Embed Size (px)
Citation preview

www.elsevier.com/locate/humpath
Human Pathology (2009) 40, 624–630
Original contribution
Treponema pallidum distribution patterns inmucocutaneous lesions of primary and secondary syphilis:an immunohistochemical and ultrastructural studyGemma Martín-Ezquerra MDa,⁎, Alex Fernandez-Casado MDa, Dídac Barco MDb,Anna Jucglà MDc, Núria Juanpere-Rodero MDh, Josep Maria Manresa PhD j,Luis Miguel Soares de Almeida MDd, Jose Luis Rodríguez-Peralto MDe,Heinz Kutzner MD f, Lorenzo Cerroni MDg, Carles Barranco MDh, Josep Lloreta MDh,Luis Requena MD i, Ramon M. Pujol MDa
aDepartment of Dermatology, Hospital del Mar-IMAS, Barcelona, 08003bDepartment of Dermatology, Hospital de la Santa Creu i Sant Pau, Barcelona, 08025cDepartment of Dermatology, Hospital de Bellvitge, Barcelona, 08907dDepartment of Dermatology, Hospital de Santa María, Universidad de Lisbon, Lisbon, Portugal, 1649035eDepartment of Pathology, Hospital Universitario 12 de Octubre, Universidad Complutense, Madrid, Spain, 28030fDermatopathologische Gemeinschaftslabor, Friederichshafen, Germany, 88048gDepartment of Dermatology, Medical University of Graz, Graz, Austria, 8010hDepartment of Pathology, Hospital del Mar-IMAS, Barcelona, 08003iFundación Jiménez-Díaz, Madrid, Spain, 28040jAMIB, IMIM, Barcelona, 08003
Received 8 July 2008; revised 2 October 2008; accepted 7 October 2008
0d
Keywords:Syphilis;Treponema;Epitheliotropic;Endotheliotropic
Summary To study the different patterns of Treponema pallidum distribution in primary and secondarysyphilis, 34 biopsy specimens of 8 patients with primary and 26 with secondary syphilis were assessed.Histopathological features, silver stain, and immunohistochemical T pallidum polyclonal antibodyexpression were investigated. The number and distribution of spirochetes were evaluated, andultrastructural studies were performed. Spirochetes were identified with Warthin-Starry stain in 17specimens (4/8 primary and 13/26 secondary syphilis), whereas immunohistochemical analysisdisclosed spirochetes in 29 (8/8 primary and 21/26 secondary syphilis). In secondary syphilis, anepitheliotropic pattern characterized by abundant spirochetes in the lower mucosa/epidermis in anintercellular distribution was observed. In contrast, primary syphilis exhibited a mixed epitheliotropicand vasculotropic pattern further manifested by treponemes surrounding the vascular walls. Thesedifferences were statistically significant. Ultrastructural examination confirmed these results.Immunohistochemistry shows greater sensitivity when compared with Warthin-Starry staining. The
⁎ Corresponding author.E-mail address: [email protected] (G. Martín-Ezquerra).
046-8177/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2008.10.017

625Treponema pallidum distribution patterns in mucocutaneous lesions of primary and secondary syphilis
immunohistochemical pattern of T pallidum distribution may permit the diagnostic differentiation ofprimary from secondary syphilis.© 2009 Elsevier Inc. All rights reserved.
1. Introduction Several technical approaches such as direct and indirect
Treponema pallidum in formalin-fixed tissue sections hasclassically been identified using silver-impregnation stainingtechniques such as the Levaditi or Warthin-Starry (WS)stains. Nevertheless, when evaluating silver stained muco-cutaneous histologic slides, difficulties often arise duemostly to the nonspecific, artifactual background stainingof tissue elements (ie, reticulum fibers, melanin), which maygive rise to false-positive or false-negative results [1].
Table 1 Clinical features, evolution and presence of T pallidum in b
Sex/age (y) Clinical features Time of evol
Primary syphilisM/41 Ulcerated nodule on the tongue NDM/23 Genital ulcer 3 wkM/34 Genital ulcer 3 wkM/30 Genital ulcer 4 wkM/46 Genital ulcer NDF/20 Genital ulcer NDM/74 Genital ulcer 2 wkM/41 Ulcer on the lip 3 wk
Secondary syphilisM/40 Maculopapular eruption (roseola) 3 wkM/42 Maculopapular eruption (roseola) 3 wkM/53 Maculopapular eruption (roseola) NDM/22 Maculopapular eruption (roseola) NDM/25 Maculopapular eruption (roseola) 1 moM/48 Maculopapular eruption (roseola) 2 wkM/34 Maculopapular eruption (roseola) 2 wkM/34 Maculopapular eruption (roseola) 6 wkM/67 Maculopapular eruption (roseola) NDM/47 Maculopapular eruption (roseola) NDF/36 Maculopapular eruption (roseola) NDF/29 Maculopapular eruption (roseola) NDM/25 Maculopapular eruption (roseola) NDM/51 Maculopapular eruption (roseola) 4 moF/32 Maculopapular eruption (roseola) 2 wkM/26 Maculopapular eruption (roseola) 2 moM/28 Maculopapular eruption (roseola) 1 moM/55 Maculopapular eruption (roseola) 2 wkM/35 Maculopapular eruption (roseola) 1 wkM/39 Maculopapular eruption (roseola) 2 wkM/38 Maculopapular eruption (roseola) 4 moM/41 Maculopapular eruption (roseola) 3 wkM/78 Penile erosion NDF/27 Vulvar erosion NDF/43 Vulvar erosion 3 wkF/20 Oral erosions 1 mo
+++, high density; ++, moderate density; +, low density; M, male; F, Female; N
immunofluorescence and immunoperoxidase techniqueshave been proposed to improve T pallidum spirochetevisualization in fresh, frozen, or paraffin-embedded tissuepreparations [2]. Recently, immunoperoxidase techniques,using specific polyclonal antibodies against T pallidum, havebeen advocated as sensitive and useful methods to avoidbackground staining and facilitate the identification andvisualization of spirochetes in paraffin-embedded tissues [3].Theoretically, this technical approachmay allowmore precise
iopsy specimens (WS stain and immunohistochemical results)
ution WS stain Antitreponemal stain HIV status
+ +++ ++ +++ –– +++ ++ +++ –– +++ ND+ +++ –– +++ –– +++ –
– – +– – ++ ++ +– ++ –– + –+ ++ ND– + +– + –+ ++ –– – –+ +++ –– +++ ++ ++ –– – –+ + +– + +– – ++ ++ ++ ++ ND– + +– +++ –– +++ –+ + ND– +++ +– +++ ++ +++ –
D: nondata.
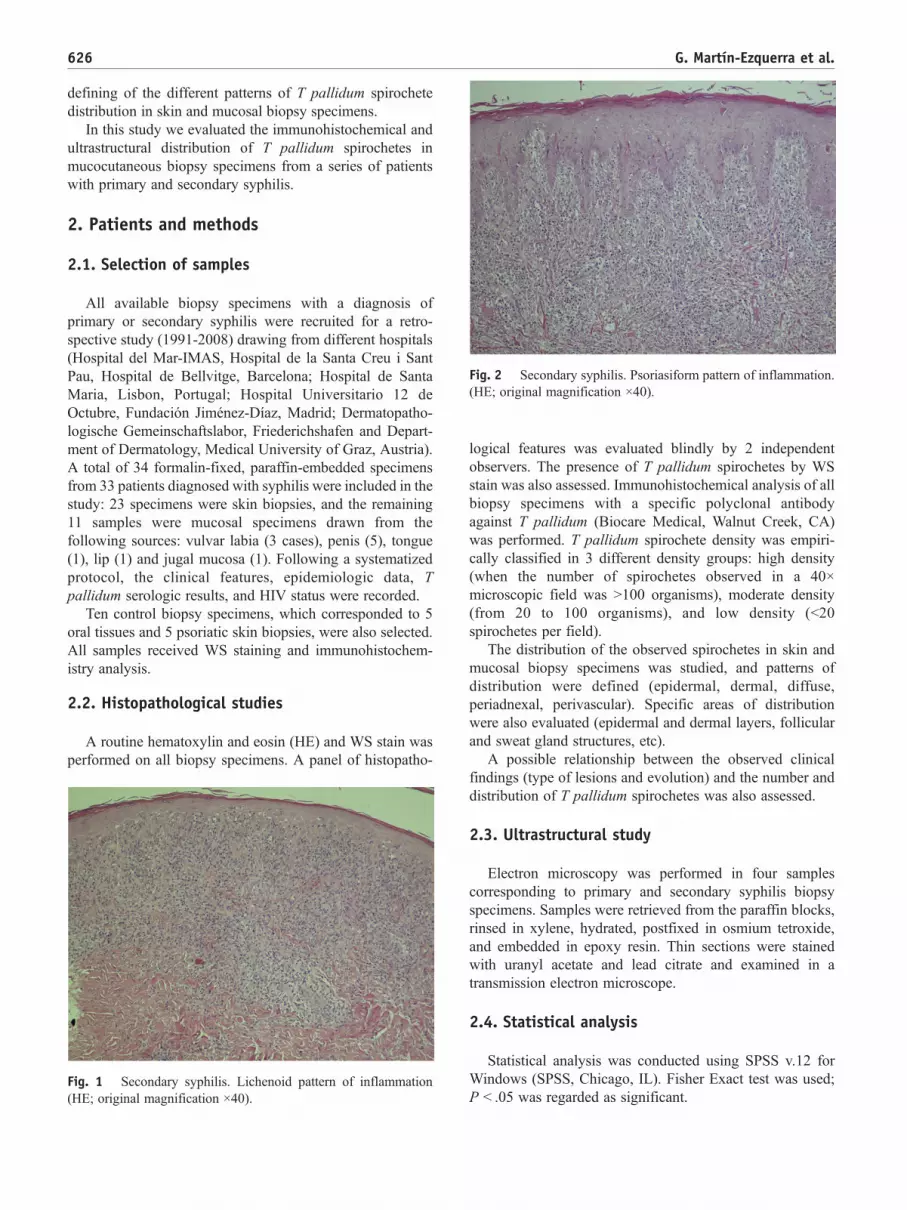
Fig. 2 Secondary syphilis. Psoriasiform pattern of inflammation.(HE; original magnification ×40).
626 G. Martín-Ezquerra et al.
defining of the different patterns of T pallidum spirochetedistribution in skin and mucosal biopsy specimens.
In this study we evaluated the immunohistochemical andultrastructural distribution of T pallidum spirochetes inmucocutaneous biopsy specimens from a series of patientswith primary and secondary syphilis.
2. Patients and methods
2.1. Selection of samples
All available biopsy specimens with a diagnosis ofprimary or secondary syphilis were recruited for a retro-spective study (1991-2008) drawing from different hospitals(Hospital del Mar-IMAS, Hospital de la Santa Creu i SantPau, Hospital de Bellvitge, Barcelona; Hospital de SantaMaria, Lisbon, Portugal; Hospital Universitario 12 deOctubre, Fundación Jiménez-Díaz, Madrid; Dermatopatho-logische Gemeinschaftslabor, Friederichshafen and Depart-ment of Dermatology, Medical University of Graz, Austria).A total of 34 formalin-fixed, paraffin-embedded specimensfrom 33 patients diagnosed with syphilis were included in thestudy: 23 specimens were skin biopsies, and the remaining11 samples were mucosal specimens drawn from thefollowing sources: vulvar labia (3 cases), penis (5), tongue(1), lip (1) and jugal mucosa (1). Following a systematizedprotocol, the clinical features, epidemiologic data, Tpallidum serologic results, and HIV status were recorded.
Ten control biopsy specimens, which corresponded to 5oral tissues and 5 psoriatic skin biopsies, were also selected.All samples received WS staining and immunohistochem-istry analysis.
2.2. Histopathological studies
A routine hematoxylin and eosin (HE) and WS stain wasperformed on all biopsy specimens. A panel of histopatho-
Fig. 1 Secondary syphilis. Lichenoid pattern of inflammation(HE; original magnification ×40).
logical features was evaluated blindly by 2 independentobservers. The presence of T pallidum spirochetes by WSstain was also assessed. Immunohistochemical analysis of allbiopsy specimens with a specific polyclonal antibodyagainst T pallidum (Biocare Medical, Walnut Creek, CA)was performed. T pallidum spirochete density was empiri-cally classified in 3 different density groups: high density(when the number of spirochetes observed in a 40×microscopic field was N100 organisms), moderate density(from 20 to 100 organisms), and low density (b20spirochetes per field).
The distribution of the observed spirochetes in skin andmucosal biopsy specimens was studied, and patterns ofdistribution were defined (epidermal, dermal, diffuse,periadnexal, perivascular). Specific areas of distributionwere also evaluated (epidermal and dermal layers, follicularand sweat gland structures, etc).
A possible relationship between the observed clinicalfindings (type of lesions and evolution) and the number anddistribution of T pallidum spirochetes was also assessed.
2.3. Ultrastructural study
Electron microscopy was performed in four samplescorresponding to primary and secondary syphilis biopsyspecimens. Samples were retrieved from the paraffin blocks,rinsed in xylene, hydrated, postfixed in osmium tetroxide,and embedded in epoxy resin. Thin sections were stainedwith uranyl acetate and lead citrate and examined in atransmission electron microscope.
2.4. Statistical analysis
Statistical analysis was conducted using SPSS v.12 forWindows (SPSS, Chicago, IL). Fisher Exact test was used;P b .05 was regarded as significant.

627Treponema pallidum distribution patterns in mucocutaneous lesions of primary and secondary syphilis
3. Results
Thirty-four biopsies from 33 patients (26 men and 7women with a mean age of 39 years) were included in thestudy. The diagnosis of primary (8 patients) or secondary (26patients) syphilis was established based on characteristicclinical and serologic findings. Fourteen patients werepositive for HIV infection. Detailed clinical features aresummarized in Table 1.
3.1. Histologic findings
Histologically, in primary syphilis, epithelial ulcerationwas a constant feature. In two mucosal ulcerated samples,no overlying or adjacent epithelium was present. Apredominantly diffuse chorial or dermal infiltration extend-ing to the deep dermis and subcutaneous tissue (7 of 8cases) was also present, composed mainly of lymphocytesand plasma cells. Vascular involvement, manifested byprominent and swollen endothelial cells and a predomi-
Table 2 Histopathological features and immunohistochemicalpatterns of T pallidum distribution
Primary syphilis(n = 8) (%)
Secondary syphilis(n = 26) (%)
P a
Histopathological featuresA. Epidermal/mucosal changesErosion 0 5 (19%) NSUlceration 5 (62%) 0 b.001Necrotickeratinocytes
5 (62%) 17 (65%) NS
Exocytosis 3 (37%) 15 (58%) NSPurpura 1 (12%) 0 NSParakeratosis 0 9 (34%) .059B. Corial or dermal infiltrate:Superficial 0 21 (81%) b.001Diffusesuperficial anddeep
7 (87%) 8 (30%) .011
Lymphocytes ++ ++Histiocytes + +Plasma cells ++ ++Granulomatousinflammation
3 (37%) 10 (38%) NS
C. Vascular changes:Prominentendothelialcells
8 (100%) 16 (61%) .041
Dilated bloodvessels
8 (100%) 16 (61%) .041
Pattern of T pallidum distribution:Epitheliotropic 0 21 (81%) b.001Mixt 6 (75%) 0 b.001Vasculotropic 2 b (25%) 0 .050
a Fisher Exact test.b No mucosal representation.
nantly plasmacytic perivascular infiltrate, was also detectedin all (8/8) biopsy specimens.
In secondary syphilis, the most common pattern was aband-like infiltrate in the upper dermis and a perivascularand periadnexal infiltrate in the mid and deep dermis.Variable numbers of necrotic keratinocytes were also noted.This lichenoid inflammatory pattern (Fig. 1) was present in17 of 26 cases. In 9 cases, a psoriasiform pattern wasobserved, manifested by acanthosis, parakeratosis, andregular epidermal hyperplasia, along with a perivascularand periadnexal infiltrate in the mid dermis (Fig. 2).Occasional necrotic keratinocytes were also noted in 17 ofthe 26 cases. The infiltrate was moderate to dense in allcases, with a predominance of plasma cells, althoughhistiocytes and lymphocytes were also present. A granulo-matous inflammatory infiltration was found in 10 of 26cases. Endothelial involvement resulting in prominence ofendothelial cells and dilated blood vessels was observed in16 biopsy specimens (Table 2).
Statistically significant differences could be seen inprimary syphilis focused on the presence of ulceration anddeep and superficial infiltration, and the presence of para-keratosis and superficial infiltration in secondary syphilis.
3.2. WS staining
WS staining led to the identification of treponemes in 17of 34 paraffin-embedded biopsy specimens (50%), corre-sponding to 4 of 8 primary syphilis and 13 of 26 secondarysyphilis cases. Spirochetes were identified in variablenumbers and scattered throughout the epidermis and theupper dermis. However, the background silver staining madeit impossible to precisely define a particular pattern ofT pallidum distribution. Control cases of inflammatorycutaneous disorders were negative under WS stain analysis.
3.3. Immunohistochemistry withantitreponemal stain
Immunohistochemical evaluation of all biopsy specimenswith anti–T pallidum antibody detected spirochetes in 29biopsies (80%), corresponding to the 8 cases of primarysyphilis and to 21 of 26 cases of secondary syphilis.Spirochetes, presenting a characteristic spiral structure high-lighted by the chromogen, were easily identified. No back-ground staining was present. All WS-determined positiveswere also positive with the immunohistochemical technique.
The 5 cases of secondary syphilis found negative forantitreponemal antibody corresponded to 3 patients who hadbeen previously treated with several antibiotic regimens, 1patient presenting with a long-standing secondary syphiliscutaneous eruption (more than 3 months), and 1 patient withsecondary syphilis of unknown evolution. Three of thesecases were HIV-coinfected patients. All control samples werenegative for anti-Treponema pallidum polyclonal antibodies.

Fig. 3 T pallidum distribution in primary syphilis. Vasculotropicpattern: numerous spirochetes delineating the submucosal vascularstructures (antitreponemal antibodies; original magnification ×400).
Fig. 5 Epitheliotropic pattern: treponemes within the follicularinfundibular epithelia (inset) (antitreponemal antibodies; originalmagnification ×200).
628 G. Martín-Ezquerra et al.
Different patterns of T pallidum distribution wereobserved (Table 2). In all primary syphilis biopsy specimens,a large number of spirochetes distributed in the dermis orlamina propria were present. Numerous spirochetes arrangedpredominately in a perivascular pattern were noted (Fig. 3).Treponemal organisms surrounded the vascular walls, high-lighting its shape. This peculiar pattern of distribution wasdefined as “vasculotropic pattern.” In 6 of the primarysyphilis biopsy specimens, in addition to this “vasculotropicpattern,” abundant T pallidum with an intercellular distribu-tion was also noted within the lower layers of the epitheliumadjacent to the ulceration. This was defined as a “mixedvasculotropic-epitheliotropic pattern” of distribution.
In contrast, the spirochetes in secondary syphilis wereprimarily located within the epidermis, mainly in its lower
Fig. 4 Epidermal distribution of T pallidum in secondarysyphilis. Epitheliotropic pattern: numerous spirochetes within thelower layers of the epidermis showing an intercellular distribution.Close-up view showing abundant spirochetes in the epidermis(inset).
layers (in the basal layer and up to the 5 upper layers), havingan intercellular distribution that delineated the keratinocytewalls (Figs. 4 and 5). This distribution, suggestive of aspecific tropism of T pallidum for superficial epithelia, wasdefined as “epitheliotropic pattern.” Scattered treponemeswere also noted either in more superficial epidermal layers orin the papillary dermis. In 5 biopsy specimens, abundant Tpallidum spirochetes were observed to be distributed withinthe follicular infundibular epithelia and acrosyringia or uppersweat gland duct epithelial cells (Fig. 5, inset). In 2 casesshowing a marked pseudoepitheliomatous hyperplasia,spirochetes did not tend to involve the deep elongated reteridges and were mainly distributed within the mid layers ofthe epidermis. The difference between these distributionpatterns is statistically significant.
Fig. 6 Primary syphilis. Electron micrograph showing trepo-nemes squeezed between adjacent pericytes and smooth musclecells of a dermal arteriole. In some sections, the microorganismsseem to be located in invaginations of the cells, but true endocytosisis not observed (inset).

Fig. 7 Ultrastructural features in secondary syphilis. In additionto occasional microorganisms in blood vessels, abundant trepo-nemes are found in the epidermis in secondary syphilis. They arelocated between keratinocytes, in invaginations, and in intercellularspaces similar to those of smooth muscle cells (inset).
629Treponema pallidum distribution patterns in mucocutaneous lesions of primary and secondary syphilis
In all biopsy specimens corresponding to primarysyphilis, a consistently high density of treponemes wasdemonstrated, whereas a variable density of treponemeswas found in those corresponding to secondary syphilis(high density in 7 cases, moderate density in 6, and lowdensity in 8). In secondary syphilis, no relationship could bedemonstrated between spirochete density and the evolutionof the disease or the serological titers. No associationsbetween density of treponeme and HIV status were recorded.
3.4. Ultrastructural study
Ultrastructural examination revealed the same distribu-tion patterns found by immunohistochemistry. Thus,microorganisms were more often found in blood vesselwalls in primary syphilis and were predominantly inter-epithelial in secondary syphilis (Figs. 6 and 7). In thevasculotropic pattern, spirochetes were identified betweensmooth muscle cells and pericytes, and some were alsoseen between smooth muscle and adjacent endothelial cells.Microorganisms were usually found in slit-like intercellularspaces and sometimes seemed to be completely surroundedby cell cytoplasm—a finding that was probably the resultof invaginations of the plasma membrane, however, withoutthe features of phagocytotic vesicles. The location ofspirochetes was similar in the epitheliotropic pattern—Tpallidum spirochetes were squeezed among adjacentepithelial cells, in the intercellular spaces between inter-cellular bridges, and sometimes seemed to displace orinvaginate the cell membrane without actually beingincorporated into the cell cytoplasm or phagocytic vesicles.Although the epithelial location predominated in the casesof secondary syphilis, perivascular microorganisms werealso found.
4. Discussion
The histopathological distribution and number ofT pallidum spirochetes in mucocutaneous lesions of syphilishave been assessed in several studies [4-7]. It is consideredthat T pallidum can be detected in large numbers in skinlesions only during the primary and early secondary stages ofsyphilis. As the disease progresses, spirochetes becomescarce, and in late stage syphilis, they seem to disappear. Inour study, we confirmed the presence of numerous Tpallidum spirochetes in either primary or early secondarysyphilitic lesions, with a higher density of treponemes foundin primary syphilitic lesions.
The histology of primary syphilis consists of an ulcercovered by necrotic material and cellular debris. The base ofthe ulcer consists of numerous dilated vessels and apredominantly perivascular infiltrate composed of lymphoidcells and many plasma cells [8]. Vascular involvementmanifested by swelling and proliferation of endothelial cellshas been classically considered an early phenomenon inprimary syphilis [9]. Although vasculitis could not bedemonstrated in any of our specimens, vascular involvementwas prominent and treponemes affected the endothelial wall.In the literature, syphilis is described as a cause of cutaneousvasculitis [10], although it is a rare phenomenon. With theuse of silver stains, it is possible to demonstrate the presenceof numerous treponemal organisms. It has been suggestedthat the number of spirochetes in primary syphilis is smallerthan in yaws and pinta [7]. However, upon silver stainingspirochetes can be found diffusely in the dermis and aroundthe wall of the capillaries.
In contrast, there is considerable variation in the clinicaland histopathological patterns of secondary syphilis, aboutwhich it has been stated that the number of spirochetes seenin sections analyzed with a silver stain varies with the type oflesion. In papular lesions, only modest numbers oftreponemes are present, whereas in most hypertrophicpapules, numerous treponemes could be demonstrated inthe dermis or submucosae. Some authors have pointed outthe presence of numerous organisms in the epidermis [9].
In our series, immunohistochemical assessment withanti-Treponema pallidum polyclonal antibodies showed ahigher diagnostic sensitivity than the routine WS staining(50% versus 80%). These results are in agreement withprevious studies (WS: 31%-71% [4,7] versus immunohis-tochemistry: 74%-94% [1,9]). Negative immunohistochem-ical results could be related to either previous antibiotictreatments or to long-standing secondary syphilis lesions.In 3 cases, coinfection with HIV was present: negativeresults could be explained by the previous use of antibioticsbefore a definitive diagnosis was achieved. However, norelationship between HIV status and spirochete densitycould be demonstrated.
In order to define more precisely the different patterns ofdistribution of T pallidum in mucocutaneous lesions ofsyphilis, Engelkens et al [7] studied skin biopsies from

630 G. Martín-Ezquerra et al.
44 patients (29 patients with primary and 15 patients withsecondary syphilis) using Steiner silver staining, as well asantibodies against T pallidum with immunofluorescencetechniques. The presence of treponemes was detected in 28of 29 biopsy samples of primary syphilis. These authorsreported that, in most cases, T pallidum could be observedat the dermal-epidermal junction. However, they alsopointed out that in the dermis most treponemes were seenperivascularly. In secondary syphilis, spirochetes weremainly observed in the dermal-epidermal junction zone orthroughout the dermis, frequently located perivascularly. Noclear-cut differences were reported regarding the treponemaldistribution between primary and secondary syphilis.
Nakamura et al [5] investigated the histologic distributionof T pallidum in the syphilitic lesions by using directimmunofluorescence techniques. Most treponemes werelocated around vessels in macular syphilitic lesions, and inthe epidermis in papular syphilitic lesions. On the other hand,Chung et al [6] stated that treponemes were distributed in theepidermis, dermoepidermal junction, papillary dermis, andvessel walls in chancres, macular syphilides, and condylomalata lesions. Nevertheless, Lee et al [4] were unable to detectmarked differences in the histologic distribution of trepo-nemes among the clinical stages and types of syphilis. Buffetet al [11] reported the presence of treponemes in 90% ofsecondary syphilis cases, with the microorganisms beinglocated in the epidermis, upper dermis, and perivascular areas.
In our experience, T pallidum distribution patterns may bea useful morphological feature in differentiating betweenprimary and secondary syphilis cases. All skin and mucosalsamples of secondary syphilis lesions in our series showed asimilar pattern of T pallidum distribution: spirochetes weremainly located within the basal and suprabasal epithelium/epidermis in an intercellular distribution delineating thekeratinocyte walls (“epitheliotropic pattern”) (Figs. 4 and 5).Treponemes were usually absent in the upper layers of thestratum spinosum. However, scattered spirochetes distrib-uted within the upper follicular epithelium or acrosyringia(when present) were occasionally observed. This peculiartropism of T pallidum for the epidermis can explain thepotential infectivity of secondary syphilitic lesions.
In primary syphilis, however, numerous spirochetes wereadditionally observed in a perivascular distribution involvingand delineating the upper and mid submucosal vessels. Thisparticular “vasculotropic pattern” was often combined withscattered or numerous treponemes in a more diffusesubmucosal distribution. The further identification of multi-ple spirochetes distributed intercellularly within the basaland suprabasal epithelia adjacent to the ulcer also conformedto the “vasculotropic-epitheliotropic” or “mixed pattern.”
Several ultrastructural studies in mucocutaneous lesionsof syphilis have also been previously reported [12].Wrzolkowa et al [13] described the vascular changes inprimary syphilis, with the accumulation of treponeme incapillaries. Poulsen et al [12] demonstrated a diffuseextracellular distribution of treponeme, in modest numbers,
in secondary syphilis, in both the epidermis and dermis. Inour ultrastructural study, we have confirmed a very selectiverelationship of T pallidum microorganisms with blood vesselwalls, in which they are mostly located among smoothmuscle cells and pericytes, and only rarely reach the outeraspect of endothelial cells. On the other hand, in secondarycases, although still some spirochetes were found in bloodvessel walls, they show a striking trend towards epidermallocation. In all cases, they are extracellular in the smallintercellular spaces between adjacent cell junctions.Although some treponemes seem completely surroundedby cell cytoplasm and appear to be enveloped by cellmembrane, different planes of sectioning suggest that this isan invagination rather than true phagocytosis.
In conclusion, our study confirms the diagnostic useful-ness of T pallidum antibodies in mucocutaneous lesions ofprimary and secondary syphilis. Characteristic patterns ofT pallidum distribution in primary and secondary syphiliswere observed, providing new insight into the pathogenicmechanisms of the disease.
References
[1] Hoang M, High W, Molberg K. Secondary syphilis: a histologic andimmunohistochemical evaluation. J Cutan Pathol 2004;31:595-9.
[2] Beckett J, Bigbec J. Immunoperoxidase localization of Treponemapallidum. Arch Pathol Lab Med 1979;103:135-8.
[3] Phelps RG, Knispel J, Tu ES, Cernainu G, Saruk M. Immunoperox-idase technique for detecting spirochetes in tissue sections: comparisonwith other methods. Int J Dermatol 2000;39:609-13.
[4] Lee WS, Lee MG, Chung KY, Lee JB. Detection of Treponemapallidum in tissue: a comparative study of the avidin-biotin-peroxidase complex, indirect immunoperoxidase. Yonsei Med J1991;32:335-41.
[5] Nakamura S, Ito F, Nakamura S, Onda S. Improved methods for thedemonstration of treponema pallidum in tissues. J Dermatol 1983;10:433-7.
[6] Chung KY, Lee MG, Lee JB. Detection of Treponema pallidumin tissue by FTA-ABS complement test. Kor J Dermatol 1987;25:486.
[7] Engelkens HJ, ten Kate FJ, Judanarso J, Vuzevski VD, van Lier JB,Godschalk JC, van der Sluis JJ, et al. The localisation of treponemesand characterisation of the inflammatory infiltrate in skin biopsies frompatients with primary or secondary syphilis, or early infectious yaws.Genitourin Med 1993;69:102-7.
[8] Kolker SE, Manz HJ, Schwartz DA. Syphilis. Pathology of infectiousdiseases. Stamford, CT: Appleton & Lange; 1997. p. 833-46.
[9] Sangüenza O, Fleet S, Requena L. Histologic findings of cutaneousinfections. Adv Dermatol 2000;16:361-423.
[10] Chao YC, Chen CH, Chen YK, Chou CT. A large ulcer and cutaneoussmall-vessel vasculitis associated with syphilis infection. Scand JRheumatol 2006;35:147-51.
[11] Buffet M, Grange PA, Gerhardt P, Carlotti A, Calvez V, Bianchi A,et al. Diagnosing Treponema pallidum in secondary syphilis by PCRand immunohistochemistry. J Invest Dermatol 2007;127:2345-50.
[12] Pulsen A, Kobayasi T, Secher L, Weissmann K. Treponema pallidumin human Chancre tissue: an electron microscopic survey. Acta DermVenereol (Stockh) 1986;66:423-30.
[13] Wrzolkowa T, Kozakiewicz J. Ultrastructure of vascular andconnective tissue changes in primary syphilis. Br J Vener Dis 1980;56:137-43.





























