Embed Size (px)
Citation preview

Ricou and J Ross, JrP Nicod, EA Gilpin, H Dittrich, H Henning, A Maisel, AR Blacky, SC Smith, Jr, F
infarctionTrends in use of coronary angiography in subacute phase of myocardial
ISSN: 1524-4539 Copyright © 1991 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
1991, 84:1004-1015Circulation
http://circ.ahajournals.org/content/84/3/1004located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]: 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1004
Clinical Investigation
Trends in Use of Coronary Angiography inSubacute Phase of Myocardial Infarction
Pascal Nicod, MD; Elizabeth A. Gilpin, MS; Howard Dittrich, MD; Hartmut Henning, MD;Alan Maisel, MD; A. Robert Blacky, MD; Sidney C. Smith Jr., MD;
Francois Ricou, MD; and John Ross Jr., MD
Background. Most patients do not undergo acute reperfusion after myocardial infarction, andwhich of these patients should undergo coronary angiography is still debated.Methods and Results. We analyzed the l-year clinical outcomes and rates of coronary
angiography performed as late as 60 days after myocardial infarction in 3,804 patients admittedbetween 1979 and 1988 and followed in six different centers. Patients less than 75 years old wereclassified into low-, medium-, and high-risk groups using a multivariate analysis of historicaland clinical variables gathered during the first 8 hospital days. Patients who underwent earlyreperfusion (17%, all after 1984) were analyzed separately. To analyze time trends, patientswere compared before and after mid-1984. Mortalities from day 9 through 1 year were similarfor the two time periods in the low- (3.3% versus 2.5%) and medium-risk (7.4% versus 5.6%)groups, but mortality was lower for the high-risk group after 1984 (31.6% versus 20.0%). Theproportion of patients undergoing coronary angiography increased dramatically in each groupafter 1984 (low risk, 18% versus 48%; medium risk, 23% versus 49%o; high risk, 10%o versus 32%,before and after 1984, respectively). Furthermore, a large percentage of patients (more than40%) in the low-risk group did not have at least one of the indications for coronary angiographyrecently recommended by a joint task force. Among patients undergoing coronary angiography,the proportion of patients with three-vessel coronary artery disease decreased after 1984,whereas the proportion undergoing mechanical revascularization in the year after infarctionincreased in all risk groups.
Conclusions. Despite the recent development of noninvasive techniques with high sensitivityfor detecting high-risk patients after myocardial infarction, coronary angiography is beingperformed increasingly in all patients, including those determined to be at low risk forcomplications based on clinical data. The economic consequences of such a trend could beconsiderable, and its impact requires careful analysis. (Circulation 1991;84:1004-1015)
T his year, as many as 1.5 million Americans willexperience an acute myocardial infarction.1Of those who survive to be discharged from
the hospital, approximately 10% will die within thefollowing year. Identification of high-risk individualswho may benefit from more aggressive medical orsurgical treatment has been the subject of manystudies.2-24 Ideally, the application of noninvasivetechniques such as electrocardiographic exercisetesting,7-13 exercise with radionuclide studies14-17 or
echocardiography,1819 or positron emission tomogra-phy20'21 should allow the identification of patients athigh risk who might benefit from mechanical orsurgical recanalization and therefore should undergocardiac catheterization.22 27
However, despite support and guidelines for theuse of noninvasive techniques as a first step in riskstratification after acute myocardial infarction,28 anincreasing proportion of patients undergo cardiaccatheterization every year, even patients at low risk
From the Division of Cardiology (P.N., E.A.G., H.D., J.RJr.),University of California San Diego; Veterans AdministrationHospital, San Diego (A.M.); Naval Hospital of San Diego(A.R.B.); the Division of Cardiology, University of British Colum-bia, Vancouver, Canada (H.H.); Sharp Memorial Hospital, SanDiego (S.C.S.Jr.); and H6pital Cantonal, Geneva, Switzerland(F.R.).Supported by National Institutes of Health Ischemic Heart
Disease Specialized Center of Research (SCOR) grant HL-17682
awarded by the National Heart, Lung, and Blood Institute.Address for correspondence: John Ross Jr., MD, Department of
Medicine 0613B, University of California San Diego, La Jolla, CA92093.
All editorial decisions for this article, including selection ofreviewers and the final decision, were made by a guest editor. Thisprocedure applies to all manuscripts with authors from the Uni-versity of California San Diego or UCSD Medical Center.
Received June 21, 1990; revision accepted April 16, 1991.
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Nicod et al Coronary Angiography After Myocardial Infarction 1005
for complications or death after hospital discharge.This practice may be a result of a lack of consensusconcerning when the test is appropriate and a lack ofconfidence in the results of noninvasive testing.We have developed a risk stratification scheme
based on multivariate analyses of clinical and histor-ical variables that can define groups of patients atlow, medium, and high risk after myocardial infarc-tion. Although such methods are cumbersome andoften replaced by simpler decision schemes to assessrisk in the clinical setting,22-26 the stratification pro-vided is advantageous as a research tool for assessingtrends in the management of patients after myocar-dial infarction within fairly homogenous subgroups.
Accordingly, the main purpose of the present studywas to assess recent trends in the use of coronaryangiography in the convalescent phase of myocardialinfarction in a large patient population stratifiedaccording to risk. In addition, the indications forcoronary angiography and the yield on coronaryangiography of patients with significant coronaryartery disease within each risk group were analyzed.
MethodsPatient Population
In the period from January 1979 through October1988, 3,804 patients who suffered an acute myocar-dial infarction were included in this analysis. Thesepatients were admitted within 24 hours of symptomonset and survived the first 8 days of hospitalization.The diagnosis of Q wave myocardial infarction wasmade when the development of new Q waves on theelectrocardiogram was accompanied by either typicalchest pain or creatine kinase elevation (twice thelaboratory upper limit of normal). The diagnosis ofnon-Q wave myocardial infarction was established bythe presence of ST segment depression or T waveinversion and creatine kinase elevation. Exclusioncriteria were the refusal to sign a consent form(n=61) and coronary bypass surgery performedwithin 1 week of admission (n=12, before August1984 only).For the analysis of time trends, patients were
divided into two groups according to whether theywere admitted before (n=1,839) or after (n=1,965)August 1984. At that time, all patients were riskstratified prospectively, and it was soon after strati-fication began that the first acute interventions (per-cutaneous transluminal coronary angioplasty [PTCA]or thrombolysis) were performed at any of our par-ticipating centers. Patients 75 years old or youngerwho underwent acute thrombolysis or acute PTCAsince August 1984 (n=331) were analyzed separatelybecause their management is unique and the focus ofseveral multicenter randomized studies. Also, 506patients more than 75 years old without an acuteintervention were considered separately. (Only sevenpatients more than 75 years old, who were notincluded, had an acute intervention.)
Patients were recruited from six centers: the Univer-sity of California San Diego Medical Center; the SanDiego Veterans Administration Hospital; the NavalHospital of San Diego; Sharp Memorial Hospital, SanDiego; the Vancouver General Hospital, British Co-lumbia, Canada; and the Hopital Cantonal, Geneva,Switzerland. Sharp Memorial Hospital and the HopitalCantonal entered the study after August 1984. All datawere entered into a data base at the Specialized Centerfor Research on Ischemic Heart Disease at the Univer-sity of California San Diego Medical Center.
Clinical VariablesClinical variables were gathered prospectively at
each center on special forms and entered into the database. Collected data included information from thehistory, daily information from the physical examina-tion, laboratory data, electrocardiogram (ECG), ther-apy, radiographic findings during the stay in thecoronary care unit, and complications occurringthroughout the hospital stay. Also included were datafrom the discharge physical examination, ECG, chestradiograph, and medications. Details concerning theexact variables recorded and their definitions havebeen reported previously.5,6 Infarct extension was di-agnosed when occurrence of typical chest pain orelectrocardiographic change was accompanied by asecond creatine kinase elevation. Persistent or recur-rent ischemic pain was noted if the episode occurredmore than 24 hours after admission. Clinical signs ofleft ventricular failure were defined as grade 2 orgreater pulmonary congestion on radiography29 or, inthe absence of this radiographic finding, both S3 gallopand pulmonary rales. The S3 gallop and rales did nothave to be present simultaneously but could occur anytime during hospitalization.A subgroup of 1,652 patients 75 years old or
younger underwent determination of left ventricularejection fraction with radionuclide ventriculographyno later than 6 weeks after discharge. Twenty-four-hour ambulatory electrocardiographic monitoring wasalso performed in 1,544 patients 75 years old oryounger before hospital discharge. The presence ofcomplex ventricular arrhythmias was defined as fre-quent ventricular premature beats (more than 1 beat/min or 30 beats/hr), multiform ventricular prematurebeats, early ventricular premature beats (R or Tphenomenon), or ventricular tachycardia (more thanthree consecutive ventricular premature beats). Pa-tients were maintained on their regular medication atthe time of the recording. Exercise tests were per-formed in 1,147 patients 75 years old or youngeraccording to several different protocols. A test wasconsidered positive if the patient experienced anginaor the exercise ECG showed 1 mm or more STsegment depression (either flat or downsloping) mea-sured 80 msec after the J point.13 The results ofnoninvasive tests are included for information onlyand did not influence the risk stratification procedure.
Cardiac catheterization performed after the early,acute phase in 1,195 patients 75 years old or younger
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1006 Circulation Vol 84, No 3 September 1991
using the standard femoral or the brachial arterialapproach was usually done near the time of hospitaldischarge; studies from day 2 to day 60 after admis-sion are included. To further examine the rate ofcoronary angiography by year, the population wasextended to include patients admitted through 1989,when the study was terminated, who had at least 60days of follow-up. Original cardiac catheterizationreports were obtained and recorded on special forms,which were reviewed by a research physician (P.N. orH.D.). Whenever possible, when the report provedinadequate to code the extent of stenosis, the filmswere reviewed. The extent of coronary artery diseasewas reported as 70% or greater coronary arterydiameter stenosis (50% or more for left main) byvisual interpretation. The Coronary Artery SurgeryStudy criteria were used to categorize the extent ofdisease as no significant disease or as one-, two-, orthree-vessel disease.30 A patient with significant leftmain coronary artery disease was classified as havingtwo-vessel disease if the circulation was right domi-nant and three-vessel disease if it was left domi-nant30. Catheterization reports were available in 92%of patients 75 years old or younger who underwentthe procedure within 60 days of admission.
Radionuclide determination of left ventricularejection fraction, 24-hour ambulatory electrocardio-graphic monitoring, exercise testing, and cardiaccatheterization were performed only if prescribed bythe attending physician; no attempt was made toinfluence these decisions.
Follow-upPatient follow-up was performed at 3, 6, and 12
months after hospital admission. Information concern-ing death was obtained from the death certificate andhospital records. Telephone interviews with personalphysicians or family members were sometimes made toclarify details. All data were reviewed by a researchphysician; when any doubt existed as to the cause ofdeath, a committee reviewed the available data andcame to a consensus decision. Death was consideredcardiac in cause when secondary to a new myocardialinfarction, extension of the myocardial infarction, con-gestive heart failure, shock, cardiac procedures, orsurgery and when sudden (resulting from fatal arrhyth-mias or sudden unexpected death with exact causeunknown but presumed to be cardiac). One-year fol-low-up was obtained in 97% of the patients eligible forfollow-up at the time of this analysis.
Risk Stratification SchemeMore than 60 clinical variables were screened
univariately for association with the end points ofcardiac death or new myocardial infarction occurringfrom day 9 to 1 year. Variables univariately signifi-cant by t test (continuous variables) or y2 (categoricalvariables) at the p<0.05 level were submitted to atwo-stage multivariate analysis (see "Appendix").
Stage 1: Identification of low-risk patients. All pa-tients with serious in-hospital complications were
excluded from the first stage of the analysis. Thesecomplications included malignant arrhythmias suchas ventricular fibrillation or tachycardia (see "Ap-pendix"), congestive heart failure, shock, persistentischemic pain, or intact extension beyond 24 hours.Multivariate analyses, including data acquired fromthe history and the first 3 hospital days, were used tobuild a scheme for the identification of patients atlow risk of new myocardial infarction or death withinthe first 3 months. The purpose of using data fromonly the first 3 days of hospitalization was to identifylow-risk patients early so that early hospital dischargecould be considered in the future. Three differentmultivariate methodologies (linear discriminationanalysis,31 logistic regression,32 and recursive parti-tioning33) were used; using a conservative approach,a patient had to be considered at low risk by all threemethodologies before being placed in the low-riskgroup. The variables selected by these multivariatemethodologies and the prognostic functions are givenin the "Appendix."
Stage 2: Identification of high- and medium-riskpatients. Patients with complications before day 8 andthose who were not identified as low risk during thefirst stage of the multivariate analysis were subjectedto a second-stage multivariate analysis based on datafrom the history and the first 8 days of hospitaliza-tion. The end point for this analysis was cardiacdeath within 1 year. Again, three multivariate meth-odologies were used, and patients were assigned tothe high-risk group if at least two of the threemethods predicted high risk. All patients not classi-fied as high risk were placed in the medium-riskgroup. Variables selected for this analysis and theprognostic functions are given in the "Appendix."Patients admitted before August 1984 were riskstratified retrospectively based on the multivariaterisk stratification scheme described above, which wasdeveloped using the first half of this population. Riskstratification was performed prospectively on pa-tients admitted since August 1984. Thus, to be as-signed to a risk group, a patient needed to survive thefirst 8 days, and such patients constitute the presentstudy population.
Risk GroupsFor patients less than 75 years old admitted before
August 1984, 21% were low risk, 55% were mediumrisk, and 24% were high risk. For all patients admit-ted subsequently, regardless of whether there was anacute intervention, 26% were low risk, 45% weremedium risk, and 27% were high risk. The reductionin medium-risk patients from 55% to 45% of thepopulation was statistically significant (p<0.001) andreflects the inclusion of two new centers in the latercohort with lower-risk patients and high rates ofacute interventions. Among the patients in the sec-ond cohort less than 75 years old with an acuteintervention, 37% were low risk, 44% were mediumrisk, and 19% were high risk.
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Nicod et al Coronary Angiography After Myocardial Infarction 1007
TABLE 1. Comparison of Patients 75 Years Old or Younger Without Acute Intervention Admitted Before August 1984and Subsequently
Late cohortEarly (no acute Acutecohort p interventions) p interventions
Patients (n) 1,575 1,385 331HistoryAge (mean+SD years)Male (%)History of previous myocardial infarction (%)History of anginaHistory of congestive heart failure (%)History of hypertension (%)Smoking at time of myocardial infarction (%)
ComplicationsPulmonary congestion on radiography (%)Persistent ischemic pain (%)Extension of myocardial infarction (%)
Non-Q wave myocardial infarction (%)Special studies
Radionuclide ventriculography (n)LVEF (mean±SD)
Ambulatory electrocardiographic monitoring (n)Complex VPCs
Exercise test (n)Positive (%)
Coronary angiography (n)Three-vessel CAD (%)Left main CAD (%)
Revascularization by 1 year (%)Cardiac mortalityDays 9-365 (%)In-hospital after day 8 (%)Postdischarge (%)
New nonfatal myocardial infarctionwithin 1 year
59.5±10.179293994354 p<0.0001t
2130521
60.3±9.8793038104540
p<0.0001 3332424
868 6880.49±0.14 p<0.0001 0.46±0.14
926 56644 44571 52943 p<0.0001 38
213 (13%) p<0.0001 598 (43%)45 265 612 p<0.0001 25
1239
4
927
2
p<0.Oltp<0.0001p<0.001p<0.0001p<0.05p<0.0001
55.4±+10.186162523850
p<0.001 24315
p<0.0001 11
960.47±0.13
52354734
301 (91%)p<O.OOOl 10
3p<0.0001 41
p<0.01 3<1§3
2
LVEF, left ventricular ejection fraction; VPCs, ventricular premature contractions; CAD, coronary artery disease.*After acute intervention.tEarly cohort compared with late cohort (no acute interventions).tSubgroups with acute interventions of the late cohort compared with those without such interventions.§One patient died before discharge.
Data AnalysisStandard statistical methods were used for com-
parison of patients admitted before August 1984 andsubsequently, using t tests for group means or x2 testsof proportions as appropriate.
ResultsCohort ComparisonThere were 1,575 patients 75 years old or younger
entered before August 1984 (early cohort) and 1,385patients 75 years old or younger without acute inter-vention entered after August 1984 (later cohort).Their main clinical characteristics are shown in Table1. The two cohorts were nearly identical with regardto historical features, except there were fewer pa-tients smoking cigarettes at the time of their infarc-
tion in the later cohort. The cohorts were also similarwith -regard to in-hospital complications, althoughpatients in the later cohort had a higher incidence ofpulmonary congestion on chest radiography. Patientswho underwent radionuclide left ventriculography inthe later cohort had a lower mean ejection fractionthan those in the early cohort (0.46 versus 0.49,p<0.0001). There were no differences in the resultsof 24-hour ambulatory electrocardiographic monitor-ing or exercise tests.
Figure 1 (top panel) shows the mortality from day9 to 1 year by risk group for the two cohorts. Most ofthe reduction in mortality between the two periodsoccurred in the high-risk patients (31.6% versus20.0%). The mortality rates in the low- (3.3% versus2.5%) and medium-risk (7.4% versus 5.6%) groups
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1008 Circulation Vol 84, No 3 September 1991
35-_
L= Early Cohort
30 Later Cohort
25 L
20 L
15-
10
5
0LOW MEDIUM
Risk GroupHIGH
% 30
20-
10LO
i~~O -.
LOW
35
! Early Cohort301_ Later Cohort
25
201
15
10
5
_0 '-- OLOW MEDIUM
Risk GroupHIGH
60
50
40i ~ ~1 ~ ~
% 30
i20
i100
79 80 81 82 83 84 85
YearFIGURE 1. Top panel: Bar graph of mortality from day 9 to 1
year by risk group. * **p<0*0l. Bottom panel: Bar graph ofpercentages ofpatients with recurrent nonfatal myocardial infarc-tion from hospital discharge to 1 year, grouped according to risk
were slightly lower in the later cohort, but thesedifferences were not significant. The rates of new
nonfatal infarction by 1 year within risk groups forthe two cohorts were similar as shown in Figure 1(bottom panel) (3.7% and 2.5%, 3.3% and 4.1%, and5.4% and 4.0% in the low-, medium-, and high-riskgroups, respectively).
Coronary Angiography, Coronary Artery BypassSurgery, and Coronary AngioplastyThe incidence of coronary angiography performed
within 60 days from the onset of infarction is shownwithin each risk group for the two cohorts in Figure2 (top panel); the yearly rate from 1979 through 1989is shown in Figure 2 (bottom panel). In the earlycohort, less than one fourth of patients from each riskgroup (18%, 23%, and 10% for the low-, medium-,and high-risk groups, respectively) underwent car-diac catheterization. However, in the later cohort,nearly half of the patients in the low- (48%) andmedium-risk groups (49%) and a third of the high-risk group (32%) underwent coronary angiographywithin 60 days. The yearly rates of coronary angiog-raphy were low before 1985, increased substantiallyto a peak of 52% in 1987, and has decreased sincethen (Figure 2, bottom panel).
FIGURE 2. Top panel: Bar graph ofpercentages ofpatientsundergoing coronary angiography within 60 days of hospitaladmission, grouped according to risk. ***p<0.001. Bottompanel: Bar graph ofpercentages ofpatients undergoing coro-
nary angiography by year from 1979 through 1989.
Revascularization procedures during the year aftermyocardial infarction were performed more thantwice as often in the later cohort regardless of riskgroup (each,p<0.01) (Figure 3) (9.5% versus 24.4%,14.4% versus 28.0%, and 8.9% versus 19.1% for thelow-, medium-, and high-risk groups, respectively).The crosshatched portions of the bars for the latercohort indicate the proportion of the revasculariza-tion procedures that were coronary artery bypasssurgery. In the later cohort, PTCA was performed in13.6%, 9.5%, and 3.0% of the low-, medium-, andhigh-risk groups, respectively. PTCA accounts fornearly all of the additional interventions in the low-and medium-risk groups but not in the high-riskgroup.There were small differences among the different
hospitals in the percentages of patients undergoingcoronary angiography or revascularization proce-dures. The use of coronary-angiography was signifi-cantly lower in only the Vancouver General Hospital(18% of all patients 75 years old or younger) com-pared with 57-84% at the other centers. However,the trend toward greater use of cardiac catheteriza-tion and revascularization procedures was seen in allfour hospitals represented in both cohorts.
60
50
40
= Early Cohort
M Later Cohort
MEDIUM
Risk GroupHIGH
86 87 88 89
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Nicod et al Coronary Angiography After Myocardial Infarction 1009
LOW MEDIUM HIGH
Risk Group
FIGURE 3. Bar graph ofpercentages ofpatients undergoingmechanical revascularization within 1 year from infarction,grouped according to risk. Before 1984 (early cohort), onlycoronary bypass surgery was performed. After 1984 (latercohort), percutaneous angioplasty (open portion ofcolumn) or
coronary bypass surgery was performed. * **p<0.001.
Indications for Coronary AngiographyIndications for coronary angiography after myocar-
dial infarction vary among institutions but may in-clude factors such as persistent ischemic pain aftermore than 24 hours, the presence of non-Q wave
myocardial infarction, young age (less than 40 years),an abnormal exercise test, a radionuclide left ventric-ular ejection fraction of less than 0.45, and thepresence of clinical (S3 gallop or pulmonary rales) or
radiographic signs of left ventricular failure duringthe hospital stay.26,27 The incidences of these variousfactors within 60 days in patients undergoing cardiaccatheterization are given in Table 2 for each riskgroup in both the early and later cohorts. As shown,in 40% of low-risk patients who underwent coronaryangiography within 60 days, none of the indicationsmentioned above could be documented. Recall thatpatients in the low- and medium-risk groups had thehighest rates of coronary angiography (Figure 2).Also, a majority of patients in the low- (69%) andmedium-risk (70%) groups of the early cohort did notundergo exercise testing before coronary angiogra-phy; these proportions increased in the later cohortto 74% and 78% for the low- and medium-riskgroups, respectively.
Results of Coronary AngiographyThe incidence of three-vessel and left main coro-
nary artery disease is shown in Figure 4 by risk groupfor each cohort. In the early cohort, a higher propor-tion of patients who underwent coronary angiogra-phy had three-vessel disease in all three risk groups(Figure 4, top panel) (34%, 44%, and 67% for thelow-, medium-, and high-risk groups, respectively). Inthe later cohort, 16% of patients who underwentcoronary angiography in the low-risk group, 25% inthe medium-risk group, and 38% in the high-riskgroup had three-vessel disease (Figure 4, top panel).However, there was no significant difference in theincidence of left main coronary artery disease be-
TABLE 2. Indications for Coronary Angiography in Patients With Coronary Angiography Within the First 60 DaysLow risk Medium risk High risk
Early cohortPatients with CA within first 60 days (n)Pain (n)Non-Q wave myocardial infarction (n)Positive ETT (n)LVEF <0.45Clinical signs of LV failure (n)*Age <40 years
At least one of the above
Later cohortPatients with CA within first 60 days (n)Persistent ischemic pain (n)Non-Q wave myocardial infarction (n)Positive EBT (n)LVEF <0.45 (n)Clinical signs of LV failure (n) *
Age <40 years
At least one of the above
625 (2%)14 (23%)15 (24%)4 (6%)6 (10%)4 (13%)
36 (58%)
15917 (11%)t36 (22%)27 (17%)2 (1%)
16 (10%)15 (9%)
94 (59%)
19673 (42%)35 (18%)37 (19%)16 (8%)52 (27%)32 (16%)
156 (80%)
306110 (36%)86 (28%)42 (14%)33 (11%)105 (34%)22 (7%)
242 (79%)
388 (21%)8 (21%)2 (5%)2 (5%)
27 (71%)0
32 (84%)
13757 (42%)37 (27%)15 (11%)18 (13%)
109 (80%)0
129 (94%)
CA, coronary angiography; LVEF, left ventricular ejection fraction; LV, left ventricle.For a patient to be eliminated from the low-risk group, two of three signs of failure had to all be present at the same
time (S3, pulmonary rales, and radiographic pulmonary congestion .2).*Generally recognized indications.27tNo more than one episode of pain relieved by nitroglycerin; not severe enough to require readmission to coronary
care unit.
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1010 Circulation Vol 84, No 3 September 1991
80
70 -=
Early CohortM Later Cohort
60 -
50h
% 40 - ..
30L
20 -
10
LOW MEDIUM
Risk GroupHIGH
80
70 vL Early CohortLater Cohort
60
50
%40
30_
LOW MEDIUM HIGH
Risk Group
FIGURE 4. Top panel: Bar graph ofpercentages ofpatientswith three-vessel coronary disease grouped according to risk.***p<0.001. Bottom panel: Bar graph of percentages ofpatients with left main coronary artery disease grouped accord-ing to risk.
tween the early and the later cohort (Figure 4,bottom panel) (2.3% versus 5.8%, 4.8% versus 3.9%,and 8.3% versus 7.3% for the low-, medium-, andhigh-risk groups, respectively).
Patients More Than 75 Years OldIn-hospital mortality after the first 8 days (3.4%
versus 1.8%) and 1-year mortality after discharge(24% versus 17%) were similar for patients more
than 75 years old without acute interventions before(n =264) and after (n =242) 1984. Coronary angiog-raphy within the first 60 days was performed in seven
patients (2%) more than 75 years old before 1984and 27 patients (11%) after 1984 (p<0.0001). Three-vessel coronary artery disease was found in four and10 patients and left main disease was found in oneand two patients before and after 1984, respectively.Only one patient in the early cohort and 13 patientsin the later cohort underwent coronary bypass sur-gery in the first year. In the later cohort, eightpatients also underwent angioplasty in the first year.
Patients Less Than 75 Years Old Undergoing AcuteThrombolysis and/or Acute Revascularization
In the later cohort, 331 patients had acute throm-bolysis and/or angioplasty or coronary artery bypass
surgery within 24 hours of admission. In-hospital mor-tality after day 8 was 0.3%, and 1-year postdischargemortality rate was 3.4%. This subgroup of patients wasyounger and had less history of coronary artery diseasethan the other patients in the later cohort (Table 1).More than 90% had coronary angiography and morethan 40% underwent a revascularization procedure inthe first year after the acute intervention.
DiscussionThe present study documents that the use of
coronary angiography after myocardial infarction hasmarkedly increased in recent years and that thisincrease is present in all risk groups, including pa-tients at low risk for death within the year afterinfarction. The yield of patients with left main orthree-vessel disease was 16% in the low-risk group. Asmaller proportion of patients was selected for coro-nary angiography in the early cohort, and thesepatients had more extensive disease (Figure 4, toppanel), regardless of risk group. However, with ahigher proportion of patients undergoing coronaryangiography, it is expected that the yield of patientswith significant disease would decrease, and thisfinding does not indicate a lower underlying preva-lence of significant disease. Mortality decreased onlyslightly for the low- and medium-risk groups (Figure1, top panel) between the two cohorts despite theincreased rate of coronary angiography (Figure 2, toppanel) and increased use of revascularization proce-dures, mainly PTCA (Figure 3). To detect the ob-served decrease in mortality from day 9 through 1year between the two cohorts for the low-risk group(3.3% to 2.5%) with 90% power and a one-tailedsignificance level of 0.05 would require 7,783 patientsin each cohort. Whether the decrease in mortality inthe high-risk group of the later cohort is a result ofmore intervention, better medical care without inter-vention, or differences in patient populations is un-certain. It is interesting to note that the percent ofpatients undergoing coronary angiography was thelowest in the high-risk group. Patients who under-went early thrombolysis or coronary angioplasty wereanalyzed separately because several randomized tri-als have already attempted to define the role andtiming of coronary angiography in those individu-als.34-36 However, this group of patients may includeonly approximately 15% of patients presenting withsymptoms suggesting acute myocardial infarction.37The role of coronary angiography remains much lessclear in the remaining patients who do not undergoacute thrombolysis or early mechanical revasculariza-tion, and they are the main subject of this study.
Indications for Coronary AngiographyThe results suggest that a large percentage of
patients undergoing coronary angiography do nothave indications as recommended recently by a sub-committee of the Joint Task Force on CardiovascularProcedures and Therapy of the American College ofCardiology and the American Heart Association.27
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Nicod et al Coronary Angiography After Myocardial Infarction 1011
These criteria included resting ischemic pain, clinicalheart failure, radionuclide left ventricular ejectionfraction of less than 0.45, exercise-induced ischemia,age of less than 40 years, and non-Q wave myocardialinfarction. Non-Q wave infarction and age of lessthan 40 years were listed among indications consid-ered controversial in the Task Force report.27 Nev-ertheless, 41% of the patients in the low-risk group ofour 1984-1988 cohort who underwent coronary an-giography within 60 days did not have at least one ofthese indications for coronary angiography aftermyocardial infarction.
It is recognized that the final decision to performcoronary angiography in a given patient will not relyon a risk stratification scheme and will be individu-alized. It is likely that some patients determined to beat low risk by multivariate analysis after myocardialinfarction may have had a valid reason for thisprocedure and benefitted from cardiac catheteriza-tion and coronary revascularization. In the 1984-1988 cohort of our study, 16% of low-risk patientswho underwent cardiac catheterization had three-vessel or left main coronary artery disease, and 11%underwent coronary bypass surgery at some timeduring the first year. Whether this rate of yieldjustifies the use of coronary angiography as a routinescreening procedure is a matter of opinion. In addi-tion, not all patients with multivessel involvementafter myocardial infarction have a poor prognosis.Furthermore, coronary angiography may not allowaccurate prediction of the site of subsequent myocar-dial infarction, which often occurs in arteries showingminor rather than high-grade stenoses.38 Likewise,functional abnormalities detected by treadmill test-ing coupled with radionuclide studies may be morevaluable than anatomy alone for predicting prognosisafter myocardial infarction.'5-17
It is intriguing that the use of coronary angiogra-phy has increased greatly at a time when multiplestudies have shown the value of various noninvasivemethods for detecting high-risk patients after myo-cardial infarction. Recent years have also witnessedthe extraordinary development of multiple newmethods in interventional cardiology, includingPTCA, atherectomy, stenting, and so on. Therefore,the trend toward a more mechanistic approach to thetherapy of coronary artery disease may explain theincreased use of coronary angiography. When acuteintervention became prevalent, there was a dramaticincrease in the use of coronary angiography, evenamong patients without acute intervention (Figure 2,bottom panel). Concomitant with the publication ofreports indicating coronary angiography is not essen-tial after thrombolysis,36,39 the rate of coronary angi-ography has decreased but is still higher than in theera before acute intervention. Also, financial incen-tives for hospitals as well as for some physiciansmight explain in part the increased recent trend inthe use of coronary angiography. Our study cannotassess the cost-benefit ratio of the observed trend inthe use of coronary angiography because benefits
cannot be adequately evaluated from a retrospectivestudy. It is possible that after myocardial infarctionsome low-risk patients may benefit from revascular-ization, particularly those with multivessel involve-ment and residual ischemia,4041 those with multives-sel disease and left ventricular dysfunction at rest,42,43and perhaps, as recently suggested, those with per-sistent total occlusion of the infarct-related artery.44A striking finding of our study was that a majority
(approximately 75%) of patients in the low- or medi-um-risk group did not undergo exercise testing beforecoronary angiography. In our study, these tests weredone only if requested by the attending physician. It ispossible, therefore, that performance of routine exer-cise testing would allow better detection of patientswith significant three-vessel or left main coronaryartery disease who are at risk of recurrent events, assuggested by many previous studies7-19 and by recentrisk stratification schemes.22-26 For instance, since1984, 16% of patients in the low-risk group whounderwent coronary angiography had three-vessel cor-onary disease, but only 11 of 26 patients (42%) withthree-vessel coronary artery disease at cardiac cathe-terization in the low-risk group underwent exercisetesting. Of those, four had a positive exercise test, fourhad a negative exercise test, and in three patientsthe test was indeterminant because of failure toachieve adequate exercise level. Of the nine pa-tients in the low-risk group with left main coronarydisease, only four underwent exercise testing, threeof which were positive. The inability of exercisetesting to detect all patients with three-vessel or leftmain disease may be a weakness of a decisionstrategy based on such noninvasive evaluation oflow-risk patients. However, it has been shown thatin patients with significant coronary artery disease,those with an abnormal exercise test response are atparticularly high risk for subsequent events. On theother hand, patients with good exercise test re-sponses may have a good outcome despite thepresence of multivessel coronary disease.'5-'7,45-49
Decision schemes for the use of coronary angiog-raphy after myocardial infarction have been pro-posed.22-26 Whether such schemes, which use exer-cise testing and noninvasive assessment of residualleft ventricular function as a first step in the evalua-tion of uncomplicated patients, can identify those atincreased risk at a rate comparable to that fromelective coronary angiography remains to be demon-strated. Even though some high-risk patients may notbe detected, such schemes may avoid unnecessarydiagnostic and therapeutic procedures with theirassociated morbidity and mortality in patients at lowrisk after myocardial infarction.The goal of our study was to document the trends
and results of coronary angiography in patients fromseveral urban, military, and university centersgrouped according to risk after myocardial infarction.It is recommended that the marked trend towardincreased use of coronary angiography documentedin our study be evaluated nationally by cost-benefit
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1012 Circulation Vol 84, No 3 September 1991
analysis because of the very significant consequencesof the cost of health care.
AcknowledgmentsWe thank Geri Cali, RN, Sharon Knowlton, RN,
and Cheryl Davies, RN, for their dedication and JodyThomas for her expert assistance in the preparationof the manuscript.
AppendixApproximately 60 variables were prescreened
univariately to develop the two-stage risk stratifica-tion procedure (Table 3). The first evaluation takesplace soon after day 3. However, the first stage isomitted if the patient has any of the followingcomplications during the first 3 days: ventricularfibrillation, cardiac arrest, second- or third-degreeheart block, other ventricular dysarrhythmias afterthe first 48 hours requiring oral antiarrhythmic drugs,shock, congestive heart failure (any two of the fol-lowing: S3 gallop, persistent bibasilar or higher rales),grade 2 or greater pulmonary congestion on the chestradiograph (see second-stage table legend) persistentischemic pain (more than one transient episoderelieved by nitroglycerin), or extension of infarctbeyond the first 24 hours.
First StageThe end points used in the multivariate analyses
were death or new nonfatal myocardial infarctionfrom day 9 through day 90 after admission. Table 4gives the variables and coefficients for the lineardiscriminant and logistic discriminant functions.For the linear discriminant function, if the sum of
the variable values multiplied by their respectivecoefficients is more than 1.9827, the patient is not atlow risk with regard to the linear discriminationfunction.
For the logistic function, the quantity F is com-
puted as the sum of the variable values multipled bytheir respective coefficients with the constant added.Then, the probability of no event is computed as:p=1.0/(1.0+EXP(-F). If the probability value is lessthan 0.8925, then the patient is not at low risk.For recursive partitioning, if the patient had a
history of previous myocardial infarction, then she orhe is not at low risk; otherwise, if the maximum heartrate during the first 3 days is more than 104.5beats/min, the patient is not at low risk.
All three multivariate methodologies must desig-nate the patient to be at low risk for the patient to beplaced in the low-risk category. If any one of themethods determines that the patient is not at lowrisk, the second-stage risk computation is performedshortly after day 8. If any of the complications listedabove occur during the period after days 3-8 for a
patient in the low-risk group, the second-stage com-putation is also performed. If none of the complica-tions occurs, the second-stage computation is omit-ted; the patient is at low risk.
TABLE 3. List of Variables Screened for Inclusion in Two-StageMultivariate Risk Stratification Scheme
AgeGenderTime from onset of symptoms to hospital admissionHistory of previous myocardial infarctionHistory of previous angina pectorisHistory of previous congestive heart failureHistory of hypertensionHistory of chronic obstructive pulmonary diseaseHistory of diabetesHistory of peripherial vascular diseaseFamily history of ischemic heart diseaseNew or changing pattern of angina within 1 monthSyncopeDyspneaNauseaDiaphoresesObesityPericarditisCardiac arrestExtension of infarctionPersistent ischemic painShockS3 gallopPeripheral edemaApex outside midclavicular lineSystolic murmur suggesting mitral regurgitationBibasilar ralesRales at or above the lower tips of the scapulaeRadiographic pulmonary congestion gradeHeart rateSystolic blood pressureDiastolic blood pressureTemperatureRespiration rateBlood urea nitrogenLeukocyte countCreatinineLocation of infarctionAtrial fibrillationAtrial flutterAny supraventricular arrhythmiaVentricular premature beats >6 min-1Ventricular tachycardiaVentricular fibrillationSinus bradycardiaSinus tachycardiaSecond-degree atrioventricular blockThird-degree atrioventricular blockRight bundle branch block (old, new, age indeterminant)Left bundle branch block (old, new, age indeterminant)Bilateral bundle branch block (old, new, age indeterminant)Left-axis deviation (old, new, age indeterminant)Left anterior hemiblockLeft posterior hemiblockLeft ventricular hypertrophy
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
Nicod et al Coronary Angiography After Myocardial Infarction
TABLE 4. Variables and Coefficients for Stage 1 Prognostic Computation
Linear Logisticdiscrimination discrimination
Variable Value coefficient coefficientMaximum blood urea nitrogen mg/dl 0.0855 0.0History of previous myocardial infarction 0=no 1.4255 -1.0920
1=yesRales above scapulae 0=no 10.3591 0.0
1 =yesMaximum heart rate beats/min 0.0 -0.01855Systolic murmur on physical examination 0=no
1=yes 0.0 -1.1142Old bundle branch block 0=no
1=yes 1.9716 -1.2450Age x maximum blood urea nitrogen Product of variables 0.0 -0.0006792Constant 5.331
Findings as observed during the first 3 days.
TABLE 5. Variables and Coefficients for Stage 2 Prognostic Computation
Linear Logisticdiscrimination discrimination
Variable Value coefficient coefficient
Age Years 0.0249 -0.0200Maximum blood urea nitrogen mg/dl 0.0493 0.0Abnormal apex on physical examination 0=no
1=yes 0.5050 -0.7507Grade of pulmonary congestion on chest radiograph See legend 0.38065 0.0History of congestive heart failure 0=no
1=yes 0.0 -0.7141Old bundle branch block 0=no
1=yes 1.0790 -0.6234Agexmaximum blood urea nitrogen Product of variables 0.0 -0.0002987Constant 2.4380
Findings as observed during the first 8 days.Radiograph pulmonary congestion grades: 0, none; 1, pulmonary venous hypertension; 2, interstitial pulmonary edema;3, localized alveolar edema; 4, diffuse alveolar edema.
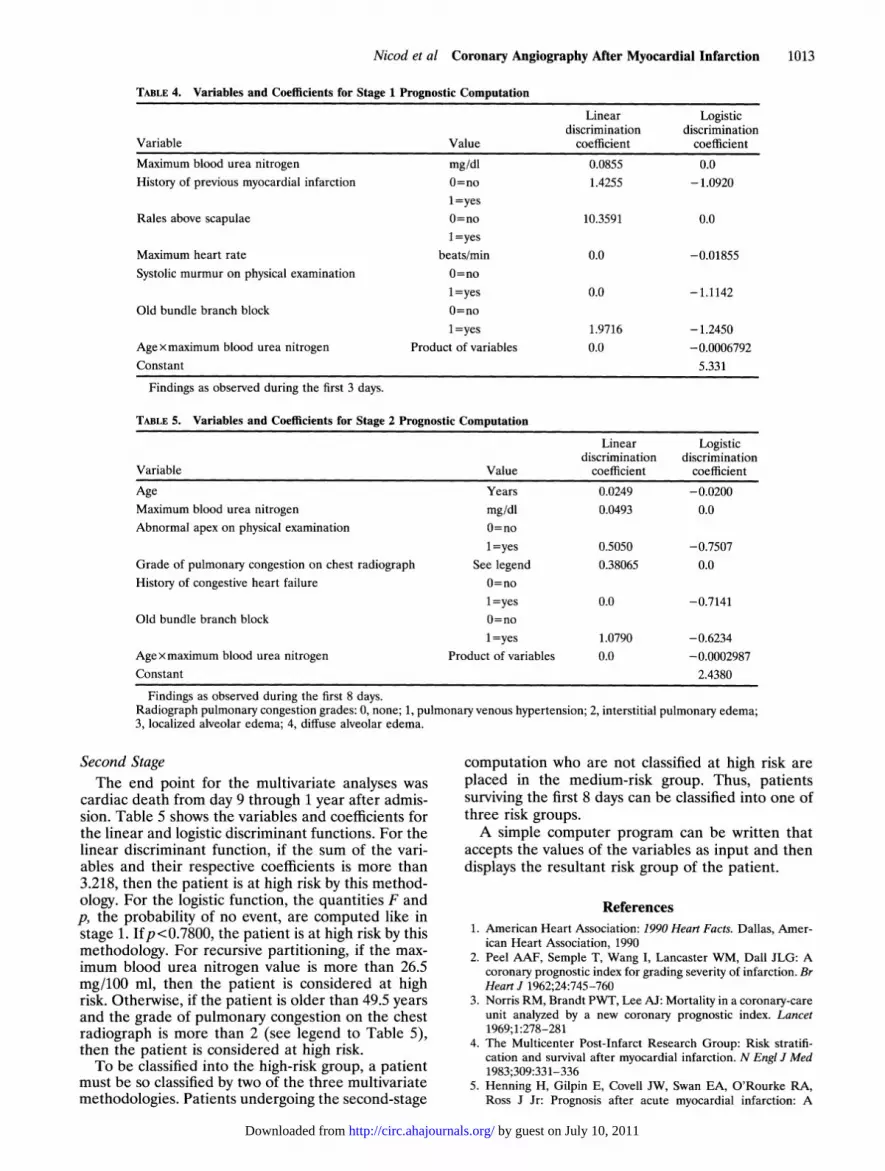
Second StageThe end point for the multivariate analyses was
cardiac death from day 9 through 1 year after admis-sion. Table 5 shows the variables and coefficients forthe linear and logistic discriminant functions. For thelinear discriminant function, if the sum of the vari-ables and their respective coefficients is more than3.218, then the patient is at high risk by this method-ology. For the logistic function, the quantities F andp, the probability of no event, are computed like instage 1. Ifp<0.7800, the patient is at high risk by thismethodology. For recursive partitioning, if the max-imum blood urea nitrogen value is more than 26.5mg/100 ml, then the patient is considered at highrisk. Otherwise, if the patient is older than 49.5 yearsand the grade of pulmonary congestion on the chestradiograph is more than 2 (see legend to Table 5),then the patient is considered at high risk.To be classified into the high-risk group, a patient
must be so classified by two of the three multivariatemethodologies. Patients undergoing the second-stage
computation who are not classified at high risk areplaced in the medium-risk group. Thus, patientssurviving the first 8 days can be classified into one ofthree risk groups.A simple computer program can be written that
accepts the values of the variables as input and thendisplays the resultant risk group of the patient.
References1. American Heart Association: 1990 Heart Facts. Dallas, Amer-
ican Heart Association, 19902. Peel AAF, Semple T, Wang I, Lancaster WM, Dall JLG: A
coronary prognostic index for grading severity of infarction. BrHeart J 1962;24:745-760
3. Norris RM, Brandt PWT, Lee AJ: Mortality in a coronary-careunit analyzed by a new coronary prognostic index. Lancet1969;1:278-281
4. The Multicenter Post-Infarct Research Group: Risk stratifi-cation and survival after myocardial infarction. N Engl J Med1983;309:331-336
5. Henning H, Gilpin E, Covell JW, Swan EA, O'Rourke RA,Ross J Jr: Prognosis after acute myocardial infarction: A
1013
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

1014 Circulation Vol 84, No 3 September 1991
multivariate analysis of mortality and survival. Circulation1979;59:1124-1136
6. Madsen EB, Gilpin E, Henning H, Ahnve S, Le Winter M,Ceretto W, Joswig W, Collins D, Pitt W, Ross J Jr: Predictionof late mortality after myocardial infarction from variablesmeasured at different times during hospitalization. Am JCardiol 1984;53:47-54
7. Markiewicz W, Houston N, DeBusk RF: Exercise testing soonafter myocardial infarction. Circulation 1977;56:26-31
8. Theroux P, Waters DD, Halphen C, Debaisieux JC, MizgalaHF: Prognostic value of exercise testing soon after myocardialinfarction. N Engl J Med 1979;301:341-345
9. Starling MR, Crawford MH, Kennedy GT, O'Rourke RA:Treadmill exercise tests predischarge and six weeks post-myocardial infarction to detect abnormalities of known prog-nostic value. Ann Intem Med 1981;94:721-727
10. Schwartz KM, Turner JD, Sheffield LT, Roitman DI, KansalSP: Limited exercise testing soon after myocardial infarction:Correlation with early coronary and left ventricular angiogra-phy. Ann Intem Med 1981;94:727-734
11. Fuller CM, Raizner AE, Verani MS, Nahormek PA, ChahineRA, McEntee CW, Miller RR: Early post-myocardial infarc-tion treadmill stress testing: An accurate predictor of multi-vessel coronary disease and subsequent cardiac events. AnnIntem Med 1981;94:734-739
12. Krone RJ, Gillespie JA, Weld FM, Miller JP, Moss AJ,Multicenter Postinfarction Research Group: Low-level exer-cise testing after myocardial infarction: Usefulness in enhanc-ing clinical risk stratification. Circulation 1985;71:80-89
13. Madsen EB, Gilpin E, Ahnve S, Henning H, Ross J Jr:Prediction of functional capacity and use of exercise testing forpredicting risk after acute myocardial infarction. Am J Cardiol1985;56:839-845
14. Turner JD, Schwartz KM, Logic JR, Sheffield LT, Kansall S,Roitman DI, Mantle JA, Russel RO, Rackley CE, Rogers WJ:Detection of residual jeopardized myocardium 3 weeks aftermyocardial infarction by exercise testing with thallium-201myocardial scintigraphy. Circulation 1980;61:729-737
15. Gibson RS, Beller GA, Gheorghiade M, Nygaard TW, WatsonDD, Huey BL, Sayre SL, Kaiser DL: The prevalence andclinical significance of residual myocardial ischemia 2 weeksafter uncomplicated non-Q wave infarction: A prospectivenatural history study. Circulation 1986;73:1186-1198
16. Corbett JR, Dehmer GJ, Lewis SE, Woodward W, HendersonE, Parkey RW, Blomqvist CG, Willerson JT: The prognosticvalue of submaximal exercise testing with radionuclide ventric-ulography prior to hospital discharge in patients with recentmyocardial infarction. Circulation 1981;64:535-544
17. Nicod P, Corbett JR, Firth BG, Lewis SE, Rude RE, HuxleyR, Willerson JT: Prognostic value of resting and submaximalexercise radionuclide ventriculography after acute myocardialinfarction in high-risk patients with single and multivesseldisease. Am J Cardiol 1983;52:30-36
18. Ryan T, Armstrong WF, O'Donnell JA, Feigenbaum H: Riskstratification after acute myocardial infarction by means ofexercise two-dimensional echocardiography. Am Heart J 1987;114:1305-1316
19. Armstrong WF, O'Donnell J, Ryan T, Feigenbaum H: Effectof prior myocardial infarction and extent and location ofcoronary disease on accuracy of exercise echocardiography. JAm Coll Cardiol 1987;10:531-538
20. Marshall RC, Tillisch JH, Phelps ME, Huang SC, Carson R,Henze E, Schelbert HR: Identification and differentiation ofresting myocardial ischemia and infarction in man withpositron computed tomography: '8F-Labeled fluorodeoxyglu-cose and N-13 ammonia. Circulation 1983;67:766-778
21. Tillisch J, Brunken R, Marshall R, Schwaiger M, MandelkernM, Phelps M, Schelbert H: Reversibility of cardiac wall-motion abnormalities predicted by positron tomography. NEnglJMed 1986;314:884-888
22. Epstein SE, Palmeri ST, Patterson RE: Evaluation of patientsafter acute myocardial infarction: Indications for cardiaccatheterization and surgical intervention. N Engl J Med 1982;307:1487-1492
23. DeBusk RF, Kraemer HC, Nash E: Stepwise risk stratificationsoon after acute myocardial infarction. Am J Cardiol 1983;52:1161-1166
24. Iskandrian AS, Hakki AH, Kotler MN, Segal BL, Herling I:Evaluation of patients with acute myocardial infarction:Which test, for whom and why?Am Heart J 1985;109:391-394
25. DeBusk RF, Blomqvist CG, Kochoukos NT, Luepker RV,Miller HS, Moss AJ, Pollock ML, Reeves TJ, Selvester RH,Stason WB, Wagner GS, Willman VL: Identification andtreatment of low-risk patients after acute myocardial infarc-tion and coronary-artery bypass graft surgery. N Engl J Med1986;314:161-166
26. Ross J Jr, Gilpin EA, Madsen EB, Henning H, Nicod P,Dittrich H, Engler R, Rittelmeyer J, Smith SC Jr, Viquerat C:A decision scheme for coronary angiography following acutemyocardial infarction. Circulation 1989;79:292-303
27. Joint American College of Cardiology/American Heart Asso-ciation Task Force on Assessment of Cardiovascular Proce-dures (Subcommittee on Coronary Angiography): Guidelinesfor coronary angiography. JAm Coll Cardiol 1987;10:935-950and Circulation 1987;76:963A-977A
28. Joint American College of Cardiology/American Heart Asso-ciation Task Force on Assessment of Diagnostic and Thera-peutic Cardiovascular Procedures (Subcommittee to DevelopGuidelines for the Early Management of Patients With AcuteMyocardial Infarction) Guidelines for the early managementof patients with acute myocardial infarction. JAm Coll Cardiol1990;16:249-292
29. Battler A, Karliner JS, Higgins CB, Slutsky R, Gilpin EA,Froelicher VF, Ross J Jr: The initial chest x-ray in acutemyocardial infarction: Prediction of early and late mortalityand survival. Circulation 1980;61:1004-1009
30. The Principal Investigators of CASS and Their Associates: TheNational Heart, Lung, and Blood Institute Coronary ArterySurgery Study (CASS). Circulation 1981;63(suppl I):I-1-1-39
31. Cornfield J: Discriminant function. White Plains, NY, Pro-ceedings of Sixth IBM Medical Symposium, 1964, p 567
32. Bishop YMM, Feinberg SE, Holland PW: Discrete MultivariateAnalysis: Theory and Practice. Cambridge, Mass, MIT Press,1974, p 357
33. Breiman L, Friedman JH, Olshen RA, Stone CJ: Classificationand Regression Trees. Belmont, Calif, Wadsworth InternationalGroup, 1984, p 18
34. Topol EJ: Coronary angioplasty for acute myocardial infarc-tion. Ann Intem Med 1988;109:970-980
35. TIMI Research Group: Immediate vs delayed catheterizationand angioplasty following thrombolytic therapy for acute myo-cardial infarction: TIMI IIA results. JAMA 1988;260:2849-2858
36. TIMI Research Group: Comparison of invasive and conserva-tive strategies after treatment with intravenous tissue plasmin-ogen activator in acute myocardial infarction. TIMI II results.N Engl JMed 1989;320:618-627
37. Lee TH, Weisberg MC, Brand DA, Rouan GW, Goldman L:Candidates for thrombolysis among emergency room patientswith acute chest pain: Potential true and false-positive rates.Ann Intem Med 1989;110:957-962
38. Little WC, Constantinescu M, Applegate RJ, Kutcher MA,Burrows MT, Kahl FR, Santamore WP: Can coronary angiog-raphy predict the site of a subsequent myocardial infarction inpatients with mild-to-moderate coronary artery disease? Cir-culation 1988;78:1157-1166
39. European Cooperative Study Group for Recombinant Tissue-Type Plasminogen Activator (rTPA): Thrombolysis with tissueplasminogen activator in acute myocardial infarction: Noadditional benefit from immediate percutaneous coronaryangioplasty. Lancet 1988;1:197-203
40. Breyer RH, Engleman RM, Rousou JA, Lemeshow S: Postin-farction angina: An expanding subset of patients undergoingcoronary artery bypass. J Thorac Cardiovasc Surg 1985;90:532-540
41. Gilpin E, Ricou F, Dittrich H, Nicod P, Henning H, Ross J Jr:Factors associated with recurrent myocardial infarction within1 year after acute myocardial infarction.Am Heart J (in press)
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

Nicod et al Coronary Angiography After Myocardial Infarction 1015
42. Passamani E, Davis KB, Gillespie MJ, Killip T, CASS Princi-pal Investigators and Their Associates: A randomized trial ofcoronary artery bypass surgery: Survival of patients with a lowejection fraction. N Engl J Med 1985;312:1665-1671
43. Killip T, Passamani E, Davis K, CASS Principal Investigatorsand Their Associates: Coronary Artery Surgery Study (CASS):A randomized trial of coronary bypass surgery. Eight-yearfollow-up and survival in patients with reduced ejection frac-tion. Circulation 1985;72(suppl V):V-102-V-109
44. Braunwald E: Myocardial reperfusion, limitation of infarctsize, reduction of left ventricular dysfunction, and improvedsurvival: Should the paradigm be expanded? Circulation 1989;79:441-444
45. McNeer JF, Margolis JR, Lee KL, Kisslo JA, Peter RH, KongY, Behar VS, Wallace AG, McCants CB, Rosati RA: The roleof the exercise test in the evaluation of patients for ischemicheart disease. Circulation 1978;57:64-70
46. Weiner DA, Ryan TJ, McCabe CH, Chaitman BR, Sheffeld T,Ferguson JC, Fisher LD, Tristani F: Prognostic importance of
a clinical profile and exercise test in medically treated patientswith coronary artery disease.JAm Coll Cardiol 1984;3:772-779
47. Ladenheim ML, Pollock BH, Rozanski A, Berman DS,Staniloff HM, Forrester JS, Diamond GA: Extent and severityof myocardial hypoperfusion as predictors of prognosis inpatients with suspected coronary artery disease. J Am CollCardiol 1986;7:464-471
48. Pryor DB, Harrell FE, Lee KL, Rosati RA, Coleman RE,Cobb FR, Califf RM, Jones RH: Prognostic indicators forradionuclide angiography in medically treated patients withcoronary artery disease. Am J Cardiol 1984;53:18-22
49. Bonow RO, Kent KM, Rosing DR, Lan KKG, Lakatos E,Borer JS, Bacharach SL, Green WV, Epstein SE: Exercise-induced ischemia in mildly symptomatic patients with coro-
nary artery disease and preserved left ventricular function. NEnglJ Med 1984;311:1339-1345
KEY WORDS * myocardial infarction * coronary angiography
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from





























