Embed Size (px)
Citation preview
1 |
International recruitment of health personnel: a WHO code of practice
Jean-Marc Braichet, Coordinator
Health Workforce Migration and Retention Team
Department of Human Resources for Health
World Health Organization, Geneva
World Health Editors NetworkMaking Global Health News
Geneva 17-18-May 2009

2 |
International and internal migration: complementary but different responses required
Responses to international migration of HRH
- bilateral agreements (e.g. South Africa - UK; Philippines - Japan, etc.)
- regional codes (e.g. Pacific code)
- draft global code of practice on the international recruitment of health personnel
Responses to internal migration:
- national measures

3 |
WHO is developing to major and complementary projects
Developing a draft global code on the international
recruitment of health personnel
Implementing a programme which aims to improve the
retention of health workers in rural and remote areas

4 |
Main objectives of a WHO code of practice
To establish and promote voluntary principles.
To serve as an instrument of reference.
To provide guidance.
To facilitate and promote international discussion and advance cooperation.

5 |
Process to develop a WHO code of practice on the international recruitment of health personnel 1/2
Jan08 Mar08 April08 May08 June08 July08 August08 Sept08 Oct08
Draft Code
EB Migration Progress Report
Kampala Forum
Draft Outline for a Code
Tallinn EuroMinisterial
Manila Forum
PAC – TWG meeting
Launch of GlobalDialogue on Migration
G8 Summit Public Hearings
Drafting of the Code

6 |
Process to develop a WHO code of practice on the international recruitment of health personnel 2/2
Jan09 May09 June09 July09 August09 Sept-October 09 January10 March10 May10
Draft Code
WHO RCs
Progress Report for EBDraft ResolutionDraft Code
Draft Code for the WHA?
Progress Report for EB
------------ Consultations ----------
Background Paper
Technical Briefing WHA09
Global consultation?

7 |
A WHO program on increasing access to health workers in remote & rural areas through improved retention
For at least three main reasons:
1. needs clearly identified
2. calls for action
3. renewal of PHC

8 |
1- Need has been clearly identified in all countries
Inequitable distribution of health workers

9 |
A programme built on three strategic pillars
1- Building the evidence base on effective retention strategies
– literature reviews, expert consultations, synthesis of the evidence, identification of knowledge gaps and commissioning research
2- Supporting countries to evaluate and adapt retention strategies
– work with interested countries to evaluate past and on-going strategies and to develop and implement country-specific plans
3- Developing and disseminating global recommendations on increasing access to health workers in remote and rural areas through improved retention
– a time-bound participatory process involving all relevant stakeholders following the steps set out by the WHO Guidelines Review Committee
10 |
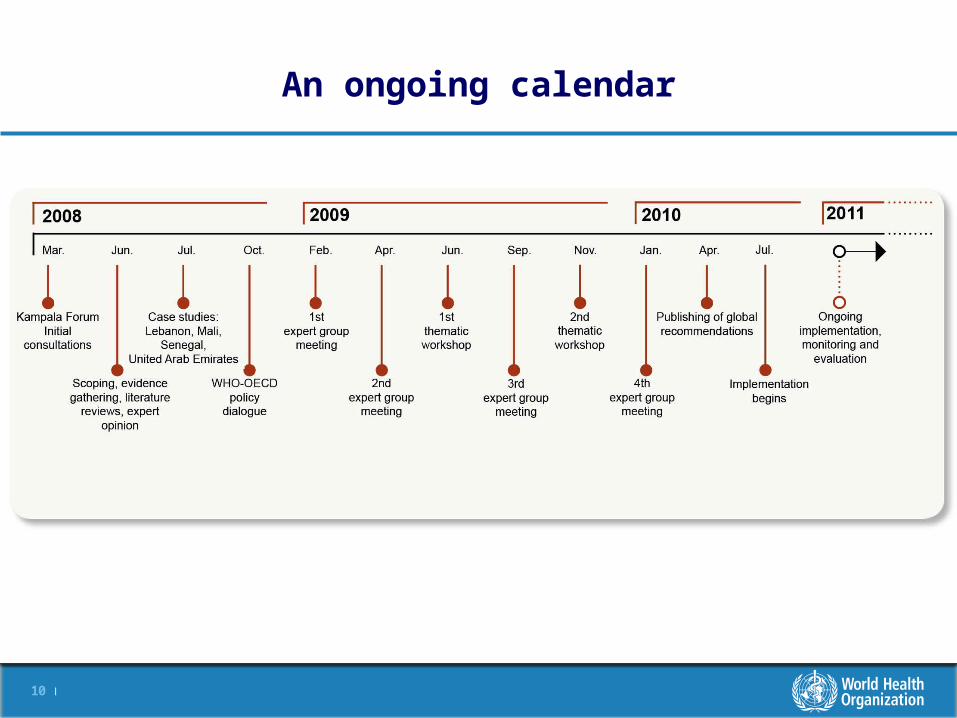
An ongoing calendar

11 |
Thank you for your attention !

12 |
Definitions
No consensus on a definition for “rural areas” - usually defined as “non-urban”
Each country has its own definition based on:– the settlement profile:
• population density • availability of economic structures
– the accessibility from an urban area: • distance in kilometres or hours drive.
Remote/underserved = areas where relatively poorer populations reside:• remote rural areas; • small or remote islands; urban slum areas; areas that are in conflict or post-conflict; refugee camps; areas inhabited by
minority or indigenous groups*
* Not specifically included in the current literature review

13 |
A complex issueno ‘single bullet’ type of answer
Ministry of Health
Ministry of Finance
Ministry of Labour
Ministry of Public
Administration
Health workers
Populations/Communities
Civil Service Commission
Ministry of Transport
Professional Associations
Ministry of Higher
Education

14 |
Categories of interventionsCategory of intervention Examples
A. Education and regulatory interventions
Targeted admission of students from rural background
Recruitment from and training in rural areas
Changes / improvements in medical curricula
Early and increased exposure to rural practice during undergraduate studies
Educational outreach programmes
Community involvement in selection of students
Compulsory service requirements (bonding schemes)
Conditional licensing (license to practice in exchange of location in rural areas)
Loan repayment schemes (paid studies in exchange of services in rural areas for 4-6 years)
Producing different types of health workers (mid-level cadres substitution task shifting)
Recognize overseas qualifications
B. Monetary compensation (direct and indirect financial incentives)
Higher salaries for rural practice
Rural allowances, including installation kit
Pay for performance
Alter the remuneration methods (fee for service, capitation etc)
Loans (housing, vehicle)
Grants for family education
Other non-wage benefits
C. Management, environment and social support
General improvement in rural infrastructure (roads, phones, water supplies, radio communication)
Improving working and living conditions, ensure adequate supplies of technologies and drugs
Supportive supervision
Support for continuous professional development, career paths
Special awards, civic movement, and social recognition
Flexible new contract opportunities for part-time work
Reduce the feeling of isolation (professional networks, telemedicine, distance learning)
Increase chances for recruitment to civil service

15 |
How can we measure “success”?
Disparities in the rural/urban ratio of health workers to population density
Percentage of health workers to choose to work in rural areas as a consequence of an intervention
Vacancy rates
Duration in post
Service utilization rates (before and after)
Patient satisfaction surveys
Health workers satisfaction surveys
Health outcomes (confounding factors!)
GP density per1,000 pop
1.54 - 1.67
1.84 and more
1.43 - 1.54
Less than 1.43
1.67-1.84
GP density per1,000 pop
1.54 - 1.67
1.84 and more
1.43 - 1.54
Less than 1.43
GP density per1,000 pop
1.54 - 1.67
1.84 and more
1.43 - 1.54
Less than 1.43
GP density per1,000 pop
1.54 - 1.67
1.84 and more
1.43 - 1.54
Less than 1.43
1.67-1.84
GP density per 1000 pop
France: General Practitioner density

16 |
Guiding principles of a WHO code of practice 1/2
The code is voluntary.
The individual right "to leave any country, including [one's]
own".
Right of everyone to the enjoyment of the highest attainable standard of health.
International recruitment can make a legitimate contribution to the development and strengthening of a national health workforce.
The development of voluntary international standards and the coordination of national policies on international health worker recruitment.

17 |
Guiding principles of a WHO code of practice 2/2
International recruitment of health personnel should be
conducted in accordance with the principles of transparency,
fairness and mutuality of benefits.
The specific needs and special circumstances of countries
should be considered.
Effective national and international data gathering, research
and information sharing are essential.





























