Embed Size (px)
Citation preview

AXIS Vol. 4, Issue 2 (Spring 2013) 1
Variation of Suprascapular Artery
Abduelmenem Alashkhama,b, Abdulrahman Alraddadia,c, Roger Soamesa
a Centre for Human Anatomy and Identification, University of Dundee, Dundee, UK
b Human Anatomy Department, Faculty of Medicine, University of Zawia, Zawia, Libya
c Human Anatomy Department, Faculty of Medicine, King Saud Bin Abdulaziz University for Health Sciences , Riyadh, Saudi Arabia.
Abstract
In a routine dissection of the left shoulder of a
62 years old female, the suprascapular artery
was observed to arise from the thyrocervical
trunk of the 1st part of the subclavian artery. It
passed anterior to scalenus anterior and ran
posterolateral anterior to the brachial plexus
and deep to the clavicle and subclavius. By
tracing its course the suprascapular artery
was found to accompany the suprascapular
nerve underneath the transverse scapular
ligament to reach the supraspinatus fossa and
then the infraspinatus fossa through the
spinoglenoid notch to share in the
anastomosis around the scapula. The right
suprascapular artery passed over the ligament
which is an important variation in cases of
suprascapular nerve compression.
Introduction
The suprascapular artery is a branch of the
thyrocervical trunk from the 1st part of the
subclavian artery (Palastanga et al., 2006;
Moore et al., 2010).
As the suprascapular artery arises from the
thyrocervical trunk of the 1st part of the
subclavian artery (Smith et al., 1983; Hall-
Craggs, 1990; Monkhouse, 2001) it runs
inferolaterally and posterior undercover of
sternomastoid crossing anterior to scalenus
anterior and the phrenic nerve to reach the
posterior triangle of the neck. It crosses the
3rd part of the subclavian artery, as well as the
brachial plexus, and descends posterior and
parallel to the clavicle and subclavius
undercover of the posterior belly of omohyoid
accompanied by the suprascapular nerve until
they approach the superior border of the
scapula. Once the suprascapular artery
reaches the superior border, it passes
superficial to the transverse scapular
ligament, separating it from the suprascapular
nerve, and enters the supraspinous fossa
deep to supraspinatus. It then emerges
through the spinoglenoid notch to reach the
infraspinous fossa and descends inferiorly as
far as the inferior angle of the scapula and
shares in the anastomosis around the scapula
(Gray, 1913; Sinnatamby, 2006; Faiz and
Moffat, 2006; Ellis, 2006).

AXIS Vol. 4, Issue 2 (Spring 2013) 2
The suprascapular artery normal gives 7
branches; (1) branches: which contribute to
the anastomosis around the scapula (Rogers,
1992; Abrahams et al., 2011), (2) Acromial
branch: emerges through trapezius to supply
the skin over the acromion and anastomoses
with the acromial branch of the
thoracoacromial artery (Gray, 1913); (3)
Nutrient branches: to the clavicle and scapula
(Gray, 1913); (4) Articular branches: to the
shoulder and acromioclavicular joints (Lumley
et al., 1995; Gray, 1913); (5) Muscular
branches: to sternomastoid, subclavius and
muscles of the shoulder girdle (Lumley et al.,
1995); (6) Suprasternal branch: supplies the
skin over the upper part of the thorax (Gray,
1913); (7) Subscapular branch: a small branch
arising at the transverse scapular ligament
which runs downwards into the subscapular
fossa to ramify in subscapularis (Gray, 1913;
Snell, 1995).
Various studies have evaluated the anomalies
of the suprascapular artery. Yang et al (2012)
demonstrated, in a study of 103 shoulders (53
right side and 50 left with a mean age 70.4
years: 28 males, 27 females paired shoulders)
that the presence of the suprascapular artery
can be classified into three types, type I: the
suprascapular vessels pass over the transverse
scapular ligament, observed in 59.4% of cases;
type II: the suprascapular vessels pass over
and beneath the scapular ligament, observed
in 29.7%; type III: all the suprascapular vessels
pass below the scapular ligament, observed in
10.9% of specimens. Yang et al (2012) also
noted that in 48.9% of specimens all types
were observed bilaterally. Mishra and Ajmani
(2003) reported that on the left side the
suprascapular artery originated from the
axillary artery from which it then ascended for
a short distance and then ran transversely
undercover of the clavicle, subclavius and the
lower trunk of the brachial plexus. Once the
suprascapular artery approached the superior
border of the scapula, it passed through the
suprascapular foramen accompanied by the
suprascapular nerve to reach the
supraspinatus fossa. Mahato (2010) reported
a case of a 68 year old male cadaver in which
the suprascapular arteries on both sides arose
from the third part of the axillary artery
instead the thyrocervical trunk of the
subclavian artery. Both ascended upwards to
lie between the lateral cord of the brachial
plexus anteriorly and the posterior cord
posteriorly. On both sides, the suprascapular
artery passed under the transverse scapular
ligament with the suprascapular nerve to
emerge into the supraspinatus fossa. In the
dissection of 30 cadavers Adibatti (2010)
reported a case where the left suprascapular
artery arose from the first part of the axillary
artery: it then ran upwards for a short
distance before passing posterior to the
clavicle and brachial plexus to approach the
suprascapular notch. The suprascapular artery
and nerve were observed to enter the
supraspinatus fossa through the
suprascapular notch under the transverse
scapular ligament. Chen and Adds (2011)
reported the case of a 94 year old female with
an accessory suprascapular artery arising from
the third part of the subclavian artery at the
outer border of scalenus anterior, where it
ran inferior to the inferior trunk of the
brachial plexus and deep to the transverse
scapular ligament with the suprascapular
nerve, while the classic suprascapular artery
took its ordinary course to pass over the
transverse scapular ligament. The
suprascapular and accessory suprascapular
arteries anastomosed in the supraspinatus
fossa undercover of supraspinatus. According
to Drake et al (2005) and Moore et al (2010)
the suprascapular artery may originate from

AXIS Vol. 4, Issue 2 (Spring 2013) 3
the 3rd part of the subclavian artery. Atsas et
al (2011) also reported a case of a 68 year old
male in which on the left side the
suprascapular artery originated from the
internal mammary (thoracic) artery just after
it arose from the subclavian artery. It passed
backwards posterior to the medial third of the
clavicle and then accompanied the
suprascapular nerve where it bridged the
transverse scapular ligament, while the
suprascapular nerve passed beneath.
Case report:
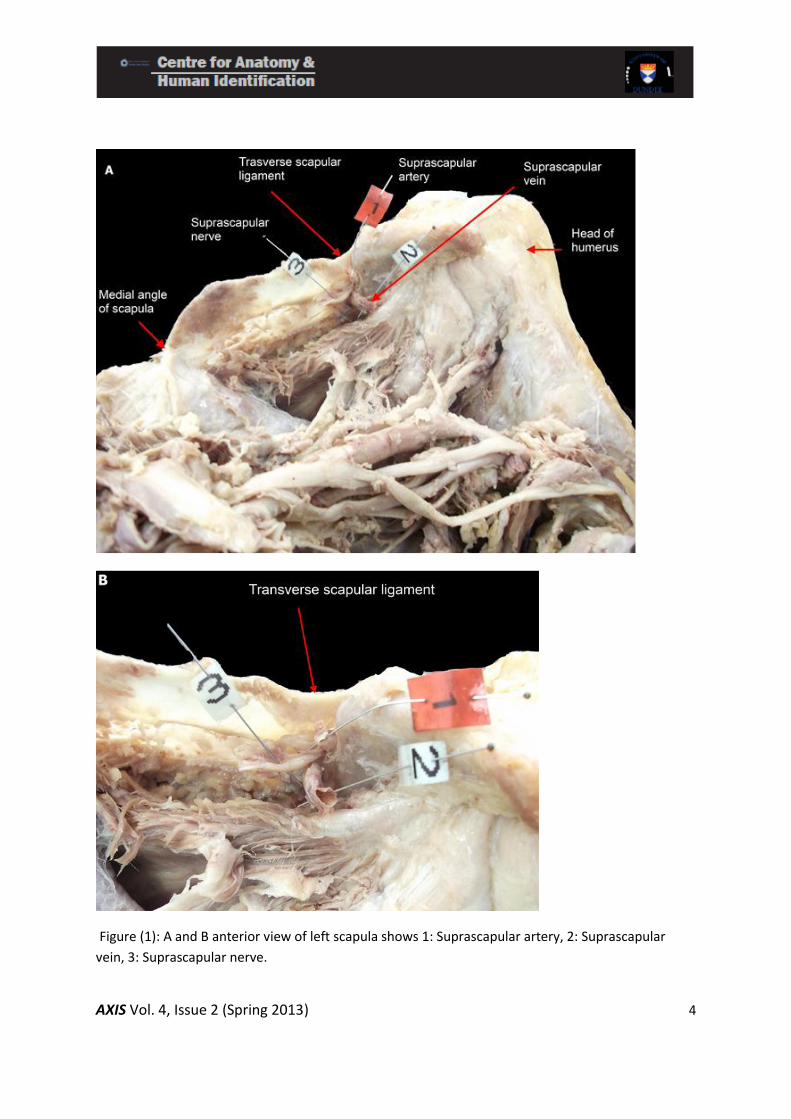
During routine dissection of a 62 year old
female the left suprascapular artery was
found to arise from the thyrocervical trunk. It
emerged between sternocleidomastoid
anteriorly and scalenus anterior posteriorly
where it ran lateral and posterior to pass
anterior to the third part of the subclavian
artery and brachial plexus, and posterior to
the clavicle and subclavius. Throughout its
course it was accompanied by the
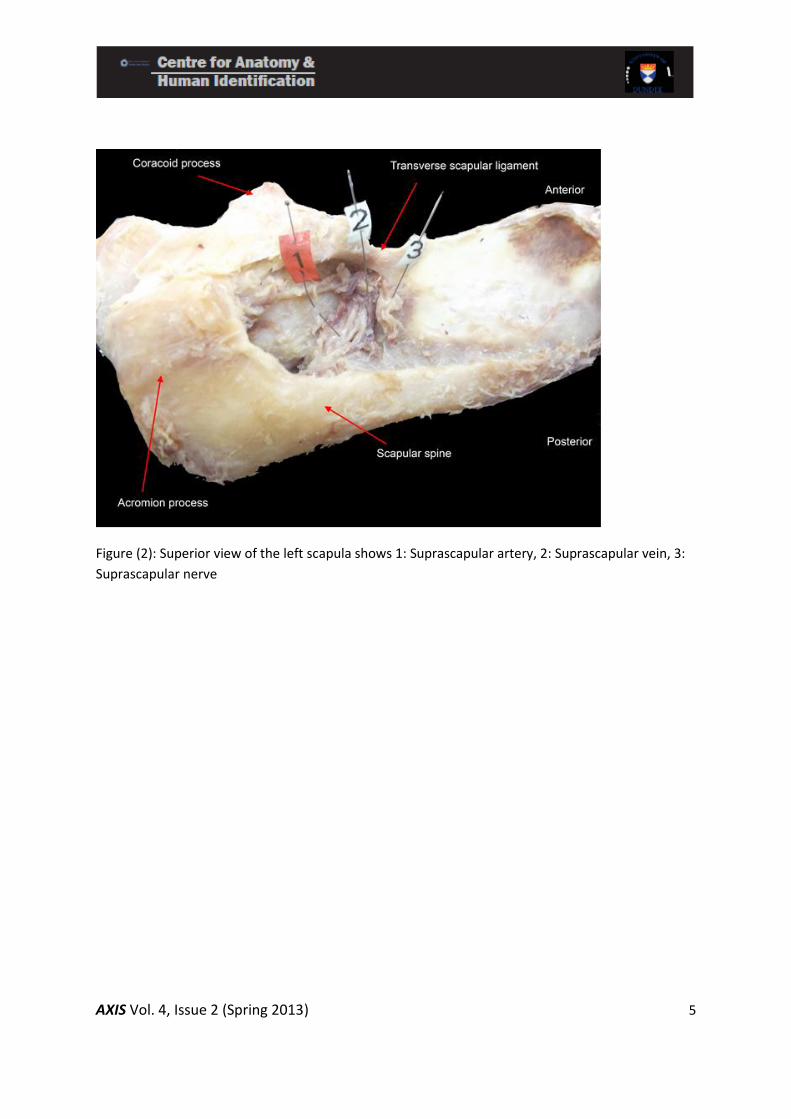
suprascapular nerve. Once they approached
the superior border of the scapula they both
passed below the transverse scapular
ligament to the supraspinous fossa deep to
supraspinatus (Figure 1, 2). The suprascapular
artery then continued through the
spinoglenoid notch to the infraglenoid fossa
deep to infraspinatus, where it contributed to
the anastomosis around the scapula. During it
course, the suprascapular artery gave
muscular branches to sternocleidomastoid
supraspinatus, infraspinatus, trapezius and a
small branch before passing through the
suprascapular notch to the subscapular fossa
to ramify in subscapularis. In addition, 2 to 3
articular branches were given to the shoulder
joint within the supraspinatus fossa. Hence
knowledge of this suprascapular artery
variation is important in cases of either open
or arthroscopic suprascapular nerve
decompression. An awareness of this variant
may also help in management of
glenohumeral region disease due to
underlying circulation problems.
AXIS Vol. 4, Issue 2 (Spring 2013) 4
Figure (1): A and B anterior view of left scapula shows 1: Suprascapular artery, 2: Suprascapular
vein, 3: Suprascapular nerve.
AXIS Vol. 4, Issue 2 (Spring 2013) 5
Figure (2): Superior view of the left scapula shows 1: Suprascapular artery, 2: Suprascapular vein, 3:
Suprascapular nerve
AXIS Vol. 4, Issue 2 (Spring 2013) 6
References
Abrahams P, Craven J, Lumley J (2011)
Illustrated Clinical Anatomy London, Arnold.
Adibatti M (2010) Variation in the origin of
suprascapular artery, International Journal of
Anatomical Variations 3: 178–179
Atsas S, Fox JN, Lambert HW (2011) The rare
origin of the suprascapular artery arising off
the internal thoracic artery in the presence of
the thyrocervical trunk: clinical and surgical
implications. International Journal of
Anatomical Variations 4: 182–184
Chen D and Adds P (2011) Accessory
suprascapular artery. Clinical Anatomy, 24,
498-500.
Drake RL, Vogl AW, Mitchell AWM (2005)
Gray`s Anatomy for Students, Philadelphia,
Churchill Livingstone Elsevier.
Ellis H (2006) Clinical Anatomy: a revision and
applied anatomy for clinical students,Oxford,
Blackwell Publishing.
Faiz O, Moffat D (2006) Anatomy at A Glance
Oxford, Blackwell Publishing.
Gray H (1913) Descriptive and Applied
Anatomy, Lea and Febiger Philadelphia and
New York.
Hall-Craggs ECB (1990) Anatomy as a Basis for
Clinical Medicine, London, Williams &Wilkins.
Lumley JSP, Craven JL, Aitken JT (1995)
Essential Anatomy and some clinical
applications, Edinburgh, Churchill Livingstone.
Mahato KN (2010) Bilateral anomalous
suprascapular arteries. European Journal of
Anatomy, 14 (1): 31-34.
Mishra, S, Ajmani ML (2003) Anomalous
Origin of Suprascapular Artery, Journal of the
Anatomical Society of India 52(2) 180-182
Monkhouse S (2001) Clinical anatomy: a core
text with self-assessment,Edinburgh: Churchill
Livingstone.
Moore KL, Dalley AF, Agur AMR (2010)
Clinically Oriented Anatomy, Philadelphia,
Pa.;London Lippincott William and Wilkins.
Palastanga N, Field D, Soames R (2006)
Anatomy and Human Movement:
structureand function, Edinburgh,
Butterworth Heinemann Elsevier.

AXIS Vol. 4, Issue 2 (Spring 2013) 7
Rogers AW (1992) Textbook of Anatomy,
Edinburgh, Churchill Livingstone.
Snell R S (1995) Clinical Anatomy for Medical
Students, 5th edition, Boston Mass. ,London:
Little, Brown.
Sinnatamby CS (2006) Last’s Anatomy:
regional and applied, Edinburgh, New York,
Elsevier/ Churchill Livingstone.
Smith JW, Murphy TR, Blair JSG, Lowe KG
(1983) Regional Anatomy Illustrated,
Edinburgh Churchill Livingstone.
Yang H J, Gil, YC, Jin JD, Ahn SV, Lee HY (2012)
Topographical anatomy of the suprascapular
nerve and vessels at the suprascapular notch.
Clinical Anatomy, 25, 359-365.





























