Embed Size (px)
Citation preview
© TANUVAS, 2011© TANUVAS, 2011
REPEAT BREEDING SYNDROME
© TANUVAS, 2011© TANUVAS, 2011
THE MOST VEXING PROBLEM FOR A VETERINARIAN!
© TANUVAS, 2011© TANUVAS, 2011
DEFINITION
A repeat breeder cow is defined as one • That has been bred 3 or more times but not conceived
• Has normal estrous cycle
• Is free from palpable abnormality
• Has no abnormal vaginal discharge
• Has calved atleast once and
• Is less than 10 years old
© TANUVAS, 2011© TANUVAS, 2011
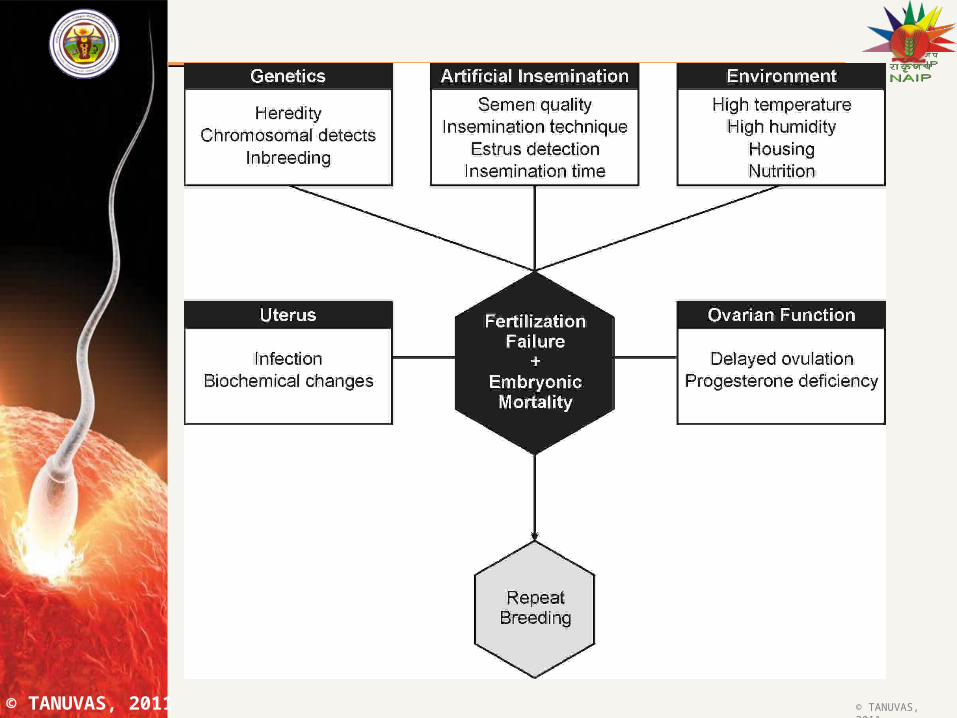
ETIOLOGY
FERTILIZATION FAILURE
EARLY EMBRYONIC DEATH
© TANUVAS, 2011© TANUVAS, 2011
© TANUVAS, 2011© TANUVAS, 2011
FERTILIZATION FAILURE ACCOUNTS FOR ABOUT 15 PER
CENT OF REPRODUCTIVE WASTAGE IN NORMAL COWS.
IN REPEAT BREEDER COWS THE FERTILIZATION FAILURE MAY BE HIGHER
AROUND 28-44 PER CENT.
FERTILIZATION FAILUREFERTILIZATION FAILURE
© TANUVAS, 2011© TANUVAS, 2011
Fertilization failures may be due to
Abnormalities in ovulation
Anovulation
Delayed ovulation
• Defective ovum
• Ageing of ovum- aged ova are viable only for few hours
• Inability of sperm to fertilize ovum
• Fertility of bull
• High sperm abnormality
• Low sperm motility
• Inflammation of genital tract
• Very early AI
© TANUVAS, 2011© TANUVAS, 2011
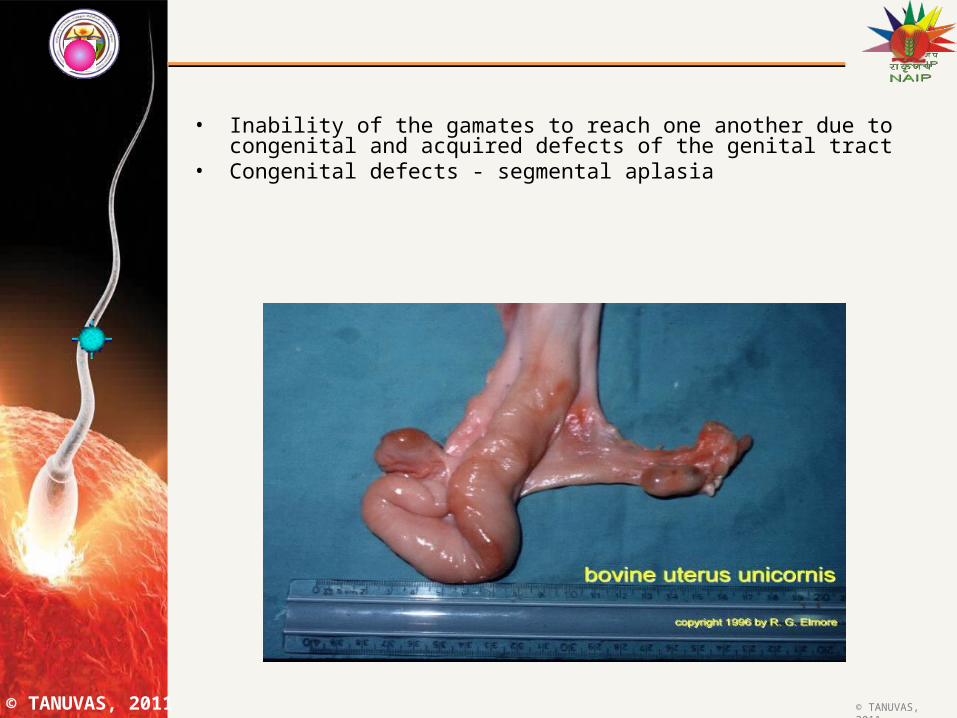
• Inability of the gamates to reach one another due to congenital and acquired defects of the genital tract
• Congenital defects - segmental aplasia
© TANUVAS, 2011© TANUVAS, 2011
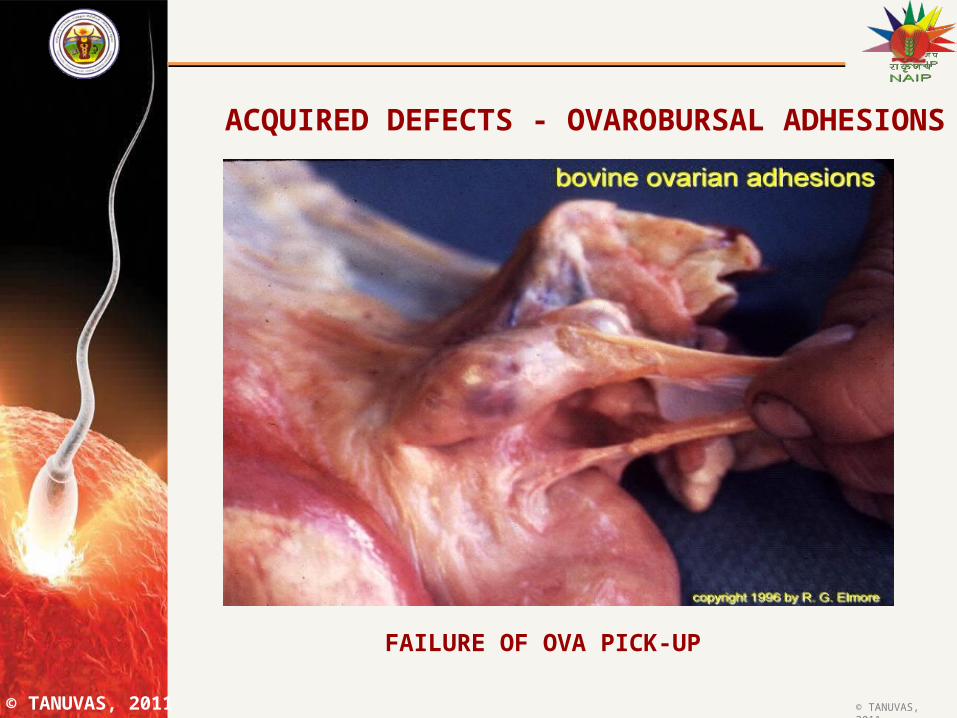
ACQUIRED DEFECTS - OVAROBURSAL ADHESIONS
FAILURE OF OVA PICK-UP
© TANUVAS, 2011© TANUVAS, 2011
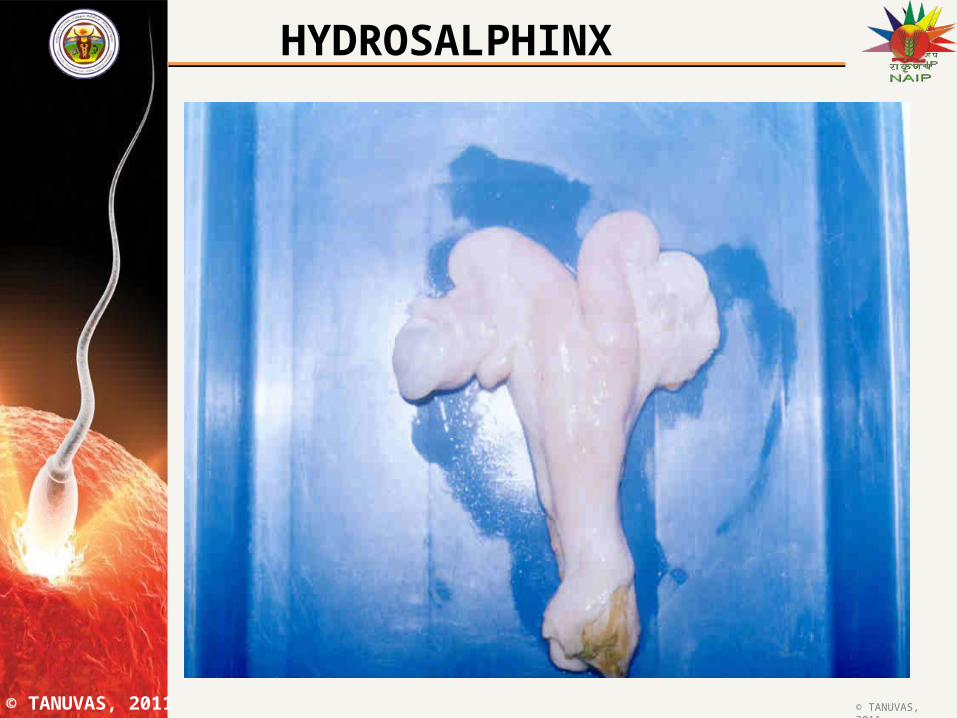
HYDROSALPHINX
© TANUVAS, 2011© TANUVAS, 2011
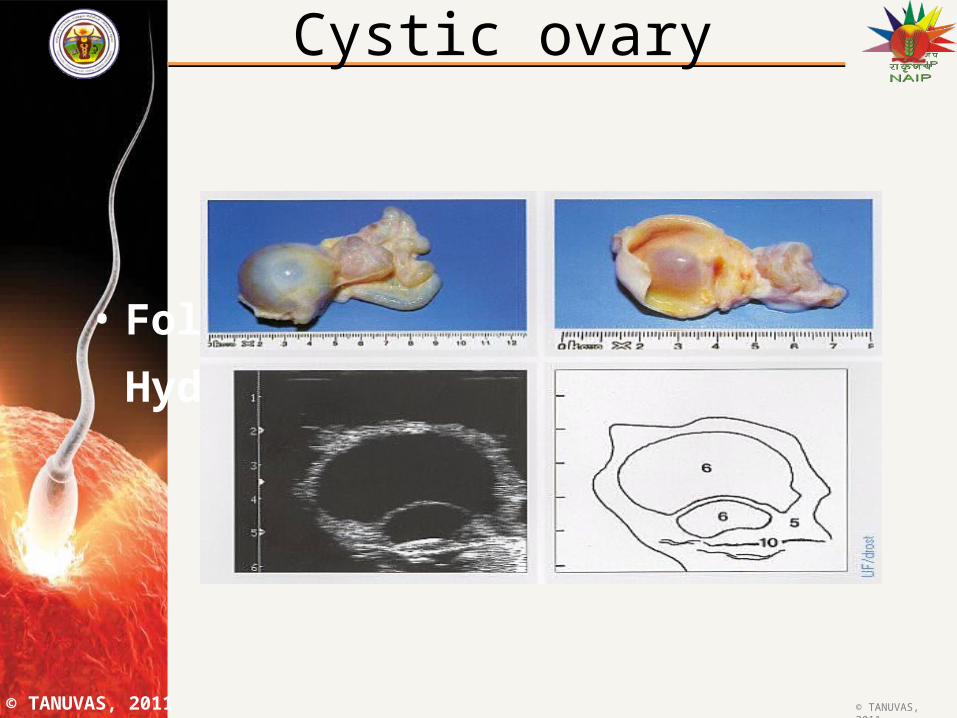
Cystic ovary
• Follicular Cyst and Hydrosalpinx.
© TANUVAS, 2011© TANUVAS, 2011
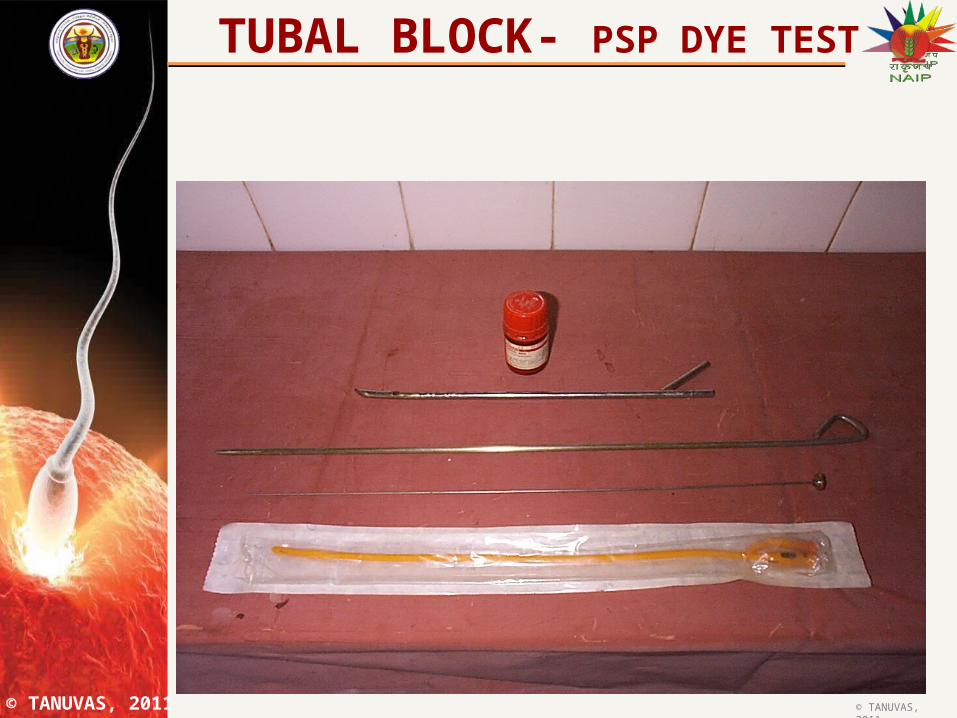
TUBAL BLOCK- PSP DYE TEST
© TANUVAS, 2011© TANUVAS, 2011
EARLY EMBRYONIC DEATH
• Accounts for 25% of reproductive wastage.
• Major portion of embryonic death occurs between days 8 and 19 after
breeding
• Most embryo death occurs before the critical stage of pregnancy recognition
and the cow will return to estrus at the normal 18-25 days interval
© TANUVAS, 2011© TANUVAS, 2011
Early embryonic death may be due to
Cytogenic abnormalities
• Critical requirement for embryo survival is the
presence of a normal complement of
chromosomes.
• Chromosomal aberrations-abnormal karyotypes
play a role in early embryo loss
© TANUVAS, 2011© TANUVAS, 2011
Unfavourable uterine environmentUterine environment can be affected by– Nutrition– Age of dam Ambient temperature Hormonal imbalance Infections
• Rectal examination• Vaginal speculum• White side test• Endometrial cytology• Endometrial biopsy

© TANUVAS, 2011© TANUVAS, 2011
Repeat breeding-Treatment
Bring the animal into +ve balance
– Additional concentrate ,greens
– Mineral supplemen
Check the semen quality. Use only high quality semen
© TANUVAS, 2011© TANUVAS, 2011
Timing of AISpin Brackiet test
Repeat AI
TREATMENT
© TANUVAS, 2011© TANUVAS, 2011
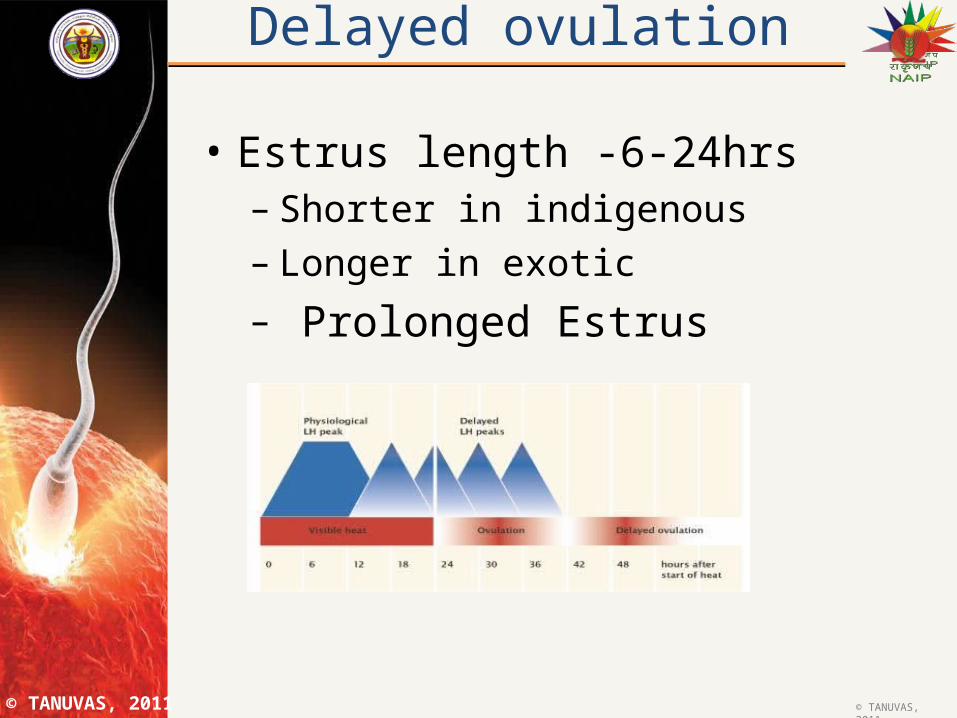
Delayed ovulation
• Estrus length -6-24hrs– Shorter in indigenous– Longer in exotic – Prolonged Estrus
© TANUVAS, 2011© TANUVAS, 2011
TREATMENT• 100 g of GnRH (20 g of GnRH analouge) OR
1000-1500 IU of LH at the time of AI
• 500 mg of depot progesterone on 5th day after AI or 1000-1500 IU of LH/GnRH on 6th day of cycle
• Skip AI, adm.PGF2 after 9-10 days and do fixed time AI at 72 and 96 hrs
• CIDR, ear implant or PRID application and fixed time AI twice at 48 and 72 hours
© TANUVAS, 2011© TANUVAS, 2011
PROSTAGLANDINS
• Prostaglandin F2 and its analogues • Cause functional and morphological
regression of CL • Estrus two to three days following inj.
© TANUVAS, 2011© TANUVAS, 2011
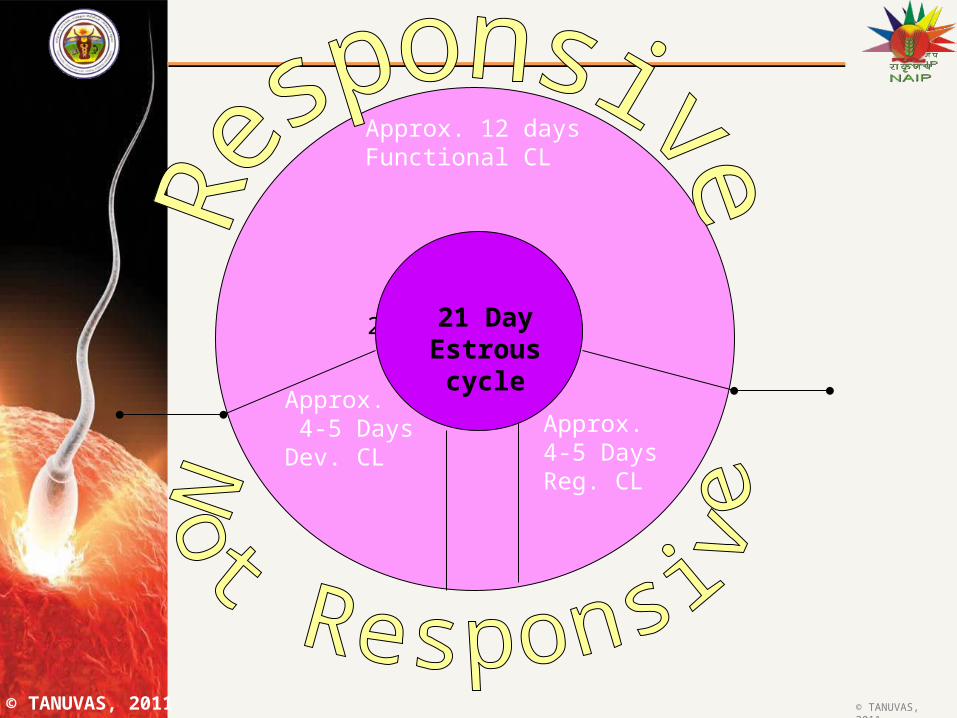
21 Day estrous Cycle
21 Day Estrous cycle
Approx. 12 daysFunctional CL
Approx. 4-5 DaysDev. CL
Approx.4-5 DaysReg. CL
© TANUVAS, 2011© TANUVAS, 2011
PRODUCTS• Cloprostenol (Estrumate) - synthetic analog.• Dinoprost tromethamine (Lutalyse) - synthetic PG F2 • similar to the natural product in the body.• Tiaprost (illiren) – synthetic analogue ADMINISTRATION• Intra muscular route
– Natural PGF2 - 25 mg– Synthetic analog - 0.5 mg
• Intra vulval sub mucosal route– Natural PGF2 - 10 mg– Synthetic analog - 0.2 mg
• Both routes are effective and have been found to give good conception rate.
© TANUVAS, 2011© TANUVAS, 2011
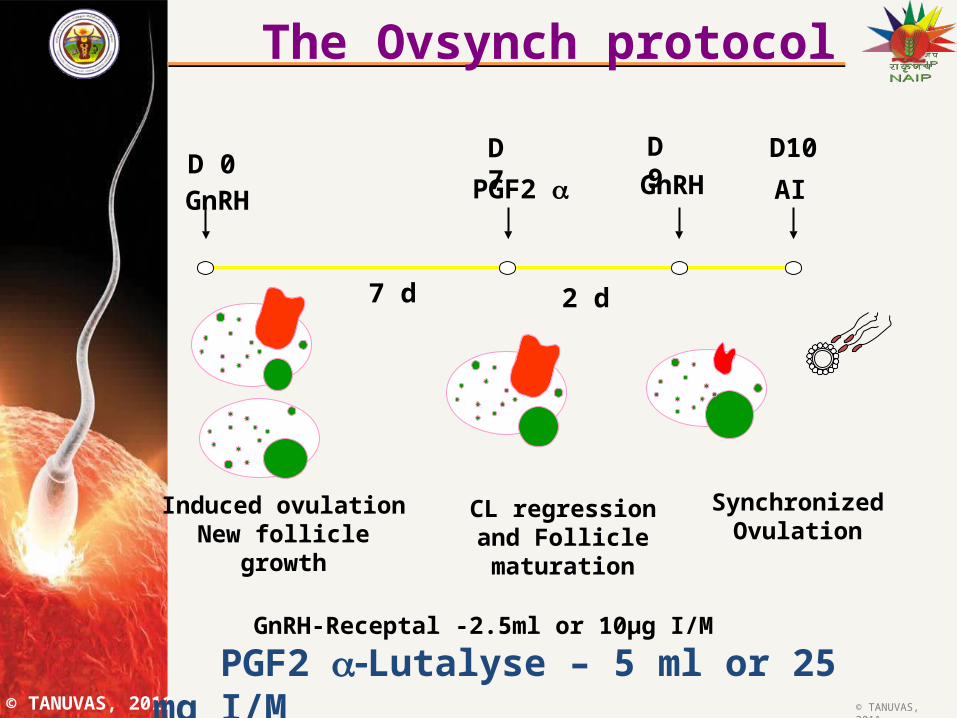
Induced ovulationNew follicle growth
CL regression and Follicle maturation
SynchronizedOvulation
GnRH GnRHPGF2 AI
7 d 2 d
D 0D 7 D 9 D10
The Ovsynch protocol
GnRH-Receptal -2.5ml or 10µg I/M
PGF2 Lutalyse – 5 ml or 25 mg I/M
© TANUVAS, 2011© TANUVAS, 2011
Conclusions
• Control of uterine infections
• Correct negative energy balance
• Correct timing of Aritificial insemination
• Assure quality of semen