Embed Size (px)
Citation preview
排尿障礙治療中心 版權所有
Spinal cord injurySpinal cord injury
Hann-Chorng KuoDepartment of Urology
Buddhist Tzu Chi General Hospital Hualien
排尿障礙治療中心 版權所有
Leading causes & Location of Spinal cord injury
Leading causes & Location of Spinal cord injury
Motor vehicle accidents (47%) Falls (21%) Sports (14%) Act of violence (14%) Location of SCI: cervical (53%), thoracic (35%),
lumbar and sacral (10%)
排尿障礙治療中心 版權所有
Urinary tract symptoms in Acute spinal cord injuryUrinary tract symptoms in Acute spinal cord injury
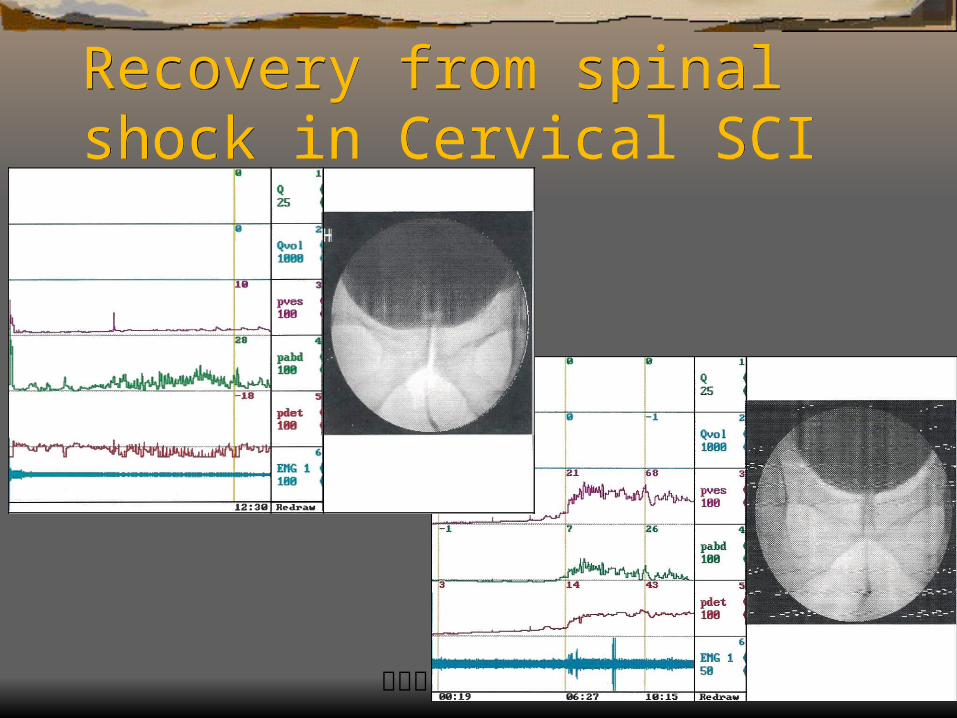
Spinal shock stage: detrusor areflexia, complete anesthesia of fullness or voiding
Recovery of micturition reflex gradually about 1-3 months after recovery of somatic reflexes
Prolonged recovery of voiding reflex may be due to overdistension of the bladder after injury or complication
排尿障礙治療中心 版權所有
Micturition ControlMicturition Control Micturition reflex center – sacral cords S 2-4 Sympathetic nucleus – T10-L1 Micturition control center – pons Sensory motor center – frontal lobe Limbic system Cerebellum, Basal ganglia
排尿障礙治療中心 版權所有
Pathophysiology of lower urinary tract dysfunction after SCI
Pathophysiology of lower urinary tract dysfunction after SCI Suprasacral cord lesion – interruption of coordin
ation of detrusor contraction and sphincter relaxation
Lesion above T6 SCI – sympathetic hyperactivity during activation of visceral input, bladder distension, rectal distention, cold and noxious stimulation, surgery and infection
排尿障礙治療中心 版權所有
Chronic spinal cord injury and urinary tract dysfunction
Chronic spinal cord injury and urinary tract dysfunction Autonomic dysreflexia – SCI above T5,6 (sympat
hetic nucleus) Detrusor external sphincter dyssynergia (DESD)
– lesion above S2-4 Detrusor hyperreflexia – complete or incomplete
SCI above sacral cords Detrosor areflexia – sacral cord SCI or cauda eq
uina lesions
排尿障礙治療中心 版權所有
Urodynamic findings in SCIUrodynamic findings in SCICervical
(n=68)
Thoracic
(n=53)
Sacral or infrasacral
(n=40)
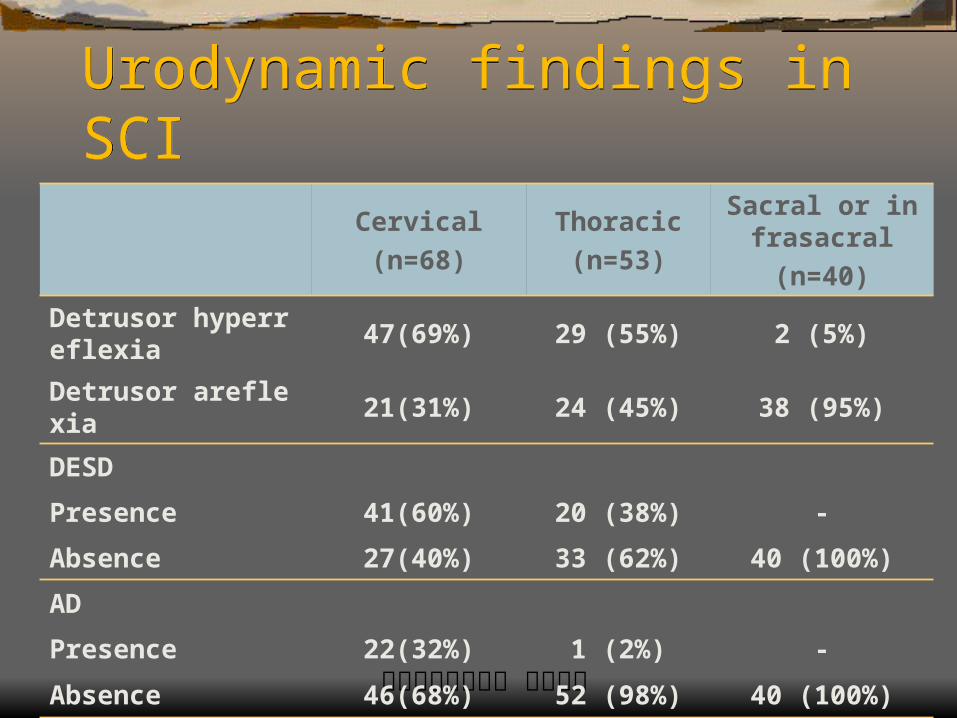
Detrusor hyperreflexia 47(69%) 29 (55%) 2 (5%)
Detrusor areflexia 21(31%) 24 (45%) 38 (95%)
DESD
Presence 41(60%) 20 (38%) -
Absence 27(40%) 33 (62%) 40 (100%)
AD
Presence 22(32%) 1 (2%) -
Absence 46(68%) 52 (98%) 40 (100%)
DESS=Detrusor external sphincteric dyssynergia; AD=autonomic dysreflexia.
排尿障礙治療中心 版權所有
Major concern in managing SCIMajor concern in managing SCI
Preservation of renal function Free of symptomatic urinary tract infection Efficient bladder emptying Freedom of catheter Continence
排尿障礙治療中心 版權所有
High risk SCI PatientsHigh risk SCI Patients
Complete neurological lesion Cervical SCI with quadriplegia Prolonged indwelling catheter High detrusor leak-point pressure Presence of DESD and AD Large residual urine Presence of vesicoureteral reflux
排尿障礙治療中心 版權所有
Detrusor leak-point pressureDetrusor leak-point pressure The intravesical pressure (detrusor pressure) at t
he end of filling or urinary incontinence A detrusor LPP of over 40cm water will endange
r the upper tract in meningomyelocele Reduction of detrusor LPP can improve renal fun
ction, reduce the risk of UTI, decrease the degree of hydronephrosis, improve vesicoureteral reflux and restore continence
排尿障礙治療中心 版權所有
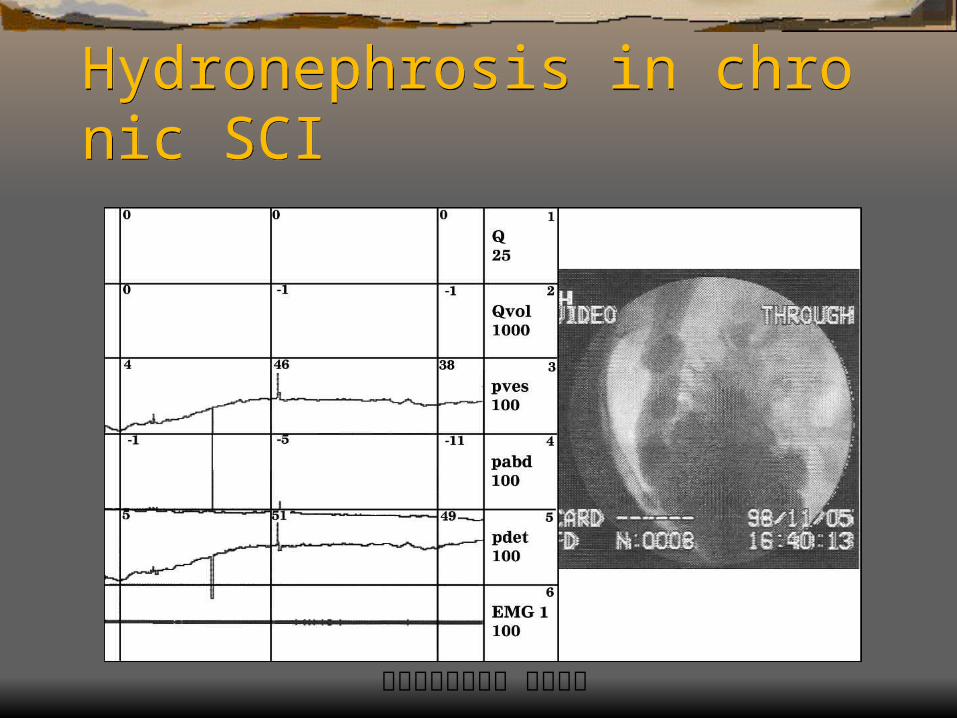
Hydronephrosis in SCIHydronephrosis in SCI Hydronephrosis is a sign of upper tract deteriorat
ion after SCI In 251 SCI patients, 24 (9.6%) had hydronephro
sis, including: Cervical SCI 7 (5.9% of 118), 7+ 4 (3-15) years Thorac& lumb 8 (8.6% of 93), 9.9+ 6.5 (3-22) Sacral 9 (22.5 of 40), 17+ 6.1 (8-26)
排尿障礙治療中心 版權所有
Autonomic dysreflexiaAutonomic dysreflexia Spinal cord lesion above T6 Hypertension and increased sympathetic
outflow, flushing, sweating above dermatome during increased visceral input (bladder over-distension,urination, rectal distension, surgery, UTI)
Risk of heart failure and stroke Bladder neck contraction during voiding
排尿障礙治療中心 版權所有
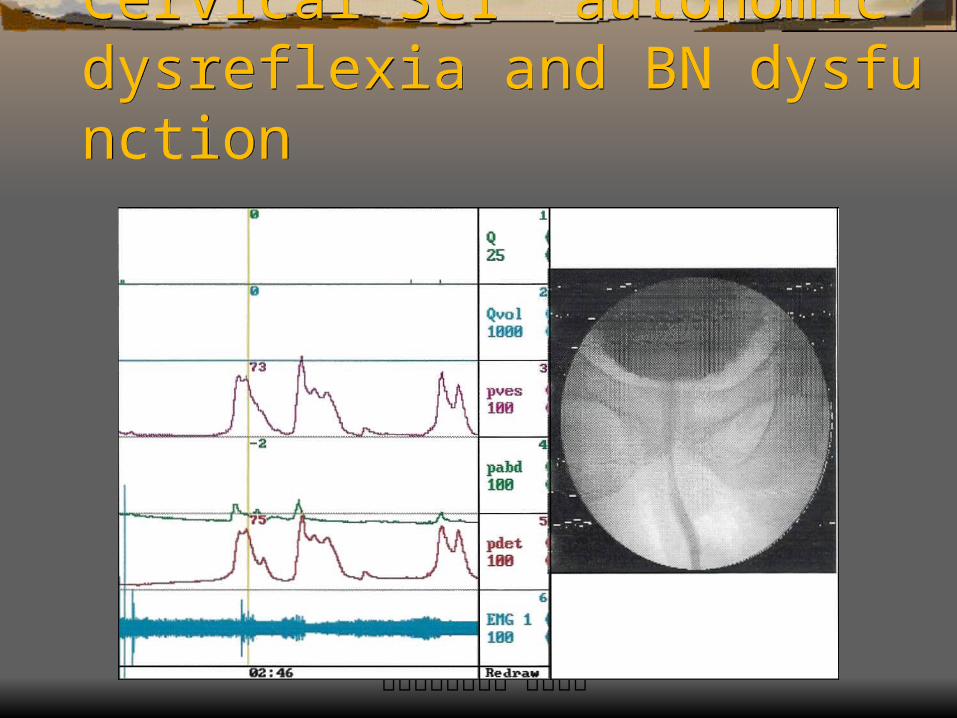
Cervical SCI autonomic dysreflexia and BN dysfunction Cervical SCI autonomic dysreflexia and BN dysfunction
排尿障礙治療中心 版權所有
Detrusor external sphincter dyssynergia (DESD)Detrusor external sphincter dyssynergia (DESD) Spinal cord lesion above micturition reflex center Lack of coordination in the micturition center External sphincter contrction during detrusor con
tractions Dysuria, difficult to initiate voiding, high voiding p
ressure, large residual urine Result in frequent UTI and upper tract damage
排尿障礙治療中心 版權所有
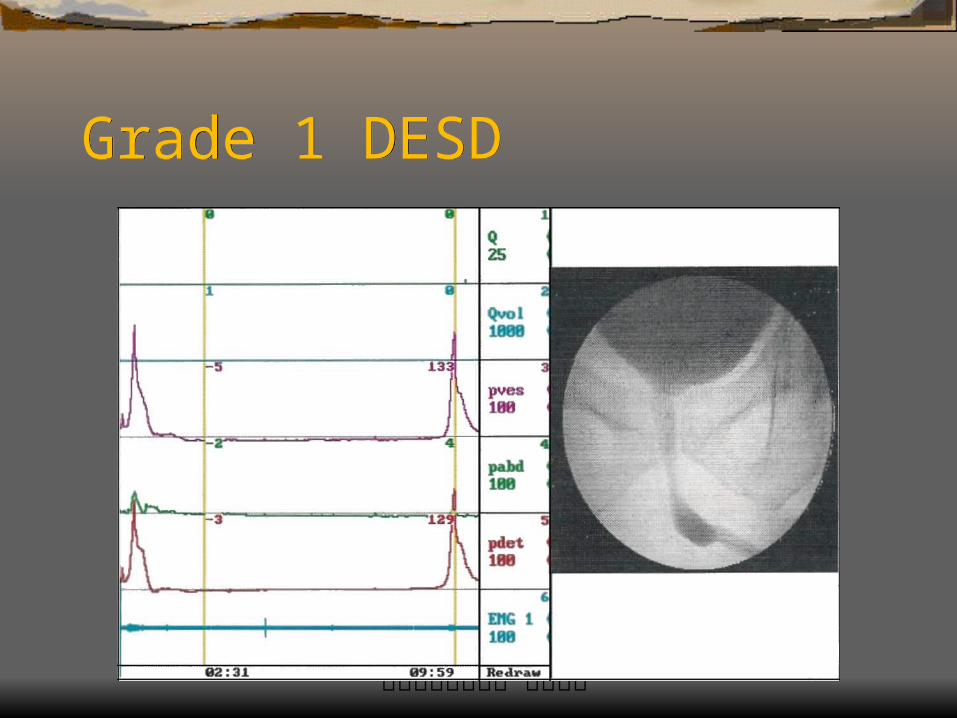
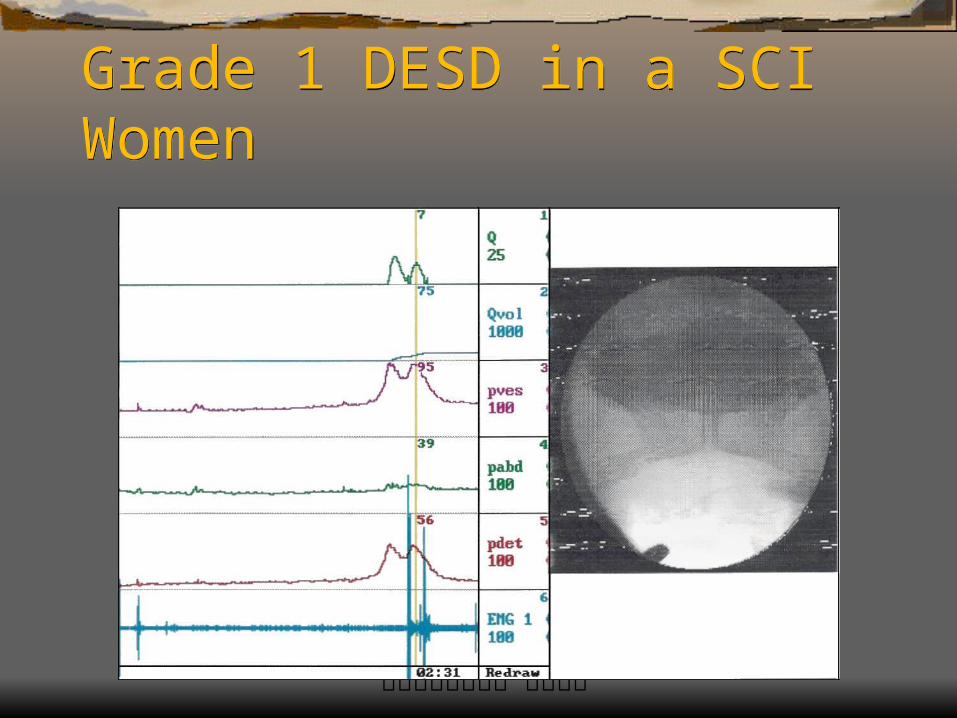
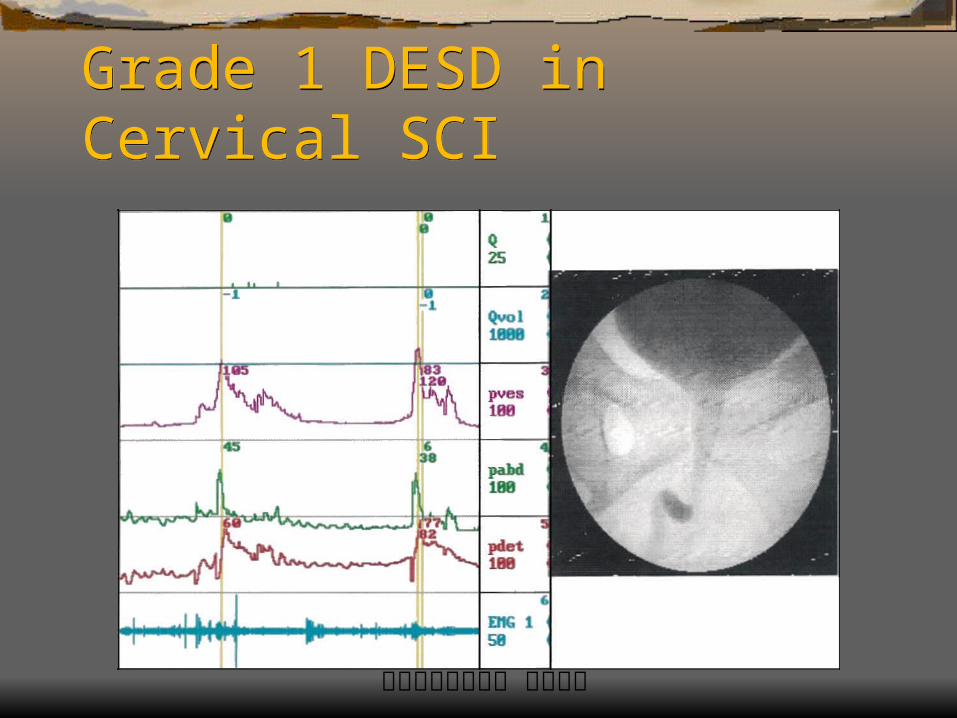
Grades of DESDGrades of DESD Grade 0- 3 according to the sphincteric activity Grade 0 – normal or synergia Grade 1 – DH &high Pves, hyerreflexic sphincter at initi
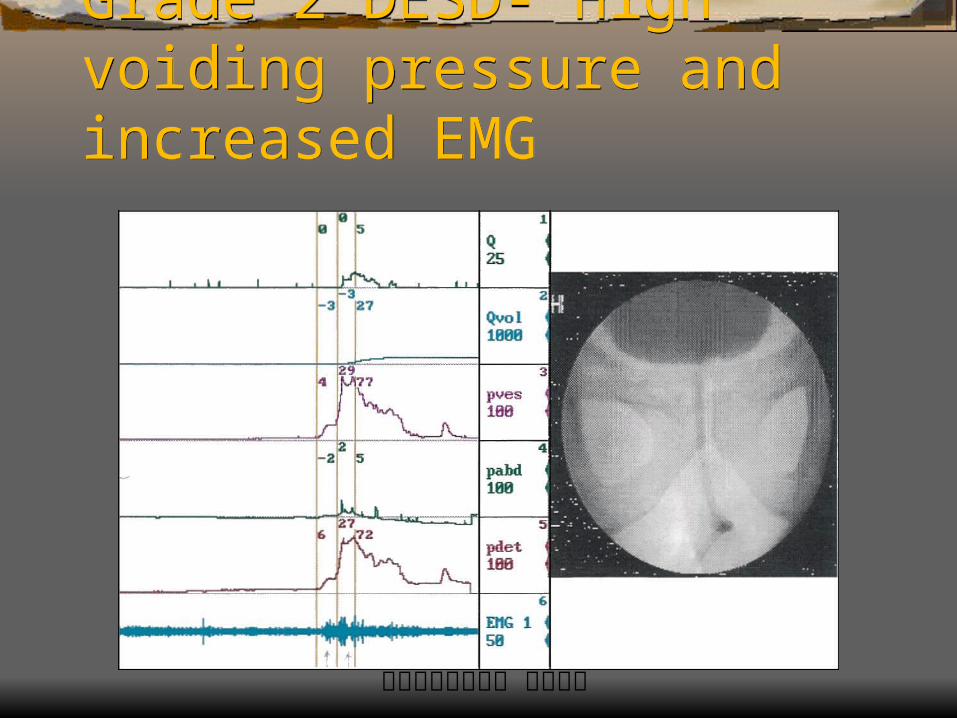
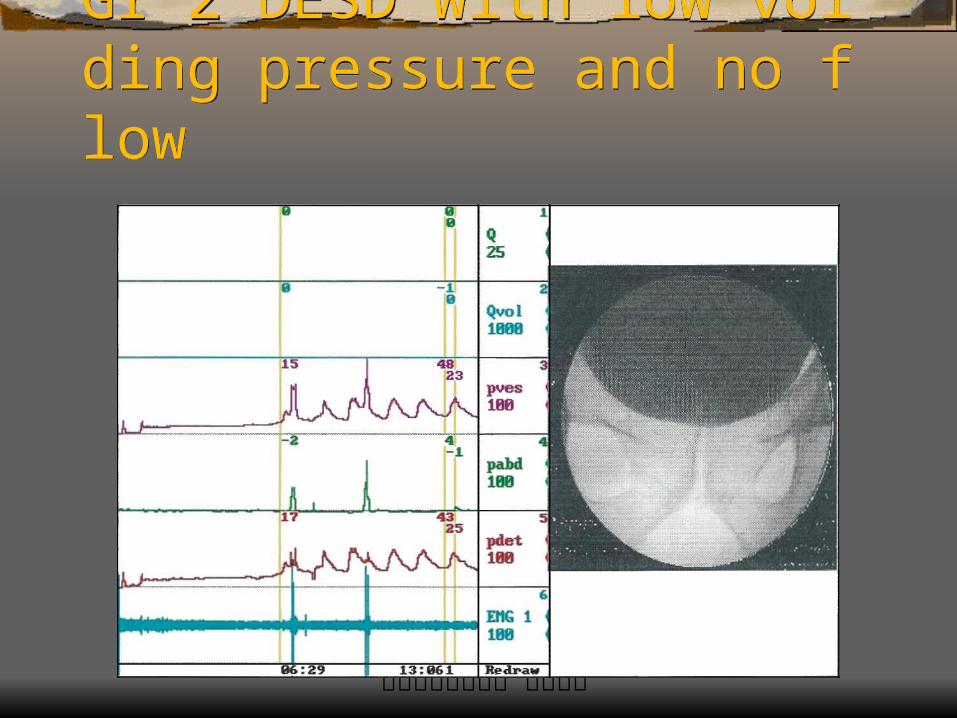
ation, voiding with mild residual urine Grade 2 – DH or hyporeflexic detrusor, intermittent hype
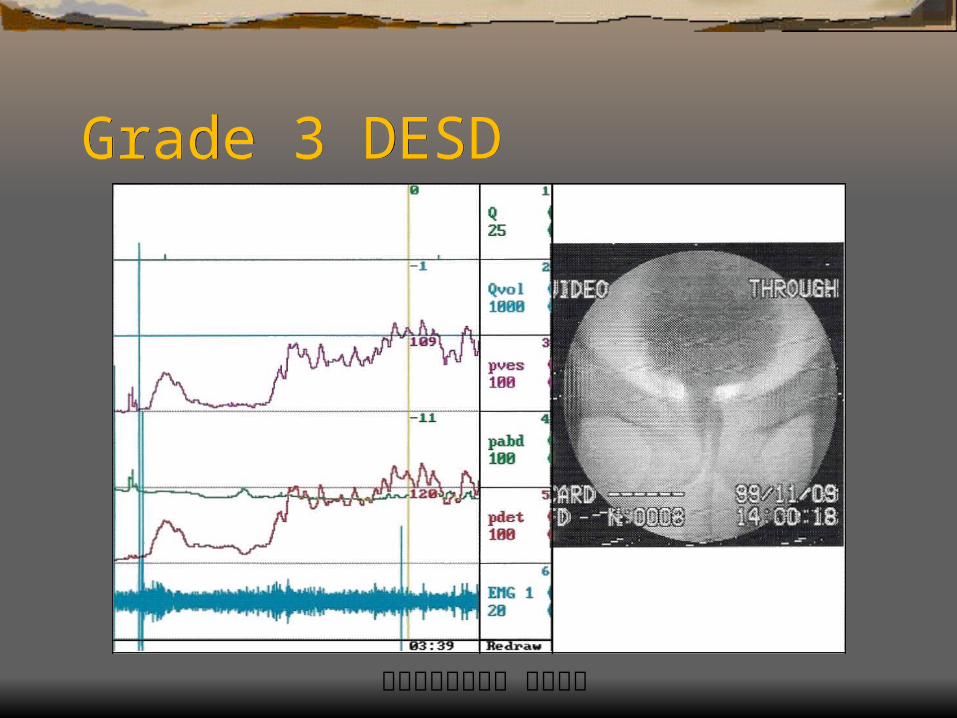
rreflexic sphincter, large residual urine Grade 3 – DH, closed hyperreflexic sphincter, no sponta
neous voiding
排尿障礙治療中心 版權所有
Grade 1 DESDGrade 1 DESD
排尿障礙治療中心 版權所有
Grade 2 DESD- High voiding pressure and increased EMG
Grade 2 DESD- High voiding pressure and increased EMG
排尿障礙治療中心 版權所有
Gr 2 DESD with low voiding pressure and no flowGr 2 DESD with low voiding pressure and no flow
排尿障礙治療中心 版權所有
Grade 3 DESDGrade 3 DESD
排尿障礙治療中心 版權所有
Recovery from spinal shock in Cervical SCI Recovery from spinal shock in Cervical SCI
排尿障礙治療中心 版權所有
Late Urological Complications in Spinal cord injury
Late Urological Complications in Spinal cord injury
Urinary tract infection induced sepsis Hydronephrosis and uremia Stone formation (renal& bladder stone) Contracted bladder & VU reflux Incontinence and associated complications Bladder tumor formation (chronic indwelling cath
eter)
排尿障礙治療中心 版權所有
Hydronephrosis in chronic SCIHydronephrosis in chronic SCI
排尿障礙治療中心 版權所有
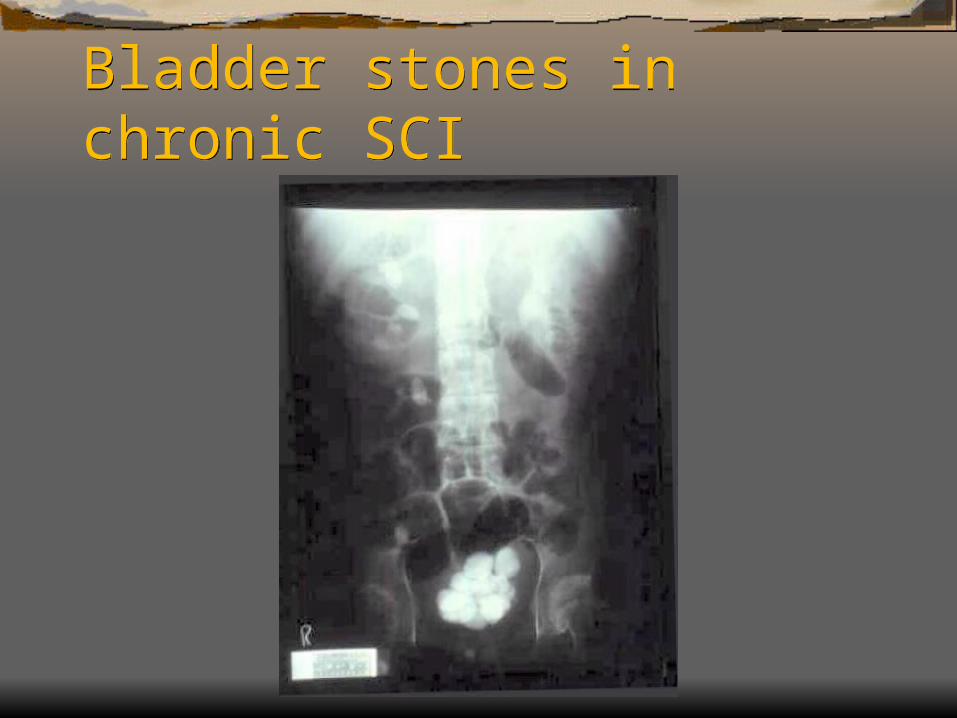
Bladder stones in chronic SCIBladder stones in chronic SCI
排尿障礙治療中心 版權所有
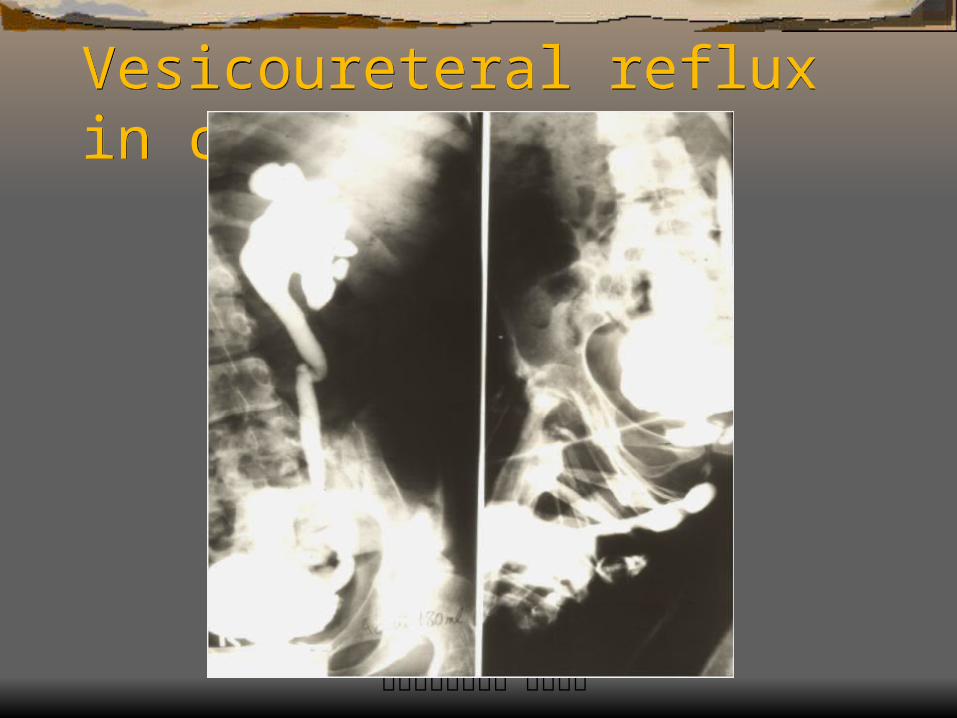
Vesicoureteral reflux in chronic SCIVesicoureteral reflux in chronic SCI
排尿障礙治療中心 版權所有
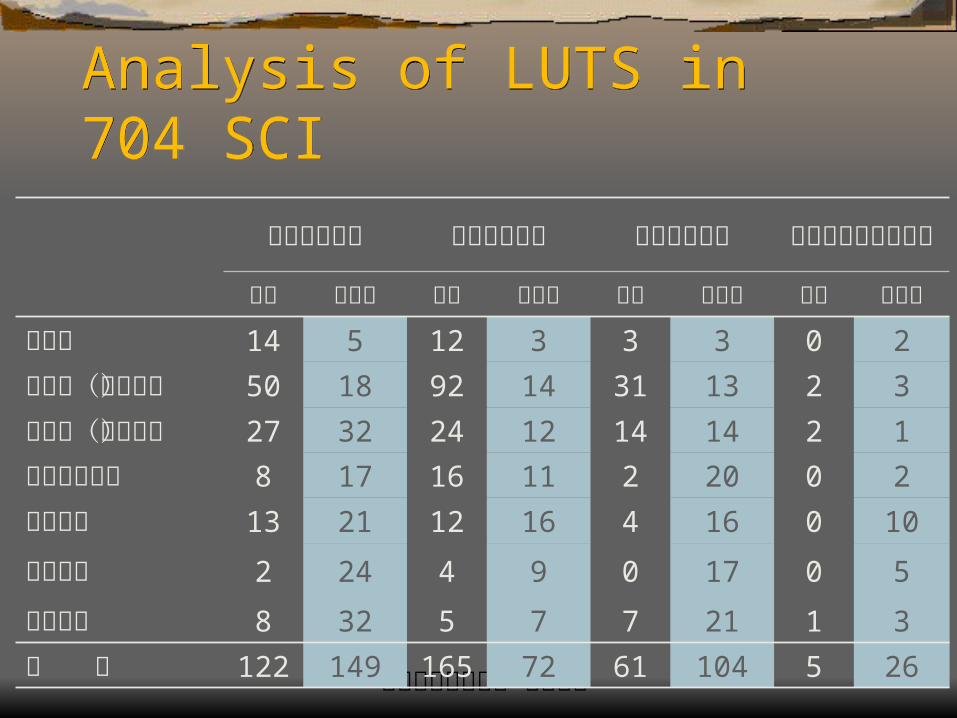
Analysis of LUTS in 704 SCI Analysis of LUTS in 704 SCI
頸髓脊髓損傷 胸髓脊髓損傷 腰髓脊髓損傷 薦髓及以下脊髓損傷
完全 不完全 完全 不完全 完全 不完全 完全 不完全
尿瀦留 14 5 12 3 3 3 0 2尿失禁(無感覺) 50 18 92 14 31 13 2 3
尿失禁(有感覺) 27 32 24 12 14 14 2 1
滿溢性尿失禁 8 17 16 11 2 20 0 2排尿困難 13 21 12 16 4 16 0 10頻尿急尿 2 24 4 9 0 17 0 5正常排尿 8 32 5 7 7 21 1 3總 計 122 149 165 72 61 104 5 26
排尿障礙治療中心 版權所有
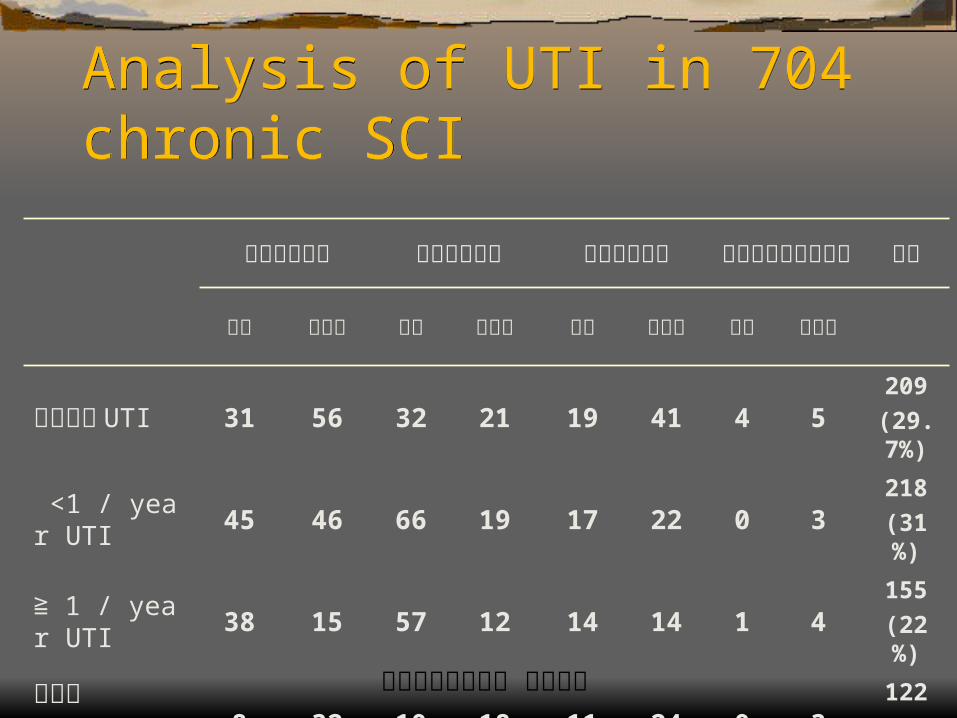
Analysis of UTI in 704 chronic SCIAnalysis of UTI in 704 chronic SCI
頸髓脊髓損傷 胸髓脊髓損傷 腰髓脊髓損傷 薦髓及以下脊髓損傷 總計
完全 不完全 完全 不完全 完全 不完全 完全 不完全
從來沒有 UTI 31 56 32 21 19 41 4 5209
(29.7%)
<1 / year UTI 45 46 66 19 17 22 0 3218
(31%)
≧ 1 / year UTI 38 15 57 12 14 14 1 4155
(22%)
不知道8 32 10 18 11 24 0 3
122
(17.3%)
排尿障礙治療中心 版權所有
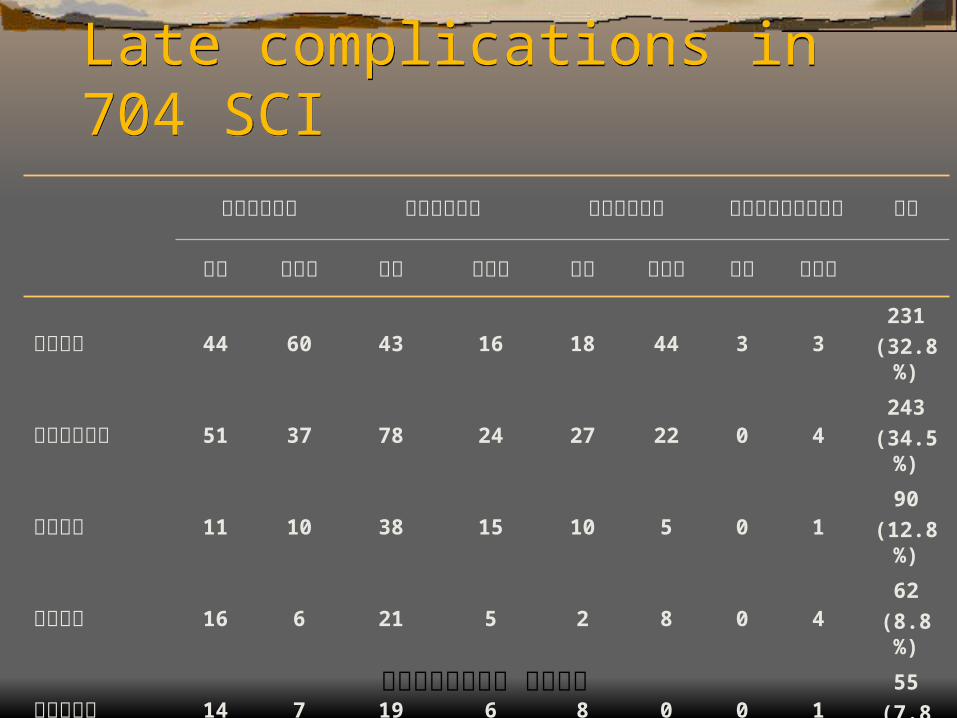
Late complications in 704 SCILate complications in 704 SCI
頸髓脊髓損傷 胸髓脊髓損傷 腰髓脊髓損傷 薦髓及以下脊髓損傷 總計
完全 不完全 完全 不完全 完全 不完全 完全 不完全
完全沒有 44 60 43 16 18 44 3 3231
(32.8%)
反覆尿路感染 51 37 78 24 27 22 0 4243
(34.5%)
尿路結石 11 10 38 15 10 5 0 190
(12.8%)
腎臟水腫 16 6 21 5 2 8 0 462
(8.8%)
輸尿管逆流 14 7 19 6 8 0 0 155
(7.8%)
腎衰竭 6 5 8 2 2 1 1 025
(3.6%)
排尿障礙治療中心 版權所有
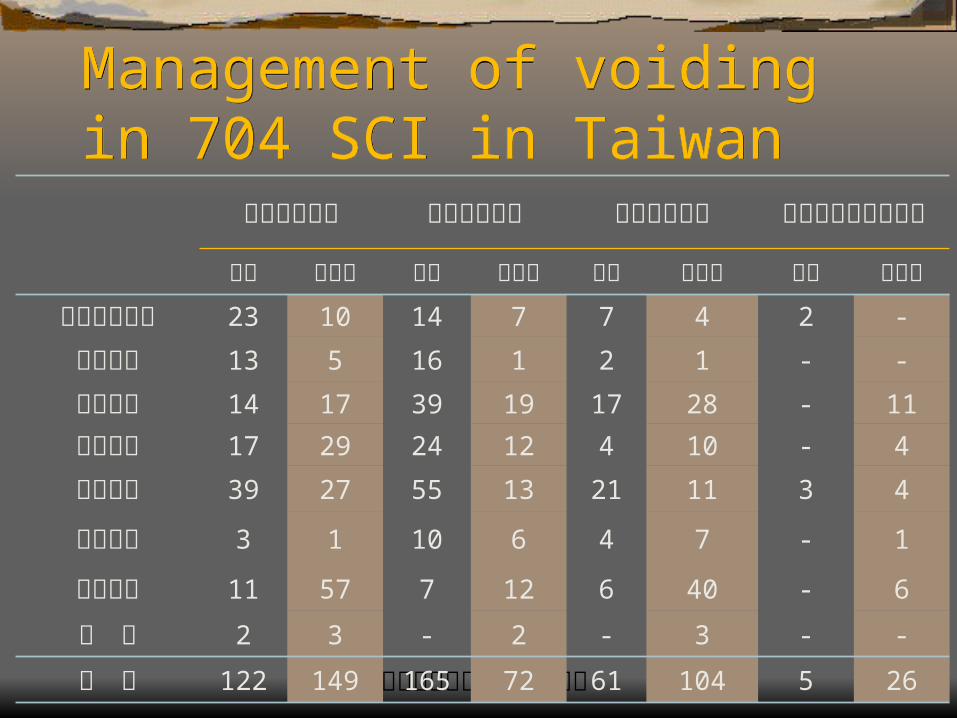
Management of voiding in 704 SCI in TaiwanManagement of voiding in 704 SCI in Taiwan
頸髓脊髓損傷 胸髓脊髓損傷 腰髓脊髓損傷 薦髓及以下脊髓損傷
完全 不完全 完全 不完全 完全 不完全 完全 不完全
尿道留置導尿 23 10 14 7 7 4 2 -
膀胱造廔 13 5 16 1 2 1 - -
腹壓排尿 14 17 39 19 17 28 - 11
敲擊腹部 17 29 24 12 4 10 - 4
自行反射 39 27 55 13 21 11 3 4
間歇導尿 3 1 10 6 4 7 - 1
正常感覺 11 57 7 12 6 40 - 6
其 他 2 3 - 2 - 3 - -
總 計 122 149 165 72 61 104 5 26
排尿障礙治療中心 版權所有
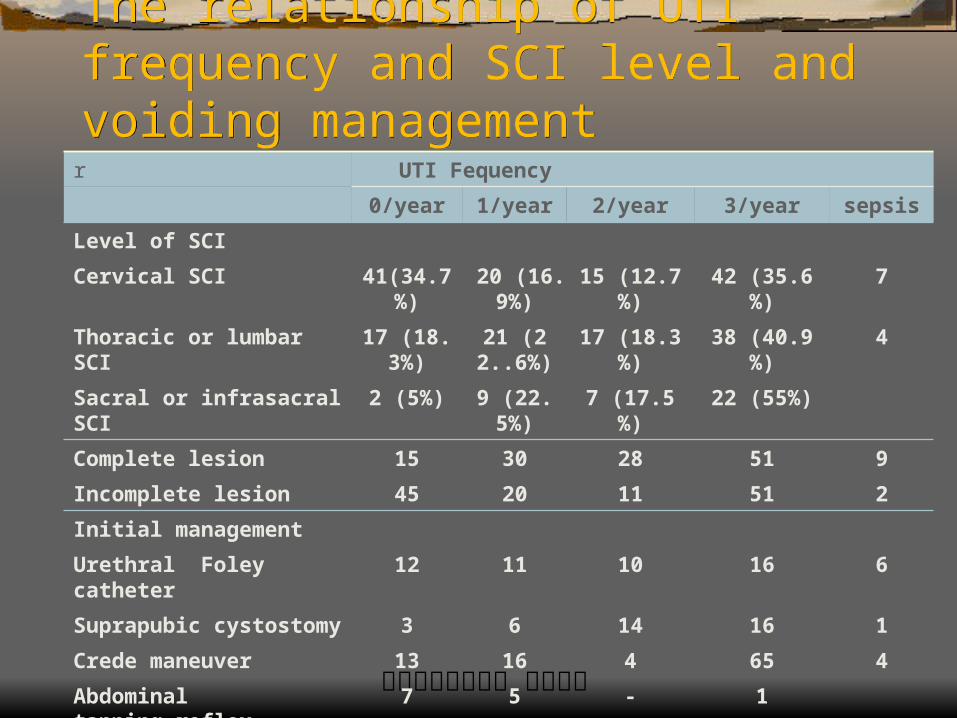
The relationship of UTI frequency and SCI level and voiding management
The relationship of UTI frequency and SCI level and voiding management
r UTI Fequency
0/year 1/year 2/year 3/year sepsis
Level of SCI
Cervical SCI 41(34.7%) 20 (16.9%)
15 (12.7%) 42 (35.6%) 7
Thoracic or lumbar SCI 17 (18.3%) 21 (22..6%)
17 (18.3%) 38 (40.9%) 4
Sacral or infrasacral SCI 2 (5%) 9 (22.5%) 7 (17.5%) 22 (55%)
Complete lesion 15 30 28 51 9
Incomplete lesion 45 20 11 51 2
Initial management
Urethral Foley catheter 12 11 10 16 6
Suprapubic cystostomy 3 6 14 16 1
Crede maneuver 13 16 4 65 4
Abdominal tapping,reflex 7 5 - 1
CISC 11 - - 3
Normal 14 12 11 1
CISC=Clean intermittent self-catheterization.
排尿障礙治療中心 版權所有
Considerations in management of LUTD in chronic SCI
Considerations in management of LUTD in chronic SCI
Correct complications Treat hydronephrosis, treat UTI, treat vesicourete
ral reflux Improve quality of life Treat incontinence, convenience of bladder empt
ying, free of catheter,free of medicationIndividual treatment strategy for each SCI patient
排尿障礙治療中心 版權所有
Medical Treatment for LUTD in chronic SCIMedical Treatment for LUTD in chronic SCI To reduce detrusor hyperreflexia – anticholinergi
cs (oxybutynin,imipramine) To reduce bladder neck hyperreflexia – alpha-bl
ocker (tamsulosin, terazosin, prazosin) To reduce striated sphincter spasticity – skeletal
muscle relaxant (baclofen, diazepam) To increase detrusor muscle tone – cholinergic a
gent (urecholine)
排尿障礙治療中心 版權所有
Combination of medication for LUTS in Chronic SCICombination of medication for LUTS in Chronic SCI
To treat incontinence – anticholinergics and adrenergic agnist (methylephedrine) – CISC is needed, residual urine, UTI should be monitored
To facilitate voiding – cholinergic agent and alpha-blocker and skeletal muscle relaxant – incontinence exacerbates, upper tract deterioration if detrusor LPP is high
排尿障礙治療中心 版權所有
Side effects of Medical Treatment in chronic SCISide effects of Medical Treatment in chronic SCI
Constipation -- anticholinergics Hypotension –alpha-blocker Nasal congestion –adrenergic agonist General weakness – skeletal muscle relaxant Side effects increase as combination of medicati
on Cost benefit should be considered
排尿障礙治療中心 版權所有
Intravesical therapy for SCIIntravesical therapy for SCI Detrusor hyperreflexia – oxybutynin, capsaicin, r
esiniferatoxin, botulinum injection Reversible response Periodic instillation or injection
排尿障礙治療中心 版權所有
Capsaicin and resiniferatoxinCapsaicin and resiniferatoxin Intravesical agents for overactive bladder have been
mostly been used in neurogenic bladder disorders Capsaicin and resiniferatoxin have been successfull
y used intravesically to reduce urinary incontinence in neurogenic detrusor hyperreflexia
Resiniferatoxin has less acute side effect and similar efficacy as capsaicin
Resiniferatoxin is effective in treating detrusor hyperreflexia refractory to capsaicin treatment

排尿障礙治療中心 版權所有
Therapeutic effects of resiniferatoxinTherapeutic effects of resiniferatoxin 10 -5 to 10 -7 M RTX is effective for DH of SCI 10 -8 M RTX can significantly improve voiding
pattern and pain score in hypersensitive disorders and bladder pain
RTX is safe for application in humans Is RTX effective for DESD through inhibition of
DH in SCI patients?
排尿障礙治療中心 版權所有
Successful Therapeutic EffectsSuccessful Therapeutic Effects
Patient became dry Increase in 50% of maximal cystometric capacity Subjective improvement rate by >50% in incontin
ence or dysuria Significant change in quality of life in urination su
bjectively
排尿障礙治療中心 版權所有
Side Effects of RTX TreatmentSide Effects of RTX Treatment
Autonomic responses Elevated blood pressure Headache Bradycardia General malaise RTX was drained out and bladder irrigation was
performed if systolic BP >200mmHg
排尿障礙治療中心 版權所有
Results of resiniferatoxin therapyResults of resiniferatoxin therapy 20 patients (7 women and 13 men) Mean age 42.2 ±13.2 (24 – 66) years 10 cervical, 10 thoracic SC lesion 18 traumatic SCI, 2 multiple sclerosis All had DESD, 9 had autonomic dysreflexia 18 incontinence, 13 dysuria, 8 recurrent UTI
排尿障礙治療中心 版權所有
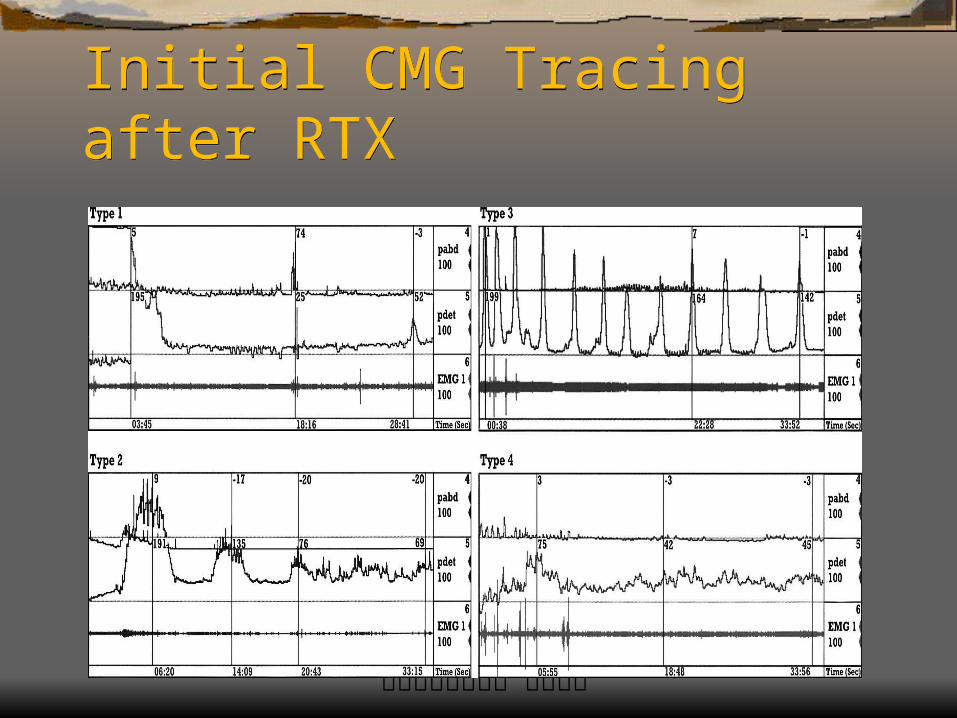
Responses of RTX instillationResponses of RTX instillation Initial excitatory response at 1-5 min Four types of initial responses Type 1: A sustained high pressure followed by c
omplete detrusor non-contraction Type 2: A high pressure contraction followed by progressively lower amplitude contractions Type 3: Intermittent high pressure contractions Type 4: Intermittent low pressure contractions
排尿障礙治療中心 版權所有
Initial CMG Tracing after RTXInitial CMG Tracing after RTX
排尿障礙治療中心 版權所有
Therapeutic Results of RTXTherapeutic Results of RTX 4/20 became dry during the daytime but incontin
ent at night time 8/20 had increased in frequency interval and voi
ded volume 8/20 had no significant improvement 8/13 with dysuria had improvement in spontaneo
us voiding (5) or on Crede maneuver (3)
排尿障礙治療中心 版權所有
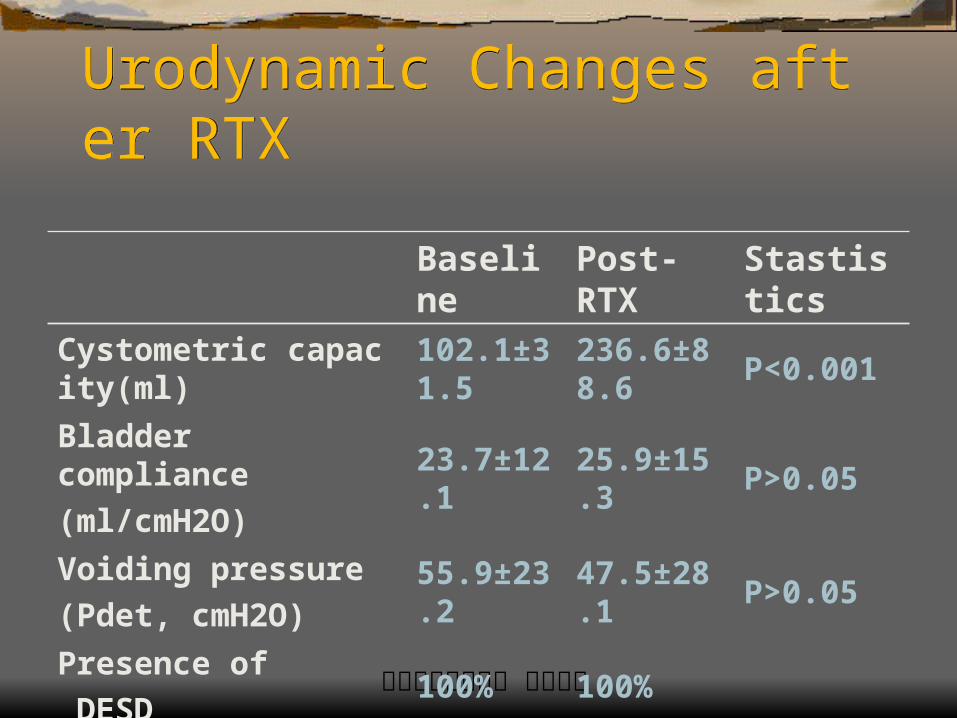
Urodynamic Changes after RTXUrodynamic Changes after RTX
Baseline Post-RTX StastisticsCystometric capacity(ml) 102.1±31.5 236.6±88.6 P<0.001
Bladder compliance
(ml/cmH2O)23.7±12.1 25.9±15.3 P>0.05
Voiding pressure
(Pdet, cmH2O)55.9±23.2 47.5±28.1 P>0.05
Presence of
DESD100% 100%
排尿障礙治療中心 版權所有
Side Effects and QOL after RTXSide Effects and QOL after RTX Dizziness and headache with high BP and brady
cardia (4/20) Initial gross hematuria (5/20) Bladder irritation and frequency in all patients 7/20 responded that quality o life improved after
RTX 13/20 did not notice any significant change in Q
OL although objective data showed improved
排尿障礙治療中心 版權所有
Correlation of RTX Responses with Therapeutic Results
Correlation of RTX Responses with Therapeutic Results
A good response was noted in 12 patients Type 1: 5 (100%) Type 2: 4 (80%) Type 3: 2 (40%) Type 4: 1 (25%) Duration of RTX responses: 1 (6m), 6 (3m), 3
(2m), 2 (1m), repeat instillation in 7/12
排尿障礙治療中心 版權所有
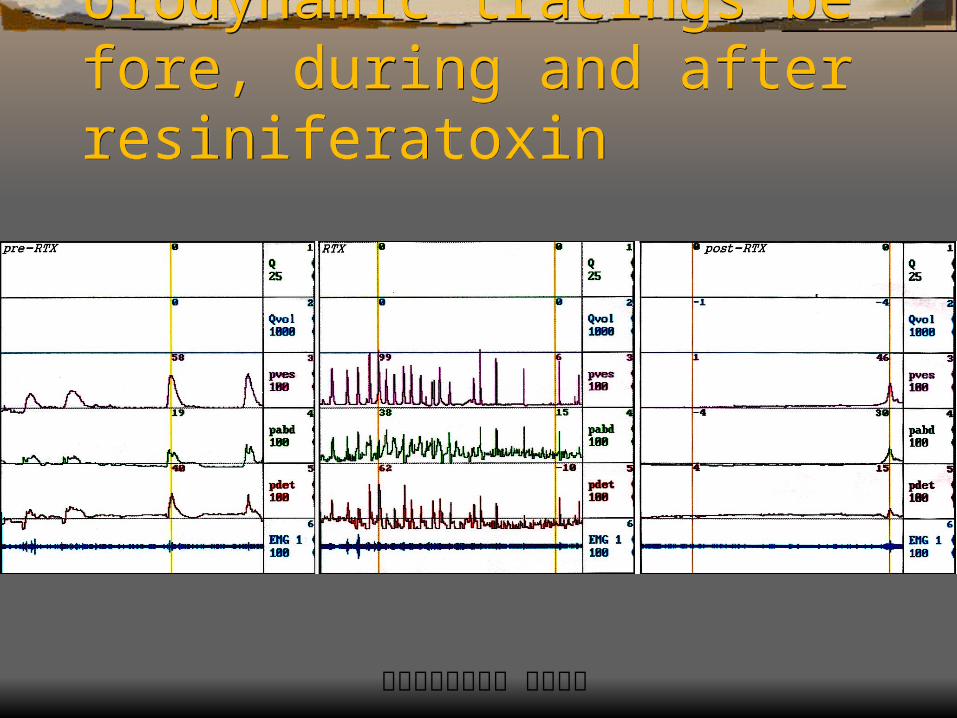
Urodynamic tracings before, during and after resiniferatoxin
Urodynamic tracings before, during and after resiniferatoxin
排尿障礙治療中心 版權所有
Botulinum toxin injectionBotulinum toxin injection Botlinum toxin has been used to inject striated ur
ethral sphincter for grade 3 DESD Refractory detrusor hyperreflexia can be eradica
ted by intra-detrusor injection of botox Reversible effect and possibilty of antibody form
ation after repeated injection Cost-benefit should be weighed
排尿障礙治療中心 版權所有
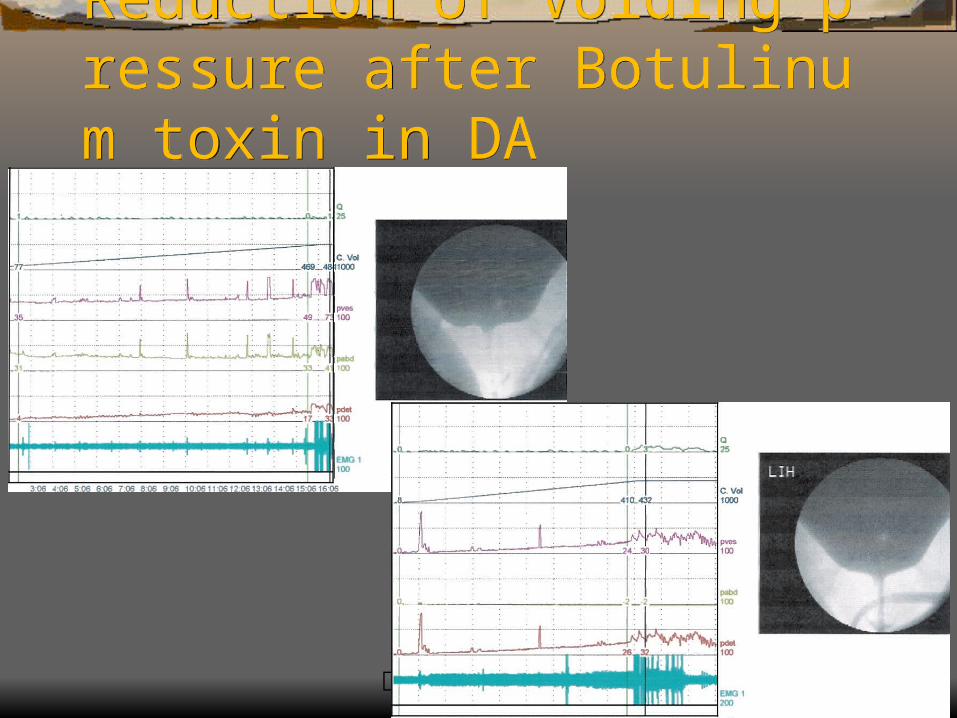
Reduction of Voiding pressure after Botulinum toxin in DAReduction of Voiding pressure after Botulinum toxin in DA
排尿障礙治療中心 版權所有
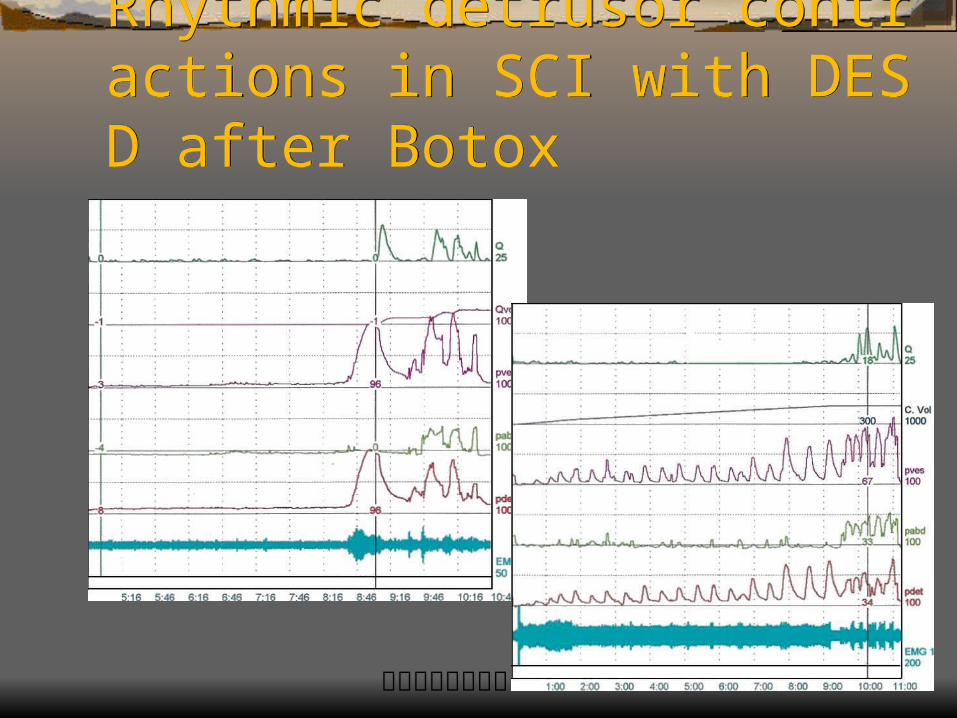
Rhythmic detrusor contractions in SCI with DESD after Botox
Rhythmic detrusor contractions in SCI with DESD after Botox
排尿障礙治療中心 版權所有
Botulinum A Toxin Detrusor Injection for Detrusor HyperreflexiaBotulinum A Toxin Detrusor Injection for Detrusor Hyperreflexia 5 IU/Kg Botox (Botulinum A toxin) was injected t
o 30 sites into detrusor muscle Decreased detrusor pressure and increased cyst
ometric capacity after Botox Increased residual urine and CISC is needed Abdominal tapping to void Indicated in refractory detrusor hyperreflexia
排尿障礙治療中心 版權所有
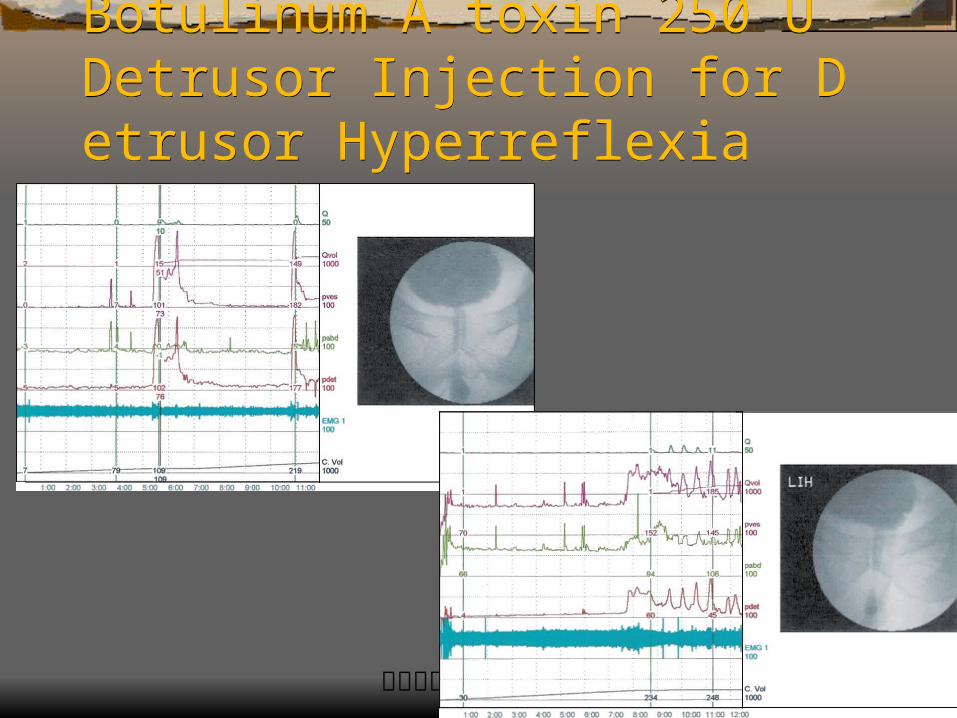
Botulinum A toxin 250 U Detrusor Injection for Detrusor Hyperreflexia
Botulinum A toxin 250 U Detrusor Injection for Detrusor Hyperreflexia
排尿障礙治療中心 版權所有
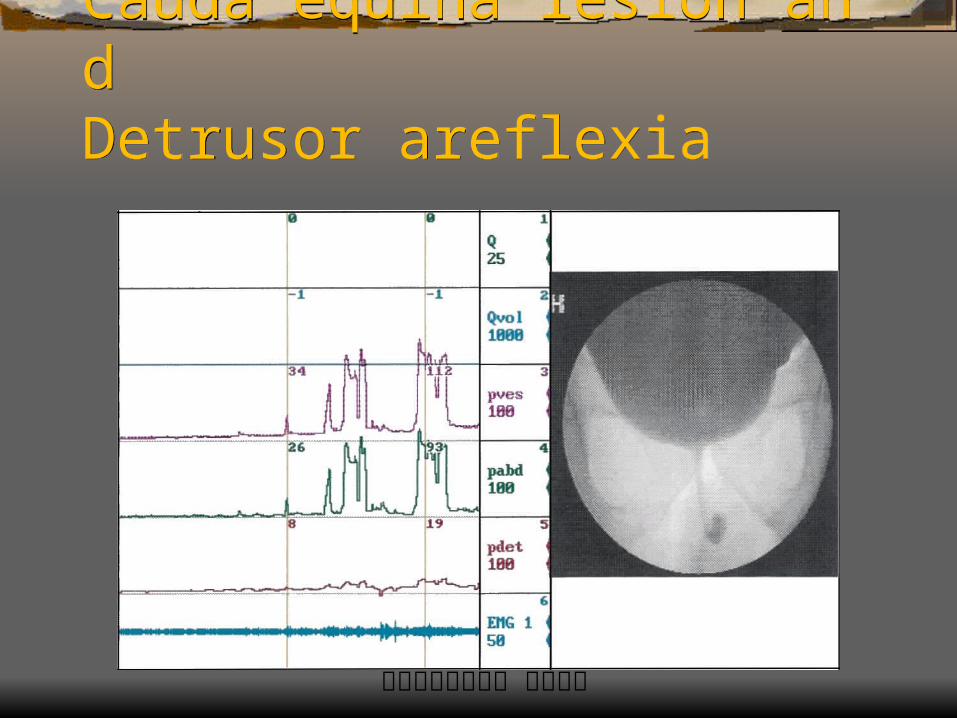
Cauda equina lesion andDetrusor areflexiaCauda equina lesion andDetrusor areflexia
排尿障礙治療中心 版權所有
Grade 1 DESD in a SCI WomenGrade 1 DESD in a SCI Women
排尿障礙治療中心 版權所有
Grade 1 DESD in Cervical SCIGrade 1 DESD in Cervical SCI
排尿障礙治療中心 版權所有
Failure of Pharmacological MxFailure of Pharmacological Mx Presence of vesicoureteral reflux Severe bladder fibrosis and trabeculation Presence of severe bladder outlet obstruction Severe outlet incompetence Azotemia or renal failure No improvement in quality of life
排尿障礙治療中心 版權所有
Surgical treatment for complications of chronic SCI
Surgical treatment for complications of chronic SCI
External sphincterotomy and urethral stent Augmentation cystoplasty Bladder autoaugmentation Continent urinary reservoir formation (Kock pouch) Pubovaginal sling procedure Continent cystostomy Ureteral reimplantation
排尿障礙治療中心 版權所有
External SphincterotomyExternal Sphincterotomy Indicated in quadriplegic patients with DESD Potentially not result in total incontinence Urinary tract infection can be eliminated Free of catheterization Re-do is possible in 25% patients with inadequat
e sphincter relaxation or scarring 25- 30 % may have persistent hydronephrosis
排尿障礙治療中心 版權所有
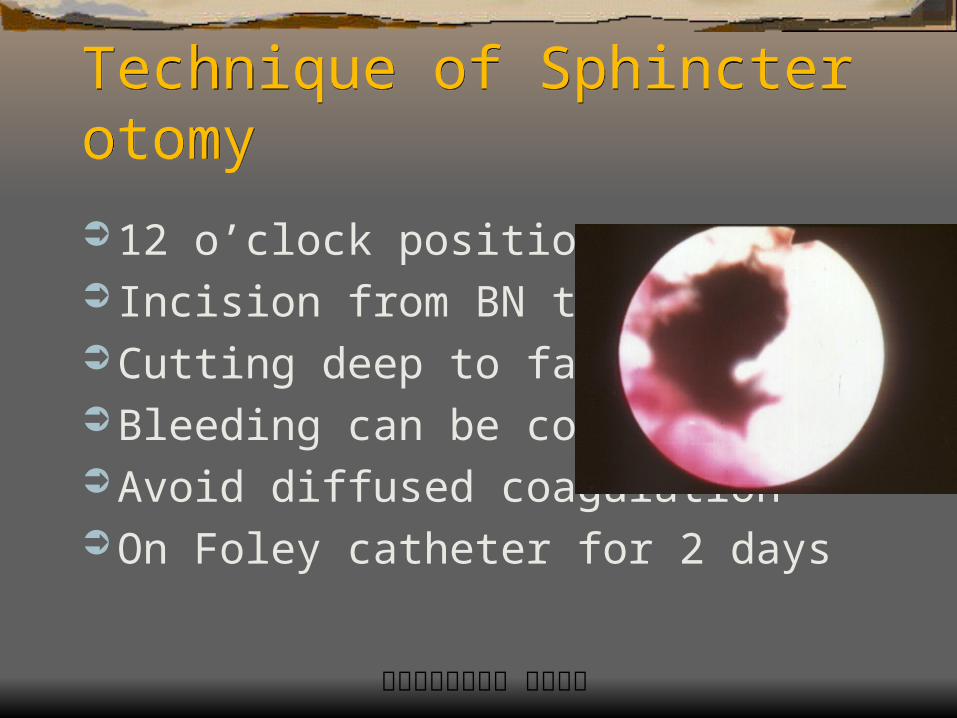
Technique of SphincterotomyTechnique of Sphincterotomy 12 o’clock position Incision from BN to bulbous Cutting deep to fat & vessel Bleeding can be controlled Avoid diffused coagulation On Foley catheter for 2 days
排尿障礙治療中心 版權所有
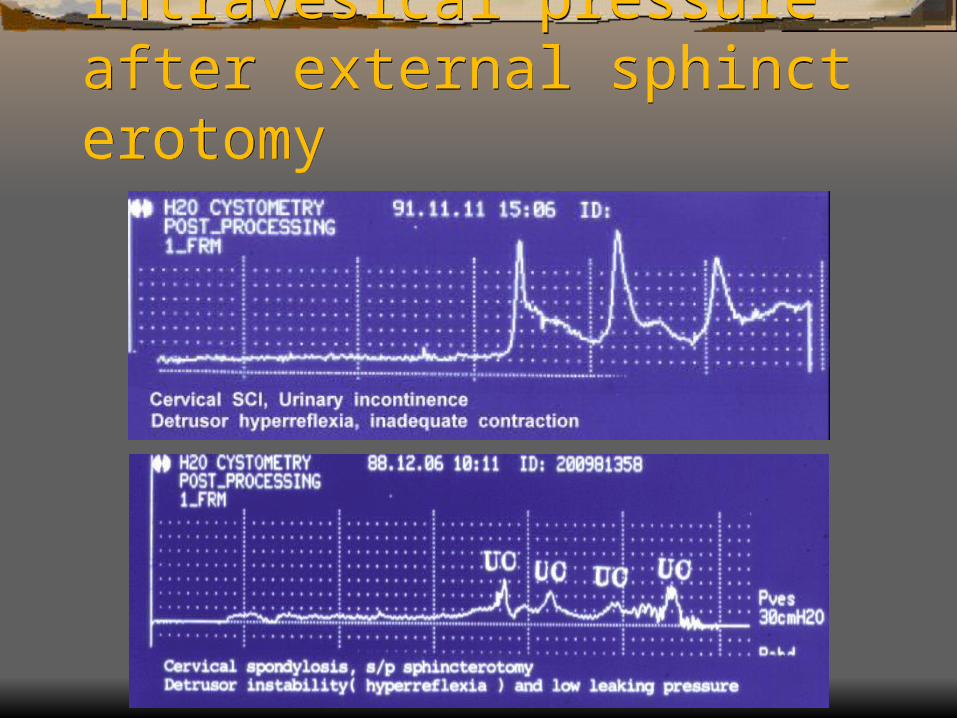
Intravesical pressure after external sphincterotomy
Intravesical pressure after external sphincterotomy
排尿障礙治療中心 版權所有
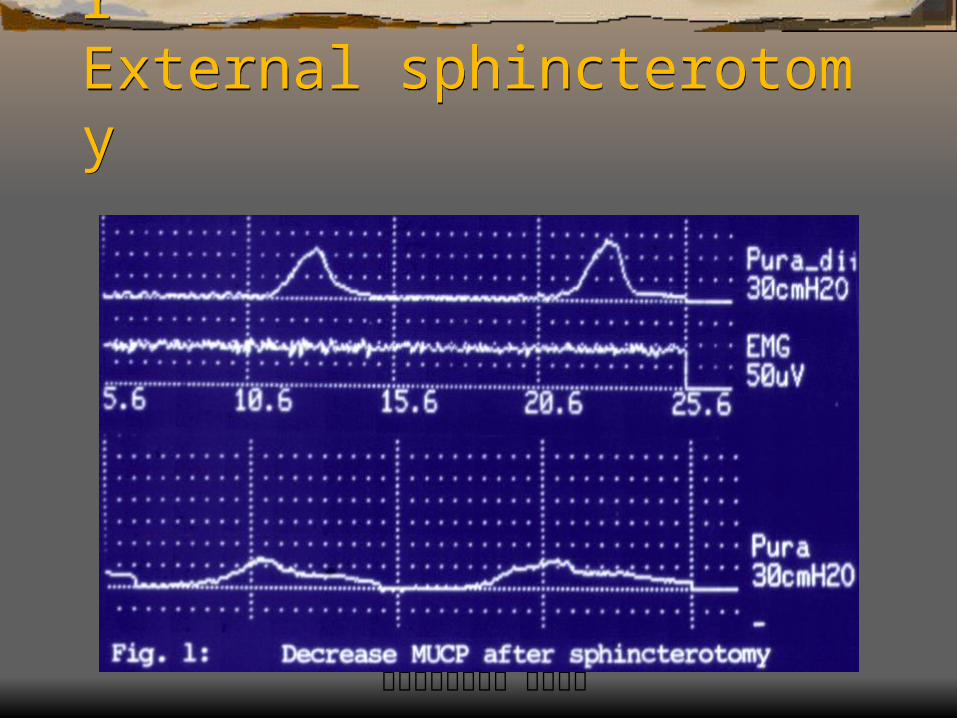
Reduction in MUCP afterExternal sphincterotomyReduction in MUCP afterExternal sphincterotomy
排尿障礙治療中心 版權所有
Urethral StentUrethral Stent Indwelling a distensible urethral stent for scarred
membranous or severe DESD refractory to sphincterotomy
Complication should be weighed: stone formation, stent erosion, persistent UTI, total incontinence
Only 2/11 longer follow-up patients needed to be removed
排尿障礙治療中心 版權所有
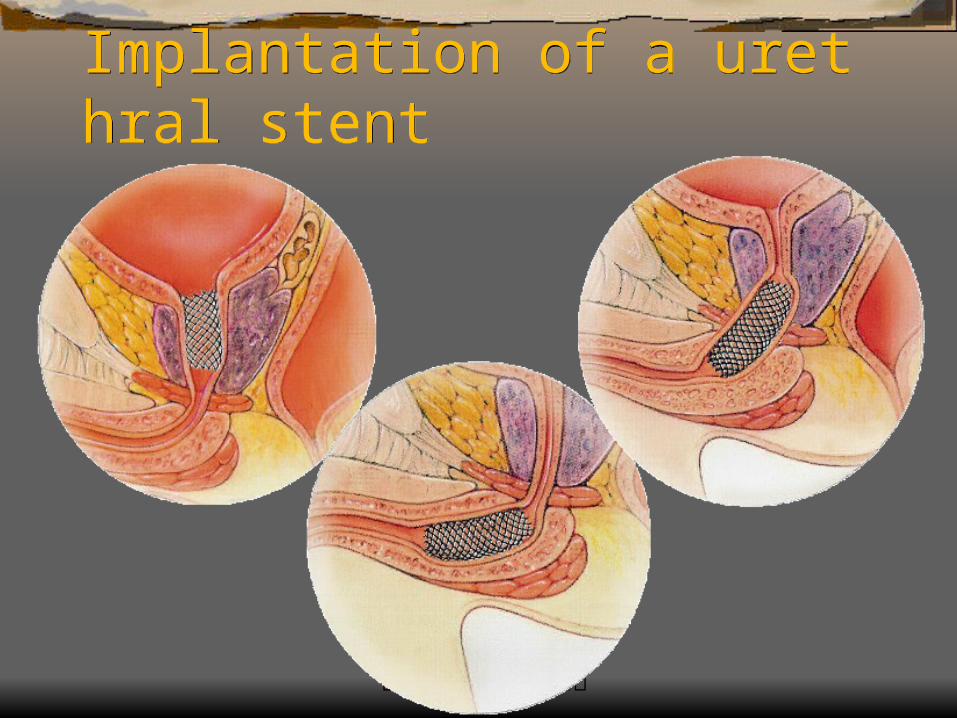
Implantation of a urethral stentImplantation of a urethral stent
排尿障礙治療中心 版權所有
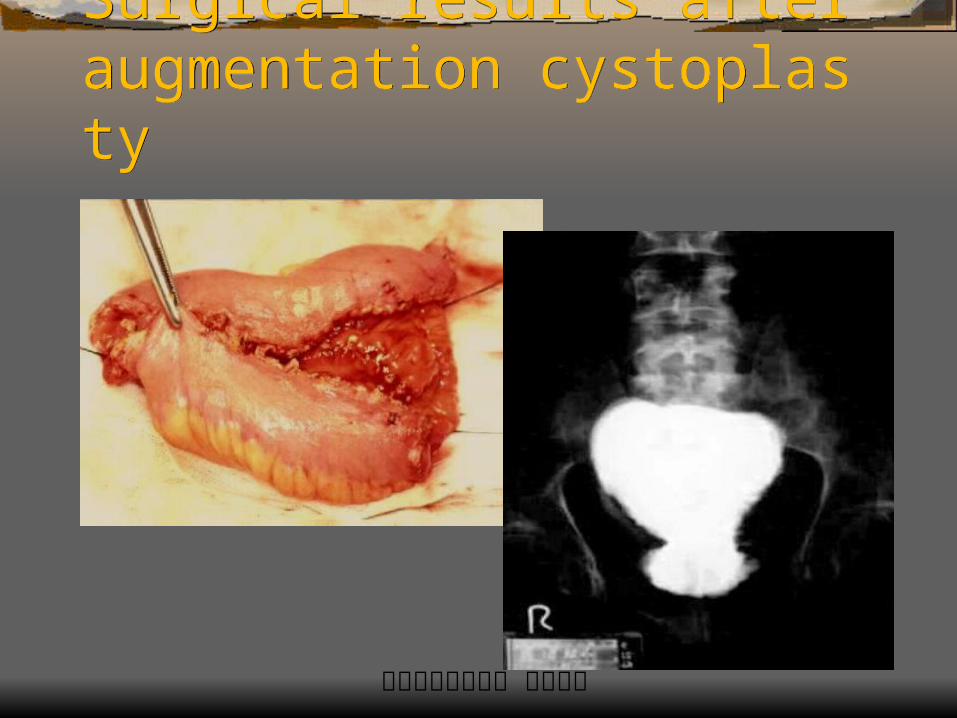
Augmentation cystoplastyAugmentation cystoplasty A bladder capacity of less than 250ml Overflow incontinence and large residual urine Presence of hydronephrosis Azotemia and frequent pyelonephritis Patient is able to catheterize by himself Side effect or refractory to pharmacological thera
py
排尿障礙治療中心 版權所有
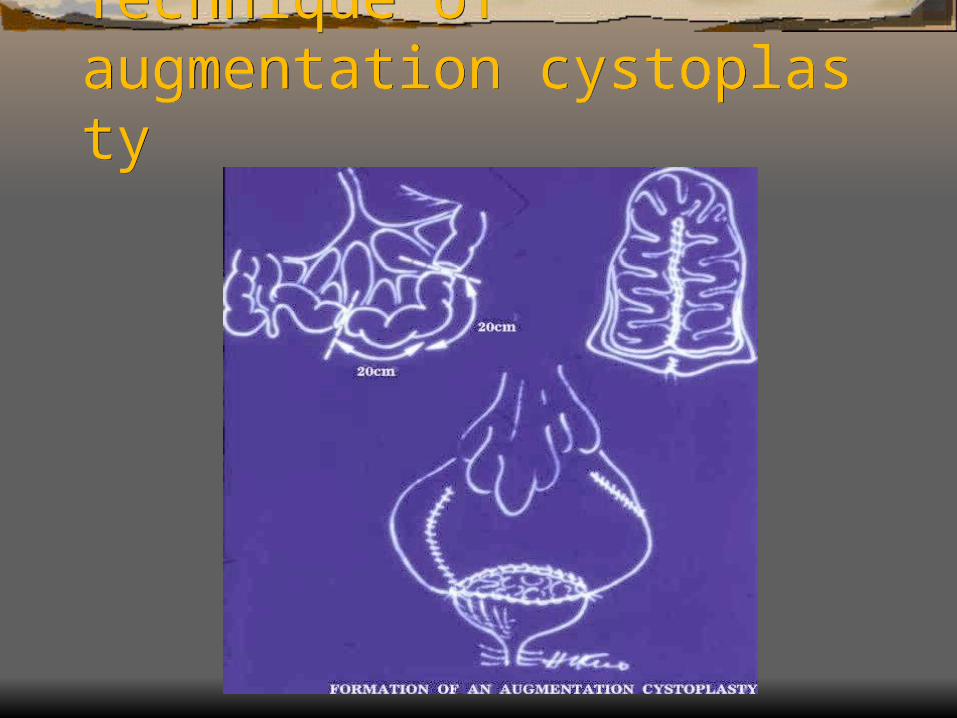
Technique of augmentation cystoplastyTechnique of augmentation cystoplasty
排尿障礙治療中心 版權所有
Surgical results after augmentation cystoplastySurgical results after augmentation cystoplasty
排尿障礙治療中心 版權所有
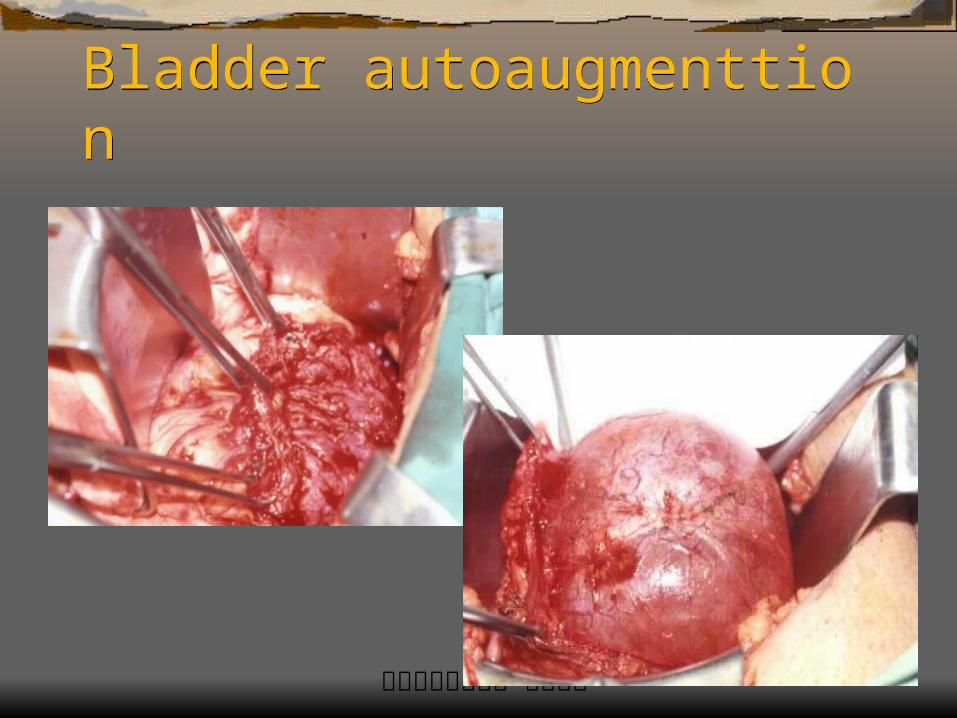
Bladder autoaugmentationBladder autoaugmentation Partial myomectomy of bladder wall Increase bladder compliance and capacity by dis
tensible bladder mucosa Less surgical morbidity and complication Secondary fibrosis and reduced capacity after lo
ng-term follow-up Serve as first line surgical procedure for SCI
排尿障礙治療中心 版權所有
Bladder autoaugmenttionBladder autoaugmenttion
排尿障礙治療中心 版權所有
Ureteral reimplantationUreteral reimplantation Not suitable in trabeculated bladder High failure rate after ureteral reimplantation or c
ollagen injection Contraindicated in SCI patients with DESD & AD Combined augmentation and anti-reflux procedu
re is a better way
排尿障礙治療中心 版權所有
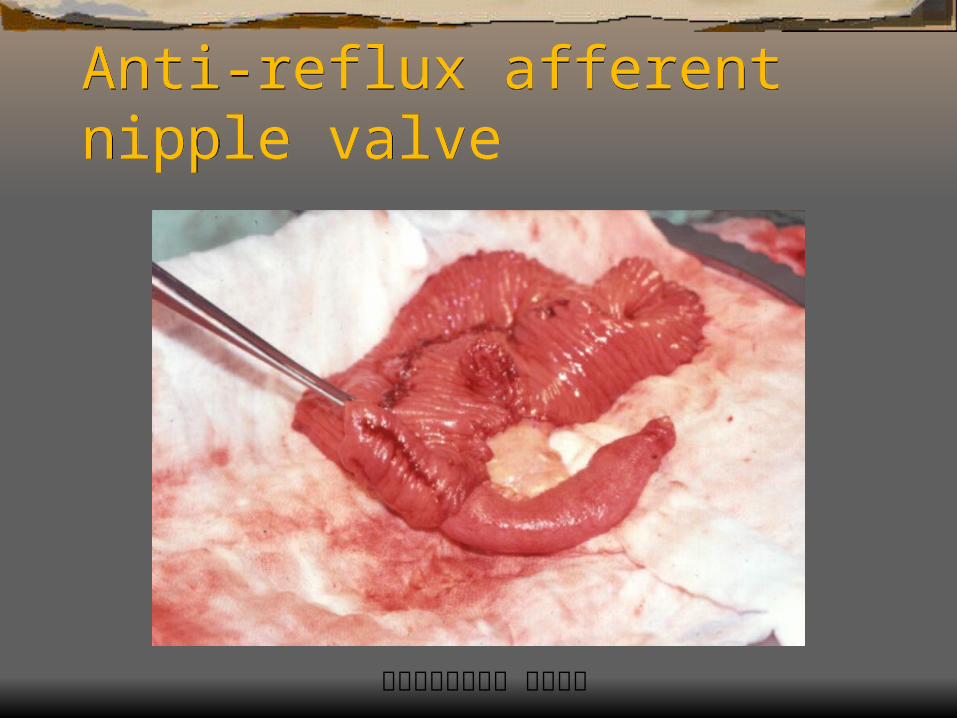
Anti-reflux afferent nipple valveAnti-reflux afferent nipple valve
排尿障礙治療中心 版權所有
Continent Reservoir (Kock pouch)Continent Reservoir (Kock pouch) Creation of a continent reservoir by a 40-cm seg
ment of ileum Detubularization and double folded ileum can ha
ve a volume of 600ml Anti-reflux and anti-incontinence nipple valves Self-catheterization is needed Suitable for female SCI with good hand function
排尿障礙治療中心 版權所有
Sonography of Kock pouchSonography of Kock pouch
排尿障礙治療中心 版權所有
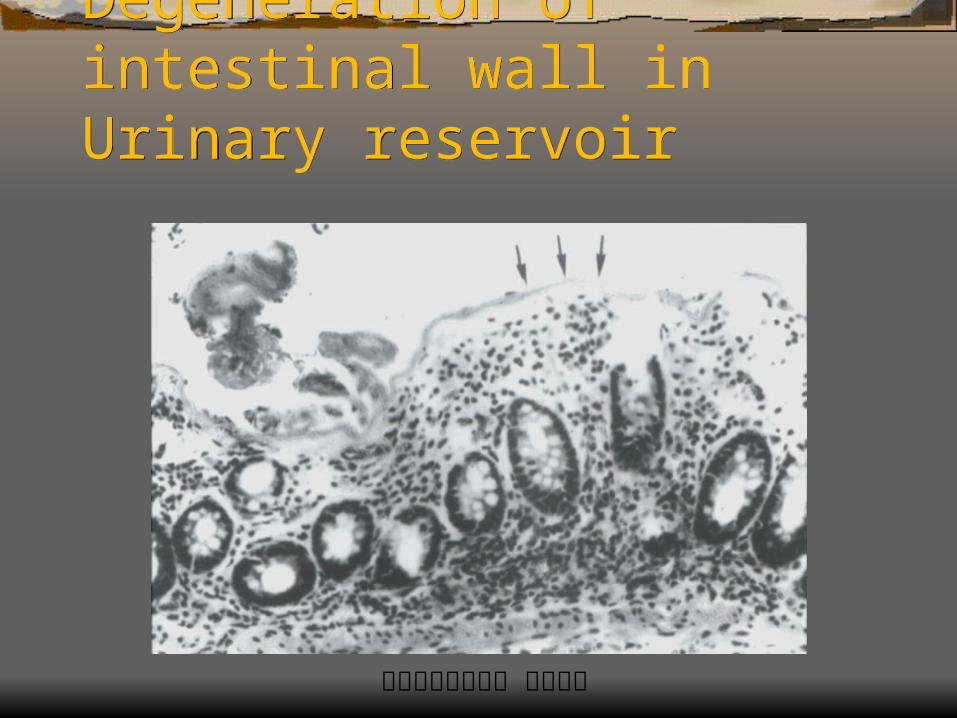
Degeneration of intestinal wall in Urinary reservoirDegeneration of intestinal wall in Urinary reservoir
排尿障礙治療中心 版權所有
Transurethral injectionTransurethral injection Transurethral injection of botulinum toxin may re
duce sphincteric tone and facilitate voiding in SCI with DESD or detrusor areflexia
Transurethral injection of collagen or Teflon paste may bulk sphincter and increase urethral tone, eliminate incontinence in lower level SCI
Other new devices implant into bladder neck or sphincteric urethra to combat incontinence
排尿障礙治療中心 版權所有
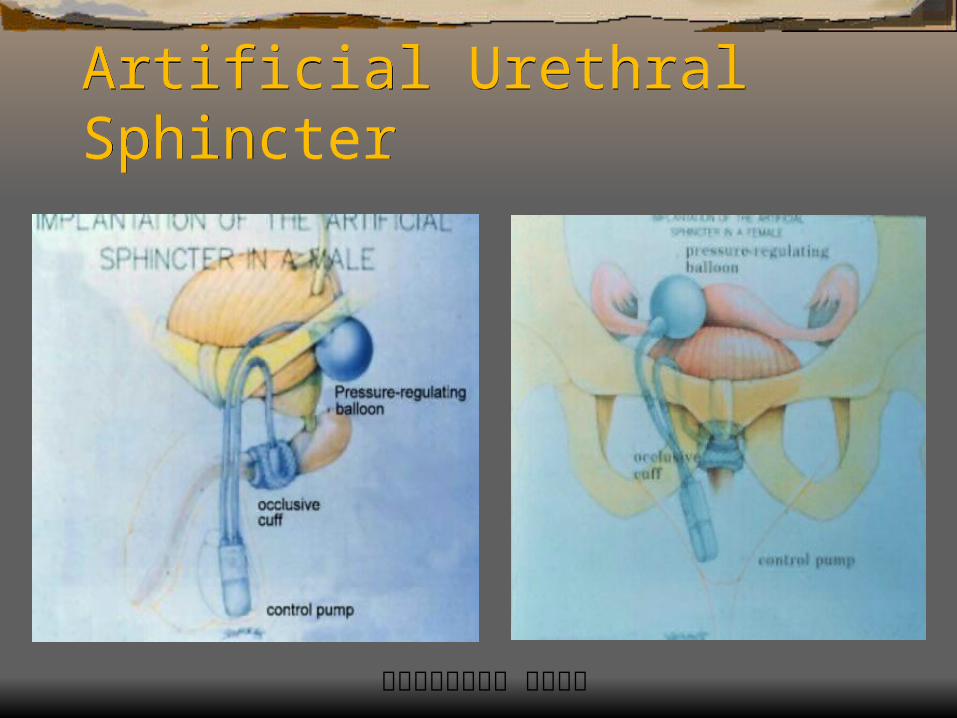
Artificial Urethral SphincterArtificial Urethral Sphincter
排尿障礙治療中心 版權所有
Artificial Urethral Sphincter Artificial Urethral Sphincter 95% in the NVD patients (half of 250) receiving
AUS implantation became continent, 78% at the first AUS attempt
Revision rate in neurogenic voiding dysfunction is 33%
Annual incidence of erosion was 5% Overall success rate was 77%,revision rate 59%
in 107 children