Embed Size (px)
Citation preview

8/7/2019 0609 Case 1
http://slidepdf.com/reader/full/0609-case-1 1/4
C O M J U N E 2 0 0 9 C A S E 1
A 47-YEAR OLD MALE WITH A CEREBELLOPONTINE ANGLE
TUMORbpa_309 739..742
Klaus Bumm1; Abbas Agaimy2; Gerald Niedobitek2; Heinrich Iro1; Helmut Steinhart1
1 Department of O torhinolaryngology, University of Erlangen-Nuremberg, Germany2 Department of Pathology, University of Erlangen-Nuremberg, Germany
CLINICAL HISTORY AND IMAGINGSTUDIES
A 47-year-old male patient presented with a fluctuating hearing
impairment in his left ear over the past 5 years. Tinnitus or vertigo
was not observed. Audiometric analysis showed an inner ear deficit
of 50 dB between 1500 and 6000 kHz on the left side. Hearing in
the right ear was normal. The facial nerve was clinically and by
means of electrophysiological testing without pathological find-
ings. BEAP (brainstem evoked auditory potentials) revealed a
latency increase between J1 and J3 up to 2.5 ms for the left side,
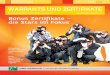
whereas only 2.3 ms on the right side. MRI (magnetic resonance
imaging) scanning showed a tumor of the cerebellopontine angle in
the left inner auditory canal (IAC) of 1.2 x 0.7 x 0.9 cm in size(Figure 1). After application of contrast media, the tumor showed
clear signal enhancement.
The tumor was entirely removed by a transtemporal approach to
the IAC. Surgical exploration found the cochlear nerve embedded
in a tumorous mass, whereas the vestibular and the facial nerve
were normal (Figure 2a, vestibular nerve arrow A and cochlear
nerve with tumor arrow B).
Nerve and tumor (Figure 2b) were removed and sent to histo-
pathological examination. The patient lost his hearing after the
operation due to the removal of the cochlear nerve, whereas a
regular postoperative vestibular function was observed. The post-
operative course as well as the 5-year follow-up examination was
unremarkable and control MRI scanning showed no recurrence.
PATHOLOGIC FINDINGS
Histopathological examination revealed a tumor composed of
loosely packed irregular nerve fibres embedded within loose con-
nective tissue (Figure 3a, H&E-stain, x 100). Mature adipose tissue
elements and numerous capillary- to medium-sized thin-walled
vascular channels were diffusely dispersed between nerve fibres. In
addition, isolated adipocytes were seen within the endoneurium of some nerve fibres, but no skeletal muscle cells, ganglionic cells,
glial elements or other tissue derivatives were seen. Also, hemosid-
erin pigment, scarring or inflammatory cells as would be antici-
pated in amputation (traumatic) neuroma were not observed.
Immunohistochemistry revealed a strong expression of protein
S100 and neurofilament protein in the nerve axons and Schwann
cells (Figure. 3b, x 100). An intact perineurial sheath was high-
lighted by reactivity for epithelial membrane antigen (Figure 3c,
EMA).
Figure 1.
doi:10.1111/j.1750-3639.2009.00309.x
739Brain Pathology 19 (2009) 739–742
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

8/7/2019 0609 Case 1
http://slidepdf.com/reader/full/0609-case-1 2/4
B
A
Figure 2.
Correspondence
740 Brain Pathology 19 (2009) 739–742
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

8/7/2019 0609 Case 1
http://slidepdf.com/reader/full/0609-case-1 3/4
B
A
C
Figure 3.
Correspondence
741Brain Pathology 19 (2009) 739–742
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

8/7/2019 0609 Case 1
http://slidepdf.com/reader/full/0609-case-1 4/4
DIAGNOSIS
Angiolipomatous hamartoma of the cochlear nerve
DISCUSSION
Most tumors of the cerebellopontine angle are schwannomas and
over 90% originate from the superior branch of the vestibular nerve. Tumors originating from the cochlear nerve are rare (1–3).
This case raises two major issues.The first one relates to the precise
allocation of the tumor to the affected nerve and the probable
histological diagnosis based on clinical and imaging findings. The
second issue concerns the pathogenesis of this peculiar lesion at
this unusual location.
The allocation of tumors to the cochlear nerve within the IAC is
most likely when they expand towards or even into the cochlea
(4–6). In this case there was no signal enhancement detectable
within the cochlea, so we did not presume a pathology arising
from the cochlear nerve. The only denominator was a progressive
hearing impairment, a non-specific symptom for cochlear nerve
involvement.After surgical exploration it became apparent that the
tumor was clearly originating from the cochlear nerve and associa-tion to the surrounding nerves could be excluded. This contrasts
with schwannomas of the vestibular nerve as they are known to
merge with surrounding nerves and therefore often hamper an easy
determination of their origin.
Since the majority of tumors originating in the IAC are schwan-
nomas, alternative diagnoses at this anatomic site seem quite
unusual. The histopathological differential diagnosis of our case
included traumatic neuroma, true circumscribed “palisaded”
neuroma, neuromuscular choristoma and lipomatous hamartoma
of the cochlear nerve. Schwannoma and neurofibroma could be
primarily excluded based on well defined criteria. Against a diag-
nosis of circumscribed neuroma argue the irregular borders of the
lesion and the prominent angiolipomatous component. Likewise,absence of a history of previous surgery or trauma of any kind, and
lacking of typical microfascicular pattern of traumatic neuroma as
well as signs of scarring, old bleeding and inflammatory cells pre-
clude a diagnosis of traumatic neuroma. A more plausible explana-
tion would be a non-traumatic “choristomatous” or “hamartoma-
tous” origin. In fact, the finely distributed adipocytic elements and
prominent vascular component represent a strong clue to the
choristomatous nature of the lesion. However, no skeletal muscle
fibers were seen, thus excluding a neuromuscular hamartoma
(choristoma) of cranial nerves.
Hamartomas of the IAC are exceedingly rare lesions and most
were described as case report or small series (7–9). Lesions
described by Wu et al (9) under the rubric of “lipochoristoma”
showed a heterogeneous histology, someof them contained skeletal
muscles and thus represent neuromuscular choristomas. Other rare
lesions described as lipomas of the IAC are probably lipomatous
hamartomas,as they were less circumscribed and lacked the encap-
sulation typical of true benign lipomatous tumors of the soft tissue.
However, given the finely dispersed fatty and vascular components
and absence of other tissue elements, we suggest the term “angioli-
pomatous hamartoma” for this peculiar lesion to alert to its high
vascularity that might suggest a more serious pathology onimaging procedures.
In summary, we described an unusual case that we believe to
represent the first description of an angiolipomatous hamartoma
of the cochlear nerve. The pathogenesis of this rare lesion at this
location remains unknown. Hamartomas should be included in
the pre-operative differential diagnosis of acoustic or vestibular
schwannoma.
REFERENCES
1. Brackmann DE, Bartels LJ (1980) Rare tumors of the cerebellopontine
angel. Otolaryngol Head Neck Surg 88:555–559.
2. Komatsuzaki A, Tsunoda A (2001) Nerve origin of the acoustic
neuroma. J Laryngol Otol 115:376–379.3. Alobid I, Gaston F, Morello A, Menendez LM, Benitez P (2002)
Cavernous hemangioma of the internal auditory canal. Acta
Otolaryngol 122:501–503.
4. Brogan M, Chakeres DW (1990) Gd-DTPA-enahanced MR imaging of
cochlear schwannoma. AJNR 11:407–408.
5. Gersdorff MC, Decat M, Duprez T, Deggouj N (1996) Intracochlear
schwannoma. Eur Arch Otorhinolaryngol 253:374–376.
6. Neff BA, Willcox TO, Sataloff RT (2003) Intralabyrinthine
schwannomas. Otol Neurotol 24:299–307.
7. Matthies C, Osorio E, Samii M (2003) Hamartomas of the internal
auditory canal: report of two cases. Carvalho GA, Neurosurgery
52:944–948.
8. Karagama YG, Bridges LR, van Hille PT (2002) Neuromuscular
hamartoma of the cochlear nerve: a rare occurrence in the internal
auditory meatus. Eur Arch Otorhinolaryngol 259:119–120.9. Wu SS, Lo WW, Tschirhart DL, Slattery WH 3rd, Carberry JN,
Brackmann DE (2003) Lipochoristomas (lipomatous tumors) of the
acoustic nerve. Arch Pathol Lab Med 127:1475–9.
ABSTRACT
A 47-year old man presented with a five-year history of fluctuating
hearing impairment in the left ear. There was no tinnitus or vertigo.
Imaging studies demonstrated a contrast-enhancing cerebellopon-
tine angle mass in the left internal auditory canal. Surgically the
lesion was attached to the cochlear nerve. Pathological evaluation
revealed what is best described as an angiolipomatous hamartoma
of the cochlear nerve. Similar lesions have only rarely been
described.
Correspondence
742 Brain Pathology 19 (2009) 739–742
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology