Embed Size (px)
Citation preview

الله بسمالرحيم الرحمن

Identifying The Patient For
Thrombolysis Or Thrombectomy
ByAhmed Shafea Ammar
MD, FACC

Epidemiology
• >600,00 patients/ year in the US
• 50,000-200,000 deaths/ year in the US
• 3-month MR is 15-20%
• 10% of symptomatic PE are fatal at 1 hour
Semin Vasc Med 2001;1(2): 139-46


Diagnosis of Pulmonary Embolism

Most Common S&S of APE Among 2454 Patients in ICOPER Registry
Symptom or sign %
Dyspnea 82RR> 20/min 60HR>100 b/min 40Chest pain 49Cough 20Syncope 14Hemoptysis 7
Lancet 353:1386, 1999

Wells Clinical Bedside Scoring System for APE
Parameter Points
Clinical S&S of DVT 3
An alterative diagnosis is less likely 3
HR > 100 1.5
Immobilization or surgery within 4 weeks 1.5
Previous DVT/PE 1.5
Hemoptysis 1
Malignancy 1
Score (< 4) APE is less likely
Score (> 6) is a high probability
Thromb Haemost 83:416, 2000

Diagnostic work up in PE
High risk Intermed. risk Low risk
Test Sensitivity Specificity ppv npv ppv npv ppv npv
(%) (%)
Helical CT 77 89 96 52 73 91 20 99
MRI 77 87 96 51 70 91 17 99
TTE 68 89 96 43 70 88 18 99
TEE 70 81 93 43 59 88 12 99
D-dimer 89 59 89 60 46 93 7 99
V/Q 98 10 80 58 30 93 3 99
Am Fam Physcian 2004, 162: 1245-8

Risk Stratification
The 3 main pillars for risk stratification are : 1- Assessment of Clinical & haemodynamic status of the patient 2- Evidence of RV strain & infarction 3- Evidence of RV dilatation & dysfunction


Risk Stratification
1- Clinical Signs Geneva Score Index Clinical evidence of RVD : JV distension TR ↑ P2 LPS impulse
2- ECG Signs RV strain (T ↓ in v1 – v4) New RBBB S1Q3T3

The Geneva Score for PE PrognosisVariable Point Score No of Points % of Pts with adverse outcome
Cancer +2 0 0
CHF +1 1 2.5Prior DVT +1 2 4.1 Hypotension +2 3 17.8Hypoxemia +1 4 27.3DVT on US +1 5 57.1 6 100
Throm Haemost 84:548, 2000


Risk Stratification
3- Echocardiographic Signs
* Direct visualization of a large thrombus In the main PA (TEE)
* RV dilatation
* TR
* RV hypokinesis sparing the apex (Mac Connell sign)
* IVS flattening
* PH ± PA dilatation
* Lack of inspiratory collapse of IVC
Outcomes with RV Dysfunction
• 2-fold ↑ 14-day MR• 3-fold ↑1-year MR• ↑ risk of PE recurrence
• ?Increased risk of in situ thrombosis in RV and
Circulation 2002;121:877

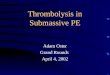
SAX view
Note marked RV dilatation & IVS flattening during systole & diastole


Risk stratification
4- Spiral CT
A- RV dilatation relative to LV size. RV dilatation and pulmonary vascular obstruction
(≥ 40%) on chest CT is a predictor of eary death after
APE (Circulation 2005; 235(3): 798-803)
B- Saddle or large proximal thrombus in the main PA

Massive PE
Note the large thrombus burden in the main pul. branches


Risk stratification
5- Biomarkers :
Troponins,
Pro-BNP
BNP

Kucher, N. et al. Circulation 2003;108:2191-2194
Mechanism of cardiac biomarker level elevation in APE

Copyright ©2004 BMJ Publishing Group Ltd.
La Vecchia, L et al. Heart 2004;90:633-637
Relation between cTnI concentrations ( 0.6 ng/ml) on admission and mortality (%).

Copyright ©2004 BMJ Publishing Group Ltd.
La Vecchia, L et al. Heart 2004;90:633-637
Time course of cardiac troponin I (cTnI) concentrations in patients with a positive assay on admission.

Circulation 2003;107:2545

Management Strategies

What is the optimal management for such embolus??
Thrombolysis, Catheter or Surgical Thrombectomy

Copyright ©2003 American Heart Association
Kucher, N. et al. Circulation 2003;108:2191-2194
Pulmonary embolism management strategy

Thrombolysis in APE (State of The Art)
A meta-analysis of all randomized trials (11 trials including 748 pts) comparing thrombolytic therapy with heparin in patients with APE, provides no evidence for a benefit of thrombolytic therapy compared with heparin for the initial treatment of unselected patients with APE.
However a benefit is clear in those at highest risk of recurrence or death.
Whether patients with RVD and stable hemodynamics should receive fibrinolytic therapy is still unknown.
(Evid. Based Med., April 1, 2005; 10(2): 41 – 41)

Possible mechanisms by which thrombolysis decreases mortality in patients with RVD
1- May prevent progressive RVD by lysis of massive PA thrombi
2- May prevent the ongoing release of vasoactive factors, such as serotonin, that may cause worsening pulmonary vasoconstriction and RVF
3- May dissolve a significant amount of thrombi in the source (e.g., pelvic and leg) veins to prevent
recurrent emboli
NB. Patients with APE are eligible for thrombolysis, if they have new S&S within 2 weeks of 1st presentation
(Goldhaber S in Braunwald” Heart Disease 2005)

1,500,000 U/1 Hour streptokinase with heparin is more effective than heparin
alone in PE with heart failure
• Randomized trial intending to enroll 40 patients
• Massive PE, hypotension, and heart failure
• Stopped after 8 patients
Results
Group Outcome
SK+Heparin 0 of 4 died
Heparin 4 of 4 died
Autopsy in 3 of 4 revealed
evidence of RV infarct and no significant CAD
Jerjes-Sanchez et al. J Thromb Thrombolysis 1995;2:227-9

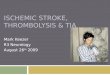
Konstantinides et al. NEJM 347 (15): 1143,October 10, 2002
Heparin + Altepase (118 pts) Heparin + Placebo (137 pts)

Before thrombolysis After thrombolysis
Note the change in RV size

NB. The risk of cerebral Hge is 1-2%

Contraindications for Thrombolytic Therapy
Absolute contraindications• Active internal bleeding• Recent spontaneous intracranial bleeding
Relative contraindications• Major surgery, delivery, organ biopsy or puncture of non-
compressible vessels within 10 days• Ischaemic stroke within 2 months• Gastrointestinal bleeding within 10 days• Serious trauma within 15 days• Neurosurgery or ophthalmologic surgery within 1 month• Uncontrolled severe hypertension (systolic pressure >180
mmHg; diastolic pressure >110 mmHg• Recent cardiorespiratory resuscitation• Platelet count <100 000/mm3, prothrombin time less than 50%• Pregnancy• Bacterial endocarditis• Diabetic haemorrhage retinopathy

Surgery or Thrombolysis
Registry of Massive PE with RV failure (n=37)
Surgical embolectomy Thrombolysis
(n=13) (n=24)
77% survival 67% survival
Recurrent PE in 1 Recurrent PE in 5
28% bleed rate
Gulba et al. Lancet 1994;343:576-7

Role of Surgery
47 patients, underwent emergency surgical embolectomy for massive central PE
The indications were (1) C/I to thrombolysis (45%), (2) failed medical treatment (10%), and (3) RVD (32%).
Preoperatively, (26%) patients were in cardiogenic shock, and (11%) were in cardiac arrest.
Mortality: (6%) operative & (12%) late deaths.Actuarial survival at 1 and 3 years was 86% and 83%, respectively.
Surgical pulmonary embolectomy can be done not only in patients with large central clot burden and H/D but also in H/D stable patients with RVD documented by means of echocardiography.
J Thorac Cardiovasc Surg 2005;129:1018-1023
•

Surgically-Removed Thrombus in Acute PE

Catheter embolectomy or Surgical embolectomy
Advantages Disadvantages Advantages Disadvantages
More accessible Distal embolization More control Less experience
Various tools Large clot burden Revascularize Need for if needed sternotomy
Limited Experience
No randomized trials

Catheter EmbolectomyInteventional catheterization techniques includes :
Mechanical fragmentation of thrombus with PA cath .
Clot pulverization with a rotating basket catheter.
Rheolytic thrombectomy.
Combination of mechanical fragmentation and thrombolysis.
Catheter embolectomy is hindered by devices that are designed normally to remove small arterial clots rather than decompressing massive PE.


Suction catheter embolectomy + full dose thrombolysis


SummaryPatients eligible for throbolysis or thrombectomy are those
who have Geneva score index (>4), ↑ S biomarkers, Echo signs of RVD and evidence of large thrombus burden on helical CT.
Thrombolytic therapy is indicated in patients with massive PE, as shown by shock or hypotension + RVD
The use of thrombolytic therapy in patients with sub-massive PE (RVD without hypotension) is controversial.
Thrombolytic therapy is not indicated in patients without right ventricular overload.
Surgical embolectomy is reserved for patients with massive PE (large thrombus burden) with C/I to thrombolysis and those having PTO or RV or RA thrmbus
Catheter embolectomy can be used for patients with massive PE (moderate thrombus burden & C/I to thrombolysis

Fibrinolytic therapy Clinical questions - a)Pathophysiology ManagementEpidemiology & costs - c)Fibrinolytic trials - d) - e)- b)
Please, do not rushAlways, weigh:
Please, do not rushAlways, weigh:
Safety Efficacy
Clinical questions - a) - e)

Ahmed Shafea MD, FACC