Embed Size (px)
Citation preview

La démarche scientifique face aux épidémies
Didier Raoult
Marseille - France
Cours L3- 08.01.13

INFECTIONS AU XXIÈME SIÈCLE
Infections dans le monde :
17 millions de morts - 30%
pas de vaccin
Étiologie?
Étiologie?
Adhésion
Circuits?
Source
Transmissible
- Les 3 grands : HIV - TB – Paludisme :
- Infections respiratoires :
- Infections digestives :
- Infections prévenues par vaccinations :
- Infections nosocomiales :
- Infections émergentes :
- Cancer :

UK investments in global infectious disease researc h 1997-2010: a case study.Head MG, Fitchett JR, Cooke MK, Wurie FB, Hayward AC, Atun R.
Lancet Infect Dis. 2012 Nov 7.
FINDINGS: We identified 6170 funded studies, with a total research investment of UK£2·6 billion. Studies with a clear global health component represented 35·6% of all funding (£927 million). By disease, HIV received £461 million (17·7%), malaria £346 million (13·3%), tuberculosis £149 million (5·7%), influenza £80 million (3·1%), and hepatitis C £60 million (2·3%). We compared funding with disease burden (DALYs and mortality) to show low levels of investment relative to burden for gastrointestinal infections (£254 million, 9·7%), some neglected tropical diseases (£184 million, 7·1%), and antimicrobial resistance (£96 million, 3·7%). Virology was the highest funded category (£1 billion, 38·4%). Leading funding sources were the WellcomeTrust (£688 million, 26·4%) and the Medical Research Council (£673 million, 25·8%).INTERPRETATION: Research funding has to be aligned with prevailing and projected global infectious disease burden. Funding agencies and industry need to openly document their research investments to redress any inequities in resource allocation.

SANTÉ PUBLIQUE : LA TYRANNIE DE L'ÉMOTION
Publié le 11/10/2011
Les accidents, maladies ou infections qui sont rapportés dans nos médias nesont jamais mis en perspective. Si bien que nous ne savons jamais quel risquenous courons vraiment. Quand un événement extraordinaire arrive (mort d'unenfant dans une voiture surchauffée, noyade d'un enfant dans une piscine privéeou cas extraordinaire d'encéphalopathie dite "maladie de la vache folle"), lesmédias jouent leur rôle d'alerte en pointant le problème qui devient un sujetmajeur d'actualité.
Par Didier Raoult

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

PRION DISEASES REMAIN A MYSTERY
Thankfully, these diseases are rare. The total number of cas es of vCJD inthe UK in 1995—2011 was 176, with another 49 being recorded in 11 othercountries. The UK has done detailed surveillance of CJD sinc e the heightof the BSE crisis in 1990. The latest report (published on Oct 8, 2012) fromthe National CJD Research and Surveillance Unit in Edinburg h shows thatalthough the cases of vCJD have declined, the number of cases ofsporadic CJD have remained fairly constant for the past 15 ye ars, hoveringaround 70 per year, although in 2008, 2009, and 2011, the numb er of deathswas 85 or higher.
UK investments in global infectious diseases research from 1997 to 2010;they found that more than £30 million had been spent on research intoprion disease, around £20 million of which came from the Depa rtment ofHealth. When compared with research investments in HIV (£46 1 million),hepatitis B (£12 million), hepatits C (£60 million), and mal aria (£346million), the spending may seem disproportionate to the bur den ofdisease.
Volume 12, Issue 12, Page 897, December 2012

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Severe acute respiratory syndromeFrom Wikipedia, the free encyclopediaFurther information: Progress of the SARS outbreak
Severe acute respiratory syndrome (SARS,/ˈsɑrz/ SARZ) is a viral respiratory disease inhumans which is caused by the SARS coronavirus(SARS-CoV).[1] Between November 2002 andJuly 2003, an outbreak of SARS in Hong Kongnearly became a pandemic[citation needed], with8,096 cases and 774 deaths worldwide[2] (9.6%fatality) according to the World HealthOrganization (WHO).[3] Within weeks, SARSspread from Hong Kong to infect individuals in 37countries in early 2003.[4]The last infected human case of the outbreakoccurred in June 2003, and there was alaboratory-induced infection case in 2004. SARSis not claimed to have been eradicated (unlikesmallpox), as it may still be present in its naturalhost reservoirs (animal populations) and mayreturn to the human population.

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Troubled. Ivins juggled at parties and
volunteered for the Red Cross but
was also plagued by strange
obsessions and criminal thoughts,
says a new report.
Anthrax investigation. Army missed warning signs ab out alleged anthrax mailer.Bhattacharjee Y.
Science. 2011 Apr 1;332(6025):27.
The only recorded use of microbe as
weapons since 45 years 64 is from the
Russian army Ekaterinbourg 1979 and
American army (Ivins) 2001!

Operation Dark WinterFrom Wikipedia, the free encyclopedia
Operation Dark Winter was the code name for a senior-level bio-terrorist attack simulation conducted
from June 22–23, 2001.[1][2][3] It was designed to carry out a mock version of a covert and
widespread smallpox attack on the United States. Tara O'Toole and Thomas Inglesby of the Johns
Hopkins Center for Civilian Biodefense Strategies (CCBS) / Center for Strategic and International
Studies (CSIS), and Randy Larsen and Mark DeMier of Analytic Services were the principal designers,
authors, and controllers of the Dark Winter project.
Dark Winter was focused on evaluating the inadequacies of a national emergency response
during the use of a biological weapon against the American populace. The exercise was solely intended
to establish preventive measures and response strategies by increasing governmental and public
awareness on the magnitude and potential of such a threat posed by biological weapons.
Dark Winter's simulated scenario involved a localized smallpox attack on Oklahoma City.
The simulation was then designed to spiral out of control. This would create a contingency in which
the National Security Council struggles to determine both the origin of the attack as well as deal with
containing the spreading virus. By not being able to keep pace with the disease's rate of spread, a new
catastrophic contingency emerges in which massive civilian casualties would overwhelm America's
emergency response capabilities.
The disastrous contingencies that would result in the massive loss of civilian life were used
to exploit the weaknesses of the U.S. health care infrastructure and its inability to handle such a
threat. The contingencies were also meant to address the widespread panic that would emerge and of
which would result in mass social breakdown and mob violence. Exploits would also include the many
difficulties that the media would face when providing American citizens with the necessary
information regarding safety procedures.
Predicting smallpox

Taking stock of the biodefense boomKaiser J.
Science. 2011 Sep 2;333(6047):1214-5.
That is a conflict of interest experts benefit of f undings!

THE DANGER IS SMALLPOX!
In the same hands than anthrax!

LE BIOTERRORISME AUX ÉTATS-UNIS : 15 MILLIARDS DE D OLLARS DE GASPILLAGE
Publié le 28/09/2011 Par Didier Raoult
C'est une anecdote dramatique qui a coûté des milliards de dollars aux États-Unis.Un article du journal Science, de septembre 2011, concernant les révélations sur lasource de l'épisode de charbon en 2001, montre comment la machine sécuritaires'est emballée aux États-Unis et dans le reste du monde.
Rappel des faits : après le 11 septembre 2001, des enveloppes avec de la poudrecontenant la bactérie de l'anthrax ont été envoyées aux États-Unis. Quelques casmortels ont été diagnostiqués. Les enveloppes étaient envoyées préférentiellementà des hommes politiques ou à des journalistes. Ce qui a entraîné des réactionsconsidérables, suivies partout dans le monde d'envois fantaisistes de poudre,jouant sur la terreur.

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

The 1918 to 1919 “Spanish” influenza pandemic virus killed up to 50 million
people. We report here clinical, pathological, bacteriological, and virological
findings in 68 fatal American influenza/pneumonia military patients dying
between May and October of 1918, a period that includes ∼4 mo before
the 1918 pandemic was recognized, and 2 mo (September–October 1918)
during which it appeared and peaked. The lung tissues of 37 of these cases
were positive for influenza viral antigens or viral RNA, including four from
the prepandemic period (May–August). The prepandemic and pandemic
peak cases were indistinguishable clinically and pathologically. All 68 cases
had histological evidence of bacterial pneumonia, and 94% showed
abundant bacteria on Gram stain. Sequence analysis of the viral
hemagglutinin receptor-binding domain performed on RNA from 13 cases
suggested a trend from a more “avian-like” viral receptor specificity with
G222 in prepandemic cases to a more “human-like” specificity associated
with D222 in pandemic peak cases. Viral antigen distribution in the
respiratory tree, however, was not apparently different between
prepandemic and pandemic peak cases, or between infections with viruses
bearing different receptor-binding polymorphisms. The 1918 pandemic
virus was circulating for at least 4 mo in the United States before it was
recognized epidemiologically in September 1918. The causes of the
unusually high mortality in the 1918 pandemic were not explained by the
pathological and virological parameters examined. These findings have
important implications for understanding the origins and evolution of
pandemic influenza viruses.
� Several variable
� Not different from the other influenzas
� Bacterial pneumonias !


Nicholson, Human Influenza, In Nicholson, Webster, H ay, Textbook of Influenza, Blackwell; Oxford 1998:p237
Pneumonia case-fatalityComplicated by pneumoniaTotal case-fatality
10 20 30 40 50 60 70 8000
1
10
100
Per
cent
age
of c
ases
(Lo
g sc
ale)
Age (years)
AGE-RELATED COMPLICATIONS OF PNEUMONIA AND DEATH, AND CASE FATALITY RATE, 1918–1919 PANDEMIC

1918 PNEUMONIA DEATHS DUE TO BACTERIAL INFECTION – 58 AUTOPSIES REVIEWED IN 2008
Morens et al . JID 2008;198:962–70
A: Typical picture of severe, widespread bacterial bronchopneumonia
B: Massive infiltration of neutrophils in the airspaces of alveoli associated with bacterial bronchopneumonia
C: Bronchopneumonia with intra-alveolar edema and hemorrhage
D: Bronchopneumonia with evidence of pulmonary repair
A B
C D

Science 14 January 2011:
Vol. 331 no. 6014 pp. 144-145
DOI: 10.1126/science.331.6014.144-c
LETTERSMicrobe Interactions Undermine PredictionsThe Report by S. Telfer et al. (“Species interactions in a parasite community drive
infection risk in a wildlife population,” 8 October 2010, p. 243) demonstrates that
the history of infection cannot be summarized by a simplified scenario involving
only a host and a microbe. Microorganisms interfere with each other and can
modify the transmissibility between humans. For example, in the recent flu
pandemics, influenza virus interfered with rhinoviruses, which modified the
transmission and hence the epidemic of H1N1 in France (1). Moreover, the severity
of the disease is modified by associated bacterial pathogens, as demonstrated in
the Spanish flu outbreak, in which bacterial secondary infection played a major
role in mortality (2). These poorly known and badly controlled elements make
prediction models for infectious disease outbreaks ineffective. To base decision-
making in public health on such models is dangerous, because of our ignorance in
the multiple partners prevailing during an epidemic.
Didier RAOULT.

PUBLIC HEALTH. PUBLIC HEALTH RISK FROM THE AVIAN H5N1 INFLUENZA EPIDEMICFerguson NM, Fraser C, Donnelly CA, Ghani AC, Anderson RM.
Science. 2004 May 14;304(5673):968-9.
H5N1

The ferret: an animal model to study influenza virusMaher JA, DeStefano J.
Lab Anim (NY). 2004 Oct;33(9):50-3.
AbstractThere has been much critical influenza research conducted in
a little-known laboratory animal--the ferret. The authors
review some of these findings, discuss the reasons the ferret
often becomes a model for influenza infection, and compare
the ferret with other animal models.
Journal influence, modelisation and reductionism
Mechanistic science rather than observation!
Role of sponsor?Benefit of experts: Massive conflit of interest

Pathogenesis of avian influenza A (H5N1) viruses in ferretsZitzow LA, Rowe T, Morken T, Shieh WJ, Zaki S, Katz JM.
J Virol. 2002 May;76(9):4420-9.
AbstractHighly pathogenic avian influenza A H5N1 viruses caused outbreaks of disease indomestic poultry and humans in Hong Kong in 1997. Direct transmission of theH5N1 viruses from birds to humans resulted in 18 documented cases of respiratoryillness, including six deaths. Here we evaluated two of the avian H5N1 virusesisolated from humans for their ability to replicate and cause disease in outbredferrets. A/Hong Kong/483/97 virus was isolated from a fatal case and was highlypathogenic in the BALB/c mouse model, whereas A/Hong Kong/486/97 virus wasisolated from a case with mild illness and exhibited a low-pathogenicity phenotype inmice. Ferrets infected intranasally with 107 50% egg infectious doses (EID 50) ofeither H5N1 virus exhibited severe lethargy, fever, weight loss, transientlymphopenia, and replication in the upper and lower respiratory tract, as well asmultiple systemic organs, including the brain. Gastrointestinal symptoms were seenin some animals. In contrast, weight loss and severe lethargy were not noted inferrets infected with 107 EID 50 of two recent human H3N2 viruses, although theseviruses were also isolated from the brains, but not other extrapulmonary organs, ofinfected animals. The results demonstrate that both H5N1 viruses were highlyvirulent in the outbred ferret model, unlike the differential pathogenicity documentedin inbred BALB/c mice. We propose the ferret as an alternative model system for thestudy of these highly pathogenic avian viruses.

En fait, pour H5N1 couramment les cas mortels sont
diagnostiqués d'abord !
Plus tard, les cas bénins et asymptomatiques sont pris en
compte.
Actuellement, il n'est pas clair que H5N1 chez les humains
est plus grave, car nous n'avons aucune série de champ.
C'est toujours une maladie zoonotique (pas inter humaine) !
Identification of H5N1-specific T-cell responses in a high-risk cohort in vietnam indicates the existence of potential asymptomatic infections.
Powell TJ, Fox A, Peng Y, Quynh Mai le T, Lien VT, Hang NL, Wang L, Lee LY, Simmons CP, McMichael AJ, Farrar
JJ, Askonas BA, Duong TN, Thai PQ, Thu Yen NT, Rowland-Jones SL, Hien NT, Horby P, Dong T.
J Infect Dis. 2012 Jan;205(1):20-7.
Evidence for subclinical avian influenza virus infections among rural Thai villagersKhuntirat BP, Yoon IK, Blair PJ, Krueger WS, Chittaganpitch M, Putnam SD, Supawat K, Gibbons RV,
Pattamadilok S, Sawanpanyalert P, Heil GL, Friary JA, Capuano AW, Gray GC.
Clin Infect Dis. 2011 Oct;53(8):e107-16.

LA GRIPPE : ET SI ON ARRÊTAIT DE SE FAIRE PEUR !
Publié le 06/12/2011 Par Didier Raoult
La grippe est l'un des pires fléaux. La grippe espagnole a causé la mort deplusieurs dizaines de millions de personnes. Par ailleurs, chaque année, le virus dela grippe contribue au décès prématuré de 5 000 à 10 000 personnes(essentiellement âgées) en France. Prendre conscience de ce problème est unenécessité de santé publique. Mais la communication sur la grippe a pris un tourdélirant, pour des raisons d'ignorance, de marketing (comme la récente annonced'un virus "mutant" mis au point par un laboratoire de virologie hollandais) etd'erreurs de modélisation (celle des Nostradamus anglais des maladiesinfectieuses).
H5N1 IN FERRETS

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

LE VIRUS DU CHIKUNGUNYA
N ENGL J MED 2007;356: 769-771
Maintenant en Italie
Et en France
Maintenant la Dengue!

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Avian influenza. The limits of avian flu studies in ferretsCohen J.
Science. 2012 Feb 3;335(6068):512-3.

Klugman and Madhi, Science, 2007, 316, 49 – 50.
BLIND TO OTHER FIELDS

Virus PCV9 vaccinees
Controls Vaccine efficacy (95% CI)
P
Influenza 31 56 45(14 to 64)
0.01
Madhi, Klugman et al. Nature Medicine 2004;10:811–1 3
PCV9 PREVENTS HOSPITALIZATION FOR PNEUMONIA IN PATIENTS WITH SEASONAL INFLUENZA
VT pneumococcal bacteremia 0 vs 1

Molecular, epidemiological, and clinical complexities of predicting patterns of infectious diseases. Raoult D. Front Microbiol.
2011;2:25. Epub 2011 Feb 11
Models cannot predict future outbreaks: A/H1N1 virus, the paradigm.Nougairède A, Charrel RN, Raoult D.
Eur J Epidemiol. 2011 Mar;26(3):183-6.
Valeurs estimées par modélisation
Données observées fin 2008
Données observéesILI = influenza-like illness Pas de grippe l’hiver!

We do not test in winter!
FLU FROM INFLUENZA DI FREDO

The incidence (per 100 000 persons) of ILI from 1996 to 2011 in the region of PACA, France and the average
temperature (represented by 7 classes) recorded on Marseille. Data from the French sentinel network and from the
web source, free available as http://www.wunderground.com/.
In 2009-2010 cases do not follow cold!

Likely correlation between sources of information and acceptability of A/H1N1 swine-origin influenza virus vaccine in Marseille, France.
Nougairède A, Lagier JC, Ninove L, Sartor C, Badiaga S, Botelho E, Brouqui P, Zandotti C, De
Lamballerie X, La Scola B, Drancourt M, Gould EA, Charrel RN, Raoult D.
PLoS One. 2010 Jun 25;5(6):e11292.
BACKGROUND:In France, there was a reluctance to accept vaccination against the A/H1N1 pandemic influenza virus despite
government recommendation and investment in the vaccine programme.
METHODS AND FINDINGS:We examined the willingness of different populations to accept A/H1N1 vaccination (i) in a French hospital
among 3315 employees immunized either by in-house medical personnel or mobile teams of MDs and (ii) in a
shelter housing 250 homeless persons. Google was used to assess the volume of enquiries concerning incidence
of influenza. We analyzed the information on vaccination provided by Google, the website of the major French
newspapers, and PubMed. Two trust Surveys were used to assess public opinion on the trustworthiness of
people in different professions. Paramedics were significantly more reluctant to accept immunisation than
qualified medical staff. Acceptance was significantly increased when recommended directly by MDs. Anecdotal
cases of directly observed severe infections were followed by enhanced acceptance of paramedical staff.
Scientific literature was significantly more in favour of vaccination than Google and French newspaper websites.
In the case of the newspaper websites, information correlated with their recognised political reputations,
although they would presumably claim independence from political bias. The Trust Surveys showed that
politicians were highly dis-trusted in contrast with doctors and pharmacists who were considered much more
trustworthy.
CONCLUSIONS:The low uptake of the vaccine could reflect failure to convey high quality medical information and advice relating
to the benefits of being vaccinated. We believe that the media and internet contributed to this problem by
raising concerns within the general population and that failure to involve GPs in the control programme may
have been a mistake. GPs are highly regarded by the public and can provide face-to-face professional advice and
information. The top-down strategy of vaccine programme management and information delivered by the
Ministry of Health could have aggravated the problem, because the general population does not always trust
politicians.
In UK they practice Flu feast!

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Reyes et al., Science 1990;247; Koonin. J Gen Virol 1991;72:2197; Koonin et al., PNAS 1992;89:8259Worm et al., Microbes and Infection 2002;4:657; Guu et al., PNAS 2009;106; Emerson and Purcell, N Engl J Med 2004
Balayan et al., Intervirology 1983;20:23

Colson et al. J Infect Dis 2010Mansuy et al., Emerg Infect Dis 2011
7/12 (58%) ARN VHE-positifs (titre, 3-6 log10 copies/ml)8/18 (44%) ARN VHE-positifs (titre, 2.0-5.8 log10 copies/ml)
∼30 millions de saucisses/an.
Les foies de porcs sont mélangés;
ex.: ∼2100 figatelli nécessitent 75 foies
� Détection moins fréquente et titres plus faibles dans d’autres produits dérivés du porc : mesenteric lymph
nodes, small and large intestine, lymph node, tonsil, spleen, kidney, muscles (Williams et al., J Clin Microbiol 2001;39;
Choi et al., J Hepatol 2003;38; de Deus et al., Vet Microbiol 2007;119; Pischke et al., Liver Transplant 2010;16)
� Dose infectante ≈ ~104-107 GE/mL (Purcell and Emerson. J Hepatol 2008;48; Kasorndorkbua et al., J Clin Microbiol 2004;42;
Meng et al., J Virol 1998;72)

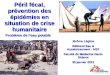
Nombre de cas d’hépatite E aiguë rapportés par les
hôpitaux généraux dans le nord et le sud de la
France.
Distribution des cas d’hépatite E autochtone
en France en 2008, et prévalence IgG chez les donneurs
de sang
Nicand et al., BEH 31-32 / 2009;Mansuy et al., 2008;
Boutrouille et al., 2007;Colson et al., 2007; P. Gallian
Renou et al., Aliment Pharmacol Ther 2008;27:086–1093
∼∼ ∼∼100
0 km
∼∼∼∼60 millions d’habitants
340 cas rapportés au Centre National de Référence en 2010 (70%
autochthonous) (Bouquet et al., Emerg Infect Dis 2011)
3%
8%
16%

4% [Rutjes et al., 2009]
5.3% [Kaci et al., 2008]; 68.2% [Adlhoch et al., 2009];14.9% [Schielke et al., 2009]
29.9% [Martelli et al., 2008]
13-42% [de Deus et al., 2008]; 26%* [Boadella et al., 2009]
2.5% [Kaba et al., 2010]
* seropositive
12.2% [Reuter et al., 2009]

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

UNDERSTANDING THE CHOLERA EPIDEMIC, HAITI.Piarroux R, Barrais R, Faucher B, Haus R, Piarroux M, Gaudart J, Magloire R, Raoult D.
Emerg Infect Dis. 2011 Jul;17(7):1161-8.
After onset of a cholera epidemic in Haiti inmid-October 2010, a team of researchersfrom France and Haiti implemented fieldinvestigations and built a database of dailycases to facilitate identification of communesmost affected. Several models were used toidentify spatiotemporal clusters, assessrelative risk associated with the epidemic'sspread, and investigate causes of its rapidexpansion in Artibonite Department.Spatiotemporal analyses highlighted 5significant clusters (p<0.001): 1 nearMirebalais (October 16-19) next to a UnitedNations camp with deficient sanitation, 1along the Artibonite River (October 20-28),and 3 caused by the centrifugal epidemicspread during November. The regressionmodel indicated that cholera more severelyaffected communes in the coastal plain (riskratio 4.91) along the Artibonite Riverdownstream of Mirebalais (risk ratio 4.60).Our findings strongly suggest thatcontamination of the Artibonite and 1 of itstributaries downstream from a military camptriggered the epidemic
Le cholera, maladie contagieuse, liée au péril fécal importée par les soldats des nations unies

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA
1 500 morts/an en France plus que le SIDA (1 200)

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

La résistance aux antibiotiques : un problème politique !
La résistance aux antibiotiques nécessite une réforme politique profonde de lapropriété intellectuelle. On le sait, le nombre de bactéries résistantes auxantibiotiques et les types de résistance augmentent partout dans le monde. Ils'agit d'un phénomène complexe dans lequel intervient l'importance de laprescription médicale. D'autres paramètres entrent en jeu, comme les épidémieschez les animaux, en particulier les animaux de ferme, et d'autres élémentsencore mal compris. Mais, dans la plupart des cas, les gènes de résistance ontété inventés par les bactéries avant que nous ne découvrions les antibiotiques.
Publié le 21/11/2011Par le professeur Didier Raoult

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Top 50 of the well identified bacteria:
Database: Sur 328.000 souches AP-HM

EPIDEMIES DU XXIe siècle
Infection urinaire à E.coli résistant d’origine aviaire.
• Résistance isolée au Bactrim• Clône unique mondialisé• Associé aux volailles!
Dutch patients, retail chicken meat and poultry share the same ESBL genes, plasmids and strains.
Leverstein-van Hall MA, Dierikx CM, Cohen Stuart J, Voets GM, van den Munckhof MP, van Essen-Zandbergen A, Platteel T, Fluit AC, van de Sande-Bruinsma N, Scharinga J, Bonten MJ, Mevius DJ;
National ESBL surveillance group.Clin Microbiol Infect. 2011 Jun;17(6):873-80.

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Increasing Rates of Cardiac Device Infections
P < 0.001
Greenspon et al J Am Coll Cardiol 2011; 58:1001-6.

Suivi des bactériémies nosocomiales

348 336 334 336
19 20 25 23
0
1
2
3
4
5
6
7
8
0
50
100
150
200
250
300
350
400
Winter Spring Summer Autumn
%Nb
Mean nb of samples/wk Mean nb of diagnoses/wk Mean % of diagnoses/wk
772 801 790 814 780
1005
1138
979
034 41 40 41 49 72 96 680
0
1
2
3
4
5
6
7
8
9
0
200
400
600
800
1 000
1 200
2003 2004 2005 2006 2007 2008 2009 2010 2011
%Nb
Mean nb of samples/wk Mean nb of diagnoses/wk Mean % of diagnoses/wk
355 361344 336 329
354326 332 334 329
354340
21 20 19 19 21 25 24 25 22 23 24 19
0
1
2
3
4
5
6
7
8
0
50
100
150
200
250
300
350
400
January February March April May June July August September October November December
%Nb
Mean nb of samples/wk Mean nb of diagnoses/wk Mean % of diagnoses/wk
Hémocultures et bactériémies
Nosocomial bacteraemia: the most neglected causes of death in Europe?Raoult D, Richet H. Clin Microbiol Infect. 2011 Aug;17(8):1123.

Signalements externes des infections nosocomiales, France, 2006Jean-Michel Thiolet ([email protected]) 1, Isabelle Poujol 1, Claude Bernet 2, Anne Carbonne 3, Catherine Dumartin 4, Isabelle Raclot 5,Hélène Sénéchal 6, Laurence Bouraoui 1, Bruno Coignard 1
1 / Institut de veille sanitaire, Saint-Maurice, France 2 / Centre de coordination de la lutte contre les infections nosocomiales (CClin) Sud-Est, Lyon, France 3 / CClin Paris-Nord, Paris, France 4 / CClin Sud-Ouest, Bordeaux, France 5 / CClin Est, Nancy, France 6 / CClin Ouest, Rennes, France
Résumé: En 2001, les autorités sanitaires ontrendu obligatoire le signalement de certainesinfections nosocomiales rares ou graves, afinde les détecter précocement et de favoriserleur investigation et contrôle. En 2006, 1 007signalements totalisant 3 239 infections ont étéreçus de 431 établissements de santé ; 304correspondaient à des cas groupés. Les tauxet délais de signalement variaient selon le typed’établissement et la région. Les micro-organismes les plus fréquemment signalésétaient Clostridium difficile (19 % dessignalements), Staphylococcus aureus (11 %des signalements), les entérobactéries (9 %) etPseudomonas aeruginosa (8 %). En 2006, lesignalement a permis la détection del’émergence d’infections à C. difficile de type027 et l’accompagnement des établissementsde santé pour la mise en oeuvre des mesuresde contrôle. La capacité du système à détecteret contrôler rapidement des épidémies restedépendante de l’adhésion des professionnels,d’un lien avec une capacité d’expertisemicrobiologique structurée et de la réactivitédes structures de coordination et d’expertise.
Encadré Critères de signalement externe d’une infection nosocomiale au CClin et à la DdassBox External reporting criteria for nosocomial infection to
CClin and Ddass
1. Infections nosocomiales ayant un caractère rare ou particulier, par rapport aux données épidémiologiqueslocales, régionales ou nationales, du fait :
a. de la nature, des caractéristiques ou du profil de résistance aux anti-infectieux de l’agentpathogène en cause (1) ;
b. de la localisation de l’infection ;c. de l’utilisation d’un dispositif médical suspect d’avoir été
préalablement contaminé ;d. de procédures ou pratiques pouvant exposer ou avoir
exposé, lors d’un acte invasif, d’autres personnes au même risque infectieux.2. Décès liés à une infection nosocomiale.3. Infections nosocomiales suspectes d’être causées par un germe présent dans l’eau ou dans l’airenvironnant.4. Maladies devant faire l’objet d’une déclaration obligatoire à l’autorité sanitaire et dont l’originenosocomiale peut être suspectée.(1) Doivent aussi être signalées les colonisations pour certains phénotypes de résistance rares
(entérocoques résistants à la
vancomycine par exemple). 300 DC!

LES CATHÉTERS ET LES SONDES URINAIRES TUENT PLUS QU E LES INCENDIES À L'HÔPITAL !
Publié le 13/08/2012
Il existe, dans les hôpitaux et dans toutes les structures publiques, un surenchérissement
permanent des exigences sécuritaires, notamment concernant le feu. Ces dernières années,
le surcoût et la gêne occasionnés par cette spirale sécuritaire sont considérables, depuis la
réfection des escaliers, des portes, des évacuations, la multiplication des exercices et les
changements de normes. La mise en perspective du temps, de l'argent et de l'énergie
consacrés à ce risque, comparé à d'autres dans les hôpitaux, est instructive.
La mortalité annuelle par incendie est estimée en France entre 300 et 400 personnes
(données de 2004). Une situation plutôt rassurante, la mortalité étant inférieure à celle des
pays les plus riches.
Par le professeur Didier Raoult

Clin Microbiol Infect. 2011 Aug;17(8):1123.
10-20 000 /an en France(soumis)

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Infections chroniques :- Cancer 25%
- Foie (Hépatites B et C)
- Estomac (Helicobacter)
- Col de l’utérus (HPV)
- Lymphome (EBV à 25%)
- Gorge (HPV16)
- Autres
- Ulcères gastro-duodénaux
- Cirrhose hépatique
- HIV et Hépatites (B-C-D)
Les infections au XXIème siècle
Dichotomie: Transmissible/Non transmissible


CES VIRUS QUI DONNENT LE CANCER
On le sait, des virus peuvent donner des cancers. Et leur nombre ne cesse d'augmenter. Des cancers
susceptibles d'être prévenus par la vaccination. Ce changement de paradigme majeur date du début du
XXe siècle, grâce en particulier à un modèle de cancer du sein chez la souris dû à un virus. Sans avoir
suscité, pour l'instant, de changement de stratégie de la part des institutions.
Ainsi, l'OMS, mais aussi les meilleurs journaux médicaux et scientifiques continuent à distinguer les
morts par maladies non transmissibles (dont tous les cancers) et transmissibles. On continue à ranger
dans les maladies non transmissibles les cancers ou les maladies chroniques (dont la cirrhose), en
réalité conséquence d'infection et donc transmissibles. Par exemple, le cancer de l'estomac est dû à
une bactérie, Helicobacter pylorii, qui est aussi l'agent des ulcères. Le virus de l'hépatite B (susceptible
d'être prévenu par la vaccination) est l'agent de la plupart des cancers du foie et d'une partie
importante des cirrhoses du foie.
Par Didier Raoult Publié le 20/10/2011

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

LES MOUSTIQUES, L'HEURE DES REPAS ET LE PALUDISME
C'est l'une des maladies qui tue le plus dans le monde et en particulier les enfants. Le
paludisme est dû à un parasite, le plasmodium, qui circule dans le sang des humains infectés,
mais aussi de nos cousins (les gorilles) et de certains moustiques, les anophèles, qui aiment
prendre leur repas de sang sur l'homme. Leurs victimes vivent plutôt dans les zones rurales. Il
arrive qu'elles avalent le parasite au cours d'un repas, et le transmettent à un autre humain
au cours d'un autre repas.
Par le professeur Didier Raoult Publié le 30/01/2012
Les moustiques résistants aux insecticides, mangent à d’autres heures et le Plasmodium devient résistant!

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Génotypage BKMultispacer sequence typing for Mycobacterium tuberculosis
genotyping.Djelouadji Z, Arnold C, Gharbia S, Raoult D, Drancourt M.
PLoS One. 2008 Jun 18;3(6):e2433.
« Nous avons la première épidémie dans une école à Marseille depuis 20 ans à cause de Beijing »

A- « EPIDÉMIE » RÉCENTE PLUS MÉDIATIQUE QUE RÉELLE1- Maladie de la vache folle et Prion
2- SRAS
3- Bioterrorisme
4- Grippe aviaire/ Grippe espagnole
B- Epidémies réelles mal gérées1- Chikungunya
2- H1N1
3- Hépatite E
4- Choléra
5- Hépatite B
6- Bactéries résistantes hospitalières
C- Epidémies invisibles
1- Infections urinaires à E.coli resistant au Bactrim
2- Septicémie sur cathéter, sur sonde urinaire
3- Cancers
D- Réapparition d’épidémies
1- Paludisme
2- Tuberculose (Beijing)
3- SIDA

Primo-infection VIH – EPIMIC
Nb et %
En France

CONCLUSION
ACTUELLEMENT
Instrument de vente médiatique
Surréactivité Influence politique
Hostilité publique Echec de gestion

PROBLEMES
Scientifique - Epidémiologique
- Biologique
- Sociologique - Politique
- Communication
- Experts
- Médias

LUTTER CONTRE LES EPIDEMIES1- Les détecter� Syndrome based surveillance- Google
- Absenteisme
- Hospitalisation
- Consommation de médicament
� Connexion de données microbiologiques rares- Déclaration individuelle
- Réseaux
2- Les analyser� Isoler les germes
� les séquencer (Real Time genomic)
� Faire des outils diagnostiques
� Etudier leur résistance
� Diffuser le savoir
3- Informer les médecins (ne pas les exclure)� Modifier les recommandations en fonction de la connaissance
� Developper les points de diagnostic
� Modifier la réglementation en vigueur
� Evaluer la possibilité de vaccin

DES CHIFFRES
• U.S.A, on compte:
- Les morts � Maladie des légionnaires � 1976 !
- Les médicaments � Lomidine et SIDA � 1981!
- Détection évènements anormaux
• En France, les réseaux!
-Canicule: statistiques des croque morts
- CHIK et rupture de stock de Doliprane à la réunion

VEILLEDu RNSP (le culte du réseau) à la veille
- Détection du signal (événement anormal)
- Veille google
- Analyse massive des données laboratoire (Mathématiciens)
- Pas de compétition chercheur/veille (!) (Rapport de J.F Girard)
- Equipes d’investigation
- Veille ressources du territoire en experts (Pub Med/mot clés)
- Quantification des risques (discordance
risque/perception/proposition/ listing annuel)

Créer un centre de compétence en surveillance
- Des signaux
- De google
- Des spectres
- Du PMSI
Manque de polytechniciens à l’INVS!Et de recherche statistiques.

LUTTER CONTRE LES EPIDEMIES1- Les détecter� Syndrome based surveillance- Google
- Absenteisme
- Hospitalisation
- Consommation de médicament
� Connexion de données microbiologiques rares- Déclaration individuelle
- Réseaux
2- Les analyser� Isoler les germes
� les séquencer (Real Time genomic)
� Faire des outils diagnostiques
� Etudier leur résistance
� Diffuser le savoir
3- Informer les médecins (ne pas les exclure)� Modifier les recommandations en fonction de la connaissance
� Developper les points de diagnostic
� Modifier la réglementation en vigueur
� Evaluer la possibilité de vaccin

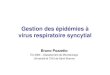
Identification Detection
Culture-dependent Culture-independent
Cloning
Research strategy for identification and detection of new pathogens
Genomesequencing
UR

Maintenant 500/an !

Comprehensive determination of the microbial composition of the gut microbiota and therelationships with health and disease are major challenges in the 21st century. Metagenomicanalysis of the human gut microbiota detects mostly uncultured bacteria. We studied stools fromtwo lean Africans and one obese European, using 212 different culture conditions (microbialculturomics), and tested the colonies by using mass spectrometry and 16S rRNA amplification andsequencing. In parallel, we analysed the same three samples by pyrosequencing 16S rRNAamplicons targeting the V6 region. The 32 500 colonies obtained by culturomics have yielded 340species of bacteria from seven phyla and 117 genera, including two species from rare phyla(Deinococcus-Thermus and Synergistetes, five fungi, and a giant virus (Senegalvirus). Themicrobiome identified by culturomics included 174 species never described previously in thehuman gut, including 31 new species and genera for which the genomes were sequenced,generating c. 10 000 new unknown genes (ORFans), which will help in future molecular studies.Among these, the new species Microvirga massiliensis has the largest bacterial genome so farobtained from a human, and Senegalvirus is the largest virus reported in the human gut.Concurrent metagenomic analysis of the same samples produced 698 phylotypes, including 282known species, 51 of which overlapped with the microbiome identified by culturomics.Thus, culturomics complements metagenomics by overcoming the depth bias inherent inmetagenomic approaches.
Keywords: Culturomics, gut microbiota, MALDI-TOF MS, metagenomic analysis, uncultured bacteriaOriginal Submission: 20 August 2012; Revised Submission: 28 August 2012; Accepted: 29 August 2012
75
MICROBIAL CULTUROMICS: PARADIGM SHIFT IN THE HUMAN GUT MICROBIOME STUDY.Lagier JC, Armougom F, Million M, Hugon P, Pagnier I, Robert C, Bittar F, Fournous G, Gimenez G, Maraninchi M, Trape JF,
Koonin EV, La Scola B, Raoult D.
Clin Microbiol Infect. 2012 Sep 4

LUTTER CONTRE LES EPIDEMIES1- Les détecter� Syndrome based surveillance- Google
- Absenteisme
- Hospitalisation
- Consommation de médicament
� Connexion de données microbiologiques rares- Déclaration individuelle
- Réseaux
2- Les analyser� Isoler les germes
� les séquencer (Real Time genomic)
� Faire des outils diagnostiques
� Etudier leur résistance
� Diffuser le savoir
3- Informer les médecins (ne pas les exclure)� Modifier les recommandations en fonction de la connaissance
� Developper les points de diagnostic
� Modifier la réglementation en vigueur
� Evaluer la possibilité de vaccin