Embed Size (px)
Citation preview

1
Book launch, Delhi
13 Aug 04
Integrating HIV prevention and antiretroviral therapy in India: Costs and Consequences of Policy Options

2
Report team:
Mead Over, Peter Heywood, Sudhakar Kurapati
(World Bank)
Julian Gold, Indrani Gupta, Abhaya Indrayan, Subhash Hira, Elliot Marseille, Nico Nagelkerke, and
Arni S.R. Srinivasa Rao
(Consultants)

3
Objectives of the study
Review the effects and consequences of ART
Use a quantitative model to predict the course of the epidemic
Use same model to determine the costs and consequences of – Maintaining current policies– Alternative government policies for ART

4
Indian context for ART policy

5
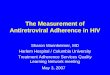
HIV Prevalence 1998
Pondichery
Gujarat
KarnatakaGoa
Lakshwadeep
Dadra Nagar HaveliMaharashtra
Madhya Pradesh
Kerala
Tamil Nadu
Andhra Pradesh
Punjab
Rajasthan
Daman & Diu
Jammu & Kashmir
Haryana
Uttar Pradesh
Himachal Pradesh
Delhi
Chandigarh
Bihar
West Bengal
Orissa
Mizoram
Meghalaya
Assam
Sikkim
Manipur
Tripura
Arunachal Pradesh
Nagaland
Source: NACO, 1998
> 1% Antenatal Women
> 5% High Risk Group
< 5% High Risk Group
No Data
TN

6
Indian context for ART policy HIV/AIDS in context of overall disease
burden– in 1998: 2% of all deaths, 6% of inf. deaths– in 2033: 17% of all deaths, 40% of inf.
Deaths Number of ART users in 2002
– >500,000 AIDS cases– 370,000 urban– 90,000 on treatment– 12,000 on ART – mostly unstructured

7
Analysis of ART policy options
Definition of policy options Health impacts of options Cost impact of options Sensitivity of results to risk
behavior Cost-effectiveness

8
Definition of policy options Adhere: Support to help patients adhere
– I.e. IEC, training, lab strengthening, subsidies for patient monitoring in both private & public sectors
MTCT+: Structured ART for identified HIV+ mothers and their partners
BPL: Structured ART for people below the poverty line
TMART: Transmission-minimizing ART

9
Structured treatment Standardized training of physician to a mandated
level of competence in ART management; Prescription of a standard triple-drug regimen as
recommended by the national guidelines; Access to support from a multi-disciplinary team
including a counselor and a nutritionist; Access to a quality laboratory for immunological
testing; Regular monitoring of the patient’s treatment status
(clinical and lab-based). Counseling to prevent transmission

10
ART can affect HIV prevention
Effects whichmight slowTransmission
Effects which mightspeed Transmission
Biological Reduces viralload
Lengthens duration Selects for
resistance
Behavioral Motivates testing Promotes
solidarity
Reduces perceivedrisk of unsafebehavior

11
Suggestive evidence of disinhibition in Kenya

12
Transmission minimizing structure
Structured ART treatment– maximize adherence– minimize infectivity– slow the development of resistant strains
Incentives – for ART physicians to assist prevention efforts of
government and non-government prevention programs– for state and local policy makers to expand and maximize
the effectiveness of prevention programs Monitoring and evaluation
– of adherence & spread of resistant strains– of prevention programs

13
The modelModified previous epidemiological
modelEstimate costs and consequences
over 35 year periodEpidemiological and biological
parameters related to transmission, disease progression, path from infection to death

14
The model assumes In 1998 15% adult males clients of sex workers
– Each client 50 sexual contacts per year
1.1% of women are sex workers
– 675 commercial transactions per sex worker per year
Condoms used in half these transactions

15
Health impacts of options
Impact of ART on the path of the epidemic
Impact of ART on the burden of the epidemic

16
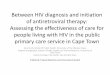
Impact of ART on the path of the epidemic: Number of new HIV infections
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Nu
mb
er
of
HIV
infe
ctio
ns
pe
r ye
ar
ADHERE Policy No Govt Policy MTCT+ Policy BPL Policy

17
Benefits of three ART policies
No change in risk behavior
-1.9%-0.4%
0.6%
5.7%
1.6% 1.1%1.8% 1.5%
11.6%
7.6%
13.8%12.4%
-4.0%
-2.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Total HIV
averted
Discounted
HIV averted
Life years
saved
Discounted
LYs saved
Alternative measures of impact
(Discount rate: 10%)
Per
cen
t ch
ang
e re
lati
ve t
o b
asel
ine
Adhere
MTCT+
BPL
Health benefits of three ART policies No change in risk behavior

18
Lessons from impact models All three ART policies save life years, but only
MTCT+ & BPL would also avert HIV infections BPL has much greater health benefits than Adhere or
MTCT+. Discount rate does not effect policy rankings Adhere policy produces effects more quickly than
other policies

19
Cost impact of options
Assumptions used Total and incremental government cost
of ART policies Components of government cost of ART
policies Lessons from the cost model

20
Assumptions used for costing
Assume constant unit costs of testing separate from treatment
Testing and monitoring: $100/patient/yr Cost of ART per year: $500 in both
public and private sectors Government subsidizes 100% of ART
cost in public sector, but only testing and monitoring in private

21
$575
$2,257
$1,173
$7,632
$1,682
$598
$7,057
0.0
1,000.0
2,000.0
3,000.0
4,000.0
5,000.0
6,000.0
7,000.0
8,000.0
9,000.0
Baseline Adhere MTCT+ BPL
Treatment option
Mill
ion
s o
f 20
02 U
S d
olla
rs
Total cost
Incremental cost
Total and incremental government cost of Art policies
(in 2002 dollars using discount rate of 10 percent)

22
Lessons from cost model The policy options will cost between $1.7 billion and
$7 billion in present value terms– Equivalent annual expense: $177 to $744 million per year for
31 years
Compare these amounts to current expenditures– about US$1,200 million/year: central health & social welfare
expenditures– about US$300 million/year: central health expenditures
Least expensive option is 59% of health budget Most expensive outcome is 62% of health & social
welfare budget combined

23
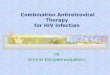
Sensitivity of results to risk behavior Alternative levels of condom use on
high risk sexual contacts– 40%, 50%, 70%, 90%
Sensitivity of the annual number of new HIV infections to these levels

24
Sensitivity of the annual number of new HIV infections to condom use on high-risk
contacts
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
8,000,000
1995 2000 2005 2010 2015 2020 2025 2030 2035
Year
Nu
mb
er
of
HIV
infe
ctio
ns
pe
r ye
ar
40% condom 50% condom 70% condom 90% condom

25
The net effect of BPL policy would then be negative on life-years saved ...
-18.1
25.2
-40
-20
0
20
40
60
80
100
120
140
40%condom
50%condom
Assumed impact of BPL ART on condom use
Mil
lio
ns
of
dis
cou
nte
d l
ife-
yea
rs s
aved
re
lati
ve t
o t
he
bas
eli
ne

26
Suppose that ART availability could be used to encourage prevention efforts …

27
Thailand succeeded in increasing condom use to even higher levels a decade ago...
0
20%
40%
60%
80%
100%
1988 1989 1990 1991 1992 1993 1994
Condom use among sex workers
Condom use

28
Condom use in Tamil Nadu during last paid sex
56
7480
88
28
41
67 67
0
20
40
60
80
100
1996 1997 1998 2000
Year
Co
nd
om
use
(%
)
Sexworkers
Truckers& helpers
Malefactoryworkers
Within India, Tamil Nadu has shown that condom use can attain high levels

29
But average state performance is well below 75%
clie
nts
with
FS
Ws
female sex workers20 40 50.4 60 75 80
20
40
57.560
7580
Andhra P
AssamBihar
Delhi
Goa
Gujarat
Haryana
Himachal
J and KKarnatak
Kerala
Madhya P
Maharash
Manipur
Orissa
Other NE
Punjab
Rajastha
Tamil Na Uttar P
W Bengal
Percent condom use in commercial sex transactionsas reported by both FSWs & clients

30
If condom use can be increased as a result of BPL policy, its benefits would be greater
-18.1
25.2
79.2
120.1
-40
-20
0
20
40
60
80
100
120
140
40%condom
50%condom
70%condom
90%condom
Assumed impact of BPL ART on condom use
Mill
ion
s o
f d
isc
ou
nte
d li
fe-y
ea
rs s
av
ed
re
lati
ve
to
th
e b
as
elin
e

31
If condom use can be increased as a result of BPL policy, its cost would be much less
$421 $389 $338 $319
$9,200
$7,632
$5,281
$4,175
0.0
1,000.0
2,000.0
3,000.0
4,000.0
5,000.0
6,000.0
7,000.0
8,000.0
9,000.0
10,000.0
40%condom
Baseline 70%condom
90%condom
Pre
se
nt
va
lue
of
futu
re e
xp
en
dit
ure
s in
mill
ion
s o
f U
S$
s
Indirect: OI costs
Direct: Cost of govttesting
Direct: Cost of ART
Total govt cost

32
Cost-effectiveness of ART
Defined as years of life saved per dollar of government expenditure
Compare to cost of saving life years– From HIV prevention programs– From other health programs
Then suppose that ART could be an instrument to achieve good prevention

33
Cost-effectiveness of alternative ART scenarios
Note: Costs and effects are discounted at 10%
$146
$199
$280
$0
$50
$100
$150
$200
$250
$300
Adhere MTCT+ BPL
Alternative ART polcies
US
$ p
er
life
ye
ar
sav
ed

34
Cost-effectiveness of alternative ART scenarios
Note: Costs and effects are discounted at 10%
$146
$199
$280
$51
$30
$0
$50
$100
$150
$200
$250
$300
Adhere MTCT+ BPL BPL + 70%condoms
BPL + 90%condoms
Alternative ART polcies
US
$ p
er
life
ye
ar
sa
ved

35
Lessons from C/E Model
Assuming ART has no effect on prevention, the Adhere policy is most cost-effective
At $146 per life year saved, Adhere is still very expensive compared to other options for saving life years
If ART causes disinhibition the losses from new infections will outweigh the gains from treatment
TMART is potentially extremely cost-effectiveonly if the incentives can be made to work

36
Transmission minimizing structure
Structured ART treatment– maximize adherence– minimize infectivity– slow the development of resistant strains
Incentives – for ART physicians to assist prevention efforts of
government and non-government prevention programs– for state and local policy makers to expand and maximize
the effectiveness of prevention programs Monitoring and evaluation
– of adherence & spread of resistant strains– of prevention programs

37
Performance-based fiscal mechanisms need:
Clear policy framework Mechanisms for independent evaluation of
proposals Effective project implementation capacity Agreements on performance-based
mechanism Independent evaluation of performance Governments willing to make disbursements
conditional on performance Capacity building