Embed Size (px)
Citation preview

1
BreastfeeBreastfeedingding
byby
Assoc. Prof. Dr. Susanha YimyamAssoc. Prof. Dr. Susanha Yimyam
Faculty of Nursing, CMUFaculty of Nursing, CMU

2
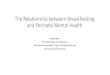
AveAveolioli
Lactiferous sinus
NipNippleple
AreAreolaola
Milk Milk ductduct
Myoepithelial cells

3
Breast & Nipple AssessmentBreast & Nipple Assessment
Breast: size, tenderness, engorgement, swelling, redness, and for heat
Nipple: asses for: 1. Size : too small or too large? 2. Crack or Fissure in nipple: red, scratched, blister, bleeding, or tender. 3. Short, flat, or inverted nipple:

4
Waller’s TestWaller’s TestWaller’s TestWaller’s Test Place thumb and forefinger on the edges of
the areola (dark area around
the nipple) just behind nipple.
Squeeze the tissue gently.
If the nipple is flat or inverted, it will flatten or
retract into the breast instead of remaining erect.
Hoffman’s maneuverHoffman’s maneuver
for short, flat & invert nipple
Normal nipple
Short nipple
Flat/ invert nipple

5
Influencing factors:1) Maternal factors:
- Mother’s beliefs, attitudes, and intention - Mother’s knowledge: learn about the mechanism of milk production and ejection, foods & beverages that promote lactation drink as well as appropriate rest.
2) Infant factors: - Physical abnormalities or other sucking problems. Examined and tested for sucking reflex.
3) Health care provider factors: play an important role to promote and support breastfeeding. Empower mothers to be confident when breastfeeding. Nursing consultation for better care
Other factors: advertisement of formula during hospital stay &
hospital policy; separation of infant and mother after birth.
Assessment for Assessment for Successful Successful
BreastfeedingBreastfeeding
Assessment for Assessment for Successful Successful
BreastfeedingBreastfeeding

6
Preparation forPreparation for BreastfeedingBreastfeedingPreparation forPreparation for BreastfeedingBreastfeeding1. Breast & nipple care:Breast & nipple care: clean water while bathing; avoid
applying soap or chemicals to nipple and breast.
2.2. BreastBreast massage: promote the let-down reflex for producing and ejecting milk.
3. Separation from infant, express breast milk3. Separation from infant, express breast milk 10-12 T/day, then at least 10 T/day thereafter, to stimulate prolactin
4. Suitable maternity bra:4. Suitable maternity bra: supports breasts to prevent pressure against the milk duct & deformity of breasts as well as relieve pain. No wire bras.

7
Preparation forPreparation for BreastfeedingBreastfeedingPreparation forPreparation for BreastfeedingBreastfeeding
5. Healthy foods,5. Healthy foods, consume about 500 Kcal’s and drink about 2,000-3,000 ml more than pre-pregnancy consumption per day. High protein, milk every day. Avoid salty, sweet and preserved foods, alcohol and caffeine beverages and foods that create gas such as those found in the cabbage family (all cabbage, broccoli, cauliflower) and some beans. Consult physician before taking any Consult physician before taking any medicationmedication.
ea sb nutsn
6. Adequate rest (8-10 hours at night and 6. Adequate rest (8-10 hours at night and 1/2–1 hour at midday).1/2–1 hour at midday).
7. Appropriate postpartum exercise daily.7. Appropriate postpartum exercise daily.
8. Relaxation both physically and 8. Relaxation both physically and mentallymentally..

8
Techniques for Techniques for breastfeedingbreastfeeding Techniques for Techniques for breastfeedingbreastfeeding
The principle of The principle of ‘three suckling’‘three suckling’: : promptly suckling, frequent suckling and correct suckling.
• Promptly suckling: WHO & UNICEF start at ½ - 2 hrs after birth: sensitive period. It also helps establish early bonding.

9
Techniques for Techniques for breastfeedingbreastfeeding Techniques for Techniques for breastfeedingbreastfeeding
The principle of The principle of ‘three suckling’‘three suckling’: : promptly suckling, frequent suckling and correct suckling.
•Frequent suckling: breastfeeding every 2-3 hrs in order to increase milk production and ejection, and decrease infant jaundice. After initiating breastfeeding, the mother should then breastfeed on demand, or at least every 3 hours during the day and at least every 4 hours at night.

10
Techniques for Techniques for breastfeedingbreastfeeding Techniques for Techniques for breastfeedingbreastfeeding
The principle of The principle of ‘three suckling’‘three suckling’: : promptly suckling, frequent suckling and correct suckling.
• Correct suckling is very important because most breastfeeding problems occur from incorrect suckling.

11
1. 1. WWashash mother mother hands hands before breastfeeding. before breastfeeding.
2 . 2 . AAwakwake the infant to e the infant to breastfeed breastfeed
3 .3 . PrivacyPrivacy, quiet place , quiet place for relaxation and for relaxation and concentration.concentration.
4 . 4 . Position Position properly for optimal properly for optimal breastfeeding: breastfeeding: cradle hold, clutch cradle hold, clutch position or football position or football hold, modified hold, modified clutch position and clutch position and side lying positionside lying position..

12
Cradle Cradle holdhold
TransitionTransitional holdal hold
Side-Side-lyinglying

13
5. Mother 5. Mother supports her supports her breastbreast is compressed slightly so that an adequate amount of breast tissue is taken into the mouth with latch-on.
7. Breastfeed on both 7. Breastfeed on both breasts; feedingbreasts; feeding about 10-15 minutes to stimulate prolactin and oxytocin and not not express the milk as it is express the milk as it is considered to be considered to be ‘hind ‘hind milk’milk’ that is, higher that is, higher energy (richer in fat) energy (richer in fat) than than ‘fore-milk’‘fore-milk’..
6. During 6. During breastfeeding: breastfeeding: Eye Eye contactcontact,, the infant’s gum on areola, stimulate infant awaken to feed once again if the infant stops sucking.

14
9. 9. Burp the infant by placing infant on mother’s lap or her shoulder
8. To change breasts or to stop feeding, push one finger into the corner of the baby’s mouth.

15
10. Not supplementNot supplement the child’s diet with formula, food or drink except when medically indicated
1 1 . NN o artificial tre o artificial tre ats or pacifiers ats or pacifiers: nippl
e confusion. If not suckling from breast; m
edicine dropper or cup.
12. Manual Manual expressexpress breast milk at least 6-8 times a day for 10-20 minutes in each time.

16
1. Conducted after bathing as the mother’s hands & body is clean 2 . Begin at the baseBegin at the base of the breastclose to areola to remove breast milkfrom milk ducts through lactiferous sinus,which is located under areola
Objective:Objective: Promote let-down reflex by stimulating milk production & ejection.
3 . 3 . MethodsMethods 31. Mother applies one hand to support the breast and then apply 4 fingers of another hand side to deep circular massage from the base of breast into areola.

17
32. 32. The mother places her hands places her hands against the chest wall against the chest wall with her fingers with her fingers encircling the breasts.encircling the breasts. She gently slides her hands forward until the fingers overlap.
4 . After breast massage, mother should express breast milkexpress breast milk by placing her hand just behind the areola, with the thumb on top and the fingers supporting the breast. The action is repeated to simulate the suckling of the infant. Moving the hands around the areola allows compression of all sinuses and completes removal of milk from the breast.

18
6 . 6 . BeginsBegins breast breast massage until milk massage until milk produces enough to produces enough to satisfy the infant’s need:satisfy the infant’s need: 6.16.1 The infant can The infant can sleep for 1 ½ - 3sleep for 1 ½ - 3 hourshours 6.26.2 For exclusive For exclusive breastfeeding, urine breastfeeding, urine output of infant is about 6-output of infant is about 6-88 times/day.times/day. 6.36.3 The infant will The infant will increase weight about 125increase weight about 125 gm./day or observation of gm./day or observation of infant’s skin.infant’s skin.
5. Suggest appropriate bra for supporting breasts.

19
• Insufficient breast Insufficient breast milk supplymilk supply• Engorged breast Engorged breast
- - Hot Hot compressioncompression
- - Expression of Expression of breast milkbreast milk
• Crack or Fissure Crack or Fissure in nipplein nipple• Short, flat, or Short, flat, or inverted nippleinverted nipple• Inhibition of Inhibition of breast milkbreast milk

20
Causes:Causes:- Delayed initiated breastfeeding, seldom suckling, and incorrect suckling. - Supplementing with other foods or drink. - Maternal malnutrition.- Postpartum hemorrhage and/ or postpartum infection.- Medications (oral pill).- Lack of confidence in breastfeeding. - Undesired breastfeeding. - Maternal stress and anxiety. - Fatigue or insufficient rest.

21
Problem solving:Problem solving:
- - Increase frequency & Increase frequency & duration of suckling on duration of suckling on demand. demand. - Correct suckling for mother’s - Correct suckling for mother’s and infant’s position. and infant’s position. - Mental support mother for - Mental support mother for physical and mental relaxingphysical and mental relaxing- Encourage confidence & - Encourage confidence & support breastfeeding. support breastfeeding. - Encourage hot compresses - Encourage hot compresses and breast massage to and breast massage to promotepromote let-down reflexlet-down reflex- Using- Using lact-aid nursing. lact-aid nursing. - Suggest - Suggest mother get mother get adequateadequate foods & drink..- Suggest mother get - Suggest mother get adequate rest.adequate rest.- Prevent hemorrhage and - Prevent hemorrhage and infectioninfection- Consult physician before - Consult physician before taking any medications.taking any medications.

22
Causes:Causes: 2 phases:1. Early engorged breast, vascular or lymph congestion. 2. Late engorged breast, accumulation of milk. This could be cause by delayed initiation, seldom suckling/ incorrect suckling.
SignsSigns and symptoms:and symptoms: Enlarged, warm, heavy in weight, tight, red or visible vascular under the breast, tender, ‘fever milk when, and in some cases, axillaries lymph nodes are enlarged.
When mother experiences breast engorgement, the areola is tight and the nipple is flat, making it difficult for the infant to latch-on. Mother may also feel extreme pain if the root of problem is not solved or breast milk is not drained.
Normal Normal suckling suckling
Infant Infant suckling suckling on on engorgeengorged breast d breast

23
Prevention:Prevention:1. Suggest mother to breastfed frequently, every 1-2 hours or 10-12 times a day during a few days after birth, then every 2-3 hours or 10 times a day. The infant should be breastfed on both breasts and after breast milk is well-established on demand. If the infant cannot suck, the mother should express breast milk.
2. Exclusive breastfeeding; no supplementing foods or drink.

24
Problem solvingProblem solving Early engorged breastEarly engorged breast 1. Remind the mother this is normal & will disappear within a few days.2. Encourage infant to feed on schedule with correct suckling until milk is finish or breast is soft.3. Before breastfeeding, mother should apply hot compresses to the breast since. 4. Breast massage in order to soften breast and nipple. 5. If mother feels extreme pain during feeding, medicine can be given to relieve pain. 6. Suggest mother to wear appropriate bra. 7. If mother does not feel better within 24 hours, she should consult with her physician.

25
Electronic Electronic PumpPump
Late engorged Late engorged breastbreast 1. Encourage the infant to suck frequently and correctly. 2. After breastfeeding, mother should express breast milk by hands or electric breast pump, in order to relieve pain from breast and enhance milk production. 3. Suggest mother to wear suitable bra for support.

26
Objective:Objective: Promote pain relief during milk production.Procedure:Procedure:
1. Position mother in a comfortable sitting.4. Help mother remove her blouse and place it under her axillaries.5. Use a big towel to cover mother’s lap to prevent from getting wet.
6. Place a towel in warm water; wrings and compresses mother’s breast slight rolling.7. Re-dip towel in warm water and repeat until mother feels comfortable.8. Wipe nipple dry. Encourage mother to wear a well-fitting bra.

27
Objectives:Objectives:1. Relieve engorged breast pain.2. Stimulate regular and continued milk production for infant feeding especially LBW infants whose hospital stay is long.3. Collect milk for hospitalized infant or during outside work.4. Stimulate the milk glands. Procedure:Procedure:
1. Wash hands before expressing milk.
2. Remove her blouse and place it under her axillaries.
3. Use large towel to cover mother’s lap to prevent her from getting wet.
4. Hot compress & Breast massage.

28
Procedure (Cont.):Procedure (Cont.): 5. If mother does not
desire to collect breast milk, she can express milk into the kidney bowl.
6. If mother would like to keep breast milk for infant, mother should clean the nipple with a wet cotton, then, squeezing milk for 2-3 times before start to collect milk and next, squeezing milk through the milk container (bottle).
While expressing milk, the mother should slightly bend her body down so that the milk will flow into the container. The mother’s breast should not touch the bottle. Once the bottle is filled, it should be stored in the refrigerator or in the ice container.

29
Procedure:Procedure: 1. Wash hands before breast
pump.2. Remove her blouse and
place it under her axillaries.3. Use a large towel to cover
mother’s lap for prevents mother to get wet.
4.1 Mother uses unskilled hand to support breast, well-fitted covering the flange over the areola, a collecting chamber is under. Slight squeeze a bulb as creating a vacuum and gentle releasing it, then milk flows to a collecting glass-chamber. Next, move a rubber bulb pump carefully and pours milk to the container. Repeat expression until clear both side.

30
4.2 Like hand breast pump, mother uses unskilled hand to support breast, well-fitted covering the flange over the areola, a collecting chamber is under. Then, milk flows to a collecting glass-chamber by electric mechanism. Repeat expression until clear both side breast pump.
5. Storage in freezer. 6. Feeding
breast milk via cup

31
Causes:Causes: 1. Incorrect position/ breast engorgement: tight and flat areola, infant is able to suck only the nipple instead of areola. Lactation is decreased so as to cause the infant sucks vigorously, accordingly increasing inflammation.2. Mother does not break the suction before removing the infant from the breast.3. Incorrect nipple cleaning such as rubbing vigorously while bathing or using soap to clean the nipples.

32
Preventions:Preventions:1. Correct breastfeeding positioning, lubricate the nipple by mother slight squeezes the breast and applies breast milk to the nipple. Open the infant’s mouth wide before latching on, well-fit hold during breastfeeding by chin-breast. If mother feels nipple pain after 1-2 minutes of sucking, remove the infant from the breast and try to latch on once again.
2. Do not drag the nipple from the infant’s mouth while infant is sucking.3. Clean the nipples no more than twice a day.4. Breastfeed frequently or follow infant’s demand in order to engorged breast, and then infant strongly suckling.

33
Problem solving:Problem solving:1. Evaluate breastfeeding position of 1. Evaluate breastfeeding position of
mother, breast and areola mother, breast and areola engorgement.engorgement.
2. Feed on the less-sore breast first.2. Feed on the less-sore breast first.3. Gently massage the 3. Gently massage the
sore nipple before sore nipple before feeding & Express a feeding & Express a little milk by hand in little milk by hand in order to help the order to help the infant to latch-on infant to latch-on well.well.
4. Suggest mother to 4. Suggest mother to hold the infant in a hold the infant in a comfort position & comfort position & alternate positions of alternate positions of feeding to prevent feeding to prevent repeated suckling repeated suckling point. point.

34
5. Correctly remove the infant 5. Correctly remove the infant from the breast & expresses from the breast & expresses hind milk to the nipple for hind milk to the nipple for enhancing wound healing. enhancing wound healing. Air-dry nipples ~ 10-15 min. Air-dry nipples ~ 10-15 min. before wearing a bra.before wearing a bra.
6. Cracked or bleeding, stop 6. Cracked or bleeding, stop sucking on that side for 24-sucking on that side for 24-36 hour; expressing milk by 36 hour; expressing milk by hand, and temporarily feed hand, and temporarily feed using spoon or cup.using spoon or cup.
7. If the wound is not better, 7. If the wound is not better, dry wound using a 20 Watt dry wound using a 20 Watt light 12–18 inches away light 12–18 inches away from the nipple for 10 from the nipple for 10 minutes, 2-3 times a day or minutes, 2-3 times a day or using a hair dryer 6-8 inches using a hair dryer 6-8 inches away from the nipple.away from the nipple.

35
Problem solving:Problem solving:1. Assure mother that her infant is able to suck. Infant may not adequately grasp the areola early on. If mother is patient and trains the infant to suck frequently, within 1-2 weeks the areola will become more elastic and the infant can grasp the areola properly.
2. Mother should pull the nipple before breastfeeding by one of these methods including: 2.1 Hoffman’s maneuver
2.2 Nipple puller

36
Problem solving (Cont.):Problem solving (Cont.):3. Assist the mother to correctly position the infant.4. Mother supports the breast and then compresses hand around the lateral margin of the areola in order to reduce the areola size for ease of latching-on.
5. In case of extreme breast engorgement, compressing with warm water & then express a little milk to soften areola in order that infant will latch on well. 6. In case the nipple does not erect, suggest that the mother use a nipple shield, which is made of thin rubber to help the infant breastfeed.

37
Problem solving (Cont.):Problem solving (Cont.):7. Apply Lact-aid-nursing by using formula supplementation during breastfeeding.
8. In case the nipple shield does not work, suggest mother to express milk and cup-feeding.9. After the infant is satisfied, suggest mother to cover nipple with a breast cup by gently inserting the nipple through the hole, then rotate the air-hold to the top and the base of a breast cup presses on areola then the nipple is everted.

38
Indicators:1. Infant death.2. Infant with congenital defect or illness, premature labor, cleft lip or palate, and abnormal GI system.3. Infant has allergy to mother’s milk.4. Mother has HIV infection, heart, pulmonary disease, or other disease.5. Mother receives medication that can transport through breast milk.6. Mother has intensive mastitis.7. Mother has psychological or neurological problem.

39
Procedure:Procedure:
1. Suggest mother to wear a supportive wear a supportive brabra.
2. Do not express, express, suck, pump or suck, pump or massagemassage the breast as this will encourage engorgement.
3. Do not place heat heat compress on breastscompress on breasts as it will stimulate vasodilatation and milk glands to produce milk and continue lactating.

40
ReferencesReferencesReferencesReferences
Lowdermilk, D.L., Perry, S.E., & Piotrowski, K.A. (Eds.). (2004).
Maternity & Women’s Health Care (8th Ed.). St.Louis: Mosby.
Pillitteri, A. (2003). Maternal & Child Health Nursing: Care of the
childbearing & childrearing family (4th Ed.). Philadelphia:
Lippincott Williams & Wilkins.
Reeder, S.J., Martin, L.L., Koniak-Griffin, D. (1997). Maternity
Nursing (18th Ed.). New York: Lippincott.
Varney, H. (1997). Varney’s Midwifery (3rd Ed.). Sudbury, MA:
Jones and Bartlett Publishers.

41
Question & Question & AnswerAnswer
Thank You for Your Thank You for Your AttentionAttention