Embed Size (px)
Citation preview

Journal of Clinical Epidemiology 59 (2006) 1049–1056
VEINES-QOL/Sym questionnaire was a reliable and valid disease-specific quality of life measure for deep venous thrombosis
Susan R. Kahna,b,*, Donna L. Lampingc, Thierry Ducrueta, Louise Arsenaulta,Marie Jos�e Mirond, Andr�e Roussind, Sylvie Desmaraise, France Joyald, Jeannine Kassisd,
Susan Solymossb, Louis Desjardinsf, Mira Johria,d, Ian Shriera,b;for the VETO Study investigators
aCentre for Clinical Epidemiology and Community Studies, Jewish General Hospital, Montreal, Quebec, CanadabMcGill University, Montreal, Canada
cHealth Services Research Unit, London School Hygiene & Tropical Medicine, London, United KingdomdUniversit�e de Montr�eal, Montr�eal, Quebec, Canada
eCentre Hospitalier Pierre Boucher, Longueuil, Quebec, CanadafUniversit�e Laval, Qu�ebec, Quebec, Canada
Accepted 16 October 2005
Abstract
Objective: To assess the validity of VEINES-QOL/Sym, a patient-reported questionnaire to evaluate quality of life and symptoms inpatients with deep venous thrombosis (DVT).
Study Design and Setting: Psychometric study within the Venous Thrombosis Outcomes (VETO) Study, a prospective cohort study oflong-term outcomes after DVT. A total of 359 English- and French-speaking patients with acute, objectively diagnosed DVT were recruitedat seven hospitals in Quebec, Canada. The VEINES-QOL/Sym questionnaire, a 26-item patient-reported measure that generates separatesummary scores for symptoms (VEINES-Sym) and quality of life (VEINES-QOL) was evaluated for acceptability, reliability, validity, andresponsiveness in VETO Study subjects.
Results: Standard psychometric tests confirmed the acceptability (missing data, item endorsement frequencies, floor and ceiling ef-fects), reliability (internal consistency, item–total and inter-item correlations, test–retest), validity (content, construct, convergent, discrim-inant, known groups), and responsiveness to clinical change of the VEINES-QOL/Sym in patients with DVT.
Conclusion: The VEINES-QOL/Sym is a practical and scientifically sound patient-reported measure of outcomes that was developedusing gold-standard methods. VEINES-QOL/Sym is valid and reliable for use as a measure of quality of life and symptoms in patients withacute DVT and provides a rigorous tool to allow more comprehensive evaluation of outcomes in clinical trials and epidemiological studiesof patients with DVT. � 2006 Elsevier Inc. All rights reserved.
Keywords: Venous thromboembolism; Deep vein thrombosis; Quality of life; Questionnaire; Patient outcomes; Outcomes research
1. Introduction
Deep venous thrombosis is a common clinical problemthat is associated with substantial morbidity and mortality[1]. Studies of the natural history or treatment of venousthrombosis have traditionally evaluated clinical endpointssuch as recurrence of venous thromboembolism. Whilesuch endpoints are important, they are limited in their abil-ity to describe and quantify the impact of venous thrombo-sis on patient health and daily functioning. Quality of life,
* Corresponding author. Tel.: 514-340-8222 ext. 4667; fax: 514-340-
7564.
E-mail address: [email protected] (S.R. Kahn).
0895-4356/06/$ – see front matter � 2006 Elsevier Inc. All rights reserved.
doi: 10.1016/j.jclinepi.2005.10.016
by defining health in broader terms than morbidity andmortality alone, provides valuable information on burdenof illness and is an important endpoint to consider whenstudying patients with venous thrombosis [2–5].Assessment of quality of life should ideally include bothgeneric and disease-specific measures that are reliable,valid, and responsive [2,3]. Generic measures allowcomparison across populations of patients with differentconditions, whereas disease-specific measures are more re-sponsive in detecting treatment effects and changes overtime in patients who have the same disease [3,6].
Recently, as part of the Venous Insufficiency Epidemio-logical and Economic Study (VEINES) [7], an internationalprospective cohort study to evaluate the epidemiology and

1050 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
outcomes of chronic venous disorders, our group developedand validated a venous-disease-specific quality of life mea-sure for use in patients with chronic venous disease, theVEINES-QOL/Sym questionnaire [8]. For the presentstudy, we performed a comprehensive psychometric evalu-ation of the VEINES-QOL/Sym questionnaire in an inde-pendent sample of patients with acute deep venousthrombosis. (The VEINES-QOL/Sym questionnaire isavailable with the on-line version of this article at http://www.elsevier.com/locate/jclinepi.)
2. Methods
2.1. Questionnaire development
The VEINES-QOL/Sym is a patient-based questionnairedesigned for self-completion. The content and format ofquestionnaire items and response scales were modeled afterthe SF-36 [9,10]. Generic SF-36 questions were modified tomake them specific to venous disease, and new venous-dis-ease-specific questions were developed using the same for-mat and response scales of the SF-36. The questionnairewas developed in English and was then translated intoFrench, French Canadian (for use with French-speakingpatients in Canada), and Italian. The development of thequestionnaire content, translation procedures, independentexpert review, pretesting with patients, and psychometricevaluation in patients with chronic venous disease are de-scribed in detail elsewhere [8].
2.2. VEINES-QOL/Sym questionnaire
The 26-item questionnaire measures the impact of deepvenous thrombosis on symptoms and quality of life fromthe patient’s perspective. The items cover symptoms (10items), limitations in daily activities (9 items), time ofday of greatest intensity (1 item), change over the past year(1 item), and psychological impact (5 items). Responses arerated on two-point to seven-point Likert response scales ofintensity, frequency, or agreement. The time frame forquestions about symptoms, daily limitations, and psycho-logical impact covers the previous 4 weeks, as in the SF-36.
2.3. Scoring the VEINES-QOL/Sym
Two summary scores can be computed. The VEINES-QOL summary score (25 items) provides an estimate ofthe overall impact of deep venous thrombosis on the pa-tient’s quality of life. The VEINES-Sym summary score(10 items) measures symptom severity. This includes ninevenous symptoms (heavy legs, aching legs, swelling, nightcramps, heat or burning sensation, restless legs, throbbing,itching, tingling sensation), rated on a five-point Likertscale of frequency (every day, several times a week, aboutonce a week, less than once a week, never), and leg painrated on a six-point scale of intensity (very severe, severe,moderate, mild, very mild, none). One item that asks about
the time of day that the leg problem is most intense is notincluded in the summary scores; it provides descriptive in-formation only, which may be of use in epidemiologicalresearch.
For both the VEINES-QOL and VEINES-Sym scales,high scores indicate better outcomes. The VEINES-QOL/Sym uses the standard method that is routinely used [11]for scoring questionnaires with items with different re-sponse scales [12]. Raw scores are first transformed toz-score equivalents (mean, 0; standard deviation, 1), whichare then transformed to T-scores (mean, 50; standard devia-tion, 10) to give an easily understood range of scores. Scoresfor missing data are imputed using the same algorithm rec-ommended for scoring the SF-36 [9,10]. A person-specificestimate is imputed for any missing item in cases wherethe patient answered >50% of the items in the scale.
A copy of the VEINES-QOL/Sym and the SAS scoringprogram can be obtained from the corresponding author.
2.4. Validation of the VEINES-QOL/Sym in deep veinthrombosis: the Venous Thrombosis Outcomes study
The Venous Thrombosis Outcomes (VETO) study is anongoing, multicenter prospective cohort study with 5-yearfollow-up that we are conducting at seven hospital centersin the province of Quebec, Canada. Its objectives are to es-timate the incidence and timing of development of the post-thrombotic syndrome (PTS) after deep venous thrombosis,to identify clinical and genetic risk factors that predict itsdevelopment, to measure the impact of deep venous throm-bosis on quality of life, and to evaluate resource utilizationand costs associated with deep venous thrombosis. An ad-ditional, prespecified objective was to assess the psycho-metric properties of the VEINES-QOL/Sym questionnairefor the evaluation of quality of life and symptoms inpatients with deep venous thrombosis.
2.4.1. PatientsDuring the study recruitment phase, all consecutive pa-
tients with objectively diagnosed, acute deep venous throm-bosis at the seven hospital centers were screened foreligibility to participate in the VETO Study. The diagnosisof deep venous thrombosis was based on a venous duplexultrasonography showing lack of compressibility or intralu-minal thrombus in the affected vein [13,14] or on a contrastvenogram showing a constant intraluminal filling defect inat least two different projections [15]. Patients were eligibleto participate if they could read and understand English orFrench. Patients were excluded if they were incapable of re-sponding to a questionnaire, had geographic inaccessibilitythat prevented return for the follow-up visits, had an ex-pected lifespan of !3 months, or were unable or refusedto provide informed consent.
Ethics approval was obtained from the relevant commit-tees in each hospital center and written informed consentwas obtained from all patients prior to study entry.

1051S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
2.4.2. Study proceduresFrom April 2001 to July 2002, 359 patients were en-
rolled in the VETO Study. To obtain data for the psycho-metric analysis, study patients were evaluated at clinicvisits that took place at the time of enrollment (baseline)and at 1 and 4 months. At each clinic visit, patient-reportedsymptoms and quality of life were assessed using the appro-priate language version (i.e., English or French Canadian)of the SF-36 [9,10] and of the VEINES-QOL/Sym [8].The SF-36 questionnaire produces two summary scores:a Physical Component Summary score (PCS) and a MentalComponent Summary score (MCS), which reflect physicaland mental health status, respectively. The VEINES-QOL/Sym questionnaire produces two summary scores,VEINES-QOL and VEINES-Sym, which reflect venousdisease-specific quality of life and venous symptoms,respectively.
At each visit, patients provided information on changesin their health and underwent a standardized clinical assess-ment for the PTS, using a clinical scale developed by Vil-lalta et al. [16]. This scale grades the severity, from 0 to3, of each of five symptoms (pain, cramps, heaviness, pru-ritus, and paresthesia) and six signs (edema, skin indura-tion, hyperpigmentation, venous ectasia, redness, painduring calf compression). A score of >5 indicates PTSand a score of >15 or the presence of a venous ulcer indi-cates severe PTS.
2.4.3. Psychometric Evaluation of the VEINES-QOL/Sym
We used gold-standard psychometric tests and criteria toevaluate the acceptability, reliability, validity, and respon-siveness of VEINES-QOL/Sym scores [8,9,12,17].
Acceptability affects the quality of the data obtained, andwas assessed by examining completeness of data and scoredistributions. Criteria for acceptability included !5%missing data for summary scores, even distribution of en-dorsement frequencies across response categories, and!10% floor and ceiling effects for summary scores.
Reliability was assessed by measuring internal consis-tency and test–retest reliability. Internal consistency refersto the extent to which items comprising the scale measurethe same construct (i.e., homogeneity of scale), and wasassessed by Cronbach’s a [18] (should be O0.70 forsummary scores) and item–total correlations (should beO0.20) [17]. Test–retest reliability, an indicator of the sta-bility of a measuring instrument, was assessed by adminis-tering the instrument to respondents on two differentoccasions and examining the correlation between test andretest scores. The length of the test–retest interval shouldbe short enough to ensure that clinical change in the symp-tom being measured is unlikely to occur, but sufficientlylong to ensure that respondents do not recall their responsesfrom first assessment. The test–retest interval in this studywas 14 days. Test–retest reliability correlations for sum-mary scores should be O0.80 [17].
Content validity refers to the extent to which the contentof a scale is representative of the conceptual domain it isintended to cover, namely venous thrombosis, and was as-sessed qualitatively through pretesting with patients, expertopinion and literature review. Construct validity is shownby within-scale analyses and analyses against external cri-teria. Within-scale analyses should show evidence that a sin-gle entity (construct) is being measured and that items canbe combined to form a summary score. This was assessedon the basis of evidence of good internal consistency (Cron-bach’s a O 0.70) and a high correlation between VEINES-QOL and VEINES-Sym scores (which purport to measurerelated aspects of outcome).
Analyses against external criteria included (a) conver-gent validity, (b) discriminant validity, and (c) known-groups differences.
Convergent validity is shown by evidence that the scaleis correlated with other measures of same or similar con-structs, and assessed on the basis of correlations betweenVEINES-QOL/Sym and SF-36 scores. Correlations are ex-pected to vary according to the similarity of the constructsbeing measured by each instrument. Both VEINES-QOLand SF-36 assess quality of life, so the two measures shouldbe correlated, but because VEINES-QOL and SF-36 differin being disease-specific vs. generic measures, correlationswere expected to be in the moderate range (|0.5) [19].VEINES-QOL/Sym items tap more physical than mentalaspects, so higher correlations were expected with SF-36PCS (physical) score than with MCS (mental) score. Fi-nally, higher correlations were expected betweenVEINES-QOL and SF-36 than between VEINES-Symand SF-36, because there is less overlap in content betweenthe latter two.
Discriminant validity is assessed by demonstrating thatthe scale is not correlated with other measures of differentconstructs. For example, low correlations were expectedbetween VEINES-QOL/Sym scores and age and sex.
Known-groups differences addresses the scale’s ability todifferentiate known groups. This was assessed by compar-ing VEINES-QOL/Sym scores for patients who differedin severity of disease (as indicated by the Villalta PTSscore). VEINES-QOL/Sym scores should decrease with in-creasing severity of disease.
Responsiveness refers to the ability of a scale to detectclinically important change over time. The standard methodfor evaluating responsiveness is in the context of an inter-vention study, where pre- and posttreatment change scoresare used to determine effect sizes. The VETO Study is a co-hort study with no systematic intervention component, sowe assessed responsiveness by calculating effect sizes[20,21] and standardized response means [22] for changein VEINES-QOL/Sym scores from 1 month to 4 months.
Effect size was calculated as the mean change score from1 month to 4 months divided by the standard deviation ofscores at the 1-month assessment. This permits translationof before-and-after changes into a standard unit of
1052 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
measurement, rather than comparing raw score changes[20]. The standardized response mean is a variant of the ef-fect size [22] and was calculated as the mean change scorefrom 1 month to 4 months divided by the standard deviationof the change score. Effect size statistics and standardizedresponse means were compared in patients defined as clin-ically improved or unimproved according to change VillaltaPTS score [16] during the same time period. Effect sizesand standardized response means of 0.20 were defined assmall, 0.50 as moderate, and >0.80 as large [20]. To com-pare the responsiveness of the disease-specific VEINES-QOL/Sym with that of a generic measure, we used the samemethods to evaluate responsiveness of SF-36 PCS and MCSscores.
2.4.4. Study samples for psychometric evaluationAcceptability of the questionnaire was assessed in the
full sample of 359 patients. Reliability and validity analy-ses were carried out in all VETO patients who providedscorable VEINES-QOL/Sym and SF-36 questionnaires(<20% missing data) at the baseline clinic visit. This sam-ple included 357 patients. Test–retest reliability was evalu-ated in 52 VETO study patients at two of the study centersfor reasons of convenience (Jewish General Hospital, 19English-speaking and 6 French-speaking patients; HopitalMaisonneuve-Rosemont, 27 French-speaking patients). Af-ter completing the VEINES-QOL/Sym questionnaire at the4-month clinic visit, patients completed the questionnaireagain within a 2-week interval and mailed it to the studycenter. Responsiveness was evaluated in all VETO patientswho satisfied two criteria: (i) !20% missing data on theVEINES-QOL/Sym and (ii) data available for both pa-tient-reported outcomes (i.e., quality of life questionnaires)and clinical outcome (i.e., PTS score) for both the 1-monthand 4-month clinic visits. The responsiveness sample in-cluded 303 patients; most exclusions were due to missed1- or 4-month clinic visits, with only 2 patients excludedbecause of O20% missing VEINES-QOL/Sym data.
3. Results
3.1. VETO Study patient characteristics
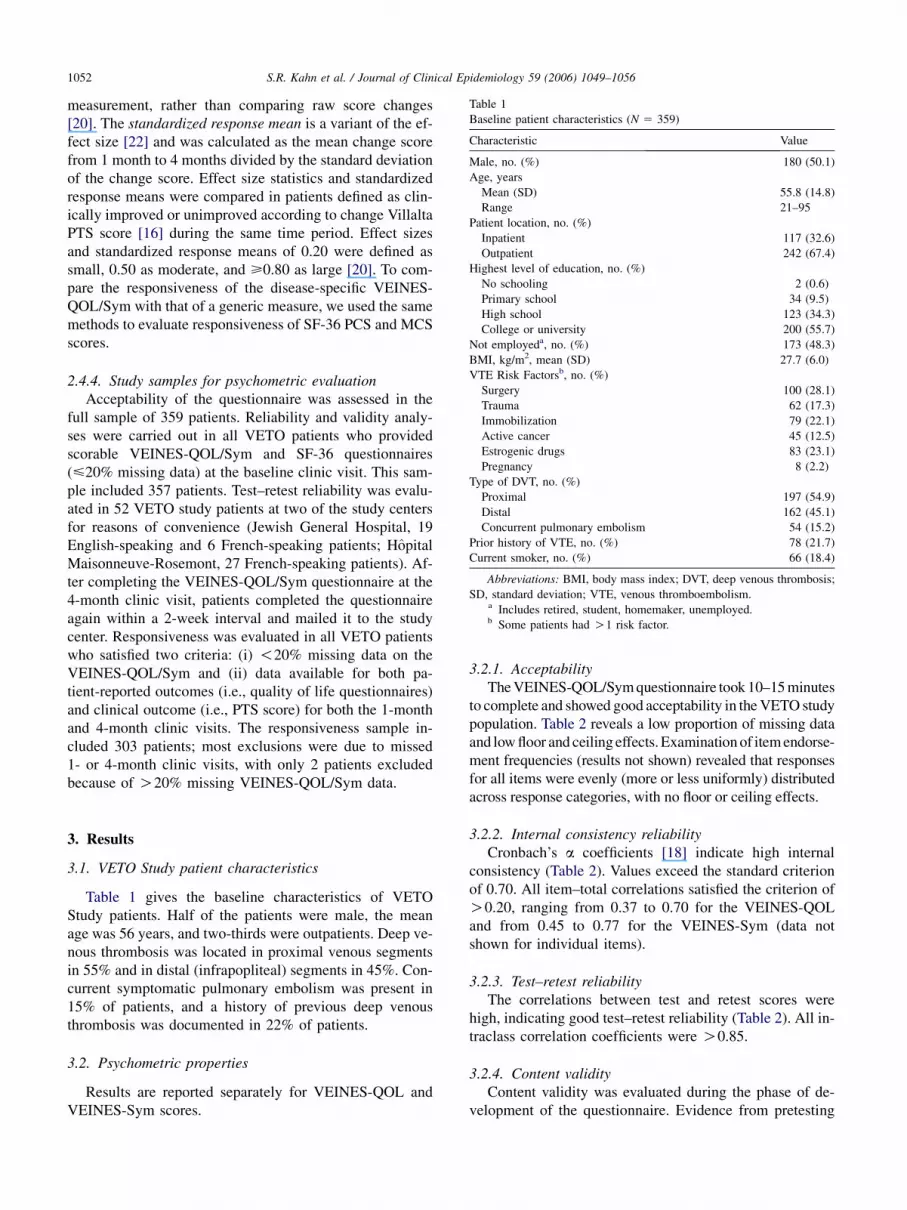
Table 1 gives the baseline characteristics of VETOStudy patients. Half of the patients were male, the meanage was 56 years, and two-thirds were outpatients. Deep ve-nous thrombosis was located in proximal venous segmentsin 55% and in distal (infrapopliteal) segments in 45%. Con-current symptomatic pulmonary embolism was present in15% of patients, and a history of previous deep venousthrombosis was documented in 22% of patients.
3.2. Psychometric properties
Results are reported separately for VEINES-QOL andVEINES-Sym scores.
3.2.1. AcceptabilityThe VEINES-QOL/Sym questionnaire took 10–15 minutes
to complete and showed good acceptability in the VETO studypopulation. Table 2 reveals a low proportion of missing dataand low floor and ceiling effects. Examination of item endorse-ment frequencies (results not shown) revealed that responsesfor all items were evenly (more or less uniformly) distributedacross response categories, with no floor or ceiling effects.
3.2.2. Internal consistency reliabilityCronbach’s a coefficients [18] indicate high internal
consistency (Table 2). Values exceed the standard criterionof 0.70. All item–total correlations satisfied the criterion ofO0.20, ranging from 0.37 to 0.70 for the VEINES-QOLand from 0.45 to 0.77 for the VEINES-Sym (data notshown for individual items).
3.2.3. Test–retest reliabilityThe correlations between test and retest scores were
high, indicating good test–retest reliability (Table 2). All in-traclass correlation coefficients were O0.85.
3.2.4. Content validityContent validity was evaluated during the phase of de-
velopment of the questionnaire. Evidence from pretesting
Table 1
Baseline patient characteristics (N 5 359)
Characteristic Value
Male, no. (%) 180 (50.1)
Age, years
Mean (SD) 55.8 (14.8)
Range 21–95
Patient location, no. (%)
Inpatient 117 (32.6)
Outpatient 242 (67.4)
Highest level of education, no. (%)
No schooling 2 (0.6)
Primary school 34 (9.5)
High school 123 (34.3)
College or university 200 (55.7)
Not employeda, no. (%) 173 (48.3)
BMI, kg/m2, mean (SD) 27.7 (6.0)
VTE Risk Factorsb, no. (%)
Surgery 100 (28.1)
Trauma 62 (17.3)
Immobilization 79 (22.1)
Active cancer 45 (12.5)
Estrogenic drugs 83 (23.1)
Pregnancy 8 (2.2)
Type of DVT, no. (%)
Proximal 197 (54.9)
Distal 162 (45.1)
Concurrent pulmonary embolism 54 (15.2)
Prior history of VTE, no. (%) 78 (21.7)
Current smoker, no. (%) 66 (18.4)
Abbreviations: BMI, body mass index; DVT, deep venous thrombosis;
SD, standard deviation; VTE, venous thromboembolism.a Includes retired, student, homemaker, unemployed.b Some patients had O1 risk factor.

1053S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
with patients, expert opinion, and a review of literature sup-ports the content validity of the VEINES-QOL/Sym [8].
3.2.5. Construct validity (within-scale analyses)Evidence of high internal consistency supports the con-
struct validity of the VEINES-QOL/Sym. High a coeffi-cients (Table 2) and moderately high item–totalcorrelations indicate that a single construct is being mea-sured and that the items can be combined to form summaryscores. A high intercorrelation between VEINES-QOL andVEINES-Sym scores (r 5 0.88) supports the convergentvalidity of the two scales.
3.2.6. Construct validity (convergent validity)Table 3 gives the correlations between the VEINES-
QOL/Sym and the SF-36. All correlations support our hy-potheses. The VEINES-QOL/Sym is moderately correlatedwith SF-36 PCS and MCS summary scores. Correlationsbetween the VEINES-QOL and SF-36 are higher for PCS(physical health status) than MCS (mental health status)scores. Correlations with the SF-36 are higher for theVEINES-QOL than for the VEINES-Sym.
Table 2
Acceptability and reliability of the VEINES-QOL/Sym
Value
Missing data, % (N 5 359)
VEINES-QOL 1
VEINES-Sym 1
Floor effects, % (N 5 357)
VEINES-QOL !1
VEINES-Sym !1
Ceiling effects, % (N 5 357)
VEINES-QOL !1
VEINES-Sym 8
Internal consistency: Cronbach’s a (N 5 357)
VEINES-QOL 0.91
VEINES-Sym 0.88
Test–retest reliability: ICCa
VEINES-QOL 0.87
VEINES-Sym 0.87
Abbreviations: ICC, Intraclass correlation coefficient.a Test–retest analyses performed on 52 patients at two centers.
Table 3
Convergent and discriminant validity of the VEINES-QOL/Sym
(N 5 357)
Correlation, r
VEINES-QOL VEINES-Sym
Other measures
SF-36 physical (PCS) 0.63 0.49
SF-36 mental (MCS) 0.37 0.29
Patient characteristics
Age 0.06 0.03
Sex 0.15 0.12
3.2.7. Construct validity (discriminant validity)Low correlations between the VEINES-QOL and
VEINES Sym and age and sex (all correlations <0.15)(Table 3) support the discriminant validity of both scalesand suggest that responses to the VEINES-QOL/Sym are notbiased in terms of age or gender.
3.2.8. Construct validity (known group differences)Table 4 gives the mean VEINES-QOL/Sym scores for
patients classified by Villalta PTS score obtained at the1-month clinic visit. As hypothesized, VEINES-QOL andVEINES-Sym scores show the expected gradient of pooreroutcome with increasing severity of PTS.
3.2.9. ResponsivenessTable 5 gives the results of the responsiveness analysis
of the VEINES-QOL/Sym and SF-36. Among patientswhose PTS scores improved from 1 month to 4 months,larger effect sizes were observed for the VEINES-QOL(0.77), VEINES-Sym (0.65) and SF-36 PCS (0.60) thanfor SF-36 MCS (0.38). Hence, VEINES-QOL is the mostresponsive, VEINES-Sym and SF-36 PCS show similar re-sponsiveness, and the SF-36 MCS is the least responsive tochange. In contrast, among patients without improvementin PTS scores, effect sizes for all measures were small.The standardized response mean showed similar patterns.Results therefore demonstrate that the VEINES-QOL andVEINES-Sym are both highly responsive to clinicalchange, indicating that VEINES-QOL and VEINES-SYMsuccessfully discriminate between clinically improved andunimproved patients.
4. Discussion
The results of our prospective psychometric evaluationof the VEINES-QOL/Sym questionnaire indicate that itmeets standard, accepted criteria of acceptability, reliabil-ity, validity, and responsiveness for use as a patient-reported measure of outcome in deep venous thrombosis.The VEINES-QOL/Sym questionnaire is available in fourlanguage versions, is quick and easy to administer, andcan be easily incorporated into epidemiological studies
Table 4
Known-group differences validity as mean VEINES-QOL/Sym scores
by PTS score at 1 month (N 5 328)
Scoreb, PTS N
Scorea, mean (SD)
VEINES-QOL VEINES-Sym
0–4 175 52.0 (4.9) 52.9 (4.6)
5–14 145 47.9 (5.5) 48.2 (5.6)
>15 8 42.1 (5.3) 40.6 (6.6)
Of the original 359 VETO patients, 31 did not attend the 1-month visit.
Abbreviations: PTS, postthrombotic syndrome; SD, standard deviation.a Higher scores indicate better outcomes.b Higher scores indicate more severe disease.

1054 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
Table 5
Responsiveness of the VEINES-QOL/Sym in patients with deep vein thrombosis
N
QOL score, mean (SD) 1 to 4 mo change
1 mo 4 mo Change Effect sizea SRMa
PTS scores improved
VEINES-QOL 158 49.6 (5.6) 54.0 (5.2) 4.3 (4.3) 0.77 1.0
VEINES-Sym 158 50.0 (5.9) 53.8 (5.1) 3.8 (4.8) 0.65 0.79
SF-36 PCS 158 36.9 (11.0) 43.5 (11.4) 6.6 (10.5) 0.60 0.63
SF-36 MCS 158 46.5 (12.1) 51.0 (10.3) 4.6 (11.2) 0.38 0.40
PTS scores did not improve
VEINES-QOL 142 50.3 (5.6) 52.1 (6.0) 1.9 (4.6) 0.33 0.41
VEINES-Sym 142 50.9 (5.6) 51.5 (6.3) 0.5 (5.4) 0.09 0.11
SF-36 PCS 145 39.2 (10.5) 42.7 (11.8) 3.4 (10.1) 0.33 0.34
SF-36 MCS 144 45.5 (11.9) 49.5 (10.7) 3.9 (10.2) 0.34 0.38
Mean scores, effect sizes, and standardized response means for change in VEINES-QOL/Sym and SF-36 scores between 1-month and 4-month assess-
ments, according to improvement or lack of improvement in PTS scores. Positive change scores indicate improvement in quality of life.
Abbreviations: MCS, mental component summary; PCS, physical component summary; PTS, postthrombotic syndrome; SRM, standardized response
mean; Sym, symptom portion of VEINES.a Effect sizes and standardized response means of 0.20 are defined as small, 0.50 as moderate, and >0.80 or greater as large [20].
and clinical trials of new drug treatments, thus providinga rigorous method for improving the evaluation of out-comes in studies of patients with deep venous thrombosis.
Deep venous thrombosis is associated with significantdisease burden in terms of pain and suffering, loss of mo-bility, impairment of function at work and at home, andpsychological distress [23]. Research on these importantpatient-reported outcomes has been limited by the lack ofpractical, scientifically rigorous outcome measures. Todate, some studies have evaluated quality of life in patientswith deep venous thrombosis using generic measures alone[24,25]. Generic measures, however, do not give a full pic-ture of the impact of deep venous thrombosis on quality oflife and are less useful than disease-specific measures inevaluating change over time.
A number of disease-specific quality of life instrumentsintended for use in patients with deep venous thrombosishave been proposed, but none have fully met standardcriteria for validity, reliability and responsiveness. VanKorlaar et al. [26] developed a measure of venous thrombo-sis-related quality of life that was evaluated at a single timepoint in 45 retrospectively identified patients with previousdeep venous thrombosis at one hospital center. The measureshowed evidence of good internal consistency reliabilityand validity, but responsiveness and test–retest reliabilityhave not been evaluated, and individual venous symptomswere not considered.
Mathias et al. [27] developed a disease-specific qualityof life measure intended for use in patients with iliofemoraldeep venous thrombosis; this measure was derived from theHealth Utilities Index and SF-12 measures, with the addi-tion of new items specific for deep venous thrombosis. Ina population of 111 retrospectively identified patients withprior iliofemoral deep venous thrombosis, this measuredemonstrated acceptable reliability and validity but limitedresponsiveness.
Hedner et al. [28] reported on a Swedish language, 29-item instrument for measuring quality of life in patientswith deep venous thrombosis; it also includes specific itemsthat relate to burden of treatment with warfarin. Consecu-tive outpatients with proximal deep venous thrombosiscompleted the questionnaire at one point in time. There isevidence for internal consistency and construct validity,but test–retest reliability and responsiveness have not beenassessed.
Finally, Hudgens et al. [29] recently reported the devel-opment and validation of a 14-item leg symptom index in-tended for monitoring of DVT-related symptoms, ratedseparately in each leg. The measure was administered bytelephone interview to 77 patients (age and sex distributionnot reported) at 3–7 days, 30–40 days, and 12 months afterhospitalization for acute deep venous thrombosis. There isevidence of internal consistency and validity, but test–retestreliability and responsiveness have not been reported.
The VEINES-QOL/Sym has potential applications inboth research and routine monitoring of health care. Asa more responsive instrument than the SF-36, theVEINES-QOL/Sym holds promise in evaluating new treat-ments for deep venous thrombosis, whose effects may notbe detected by less sensitive generic measures. As an out-come measure in clinical trials, VEINES-QOL/Sym willprovide scientifically robust information about the efficacyof treatment from the patient’s point of view. This informa-tion, when combined with data on clinical outcomes andcosts, will allow comprehensive evaluation of new treat-ments. The VEINES-QOL/Sym measure offers flexibility,because it provides a validated measure of both deep ve-nous thrombosis-related quality of life and deep venousthrombosis-related symptoms. Although DVT treatment-re-lated issues (e.g., blood test monitoring while on warfarin)may indeed have an impact on quality of life, the objectiveof the VEINES-QOL measure is to evaluate the impact of

1055S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
the condition, not its specific treatment, on quality of life.As such, it is flexible for use in a broad range of situations,and permits comparability of studies that use different treat-ments or interventions.
Our conclusions about the acceptability, reliability, val-idity, and responsiveness of the VEINES-QOL/Sym arebased on a sample of patients with objectively diagnosedsymptomatic deep venous thrombosis recruited and pro-spectively followed at seven hospital centers. Our sampleis likely to be representative, given that our study was mul-ticenter, both inpatients and outpatients were enrolled, andinclusion criteria were broad. Nevertheless, future workshould be undertaken to establish population norms forVEINES-QOL and VEINES-Sym scores in deep venousthrombosis patients in different countries, so that the appro-priate population-based weights can be used in place of cur-rent sample-specific scoring algorithms. In addition, furtherevaluation of the ability of the VEINES-QOL/Sym measureto detect change following different treatments for deep ve-nous thrombosis would provide additional useful evidenceof responsiveness to specific interventions. Finally, testingof the VEINES-QOL/Sym measure in independent samplesof patients with deep venous thrombosis would be useful toconfirm its psychometric properties.
In conclusion, our results indicate that VEINES-QOL/Sym is a practical, reliable, valid and responsive measureof quality of life and symptoms in patients with deep ve-nous thrombosis. Use of this measure in clinical trialsand epidemiological studies of patients with deep venousthrombosis will allow more comprehensive evaluation ofpatient outcomes and burden of illness than is currentlyprovided using clinical endpoints alone.
Acknowledgments
This study was conducted as part of the VETO Study,a research program on long-term outcomes after venousthrombosis supported by the Fonds de la Recherche enSant�e du Qu�ebec and by an unrestricted grant from SanofiSynthelabo. Drs. Kahn and Shrier are recipients of ClinicalInvestigator Awards from the Fonds de la Recherche enSant�e du Qu�ebec, and Dr. Johri is a recipient of an Investi-gator Award from the Fonds de la Recherche en Sant�e duQu�ebec.
We thank the VETO study personnel at the clinical studysites for their dedication to this project.
References
[1] Bates SM, Ginsberg JS. Treatment of deep-vein thrombosis. N Engl J
Med 2004;351:268–77.
[2] Lamping DL. Measuring health-related quality of life in venous dis-
ease: practical and scientific considerations. Angiology 1997;48:51–7.
[3] Patrick DL, Deyo RA. Generic and disease-specific measures in as-
sessing health status and quality of life. Med Care 1989;27(3
Suppl):S217–32.
[4] Kahn SR, Solymoss S, Lamping DL, Abenhaim L. Long-term out-
comes after deep vein thrombosis: postphlebitic syndrome and qual-
ity of life. J Gen Intern Med 2000;15:425–9.
[5] van Korlaar I, Vossen C, Rosendaal F, Cameron L, Bovill E,
Kaptein A. Quality of life in venous disease. Thromb Haemost
2003;90:27–35.
[6] Wiebe S, Guyatt G, Weaver B, Matijevic S, Sidwell C. Comparative
responsiveness of generic and specific quality-of-life instruments.
J Clin Epidemiol 2003;56:52–60.
[7] Abenhaim L, Kurz X. The VEINES study (VEnous INsufficiency Ep-
idemiologic and Economic Study): an international cohort study on
chronic venous disorders of the leg. Angiology 1997;48:59–66.
[8] Lamping DL, Schroter S, Kurz X, Kahn SR, Abenhaim L. Evaluating
outcomes in chronic venous disorders of the leg: development of a sci-
entifically rigorous, patient-reported measure of symptoms and qual-
ity of life. J Vasc Surg 2003;37:410–9.
[9] Ware JE, Snow KK, Kosinski MA, Gandek B. SF-36 Health Survey:
Manual and interpretation guide. Boston, MA: The Health Institute,
New England Medical Center; 1993.
[10] Ware JE, Kosinski M, Keller SD. SF-36 physical and mental sum-
mary measures: a user’s manual. Boston, MA: The Health Institute,
New England Medical Center; 1994.
[11] Ware J, Kosinski M. SF-36 physical and mental health summary
scores: a manual for users of version 1. 2nd ed. Lincoln, RI: Quality-
Metric; 2001.
[12] Streiner DL, Norman GR. Health measurement scales: A practical
guide to their development and use. 2nd ed. Oxford: Oxford Univer-
sity Press; 1995.
[13] Lensing AWA, Prandoni P, Brandjes DPM, Huisman PM, Vigo M,
Tomasella G, Krekt J, Wouter Ten Cate J, Huisman MV,
Buller HR. Detection of deep vein thrombosis by real-time B mode
ultrasonography. N Engl J Med 1989;320:342–5.
[14] Kearon C, Ginsberg JS, Hirsh J. The role of venous ultrasonography
in the diagnosis of suspected deep venous thrombosis and pulmonary
embolism. Ann Intern Med 1998;129:1044–9.
[15] Lensing AWA, Buller HR, Prandoni P, Batchelor D, Molenaar AH,
Cogo A, Vigo M, Huisman PM, ten Cate JW. Contrast venography,
the gold standard for the diagnosis of deep vein thrombosis: improve-
ment in observer agreement. Thromb Haemost 1992;67:8–12.
[16] Villalta S, Bagatella P, Piccioli A, Lensing A, Prins M, Prandoni P.
Assessment of validity and reproducibility of a clinical scale for the
post-thrombotic syndrome. Haemostasis 1994;24:158a. [Abstract].
[17] Nunnally JC, Bernstein IH. Psychometric theory. 3rd ed. New York:
McGraw-Hill; 1994.
[18] Cronbach L. Coefficient alpha and the internal structure of tests. Psy-
chometrika 1951;16:297–334.
[19] Colton T. Statistics in medicine. 1st ed. Boston, MA: Little, Brown;
1974. 210–1.
[20] Cohen J. Statistical power analysis for the behavioral sciences.
Revised ed. New York: Academic Press; 1977.
[21] Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting
changes in health status. Med Care 1989;27(3 Suppl):S178–89.
[22] Liang MH, Fossel AH, Larson MG. Comparisons of five health status
instruments for orthopedic evaluation. Med Care 1990;28:632–42.
[23] Kahn SR, Ginsberg JS. Relationship between deep venous thrombo-
sis and the postthrombotic syndrome. Arch Int Med 2004;164:
17–26.
[24] Beyth RJ, Cohen AM, Landefeld CS. Long-term outcomes of deep-
vein thrombosis. Arch Intern Med 1995;155:1031–7.
[25] O’Brien B, Levine M, Willan A, Goeree R, Haley S, Blackhouse G,
Gent M. Economic evaluation of outpatient treatment with low-mole-
cular-weight heparin for proximal vein thrombosis. Arch Intern Med
1999;159:2298–304.
[26] Van Korlaar IM, Vossen CY, Rosendaal FR, Bovill EG, Cushman M,
Naud S, Kaptein AA. The impact of venous thrombosis on quality of
life. Thromb Res 2004;114:11–8.

1056 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
[27] Mathias SD, Prebil LA, Putterman CG, Chmiel JJ, Throm RC,
Comerota AJ. A health-related quality of life measure in patients with
deep vein thrombosis: a validation study. Drug Inf J 1999;33:
1173–87.
[28] Hedner E, Carlsson J, Kulich KR, Stigendal L, Ingelgard A,
Wiklund I. An instrument for measuring health-related quality of life
in patients with deep venous thrombosis (DVT): development and
validation of Deep Venous Thrombosis Quality of Life (DVTQOL)
questionnaire. Health Qual Life Outcomes 2004;2:30.
[29] Hudgens S, Cella D, Caprini C, Caprini J. Deep vein thrombosis: val-
idation of a patient-reported leg symptom index. Health Qual Life
Outcomes 2003;1:76.

1056.e1S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
You have had a venous thrombosis. In this survey, we are interested in finding out more
about the effects of your leg problem on your daily activities, both at home and at work.
This information will give us a better idea about how to treat such problems.
Thank you for participating in this study. This questionnaire includes questions about
your health in general and about your leg problem, as well as questions about your life
and usual activities. It will take about 10 minutes to complete. All of your answers are
confidential. Do not write your name on the questionnaire.
Thank you for your help.
VEINES-QOL/SymQUESTIONNAIRE

1056.e2 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
INSTRUCTIONS
HOW TO ANSWER:
Answer every question by marking the answer as indicated. If you are unsure about how to answer a question, please give the best answer you can.
These questions are about your leg problem(s).
1. During the past 4 weeks, how often have you had any of the following leg problems?
(check one box on each line) Every
day
Several
times a
week
About
once
a week
Less than
once a
week Never
1. Heavy legs 1 2 3 4 5
2. Aching legs 1 2 3 4 5
3. Swelling 1 2 3 4 5
4. Night cramps 1 2 3 4 5
5. Heat or burning sensation 1 2 3 4 5
6. Restless legs 1 2 3 4 5
7. Throbbing 1 2 3 4 5
8. Itching 1 2 3 4 5
9. Tingling sensation (e.g.pins and needles)
1 2 3 4 5
2. At what time of day is your leg problem most intense ? (check one)
1 On waking 4 During the night
2 At mid-day 5 At any time of day
3 At the end of the day 6 Never
3. Compared to one year ago, how would you rate your leg problem in general now? (check one)
1 Much better now than one year ago 4 Somewhat worse now than one year ago
2 Somewhat better now than one year ago 5 Much worse now than one year ago
3 About the same now as one year ago 6 I did not have any leg problem last year

1056.e3S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
4. The following items are about activities that you might do in a typical day. Does your leg problem now limit you in these activities? If so, how much ?
(Check one box on each line)
I do not
work
YES,
Limited A
Lot
YES,
Limited A
Little
NO, Not
Limited At
All
a. Daily activities at work 0 1 2 3
b. Daily activities at home (e.g. housework, ironing, doing odd jobs repairs around the house, gardening, etc...)
1 2 3
c. Social or leisure activities in which you are standing for long periods (e.g. parties, weddings, taking public transportation, shopping, etc...)
1 2 3
d. Social or leisure activities in which you are sitting for long periods (e.g. going to the cinema or the theater, travelling, etc...)
1 2 3
5. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your leg problem?
(check one box on each line) YES NO
a. Cut down the amount of time you spent on work or other activities 1 2
b. Accomplished less than you would like 1 2
c. Were limited in the kind of work or other activities 1 2
d. Had difficulty performing the work or other activities (for example, it took extraeffort)
1 2
6. During the past 4 weeks, to what extent has your leg problem interfered with your normal social activities with family, friends, neighbors or groups? (check one)
1 Not at all 4 Quite a bit
2 Slightly 5 Extremely
3 Moderately
7. How much leg pain have you had during the past 4 weeks? (check one)
1 None 4 Moderate
2 Very mild 5 Severe
3 Mild 6 Very severe
1056.e4 S.R. Kahn et al. / Journal of Clinical Epidemiology 59 (2006) 1049–1056
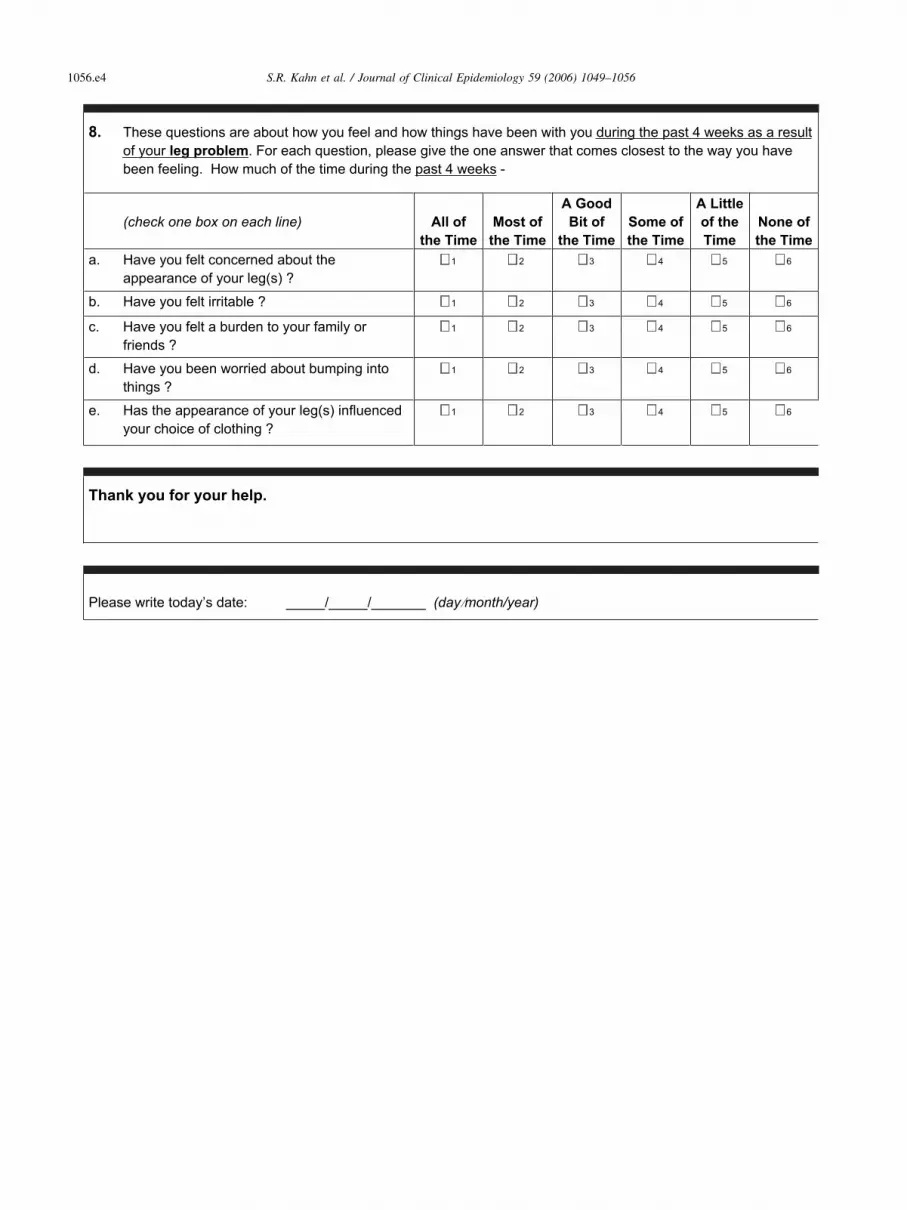
8. These questions are about how you feel and how things have been with you during the past 4 weeks as a result of your leg problem. For each question, please give the one answer that comes closest to the way you have been feeling. How much of the time during the past 4 weeks -
(check one box on each line) All of
the Time
Most of
the Time
A Good
Bit of
the Time
Some of
the Time
A Little
of the
Time
None of
the Time
a. Have you felt concerned about the appearance of your leg(s) ?
1 2 3 4 5 6
b. Have you felt irritable ? 1 2 3 4 5 6
c. Have you felt a burden to your family or friends ?
1 2 3 4 5 6
d. Have you been worried about bumping into things ?
1 2 3 4 5 6
e. Has the appearance of your leg(s) influenced your choice of clothing ?
1 2 3 4 5 6
Thank you for your help.
Please write today’s date: _____/_____/_______ (day month/year)




























