Embed Size (px)
Citation preview

• Dengue• Leptospirosis• Malaria• Murine typhus
Air-/D
roplet-B
orneD
iseases
Vector-Borne/
ZoonoticD
iseases
Food-/Water-
Borne
Diseases
Blood-B
orneD
iseasesE
nvironment-
Related
Diseases
Childhood
Imm
unisation

Communicable Diseases Surveillance in Singapore 2003
IIVECTOR-BORNE DISEASES
Vector-borne and zoonotic diseases are diseases transmitted to humans by insects or animals. Vectors may transmit infectious diseases to humans by the blood-feeding of arthropods such as mosquitoes and ticks or through contaminated
urine, tissues or bites of infected animals such as rats or dogs. The causative organism may be viral, bacterial, fungal, protozoan or parasitic and the transmission could be direct or via food and water.
Dengue fever is an acute febrile viral disease characterised by sudden onset of fever for 3-5 days, intense headache, myalgia, arthralgia, retro-orbital pain, anorexia, gastrointestinal disturbances and rash. Early generalised erythema may occur in some cases. The infectious agents are flaviviruses comprising four serotypes (dengue-1, 2, 3 and 4) and are
DENGUE FEVER/DENGUE HAEMORRHAGIC FEVER (DF/DHF)transmitted by the Aedes mosquito.
In 2003, a total of 4788 cases of DF/DHF were reported compared to 3945 cases in 2002. The majority of the cases (78%) received inpatient treatment. The incidence was highest in June, during e-week 23. (Figure 2.1)
0
50
100
150
200
250
300
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53Week
No.
of c
ases
2002 2003
Figure 2.1E-weekly distribution of DF/DHF cases, 2002 - 2003
23

The incidence rate among local residents was highest in the 15-24 years age group. (Table 2.1) Among the three major ethnic groups, Chinese residents had the highest incidence rate, followed
by Indians and Malays. Foreigners comprised 22.5% of the indigenous cases (Table 2.2), with majority employed as labourers or related workers in the construction and manufacturing industry.
Table 2.2Ethnic-gender distribution and ethnic-specific incidence rates of indigenous# DF/DHF cases, 2003
Male
1647
152
102
45
692
2638
Singapore Resident
Chinese
Malay
Indian
Others
Foreigner
Total
Total (%)
3011 (66.3)
253 (5.6)
179 (3.9)
78 (1.7)
1021 (22.5)
4542 (100.0)
Female
1364
101
77
33
329
1904
Incidence rateper 100,000 population*
# Cases acquired locally among Singaporeans, permanent and temporary residents.* Rates are based on 2003 estimated mid-year population.
(Source: Singapore Department of Statistics)
Table 2.1Age-gender distribution and age-specific incidence rates of indigenous# DF/DHF cases, 2003
Male
27
232
481
714
599
332
253
2638
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Total
Total (%)
48 (1.1)
417 (9.2)
858 (18.9)
1102 (24.3)
974 (21.4)
619 (13.6)
524 (11.5)
4542 (100.0)
Female
21
185
377
388
375
287
271
1904
Incidence rateper 100,000 population*
# Cases acquired locally among Singaporeans, permanent and temporary residents.* Rates are based on 2003 estimated mid-year population.
(Source: Singapore Department of Statistics)
22.3
77.7
138.4
128.1
126.5
106.9
86.7
108.5
114.9
53.4
63.1
132.7
136.5
108.5
24

Communicable Diseases Surveillance in Singapore 2003
Table 2.3Economic/occupational profile of indigenous DF/DHF cases, 2003
Economic status/occupation
Economically active
Working
Senior officials & managers
Professionals
Associate professionals & technicians
Clerical workers
Service & sales workers
Production craftsmen & related workers
Plant & machine operators & assemblers
Cleaners, labourers & related workers
Workers not classifiable by occupation
Unemployed
Economically inactive
Homemakers
Students
Others
Total
%
7.3
10.0
4.3
4.2
5.6
0.7
0.6
13.2
8.3
7.7
14.0
17.9
6.2
100.0
No.
332
454
197
189
255
32
29
599
376
350
637
811
281
4542
The economic/occupational profile of indigenous DF/DHF cases is given in Table 2.3. Students accounted for 17.9%, 14.0% were homemakers
and 13.2% were cleaners, labourers and related workers.
25

Year
Southeast Asia Indonesia Malaysia Thailand Philippines Vietnam Cambodia Brunei Myanmar Laos East Timor
South Asia India Bangladesh Sri Lanka Pakistan Nepal
Other Regions
Total
1999
11665
91220300
74600
2
217
2000
17164
53025000
69300
3
271
2001
1427732
5082801
198310
2
308
2002
155139
436040200
143910
9
385
2003
93100
182280100
141311
2
246
There were 246 (5.1%) imported cases, defined as cases with a history of travel to endemic areas seven days prior to the onset of illness.
The majority of these cases (92%) were from neighbouring countries: 93 from Indonesia and 100 from Malaysia. (Table 2.4)
Table 2.4Imported DF/DHF cases, 1999-2003
Residents in Housing and Development Board (HDB) flats, compound houses and condominiums accounted for 55.0%, 31.9%, and 12.9%, respectively, of the cases. However, the incidence rate for residents of compound houses was ten times higher than that of HDB dwellers.
(Table 2.5)
Most of the cases were concentrated in the south-eastern (39.1%) and central (33%) areas of Singapore. (Figure 2.2)
Table 2.5Incidence rates of reported indigenous DF/DHF cases
(Singaporeans and Permanent Residents) by housing type, 2003
%
31.9
55.0
12.9
0.2
100.0
Incidence rateper 100,000 population Cases
1124
1937
453
7
3521
Housing Types
Compound houses (including shophouses)
HDB flats
Condominiums
Bangsals, containers/workers’ quartersand others
Total
633.7
63.9
220.4
-
102.9
26

Communicable Diseases Surveillance in Singapore 2003
Figure 2.2Geographical distribution of DF/DHF clusters having 10 or more reported cases, 2003
A total of 180 clusters involving 1405 epidemiologically linked cases were identified. The median number of cases in each cluster
was 4.5 (range 2 to 59) and the median duration of transmission was 12 days (range 1 to 79). (Table 2.6)
No. ofClusters*
40
74
134
33
75
118
143
198
239
54
9
93
73
180
No. of cases in cluster area
(% total cases)
270 (16.5)
414 (20.1)
733 (26.7)
183 (23.0)
424 (39.1)
679 (38.7)
1088 (37.8)
1124 (27.8)
1197 (23.4)
230 (20.2)
40 (10.0)
531 (25.7)
725 (20.4)
1405 (31.0)
Median no. of cases
per cluster
4.5
3.5
3.0
3.0
3.0
3.0
3.0
3.0
2.0
3.0
4.0
3.0
7.0
4.5
Median duration of transmission
(days)
10.0
6.0
5.0
8.0
7.0
7.0
6.0
5.0
7.0
11.0
15.0
8.0
20.0
12.0
Year
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
No. ofindigenous
cases
1640
2062
2741
794
1084
1756
2877
4039
5105
1138
402
2064
3560
4542
No. of clusters with 10 cases
(% total clusters)
11 (27.5)
9 (12.2)
13 (9.7)
4 (12.1)
8 (10.7)
16 (13.6)
27 (18.9)
24 (12.1)
23 (9.6)
6 (11.1)
1 (11.1)
15 (16.1)
30 (41.1)
38 (21.1)
Table 2.6Dengue clusters identified during the period 1990-2003
*A cluster is defined as two or more cases epidemiologically linked by place (within 250 metres) and time (within three weeks or approximately two incubation periods)
2 or more epidemiologically linked cases in a locality
27

Of the 180 clusters identified, there were 38 clusters (21.1%) having 10 cases or more. They were in the areas listed below:
S/No
123456789
1011121314151617181920212223242526272829303132333435363738
Location
Bishan St 24/Bishan St 22
Jalan Lembah Thomson/Soo Chow WalkAng Mo Kio Ave 2/Ang Mo Kio St 11Tampines Ave 4/Tampines Ave 1Bright Hill Road/Fulton RoadSerangoon Garden Way/Medway DriveSims Drive/Aljunied RoadMinbu Road/Mandalay RoadUbi Road 1/Ubi Ave 2Bedok North Ave 4Jalan Tua Kong/Jalan Ulu SiglapLorong 1 Toa Payoh/Toa Payoh NorthLorong 4 Geylang/Mountbatten RoadKallang Bahru MUP 14Whampoa Drive/Kim Keat RoadPark Road/Eu Tong Sen StChancery Hill Road/Dyson RoadAng Mo Kio Ave 4/Ang Mo Kio St 13Clover Crescent/Binjang Rise areaPoh Huat Road/Park Villas TerraceFidelio Street/Siglap Road areaBoon Teck/Jalan Ampas areaHougang Ave 7Bayshore Road/Upper East Coast RoadKew Ave/Kew DriveDefu Lane 6/Defu Lane 5Tanjong Katong Road/Amber RoadChai Chee St/Bedok North RoadJalan Seaview/Meyer RoadSerangoon Ave 3/Serangoon Ave 2Melrose Drive/Jalan Girang areaChuan Hoe Ave/Limbok TerracePoh Huat Road West/Yio Chu Kang RoadProposed Armanda CondominiumSerangoon North Ave 1Jalan Ikan Merah/Jalan SembilangGlasgow Road/Jansen RoadLichfield Road/Raglan Grove area
No. of cases
1214161559102131122029171214412228152513101048102211251219501323111242101225
Month
JanFeb
Jan-FebJan-MarFeb-MarJan-MarFeb-Mar
MarMar-Apr
AprApr-JunApr-MayApr-MayApr-MayMay-JunApr-MayMay-JunMay-JunMay-JunMay-JunMay-JunMay-Jun
Jun-JulJun-Jul
Jun-SepAug
Aug-SepAug
Aug-SepSep-OctSep-OctSep-OctSep-Oct
OctOct-DecNov-Dec
DecDec-Jan
The median number of cases in these 38 clusters was 15.5 (range 10 to 59) and the median duration of transmission was 32 days (range 13 to 79).
28

Communicable Diseases Surveillance in Singapore 2003
There were six deaths from dengue, of which five were classified as local and one as imported.
The first case was a 41-year-old Chinese male security guard from Clementi. He had no history of travel prior to his onset of illness; however his job required him to travel around Singapore. He was admitted to Alexandra Hospital with high fever, headache, malaise, abdominal discomfort, vomiting and diarrhoea for five days duration. Dengue IgM antibody tested positive on admission and he developed haemorrhagic features over the following two days. His condition deteriorated over the following two weeks and he died on 3 January 2003 from Dengue Shock Syndrome (DSS) with multi-organ failure.
The second case was a 70-year-old Malay male retiree with a travel history of a trip to Johor Bahru four days prior to the onset of symptoms. He developed fever on 9 January and was treated by a general practitioner and prescribed antibiotics. The fever persisted and on 13 January, he was admitted to Singapore General Hospital. Dengue IgM antibody tested positive. Following admission, the platelet count dropped from 60,000/mm3 to 14,000/mm3 and he developed gastrointestinal bleeding. His condition deteriorated rapidly over two days and he died on 17 January 2003 from DSS and bleeding from GI tract.
The third case was a 31-year-old Indian labourer residing at a work-site in an industrial area. He had no history of travel prior to his onset of illness. He was admitted to Changi General Hospital on 2 February 2003 and Dengue IgM antibody tested positive. He died on 6 February 2003 from DHF.
The fourth case was a 71-year-old Chinese retiree
DHF Deaths residing in Serangoon. He had previous history of stroke and hypertension. He developed high fever and myalgia and sought treatment from a general practitioner. He was subsequently admitted to East Shore Hospital on 5 April 2003 in an unconscious state. On admission he was found to have a low platelet count of 43,000/mm3 and a CT scan indicated a cerebral haemorrhage. His condition did not improve despite platelet and plasma transfusion and died on 6 April 2003. The cause of death was cerebral haemorrhage associated with DHF.
The fifth case was a 59-year-old Chinese housewife residing in Hougang area. She developed high fever on 26 June 2003 and presented to Tan Tock Seng Hospital on 29 June 2003 with giddiness and a history of fall at home. At admission she was managed for septic shock in the Intensive Care Unit (ICU). Laboratory findings revealed Dengue PCR positive and marked thrombocytopenia. Her condition deteriorated despite ventilation support and fresh frozen plasma transfusion. She died of DSS and multi-organ failure on 4 July 2003.
The sixth case was a 77-year-old Chinese housewife residing in Joo Chiat area. She had no history of travel prior to the onset of illness. She developed fever, myalgia and rash on 28 August 2003, and sought treatment from a general practitioner. She was subsequently referred to Gleneagles Hospital and was admitted on 30 August 2003. The Dengue PCR tested positive on 1 September 2003. The patient died on 3 September 2003 due to DSS with multi-organ failure, sepsis with disseminated intravascular coagulation (DIVC), fulminant hepatitis and severe acidosis.
29

All reported cases of dengue fever were confirmed by one or more laboratory tests; viz. anti-dengue IgM antibody, enzyme linked immunosorbent assay (ELISA), and polymerase chain reactions (PCR).
Dengue virus serotype identification was performed on a total of 525 blood samples by
Laboratory Surveillancethe Department of Pathology Singapore General Hospital and Environmental Health Institute at the National Environment Agency.
The predominant strain in Singapore in 2003 was DEN-2 serotype. All four serotypes were isolated. 8 DEN-1, 58 DEN-2, 4 DEN-3 and 5 DEN-4. (Table 2.7)
DEN-1
4(2.6)
1(0.4)
8(2.6)
20(7.8)
10(3.9)
18(7.1)
12(4.5)
11(3.2)
4(1.2)
1(0.3)
16(4.8)
8(1.5)
Year
1992 (May - Dec)
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Total no. of samples
tested
154
257
309
257
255
254
266
348
327
354 [119]
331[99]
525
DEN-2
5(3.2)
14(5.4)
16(5.2)
8(3.1)
5(2.0)
15(5.9)
19(7.1)
8(2.3)
4(1.2)
12(3.4)
28(8.5)
70(13.3)
DEN-3
21(13.6)
4(1.6)
20(6.5)
17(6.6)
2(0.8)
0
3(1.1)
2(0.6)
1(0.3)
0
2(0.6)
4(0.8)
DEN-4
0
0
0
2(0.8)
1(0.4)
0
0
0
2(0.6)
2(0.6)
6(1.8)
5(1.0)
Untyped
0
2(0.8)
1(0.3)
0
0
0
0
0
0
0
0
0
No. of positive isolates (%)
[ ] denotes specimens from Dengue Project (general physicians and construction sites)
Table 2.7Surveillance of dengue serotypes, 1992-2003
30

Communicable Diseases Surveillance in Singapore 2003
Serangoon Ave 3/Serangoon Ave 2 areasOn 16 September 2003, the Ministry of Health was notified of six cases of dengue fever involving students of Nanyang Junior College and residents of Serangoon Avenue 2 and 3. Within the next five days, four more cases from the same area were confirmed to be dengue fever. As soon as the cluster of cases was identified, vector control operations were carried out.
A total of 50 serologically confirmed cases were identified in the outbreak. Illness onsets were between 7 September and 5 October 2003. Seventy per cent of the cases were hospitalised.
The cases comprised of 18 students, 14 working adults, 8 construction workers, 3 retirees, 3
Outbreaks of Dengue
Table 2.8Age-gender distribution of reported DF/DHF cases at Serangoon Ave 3/Serangoon Ave 2
September–October 2003
Male
0
5
4
7
7
3
3
29
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Total
Total (%)
0 (0)
7 (14)
11 (22)
14 (28)
9 (18)
6 (12)
3 (6)
50 (100)
Female
0
2
7
7
2
3
0
21
Figure 2.3 Geographical distribution of 50 DF/DHF cases at Serangoon Ave 2/3 area, September-October 2003
One Case
Culex Breeding
Aedes albopictus Breeding
Aedes aegypti Breeding
Aedes Breeding
307
308
309
310
313 312
314 315
311
316
317318
302
303
305
306
304301
319
239
238
243
244
245
240
232 234
236
237
242
241
246
322
321 325
324
327
328
329
326
323
332
333
331
330
334
335
267266
265264
263
261
262
254A254
253
Nanyang Junior College
Yangzheng Pri Sch
ZhonghuaSec Sch
Chuan Park
Lor C
huan
Serangoon A
ve 2
TheSunnydale
Serangoon Ave 3
AmandaGarden
unemployed, 2 maids and 2 housewives. The majority of the cases were in the 25–34 years age group with a male to female ratio of 1.4:1. (Table 2.8)
All cases were clustered within a 250-metre radius from the initial focus of transmission. (Figure 2.3)
Aedes mosquito breeding habitats were identified in 63 (1.7%) of 3682 premises inspected. Abundant breeding habitats were found in ornamental containers (42.0%), domestic containers (14.8%) and bamboo pole holders (14.8%). Aedes aegypti and Aedes albopictus accounted for 51.4% and 47.9% of the breeding detected respectively.
31

Bright Hill Road/Fulton Road areasOn 11 February 2003, a case of dengue fever involving a resident of Fulton Ave was notified. Two days later, another 16 cases from a construction site in the same area were reported. The NEA was immediately alerted when the cluster of cases in the area was identified on 13 February 2003. Vector control measures were implemented to prevent further disease transmission.
Table 2.9Age-gender distribution of reported DF/DHF cases at Bright Hill Road/Fulton Road areas
February-March 2003
Male
0
1
2
22
21
3
1
50
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Total
Total (%)
0 (0.0)
2 (3.4)
6 (10.2)
24 (40.6)
22 (37.3)
4 (6.8)
1 (1.7)
59 (100.0)
Female
0
1
4
2
1
1
0
9
All cases were clustered within a 250-metre radius from the initial focus of transmission. (Figure 2.4)
A total of 463 premises were checked. Eight were found to be breeding mosquitoes. In addition,
A total of 59 serologically confirmed cases were reported with onsets of illness between 1 February and 10 March 2003. Seventy-eight per cent of these cases received inpatient treatment.
The cases comprised of 43 construction workers, 6 working adults, 6 students, 1 unemployed, 1 housewife, 1 domestic helper and 1 retiree. The majority of the cases were in the 25–34 years age group and the overall male to female ratio was 5.6:1. (Table 2.9)
Figure 2.4 Geographical distribution of 59 DF/DHF cases at Bright Hill Road/Fulton Road,
February-March 2003
One Case
Aedes albopictus Breeding
Aedes aegypti Breeding
Bishan ParkSec Sch
Ai Tong Pri Sch
Sin
Min
g A
ve
Bishan Park
Sin
Min
g D
r
Kong Meng SanTempleProposed Extension
Bright HillEvergreen Home
Fulto
n R
d
Fulton Rd
Fulto
n Av
e
Brig
ht H
ill D
r
VicomVehicleInspectionCentre
402403
401
406
407408
405
404
there was one breeding habitat found in the public area. The main breeding habitats were plastic pails (55.6%) and flowerpot plates (16.7%). Aedes albopictus and Aedes aegypti accounted for 55.6% and 44.4%, respectively.
32

Communicable Diseases Surveillance in Singapore 2003
Leptospirosis is a zoonotic bacterial disease of variable clinical manifestations. The common presenting features are fever, headache, chills, severe myalgia and conjunctival suffusion. The etiologic agent is a spiral organism, Leptospires, a member of the order Spirochaetales found mainly in infected wild and domestic animals. The mode of transmission is through direct contact of the skin (especially if broken) or mucous membranes with the urine or tissues of infected animals. Soil or vegetation contaminated by
LEPTOSPIROSISinfected animals may also result in infection. Occasionally leptospirosis has occured following the ingestion of food contaminated by the urine of infected rats.
In 2003, there were 29 reported cases of Leptospirosis. Of these 12 were classified as imported cases. Leptospirosis is a disease of young males (male to female ratio 13.5:1). They tend to be foreigners in the 25-34 year age group. (Tables 2.10 and 2.11)
Table 2.10Age-gender distribution and age-specific incidence rates of reported leptospirosis cases, 2003
Male
0
0
5
10
6
2
3
1
27
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Unknown
Total
Total (%)
0 (0.0)
0 (0.0)
5 (17.2)
10 (34.5)
6 (20.7)
2 (6.9)
5 (17.2)
1 (3.5)
29 (100.0)
Female
0
0
0
0
0
0
2
0
2
Incidence rateper 100,000 population*
* Rates are based on 2003 estimated mid-year population.(Source: Singapore Department of Statistics)
Table 2.11Ethnic-gender distribution and ethnic-specific incidence rates of reported leptospirosis cases, 2003
Male
7
2
2
0
16
27
Singapore Resident
Chinese
Malay
Indian
Others
Foreigner
Total
Total (%)
8 (27.6)
2 (6.9)
2 (6.9)
0 (0.0)
17 (58.6)
29 (100.0)
Female
1
0
0
0
1
2
Incidence rateper 100,000 population*
* Rates are based on 2003 estimated mid-year population.(Source: Singapore Department of Statistics)
0.3
0.4
0.7
0.0
2.3
0.7
0.0
0.0
0.8
1.2
0.8
0.4
0.8
-
0.7
33

Malaria is a parasitic disease characterised by fever and chills. Serious malarial infections may present with cough, diarrhoea, respiratory distress and headache. The infectious agent is a protozoan parasite, Plasmodium, and there are four different species namely, P. vivax, P. malariae, P. faciparum and P. ovale. The mode of transmission is via a bite
MALARIAfrom an infective female Anopheles mosquito.
In 2003, a total of 118 cases were reported compared with 175 cases in 2002. Of these, 81 were local residents, while the remaining were either tourists (13) or foreigners seeking medical treatment in Singapore (24).
Table 2.12Age-gender distribution and age-specific incidence rates of reported malaria cases^, 2003
Male
0
1
14
23
12
8
9
67
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Total
Total (%)
0 (0.0)
2 (2.5)
18 (22.2)
26 (32.1)
13 (16.0)
11 (13.6)
11 (13.6)
81 (100.0)
Female
0
1
4
3
1
3
2
14
^excluding 24 foreigners seeking medical treatment in Singapore and 13 tourists *Rates are based on 2003 estimated mid-year population.
(Source: Singapore Department of Statistics)
Figure 2.5 E-weekly distribution of reported malaria cases, 2002 - 2003
0
3
6
9
12
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Week
No.
of c
ases
2002 2003
Incidence rateper 100,000 population*
0.0
0.4
2.9
3.0
1.7
1.9
1.8
1.9
Among the 81 reported cases of malaria in local residents, the age-specific incidence rate was highest in the 25-34 years age group and the male to female ratio was 4.8:1. (Table 2.12)
The ethnic-specific incidence rate for Malay residents was about 4 times that of Chinese and 1.3 times that of Indians. (Table 2.13)
34

Communicable Diseases Surveillance in Singapore 2003
Table 2.13Ethnic-gender distribution and ethnic-specific incidence rates of reported malaria cases^, 2003
^excluding 24 foreigners seeking medical treatment in Singapore and 13 tourists*Rates are based on 2003 estimated mid-year population.
(Source: Singapore Department of Statistics)
Male
19
10
6
0
32
67
Singapore Resident
Chinese
Malay
Indian
Others
Foreigner
Total
Total (%)
21 (25.9)
15 (18.5)
7 (8.6)
0 (0.0)
38 (47.0)
81 (100.0)
Female
2
5
1
0
6
14
Incidence rateper 100,000 population*
Malaria parasite speciesOf the total 118 reported cases, 113 (95.8%) were acquired overseas, 4 (3.4%) were introduced, and 1 (0.8%) was cryptic. No indigenous cases were reported.
The distribution of the cases by parasite species was P. vivax (64.4%), P. falciparum (33.9%), and mixed infection (1.7%). (Table 2.14)
P.f
40
0
0
0
0
40
Classifications
Imported*
Introduced
Indigenous
Cryptic
Induced
Total
P.v.
71
4
0
1
0
76
Total (%)
113 (95.8)
4 (3.4)
0 (0.0)
1 (0.8)
0 (0.0)
118 (100.0)
Mixed(P.v. & P.f.)
2
0
0
0
0
2
Mixed(P.v. & P.m.)
0
0
0
0
0
0
P.m.
0
0
0
0
0
0
Parasites species
P.v. - Plasmodium vivax P.m. - Plasmodium malariae P.f. - Plasmodium falciparum *Including relapsed and induced cases which were imported.
Table 2.14Classification of reported malaria cases by parasite species, 2003
0.8
3.2
2.5
0.0
5.1
1.9
35

The majority of the malaria cases acquired overseas were infected in Indonesia (47.8%) and
Table 2.15Malaria cases^ by country of origin and by parasite species, 2003
P.f
24
0
2
0
0
6
0
1
0
1
5
1
40
P.v.
29
4
1
1
1
32
1
0
1
0
1
0
71
Mixed(P.v. & P.f.)
1
0
0
0
0
0
0
0
0
0
1
0
2
Mixed(P.v. & P.m.)
0
0
0
0
0
0
0
0
0
0
0
0
0
P.m.
0
0
0
0
0
0
0
0
0
0
0
0
0
Countries
Southeast Asia
Indonesia
Malaysia
Myanmar
Thailand
Vietnam
South Asia
India
Nepal
Pakistan
Other Asian countries
Papua New Guinea
Taiwan
Africa
Central African Republic
South Africa
Total
Total (%)
54 (47.8)
4 (3.5)
3 (2.6)
1 (0.9)
1 (0.9)
38 (33.6)
1 (0.9)
1 (0.9)
1 (0.9)
1(0.9)
7 (6.2)
1 (0.9)
113 (100.0)
P.v. - Plasmodium vivax P.m. - Plasmodium malariae P.f. - Plasmodium falciparum
India (33.6%). (Table 2.15) P. falciparum accounted for 44.4% of the infections acquired in Indonesia.
Overseas-acquired malaria
^ Excluding 4 introduced cases and 1 cryptic case.
36
Communicable Diseases Surveillance in Singapore 2003
P.f
33
7
0
0
0
0
0
0
0
0
0
0
0
0
0
0
40
P.v.
38
10
3
4
1
0
3
0
2
0
1
2
3
1
1
2
71
Mixed(P.v. & P.f.)
0
1
1
0
0
0
0
0
0
0
0
0
0
0
0
0
2
Mixed(P.v. & P.m.)
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
P.m.
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Interval inweeks
< 2
2 - 3
4 - 5
6 - 7
8 - 9
10 - 11
12 - 13
14 - 15
16 - 17
18 - 19
20 - 23
24 - 27
28 - 31
32 - 35
36 - 39
40+
Total
Total (%)
71 (62.8)
18 (15.9)
4 (3.5)
4 (3.5)
1 (0.9)
0 (0.0)
3 (2.6)
0 (0.0)
2 (1.8)
0 (0.0)
1 (0.9)
2 (1.8)
3 (2.7)
1 (0.9)
1 (0.9)
2 (1.8)
113 (100.0)
P.v. - Plasmodium vivax P.m. - Plasmodium malariae P.f. - Plasmodium falciparum
Parasite species
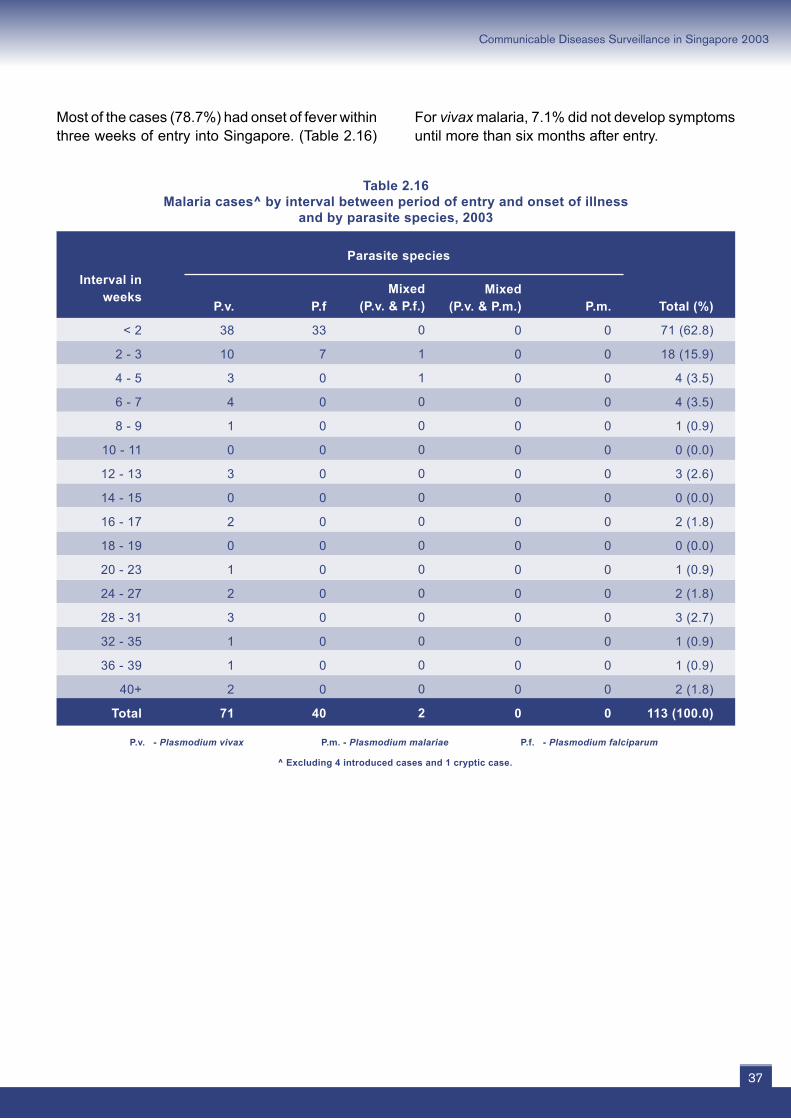
Most of the cases (78.7%) had onset of fever within three weeks of entry into Singapore. (Table 2.16)
Table 2.16Malaria cases^ by interval between period of entry and onset of illness
and by parasite species, 2003
For vivax malaria, 7.1% did not develop symptoms until more than six months after entry.
^ Excluding 4 introduced cases and 1 cryptic case.
37
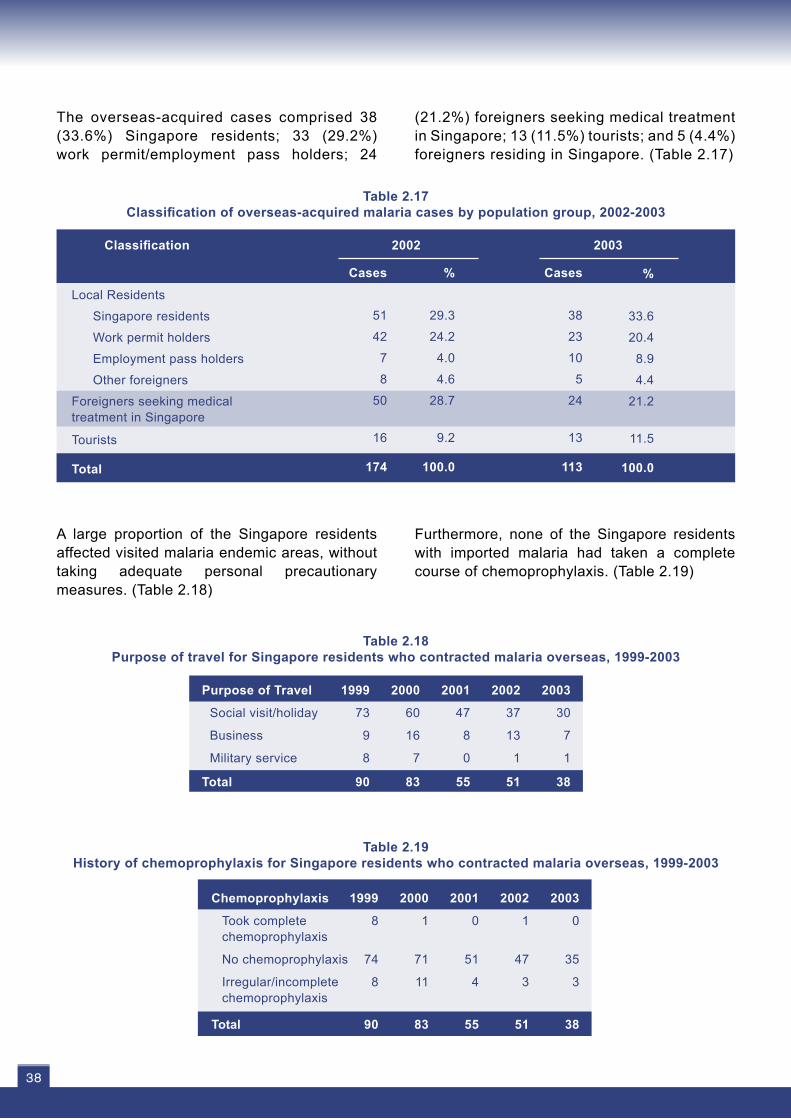
The overseas-acquired cases comprised 38 (33.6%) Singapore residents; 33 (29.2%) work permit/employment pass holders; 24
%
29.3
24.2
4.0
4.6
28.7
9.2
100.0
Cases
51
42
7
8
50
16
174
Local Residents
Singapore residents
Work permit holders
Employment pass holders
Other foreigners
Foreigners seeking medical treatment in Singapore
Tourists
Total
Classification 2002 2003
%
33.6
20.4
8.9
4.4
21.2
11.5
100.0
Cases
38
23
10
5
24
13
113
(21.2%) foreigners seeking medical treatment in Singapore; 13 (11.5%) tourists; and 5 (4.4%) foreigners residing in Singapore. (Table 2.17)
Table 2.17Classification of overseas-acquired malaria cases by population group, 2002-2003
A large proportion of the Singapore residents affected visited malaria endemic areas, without taking adequate personal precautionary measures. (Table 2.18)
Table 2.18Purpose of travel for Singapore residents who contracted malaria overseas, 1999-2003
Table 2.19History of chemoprophylaxis for Singapore residents who contracted malaria overseas, 1999-2003
1999
8
74
8
90
2000
1
71
11
83
2001
0
51
4
55
2002
1
47
3
51
2003
0
35
3
38
Chemoprophylaxis
Took complete chemoprophylaxis
No chemoprophylaxis
Irregular/incomplete chemoprophylaxis
Total
1999
73
9
8
90
2000
60
16
7
83
2001
47
8
0
55
2002
37
13
1
51
2003
30
7
1
38
Purpose of Travel
Social visit/holiday
Business
Military service
Total
Furthermore, none of the Singapore residents with imported malaria had taken a complete course of chemoprophylaxis. (Table 2.19)
38

Communicable Diseases Surveillance in Singapore 2003
Blood film examinationA total of 1955 blood films were collected during routine epidemiological investigations and examined for malaria parasites.
No. positive formalaria parasites
00
00
00
01000000000000
1
Locality
Lim Chu Kang areaPulau Ubin & Tekong area
Bedok South areaSungei Gedong areaSungei Khatib Bongus area
Yishun St 23
Tekong HQTekong Campsite 1Rivervale LinkSengkang areaWoodlands Ave 5/6Tampines St 22Mount Vernon areaMandai estate Senja RoadMandai LinkHindhede RoadBukit Batok areaMandai RoadBukit Batok East Ave 2
Total
No. of blood films examined
51496
2272
10
231
22261137182
74
624
6922222953
199
1955
Introduced/cryptic malariaThere were five introduced/cryptic cases of malaria. One cryptic case was detected in Yishun
Street 21 area and the four introduced cases were from Pulau Tekong.
Only one blood film was tested positive for malaria parasite. (Table 2.20)
Table 2.20Malaria surveillance, 2003
39
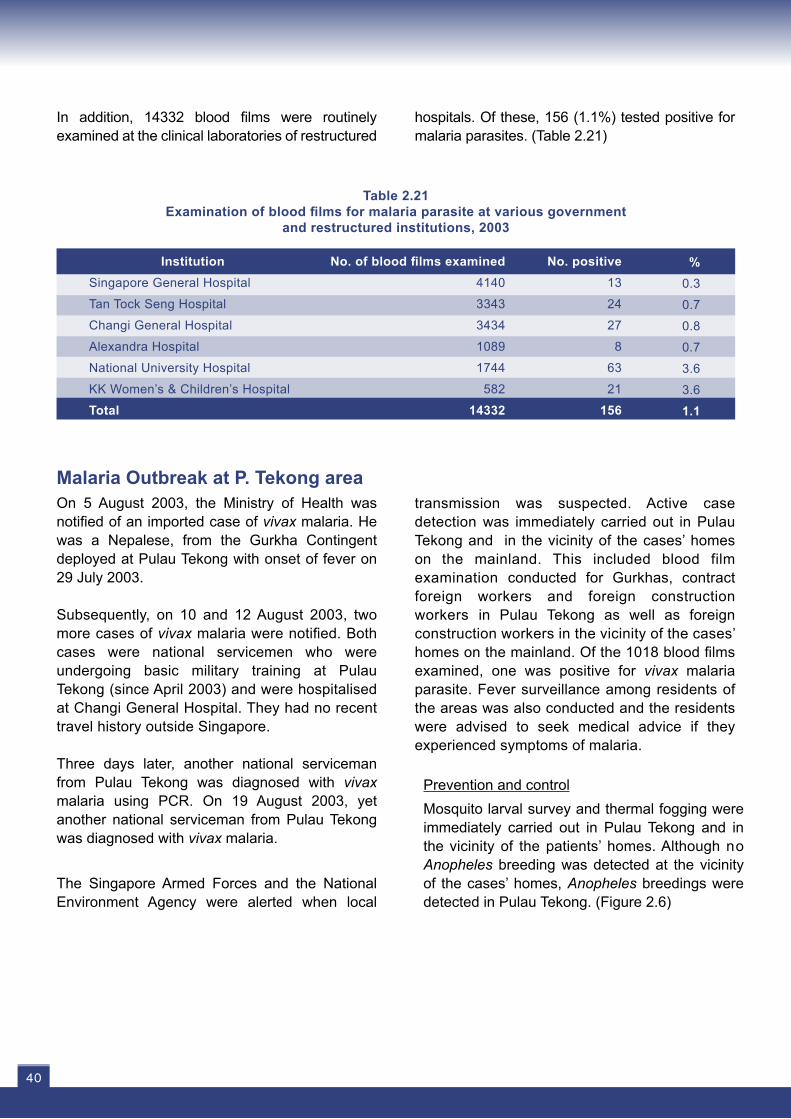
In addition, 14332 blood films were routinely examined at the clinical laboratories of restructured
Malaria Outbreak at P. Tekong area On 5 August 2003, the Ministry of Health was notified of an imported case of vivax malaria. He was a Nepalese, from the Gurkha Contingent deployed at Pulau Tekong with onset of fever on 29 July 2003.
Subsequently, on 10 and 12 August 2003, two more cases of vivax malaria were notified. Both cases were national servicemen who were undergoing basic military training at Pulau Tekong (since April 2003) and were hospitalised at Changi General Hospital. They had no recent travel history outside Singapore.
Three days later, another national serviceman from Pulau Tekong was diagnosed with vivax malaria using PCR. On 19 August 2003, yet another national serviceman from Pulau Tekong was diagnosed with vivax malaria. The Singapore Armed Forces and the National Environment Agency were alerted when local
transmission was suspected. Active case detection was immediately carried out in Pulau Tekong and in the vicinity of the cases’ homes on the mainland. This included blood film examination conducted for Gurkhas, contract foreign workers and foreign construction workers in Pulau Tekong as well as foreign construction workers in the vicinity of the cases’ homes on the mainland. Of the 1018 blood films examined, one was positive for vivax malaria parasite. Fever surveillance among residents of the areas was also conducted and the residents were advised to seek medical advice if they experienced symptoms of malaria.
Prevention and controlMosquito larval survey and thermal fogging were immediately carried out in Pulau Tekong and in the vicinity of the patients’ homes. Although no Anopheles breeding was detected at the vicinity of the cases’ homes, Anopheles breedings were detected in Pulau Tekong. (Figure 2.6)
Table 2.21Examination of blood films for malaria parasite at various government
and restructured institutions, 2003
%0.3
0.7
0.8
0.7
3.6
3.6
1.1
No. positive13
24
27
8
63
21
156
No. of blood films examined4140
3343
3434
1089
1744
582
14332
InstitutionSingapore General Hospital
Tan Tock Seng Hospital
Changi General Hospital
Alexandra Hospital
National University Hospital
KK Women’s & Children’s Hospital
Total
hospitals. Of these, 156 (1.1%) tested positive for malaria parasites. (Table 2.21)
40

Communicable Diseases Surveillance in Singapore 2003
Figure 2.6Geographical distribution of four reported local malaria cases in Pulau Tekong,
July–August 2003
Comments One possible source of infection in this outbreak could have been the index Nepalese imported relapse case. He had a history of similar illness in
December 2002 prior to arrival in Singapore and did not complete his medication during the first episode of illness.
41

MURINE TYPHUSMurine typhus is a rickettsial disease whose course resembles that of a louseborne typhus. The infectious agents are Rickettsia typhi (Rickettsia mooseri) and Rickettsia felis. Mode of transmission is by infective rat fleas that defecate ricketsiae while sucking blood. This contaminates the bite site and other fresh skin wounds. Occasionally cases occur following the inhalation of dried
infective flea faeces.
In 2003, there were 16 reported cases of Murine typhus; of these, 3 (18.8%) were Singapore residents and 13 (81.2%) were foreign workers. The incidence rate was highest in the 15-24 years age group and amongst foreigners. (Tables 2.22 and 2.23)
Table 2.22Age-gender distribution and age-specific incidence rates of reported murine typhus cases, 2003
Male
0
0
5
5
4
0
0
14
Age (Yrs)
0 – 4
5 – 14
15 – 24
25 – 34
35 – 44
45 – 54
55+
Total
Total (%)
0 (0.0)
0 (0.0)
5 (31.2)
5 (31.2)
5 (31.2)
0 (0.0)
1 (6.4)
16 (100.0)
Female
0
0
0
0
1
0
1
2
Incidence rateper 100,000 population*
* Rates are based on 2003-estimated mid-year population.(Source: Singapore Department of Statistics)
Table 2.23Ethnic-gender distribution and ethnic-specific incidence rates of reported murine typhus cases, 2003
Male
1
0
0
0
13
14
Singapore Resident
Chinese
Malay
Indian
Others
Foreigner
Total
Total (%)
1 (6.3)
1 (6.3)
1 (6.3)
0 (0.0)
13 (81.1)
16 (100.0)
Female
0
1
1
0
0
2
Incidence rateper 100,000 population*
* Rates are based on 2003-estimated mid-year population.(Source: Singapore Department of Statistics)
0.0
0.0
0.8
0.6
0.7
0.0
0.2
0.4
0.04
0.2
0.4
0.0
1.7
0.4
42





























