Embed Size (px)
Citation preview

Treatment of Internal Root Resorption with MTA: Case Reports Review
Subject: PTD IIAdvisers: Arlinda Luzi Luzi, Mar Jovani Sancho, Raquel GonzalezStudent: Chen-Che Hung (Victor)
1
Abstract Root resorption is a dental complication especially involved in endodontic treatment, which represents a clinical challenge. The failure could lead to dental loss. Factors of resorption could be dental trauma, surgical procedures, excessive pressure or irritation from bleaching agents.[1] Internal root resorption has not been proven to be hereditary or to be contagious. The process is slow to advance and therefore many cases are not detected until the painful response from the patients. As mineral trioxide aggregate (MTA) has been indicated for the treatment because of its sealing ability, biocompatibility and potential induction of osteogenesis and cementogenesis.2 The following case reviews represent the diagnosis, treatment methods and the results of the use of MTA in internal root resorption.
Introduction Root resorption is a complex dental application that can lead to dental loss. Di fferent c lassificat ions are made according to the cause and location.[1]
Including the inflammatory root resorption, w h e t h e r i s p r e d e n t i n o r o n t h e precementum. Dental trauma, surgical procedures, excessive pressure and irritation from bleaching agents are also considered as one of the causes.[1] Majorly with two types of root resorption depending on the location, external and internal root resorption. In advanced stages, it is often very difficult to distinguish external from internal root resorption and aiming at a more predictable outcome some clinicians suggest extraction of the tooth and implant treatment.[2] Generally speaking, external root resorption is similar to internal root resorption but the resorption occurs from the outside and goes inwards. It is caused by an injury to the external surface and
occurs resorption in following weeks. Internal root resorption is a rare condition in permanent teeth, characterized by progressive loss of tooth substance staring from the root canal wall. It is caused by transformation of normal pulp tissue into granulomatous tissue with giant cells, which resorb dentin.[3] Traumatic injury, infection and orthodontic treatment have been suggested as etiological factors for internal resorption.[2] Usually the internal root resorbing process is asymptomatic and diagnosed upon routine radiographic examination. The appearance in the radiograph is an uniform, round-to-oval radiolucent enlargement of the canal.[4] The margins are smooth and clearly defined, with distortion of the original root canal outline. If the internal resorption involves the crown, a pink area may show through the enamel, referred to as a “pink spot.”[3] It is common to detect the symptoms because of the routine checking

2
or the painful response from the patients. Sometimes it can be discovered in an advanced stage that no guarantee of success is certain even in a well-done treatment. In order to control the internal root root resorption, it is necessary to treat the root canal aiming to remove all the pulp tissue and achieve a posterior better sealing. So as to avoid gaps and infection, thermoplasticized gutta-percha fillings are the most commonly techniques used.[1]
Mineral trioxide aggregate (MTA) was proposed by Torabinejad et al. And has been indicated in the literature for the treatment of resorptions, specially when there i s commun ica t ion w i th the periodontium.[1] MTA is a material for perforation repair that has offered many favorable properties, including good sealing ability, biocompatibility, radiopacity, and moisture resistance. Those properties have promoted the use of MTA for sealing purpose in cases of perforation and internal root resorption.[4] In another case report, also mention the properties of MTA with potential induction of osteogenesis and cementogenesis and could be used in a humid environment. Studies using an experimental immature tooth model, demonstrated that the MTA also increased the fracture resistance of bovine incisors when submitted to different reinforcement treatments.[2] Thus, MTA is a suitable material for the treatment of root perforations with the goal of regenerating a periodontal attachment. It has suggested indications for root-end filling, pulp capping, apical filling of teeth with open apices, apexification therapy, and repair of root perforations.[3] Although the properties of MTA are well described, it
has not been employed very frequently in the treatment of internal root resorption.[4]
Case ReportClinical case report concluding journals treating internal root resorption in different tooth and region of the oral cavity.
[Case 1]Initial internal root resorption. Male patient, aged 52, attended to private office for evaluation and if possible, treatment of maxillary left canine. Clinically the tooth s h o w e d u p healthy, except for an alteration of color. The patient did not p r e s e n t a n y symptoms but t h e radiographical exam showed a large internal r e s o r p t i o n , w h i c h w a s communicating w i t h t h e p e r i o d o n t a l ligament (Fig.1).[1] The coronary access was performed and the chemical-mechanical preparation was difficult, the root canal system was extensively irrigated with sodium hypochlorite at 2,5%.[1]
It was used ad an intracanal dressing a calcium hydroxide paste with a viscous hydrosoluble vehicle (polyethylene glycol) and iodoform. The dressing was changed and reapplied for six weeks till the complete filling of the pulp cavity (Fig.2).[1]
Because of the extensive area in the canal, filling white MTA (Angelous) is
Figure 1Initial internal root resorption. (case 1)

3
recommended (Fig.3). The coronal cavity was sealed with glass ionomer cement. Follow-up were performed after 1 month, 6 months, 12 months and 2 years after the conclusion of the case. It is worth to highlight that the patient had no pain, no increasing of volume, normal space on the periodontal ligament, no mobility of the tooth and the radiography indicated that the resorption was paralyzed.[1]
[Case 2]A 32-year-old female patient attended to endodontic clinic complaining of recurrent pain and inflammation in the buccal region of the maxillary right lateral incisor. The
tooth had been traumatized in a bicycle accident during childhood, w h i c h w a s followed by root canal treatment.[2]
A sinus trace was observed upon c l i n i c a l examination (Fig.5). Radiographic e x a m i n a t i o n revealed faulty e n d o d o n t i c treatment, with i n a d e q u a t e s h a p i n g a n d fi l l i n g . T h e presence of a r a d i o l u c e n t image was also no ted in the middle third of t h e r o o t i n t e r n a l l y, i n add i t ion to a circumscribed bone rarefaction at the same level, suggesting perforating internal root resorption (Fig.6).[2] During the first session, after placement of a rubber dam, the root canal filling was removed with the aid of eucalyptol and K-files, under a surgical microscope (DF Vasconcellos, Belo Hor izonte, MG, Brazi l ) at a magnification of 16×. The canal was then gently irr igated with 2.5% sodium hypochlorite using a 27-gauge needle connected to a disposable 5-ml syringe with simultaneous aspiration in order to avoid accidental injection of hypochlorite into the periodontal t issues. After determination of the working length (WL) 1
Figure 2C a l c i u m h y d r o x i d e dressing - last change. (case 1)
Figure 3 Rot canal filled in all its extension with white MTA. (case 1)
Figure 4 2 years fo l low-up. (case 1)
Figure 5The sinus tract. (case 2)
Figure 6Radiographic examination suggested per fora t ing internal root resorption. (case 2)

4
mm short of the apex, chemo-mechanical preparation was performed with K-files up to #50 by the step-back technique followed by final irrigation with 17% EDTA solution (Biodinámica Química e Farmacêutica Ltda, Ibiporã, Paraná, Brazil) for 3 min. Next, a calcium hydroxide paste with saline was applied for 30 days (Fig. 7).[2]
After coronal sealing with Cavit (3M ESPE, Seefeld, Germany), the rubber dam was removed and extrusion of paste was observed through the sinus tract (Fig. 8).
The root canal dress ing was changed 4 times in an 8-month period, by the end of which the sinus tract had d i s a p p e a r e d (Fig. 9). Before r o o t c a n a l
obturation, the c a l c i u m hydroxide paste
was removed from the root canal using the working length file and the canal was irrigated with 2.5% sodium hypochlorite
so lu t ion , f o l l o w e d b y fi n a l i r r igat ion with 2 ml o f EDTA for 3 min and drying w i t h absorbent paper points. With the aid of a cal ibrat ion ruler, a medium point extending up to 1 mm from the WL was selected and then passively inserted into the root canal with a small amount of endodontic sealer (Pulp canal sealer, Ker r Sybron Denta l Spec ia l t ies , Glendora, CA, USA), taking care to avoid extrusion into the resorbed area. The point was partially removed using the System B (SybronEndo Corporation, Orange, CA, USA) with a Buchanam FM (fine med ium) p lugger (Ana ly t i c Endodontics, Redmond, WA, USA) in the touch mode at 200oC and full power at 10 s, leaving 4 mm of apical filling (Fig. 10). Subsequently, aided with the surgical microscope, MTA (Gray Pro Root Maillefer, Ballaigues, Switzerland) was inserted with slight pressure into the resorption area with the aid of an amalgam carrier and Schilder pluggers, after which a periapical radiograph was taken (Fig.11). After placement of MTA, a cotton pellet soaked in saline was placed to stimulate material setting, and the cavity was sealed with temporary restorative material.In the following session, 24 hours later, MTA setting was checked and the coronal opening on the palatal aspect was restored with light-cured resin. In the followup after 11 years and 8 months, clinical examination
Figure 7Roo t cana l w i t h calcium hydroxide dressing.
Figure 8Extrusion of calcium h y d r o x i d e d r e s s i n g through the sinus tract.
Figure 9Buccal mucosa with no sinus tract.
5
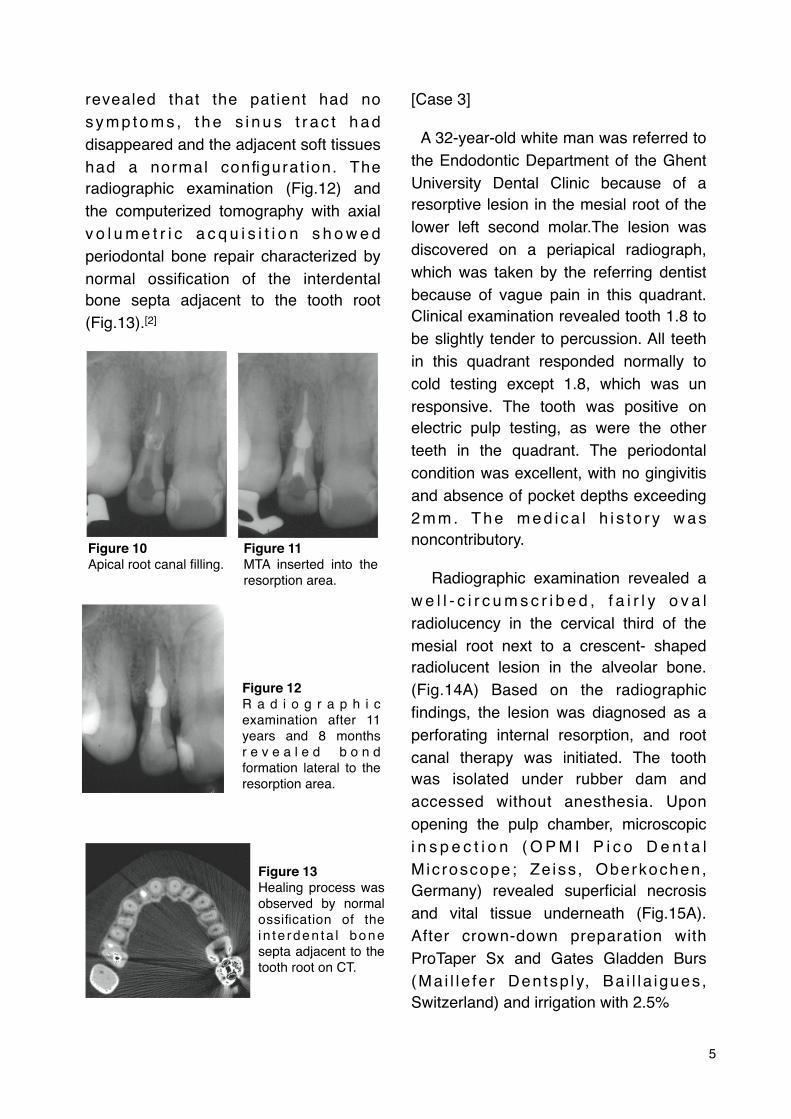
revealed that the patient had no s y m p t o m s , t h e s i n u s t r a c t h a d disappeared and the adjacent soft tissues had a normal configurat ion. The radiographic examination (Fig.12) and the computerized tomography with axial v o l u m e t r i c a c q u i s i t i o n s h o w e d periodontal bone repair characterized by normal ossification of the interdental bone septa adjacent to the tooth root (Fig.13).[2]
[Case 3]
A 32-year-old white man was referred to the Endodontic Department of the Ghent University Dental Clinic because of a resorptive lesion in the mesial root of the lower left second molar.The lesion was discovered on a periapical radiograph, which was taken by the referring dentist because of vague pain in this quadrant. Clinical examination revealed tooth 1.8 to be slightly tender to percussion. All teeth in this quadrant responded normally to cold testing except 1.8, which was un responsive. The tooth was positive on electric pulp testing, as were the other teeth in the quadrant. The periodontal condition was excellent, with no gingivitis and absence of pocket depths exceeding 2 m m . T h e m e d i c a l h i s t o r y w a s noncontributory.
Radiographic examination revealed a w e l l - c i r c u m s c r i b e d , f a i r l y o v a l radiolucency in the cervical third of the mesial root next to a crescent- shaped radiolucent lesion in the alveolar bone. (Fig.14A) Based on the radiographic findings, the lesion was diagnosed as a perforating internal resorption, and root canal therapy was initiated. The tooth was isolated under rubber dam and accessed without anesthesia. Upon opening the pulp chamber, microscopic i n s p e c t i o n ( O P M I P i c o D e n t a l M ic roscope; Ze iss , Oberkochen, Germany) revealed superficial necrosis and vital tissue underneath (Fig.15A). After crown-down preparation with ProTaper Sx and Gates Gladden Burs (Ma i l l e fe r Den tsp ly, Ba i l l a igues , Switzerland) and irrigation with 2.5%
Figure 10Apical root canal filling.
Figure 11MTA inserted into the resorption area.
Figure 12R a d i o g r a p h i c examination after 11 years and 8 months r e v e a l e d b o n d formation lateral to the resorption area.
Figure 13Healing process was observed by normal ossification of the i n te rden ta l bone septa adjacent to the tooth root on CT.

6
Sodium hypochlorite,a large resorptive cavity was observed in the coronal third of the mesiolingual root (Fig.15B). Length d e t e r m i n a t i o n w a s p e r f o r m e d electronically using the Apex Finder AFA Model 7005 (EIE Analytic Technology, Orange, CA) and radiographically (Fig.14B), and the two mesial and distal canals were cleaned and shaped provisionally. Calcium hydroxide (Ultracal XS; Ultradent Products Inc., South Jordan, UT) was placed as temporary dressing because the granulation tissue could not be removed completely by mechanical instrumentation.
The calcium hydroxide paste was changed 2 weeks later. In a third office visit 3 weeks later, the resorptive cavity was completely free of pulpal tissue. Communication with the external root su r face was ev iden t . Wh i le the mesiolingual canal was sealed with a paper point, white MTA (Maillefer Dentsply) was condensed into the resorption cavity using a nonsurgical MTA carrier (Micro Apical Placement System, Produits Dentaires, Vevey, Switzerland) and root canal pluggers (Maillefer Dentsply) (Fig.15C) Again, calcium hydroxide and a temporary glass ionomer cement filling (Ketac-Fil; 3M ESPE, Sheffield, Germany) were applied. In the final office visit, after checking the set of the MTA, all 3 canals were obturated with gutta percha and AH26 sealer (Dexterity; Dentsply, Konstanz, Germany) using a hybrid condensation technique (a combination of apical cold l a t e r a l c o n d e n s a t i o n a n d thermomechanical compaction using gutta condensers) The access cavity was
restored with a glass ionomer cement filling (Ketac-Fil), and the patient was sent to the referring dentist for further coronal restoration. After 11 months, the patient was recalled, and the tooth was found to be symptom free. No percussion
sensitivity was observed, and the patient had a healthy gingiva and no periodontal pockets on probing. The periapical
Figure 14Periapical radiographs before, during and after endodontic treatment of mandibular left second molar with internal resorption in the medial root. A) Preoperative radiograph showing crescent radiolucent lesion in the alveolar bone next to a resorptive lesion in the mesial root. (B) A radiograph taken to establish working length in mesiobuccal and distal canal. (C) A radiograph taken immediately after filling of the resorption space with MTA and obturation of the root canals with gutta percha and sealer by hybrid condensation. (D) Eleven-month follow-up: healing of the mesial bone lesion is evident. (E) Two-year follow-up shows complete resolution of the radiolucency. (F) Distal ly angulated radiograph at 2-year follow-up.

7
radiograph showed satisfactory healing of the mesial radiolucency (Fig.14D). At a 2-year follow-up visit, the tooth was still symptom free. There was no percussion or palpation sensitivity, and periodontal probing did not exceed 3 mm. There were no signs of gingival retraction (Fig.15E). Furthermore, the periapical radiograph showed complete resolution of the mesial radiolucency. (Fig.14E, F)[3]
[Case 4]
A 16-year-old male was referred to the Dental School of the Federal University of Rio Grande do Sul because of a dental trauma suffered 5 years before. Clinical examination revealed coronal fracture on tooth 21, witch was slightly tender to percussion. All the teeth in this quadrant responded normally to cold testing except 21, which was unresponsive. A resorptive
lesion in the apical third and thickening of the periodontal ligament space was discovered on a periapical radiograph (Fig.16A). Based on the clinical and radiographic findings, root canal therapy was initiated. The rubber dam was placed and tooth was accessed wi thout anesthesia. Crown-down preparation was performed with K-Fi les (Mai l lefer Dentsply, Baillaigues, Switzerland) and Gates Glidden Burs (Maillefer Dentsply, Baillaigues, Switzerland) (Fig.16B). During preparation the canal was irrigated with 2.5% sodium hypochlorite. A fi n a l r i n s e w i t h 1 7 % E D TA (Biodinâmica, Ibiporã, Paraná, Brazil), to remove the smear layer, was performed. Hemorrhage and exudate from the apical reg ion was observed dur ing the instrumentat ion, which suggested resorption exteriorization. Calcium hydroxide (Calen, SS White, São Cristóvão Rio de Janeiro, Brasil) was
Figure 15Clinical images of mandibular left second molar with internal resorption in mesial root. (A) The view of the pulp chamber after gaining access; superficial necrosis was observed. (B) The view of the resorption cavity showing extension beyond the confines of the root. (C) The resorptive cavity has been filled with MTA. (D) The clinical image of the tooth at the 2-year follow-up.
Figure 16(A) Radiographic aspects of apical third root resorption observed in the tooth (21). (B) Crown-down technique performed. (C) Root canal filled with calcium hydroxide dressing. (D) MTA condensed into the apical resorption cavity after 14 days. (E) Canal fi l led using lateral condensation. (F) Six-month follow-up.

8
used for dressing (Fig.16C) and a temporary glass ionomer cement filling (Ketac-Fil; 3M Espe, Seefeld, Germany) was applied. The calcium hydroxide paste was removed 2 weeks later. White MTA (Maillefer Dentsply, Baillaigues, Switzerland) was condensed into the resorption cavity, by the means of a 5-mm apical plug (Fig.16D). After seven days, the canal was obturated using lateral condensation (Fig.16E).
After 6 months, the periapical lesion showed signs of resolution (Fig.16F). The post core preparation, cementation of intra radicular post and restoration were performed. After 1 year, the patient was recalled, and the tooth was found to be symptom free. No percussion sensitivity was observed. The periapical radiograph showed a satisfactory image (Fig.17G, H).[4]
Discussion
Extensive internal resorption may complicate the prognosis of endodontic treatment due to weakening of the remaining dental structure and possible periodontal involvement.[2] According to a Andreassen & Andreassen, internal resorption is a rare finding in permanent traumatized teeth with approximately 2% of them showing clinical signs of this type
of resorption.[4] In clinical case 1, it is considered that the knowledge about the mechanisms of microbial aggression after pu lpa l in fec t ion and therapeut ic resources to neutralize them has motivated the study of substances with an t im ic rob ia l and b iocompat ib le characteristics.[1] Sodium hypochlorite was chosen because it acts as an organic sol- vent. Dissolution of organic t i s s u e c a n b e v e r i fi e d i n t h e saponification reaction when sodium hypochlorite is used. It has been observed pulp tissue dissolution capacity, reporting that 5% sodium hypochlorite dissolves this tissue in 20 mins to 2 h o u r s . S o d i u m h y p o c h l o r i t e i s recommended and used by the majority of dentists because this solution presents s e v e r a l i m p o r t a n t p r o p e r t i e s : antimicrobial effect, tissue dissolution capaci ty and acceptable biologic compatibility.[1] In Case 2, the using of surgical microscope makes routine endodontic procedures because it enhances visibility and lighting. Another advantage is the improved visualization of root canal anatomy, which enables the operator to thoroughly examine the root canal system and clean and shape it more efficiently. Referring to Case 4, Internal resorptions on the apical third of root canal are even more rare and bring along with them technical difficulties.[4] However, in this case MTA presents some advantages. One of them is its physical characteristics which guarantees expansion during the attachment, which favor sealing and the maintenance of biological properties presented by calcium hydroxide.[4] It is worthwhile to emphasize that, in spite of the excellent
Figure 17(G, H) One-year follow-up: radiographic and clinical aspects.
9
results obtained with MTA in the treatment of perforations, the prognosis is directly related to the lapse of time in which the perforation remained without treatment, allowing contamination to occur. [1 ] When the inflammato ry resorption was observed, MTA was suggested to be applied. As both teeth had a good coronal structure and no post was indicated, it was possible to fill the middle and coronal third of the root canal with this material. MTA showed a favorable periapical tissue response, with neoformation of cemental coverage over MTA.[1] MTA has been proved good for solving the problems derived from perforation, as it does not interfere in the presence of moisture and inhibits the activity of bacteria. On the other hand, MTA characteristics make deobturation difficult when it is necessary to use intraradicular retentor.[4] Evidence of a long-term positive outcome supports the application of MTA for treatment of root perforation originating from internal/external resorption. Moreover, it can be concluded that the use of MTA in situations where extensive dental destruction is found may lead to an increase in resistance.[2] During treatment planning, the decision to extract the tooth and place an implant rather than endodontically treating it must be carefully considered, since it may well be the final treatment option offered to the patient.[2]
The use of biomaterials, such as MTA, in teeth with perforating internal root resorption gave optimal results, as demonstrated by clinical, radiographic, and CT examination after a follow-up of
over 11 years and this might serve as an exce l l en t a l t e rna t i ve t o imp lan t placement.[2]
Conclusion
In modern dentistry, patients demand more than restoration of function; they are particular about the esthetics as well, especially in the anterior region. The patient’s smile line, the periodontal biotype, the presence of the interproximal papilla, the positioning of the implant and soft tissue preservation are critical factors to be considered dur ing implant placement.[2] On the basis of the review of literature and the clinical-radiographic outcomes hereby presented, it might be concluded that (1) large internal root resorptions might and should be treated as in an attempt to save the tooth. (2) Because of i ts character ist ics of promoting excellent marginal sealing and stimulating osteoblastic adherence to the root surface, MTA has been considered as a good filling material to be used in communicating or perforating internal root resorption.[1] Nowadays literature proposed that the MTA should be maintained in the root canal to fill the resorption area and the placement of MTA for non-surgical treatment may be a good option, provided it is care- fully placed and condensed on the resorption area.[1] However, because of the price of MTA and the techniques, the employment of the material is not frequent in the clinic office. With time and improvement to achieve the goal of good internal root resorption.

10
References
[1] Georgiana Amaral, Renata Santiago Gonçalves Kattenbach, Rivail Antonio Sergio Fidel, Sandra Rivera Fidel. MTA as a Filling Material in Internal Root Resorption. Brazilian Journal of Dental Traumatology, Vol.1(2), 2009.
[2] Eduardo Nunes, Frank F. Silveira, Janir A. Soares, Marco A. H. Duarte, Sullener M. C. S. Soares. Treatment of Perforating Internal Root Resorption with MTA: A Case Report. Journal of Oral Science, Vol.54, No.1,127-131, 2012
[3] Maarten Meire, DDS, MSc, and Roeland De Moor, DDS, PhD, MSc. Mineral Trioxide Aggregate Repair of a Perforating Internal Resorption in a Mandibular Molar. JOE, Vol.34, No.2, Feb, 2008.
[4] Débora Franzon Brun, Roberta Kochenborger Scarparo, Patricia Maria Poli Kopper, Fabiana Soares Grecca. Apical Internal Inflammatory Root Resorption and Open Apex Treated with MTA: A Case Report. Rev. Odonto ciênc. Vol.25(2), 213-215, 2010.
[5] Hasan Guney Yilmaz, DDS, PhD, Atakan Calendar, DDS, PhD, Esra Cengiz, DDS. Use of Mineral Trioxide Aggregate in the Treatment of Invasive Cervical Resorption: A Case Report. JOE, Vol.36, No.1, Jan, 2010.





























