Embed Size (px)
Citation preview

排尿障礙治療中心 版權所有
EnterocystoplastyEnterocystoplasty
Bladder augmentation – increase bladder capacity without (autoaugmentation) or with tissues such as stomach,intestine, or ureter
Bladder substitution—total in situ replacement of bladder with anastomosis to bladder neck or urethra

排尿障礙治療中心 版權所有
Indication for Indication for augmentation cystoplastyaugmentation cystoplasty
Intractable detrusor hyperreflexia – and incontinence refractory totreatment
Poor bladder compliance and hydronephrosis – compliance is more important than end-filling pressure
Contracted bladder and incontinenceChronic interstitial cystitis causes bladder p
ain

排尿障礙治療中心 版權所有
Causes of contracted bladder Causes of contracted bladder for enterocystoplastyfor enterocystoplasty
Irradiation cystitisChronic non-bacterial cystitisTuberculosis granulomatous cystitisStatus post partial cystectomy Unknown origin resulting contracted bladde
r – surgical trauma, frequent cystitisContracted bladder with vesicoureteral reflu
x

排尿障礙治療中心 版權所有
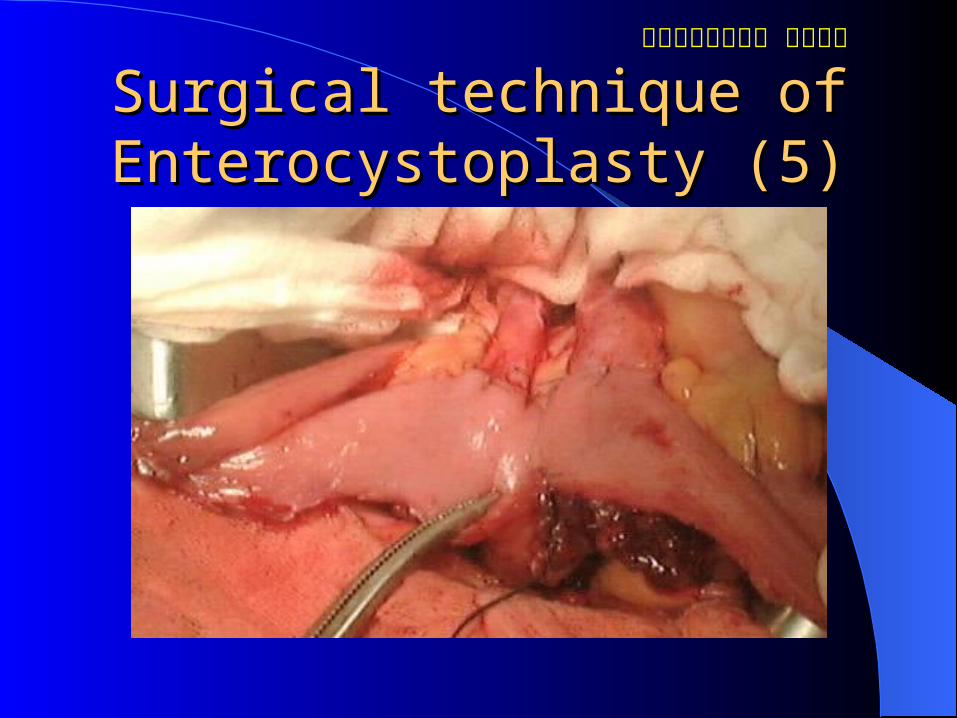
Surgical techniquesSurgical techniques
A 40-cm segment of terminal ileum Detubularization and fashioned into a W-sh
aped or double-folded cupAntireflux mechanism by a nipple valve or
direct reimplantation with a submucosal segment of ureter
Bladder was opened as clam-shapeDouble layer meticulous anastomosis

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (1)ystoplasty (1)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (2)ystoplasty (2)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (3)ystoplasty (3)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (4)ystoplasty (4)
排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (5)ystoplasty (5)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (6)ystoplasty (6)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (7)ystoplasty (7)

排尿障礙治療中心 版權所有
Surgical technique of EnterocSurgical technique of Enterocystoplasty (8)ystoplasty (8)

排尿障礙治療中心 版權所有
Results of Results of Augmentation cystoplastyAugmentation cystoplasty

排尿障礙治療中心 版權所有
Complications of enterocystopComplications of enterocystoplastylastyUreteral reimplantation stenosis 9-16%Continence 27- 65%Need for clean intermittent catheterization
8- 44%Stone formationImpairment of bone formation & mineraliza
tion

排尿障礙治療中心 版權所有
Stone formation after enterocyStone formation after enterocystoplastystoplastyMore in intestinal reservoir than gastrocysto
plastyStaples, suture materials, metabolic abnorm
ality, PH valueMucus plays an important rolePH conducive to crystallization of uric acidCalcium-phosphate ration is elevated in for
ming stone in intestinal reservoir

排尿障礙治療中心 版權所有
Late complications of EnterocLate complications of Enterocystoplastyystoplasty
Mucus production and obstructionBacteriuriaStone formationMetabolic alterationBowel dysfunctionSecondary malignancy

排尿障礙治療中心 版權所有
Changes of intestinal mucosaChanges of intestinal mucosa

排尿障礙治療中心 版權所有
Mucosal alteration inMucosal alteration in ileal bladder ileal bladder
Started at 1 year and completed at 4 yearsReduction in microvilli and inflammatory in
filtration of lamina propriaFlattening of mucosa with pseudourothelial
morphologyMuscular degeneration and hypertrophyCollagen deposition and fibrosis

排尿障礙治療中心 版權所有
Ileal mucosa in enterocystoplastyIleal mucosa in enterocystoplasty

排尿障礙治療中心 版權所有
Muscular degeneration at 1 mMuscular degeneration at 1 month after Enterocystoplastyonth after Enterocystoplasty

排尿障礙治療中心 版權所有
Active peristalsis at initial stagActive peristalsis at initial stage of enterocystoplastye of enterocystoplasty

排尿障礙治療中心 版權所有
Muscular degeneration at 6-mMuscular degeneration at 6-month after Enterocystoplastyonth after Enterocystoplasty

排尿障礙治療中心 版權所有
Decrease in peristaltic pressurDecrease in peristaltic pressure in enterocystoplastye in enterocystoplasty

排尿障礙治療中心 版權所有
Muscular degeneration at 1-yeMuscular degeneration at 1-year after Enterocystoplastyar after Enterocystoplasty

排尿障礙治療中心 版權所有
Silence of peristaltic waves after Silence of peristaltic waves after enterocystoplastyenterocystoplasty

排尿障礙治療中心 版權所有
Contracture of anastomosis of enContracture of anastomosis of enterocystoplasty in TB patientterocystoplasty in TB patient

排尿障礙治療中心 版權所有
Changes in bladder compliance iChanges in bladder compliance in enterocystoplastyn enterocystoplasty

排尿障礙治療中心 版權所有
Persistent DESD and poor compliPersistent DESD and poor compliance in enterocystoplastyance in enterocystoplasty

排尿障礙治療中心 版權所有
Significance in low compliancSignificance in low compliance after enterocystoplastye after enterocystoplasty
Persistent hydronephrosis after augmentation cystoplasty
Urinary incontinence at full bladderNight time urinary incontinence due to high
peristaltic pressureProne to urinary tract infection due to muco
sal defectsDysuria due to small bladder capacity
排尿障礙治療中心 版權所有
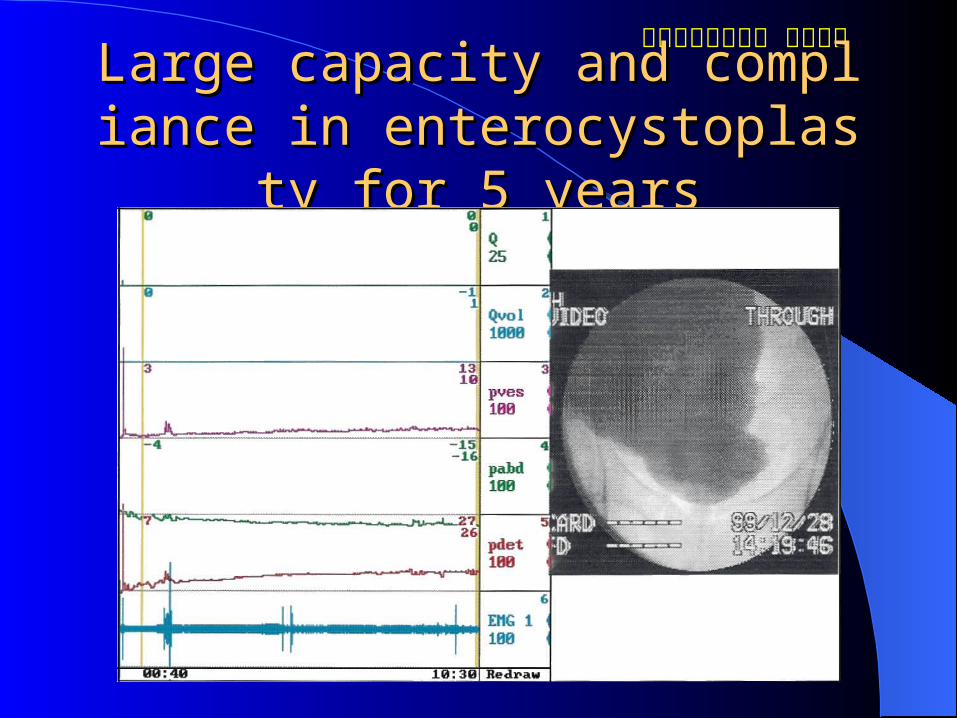
Large capacity and compliance in Large capacity and compliance in enterocystoplasty for 5 yearsenterocystoplasty for 5 years

排尿障礙治療中心 版權所有Changes in peristaltic pressure and com-pliaChanges in peristaltic pressure and com-pliance before and after enterocystoplastynce before and after enterocystoplasty

排尿障礙治療中心 版權所有
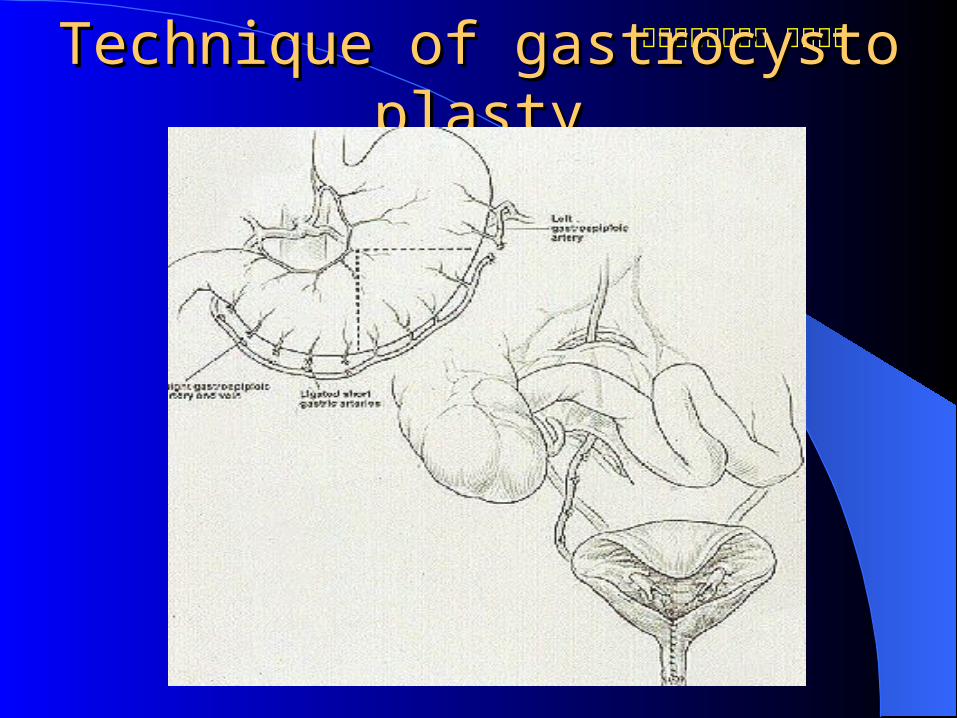
GastrocystoplastyGastrocystoplasty
Advantages of gastrocystoplasty– absence of mucus production, hydrogen ion absorption, bacteriuria, acidexcretion
Preferable in patients with chronic renal failure
Disadvantages – excessive acid depletion, metabolic alkalosis, hematuria, peptic ulceration, perforation, dumping syndrome
排尿障礙治療中心 版權所有
Technique of gastrocystoplastyTechnique of gastrocystoplasty

排尿障礙治療中心 版權所有
UreterocystoplastyUreterocystoplasty
Avoid performing gastroenteral surgeryPrevent mucus secretion, secondary malign
ancy, frequent infectionIndicated only in patients with megaloureter
and contracted bladderTissue expansion may be another way in ac
hieving a dilated ureter for harvest

排尿障礙治療中心 版權所有
Bladder autoaugmentationBladder autoaugmentation
Increase of bladder capacity is limitedSuccessful result in detrusor instability com
parable with enterocystoplastyMay be indicated in chronic interstitial cysti
tis with bladder pain The preoperative bladder capacity determin
es the final outcomeMinimal surgical morbidity

排尿障礙治療中心 版權所有
Surgical technique forSurgical technique forbladder autoaugmentationbladder autoaugmentation Extraperitoneal exploration of bladder Inserting Foley catheter and tenting the draining tub
e to a pressure to keep the intravesical pressure and bladder volume
Dissection of detrusor muscle to mucosa Dissect the detrusor muscles off mucosa (detrusor m
yomectomy) with perforation Dissecting half of bladder wall Covering with omentum or mucosectomized intestin
al wall

排尿障礙治療中心 版權所有
Bladder autoaygmentationBladder autoaygmentation

排尿障礙治療中心 版權所有
Continent urinary reservoir (KContinent urinary reservoir (Kock pouch)ock pouch)
Indicated in quadriplegics with less good hand function
Women who cannot perform CISCSevere urethral incompetence and inconti- n
ence after repeat surgical proceduresPatient with a severely damaged or scarred
urethra

排尿障礙治療中心 版權所有
Contracted bladder with a Contracted bladder with a non-functioning urethranon-functioning urethra

排尿障礙治療中心 版權所有Technique of formation of a Kock pouchTechnique of formation of a Kock pouch

排尿障礙治療中心 版權所有
Intraluminal pressure and anti-Intraluminal pressure and anti-incontinence mechanismincontinence mechanism
排尿障礙治療中心 版權所有
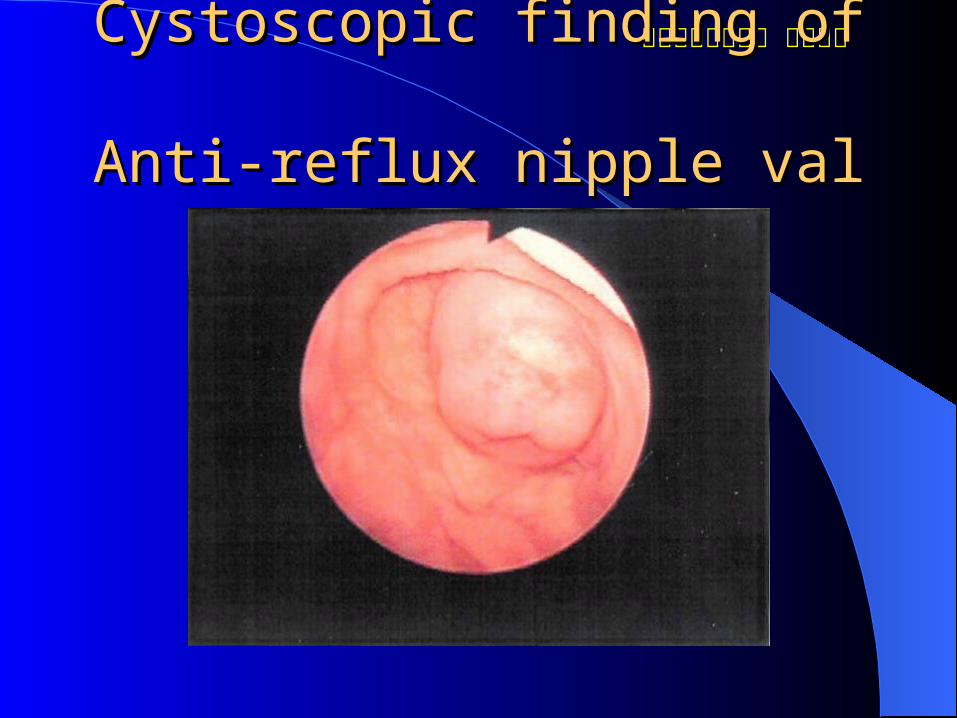
Cystoscopic finding of Cystoscopic finding of Anti-reflux nipple valveAnti-reflux nipple valve

排尿障礙治療中心 版權所有
Sonography of anti-incontinenSonography of anti-incontinence efferent loopce efferent loop

排尿障礙治療中心 版權所有
Urodynamic results after augUrodynamic results after augmentation cystoplastymentation cystoplasty
Cystometric capacity cmH2O
End filling pressure cmH2O
Bladder compliance ml/cmH2O
MUCP cmH2O
Preoperative 165±97 50±23 10.8±2.7 62±28
Postoperative 760±289 13±4.7 75±43 -
Statistics p<0.005 p<0.005 p<0.005
MUCP= Maximal urethral closure pressure.
排尿障礙治療中心 版權所有
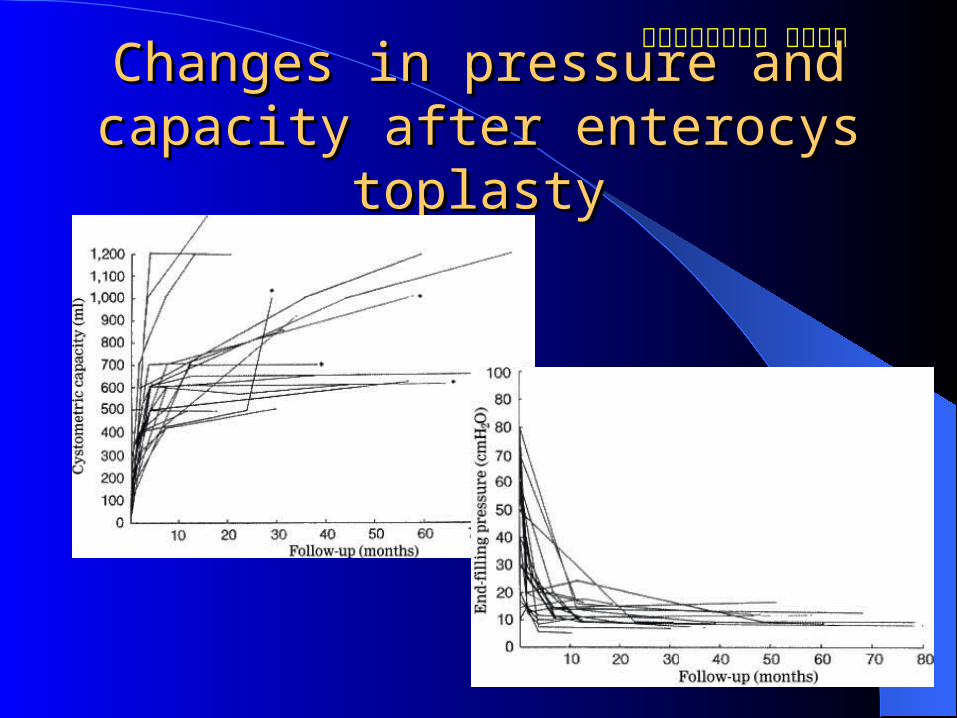
Changes in pressure and capacitChanges in pressure and capacity after enterocystoplastyy after enterocystoplasty

排尿障礙治療中心 版權所有
Continent cystostomyContinent cystostomy
Indicated for patients with a fair bladder compliance but a damaged urethra and incontinence
Closed the bladder outlet and augmented with anti-incontinence ileum or cecum with appendix
Avoid excessive intestinal surgery and prevent the need of ureteral reimplantation

排尿障礙治療中心 版權所有
Seromuscular enterocystoplasSeromuscular enterocystoplastytyTo avoid mucus secretion and complication
from enterocystoplastyTo prevent secondary contracture of the bla
dder after autoaugmentationCombined detrusor myomectomy and enter
ocystoplasty with a segment of mucosecomized ileum
Adequate myomectomy is necessary

排尿障礙治療中心 版權所有
Technique of Seromuscular eTechnique of Seromuscular enterocystoplastynterocystoplasty

排尿障礙治療中心 版權所有
Orthopedic neobladder in woOrthopedic neobladder in womanman
Urinary incontinence is not a problem after neobladder formation without preserving bladder neck
Pelvic floor muscle exercises improve stress urinary incontinence
Pubovaginal sling procedure may help in achieving continence
Complete daytime and night time continence rates are 88% and 79-82%

排尿障礙治療中心 版權所有
Orthotopin Neobladder in womaOrthotopin Neobladder in woman after radical cystectomyn after radical cystectomy

排尿障礙治療中心 版權所有
Contraindication for enterocystContraindication for enterocystoplasty in NVDoplasty in NVD
Azotemia with elevated creatinine (>2.5mg%) and BUN, CCr <10ml/min
Severely damaged or incompetent urethraLow abdominal straining ability and poor h
and function for catheterizationSevere intestinal dysfunction and diarrheaLow social status and far to reach medical r
esources