Embed Size (px)
Citation preview

PET scan in lung cancer: Myths and facts
Wichana Chamroonrat, MDThe 1st Ramathibodi Lung cancer consortium
Dusit Thani Hall8 Feb 2018

Name
Myth• PETPositron Emission Tomography
18F-FDG• Fluorodeoxy glucose
(FDG): Glucose analog
• 18F: Positron emitter: 110 minutes half life
Fact• FDG PET/CT• F-18 FDG PET/CT

FDG PET

FDG Glucose analog
Myth• Imaging for all (lung) cancer
Fact• Non-specific tumor imaging

Lung cancer
• 85% NSCLC
• 10% SCLC
• 5% Lung NET
Adenocacinoma SCC Large cell
TypicalAtypical
High
Vary
Vary
and FDG uptake
moreless

e.g. positron-emitting tracers
• F-18 FDG • Ga-68 DOTA-TATE (Tc-99m HYNIC-TOC)• Ga-68 PSMA• F-18 DOPA• F-18 NaF (Tc-99m MDP: Bone scan)• F-18/C-11 choline• Amyloid, tau imaging• C11-Erotinib
(alternative gamma emitting tracer)
(alternative gamma emitting tracer)

PET tracers
F-18 FDG Ga-68 DOTA-TATE Ga-68 PSMAGlucose somatostatin recepter Prostate specific membrane Ag
General Lung NET, typical Non-FDG avid lung cancer

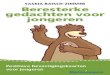
Fused PET/CT (left) and maximum-intensity-projection (right) images of 85-y-old man (patient 4) with typical bronchial carcinoid in right lower lobe. Irfan Kayani et al. J Nucl Med 2009;50:1927-1932
(c) Copyright 2014 SNMMI; all rights reserved
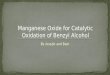
Ga-68 DOTATATE
F-18 FDG

Ga-68 PSMA
Ref: Jochumsen et.al CNM 2018 Feb

F-18 FDG
Ref: Jochumsen et.al CNM 2018 Feb

Lung cancer
• 85% NSCLC
• 10% SCLC
• 5% Lung NET
Adenocacinoma SCC Large cell
TypicalAtypical
High:FDG
Vary: FDG etc
Vary
and …?tracers
FDGDOTATATE
More FDG uptakeMore aggressive/worse
outcome

Low to no FDG uptake
• Low grade adenocarcinoma• Adenocarcinoma in situ• Well-differentiated adenocarcinoma• Carcinoid tumor
• Ground glass nodule/opacity
• Mucinous carcinoma (low tumor cells)
• Lesion <1 cm

Ref: PET clinics 2018

FDG Glucose analog
Myth• Imaging for all (lung) cancer
Fact
• Non-specific tumor imaging• Non-specific tumor imaging• Inflammatory/infectious
imaging

Malignant FDG uptake
• Glut (membrane transporter)• Intracellular hexokinase• Glucose-6-phosphatase• Vascularity of tissue• mitotic rate of the cells• No. of tumor cell per volume of tumor• Presence of inflammatory cell within tumor

Inflammatory/infectious FDG uptake
• Glut (membrane transporter)• Vascularity of tissue• No. of inflammatory cell e.g. activated WBC


Lung cancer vs Lung TB

• FDG PET in diagnosing malignant pulmonary lesions/nodules
• Sensitivity 96.8% 96%• Specificity 77.8% 80%
Hellwig D (2001)Gould MK (2001)

50 M

50 M

Mediastinal nodal metastasis
• Sensitivity• Specificity • Accuracy
CT PET PET/CT (early stage) 45-63% 79-84% 80% (42%)43-57% 89-91% 90% (100%)39-59%
FDG PET/CT detecting malignant involvement -34% in nodes < 1cm-85% in nodes ≥ 1cm

Mediastinal Nodal Staging of Non small Cell Lung Cancer (early stage) Using 18F-FDG PET/CT
Non TB country• Sensitivity 42% • Specificity 100%• Accuracy
TB endemic country (Kim YK)• Sensitivity 61% • Specificity 96% (more FP)• Accuracy 86%*All sx, possible lower stage*Excluded FDG uptake with calcified nodes (>70HU)
Kim YK, Lee KS, Kim BT, Choi JY, Kim H, Kwon OJ, Shim YM, Yi CA, Kim HY, Chung MJ. Mediastinal nodal staging of nonsmall cell lung cancer using integrated 18F-FDG PET/CT in a tuberculosis-endemic country: diagnostic efficacy in 674 patients. Cancer. 2007 Mar 15;109(6):1068-77

Ref: Hu N, Tan Y, Cheng Z, Hao Z, Wang Y. FDG PET/CT in Monitoring Antituberculosis Therapy in Patient With Widespread Skeletal Tuberculosis. Clin Nucl Med. 2015 Nov;40(11):919-21
Post TB meds

Malignant vs benign lesion
Myth• Can be differentiated by
degree of FDG uptake
Fact• Can NOT be differentiated
by degree of FDG uptake

FDG PET/CT in lung cancer
• Staging: Unexpected malignant lesion• Recurrence: Early detection• Restaging: Metastatic spread• Distinguish: Fibrosis/scaring • Post treatment: residual viable tumor

57F Staging: Unexpected malignant lesion

Pre-op
56F
6 months 2 years 4.5 years post op
Recurrence: Early detection

66F
T2N1M0
Distinguish: Fibrosis/scaring

69M Lung cancer and prostate cancer
On Gefitinib, about 3 month F/U
Post treatment: residual viable tumor
Pre SUV 10.3 Post SUV 3.1

Limitation if only tumor size change
• Tumor=malignant cells, stroma, inflammatory cells
• Confounding effects as atelectasis, postRxfibrosis, radiation pneumonitis
• Asymmetric growth pattern, difficult to measure
• Tumor cavitation, difficult to measure

Metabolic response criteria
EORTC criteria• > 25% SUV mean• (normalized to lean body
surface)
PERCIST criteria• >30% in SUV peak(normalized to lean body mass)

FDG PET and distant metastasis
Myth• High sensitivity for all type
of distant metastasis
Fact
• Low sensitivity for brain metastasis

FDG PET: M-staging
• 18-36% distant metastasis in new diagnosed lung cancer patients
• Common sites: adrenal glands, bones, liver, brain
• Preferred MRI for only brain site• Pooled sensitivity/specificity 93%/96%• 27-62% staging changes• 19-52% altered patient management

Brain metastasis (FDG PET/CT)
• Sensitivity• Specificity • PPV• NPV• Accuracy
27% 24% MRI 88%98% 100% 98%75% 83%
91% 97%
Lee HY (2009)Kruger (2011)


FDG PET and distant metastasis
Myth• FDG PET better than bone
scan for bone metastasis in lung cancer
Fact
• FDG PET: better for osteolytic lesion
• Bone scan: better for osteoblastic lesion

Pre Rx
Post Rx

Bone marrow metastasis (FDG PET/CT)
• Sensitivity• Specificity
92% PET87% MRI77% Bone scan86%98% 94% 92% 88%
Qu X (2012)
*PET: best modality to detect bone marrow metastases (per-patient and per-lesion)
*MRI: highest specificity (per lesion)

G.K Azad. G.J. Cook/Clinical Radiology 71 (2016) 620-631
F-18 NaF F-18 FDG

G.K Azad. G.J. Cook/Clinical Radiology 71 (2016) 620-631
Pre treatment Post treatment
F-18 FDG
F-18 NaF

Al-Muqbel KM et.al. Medicine (Baltimore). 2016
Pre treatment Post treatment

SUV (Standard Uptake Value)
Myth• Only semi-qualitative
measurement for PET
Fact• One of good semiqualitative
measurements for PET• Easily collected: SUVmax• Other promising
measurements: MTV, TLG


Factors interfering SUV values
• Physiologic uptake• Technique: FBS
Uptake timePatient body composition Reconstruction techniqueSelection of ROIUse of contrast agents for CT AC

Trends
• Targeted drug (e.g. EGFR TKI)
• Targeted imaging(e.g. C-11 erlotinib)

C-11 erlotinib
Ref: Bahce I et.al EJNMMI 2016 Dec

Trends
• Targeted drug (e.g. EGFR TKI)
• Theranostic(Therapy + Diagnosis)
• Targeted imaging(e.g. C-11 erlotinib)

Ref: PET clinics 2018
Ga-68 DOTA-TATE F-18 FDG Lu-177 DOTA-TATE After 1 day and after 2cycle PRRT
Theranostic
PRRT=Peptide Receptor Radionuclide Therapy

Thank you