Embed Size (px)
Citation preview

1
הפרעות במצב הרוח
Diagnosis and treatment

First, a quick reminder…
• Remember, by definition, a “primary” psychiatric disorder can be neither:– Attributable directly to the effects of a
substance (intoxication or withdrawal)– Better explained as a manifestation of an
underlying medical condition

Fact: Depression is grossly under-diagnosed

Üstün and Sartorius (1995); Murray and Lopez (1996)
Prevalence – 10%.
Depression
Recognised – 5%.
Treated – 3%.
World Health Organisation’s guideline for length of treatment for depression is 12 months.
Actual length of treatment is 3-4 months.

1. Depression Guideline Panel. Depression in Primary Care: Volume 1. Detection and Diagnosis. Clinical Practice Guideline, Number 5. AHCPR publication no. 93-0550. April 1993.
2. National Vital Statistics Reports. Vol 48, No. 11, July 24, 2000.
Depression and Suicide
Up to 15% of patients with MDD severe enough to require hospitalization eventually commit suicide1
Suicide is the 8th leading cause of death in the U.S.2

Why We Miss the Diagnosis:
• False assumption that a stressor or loss warrants a “clinical” depression
• Improper screening in primary care• Misperception by patients that it’s
deserved (guilt) or normal to feel down

Why We Miss the Diagnosis:
• Cultural sanctions against mental illness
• Atypical Symptom presentations:– Children: irritability, conduct disturbance– Elderly: pseudodementia or masked
depression – Cultural-specific presentations (ex.
physical symptoms)

Underdiagnosis and undertreatment of depression
• Stigma
• Lack of public knowledge
• Patients do not always complain of depressed mood
• Depressive symptoms are often masked by somatic anxiety or other medical conditions
• Poor compliance with therapy
Contributing factors:
Depression Guideline Panel. Depression in Primary Care: Vol 1, Detection and Diagnosis, 1983

Major Depression; symptoms
• Depressed mood• Diminished interest• Loss of appetite/ weight loss• Psychomotor retardation• Loss of energy• Feelings of worthlessness/ feelings of guilt• Diminished ability to concentrate• Suicidal thoughts• Insomnia• Anxiety symptoms

What is severe depression?
1. Hospitalised
2. Psychotic
3. Endogenous depression (Newcastle Scale)
Melancholia (ICD-10, DSM-IV)
4. High scores on a global severity scale (CGI)
5. High scores on a rating scale (HAMD, MADRS)
Guelfi et al (1992) : 1 + 3 + 5
Angst (1993) : 1 + 2 + 5
Angst et al (1995 ) : 1 + 2 or 1 + 5

Definition of severe depression
• Diagnostic criteria according to DSM-IV and ICD-10• Severity of depressive symptoms (e.g. 17-HAMD > 25)• Hospitalization• Endogenous depression (NEDRS > 6)• Constellation of symptoms• Presence of psychotic features• Overall symptomatic + functional impairment (e.g. GAS <
50)

Outlook
• Life time prevalence 4,1 - 19,6%• Point prevalence 5 - 8%• Untreated one episode of depression lasts an average of
10 months
• About 50 per cent of individuals who experience one episode of depression will have a further attack
• The average number of recurrences in a life time is 5

Depression
• Affects all ages and cultures
• Woman; men-ratio (in adults) 2 : 1
• Not related with: - education - ethnic differences - income - marital status

Overview of the Disorders

Unipolar/ Depressive Disorders
• Major Depressive Disorder

Bipolar Disorders
• Bipolar Disorder Type I
• Bipolar Disorder Type II
• Cyclothymic Disorder

Some Basic Definitions First

Euthymia
• Euthymic mood/affect: normal range of mood states; implying the absence of depression or elevated mood

Anhedonia
• Loss of interest in, and withdrawal from all regular and pleasurable activities

Expansive
• Expansive mood/affect: expression of one’s feelings without restraint, frequently with an overestimation of one’s importance
• Often associated with grandiosity

Euphoria
• Intense elation with feelings of grandeur

Dysphoria
• Dysphoric Mood: an unpleasant mood

The Building Blocks
Major Depressive Episode
Manic Episode
Mixed Episode
Hypomanic Episode

1. Insomnia or hypersomnia
2. Depressed mood or loss of interest or pleasure
3. Feelings of worthlessness
4. Fatigue
5. Diminished ability to think or make decisions
6. Weight change
7. Psychomotor retardation or agitation
8. Preoccupation with death,hopelessness
DSM-IV Criteria for Major Depressive Episode
5 symptoms in the same 2-week period
DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000.

What’s a “Major Depressive Episode?”
• At least 2 weeks of feeling depressed, OR losing interest in previously pleasurable activities (anhedonia), plus…
• Some additional characteristic symptoms of depression

What are these other Characteristic Symptoms?– Appetite changes– Trouble with sleep– Psychomotor agitation or retardation– Fatigue or low energy– Lots of worthlessness and guilt– Poor concentration– Indecisiveness– Suicidal ideations

Major Depressive Episode: Additional Criteria
• The depression must cause significant distress or functional impairment
• Depressive symptoms don’t have a medical cause and cannot be attributed to drug intoxication, withdrawal, etc.

Manic Episode
• At least one week of feeling euphoric, expansive, or irritable, plus…
• Some additional characteristic symptoms of mania

What are these additional characteristic symptoms?
– Grandiosity– Decreased NEED for sleep– Rapid or pressured speech– Flight of ideas and/or racing thoughts

Characteristic Symptoms of Mania (continued)
– Increased distractibility– Increased goal-directed activity– Agitation– Impulsivity– Hedonism, increased risk-taking behavior
Additional Criteria of Mania
• Person must experience either:– Profound difficulty functioning– Psychotic symptoms– Or represent a danger to themselves or
others, and hence need hospitalization

Things that look like Mania:
• Mania has a large differential: – ADHD– Compulsive Disorders (Shoplifting, etc.)– Impulse Control Disorders– Schizophrenia– Personality Disorders– Substance Intoxication– Secondary Mania (medical cause)

Mixed Episode
• When a person has symptoms of both mania and depression at the same time

How is that possible?
• Decreased need for sleep, insomnia
• Psychomotor agitation (due to increased energy or nervous energy)
• Poor concentration (due to distractibility)
• Decreased appetite (due to excessive goal-directed activities)
• Irritability
Hypomanic Episode
• At least four days of feeling euphoric, expansive, or irritable, plus…
• Some other characteristic symptoms of mania
• Change in functioning from baseline, observable by others, but not psychotic, dangerous, or markedly impaired

And now…the disorders

Unipolar/ Depressive Disorders

Major Depressive Disorder
• A syndrome of recurrent depressive episodes that cause significant distress or problems functioning

Major Depressive Disorder
• Technically, defined by one or more Major Depressive Episodes
• Usually episodic (occasionally chronic)
• Aka: MDD

MDD: Epidemiology
• Lifetime prevalence of up to 25% in women, up to 12% in men, hence
• Female/Male ratio is 2:1

Prevalence of depression in other chronic illnesses
(%)
Multiple sclerosis 6–57
Stroke 30–50
Cancer (inpatients) 42
Parkinson’s disease 40
Diabetes mellitus 33
Coronary artery disease 18–26
Goldberg. Depression in medical patients RI Med 1993

1. Frasure-Smith N, et al. JAMA. 1993;270:1819-1825.
2. Penninx BW, et al. Arch Gen Psychiatry. 2001;58:221-227.
3. Jiang W, et al. Arch Intern Med. 2001;161:1849-1856.
4. Vaccarino V, et al. J Am Coll Cardiol. 2001;38:199-205.
5. Rovner BW, et al. JAMA. 1991;265:993-996.
6. Pohjasvaara T, et al. Eur J Neurol. 2001;8:315-319.
Depression May Worsen Outcome of Many General Medical Conditions
• Depression may worsen morbidity and mortality after myocardial infarction1,2
• Depression increases morbidity and mortality in patients with CHF3,4
• Depression increases risk of mortality in patients in nursing homes5
• Depression worsens morbidity post-stroke6

What Causes Depression?
Bio-Psycho-Social Etiology

MDD Etiology: Biology
• Abnormalities in neurotransmission involving Norepinephrine, Serotonin, Dopamine, and possibly Acetylcholine
• Genetics/ Familial link: 1st degree relatives are at much higher risk
MDD Etiology: Psychology
• Significant losses, traumas, abuse, neglect during development
• Loss of a parent before the age of 11 is life event most associated with development of depression
• Poor coping strategies, certain personality disorders

MDD Etiology: Social
• Recent stressful events = powerful predictor of depression
• Initial episode often has a precipitator
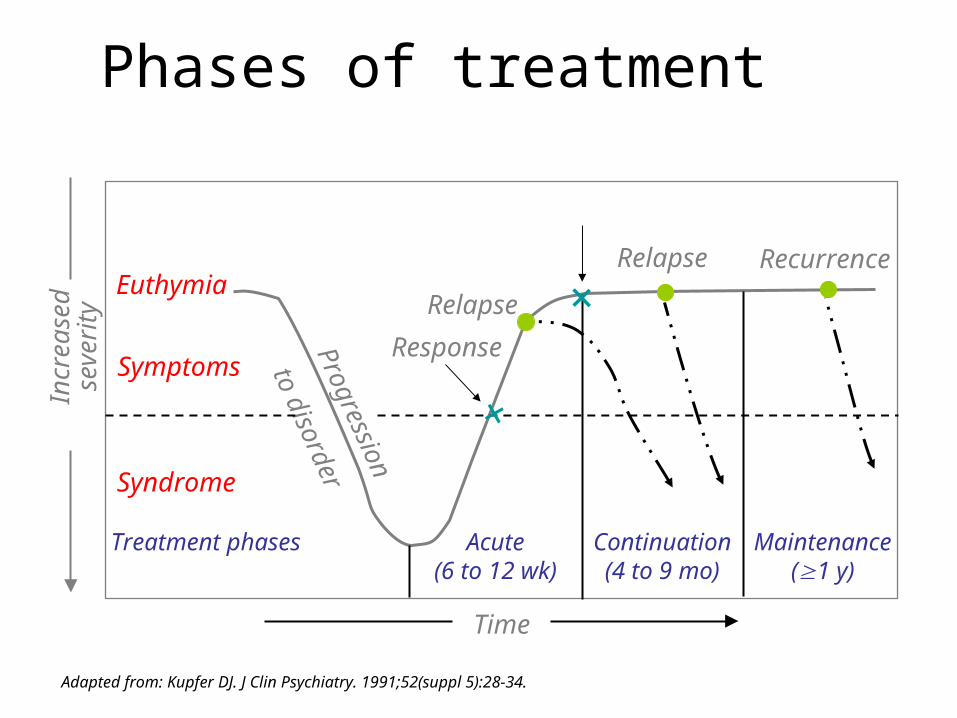
Euthymia
Symptoms
Syndrome
Treatment phases
Progression
to disorder
Acute(6 to 12 wk)
Continuation(4 to 9 mo)
Maintenance(1 y)
Time
Incr
ease
dse
veri
ty Relapse
Remission
RecurrenceRelapse
Response
Adapted from: Kupfer DJ. J Clin Psychiatry. 1991;52(suppl 5):28-34.
+
+
Phases of treatment

Nierenberg AA, et al. J Clin Psychiatry. 1999;60(suppl 22):7-11.
The goal of treatment in clinical practice should be remission of symptoms
Treatment of Depression: Facing the Problem

-DSM-5יעדי ה "not otherwise specified•להפחית משמעותית אבחנות
NOS ," ולקבוע קריטריונים יותר ספציפיים •להוסיף לאבחנות מימד נוסף של הערכת חומרה של
הסימפטומים.•ליישר קו עם ארגון הבריאות העולמי ולשאוף להתאמה
בין האבחנות-ICDלבין אלו שצפויים להופיע ב - DSM-5והקריטריונים ב
11- •לוודא שהקריטריונים להגדרה ולאבחנה של הפרעות ה-
DSM ישקפו את העדויות המחקריות העדכניות והחזקותביותר.
•לשאוף לכך שארגון הפרקים ומסגרת המדריך ייערכו לפי רצף התפתחותי שיסייע להבין את קשרי הגומלין בין
ההפרעות השונות.

-DSM-5שינויים מבניים ב •ביטול המערכת הרב-צירית: האבחנות לא יתבססו
חמשת הצירים5לפי שיטת •הערכה רב מימדית: הכוללת גם ניסיון להערכת
חומרת הסימפטומים•ארגון מחדש של סדר הפרקים במדריך: הפרקים אורגנו כך שישקפו את יחסי הגומלין בין ההפרעות
שבבסיסן מאפיינים דומים של סימפטומים ושל פגיעות. 3מספר האבחנות נשאר כמעט ללא שינוי, אך נוספו
פרקים •טרמינולוגיה: בכל ההפרעות בהן היה שימוש במונח
general medical condition :הוחלף המינוח ל another medical condition על-מנת לחזק ולשרש
את תפיסת מקצוע הפסיכיאטריה כמקצוע רפואי

-DSM-5שינויים ספציפיים ב
•Bipolar and Related Disorders
Bipolar and Related Disorders מופיע Moodכפרק נפרד ולא תחת פרק
Disorders -כפי שהיה בDSM-IV-TR•כדי להגדיל את הדיוק של האבחנה
ולאפשר זיהוי מוקדם במסגרות הקליניות, של אפיזודות מאניות Aקריטריון
והיפומאניות שם כעת דגש על שינויים בנוסף למצב הרוח בפעילות ובאנרגיה

-DSM-5שינויים ספציפיים ב
•Bipolar and Related Disorders Mixed Bipolar Iאבחנת DSM-IV-TRב- •
Disorder, Most Recent Episode דרשה שהאדםזמנית גם את הקריטריונים לאפיזודה ימלא בו
מאנית וגם את הקריטריונים לאפיזודה של מופיע - DSM-5. במקום זאת ב דיכאון
specifier חדש with mixed features שיכול להתאים
לאפיזודות של מאניה או היפומאניה

-DSM-5שינויים ספציפיים ב
Other Specified Bipolar and Related Disorderמצוינים מצבים מיוחדים לאבחנה זו הכוללים:- DSM-5ב - אנשים עם היסטוריה של הפרעת דיכאון מאג'ורי שיש 1
להם את כל הקריטריונים להיפומאניה מלבד קריטריון - ימים רצופים4הזמן כלומר, משך הסימפטומים פחות מ
- יש מעט מידי סימפטומים של היפומאניה כך שלא 2המלא של Bעונים על קריטריון Bipolar II Disorder , אבל משך הופעת הסימפטומים הוא
ימים או יותר.4לפחות

-DSM-5שינויים ספציפיים ב
Anxious Distress Specifierלמצוקה חרדתית שנוסף בפרק של specifierזהו • Bipolar and Related Disorders ובפרק של.Depressive Disorders

-DSM-5 שינויים ספציפיים ב
Depressive Disordersכפי Mood Disorders מופיע כפרק נפרד ולא תחת פרק:וכאן הוסיפו -DSM -שהיה ב•Disruptive Mood Dysregulation Disorder
המתאפיינים באי שקט 18אבחנה חדשה של ילדים עד גיל קבוע ואפיזודות תכופות של אי שליטה קיצונית בהתנהגותPremenstrual DysphoricDisorderPersistent Depressive Disorder (Dysthymia)DSM-IV-TR: -אבחנה זו מאחדת את שתי האבחנות שהופיעו בDysthymic DisorderChronic Major Depressive Disorder

Depressive Disorders
Bקריטריון - DSM-5עובר להיות ב Major Depressive Episodeשל Cקריטריון תוכן הקריטריון ללא שינוי: הסימפטומים צריכים לגרום לפגיעה או מצוקה משמעותית
קלינית בתפקוד החברתי, התעסוקתי או בתפקוד בתחומים חשובים אחרים. ומעלה3הישן, כאשר יש אפיזודה של דיכאון מאג'ורי ובמקביל B•במקום קריטריון
סימפטומים מאניים אך עדיין מצב שאינו עונה על כל הקריטריונים של אפיזודה with mixed features specifierמאנית האבחנה תעשה שימוש ב-
כל עוד אין עמידה בקריטריונים של אפיזודה מאנית או היפומאנית, נשארת האבחנה הראשית של הפרעת דיכאון מאג'ורי ולא של הספקטרום הדו-קוטבי.
Bereavement Exclusion• Major Depressive Episodeשל Eמבוטל קריטריון - DSM-5ב

Specifiers/ Subtypes

MDD: Specifiers/Subtypes
• Melancholic Features
• Atypical Features
• Catatonic
• Postpartum
• Seasonal
• With Psychotic Features

“Melancholia”- black bile
• Extreme anhedonia
• Lack of mood reactivity
• Decreased sleep and appetite
• Worse in the AM (diurnal variation)
• Early morning awakenings
• Excessive guilt

Atypical Depression
• Mood reactivity
• Excessive sleep and eating
• Interpersonal rejection sensitivity
• More common in women
• Closer link to Bipolar Disorder

Psychotic Depression
• With hallucinations or delusions
• Usually mood-congruent
• Usually indicative of a severe episode

Postpartum Depression
• Far beyond the “Baby Blues”
• Often associated with psychosis
• More suggestive of Bipolar illness
• Far more common in women than men

Outlook
• Untreated one episode of depression lasts an average of 10 months
• About 50 per cent of individuals who experience one episode of depression will have a further attack
• The average number of recurrences in a life time is 5

1. Depression Guideline Panel. Depression in Primary Care: Volume 1. Detection and Diagnosis. Clinical Practice Guideline, Number 5. AHCPR publication no. 93-0550. April 1993.
2. National Vital Statistics Reports. Vol 48, No. 11, July 24, 2000.
Depression and Suicide
• Up to 15% of patients with MDD severe enough to require hospitalization eventually commit suicide1
• Suicide is the 8th leading cause of death in the U.S.2

Dysthymic Disorder
Chronic, low-grade depression
Dysthymic Disorder
• Two or more years of depression of moderate severity
• Person feels depressed more days than not and never goes more than 2 months without symptoms
• Previously called “Depressive Personality Disorder” and “Neurotic Depression”

Dysthymic Symptoms
• Change in appetite
• Change in sleep
• Low energy
• Low self worth
• Poor concentration
• Hopelessness

Epidemiology of Dysthymia
• Female: Male ratio is 3:1
• Often has insidious onset in early adolescence
• Often co-morbid with certain personality types

Depression NOS
Not Otherwise Specified

Depression NOS (examples):
• Premenstrual Dysphoric Disorder
• Not enough information to narrow diagnosis

Bipolar Disorders

Bipolar Disorder Type I
• An episodic illness characterized by recurrent episodes of mania and depression, usually with good inter-episode recovery
• Technically, only need a single Manic or Mixed episode to make the diagnosis
Bipolar I: Epidemiology
• Earlier onset than MDD
• Male: Female ratio is equal
• Strong genetic component: Twin studies show very high concordance

Bipolar Tidbits
• Psychotic features often present– Abnormal thought form– Perceptual abnormalities– Delusions– Disorganization
• Postpartum psychosis often = Bipolar

755-5 Stahl S M, Essential Psychopharmacology (2000)
DEPRESSION
NORMAL MOOD
MANIA
HYPOMANIA
MIXED EPISODE

Seasonal Affective Disorder
• Variant of Bipolar Disorder
• Consistent seasonal pattern to occurrence of episodes

Rapid Cyclers
• Specify “rapid cycling” if patient has 4 or more mood episodes in a given year

78
12 months
DEPRESSION
NORMAL MOOD
RAPID CYCLINGRAPID CYCLING
5-6 Stahl S M, Essential Psychopharmacology (2000)

Bipolar Disorder II
• An episodic illness characterized by recurrent episodes of hypomania and major depression, usually with good inter-episode recovery
• No Manic or Mixed Episodes
• Rarely require hospitalization

Cyclothymic Disorder
Chronic fluctuations between minor mood episodes

Cyclothymic Disorder
• Chronic
• Duration of 2 or more years
• Numerous Hypomanic and Minor Depressive Episodes
• Few periods of euthymia (ie., never symptom-free for more than 2 months)

Bipolar Disorder NOS
• When distinction between Type I vs. II vs. Cyclothymia cannot be made
• When underlying cause (ex. Substance or General Medical Condition) has not yet been ruled out

Other Mood Disorders

Mood Disorder Due to a GMC (General Medical Condition)
• Large number of conditions produce symptoms of depression, mania

Neurological
• Parkinson’s Disease • Huntington’s Disease• Stroke• Tumors• Central Nervous System Infections• Autoimmune Disorders like Lupus• Dementia

General Medical Conditions:
• Systemic Infections– AIDS, Epstein Bar Virus
• Endocrine Abnormalities– Thyroid, Adrenal (Cushing’s Disease)
• Cardiovascular Disease– After Heart Attacks
• Certain Carcinomas– Pancreatic Cancer

Substance-Induced Depression
• Variety of substances can cause depression
• Cardiovascular Drugs– Antihypertensives (notoriously Beta
Blockers) and Digitalis

Substance-Induced Depression
• Sedative/Hypnotics– Chronic use of Alcohol, benzodiazepines
• Steroids and Hormones– Oral contraceptives and steroids may
precipitate depression (and mania)
Substance-Induced Depression
• Stimulants– Repeated use of Amphetamines, cocaine
may deplete neurotransmitters
• Antipsychotics– Often via secondary negative symptoms
• Analgesics– Chronic use may cause depression

Substance Induced Mania
• Variety of substances may induce mania
• Dopamine agonists– May also cause psychosis
• Sympathomimetics– Cocaine, Amphetamine, PCP intoxication
• Steroids

The End





























