Embed Size (px)
Citation preview

S
Health PromotionThe Final Objective Set
What is Health Promotion
Health promotion is the process of enabling people to increase control over, and to improve, their health.
It moves beyond a focus on individual behavior towards a wide range of social and environmental interventions.
What is Health Promotion
Health Promotion initiatives comes in many different forms, but the main purpose is to encourage individuals to take preventive measures to avert the onset or worsening of an illness or disease and to adopt healthier lifestyles.
The Heath Promotion Research looks to find empirically based interventions that promote healthy lifestyles and tests these interventions in the community, especially among populations disproportionately burdened with chronic disease.
What is the aim ofHealth Promotion?
The aim of health promotion is to help an individual or group reach a state of complete physical, mental and social well-being. It involves an individual or group being able to:
• Identify and understand biological risk factors for certain health-related disorders
• Understand cognitive factors that influence and treat/prevent health related disorders.
• Change with the environment/culture/lifestyle of individuals suffering from or looking to prevent health-related disorders
Health promotion makes it possible for people to increase control over the determinants of health and thereby improve their health.
Behavioral Change Models
There are many different theories that guide health promotion interventions
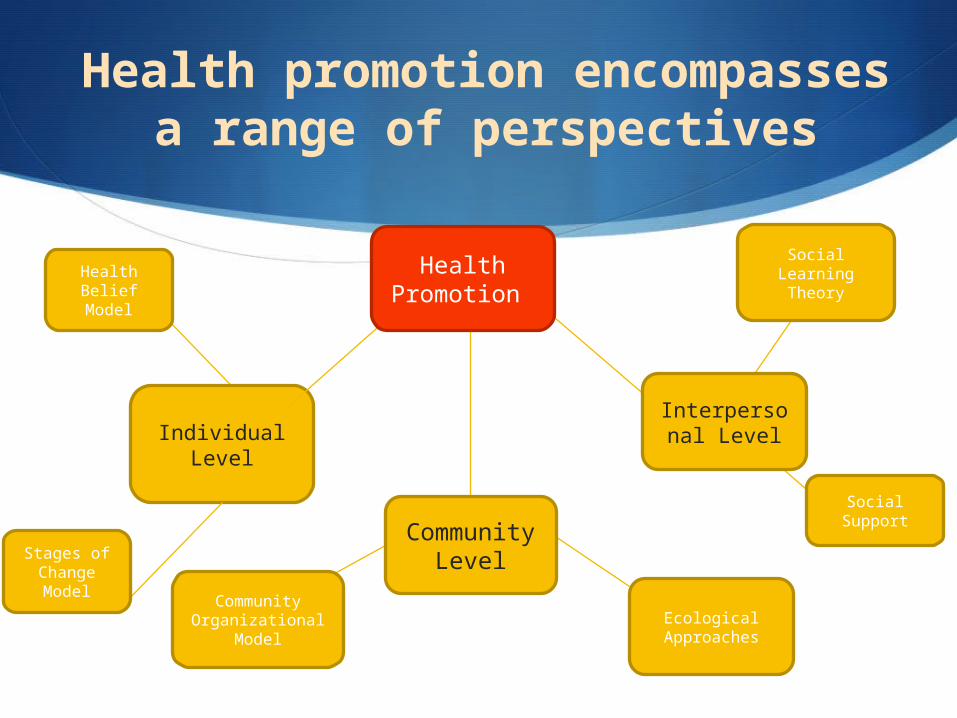
Most theories are based on one of three levels: Individual Level Community Level Interpersonal Level
Different approaches to health promotion tap into different theoretical perspectives and academic disciplines
Behavioral Change Models
No one theory or model can address all variables that contribute to a person’s behavior, and not all theories are applicable to all situations. But elements of different theories may be combined to create a program tailored for a specific issue and target population (such as programs that include considerations from each level of analysis).
Social LearningTheory
Community Organizational
ModelEcological
Approaches
Health promotion encompasses a range of perspectives
Health Belief Model
Individual Level
Stages of Change Model
Interpersonal Level
Social Support
Community Level
Health Promotion
S
Objective 4.1Examine models and theories of health promotion (Be ready to evaluate one specific theory as well)
How should you approach this objective
Understand the command term Examine: Consider the theory/model in a way that uncovers
the assumptions and interrelationships of the issue (how model relates to the promotion of health)
This command term is descriptive (not analytical)
Types of Health Promotion Models
Health Belief Model
Stages of Change Theory
Social Learning Theory
Theory of Reasoned Action
Social Support
Health Belief Modela cognitive approach
History and Orientation
The Health Belief Model (HBM) is a psychological model that attempts to explain and predict health behaviors.
This is done by focusing on the attitudes and beliefs of individuals. The HBM was first developed in the 1950s by social psychologists Eugene Rosenstock and Kegels working in the U.S. Public Health Services.
Health Belief Modela cognitive approach
History and Orientation
The HBM is currently one of the most widely used models for Health Promotion. Since its origin, it has been used in various health promotional strategies.
It has also been adapted to explore a variety of long- and short-term health behaviors, including sexual risk behaviors obesity, addictions and others.
Core Assumptions of HBM
The Health Belief Model has four major assumptions.
1. Perceived SusceptibilityPeople will not change their health behaviors unless they believe that they are at risk.Those who does not think that they are at risk of acquiring becoming overweight will not stop overeating.
2. Perceived SeverityThe probability that a person will change his/her health behaviors to avoid a consequence depends on how serious he or she considers the consequence to be. In other words, if a alcoholic doesn’t feel like the problem is severe, they will not seek help.
Core Assumptions of HBM
The Health Belief Model has four major assumptions.
3. Perceived BenefitsIt's difficult to convince people to change a behavior if there isn't something in it for them. If the addict does not feel like quitting the substance or process will benefit them, quitting is highly unlikely.
4. Perceived BarriersOne of the major reasons people don't change their health behaviors is that they think that doing so is going to be hard (both socially, cognitively and biologically). Many weightless programs are difficult, thus the perceived barriers usually stop “yo-yo diets” in their tracks.
Core Assumptions of HBM
Other components of HBM
Cues to actionExternal influences promoting the desired behavior, may include information provided or sought, reminders by powerful others, persuasive communications, and personal experiences
Self-efficacyConfidence in one's ability to take action
Appraisal of HBM
Strengths
“User friendly” constructs easy for non-psychologists to assimilate and apply. Which speaks to its wide range use in many health issues.
The cognitive component of HBM has stood the test of empirical time. Large body of data/many meta-analyses have been done to test for reliability.
Perceived cost/benefit component has been applied to many theories related to addiction relapse and obesity relapse.
Appraisal of HBM
Limitations
Neglects the significant social component of health-related illnesses (such as social learning and unlearning, cultural factors, etc.)
Blames the “individual” when factors beyond the individual may be causing the illness (genetic factors, biological factors, etc.)
Stages of Change Model
The Stages of Change Model was originally developed in the late 1970's and early 1980's by James Prochaska and Carlo DiClemente at the University of Rhode Island when they were studying how smokers were able to give up their habits or addiction.
Although this theory was originally applied to addictions, it has also been applied to obesity/stress and overeating health promotional strategies.
Stages of Change Model
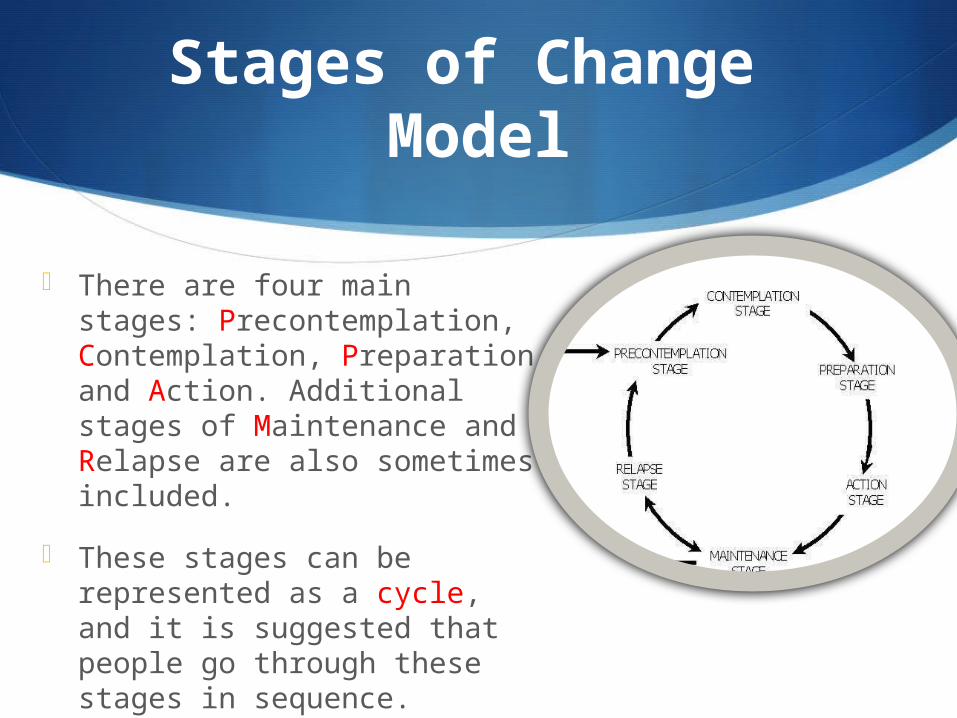
There are four main stages: Precontemplation, Contemplation, Preparation and Action. Additional stages of Maintenance and Relapse are also sometimes included.
These stages can be represented as a cycle, and it is suggested that people go through these stages in sequence.
Stages of Change Model
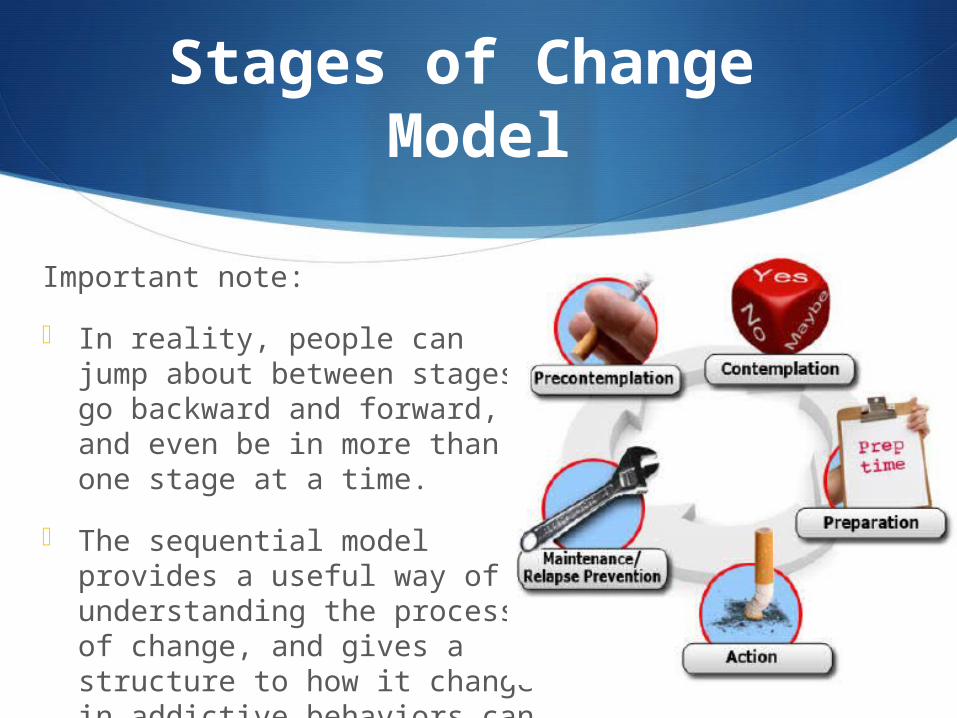
Important note:
In reality, people can jump about between stages, go backward and forward, and even be in more than one stage at a time.
The sequential model provides a useful way of understanding the process of change, and gives a structure to how it change in addictive behaviors can be encouraged and managed.
Stages of Change Model
HOW DO PEOPLE MOVE FROM ONE STAGE TO ANOTHER?
Important note:
In reality, people can jump about between stages, go backward and forward, and even be in more than one stage at a time.
The sequential model provides a useful way of understanding the process of change, and gives a structure to how it change in addictive behaviors can be encouraged and managed.
The model also relies on cognitive factors to move into progressive and digressive stages.
Read more: http://www.uri.edu/research/cprc/TTM/detailedoverview.htm
Ecological use of the model
Stress Management
The Stages of Change Model has been applied to many stress treatment programs.
A national sample of pre-Action adults was provided Pro-Change’s Stress Management intervention. At the 18-month follow-up, a significantly larger proportion of the treatment group (62%) was effectively managing their stress when compared to the control group.
The intervention also produced statistically significant reductions in stress and depression and an increase in the use of stress management techniques when compared to the control group.
Ecological use of the model
Weight Management
When applied to weight management programs, pre-action treatment groups showed significant action when the model was used in conjunction with exercise and lifestyle change.
Smoking Cessation
Multiple studies have found individualized interventions tailored on the SCM model produced long-term abstinence rates within the range of 22% – 26%.
These interventions have also consistently outperformed alternative interventions including best-in-class action-oriented self-help programs.
Other Health Promotion Strategies
Social Learning Theory
Theory of Reasoned Action
Social Support
Read more:http://azrapeprevention.org/sites/azrapeprevention.org/files/2008_01_UA.pdf
S
Tomorrow…• The last (new) lecture!