Embed Size (px)
Citation preview

CRF Completion Guidelines March 23rd, 2012, v1.2.2
- COMPLETION GUIDELINES -
BIOSTAT-CHF
Date: March 23rd, 2012
Version: 1.2.2
Based on:
Protocol version 2.6, dated 16 July 2010
Based on pCRF version 1.0.4., dated: 13 December 2010
(eCRF version 1.2.7 dated 25 October 2011)
DSS version 1.4.4 dated October 2011

BIOSTAT-CHF Page: II
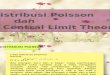
FLOWCHART
CRF Completion Guidelines March 23rd, 2012, v1.2.2
En
rolm
en
t
9-m
on
th v
isit
±1
mo
nth
Fo
llo
w-u
p v
isit
Ev
ery
six
mo
nth
s
En
d o
f In
de
x
stu
dy
Fe
b-A
pr
201
4
Assessments
Informed consent X
Medical history and demographics X
Physical examination X X
Signs and symptoms of HF X X
6MWT X X
EQ5D, KCCQ X X
Local laboratory1 X X
Sample (blood) X3 X
Sample (urine) X3 X
ECG X X
Echocardiography1 X X
Chest x-ray1 X X
Coronary angiography1 X X
Right heart catheterization1 X X
Up-titration ACEi / ARBs / β-blockers
X
Concomitant medication X X X X
Death or hospitalizations2 X X X
1
These examinations may be done as part of routine clinical care. If these examinations are done, then the data is recorded. They are not performed specifically for this study.
2 If patient is hospitalized or has deceased at any time during follow-up then a hospitalization or death form (EVENT
FORM) is completed.
3 Samples at enrolment visit should be taken within 48 hours prior to anticipated initiation or up-titration of medication.

BIOSTAT-CHF Page: III
INSTRUCTIONS
CRF Completion Guidelines March 23rd, 2012, v1.2.2
General (e)CRF Completion Guidelines
An eCRF (electronic Case Report Form) is designed to enter all the data collected during a study.
The instructions provided in these guidelines refer to all situations that can occur during the input of data into the eCRF.
1. General Instructions
Each eCRF page has a header like the one below:
The fields Patient, Visit Name and Subevent# will be filled automatically.
The field Entry Date should contain the date of first entry of this page.By entering “t” the date of today will automatically be completed.
The General Comment field can be used to clarify the entered data if necessary. The Is Blank field must be ticked if there is no data available and in that case, a clarification comment must be entered in the General Comment field.
2. Data Completion
Missing data
Complete all questions on every form unless otherwise directed.
A field that is left open but should have been filled will result in a query which has to be answered by the site and forwarded to the data manager.
Sometimes it is possible to enter NA/ND/UNK in a field that only accepts numbers. In this case, a magnifying glass appears at the right side of the field when you select the field. This allows the operator to classify the missing data by entering NA, ND or UNK. Click on the magnifying glass to see the possible answers
Use NA to mark missing data as Not Applicable Use ND to mark missing data as Not Done Use UNK or UK to mark missing data as UNKnown
In case the field is a date/time field and only a partial date/time is known then replace the missing items with UK. E.g. when the day is missing enter UK-05-2010 and when the date and month are missing enter the date as UK-UK-2010. This will however create a Validation Error and produce the following dialog box:
In the comment box specify the reason why the date is incomplete and in the action box select the option Send to Data Mgt and click on Ok.

BIOSTAT-CHF Page: IV
Instructions
CRF Completion Guidelines March 23rd, 2012. V1.2.2
Date and Time
Dates can be entered as a continuous line of numbers. E.g. 01052010 is 01-May-2010. The EDC will automatically change the date in 01-05-2010. If you use 2 digits for the year then it will use the following rule if the 2 digit year is > current 2 digit year it will assume that the year was in the previous century (1900-1999). If the 2 digit year <= current 2 digit year it will assume that the year is in the current century (2000-2099). To avoid mistakes always enter the year with 4 digits.
Time can be entered as a continues line of numbers (at least 3). E.g. 1225 is 12:25. RDC will automatically enter the semi-colon (:) when leaving the time field. When you enter only 3 digits RDC will assume that the first digit is a 0. So 123 will become 01:23. Ensure you always use the 24 hour clock notation.
It is possible to change the input and display format of a date field by using the preferences option found in the top
right corner of the application (see below the options that can be changed).
Select the input and display format you would like to use and press apply to activate the chosen values.
Numbers
Numerical values are checked against the field definition when being entered. If the entered value does not comply with the definition a Validation Error dialog box will appear (e.g. where a number is expected and text is entered).
For numbers with decimals, the point (.) is used as a decimal symbol.
It is not necessary to add zeros before the numerical value to fill up the field.
Free Text
Please use precise medical terminology. Common medical abbreviations are acceptable. Answers should be provided in English Keep in mind that a text field can contain a limited number of characters (at most 200). To see how many characters a field can contain, select the field with your right mouse button. In the pop-up menu select Field Help. A dialog will open and list information about the field. A query will be generated if you try to store more characters than the field can contain and the surplus of text will be lost.
Radio Buttons
Radio buttons are used to make a selection from a predefined number of options. Below are 2 examples.
You select the correct answer by a mouse click. To select a different answer click on the correct button. In order to clear the selection, click on the selected radio button again.
List of Values
A list of values is used in case the predefined options are too many to display as radio buttons. To display the list of possible values, select the field and click on the magnifying glass that will appear next to the field, or press ALT-L.

BIOSTAT-CHF Page: V
Instructions
CRF Completion Guidelines March 23rd, 2012. V1.2.2
Use the scrollbar on the right to see all values. Mark the value you want to enter in the Select column and press Ok. If you know which values are allowed you can also enter them directly in the field. However, if you make a mistake a Validation Error dialog box will show.
Check box
Ticking a check box means YES. When you leave the Check box blank this means NO. An example of a check box:
A mouse click will tick the box and to clear the selection you can click again.
Contact information for questions regarding CRF completion
Your first line of contact is your Country Coordinator. If she / he is unavailable, you can also contact TCC for specific questions, preferably by e-mail ([email protected]). Please indicate study name, patient number and CRF page and then write your question. Please copy your Country Coordinator in your message.
3. Saving data and Data Correction
When you save the page the eCRF will ask if you want to save the page as Complete or Incomplete. If you save the page as Complete the system will start the audit trail for this page and for every change to the data hereafter a reason for change has to be given. If you save the page as Incomplete you can change the data without a reason for change.
Automatic queries will not be generated until you save the page as Complete.

BIOSTAT-CHF Page: VI
Instructions
CRF Completion Guidelines March 23rd, 2012. V1.2.2
4. Additional Clarifying Information
To avoid any unnecessary queries from the Monitor or Data Manager you can give comments on the data in the general comment field on top of each page or use the AddInfo page at the SUMMARY visit in the eCRF.
It is also possible to add an investigator comment. To enter information in this field please press the button . This will open the Add Investigator Comment dialog box seen below.
Open CRF Navigator
Add your comment in the field Investigator comment and press OK. Investigator comments are listed in the CRF navigator which is located on the right side of the screen. If not visible you can click on the arrow located on the right side of the Internet Explorer window half way down (see image above).
5. Repeating Pages
For some panels it cannot be defined in advance how much data will be collected, e.g. Adverse Events or Medication. In order to allow unlimited entry of data it is possible to add additional pages. The procedure for this is as follows:
Go to the applicable patient and applicable visit where you wish to add more data
Select the patient by ticking the box on the left side of the patient icon
Click on the button Add Visit Page
Select the page you want to add and click Continue
The next screen shows information about the Sub-Visit value. This is a system variable that cannot be changed
Click apply to create the page
A new page will be visible. Click on it to start entering the data. If you do not enter any data the page will be removed when you change to another visit.
6. Withdrawal of patients
In case a patient withdraws from a study, the first page of the next visit must be checked as blank. Add in the General Comment field “patient withdrawn”. Furthermore the EOS page in the END OF STUDY visit should be completed.

BIOSTAT-CHF Page: 1 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
PATIENT STUDY NUMBER
For every patient that signs a written informed consent form (ICF), a unique study number should be assigned.
It is important to distinguish between two types of patients. If the patient has signed ICF, but turns out not to be eligible for the study, then this patient is considered to be a Pre-screening failure. Pre-screening failures should be assigned a unique study number starting with an “S” and then a number, i.e. S01, S02, etc. No data will be entered for these subjects in the study database. Informed consent should be filed and the screening log should be updated only.
For patient that have signed ICF and are eligible are enrolled in the study. These patients should be assigned unique study numbers starting with 001, 002 etc. If the patient drops out during the baseline visit, but before the sampling is performed, or if the sampling procedure fails, then the patient is considered a Screening failure and panels 1, 2, 3 and 4 should be recorded in the study database for this patient.
1 ENROLMENT
Patients may be recruited as in-patients or from the outpatient clinic. Patient is enrolled before anticipated initiation or up-titrating of ACEi/ARBs and beta-blockers. It is critical that all blood samples are obtained within 48 hours prior to anticipated initiation of medication up-titration.
Data collected in the previous 3 months can be recorded as study data. If patient has multiple assessments of the same type of assessment in the 3 months before enrolment, then the most recent is used. For recording of optional examinations in the eCRF at baseline: record the examination which is closest to the date of enrolment. The examination should have been performed within three months before or after enrolment. Exception is the Echo, which is permitted up to 24 months before enrolment (or 3 months after enrolment).
After enrolment, physicians will be allowed to modify ongoing oral therapy according to the ESC guidelines. This will likely include initiation or up-titration of ACEi/ARBs and beta blockers according to the ESC guideline. After 3 months, patients are expected to be optimally treated.
Enter date of enrolment visit (dd mon yyyy) Date of enrolment (screening) visit:use the date of when the in and exclusion criteria are checked and when it is decided that the patient can be enrolled. This date will be either the date of informed consent or just thereafter.
Was the patient a screening failure If the patient is a screening failure (see above Patient Study Number), then please indicate this here. Note that the panels 1, 2, 3 and 4 should be completed for screening failures.
2 INFORMED CONSENT
Enter the date the subject signed the consent form (dd mon yyyy).
Date of WIC should always be before any study related activity.
3 INCLUSION - EXCLUSION CRITERIA
Inclusion criteria All should be “Yes”; else this patient is a screening failure.
The patient should not be included if the answer to any of the inclusion criteria is NO, however for inclusion criteria 3.2a) and 3.2b) it is required that at least one should be YES.
Clarification inclusion criterion 2:
For criterion a) a left ventricular ejection fraction which was determined up to 24 months prior to enrolment, is acceptable for enrolment into the study.

BIOSTAT-CHF Page: 2 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
For criterion b) a BNP and/or NT-proBNP plasma level should be used only if it was determined during the hospitalization / outpatient clinic visit when the patient is intended to be enrolled into the study.
Clarification inclusion criterion 3:
40 mg furosemide is equivalent to 1 mg bumetanide and 10 mg torasemide
Clarification inclusion criterion 4:
ARB: Total daily dose of 320 mg Valsartan, respectively 32 mg Candesartan, is equivalent to 300 mg Irbesartan
A patient should not be included, if prior to inclusion it is already known that a patient does not tolerate higher doses of beta-blocker and/or ACEi/ARB, because this is not considered as anticipated uptitration.
Exclusion criteria All should be “No”; else this patient is a screening failure.
Inclusion and exclusion exceptions are not allowed and requests for waivers will not be granted.
If a inclusion and/or exclusion criterion has been violated, this has to be documented on the protocol deviation form.
4 DEMOGRAPHICS
4.1 Date of birth
4.2 Sex
4.3 Race Caucasian: A person having origins in any of the original peoples of Europe, the Middle East, or North Africa.
Asian: A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent, including, e.g. Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.
Black: A person having origins in any of the black racial groups of Africa.
Other: please specify.

BIOSTAT-CHF Page: 3 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
5 MEDICAL HISTORY: HEART FAILURE
5.1 Date of first diagnosis Heart Failure Enter month and year that the subject was first diagnosed with HF. If the qualifying episode was also the subject‟s first episode of HF, enter the month and year of the qualifying episode.
HF is diagnosed based on the ESC guideline definition of HF.
5.2 Aetiology assessed The primary aetiology of HF is the most likely primary cause of HF as assessed by the treating physician.
Ischemic heart disease
Ischemic heart disease defined as:
At least one major epicardial coronary artery with more than 70% obstruction by coronary angiography or patients has undergone PCI or CABG in history;
History of acute myocardial infarction;
Stress testing (with or without imaging) diagnostic of coronary artery disease.
Hypertension
Hypertension defined as any of the following:
History of hypertension diagnosed and treated with medication, diet, and/or exercise;
Blood pressure > 140 mm Hg systolic or 85 mm Hg diastolic on at least 3 occasions within a 24-hour time period;
Current use of antihypertensive pharmacological therapy to treat hypertension.
Cardiomyopathy
Cardiomyopathy defined as any chronic disease of the heart muscle (myocardium), in which the muscle is abnormally enlarged, thickened, and/or stiffened resulting in loss of ability to pump blood effectively.
Valvular disease Any condition of the heart valves that has caused HF.
Unknown aetiology Unknown aetiology should be used to indicate any cardiac failure that cannot be explained by above causes.
5.3 NYHA Class prior to decompensation or worsening HF
Select NYHA class or “NYHA class not assessed”. Use the usual NYHA status in the month prior to enrolment and decompensation / worsening HF:
Class I: patients with no limitation of activities; they suffer no symptoms from ordinary activities.
Class II: patients with slight, mild limitation of activity; they are comfortable with rest or with mild exertion.
Class III: patients with marked limitation of activity; they are comfortable only at rest.
Class IV: patients who should be at complete rest, confined to bed or chair; any physical activity brings on discomfort and symptoms occur at rest.
5.4 Previous Heart Failure hospitalisation(s) in last year

BIOSTAT-CHF Page: 4 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
6 CLINICAL HISTORY: CARDIOVASCULAR RISK FACTORS
6.1 Myocardial Infarction Select “Yes” for any documented history of MI.
6.2 Coronary Artery Bypass Graft (CABG) Select “Yes” for documented CABG in history, defined as bypass grafts of any coronary arteries (target or nontarget vessels).
6.3 Valvular Surgery Select “Yes” for documented surgery to any heart valve in history.
6.4 Percutaneous Coronary Intervention (PCI) Select “Yes” if PCI in history. Prior PCI includes balloon angioplasty, atherectomy, stent, or other percutaneous procedure.
6.5 Atrial Fibrillation Select “Yes” for current or history of atrial fibrillation/flutter defined as any prior diagnosis of atrial fibrillation or atrial flutter, even if transient/paroxysmal.
6.6 Stroke Select “Yes” for a cerebrovascular accident with loss of neurological function caused by an ischemic or hemorrhagic event with residual symptoms at least 24 hours after onset.
6.7 Peripheral Arterial Disease Select “Yes” for peripheral arterial vascular disease defined as clinically significant atherosclerosis of an extracoronary arterial bed including the carotids, vertebrals, subclavians, aorta, renal, ilio-fermoral, and distal extremities. PAD can include, but is not limited to, the following:
Claudication, either with exertion or at rest;
Amputation of arterial vascular insufficiency;
Vascular reconstruction, bypass surgery, or percutaneous intervention to the extremities;
Documented aortic aneurysm;
Positive non-invasive test (e.g. ankle brachial index < 0.8);
Radiologic evidence of 50% stenosis in an extracoronary arterial bed.
6.8 Device Therapy Select None, Pacemaker only, ICD only, Biventricular Pacer (CRT) only, Biventricular Pacer (CRT) and ICD or Other.
6.9 Hypertension Select “Yes” for hypertension defined as documentation of any of the following:
History of hypertension diagnosed and treated with medication, diet, and/or exercise;
Blood pressure > 140 mm Hg systolic or 85 mm Hg diastolic on at least 3 occasions within a 24-hour time period;
Current use of antihypertensive pharmacological therapy to treat hypertension.
6.10 Smoking Select 1 smoking status.
Current: Subject has smoked cigarettes within the 3 months
Past: Subject has stopped smoking more than 3 months prior to enrolling in the study
No: Subject has no history of cigarette smoking

BIOSTAT-CHF Page: 5 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
6.11 Current alcohol use?
If Yes, specify units / week 1 unit is equivalent to 1 glass of beer, wine or small glass of spirits.
6.12 Diabetes Select “Yes” for a history of diabetes (regardless of duration). Include subjects diagnosed with diabetes during the current admission. If “Yes”, check all disease-control methods (diet, insulin or oral anti-diabetic drugs) used.
6.13 Chronic Obstructive Pulmonary Disease (COPD)
Select “Yes” for a documented diagnosis of COPD.
6.14 Renal disease Select “Yes” for history of renal disease if eGFR<60 ml/min (4 factor MDRD).
6.15 Treated thyroid dysfunction
6.16 Current malignancy
7 FAMILY HISTORY
7.1 Family history of heart failure Select “No” or “Yes” if subject is aware of this, else choose unknown.
7.2 If Yes, specify: Select relationship to subject. Use Sibling 1 to indicate blood relationship with sibling with same father and mother, or Sibling 2 if only one blood related parent is shared.
You can choose multiple relatives
7.3 Family history of Angina/MI/CABG/PCI Select “No” or “Yes” if subject is aware of this, else choose unknown.
7.4 If Yes, specify: Select relationship to subject. Use Sibling 1 to indicate blood relationship with sibling with same father and mother, or Sibling 2 if only one blood related parent is shared.
You can choose multiple relatives
7.5 Family history of Hypertension Select “No” or “Yes” if subject is aware of this, else choose unknown.
7.6 If Yes, specify: Select relationship to subject. Use Sibling 1 to indicate blood relationship with sibling with same father and mother, or Sibling 2 if only one blood related parent is shared.
You can choose multiple relatives
7.7 Cause of the Heart Failure is a dilated cardiomyopathy?
Select “No” or “Yes”.
If Yes, does family history suggest that it is familial?
Select “No” or “Yes” if subject is aware of this, else choose unknown.

BIOSTAT-CHF Page: 6 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
8 PHYSICAL EXAMINATION
8.1 Height Height must be recorded in centimetres (cm). If conversion from inches is needed, the following conversion must be used cm = inches x 2.54
8.2 Body Weight Weight must be recorded in kilograms (kg). If conversion from Imperial pounds (lbs) is needed, the following conversion must be used kg = pounds / 2.2
8.3 Heart rate Heart rate should be measured lying down (or taken from an ECG where patient is lying flat).
8.4 Blood Pressure BP should be measured with the BP cuff at the same level as the heart. Patient may be either sitting or lying down.
8.5 Auscultation performed?
8.5.1 Pulmonary congestion/oedema with rales/crackles?
Indicate where the rales / crackles can be auscultated, if at all.
8.6 Peripheral oedema assessed? If the oedema assesment was performed but the patients does not have oedema, indicate yes for the assessment (8.6) and fill in „Not present‟ for item 8.6.1 in the eCRF
8.6.1 Extent of peripheral oedema Indicate to which height the oedema extends.
8.7 Jugular venous pressure assessed?
8.7.1 Elevated JVP JVP is estimated by positioning the head of a supine patient at a 30- to 45-degree angle and observing the neck veins. If the neck veins are filled only to a point a few millimetres above the clavicle at the end of exhalation, JVP is usually normal. With an elevated JVP the neck veins may be distended as high as the angle of the jaw.
8.8 Haepatomegaly
8.9 3rd
heart tone Extra heart tone soon after S1 and S2.
9 SYMPTOMS OF HEART FAILURE
9.1 Was NYHA classification performed during this visit?
9.1.1 NYHA class Class I: patients with no limitation of activities; they suffer no symptoms from ordinary activities.
Class II: patients with slight, mild limitation of activity; they are comfortable with rest or with mild exertion.
Class III: patients with marked limitation of activity; they are comfortable only at rest.
Class IV: patients who should be at complete rest, confined to bed or chair; any physical activity brings on discomfort and symptoms occur at rest.

BIOSTAT-CHF Page: 7 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
9.2 Did the patient complete the Dyspnoea VAS?
9.2.1 Please fill out score Use a VAS score between 0 – 100.
9.3 Orthopnoea present?
10 INPATIENT HOSPITALIZATION / OUTPATIENT CLINIC
10.1 Date of hospitalisation / outpatient clinic visit
10.2 Type of visit
10.3 Reason for hospitalisation / outpatient clinic visit
If Other reason, then specify If other reason, please verify that the patient is eligible according to the inclusion criteria.
10.4 Precipitating factors for this hospitalisation / outpatient clinic visit?
If Yes, specify: For precipitating factors, use Present if can be confirmed. Use Absent if can be ruled out. Use Not Certain if not able to confirm, but cannot be ruled out.
(UseOther only if you can specify it)
10.5 Parenteral support during hospitalisation / outpatient clinic visit?
Select “No” or “Yes” and if yes, select which.
If this is an inpatient hospitalisation, then the following section should be completed:
10.5.1 Dobutamine
10.5.2 Levosimendan
10.5.3 Milrinone, Enoximone
10.5.4 Dopamine
10.5.5 Noradrenaline
10.5.6 Nitrates i.v.
10.5.7 Diuretics i.v.
If the patient has received bolus at admission and is then put on a continuous infusion, please fill out continuous infusion in the eCRF. Bolus can be filled out if the patient has only received bolus (and no continuous infusion).
10.5.8 Date discharge / death Indicate the date patient was discharged from hospital, or deceased.
10.5.9 Patient deceased during hospitalization
If the patient dies during the hospitalization following inclusion into the study, an event form should be completed to capture full details of the death.
10.6 Hospital presentation, clinical profiles: Based on the ESC guideline
10.6.1 Pulmonary oedema
10.6.2 Cardiogenic shock

BIOSTAT-CHF Page: 8 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
10.6.3 Decompensated chronic HF
10.6.4 Hypertensive HF
10.6.5 Right HF
10.6.6 Acute coronary syndrome
11 ELECTROCARDIOGRAM (ECG)
11.1 Was an ECG performed? Select “No” or “Yes”. 12 lead ECG should be performed with patient lying down.
11.2 Date of ECG
11.3 Heart rate
11.4 Rhythm
11.5 QRS-duration QRS is measured from the initial deflection of the QRS from the isoelectric line to the end of the QRS complex.
11.6 RBBB
11.7 LBBB
11.8 LVH
11.9 Crude QT length There are differences in presentation of the Crude QT length on ECG print-outs. Please ensure that the “crude” QT is used and not e.g. the “corrected” QT.
12 CHEST X-RAY
This examination may have been done as part of routine clinical care before BIOSTAT. It is not performed specifically for BIOSTAT. If this examination has been done within 3 months before or 3 months after the first visit of BIOSTAT , then the most recent data, i.e. closest to the date of enrolment is recorded.
12.1 Was a chest x-ray performed?
12.2 Date of chest x-ray
12.3 Upper lobe venous congestion
12.4 Pulmonary oedema Any significant fluid in the alveolar walls.
12.5 Cardiomegaly (defined as CTR > 0.5) Defined as CTR > 0.5

BIOSTAT-CHF Page: 9 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
13 ECHOCARDIOGRAM
This examination may have been done as part of routine clinical care before BIOSTAT. It is not performed specifically for BIOSTAT. If this examination has been done within 24 months before or 3 months after the first visit of BIOSTAT , then the most recent data, i.e. closest to the date of enrolment is recorded.
13.1 Was an echocardiogram performed?
13.2 Date of echocardiogram
13.3 Left ventricular ejection fraction (LVEF) Both Simpson and Eyeballing allowed. Unit is %.
If a range of the LVEF is available, the mean value of the range is recorded (e.g 20-25% will be entered as 23%).
If LVEF was assessed only qualitatively (good/moderate/poor), you can leave this field empty and record the qualitative assessment in the next field.
If WMSI has been assessed instead of LVEF, please use the table below for conversion:
WMSI LVEF
1.50 45% 1.53 44 1.57 43 1.60 42 1.63 41 1.67 40 1.70 39 1.73 38 1.77 37 1.80 36 1.83 35 1.87 34 1.90 33 1.93 32 1.97 31 2.00 30 2.03 29 2.07 28 2.10 27 2.13 26 2.17 25 2.20 24 2.23 23 2.27 22 2.30 21 2.33 20 2.37 19 2.40 18 2.43 17 2.47 16 2.50 15
13.4 LVEF – Qualitative assessment Qualitative assessment of the LVEF, expressed as Good, Moderate or Poor. (not the quality of the images, but quality of the LV function)
If LVEF was assessed only quantatively (in percentages), you

BIOSTAT-CHF Page: 10 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
can leave this field empty and fill in the percentage in the previous field
13.5 Left ventricular end diastolic diameter (LVEDD)
13.6 Left ventricular end systolic diameter (LVESD)
13.7 Interventricular wall thickness
13.8 Posterior wall thickness
13.9 Left atrial diameter (parasternal long axis view)
13.10 Mitral valve regurgitation (moderate-severe)
13.11 E/A ratio
13.12 Tissue velocity (E‟ as mean from septal and lateral wall)
Preferably E‟ as mean from septal and lateral wall, but if not available then mean from all 4 walls should be used.
13.13 Type assessment tissue velocity
14 6 MINUTES WALKING TEST (6MWT)
Please refer to the 6MWT protocol. Only the total distance walked is recorded.
If “did the patient complete the 6MWT?” is no, then nevertheless the total distance should be recorded.
In some cases the 6MWT cannot be performed because of medical reasons. If this is the case, the not performing of the test is not regarded a protocol violation and the eCRF should be completed as indicated below:
- Was the 6 minutes walking test (6MWT) performed? Response: Yes - Date of planned test? Response: date test would have been performed. - Did the patient complete the 6MWT? Response: No - Meters? Response: 0 meters Please be informed that this is only the case for patients where the site is planning the 6MWT, and also if the patient does want to perform the test, however it cannot be performed because of medical reasons. If for example the site forgets to perform the test this is regarded a protocol violation, because the 6MWT is obliged for the protocol.
15 EQ5D
Please refer to the EQ5D user guide.
16 KCCQ
Please refer to the “Annotated KCCQ” (Annex 1) for instruction on how to enter the questionnaire in the eCRF.
IMPORTANT: Note that the answering options are not always predictable. Look closely into the options to choose the correct value!

BIOSTAT-CHF Page: 11 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
Unanswered questions have to be recorded as ND which can be chosen from the dropdown codelist.
17 CORONARY ANGIOGRAPY
This examination may have been done as part of routine clinical care before BIOSTAT. It is not performed specifically for BIOSTAT. If this examination has been done within 3 months before or 3 months after the first visit of BIOSTAT , then the most recent data, i.e. closest to the date of enrolment, is recorded.
17.1 Was a Coronary Angiography performed?
17.2 Date of Coronary Angiography
17.3 Number of vessels with critical stenosis (≥70%)
Critical stenosis defined as ≥70% stenosis of any of the coronary arteries.
18 RIGHT HEART CATHETERIZATION
This examination may have been done as part of routine clinical care before BIOSTAT. It is not performed specifically for BIOSTAT. If this examination has been done within 3 months before or 3 months after the first visit of BIOSTAT , then the most recent data, i.e. closest to the date of enrolment, is recorded.
18.1 Was a right heart catherization performed?
18.2 Date of right heart catherization
18.3 Pulmonary artery pressure
18.4 Right atrial pressure
18.5 Pulmonary capillary wedge pressure
18.6 Pulmonary resistance
18.7 Systemic vascular resistance
18.8 Cardiac index
19 ROUTINE LABORATORY ANALYSES
This examination may have been done as part of routine clinical care before BIOSTAT. It is not performed specifically for BIOSTAT. If this examination has been done within 3 months before or 3 months after the first visit of BIOSTAT , then the most recent data, i.e. closest to the date of enrolment, is recorded.
If a laboratory value has been reported as i.e. „<0.01‟ the „<‟ can be entered in the eCRFby selecting the „=‟ and click the magnifying glass. A list of values will become available. Here you can choose „<‟ or „>‟ .
20 SAMPLES FOR CENTRAL ANALYSIS
Record the time that the patient last ate.
The timing of the samples, and whether there were any deviations from the collection protocol during sampling procedure should be noted here. Please ensure that you record these data and note them down accurately.

BIOSTAT-CHF Page: 12 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
21 PATIENT MANAGEMENT
21.1 Were ACEi/ARBs initiated / up-titrated according to ESC guidelines?
Indicate “Yes” if treatment with ACEi/ARBs was initiated or up-titrated.
For patients that are not up-titrated because of complaints indicate “No” (although this is indeed according to guidelines) and specify at 21.1.2 the reason why this was not done.
A patient should not be included, if prior to inclusion it is already known that a patient does not tolerate higher doses of ACEi/ARB, because this is not considered as anticipated uptitration.
21.1.1 If Yes, please specify date / time Record date/time of first dose, or increase in dose of ACEi/ARBs. Please record the time of actual intake, not the time of prescription.
21.1.2 If No, please specify reason Provide reason for not initiating or up-titrating the ACEi/ARBs.
When initiation / up-titration was ANTICIPATED, please state this in your explanation.
21.2 Were beta-blockers initiated / up-titrated according to ESC guidelines?
Indicate “Yes” if treatment with betablockers was initiated or up-titrated.
For patients that are not up titrated because of complaints indicate “No” (although this is indeed according to guidelines) and specify at 21.1.2 the reason why this was not done.
A patient should not be included, if prior to inclusion it is already known that a patient does not tolerate higher doses of beta-blocker, because this is not considered as anticipated uptitration.
21.2.1 If Yes, please specify date / time Record date/time of first increase in dose of beta-blockers. Please record the time of actual intake, not the time of prescription.
21.2.2 If No, please specify reason Provide reason for not initiating or up-titrating the beta-blockers.
When initiation / up-titration was ANTICIPATED, please state this in your explanation
22 CONCOMITANT MEDICATION
Record only the concomitant medication that was used at time of Written Informed Consent.
For concomitant medication (NOT ACEi, ARBs and Beta-Blockers as these are recorded in the study medication panel) generic names are preferred. Use trade name only when the generic name is unknown.
For compound drugs (drug containing more than one generic drug) different generic drug names and details are recorded separately.
Unit/Frequency/Route are all three coded, if you select the corresponding field, a magnifying glass will appear. If you click this, a list will appear with all available codes for resp unit (e.g.mg), frequencies (e.g. BID) and routes (e.g. PO). If a code is not available, you can leave the field empty, in which case a query will come up where you can record the

BIOSTAT-CHF Page: 13 of 15
VISIT 1
CRF Completion Guidelines March 23rd, 2012. V1.2.2
desired text. Data Management will deal with it.
For concomitant medication where more than one dose is used enter PRN for frequency and for dose NA (e.g. for Sintrom as it is based on the INR and is different every time).
New entries must be made for any medications with a change in total daily dose. Please make sure the end-date of the first record matches, but does not overlap the start-date of the new record and that you use the identical medication name.

BIOSTAT-CHF Page: 14 of 15
9 Month visit
CRF Completion Guidelines March 23rd, 2012. V1.2.2
23 9 MONTH VISIT
Treatment of patients is expected to be optimized after 3 months, after which a 6 months stabilisation phase will follow At 9 months after baseline, a second visit is scheduled. At this 9 months visit the second blood and urine samples are obtained. A physical examination is done and the signs and symptoms of HF are recorded. An ECG is done.
If an echocardiograph, a chest x-ray, a cardio angiography or right heart catheterization is done (or was done in the prior 3 months), then the data is recorded as well.
In general, record the examination which is closest to the date of month 9 visit. The examination should have been performed within the period after enrolment and on the date or before the date of the month 9 visit.
For definitions of panels 24 - 35, please refer to baseline visit 1.
24 PATIENT MANAGEMENT
24.1 Has the patient been up-titrated according to ESC guidelines up until this visit?
Patient is either on optimal doses or maximum tolerable doses of ACEi/ARB and beta-blocker.
24.1.1 If No, please specify reason If no, try to record as exact as possible, the reason why the patient was not treated according to guidelines
24.2 Any hospitalizations since previous visit For any hospitalization an Event Form should be completed, regardless of the cause of the hospitalization.
24.3 Please specify number of hospitalizations Total number of hospitalizations since discharge from the initial hospitalization or outpatient clinic visit in the study.
24.4 Patient deceased since previous contact In case of death, an Event Form should be completed specifying the details surrounding the patient‟s death.
25 PHYSICAL EXAMINATION
26 SYMPTOMS OF HEART FAILURE
27 ELECTROCARDIOGRAM (ECG)
28 CHEST X-RAY
This examination at the 9 months visit may have been done as part of routine clinical care. It is not performed specifically for BIOSTAT. If this examination has been done within 9 months before the 9-months visit of BIOSTAT, results can be recorded here. (But do not record the same results as at screenings visit!)
29 ECHOCARDIOGRAM
This examination at the 9 months visit may have been done as part of routine clinical care. It is not performed specifically for BIOSTAT. If this examination has been done within 9 months before the 9-months visit of BIOSTAT, results can be recorded here. (But do not record the same results as at screenings visit!)
30 6 MINUTES WALKING TEST (6MWT)
31 EQ5D
32 KCCQ
33 CORONARY ANGIOGRAPY
This examination at the 9 months visit may have been done as part of routine clinical care. It is not performed specifically for BIOSTAT. If this examination has been done within 9 months before the 9-months visit of BIOSTAT, results can be recorded here. (But do not record the same results as at screenings visit!)

BIOSTAT-CHF Page: 15 of 15
9 Month visit
CRF Completion Guidelines March 23rd, 2012. V1.2.2
34 RIGHT HEART CATHETERIZATION
This examination at the 9 months visit may have been done as part of routine clinical care. It is not performed specifically for BIOSTAT. If this examination has been done within 9 months before the 9-months visit of BIOSTAT , results can be recorded here. (But do not record the same results as at screenings visit!)
35 ROUTINE LABORATORY ANALYSES
Laboratory analyses may have been done as part of routine clinical care. It is not performed specifically for BIOSTAT. If lab results are available from the 9 months period before the 9-months visit of BIOSTAT , results can be recorded here. (But do not record the same results as at screenings visit!)
36 SAMPLES FOR CENTRAL ANALYSIS
37 CONCOMITANT MEDICATION
Record only the concomitant medication that was used at time of the 9-month visit
For further instruction see visit 1
For definitions of panels 24 - 37, please refer to baseline visit 1.

BIOSTAT-CHF Page: 16 of 15
Follow-up visit / Every 6 months
CRF Completion Guidelines March 23rd, 2012. V1.2.2
38 FOLLOW-UP VISIT / CONTACT EVERY 6 MONTHS (REPEATING VISIT)
Patients will be contacted throughout the study every 6 months to record any changes in concomitant medication and to ensure all deaths and hospitalisations are captured. The follow-up contact can be performed by telephone. If patient is already anticipated to visit the clinic as part of routine HF follow-up then this can be combined.
The last contact for the study with all patients will be in the period between February 2014 and April 2014. Final data on concomitant medication and hospitalisations / death will be collected at that time.
38.1 Date of this visit / contact
38.2 Type of contact
38.3 Any hospitalizations since previous study contact
38.4 Please specify number of hospitalizations
38.5 Patient deceased since previous contact

BIOSTAT-CHF Page: 17 of 15
Medication and End of Study
CRF Completion Guidelines March 23rd, 2012. V1.2.2
STUDY MEDICATION / ACEI / ARBS AND BETA BLOCKERS
Any ACEi, ARB or Beta-Blocker used within the three months prior to the study should also be recorded on these pages.
For concomitant medication other than the ACEi, ARBs and Beta-Blockers . please use the concommitant medication page at the relevant visit
For compound drugs (drug containing more than one generic drug) different generic drug names and details are recorded separately.
For Study medication the total daily dose is recorded
New entries must be made for any medications with a change in total daily dose. Please make sure the end-date of the first record matches, but does not overlap the start-date of the new record and that you use the identical medication name.
Stop date is recorded OR tick box can be ticked for “Ongoing at end of study”
For Study medication, reasons for changing the medication must be given as soon as the stopdate for that record is filled in..
For Study medication, reasons for changing the medication must be given as soon as the stopdate for that record is filled in.
1=Non optimal dose acc. to ESC guidelines Use this reason if the dose was increased according to the ECS guidelines (i.e. uptitration after 2-4 weeks) because the optimal dose was not yet reached
2=Symptoms, use this reason if the dose was increased faster that the guidelines indicate
3=Side effects, use this reason if the dose was not increased according to the ECS guidelines because of side effects of the treatment,
4=Non-cardiac organ dysfunction, use this reason if the dose was not increased according to the ECS guidelines because of organ dysfunction other than the heart,
99=Other, specify Use correct spelling and common medical abbreviations only.

BIOSTAT-CHF Page: 18 of 15
Medication and End of Study
CRF Completion Guidelines March 23rd, 2012. V1.2.2
END OF STUDY
Did patient discontinue the study prematurely?
If Yes, Date study termination The date used here should reflect the date when the last data from the patient is available.
If patient did not complete the study, one primary reason for discontinuation must be checked.
CONCOMITANT MEDICATION
Record only those concomitant medication that was used at end of study OR at time of death
For further instruction see visit 1

BIOSTAT-CHF
ANNEX I: KCCQ
CRF Completion Guidelines April 1st, 2011. V1.1.1





BIOSTAT-CHF
ANNEX II: Event Form
CRF Completion Guidelines March 23rd, 2012. V1.2.2
EVENT FORM
How to complete the Event form when a patient is hospitalized and/or dies during the hospitalization.
Please find below an overview of different situations and the consequences for the Event form:
When a patient is hospitalized you can only complete the event form after you know the outcome. For example:
if the patient is discharged: Event = hospitalization complete the hospitalization questions of the event form + narratives (for hospitalization in the eCRF)
if the patient dies during the hospitalization: Event = death complete death questions of the event form + narratives (for Death in the eCRF) + fill out questions in the event form regarding the hospitalization
However if a patient dies during the hospitalization at screening (so if the patient is included during a hospitalization) and the patient dies (so the patient was not discharged) you do not have to complete the hospitalization questions of the Event form because these are already captured in the CRF questions at baseline, so it is not necessary to repeat this.
If patient dies during the same hospitalization in which the patient was included: Event = Death complete questions about death + narratives (for Death in eCRF)
If a patient is not hospitalized and dies:
If a patient dies without hospitalization: Event = Death complete questions about death + narratives (for Death in the eCRF)

Form EVENT ADJUDICATION INSTRUCTIONS
Project name and number 2009015 BIOSTAT-CHF v0.1
Version 1.0.0 Date created 18 March 2011 Author Marco Metra
©TCC (tcc.umcg.nl) Page 1 of 2
Definition of Endpoints for Adjudication 1. Death
Deaths are classified as: cardiovascular, non-cardiovascular, or unknown.
1.1 Cardiovascular death Cardiovascular deaths comprises the following: • sudden cardiac death (SCD), • Heart Failure (HF) death, • acute myocardial infarction (MI), • stroke, • other cardiovascular Definitions are shown below. 1.1.1. SCD An unexpected death in a previously stable patient with recent human contact. This definition includes subjectswho are comatose and then die after attempted resuscitation. Subjects in this category should have had recenthuman contact before the event 1.1.2 HF death A death involving a substantive worsening of HF symptoms and/or signs resulting in augmentation or additionof HF therapies. 1.1.3. Acute MI Death occurring after a hospital-verified, definite acute MI, or if the death was outside the hospital, with autopsyfindings showing a recent MI or recent occluding coronary thrombus. 1.1.4 Stroke death Persistent abnormalities of focal neurologic function resulting in symptoms thought to be due to thromboticcerebral infarction, embolus, or hemorrhage based on history, physical, imaging techniques, and/or autopsydata. 1.1.5 Other cardiovascular death Any other vascular death that does not fit into the above criteria.
1.2 Other non cardiovascular Any death that does not fit into criteria above, except when cause of death is unknown.
1.3 Unknown A death in which no information is available. The databases will be queried for any hospitalization dates in recent proximity to the death that may help in presuming a cause of death. Investigators will be encouraged toinquire to primary care or other health care providers that may have treated the patient in close proximity totheir death. Unknown will only be utilized in the rare case that no information can be obtained surrounding thedeath.

Form EVENT ADJUDICATION INSTRUCTIONS
Project name and number 2009015 BIOSTAT-CHF v0.1
Version 1.0.0 Date created 18 March 2011 Author Marco Metra
©TCC (tcc.umcg.nl) Page 2 of 2
2. Hospitalization Classification of the cause of hospitalization will be based on the primary reason for which the subject wasadmitted. A hospitalization is defined as a non-elective hospital admission for medical therapy lasting more than onecalendar day. Hospitalization that is ongoing at the time of inclusion will not be adjudicated as a study endpoint.If a hospitalization occurs on the same calendar day as death, only the death will be adjudicated.
2.1 Heart Failure hospitalization A heart failure hospitalization requires that all 3 criteria are met:
1. The primary reason for hospitalization was worsening of the signs or symptoms of heart failure 2. The subject required intravenous medications, i.e., diuretics, inotropic agents, vasodilators for the
treatment of heart failure or an increase of the dose of an oral diuretic 3. Admission lasting more than 1 calendar day (overnight or longer), to hospital.
2.2 Other cardiac, non HF hospitalization
An event that is cardiac in origin but does not meet the criteria for HF. This includes arrhythmias and acutecoronary syndromes, as the most likely, more common cases.
2.3 Other vascular hospitalization An event that is vascular in origin but does not meet the criteria for HF, arrhythmias, acute coronary syndrome.This includes hospitalizations for stroke, peripheral embolism, pulmonary embolism.
2.4 Hospitalization for renal dysfunction Hospitalization will be classified as due to renal cause when the reason for admission is due to signs, symptomsor laboratory abnormalities directly related to renal dysfunction as primary cause and therapeutic interventionsare primarily directed toward improving renal function.
2.5 Non-Cardiovascular hospitalization A hospitalization that does not fit into criteria as provided in 2.1 — 2.4.
3. Hospitalization Equivalent Subjects entering hospice or end of life care will be considered equivalent to being hospitalized and the numberof days the subject is in hospice or end of life care will count as days hospitalized. Patients who are in or referredto nursing home or assisted living facilities do not qualify as a hospitalization equivalent event.