated control animals compared with the two diabetic animal groups at day 7 lowast119875 lt 005 by ANOVA for each of the groupsmarked versus Control + CTGF No such differences were observed at day 14 in (b) In (c) increased 120572-SMA staining in endothelial cells wasobserved at day 7 in control animals (treated and untreated combined) compared with diabetic animals (treated and untreated combined)lowast
119875 lt 005 by unpaired 119905-test No such differences were observed at day 14 (d) Results are expressed as mean plusmn SEM Representative imagesat day 7 are shown in (e)
34 Endogenous CTGF Changes in Human Diabetic FootUlcer Wound Fluid Postdebridement wound fluid samplesobtained from people with type 2 diabetes who had footulcers were analyzed for CTGF byWestern immunoblot anal-ysis and wound area was determined at each visit based onacetate tracings Figure 5(a) shows a typical cutaneouswoundarea profile in a patient with a neuropathic hallux plantarulcer with times (arrows) when ulcer fluid was collectedand then analyzed the following serial debridements Therespective Western immunoblot analysis for CTGF in theulcer fluid is shown in Figure 5(b) CTGF was detected asa predominant intact sim36ndash38 kDa series of molecular mass
bands typical of known intact CTGF glycoforms [24] Insome immunoblots there was also lower molecular masssignal at sim26 kDa (Figure 5(b)) as previously observed inbiological fluids [18]
The group data (119899 = 32 study subjects) relating ulcerhealing rate to rate of change in CTGF in ulcer fluid acrossan average time period of 10 days showed that an increasein CTGF levels correlates highly significantly with woundhealing rate indicated as percentage reduction in ulcer areaper 10 days (Figure 5(c)) 119903 = 0406 119875 lt 0001 Whilethere was quite marked interindividual variation in the dataon average a 10 increase in CTGF levels in wound fluid
6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Journal of Diabetes Research
Table 2 Wound breaking strength data in all groups
Youngrsquos modulus Tear strength Tear strain Ultimate strength Final strainC + PBS alone 093 plusmn 009 056 plusmn 006 117 plusmn 010 106 plusmn 001 345 plusmn 022lowast
DM + PBS alone 087 plusmn 013 046 plusmn 005 071 plusmn 006 081 plusmn 013 220 plusmn 016C + CTGF 121 plusmn 011 053 plusmn 005 104 plusmn 010 089 plusmn 006 308 plusmn 027lowast
DM + CTGF 101 plusmn 017 053 plusmn 005 087 plusmn 018 086 plusmn 010 232 plusmn 022Data are mean plusmn SD each lowast119875 lt 005 versus DM + PBS by ANOVA
0
50
100
150
200
250
300
C C + CTGF D D + CTGF
lowast
lowast
Mac
roph
ages
(n) p
er20
sect
ions
(a) Day 7
0
50
100
150
200
250
300
C C + CTGF D D + CTGFM
acro
phag
es (n
) per
20
sect
ions
(b) Day 14
Figure 1 Wound macrophage counts (a) CTGF treated (control and diabetic groups combined) is different to CTGF untreated (control anddiabetic groups combined) lowast119875 lt 005 by unpaired 119905-test at day 7 No statistical difference was observed between groups at day 14 (b) Resultsare expressed as mean plusmn SEM
Table 3 Demographics of patients with diabetes who had postde-bridement foot ulcer fluid analyzed
Patient demographicsStudy subject number (119899) 32Age (years)lowast 641 plusmn 18Diabetes duration (years) 176 plusmn 19Gender ( male) 75Ulcer type
Neuropathic only 29Neuroischemic 3
lowastAll data are mean plusmn SD
32 CTGFTherapy and Wound Breaking Strength The effectof CTGF on the wound breaking strength at the woundsite was also measured Analysis by ANOVA showed thatuntreated diabetic wounds elongate less well before breakingthan either treated or untreated control wounds (119875 lt 005)(average 220MPa compared with 308 and 345MPa resp)indicating that diabetic wounds are functionally less flexible(Table 2) CTGF treated diabetic wounds had a slightly highermean final strain (232MPa) than the untreated diabeticwounds (220MPa) however this did not reach statisticalsignificance Youngrsquos modulus which measures stress in rela-tion to strain and thus wound elasticity was not significantlydifferent between groups in this model
33 Effect of CTGF Treatment onWound Cellular Content andMatrix Macrophage cell counts in CD68 stained sections
(Figure 1) were lower in PBS alone treated animals comparedwith CTGF treated animals at day 7 Macrophage cell countdeclined in both treated and untreated groups by day 14comparedwith day 7 Interestingly themacrophages appearedto persist in the CTGF treated diabetic animals (119899 =107 macrophages20 fields) compared with the nontreateddiabetic animals (119899 = 73 macrophages20 fields) at day 14although this did not reach statistical significance
Intensity of staining by 120572-SMA a marker of activatedfibroblasts and mature vascular blood vessel cells was mea-sured at days 7 and 14 The fibroblast 120572-SMA in the nondi-abetic rat wounds was higher (Figures 2(a) and 2(b)) thanboth the treated and untreated diabetic animals indicating arelative lack of activated fibroblasts in the diabetic wounds byANOVA (119875 lt 005) Increased120572-SMA staining in endothelialcells was observed at day 7 in control compared with diabeticanimals regardless of treatment (119875 lt 005) (Figures 2(c)and 2(d)) The CTGF topical treatment of diabetic micetrended at day 7 to higher 120572-SMA staining score in fibroblasts(Figure 2(a)) and endothelial cells (Figure 2(c)) comparedwith scores in untreated diabetic mouse although on eachoccasion this did not reach statistical significance Represen-tative images of 120572-SMA staining are shown in Figure 2(e)
Collagen IV staining was lower in untreated diabeticwounds at day 7 and was increased by rhCTGF (119875 lt005) (Figure 3(a)) At day 14 CTGF treated diabetic woundsshowed significant increases in wound collagen IV comparedwith untreated diabetic wounds (119875 lt 0005) (Figure 3(b))Representative collagen IV images for days 7 and 14 from ratswithin respective groups are shown in Figure 4
Journal of Diabetes Research 5
0
05
1
15
2In
tens
ity
C C + CTGF D D + CTGFlowast
lowast
lowastDifferent to C each P lt 005 by ANOVA
(a) Day 7 fibroblasts
0
05
1
15
2
Inte
nsity
C C + CTGF D D + CTGF
(b) Day 14 fibroblasts
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
lowast
by unpaired t-testlowastDifferent to C and C + CTGF combined P lt 005
(c) Day 7 endothelial cells
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
(d) Day 14 endothelial cells
Control Control + rhCTGF Diabetes + PBS Diabetes + rhCTGF
200120583m200120583m 200120583m200120583m
(e) Day 7
Figure 2 Wound 120572-smooth muscle actin staining in fibroblasts and endothelial cells (a) shows 120572-SMA staining intensity scoring infibroblasts in treated control animals compared with the two diabetic animal groups at day 7 lowast119875 lt 005 by ANOVA for each of the groupsmarked versus Control + CTGF No such differences were observed at day 14 in (b) In (c) increased 120572-SMA staining in endothelial cells wasobserved at day 7 in control animals (treated and untreated combined) compared with diabetic animals (treated and untreated combined)lowast
119875 lt 005 by unpaired 119905-test No such differences were observed at day 14 (d) Results are expressed as mean plusmn SEM Representative imagesat day 7 are shown in (e)
34 Endogenous CTGF Changes in Human Diabetic FootUlcer Wound Fluid Postdebridement wound fluid samplesobtained from people with type 2 diabetes who had footulcers were analyzed for CTGF byWestern immunoblot anal-ysis and wound area was determined at each visit based onacetate tracings Figure 5(a) shows a typical cutaneouswoundarea profile in a patient with a neuropathic hallux plantarulcer with times (arrows) when ulcer fluid was collectedand then analyzed the following serial debridements Therespective Western immunoblot analysis for CTGF in theulcer fluid is shown in Figure 5(b) CTGF was detected asa predominant intact sim36ndash38 kDa series of molecular mass
bands typical of known intact CTGF glycoforms [24] Insome immunoblots there was also lower molecular masssignal at sim26 kDa (Figure 5(b)) as previously observed inbiological fluids [18]
The group data (119899 = 32 study subjects) relating ulcerhealing rate to rate of change in CTGF in ulcer fluid acrossan average time period of 10 days showed that an increasein CTGF levels correlates highly significantly with woundhealing rate indicated as percentage reduction in ulcer areaper 10 days (Figure 5(c)) 119903 = 0406 119875 lt 0001 Whilethere was quite marked interindividual variation in the dataon average a 10 increase in CTGF levels in wound fluid
6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
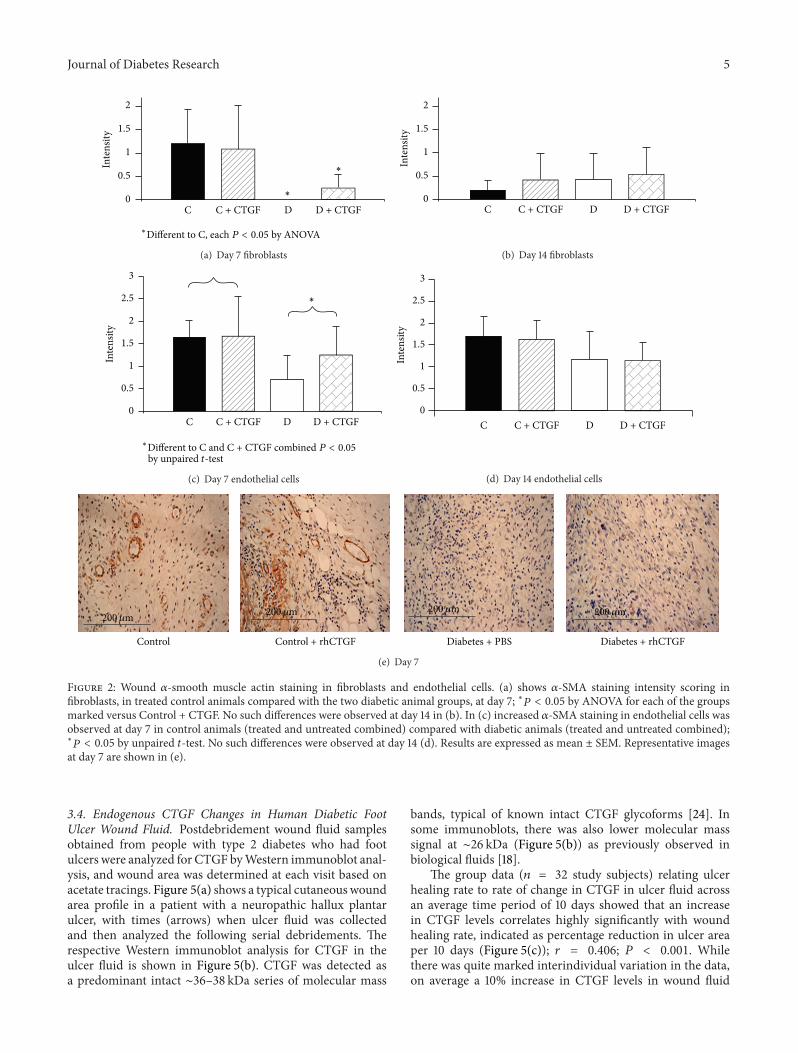
Journal of Diabetes Research 5
0
05
1
15
2In
tens
ity
C C + CTGF D D + CTGFlowast
lowast
lowastDifferent to C each P lt 005 by ANOVA
(a) Day 7 fibroblasts
0
05
1
15
2
Inte
nsity
C C + CTGF D D + CTGF
(b) Day 14 fibroblasts
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
lowast
by unpaired t-testlowastDifferent to C and C + CTGF combined P lt 005
(c) Day 7 endothelial cells
0
05
1
15
2
25
3
Inte
nsity
C C + CTGF D D + CTGF
(d) Day 14 endothelial cells
Control Control + rhCTGF Diabetes + PBS Diabetes + rhCTGF
200120583m200120583m 200120583m200120583m
(e) Day 7
Figure 2 Wound 120572-smooth muscle actin staining in fibroblasts and endothelial cells (a) shows 120572-SMA staining intensity scoring infibroblasts in treated control animals compared with the two diabetic animal groups at day 7 lowast119875 lt 005 by ANOVA for each of the groupsmarked versus Control + CTGF No such differences were observed at day 14 in (b) In (c) increased 120572-SMA staining in endothelial cells wasobserved at day 7 in control animals (treated and untreated combined) compared with diabetic animals (treated and untreated combined)lowast
119875 lt 005 by unpaired 119905-test No such differences were observed at day 14 (d) Results are expressed as mean plusmn SEM Representative imagesat day 7 are shown in (e)
34 Endogenous CTGF Changes in Human Diabetic FootUlcer Wound Fluid Postdebridement wound fluid samplesobtained from people with type 2 diabetes who had footulcers were analyzed for CTGF byWestern immunoblot anal-ysis and wound area was determined at each visit based onacetate tracings Figure 5(a) shows a typical cutaneouswoundarea profile in a patient with a neuropathic hallux plantarulcer with times (arrows) when ulcer fluid was collectedand then analyzed the following serial debridements Therespective Western immunoblot analysis for CTGF in theulcer fluid is shown in Figure 5(b) CTGF was detected asa predominant intact sim36ndash38 kDa series of molecular mass
bands typical of known intact CTGF glycoforms [24] Insome immunoblots there was also lower molecular masssignal at sim26 kDa (Figure 5(b)) as previously observed inbiological fluids [18]
The group data (119899 = 32 study subjects) relating ulcerhealing rate to rate of change in CTGF in ulcer fluid acrossan average time period of 10 days showed that an increasein CTGF levels correlates highly significantly with woundhealing rate indicated as percentage reduction in ulcer areaper 10 days (Figure 5(c)) 119903 = 0406 119875 lt 0001 Whilethere was quite marked interindividual variation in the dataon average a 10 increase in CTGF levels in wound fluid
6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Journal of Diabetes Research
0
05
1
15
2
25In
tens
ity
C C + CTGF D D + CTGF
lowast
lowastP lt 005 by ANOVA
(a) Day 7
0
05
1
15
2
25
Inte
nsity
C C + CTGF D D + CTGFlowastP lt 005 by ANOVA
lowast
(b) Day 14
Figure 3Wound collagen IV staining (a) shows collagen IV staining was lagging in untreated diabetic wounds at day 7 lowast119875 lt 005 comparedwith Control + CTGF treated animals by ANOVA (b) shows at day 14 the CTGF treated diabetic animals showed significantly increasedcollagen IV compared with the other groups lowast119875 lt 005 by ANOVA Results are expressed as mean plusmn SEM
Day 7
Day 14
Figure 4 Wound collagen IV staining images Representative images reflect that collagen IV is increased at day 14 in CTGF treated diabeticrodent wounds relative to the other groups and remained at a level similar to that observed at day 7
across 10 days correlated with sim176 improvement (ie areduction) in ulcer area (Figure 5(c))
4 Discussion
In diabetic wounds healing is known to be impaired byseveral abnormalities including prolonged inflammationimpaired neovascularisation decreased synthesis of collagenand defective macrophage functions [6] CTGF has beenshown in vitro to be important in wound healing [25] and toaccelerate healing rate of burns in rhesus monkeys [13]
The current study shows that topical application of CTGFimproves wound healing in a diabetic rodent model of fullthickness cutaneous wound healing The main end pointrate of epithelial closure as a percentage of original woundsize was accelerated in the group of diabetic rats that were
treated with CTGF This was demonstrated by the serialmeasurement of wound area over time Occlusion of thewounds using a semipermeable filmdressing ldquoTegadermrdquo fur-ther validates this model as occlusion enabled more accuratevisualisation of the wound as no scab or foreign matter wasable to distort or contaminate the wound Furthermore it hasbeen shown that in diabetic rodent models the film dressingexerts a ldquosplintingrdquo effect to the wound margins and con-traction thus promoting healing through reepithelialization[26]which better approximates humanwoundhealing ratherthan through contractionwhich predominates in nonsplintedrodent wounds
A lack of detectable effect of CTGF on control woundsindicates that CTGF is able to normalise certain deficits foundwithin diabetic wounds without affecting healing in normalwounds It is possible that CTGF is able to improve wound
Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Journal of Diabetes Research 7
00102030405
0 6 15 36 50 62 92 120Time of treatment (days)
Ulc
er ar
ea (c
m2)
(a) Typical pattern of foot ulcer cutaneous healing
Intact CTGF
Day of wound fluid collection6 36 62 Lower molecular
mass CTGF
(sim36ndash38kDa)
signal (sim26kDa)
(b) CTGF wound fluid analysis
minus60 minus40 minus20 0 20 40 60 80
20
10
0
minus10
minus20
minus30
minus40
minus50
minus60
Change in CTGF level10 days ()
Chan
ge in
ulc
er ar
ea10
day
s (
)y = minus0344x minus 14145
R2 = 0165
P lt 0001
(c) Change in immunoreactive CTGF versus change in ulcer area per10 days
Figure 5 Endogenous ulcer fluid CTGF and diabetic foot ulcer healing In (a) ulcer area versus time is shown for a typical small hallux plantarulcer with the arrows indicating sampling of postdebridement ulcer fluid The ulcer fluid in (a) was analyzed by Western Immunoblot todetect CTGF immunoreactivity under nonreducing conditions as shown in (b) Both intact monomeric CTGF and a lower molecular masssim26 kDa CTGF are observed Images such as those in Figure 5(b) were quantitated by densitometry to compare change in ulcer fluid CTGFimmunoreactivity versus change in ulcer area each across 10 days In (c) CTGF was found to increase as ulcer area reduced (1198772 = 0165119875 lt 0001)
healing through augmentation of cellular chemotaxis andmitosis andor through upregulation of related mediatorsof CTGF such as TGF-120573 These actions may attenuate thepersistent inflammation which is detrimental within the dia-betic woundThemonkey cutaneous burns model previouslypublished that also responded to rhCTGF topically withulcer closure [13] also has a proinflammatory environmentsuggesting that rhCTGF may be working through suchmechanism in cutaneous wounds
The beneficial effect of the rhCTGF therapy in terms ofepithelial closure appeared to occur quite early in woundhealing A CTGF effect was observed in diabetic woundswhich was statistically significant by day 7 after woundingIn this context it is notable that CTGF is known to inducemacrophage chemotaxis [27] In addition application ofmacrophages or stem cells onto diabetic rodent woundshas been shown to accelerate wound healing and epithe-lial closure [28] In the current work while it appearsthat macrophage number was increased in wounds treatedwith CTGF this was not statistically significant It maybe that some of the CTGF effect was through inductionof macrophage presence in diabetic wounds increasedmacrophage infiltration observed within the CTGF treateddiabetic wounds at day 7 cosegregated with acceleratedhealing of these wounds In turn macrophages upreg-ulate healing through their inflammatory and reparativephenotypes and the balance between inflammatory andrepair macrophages is crucial for successful healing [29]
Inflammatory macrophages synthesize a plethora of growthfactors which in turn attract fibroblasts and endothe-lial cells and promote their proliferation [30] Reparativemacrophages also support ECM remodeling [29]
The finding that Youngrsquos modulus was lower in thediabetic animals than the controls is in keeping with recentliterature [31] Interestingly Youngrsquos modulus was increasedby 119905-test (119875 lt 005) in animals that were treated with CTGFcompared to untreated animals regardless of diabetes statusIt is likely that the observed increase in collagen IV seen inearlier experiments after CTGF treatment is contributing tothe greater stiffness of the wound sites Collagen is knownto contribute to wound strength and therefore increasedstiffness and strain in CTGF treated wounds is probablyattributable to increased collagen IV in these tissues Theseobservations are consistent with similar findings for othergrowth factors such as PDGF where treatment inducedcollagen IV and increased strength in corneal tissue [32] andin preclinical models of diabetic ulceration [33]
Collagen IV was markedly increased in CTGF treateddiabetic ulcers compared with both untreated diabetic ulcersand controlsThis formation shows progression of the woundto remodeling and therefore end stage repair Collagen IVpeptides have been shown to promote cell adhesion andmigration in corneal epithelial cells [34]The overall collagenprotein content of a wound is determined by the balancebetween collagen production and absorption [7] andMMP 9is a key regulator of collagen IV [6]Thedirect effects ofCTGF
8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Journal of Diabetes Research
onMMP activity have not been extensively studied Howeverrecently we reported that CTGF upregulates the expressionof TIMP-1 an MMP inhibitor in mesangial cells [19] andWang et al reported earlier that rhCTGF induced TIMP-1 and TIMP-2 in porcine skin [35] It is therefore possiblethat increased collagen content in the diabetic wound isattributable to CTGF mediated upregulation of TIMPS andcorresponding inhibition of MMP 9
CTGF treatment increased expression of smooth muscleactin in both fibroblast and endothelial cells This findingis similar to the enhanced expression of 120572-SMA seen insubcutaneous rat fibroblasts following treatment with trans-forming growth factor-1205731 [36 37] Both endothelial celland fibroblast expression of 120572-SMA are robust predictors ofhealing [38] Increased 120572-SMA in these cells is indicative thatthe wound is progressing from the inflammatory phase andthat contraction remodeling and closure are occurring at anaccelerated rate While some recent reports have implicatedCTGFCCN2 in postwound scar formation [39 40] we didnot observe macroscopic excessive scarring in the treatedCTGFCCN2 wounds although the planned limited studyduration may have prevented optimal detection of such achange This lack of late time point assessment is a limitationof the current study As the wound breaking strength datashow no marked change in final strain after CTGF treatmentof wounds it is likely that fibrosis is not induced significantlyin this model by rhCTGF However future studies in diabeticcutaneous wounding will be required to formally address thatissue of any potential late histological fibrosis induction byrhCTGF which was not the primary focus of the currentresearch
This is the first time that changes in endogenousCTGFCCN2 have been reported in human diabetic footulcers or related ulcer fluid Across a series of samples in32 study subjects we have found that as immunoreactiveCTGF increases in the postdebridement ulcer fluid the ulcerdemonstrates signs of healing CTGF is known to be inducedduring wounding of human skin [41 42] This data supportsthe concept that CTGF may have a role in ulcer healingin diabetes and combined with the rodent data describedin this paper and our previous data in a primate non-human (baboon)model of diabetic wounding [18] it providesgreater rationale for studying CTGF as therapy in diabeticfoot ulcers The correct dosing and timing schedule as wellas whether CTGF should be used alone in combinationwith other growth factors [43] such as in matrix [44] orprotease inhibitors [45] or in expression vectors remains tobe defined
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors thank the Diabetes Centre Podiatry staff for theirassistance in collecting human wound fluid and Diabetes
Australia Research Trust and Novo Nordisk for RegionalDiabetes Support Scheme for competitive funding support ofthis study
References
[1] J Bentley and A Foster ldquoMultidisciplinary management of thediabetic foot ulcerrdquo British Journal of Community Nursing vol12 pp S6ndashS10 2007
[2] R SMost andP Sinnock ldquoThe epidemiology of lower extremityamputations in diabetic individualsrdquo Diabetes Care vol 6 no1 pp 87ndash91 1983
[3] WHVanHoutumandLA Lavery ldquoOutcomes associatedwithdiabetes-related amputations in theNetherlands and in the stateof California USArdquo Journal of Internal Medicine vol 240 no 4pp 227ndash231 1996
[4] J S Wrobel J A Mayfield and G E Reiber ldquoGeographicvariation of lower-extremity major amputation in individualswith andwithout diabetes in theMedicare populationrdquoDiabetesCare vol 24 no 5 pp 860ndash864 2001
[5] A Gordois P Scuffham A Shearer A Oglesby and J ATobian ldquoThehealth care costs of diabetic peripheral neuropathyin the USrdquo Diabetes Care vol 26 no 6 pp 1790ndash1795 2003
[6] V Falanga ldquoWound healing and its impairment in the diabeticfootrdquoThe Lancet vol 366 no 9498 pp 1736ndash1743 2005
[7] W K Stadelmann A G Digenis and G R Tobin ldquoPhysiologyand healing dynamics of chronic cutaneous woundsrdquo TheAmerican Journal of Surgery vol 176 no 2 supplement 1 pp26Sndash38S 1998
[8] P Bork ldquoThe modular architecture of a new family of growthregulators related to connective tissue growth factorrdquo FEBSLetters vol 327 no 2 pp 125ndash130 1993
[9] A Daniels M van Bilsen R Goldschmeding G J Van DerVusse and F A Van Nieuwenhoven ldquoConnective tissue growthfactor and cardiac fibrosisrdquoActa Physiologica vol 195 no 3 pp321ndash338 2009
[10] C Fonseca G E Lindahl M Ponticos et al ldquoA polymorphismin the CTGF promoter region associated with systemic sclero-sisrdquo The New England Journal of Medicine vol 357 no 12 pp1210ndash1220 2007
[11] G Yosimichi T Nakanishi T Nishida T Hattori T Takano-Yamamoto and M Takigawa ldquoCtgfhcs24 induces chondro-cyte differentiation through a p38 mitogen-activated pro-tein kinase (p38mapk) and proliferation through a p4442mapkextracellular-signal regulated kinase (erk)rdquo EuropeanJournal of Biochemistry vol 268 no 23 pp 6058ndash6065 2001
[12] DM Bradham A Igarashi R L Potter and G R GrotendorstldquoConnective tissue growth factor a cysteine-rich mitogensecreted by human vascular endothelial cells is related to theSRC-induced immediate early gene product CEF-10rdquo Journal ofCell Biology vol 114 no 6 pp 1285ndash1294 1991
[13] L-D Liu H-J Shi L Jiang et al ldquoThe repairing effect of arecombinant human connective-tissue growth factor in a burn-wounded rhesus-monkey (Macacamulatta)modelrdquoBiotechnol-ogy and Applied Biochemistry vol 47 no 2 pp 105ndash112 2007
[14] S M Twigg and M E Cooper ldquoThe time has come to targetconnective tissue growth factor in diabetic complicationsrdquoDiabetologia vol 47 no 6 pp 965ndash968 2004
[15] S Wang M DeNichilo C Brubaker and R HirschbergldquoConnective tissue growth factor in tubulointerstitial injury of
Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Journal of Diabetes Research 9
diabetic nephropathyrdquo Kidney International vol 60 no 1 pp96ndash105 2001
[16] K J Way K Isshiki K Suzuma et al ldquoExpression of connec-tive tissue growth factor is increased in injured myocardiumassociated with protein kinase C beta2 activation and diabetesrdquoDiabetes vol 51 no 9 pp 2709ndash2718 2002
[17] D R Hinton C Spee S He et al ldquoAccumulation of NH2-terminal fragment of connective tissue growth factor in thevitreous of patients with proliferative diabetic retinopathyrdquoDiabetes Care vol 27 no 3 pp 758ndash764 2004
[18] S E Thomson S V McLennan A Hennessy et al ldquoA novelprimate model of delayed wound healing in diabetes dysregu-lation of connective tissue growth factorrdquo Diabetologia vol 53no 3 pp 572ndash583 2010
[19] S V McLennan X Y Wang V Moreno D K Yue and SM Twigg ldquoConnective tissue growth factor mediates highglucose effects on matrix degradation through tissue inhibitorof matrix metalloproteinase type 1 implications for diabeticnephropathyrdquo Endocrinology vol 145 no 12 pp 5646ndash56552004
[20] S V McLennan J Bonner S Milne et al ldquoThe anti-inflammatory agent Propolis improves wound healing in arodent model of experimental diabetesrdquo Wound Repair andRegeneration vol 16 no 5 pp 706ndash713 2008
[21] S E Thomson S V McLennan P D Kirwan et al ldquoRenalconnective tissue growth factor correlates with glomerularbasement membrane thickness and prospective albuminuria ina non-human primate model of diabetes possible predictivemarker for incipient diabetic nephropathyrdquo Journal of Diabetesand Its Complications vol 22 no 4 pp 284ndash294 2008
[22] Y Liu D Min T Bolton et al ldquoIncreased matrix metallopro-teinase-9 predicts poor wound healing in diabetic foot ulcersrdquoDiabetes Care vol 32 no 1 pp 117ndash119 2009
[23] L Xu S V McLennan L Lo et al ldquoBacterial load predictshealing rate in neuropathic diabetic foot ulcersrdquo Diabetes Carevol 30 no 2 pp 378ndash380 2007
[24] C Tikellis M E Cooper S M Twigg W C Burns and MTolcos ldquoConnective tissue growth factor is up-regulated in thediabetic retina amelioration by angiotensin-converting enzymeinhibitionrdquo Endocrinology vol 145 no 2 pp 860ndash866 2004
[25] Y Chen D J Abraham X Shi-Wen et al ldquoCCN2 (con-nective tissue growth factor) promotes fibroblast adhesion tofibronectinrdquo Molecular Biology of the Cell vol 15 no 12 pp5635ndash5646 2004
[26] P V Peplow T-Y Chung and G D Baxter ldquoLaser photo-biomodulation of wound healing a review of experimentalstudies in mouse and rat animal modelsrdquo Photomedicine andLaser Surgery vol 28 no 3 pp 291ndash325 2011
[27] I Cicha A Yilmaz M Klein et al ldquoConnective tissue growthfactor is overexpressed in complicated atherosclerotic plaquesand induces mononuclear cell chemotaxis in vitrordquo Arterioscle-rosis Thrombosis amp Vascular Biology vol 25 no 5 pp 1008ndash1013 2005
[28] H V Waugh and J A Sherratt ldquoMacrophage dynamics indiabetic wound healingrdquo Bulletin of Mathematical Biology vol68 no 1 pp 197ndash207 2006
[29] L A DiPietro ldquoWound healing the role of the macrophage andother immune cellsrdquo Shock vol 4 no 4 pp 233ndash240 1995
[30] R D Stout C Jiang B Matta I Tietzel S K Watkins andJ Suttles ldquoMacrophages sequentially change their functionalphenotype in response to changes in microenvironmental
influencesrdquoThe Journal of Immunology vol 175 no 1 pp 342ndash349 2005
[31] D P Greenwald S Shumway L S Zachary et al ldquoEndogenousversus toxin-induced diabetes in rats a mechanical comparisonof two skin wound-healing modelsrdquo Plastic and ReconstructiveSurgery vol 91 no 6 pp 1087ndash1093 1993
[32] S Murali D R Hardten S DeMartelaere et al ldquoEffect of top-ically administered platelet-derived growth factor on cornealwound strengthrdquo Current Eye Research vol 13 no 12 pp 857ndash862 1994
[33] H Li X Fu L Zhang Q Huang Z Wu and T Sun ldquoResearchof PDGF-BB gel on the wound healing of diabetic rats and itspharmacodynamicsrdquo Journal of Surgical Research vol 145 no1 pp 41ndash48 2008
[34] J D Cameron A P N Skubitz and L T Furcht ldquoTypeIV collagen and corneal epithelial adhesion and migrationeffects of type IV collagen fragments and synthetic peptides onrabbit corneal epithelial cell adhesion and migration in vitrordquoInvestigative Ophthalmology and Visual Science vol 32 no 10pp 2766ndash2773 1991
[35] J F Wang M E Olson D K Ball D R Brigstock and D AHart ldquoRecombinant connective tissue growth factor modulatesporcine skin fibroblast gene expressionrdquo Wound Repair andRegeneration vol 11 no 3 pp 220ndash229 2003
[36] L Ronnov-Jessen and O W Petersen ldquoInduction of alpha-smooth muscle actin by transforming growth factor-beta 1in quiescent human breast gland fibroblasts Implications formyofibroblast generation in breast neoplasiardquo Laboratory Inves-tigation vol 68 no 6 pp 696ndash707 1993
[37] A Desmouliere A Geinoz F Gabbiani and G GabbianildquoTransforming growth factor-1205731 induces 120572-smooth muscleactin expression in granulation tissue myofibroblasts and inquiescent and growing cultured fibroblastsrdquo Journal of CellBiology vol 122 no 1 pp 103ndash111 1993
[38] M H Katz A F Alvarez R S Kirsner W H Eaglstein andV Falanga ldquoHuman wound fluid from acute wounds stimulatesfibroblast and endothelial cell growthrdquo Journal of the AmericanAcademy of Dermatology vol 25 no 6 I pp 1054ndash1058 1991
[39] XHuHWang J Liu et al ldquoThe role of ERK and JNK signalingin connective tissue growth factor induced extracellular matrixprotein production and scar formationrdquo Archives of Dermato-logical Research vol 305 no 5 pp 433ndash445 2013
[40] J-S Kim I-GChoi B-C Lee et al ldquoNeuregulin inducesCTGFexpression in hypertrophic scarring fibroblastsrdquoMolecular andCellular Biochemistry vol 365 no 1-2 pp 181ndash189 2012
[41] E Kiwanuka F Hackl E J Caterson et al ldquoCCN2 is tran-siently expressed by keratinocytes during re-epithelializationand regulates keratinocyte migration in vitro by the ras-MEK-ERK signaling pathwayrdquo Journal of Surgical Research vol 185no 2 pp e109ndashe119 2013
[42] M P Alfaro D L Deskins M Wallus et al ldquoA physiologicalrole for connective tissue growth factor in early wound healingrdquoLaboratory Investigation vol 93 no 1 pp 81ndash95 2013
[43] B Orcajo F Muruzabal M C Isasmendi et al ldquoThe use ofplasma rich in growth factors (PRGF-Endoret) in the treatmentof a severe mal perforant ulcer in the foot of a person withdiabetesrdquo Diabetes Research and Clinical Practice vol 93 no 2pp e65ndashe67 2011
10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 Journal of Diabetes Research
[44] M Yao K Attalla Y Ren M A French and V R Driver ldquoEaseof use safety and efficacy of integra bilayer woundmatrix in thetreatment of diabetic foot ulcers in an outpatient clinical settinga prospective pilot studyrdquo Journal of the American PodiatricMedical Association vol 103 no 4 pp 274ndash280 2013
[45] R Marfella F C Sasso M R Rizzo et al ldquoDipeptidyl peptidase4 inhibition may facilitate healing of chronic foot ulcers inpatients with type 2 diabetesrdquo Experimental Diabetes Researchvol 2012 Article ID 892706 11 pages 2012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom





























