Embed Size (px)
Citation preview
排尿障礙治療中心 版權所有
Conservative Treatment of Stress Urinary Incontinence
Hann-Chorng Kuo. M.D.Department of Urology
Buddhist Tzu Chi General Hospital, Hualien, Taiwan
排尿障礙治療中心 版權所有
Pathophysiology of Stress urinary incontinence Intrinsic sphincteric deficiencyIntrinsic sphincteric deficiency Defects in extrinsic continence mechanismDefects in extrinsic continence mechanism
Defects of attachments to archus tendineus fascia pelvisDefects of attachments to archus tendineus fascia pelvis
Defects of attachments to levator aniDefects of attachments to levator ani
Damage or degenerative change of endopelvic fasciaDamage or degenerative change of endopelvic fascia
Pelvic floor muscle relaxationPelvic floor muscle relaxation
Damage of anococcygeal ligamentsDamage of anococcygeal ligaments Urethrovesical facilitative reflex (detrusor overactivity ?)Urethrovesical facilitative reflex (detrusor overactivity ?)

排尿障礙治療中心 版權所有
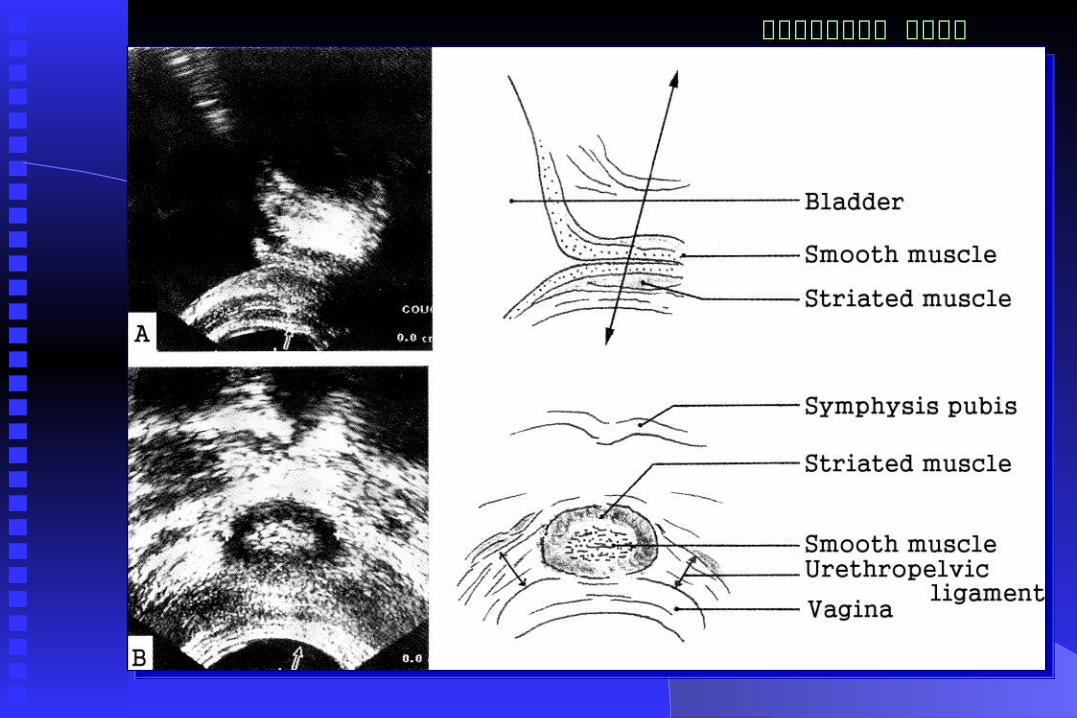
Damage of continence mechanism
排尿障礙治療中心 版權所有
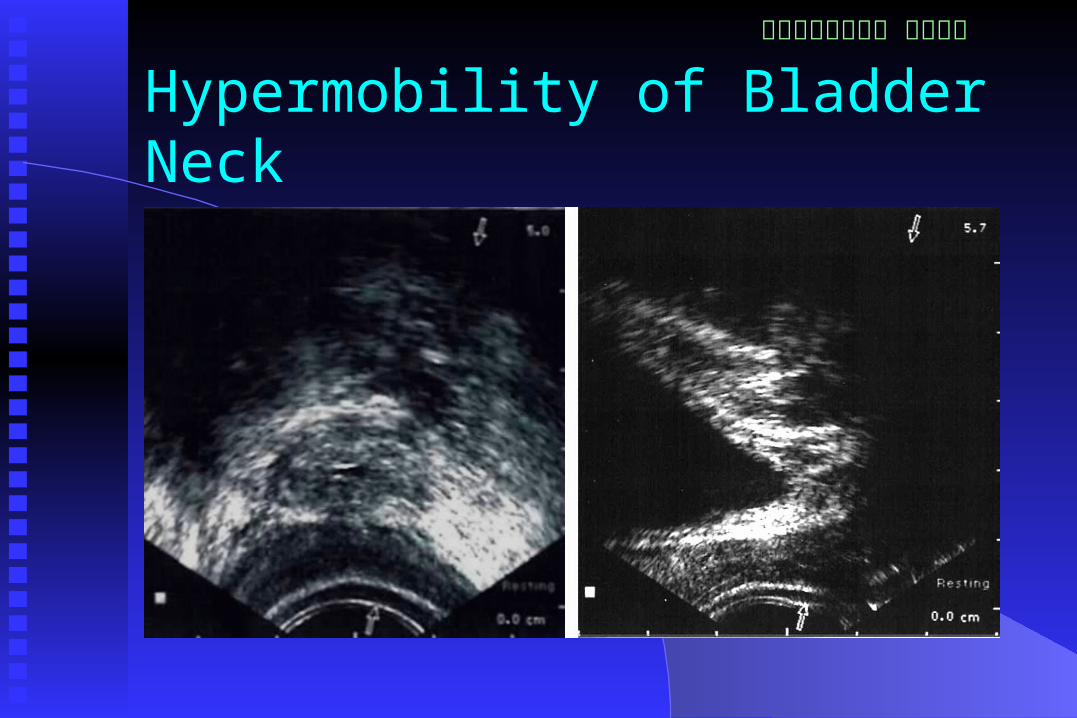
Hypermobility of Bladder Neck
排尿障礙治療中心 版權所有
Factors Influencing Continence
Bladder neckBladder neck Urethral smooth muscleUrethral smooth muscle External urethral sphincterExternal urethral sphincter Pelvic floor musculaturesPelvic floor musculatures Connective tissue and collagenConnective tissue and collagen Intact neurological innervationIntact neurological innervation

排尿障礙治療中心 版權所有
Conservative management of Stress incontinence Weight reductionWeight reduction Stop smokingStop smoking Reduced caffeine intakeReduced caffeine intake Decrease fluid intakeDecrease fluid intake Resolving chronic straining and constipationResolving chronic straining and constipation Prevent heavy exertion or exercisePrevent heavy exertion or exercise
排尿障礙治療中心 版權所有
Physical Therapies for Stress Incontinence
Bladder retraining
Pelvic floor muscle exercises
Vaginal cones
Biofeedback
Functional electrical stimulation
排尿障礙治療中心 版權所有
Pelvic floor muscle training (PFMT)
Kegel 1948Kegel 1948 Effective PFM contractions increase urethral resistEffective PFM contractions increase urethral resist
ance, increase activated motor units, frequency of eance, increase activated motor units, frequency of excitation, and muscle volumexcitation, and muscle volume
Repeat PFMT may reflexly inhibit detrusor contracRepeat PFMT may reflexly inhibit detrusor contractionstions
Successful PFMT depends on ability to perform a cSuccessful PFMT depends on ability to perform a correct contraction, 50% women failed to do PFMTorrect contraction, 50% women failed to do PFMT

排尿障礙治療中心 版權所有
ICS recommendedIdeal PFMT Program
Three sets of 8 to 12 slow velocity
maximal contractions
Sustained for 6 to 8 seconds each
Performed 3 to 4 times a week
Continued for at least 15 to 20 weeks

排尿障礙治療中心 版權所有
Correct PMF contraction
Co-contraction of related muscles should be Co-contraction of related muscles should be discourageddiscouraged
Use of voluntary PFMC prior to anticipated Use of voluntary PFMC prior to anticipated increased intra-abdominal pressureincreased intra-abdominal pressure
Near maximal contractions are the most Near maximal contractions are the most significant factor in increasing strengthsignificant factor in increasing strength
Prevent muscle fatigue with vigorous exercisePrevent muscle fatigue with vigorous exercise Assessed by a specialist for correct PFMCAssessed by a specialist for correct PFMC

排尿障礙治療中心 版權所有
Effects of PFMT in Incontinence
A meta-analysis of 10 studies concluded A meta-analysis of 10 studies concluded improvement ranges from 61 to 85%improvement ranges from 61 to 85%
Cure ranges from3 to 38%Cure ranges from3 to 38% Severity of urine loss decreases by 61 to 82% in Severity of urine loss decreases by 61 to 82% in
women who leaks after PFMTwomen who leaks after PFMT In 23 women with repeat training for 5 years, 14 In 23 women with repeat training for 5 years, 14
were satisfied with current condition, 15 were were satisfied with current condition, 15 were continent, a high durability was notedcontinent, a high durability was noted
排尿障礙治療中心 版權所有
Combination of PFMT with other Physical therapies For a woman with stress, urge, and mixed incontinence, For a woman with stress, urge, and mixed incontinence,
PFMT is better than no treatmentPFMT is better than no treatment Combined PFMT with electrical stimulationCombined PFMT with electrical stimulation PFMT with biofeedbackPFMT with biofeedback PFMT with intravaginal resistance devisesPFMT with intravaginal resistance devises No consistent data proves that combination therapies are No consistent data proves that combination therapies are
better than PFMT alone, but can be used as an initial traibetter than PFMT alone, but can be used as an initial training for women who cannot perform VPFCning for women who cannot perform VPFC

排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
Effects of Conservative Treatment
Increased maximal cystometric capacity Fewer detrusor contractions Less incontinence episodes Expected cure/improvement rates 65-75% About 50% of patients avoid surgery

排尿障礙治療中心 版權所有
Predictive Factors for a Successful Physiotherapy
Low patient age and presence of estrogen Absence of detrusor instability Absence of intrinsic sphincteric deficiency Low urethral hypermobility Good compliance with treatment

排尿障礙治療中心 版權所有
Postulated Physiological Changes after PFMT
Press urethra against pubis symphysis Increase activated motor units and muscle
volume Build a structural support for urethra Reflexic inhibition of detrusor contractions
排尿障礙治療中心 版權所有
Reported Urodynamic Findings in PFMT Increased in MUCP (Wilson 1987, Bo 1990, Elia 199
3) Increased in MUCP and FPL (Benevenuti 1987) No changes in MUCP or FPL (Ferguson 1990, Meye
r 1992, Burns 1993) No changes in all urodynamic parameters (McClis
h 1991, Elser 1999)

排尿障礙治療中心 版權所有
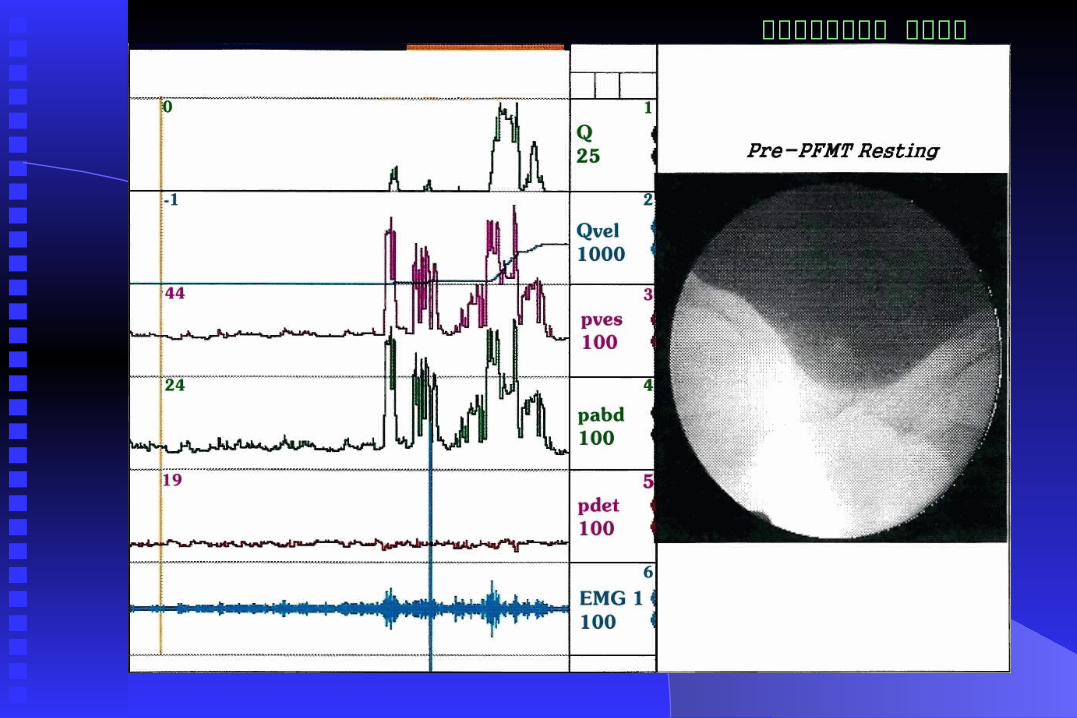
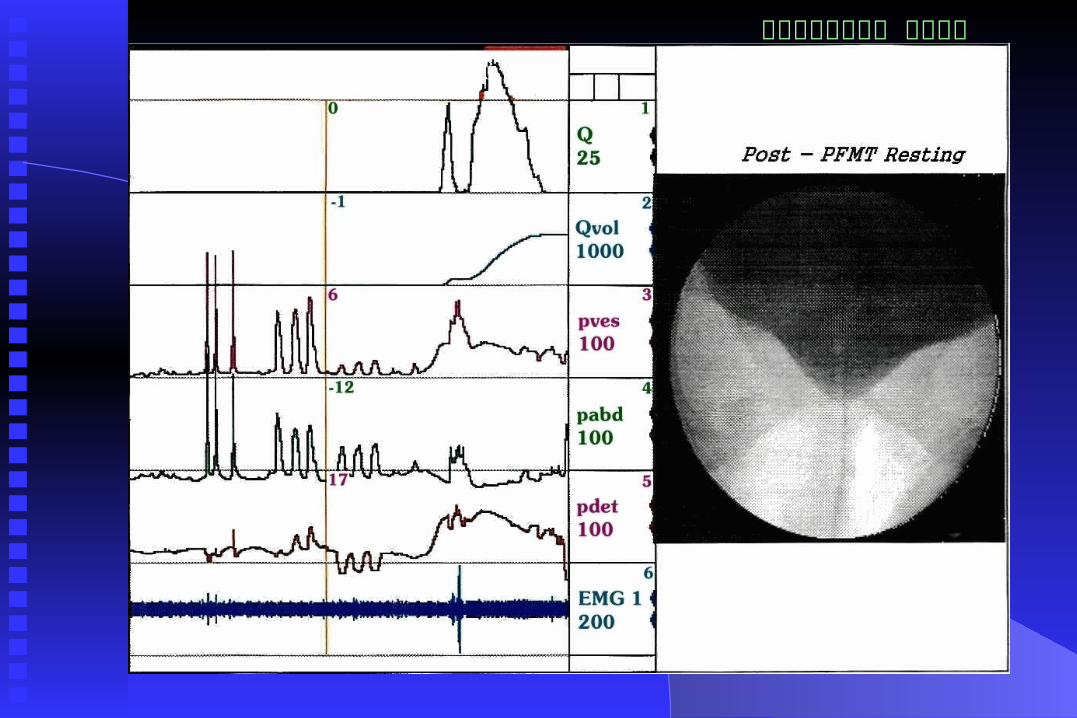
Videourodynamics in Evaluation of PFMT Determine abdominal leak point pressure
Measure bladder base descent during
straining
Measure bladder base elevation during PME
Educate patient to perform an effective PME
排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
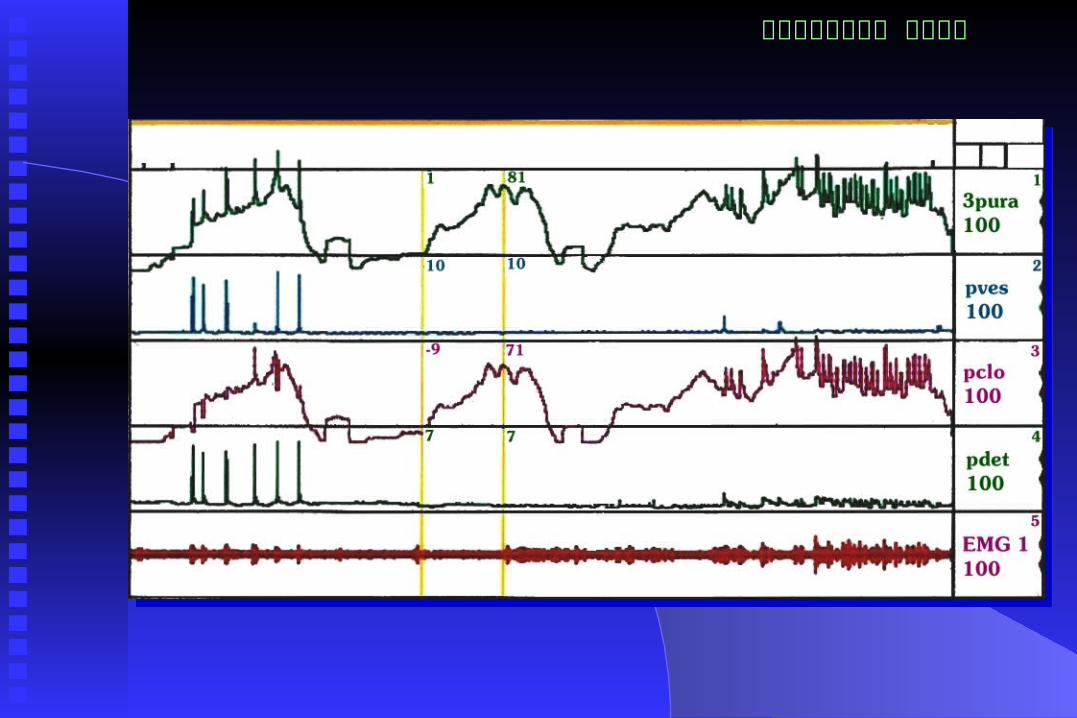
Dynamic Urethral Pressure Profilometry Resting UPP – Maximal urethral closure press
ure – Functional profile length
Stress UPP – Pressure transmission ratio PFMT UPP – Maximal pelvic floor muscle
contractions Concomitant recording Pves and Pabd

排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
陰道壓力儀

排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
Materials and Methods
40 women with GSI with/out frequency urgency Gr. 3 or 4 cystocele and pure ISD were excluded Structured 12-week PFMT with biofeedback Videourodynamic study and UPP study Abdominal leak point pressure determination Compare the parameters between successful and
failed treatment groups

排尿障礙治療中心 版權所有
PFMT Program
A 12- week structured treatment course
Performed by a trained nurse specialist
Involve a gradual home exercise and 6 office biofeedback sessions
15 sustained 10-second contractions, 3 timed daily
Results assessed by subjective satisfaction and improvement rate

排尿障礙治療中心 版權所有
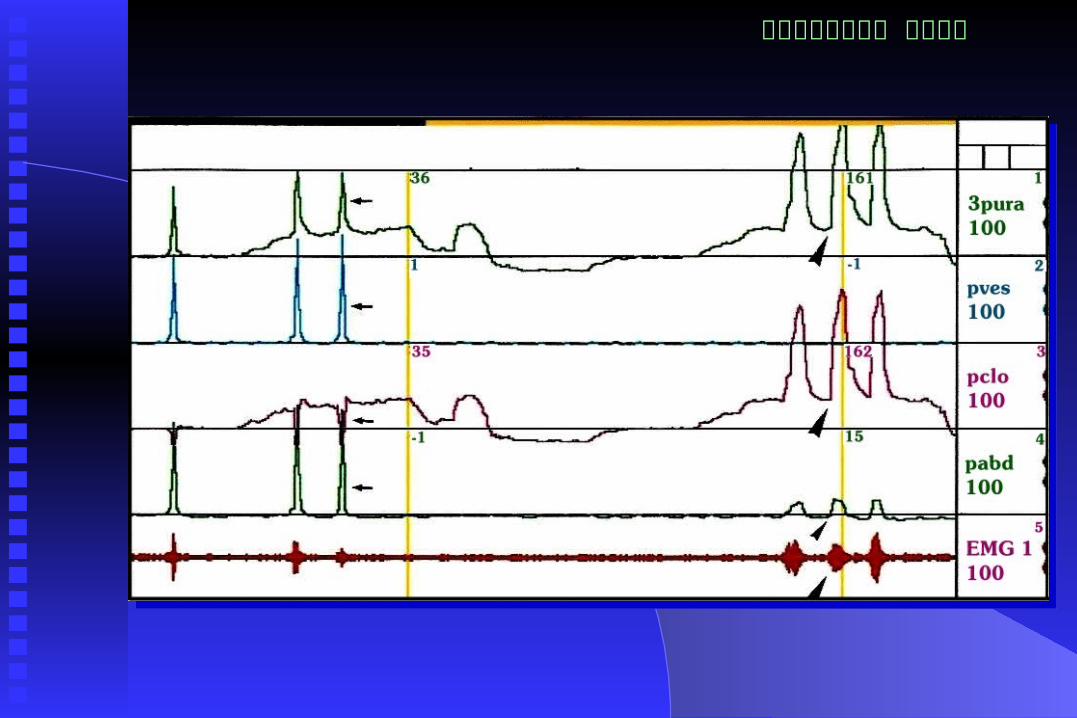
Abdominal Muscle EMG Recording

排尿障礙治療中心 版權所有
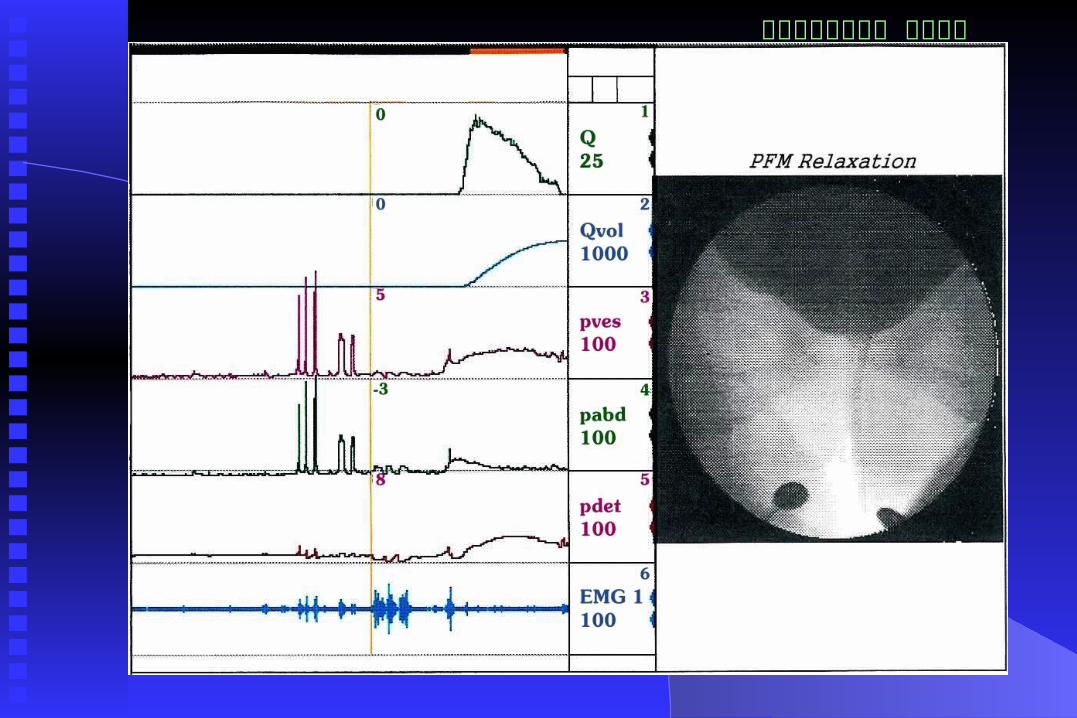
Correct Pelvic Floor Muscle Contractions No Abdominal muscle contractions
排尿障礙治療中心 版權所有
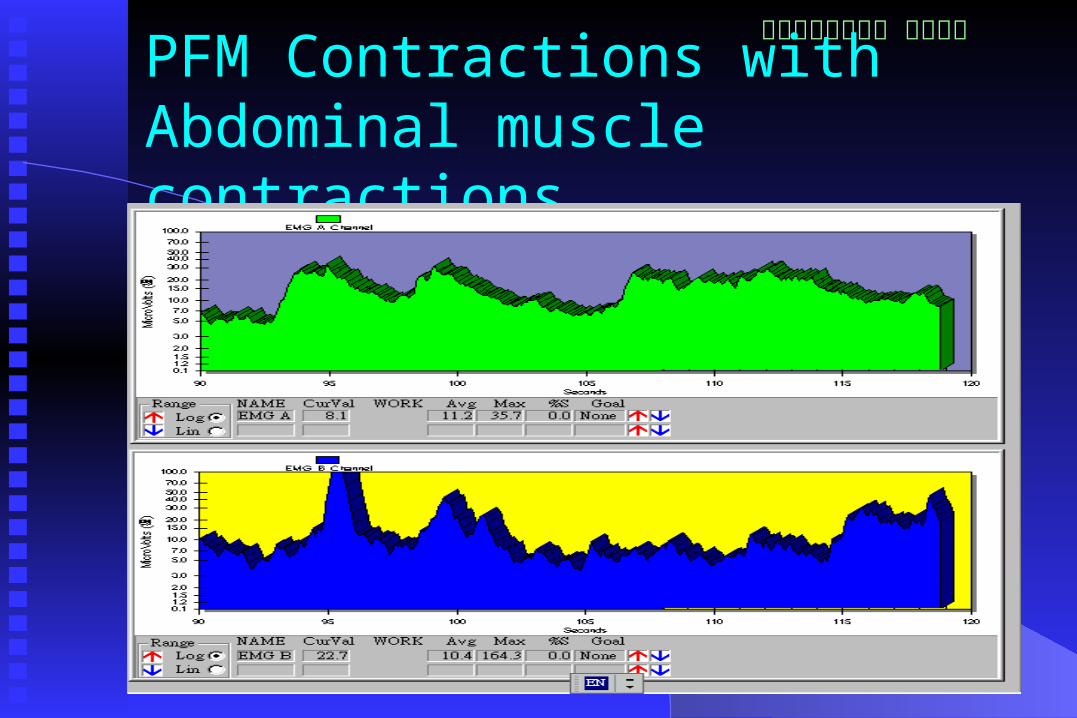
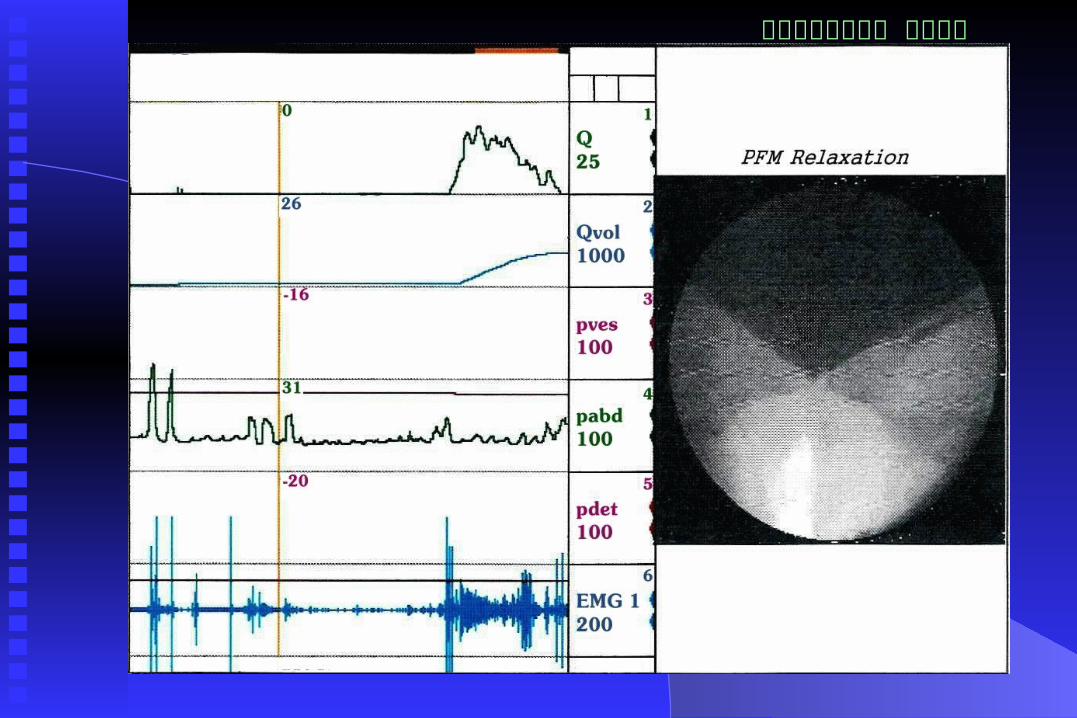
PFM Contractions with Abdominal muscle contractions
排尿障礙治療中心 版權所有
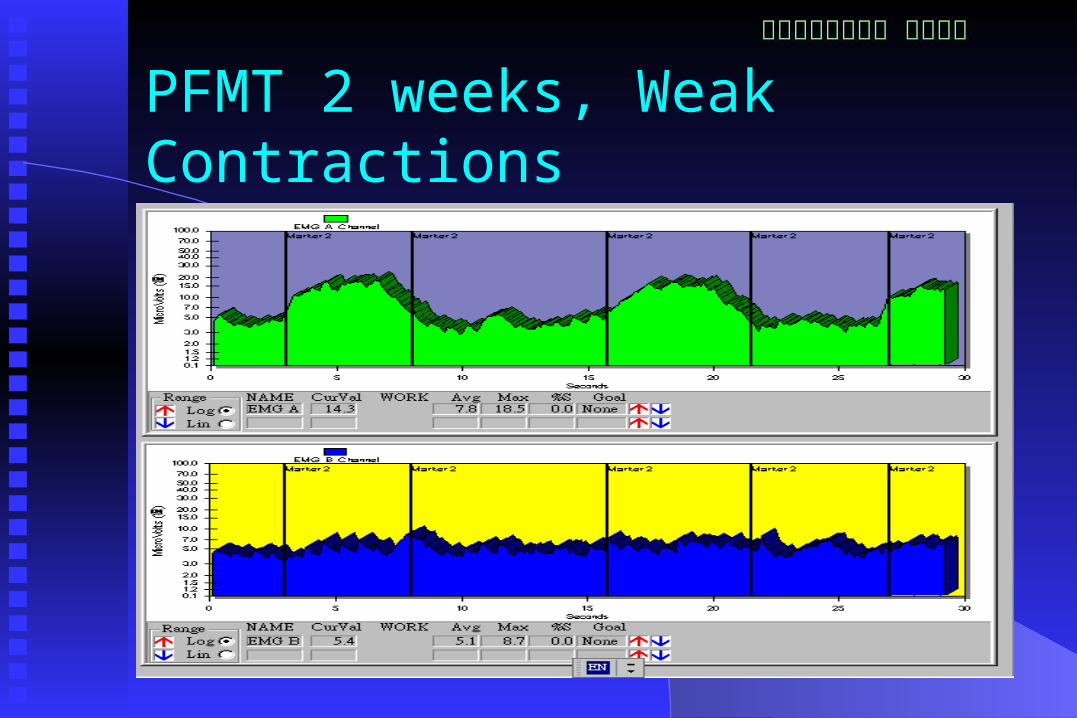
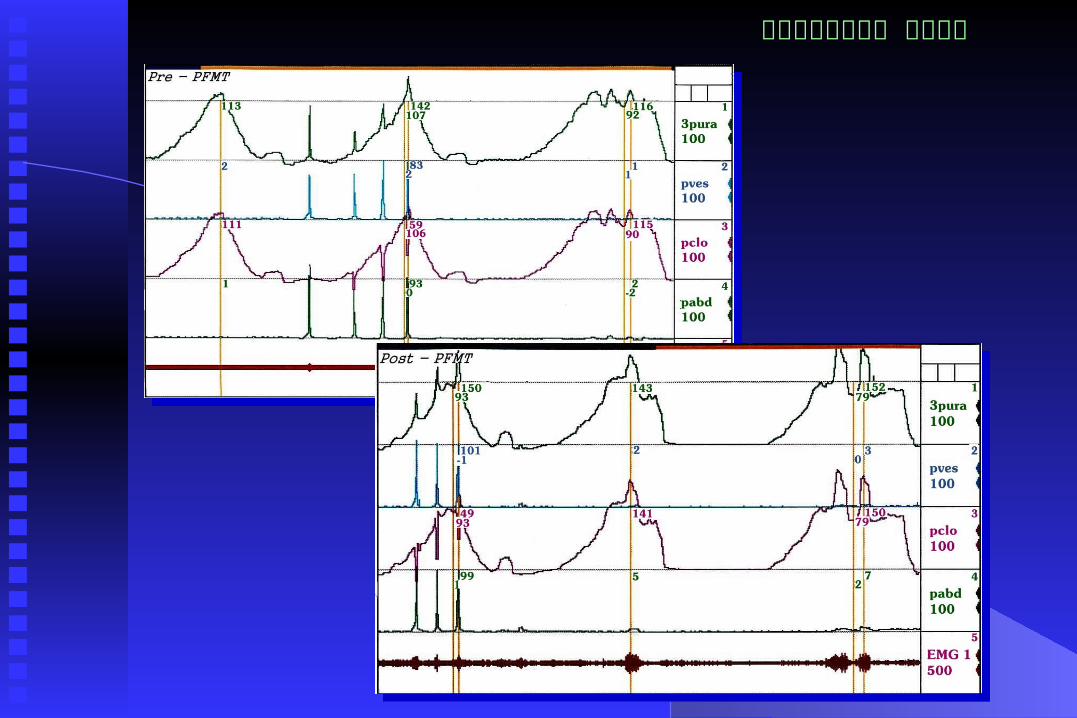
PFMT 2 weeks, Weak Contractions
排尿障礙治療中心 版權所有
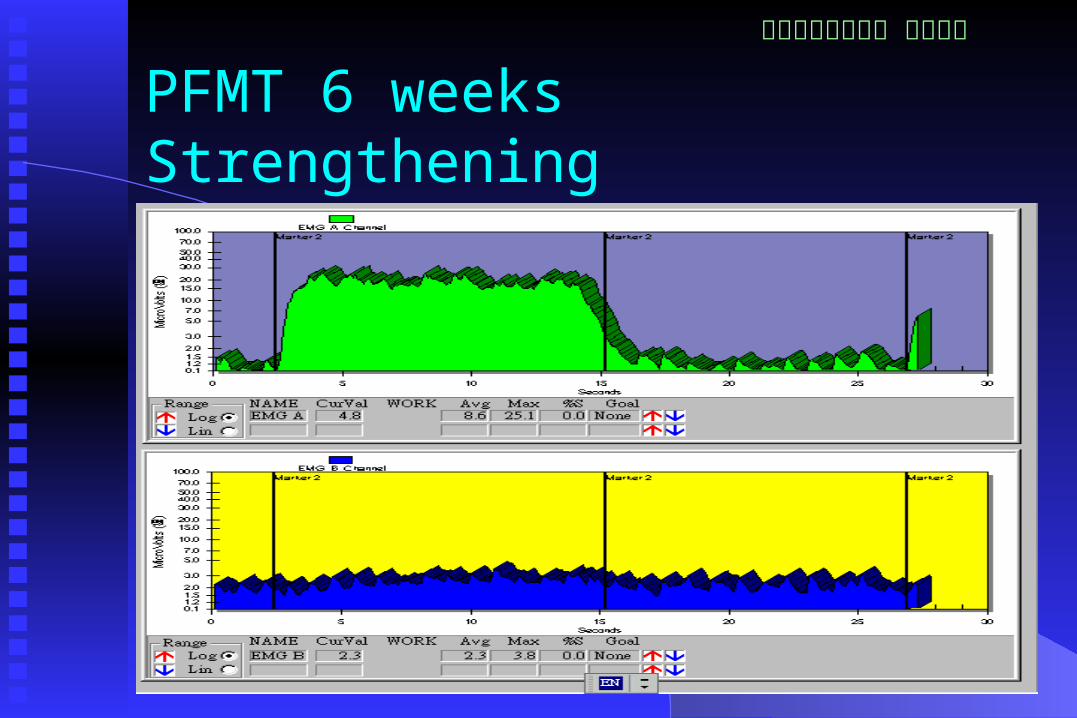
PFMT 6 weeks Strengthening

排尿障礙治療中心 版權所有
Strengthened PFM after 3 M training
排尿障礙治療中心 版權所有
Results of PFMT
Cure or improvement in 22 patients
(55%)
Treatment failure in 18 patients (45%)
Mean age 45 ± 12 and 47 ± 15 years
(p>0.05) of successful and failed
treatment group
排尿障礙治療中心 版權所有
Urodynamic Changes after PFMT Increase in first sensation, full sensation and cyst
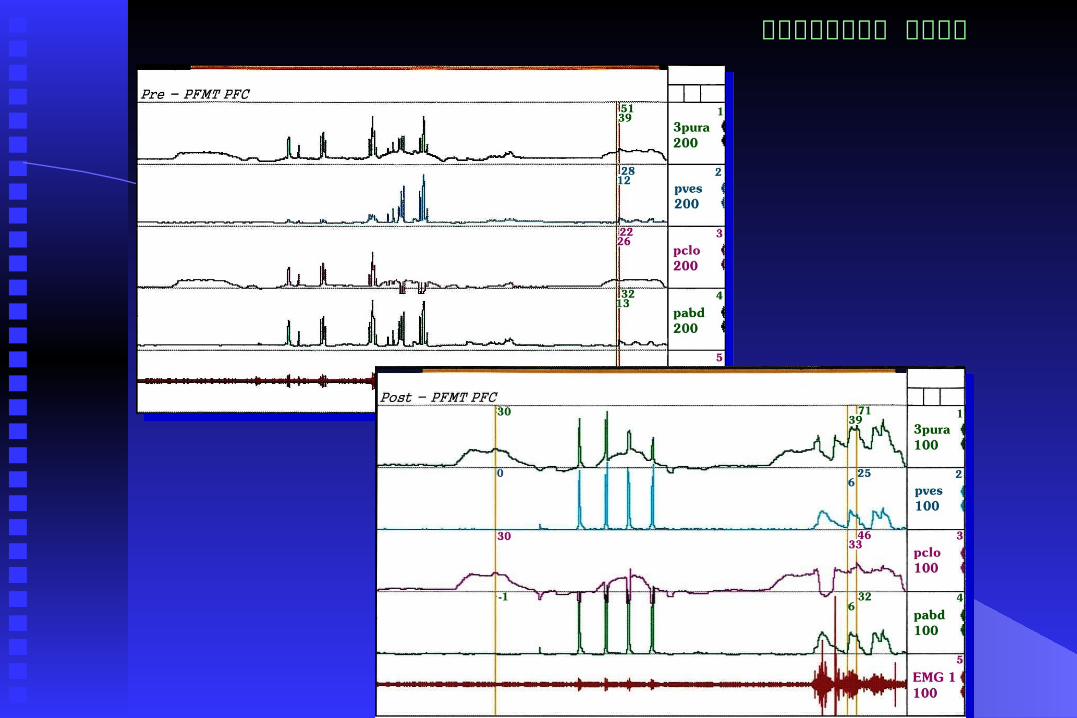
ometric capacity No change in MUCP, PTR, and FPL Significant increase in pelvic floor contraction pre
ssure in PFC - UPP Successfully treated patients had more changes ALPP changed little in patients with persistent UI

排尿障礙治療中心 版權所有The Urodynamic Parameters after Pelvic Floor Muscle Training (I)
Pre-treatment
Post-treatment
Statistics (p value)
Qmax (mL/s) Total 22.6 ± 13.0 20.9 ± 10.2 0.390
Successful26.0 ± 10.7
7 23.4 ± 10.7 0.236
Failure 18.3 ± 14.9 17.8 ± 9.2 0.881Voided volume
Total340.5 ± 123.
4 386.1 ± 152.9 0.240
Successful395.4 ± 69.
8 414.1 ± 176.3 0.780
Failure273.3 ± 144.
5 351.9 ± 119.4 0.021
FSF (mL) Total101.0 ± 26.
8 128.2 ± 41.6 0.025
Successful 96.1 ± 21.1 136.4 ± 45.8 0.027
Failure107.0 ± 32.
7 118.1 ± 35.7 0.484
FS (mL) Total189.0 ± 47.
5 229.5 ± 46.9 0.006
Successful190.4 ± 51.
4 245.0 ± 47.4 0.015
Failure187.3 ± 45.
2 210.4 ± 40.9 0.218

排尿障礙治療中心 版權所有The Urodynamic Parameters after Pelvic Floor Muscle Training (II)
Pre-treatmentPost-
treatmentStatistics (p
value)
Cystometric Capacity (mL)
Total 288.2 ± 83.8 338.0 ± 96.1 0.050Successful 303.0 ± 82.9 377.8 ± 100.6 0.086Failure 270.1 ± 86.0 289.3 ± 66.8 0.376
Compliance (mL / cmH2O)
Total 63.8 ± 69.7 138.3 ±170.3 0.069Successful 58.7 ± 53.0 190.4 ± 208.0 0.045Failure 70.0 ± 89.1 74.7 ± 80.4 0.914
Pdet (cmH2O) Total 22.5 ± 9.0 21.9 ± 10.3 0.777Successful 21.5 ± 8.9 18.3 ± 8.3 0.328Failure 23.8 ± 9.5 26.2 ± 11.3 0.465
LPP(cmH2O) Total 111.7 ± 43.9 113.9 ± 20.7 0,816Successful 122.3 ± 44.9 109.3 ± 23.3 0.518Failure 99.6 ± 42.8 119.3 ± 17.4 0.233

排尿障礙治療中心 版權所有The Urodynamic Parameters after Pelvic Floor Muscle Training (III)
Pre-treatmentPost-
treatmentStatistics (p
value)
MUCP (cmH2O)
Total 75.4 ± 30.2 70.5 ± 23.9 0.304Successful 72.5 ± 24.3 76.9 ± 23.6 0.393Failure 78.9 ± 37.5 62.7 ± 23.3 0.047
FPL (mm) Total 34.5 ± 4.59 36.6 ± 4.9 0.300Successful 34.4 ± 4.9 36.3 ± 5.1 0.089Failure 34.8 ± 4.4 36.9 ± 5.0 0.198
PTR (%) Total 47.9 ± 15.1 50.8 ± 10.2 0.486Successful 51.6 ± 17.4 50.2 ± 9.9 0.847Failure 43.4 ± 11.1 51.7 ± 11.1 0.049
PFC (cmH2O) Total 15.7 ± 13.4 23.0 ± 22.2 0.043Successful 20.5 ± 12.5 36.0 ± 21.2 0.009Failure 9.9 ± 12.7 7.1 ± 9.6 0.051

排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
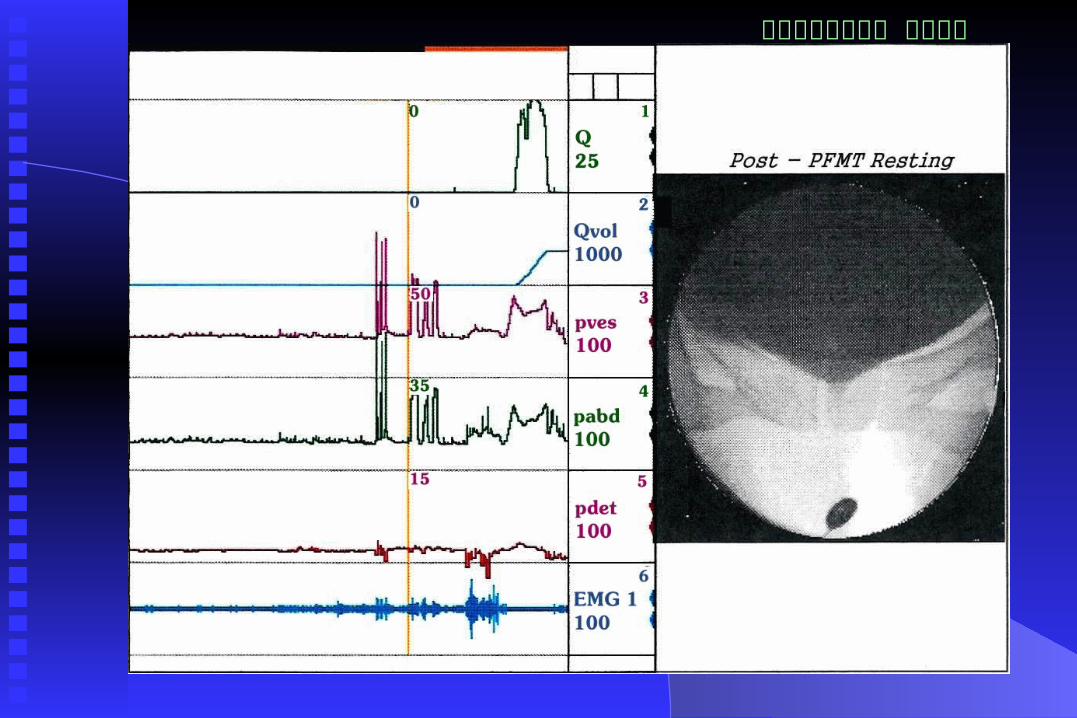
Bladder Base Changes after PFMT Less bladder neck descent after PFMT
Increased bladder neck elevation after PFMT
Both successfully and failure treated patients
had significant reduction of BN descent after
PFMT
BN descent and increase of BN elevation after
PFMT

排尿障礙治療中心 版權所有
The Urodynamic Parameter after Pelvic Floor Muscle Training (Ⅳ)
Pre-treatmentPost-
treatmentStatistics (p
value)
Resting BN position (cm)
Total 1.40 ± 0.74 1.65 ± 1.13 0.304Successful 1.14 ± 0.95 1.54 ± 1.21 0.213
Failure 1.72 ± 1.20 1.77 ± 1.06 0.886
Straining BN position (cm)
Total 2.79 ± 1.78 2.29 ± 1.47 0.138Successful 2.55 ± 1.56 2.18 ± 1.53 0.372Failure 3.13 ± 2.12 2.44 ± 1.45 0.270
BN descent (cm)
Total 1.45 ± 1.01 0.68 ± 0.49 0.000Successful 1.31 ± 1.19 0.59 ± 0.37 0.031Failure 1.61 ± 0.78 0.78 ± 0.62 0.004
BN elevated PFMT (cm)
Total 0.83 ± 0.49 1.40 ± 0.74 0.000Successful 1.14 ± 0.32 1.91 ± 0.44 0.000Failure 0.44 ± 0.39 0.78 ± 0.51 0.022

排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
Prediction for a Successful PFMT Young age, fewer pad changes, less
urethral incompetence, higher MUCP
A greater voluntary BN elevation on PME
A greater PFM contractility
Pretreatment BN position and BN descent
does not affect outcome of PFMT
排尿障礙治療中心 版權所有

排尿障礙治療中心 版權所有
排尿障礙治療中心 版權所有
Results of PFMT for SUI
PFM can be strengthened by a 12-week PFMT program
Effective PFMT increases Pura during voluntary contractions
Strengthened PFM do not change BN resting position
Strengthened PFM reduce BN descent on straining
55% of SUI patients have benefit from PFMT

排尿障礙治療中心 版權所有Pelvic floor muscle training for Stress urinary incontinence An improved hammock effect after PFMT
can be achieved No effect of PFMT on intrinsic continence
mechanism Patients with ISD might not benefit from
PFMT Patients with low cortical control of PFM
have unfavorable results Good patient intention and compliance are
the utmost important

排尿障礙治療中心 版權所有
Electrical Stimulation for SUI
Transvaginal ES has been used for genuine SUI, uTransvaginal ES has been used for genuine SUI, urge and mixed urinary incontinencerge and mixed urinary incontinence
Reported efficacy ranges 35 to70%Reported efficacy ranges 35 to70% A placebo-controlled study revealed after 15-weeA placebo-controlled study revealed after 15-wee
k treatment course, pad usage diminished by >50k treatment course, pad usage diminished by >50% in 62% women compared to 19% in sham devi% in 62% women compared to 19% in sham device, incontinence episode reduced >50% in 48% wce, incontinence episode reduced >50% in 48% women compared to 13% in sham deviceomen compared to 13% in sham device

排尿障礙治療中心 版權所有
Transvaginal electrical simulator

排尿障礙治療中心 版權所有Transvaginal electrical stimulation for Urge incontinence Leach reported 6% after long period of stimulationLeach reported 6% after long period of stimulation McGuire observed improvement in 93% women with urgMcGuire observed improvement in 93% women with urg
e incontinencee incontinence Plevnik found 52% improved (30% cured) in pure urge iPlevnik found 52% improved (30% cured) in pure urge i
ncontinencencontinence Brubaker used 20 Hz frequency current and cured 49% wBrubaker used 20 Hz frequency current and cured 49% w
ith urodynamic DIith urodynamic DI Smith found ES reduced urine loss by 50% in 20womenSmith found ES reduced urine loss by 50% in 20women Sand reported 38% success rate in 20 women with DISand reported 38% success rate in 20 women with DI
排尿障礙治療中心 版權所有
Transvaginal electrical stimulation
Low frequency (20 Hz) was appliedLow frequency (20 Hz) was applied Contrasting data of effects on genuine SUIContrasting data of effects on genuine SUI Transvaginal ES is effective in urge UITransvaginal ES is effective in urge UI First line treatment for women with pure urge incFirst line treatment for women with pure urge inc
ontinenceontinence For the women with mixed type UI who does not For the women with mixed type UI who does not
wish to undergo PME or surgery wish to undergo PME or surgery
排尿障礙治療中心 版權所有
Other Non-surgical Therapiesfor Incontinence Vaginal cones are a method of biofeedbackVaginal cones are a method of biofeedback 70% (19/27) with mild SUI had complete or >5070% (19/27) with mild SUI had complete or >50
% improvement after vaginal cone therapy, 7/50 % improvement after vaginal cone therapy, 7/50 with severe SUI had similar success ratewith severe SUI had similar success rate
Electrostimulation of pudendal nerve Electrostimulation of pudendal nerve (prolonged (prolonged pudendal nerve conduction velocity in 97% SUI)pudendal nerve conduction velocity in 97% SUI) i is effective in 62% with SUI and 20% were drys effective in 62% with SUI and 20% were dry
Electromagnetic stimulationElectromagnetic stimulation

排尿障礙治療中心 版權所有
Multiple purposesElectrostimulator and Biofeedback

排尿障礙治療中心 版權所有
Patient visualization & biofeedback

排尿障礙治療中心 版權所有
Cystometry biofeedback for urge incontinence For women who failed electrical stimulation, werFor women who failed electrical stimulation, wer
e intolerant to anticholinergics, e intolerant to anticholinergics, Urodynamic detrusor overactivity was provenUrodynamic detrusor overactivity was proven Performed several voluntary PFMC at episodes of Performed several voluntary PFMC at episodes of
DI while watching CMG tracing and EMG activitDI while watching CMG tracing and EMG activityy
Try to inhibit urge incontinence as longer duratioTry to inhibit urge incontinence as longer duration as possible at homen as possible at home

排尿障礙治療中心 版權所有
Detrusor overactivity and CMG biofeedback

排尿障礙治療中心 版權所有
Biofeedback to inhibit detrusor instability