Embed Size (px)
Citation preview

EDITOR-IN-CHIEF
Dr. Shobha Rani R. Hiremath [email protected]
ASSOCIATE EDITORS
Dr. G. Parthasarathi Dr. Pramil [email protected] [email protected]
ASSISTANT EDITORS
Mr. Ramjan Shaik Ms. Mahvash Iram [email protected] [email protected]
EDITORIAL OFFICE
INDIAN JOURNAL OF PHARMACY PRACTICE
An Official Publication of Association of Pharmaceutical Teachers of India
H.Q.: Al-Ameen College of Pharmacy,
Opp. Lalbagh Main Gate, Hosur Road, Bangalore 560 027, INDIA Mobile: +91 9845399431 | +91 9845659585 | +91 9878488050 | +91 9972588878
+91 9916069842 | Ph: +91 80 22107467; Fax: +91 80 22225834www.ijopp.org || [email protected]
Vol.3(2), Apr-Jun, 2010
A
P
T
I
ijopp
Indian Journal of Pharmacy Practice

EDITORIAL ADVISORY BOARD
Dr. Anil Kumar, Chattisgarh
Dr. Atmaram P. Pawar, Pune
Dr. Claire Anderson, UK.
Dr. Dhanalakshmi Iyer, Mumbai
Prof. Ganachari M S, Belgaum
Dr. Geeta.S, Bangalore
Dr. Hukkeri V.I, Ratnagiri (Dist)
Dr. Krathish Bopanna, Bangalore
Prof. Mahendra Setty C.R, Bangalore
Dr. Miglani B D, New Delhi
Dr. Mohanta G.P., Annamalai Nagar
Disclaimer: The editor-in-chief does not claim any responsibility, liability for
statements made and opinions expressed by authors
Vol.3(2), Apr-Jun, 2010
Nottingham,
Dr. Nagavi B.G, Ras Al-Khaimah, UAEDr. Nalini Pais, BangaloreDr. Rajendran S.D, HyderabadDr. Ramananda S.Nadig, Bangalore Dr. Revikumar K G, CochinDr. Sampada Patawardhan, MumbaiDr. Sriram. S, CoimbatoreDr. Sreekant Murthy, Philadelphia, USADr. Sunitha C. Srinivas, Grahamstown, RSADr. Suresh B, MysoreDr. Tipnis H.P, Mumbai
ijopp
Indian Journal of Pharmacy Practice

CONTENTS
Editorial
Review Articles
= Citalopram Drug Interactions
Dilip KV, Mahesh NM, Raghunathaguptha A------------------------------------------------------------------------1-10
Research Articles
=Evaluation of prescription pattern in terms of essentiality and rationality and assessment of Hospital
pharmacy services utilization in tertiary care teaching rural hospital.
Shah AM, Dhanani JV, Shah RB, Agrawal A, Gajjar BMr--------------------------------------------------------11 -15
Pattern of potential medication errors in a tertiary care hospital in Nepal.
Kadir A, Subish P, Anil K, Ram B----------------------------------------------------------------------------------16-22
l Study of prescription practice for Antipsychotic drugs by Psychiatrists- A Survey
Mukesh R, Mohanta GP, Lokesh U--------------------------------------------------------------------------------23-27
=A retrospective review on Malaria and Antimalarial drugs in Tripura, India – A Survey Report
Mallik S, Nilesh K, Rajesh G---------------------------------------------------------------------------------------28-33
l Comparative Study on the Sensitivity Pattern of Microorganisms
Vidhya D, Sriram S, Manjula Devi A.S, Rajalingam B, Shivashankar S, Chitra B, Rajeswari R--------34-40
Vol.3(2), Apr-Jun, 2010
l
ijopp
Indian Journal of Pharmacy Practice

Short Communication
=Counterfeiting of medicine is no more incurable now
Sayed AHA-------------------------------------------------------------------------------------------------------------41-42
=Medicines Procurement Practices in Public Sector
Mohanta GP, Veena R------------------------------------------------------------------------------------------------43-45
Case Report
= Lamotrigine Induced Erythema Multiforme: A Case Report
Mahvash I, ShobhaRani R.H, MeghaBhat.Y----------------------------------------------------------------------46-49
=Ibuprofen Induced Stevens Johnson Syndrome -A Case Report
Tapan S, Yogesh BS, Amit R-----------------------------------------------------------------------------------------50-53
Instructions to authors-----------------------------------------------------------------------------------------54-57
Vol.3(2), Apr-Jun, 2010
ijopp
Indian Journal of Pharmacy Practice

Editorial
Dear Readers,
Season’s greetings to you all! Many thanks for your encouragement to ijopp in the form of contribution of
articles and readership. We value your support.
One of the key areas of Clinical Pharmacy is ‘Pharmacovigilance’ and an important activity of a clinical
pharmacist is ADR monitoring.
‘Pharmacovigilance’ as we all know is the science relating to the detection, assessment, understanding and
prevention of adverse effects of drugs.
‘Pharmacovilance’ is currently of global improtance due to the reporting of several life threatening and fatal
drug reactions, increased awareness of consumers regarding drug safety, withdrawal of few drugs in some
countries leading to doubts regarding their safety in our country.
In India, Central Drugs Standard Control Organization (CDSCO) launched a National Pharmacovigilance
Programme in Nov 2004. It identified zonal, regional and peripheral centres across the nation to collect,
document and report the ADRs. This was a welcome move towards monitoring drug safety. Centres involved
were also actively participating in the programme.
But unfortunately from the past two years due to certain reasons best known to them, National
Pharmacovigilance Programme has come to a stand still.
Our earnest hope is the revival of this programme with the participation of self motivated centres and
involvement of more clinical pharmacists and Pharmacy Practice departments.
Dr. Shobha Rani R Hiremath
Editor-in-Chief

INTRODUCTION
Citalopram is an antidepressant drug belonging to pharmacodynamic drug interactions are likely to occur
selective serotonin reuptake inhibitor (SSRI) class. with citalopram. Citalopram is frequently prescribed to
Citalopram selectively inhibits serotonin (5HT) reuptake treat the depressive patients when compared to other
into the presynaptic neurons. This leads to elevated SSRI class antidepressants such as fluoxetine, sertraline,
serotonin levels in the synaptic clefts. Serotonin acts on fluoxamine and paroxetine. Fluoxetine, sertraline,
different types of serotonin receptors to produce fluoxamine and paroxetine can cause severe adverse drug
antidepressant and other pharmacological effects. interactions with other drugs when compared to 2Citalopram is demethylated by CYP2C19 and CYP2D6 citalopram. Hence, all the drug interactions identified
to N-desmethylcitalopram and N-desmethylcitalopram with citalopram were reviewed to know its interaction
is further demetylated to di-desmethylcitalopram by potential especially when used to treat the depressive 1
CYP3A4. Both of its metabolites are inactive. Some patients with or without co-morbidity.
drugs which induce or inhibit these enzymes can also Interaction Potential of citalopram
alter the plasma concentrations of citalopram by altering Citalopram has the potential to interact with many drugs its liver metabolism. Citalopram is an inhibitor of through the pharmacodynamic and pharmacokinetic CYP2D6 and also a weak inhibitor of CYP2C19 and mechanisms. Its pharmacodynamic interaction is due to
CYP3A4. Hence, the plasma concentration of drugs elevated levels of 5HT in the synaptic cleft. Such which are substrates of these enzymes may be affected. citalopram pharmacodynamic interaction was observed And some drugs which have the potential to affect the with non-steroidal antiinflammatory drugs (NSAIDs), synaptic levels of serotonin may affect the outcome of antimigraine, anxiolytics, tricyclic antidepressants, citalopram therapy. Thus, pharmacokinetic and monoamineoxidase inhibitors, beta blockers and opioids.
Pharmacokinetically, citalopram inhibits different drug
metabolising CYP450 isoenzymes. This mechanism
increases the plasma levels of desipramine, trazadone,
Abstract
Citalopram is an antidepressant belonging to selective serotonin reuptake inhibitors. Citalopram produces its
activity by inhibiting the reuptake of serotonin in the synaptic clefts. So, concomitant administration of drugs
(opioids, Monoamino oxidase inhibitors) which are having affect on serotonin or other monoamine levels in the
synaptic cleft may produce some adverse effects as a pharmacodynamic interaction. Citalopram is metabolized by
CytochromeP450 (CYP) 2C19 and CYP2D6 to desmethylcitalopram and further by CYP3A4 to di-
desmethylcitalopram. Some drugs may either induce (carbamazepine and rifapicin) or inhibit (buspirone, tramodol,
Tricyclic antidepressants) these enzymes and affecting the citalopram levels producing either therapeutic failure or
serotonin toxicity. Similarly, citalopram mildly inhibits CYP2C19, CYP2D6 and CYP3A4 and thus affects the plasma
levels of the drugs (imipramine, â-blockers, trazodone) which are metabolized by the above enzymes. So, in this
review we tried to summarize both the interactions of citalopram with other drugs and other drugs interaction with
citalopram and their probable mechanisms which may be helpful for the psychiatrists or physicians to judge the
appropriate therapy when the patient is to be co-administered with citalopram.
Key words: Citalopram; Drug interactions; Pharmacodynamic; Pharmacokinetic.
APTI ijopp
Citalopram Drug Interactions1 1 2
Dilip Kumar V , Mahesh NM* ,Raghunathaguptha A1Department of Pharmacology, J.S.S. College of Pharmacy (Constituent College of J.S.S.
2University, Mysore), S.S. Nagar, Mysore-570 015, Karnataka; Guptha's Clinic, Neuropsychiatry, Agrahara,
Mysore-570004, Karnataka
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on 23/03/201 0
Accepted on 29/03/2010 © APTI All rights reserved
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
1

2
aripiprazole, haloperidol, clozapine, reserpidone, inhibition of CYP3A4 metabolising enzymes
metoprolol and perhexitine. Citalopram plasma levels responsible for the metabolism of trazodone. Increased
can be decreased by carbamazepine and rifampicin, trazodone plasma levels may result additive serotonergic 10,11which induce CYP2C19, CYP3A4 and CYP2D6 effects like serotonin syndrome.
3,4enzymes. The interaction of many drugs with Antiparkinsonian drugs
citalopram is individually explained with respect their Citalopram can decrease the bioavailability of selegiline. effect on clinical outcome. The bioavailability of selegiline was reduced by 30% in Citalopram interactions with other drugs the presence of citalopram in a study involving 18
Non steroidal anti inflammatory drugs healthy subjects who were given citalopram 20 mg or a
All selective serotonin reuptake inhibitors (SSRIs) placebo daily for 10 days followed by four days with
(example, citalopram) increase the risk of upper concurrent selegiline (10 mg/day). However, there was
gastrointestinal bleeding. This effect is potentiated by no change in the serum concentrations of the three main
concurrent use of NSAIDs in depressive patients who are metabolites of selegiline and also vital signs or frequency
under treatment of SSRIs. The risk of upper of adverse events. The study concluded that there is no
gastrointestinal bleeding was found to be increased in the clinically relevant interaction between selegiline and 12range of 5.2% to 12.2% when SSRIs and NSAIDs were citalopram.
5 administered together. SSRIs inhibits the serotonin Cardiovascular drugstransporter, which is responsible for the uptake of
Concurrent use of metoprolol and citalopram resulted in
serotonin into platelets. Serotonin released from platelets the twofold increase in the plasma levels of metoprolol.
in response to vascular injury promotes the
This may decrease its cardioselectivity. This interaction
vasoconstriction and changes the shape of the platelets is due to inhibition of CYP2D6 and 2C19 isoenzymes by
leading to aggregation. SSRIs also inhibit the pulmonary SSRIs. These metabolizing enzymes are involved in the
endothelial metabolism of serotonin. It could thus be metabolic clearance of beta-adrenergic blockers such as
predicted that SSRIs would deplete platelet serotonin, carvedilol, labetalol, metoprolol, nebivolol, propranolol
leading to a reduced ability toform clots and a subsequent 10,13 and timolol. In another case study, citalopram raised 5,6
increase in the risk of bleeding.perhexiline levels when concurrently administered in an
Anticoagulants 14elderly man. In vitro studies with human liver
Citalopram can increase the maximum prothrombin time microsomes found that fluoxetine and paroxetine are
when co-administered with oral anticoagulants (e.g., potent inhibitors of metoprolol metabolism and
warfarin, acenocoumarol). Citalopram (40 mg/day) fluvoxamine, sertraline and citalopram less potent. These
increased the normal maximum prothrombin time by results suggest the need for monitoring of the changes in
6.4% in a patient who was taking warfarin. It was the cardiovascular dynamics when SSRIs and
considered as clinically insignificant as there was no 15
cardiovascular drugs are concurrently administered.7evidence of bleeding. But, in another 63-year-old patient
Anxiolyticswho was taking acenocoumarol (18 mg/week),
Citalopram was found to have no effect on alprazolam citalopram (20 mg/day) addition resulted in the plasma levels, although the time to maximum alprazolam spontaneous gingival haemorrhage after 10 days. The concentration was delayed by 30 minutes. The haemorrhage, however, stopped five days after prolongation of time of maximum plasma concentration citalopram was withdrawn. This suggests the ability of of alprazolam (T ) is probably due to the effect of maxcitalopram including other SSRIs to increase the risk of
citalopram on the absorption of alprazolam. It is possible bleeding by inhibiting serotonin levels and thus causing 8,9 that citalopram may have a yet undiscovered effect on P-decreased platelet aggregation.
glycoproteins in the gut or some other effect on the gut Atypical antidepressants16
wall to produce such effect.Citalopram can increase the plasma concentrations and
Antipsychoticspharmacodynamic aspect of trazodone. Citalopram
Escitalopram and citalopram in 6 patients taking increased the mean plasma concentrations of trazodone
by 30% when compared to the trazodone monotherapy in aripiprazole elevated the plasma levels of latter by 39%
depressive patients. This interaction is perhaps due to and 34% respectively than that was found in patients
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

3
17 medications were discontinued. But, rhabdomyolysis taking aripiprazole alone. Aripiprazole is metabolized
was found exacerbated upon restarting citalopram to treat by CYP3A4 and CYP2D6 isoenzymes. In two
the depression. When citalopram was discontinued, he individual studies in schizophrenics citalopram did not 18,19 improved over the next five days. It was thought that the affect the plasma levels of clozapine. But in another
levels of citalopram might have increased because study initiation of citalopram 20 mg/kg therapy in a
citalopram and irinotecan share at least one metabolic schizophrenic patient who was regularly under clozapine
pathway through CYP3A4 enzymes. The cytochrome treatment raised the plasma levels of clozapine. The
enzymes system may also have been compromised in the patient reported sedation, hypersalivation and confusion. 28
cancer patient.Total clozapine serum levels were found to be 1097
ng/ml. The total clozapine level dropped to 792 ng/ml Other drugs interaction with citalopram
when the citalopram dose was reduced to 20 mg daily and Anti-migraine drugs20
the symptoms resolved over the following 2 weeks. In a Concurrent administration of triptan (e.g., Almotriptan,
case study it was reported that a man with idiopathic eletriptan, frovatriptan, naratriptan, rizatriptan,
priapism for 4 hours every 1-2 months experienced a sumatriptan, zolmitriptan) and citalopram results in
prolonged bouts lasting for 6-8 hours when he was given serotonin syndrome. Serotonin syndrome occurs due to
resperidone. Then he experienced almost daily erections excessive serotonergic effect. The symptoms include
when he was given with citalopram with reduced restlessness, hallucinations, loss of coordination, 21
resperidone dose which lasted for 12 hrs. Another study tachycardia, rapid changes in blood pressure,
found that paroxetine, fluoxetine and sertraline increased hyperthermia, over reactive reflexes, nausea, vomiting,
olanzapine levels by about 32%, but citalopram had no and diarrhoea. Triptans are the agonists of 5HT 1B/1D
22 effect. SSRIs including citalopram inhibit CYP2D6 receptors. SSRIs cause the accumulation of serotonin at
29,30isoenzyme involved in the metabolism of the the synaptic clefts. Combined use of these drugs
antipsychotics to cause such interactions. results in serotonin syndrome due to additive Tricyclic antidepressant serotonergic effect at the synaptic level. The clinicians
should be aware of this drug interaction for better patient The contradictory reports are available about the 31
pharmacokinetic interaction outcome associated care.
between tricyclic antidepressants and citalopram. In five Appetite suppressant
patients who were taking amitriptyline, clomipramine or Serotonin syndrome may occur when appetite maprotiline, addition of citalopram (20 to 60 mg/day), suppressants such as sibutramine, dexfenfluramine or did not change the plasma tricyclic antidepressant fenfluramine are co-administered with citalopram. A 43-
23 levels. But, in a study in eight healthy volunteers year-old depressive woman taking citalopram 40 mg
citalopram caused 50% increase in the area under the daily was given sibutramine 10 mg daily to treat
curve of desipramine, a primary metabolite of obesity.Within a few hours of taking the first dose of
imipramine. This was attributed to the strong ability of sibutramine, symptoms of serotonin syndrome
desmethylcitalopram to inhibit CYP2D6 enzymes developed and continued for three days till she continued 24
involved in the hydroxylation of desipramine. Similarly, to take sibutramine. Sibutramine inhibits the reuptake of
in another study, the levels of imipramine metabolites, norepinephrine, dopamine, and 5HT. Dexfenfluramine
desmethylclomipramine and 8-hydroxydesmethyl- and fenfluramine are nonspecific serotonin agonists that .25,26
clomipramine was found elevated. However, enhance the release of serotonin and also inhibit 32,33
citalopram was successfully substituted for paroxetine in serotonin reuptake. The combination of these drugs 34a case of tricyclic antidepressant toxicity during may thus leads to excessive serotonergic effects.
27coadministration of desipramine and paroxetine. Anxiolytics
Chemotherapeutic agent On administration of buspirone and citalopram,
Pharmacokinetic interaction was observed between the serotonin syndrome and hyponatraemia were produced
chemotherapeutic drugs and citalopram. A 74-year-old in an isolated case. Buspirone is metabolised by the same
man who had been taking citalopram for two months CYP3A4 isoenzymes responsible for the metabolism of
developed rhabdomyolysis after undergoing initial citalopram. This may have caused increase in the plasma
treatment with irinotecan for gastrointestinal cancer. All concentrations of citalopram leading excessive
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

4
35 Antiepileptic drugsserotonergic effect. There are no pharmacodynamic
interactions noted in clinical studies in which citalopram Approximately 30% plasma levels of citalopram were 36,37
was given with benzodiazepines But, alprazolam reduced when it was given along with carbamazepine.
significantly elevated the plasma levels of citalopram by Because, carbamazepine induces CYP3A4 isoenzyme 38 involved in the metabolism (N-demethylation) of 13%. Hence, caution is required when these drugs are
49required to be administered. citalopram. In contrast, increase in the plasma levels of
citalopram was observed when carbamazepine was Monoamine Oxidase Inhibitors50
replaced with oxcarbamazepine.Serotonin syndrome was observed in a 34-year-old
depressive patient when he was switched to citalopram Opioid analgesics
20 mg daily from moclobemide 100 mg administered The symptoms of serotonin syndrome and hallucinations 39
thrice a day for several months. Moclobemide and were observed when the opioid analgesics were
citalopram when taken in overdoses produces serotonin administered along with citalopram. A 70-year-old 40,41,42
syndrome and may even lead to death. Limited woman with mild recurrent depressive disorder who was
animal data on the effects of combined use of SSRIs and taking citalopram 10 mg daily for three years showed the
monoamine oxidase inhibitors suggest that these drugs symptoms of serotonin syndrome when started taking
may act synergistically to elevate blood pressure and tramadol 50 mg daily for pain relief following an
evoke behavioural excitation. In contrast these reports, operation. It was observed that CYP2D6 and CYP2C19 51citalopram does not appear to have any influence on the levels were lowered. A 44 year old woman who was on
wet-dog shakes response induced by the combination of a citalopram treatment for 9 months developed the signs of
monoamine oxidase inhibitor and L-tryptophan, which is serotonin syndrome after 24 hours of meperidine 43 52 a precursor of 5HT. administration. A 65-year-old patient chronically
treated with citalopram developed serotonin syndrome Selective Serotonin Reuptake Inhibitors
following initiation of fentanyl. It was concluded that The depressive patients, who did not respond to
development of serotonin syndrome is due to its property citalopram, have responded when another SSRI was co-
of inhibition of reuptake of serotonin causing administered. Fluvoxamine was (50 to100 mg/day) co-
overstimulation of the 5-HT and possibly the 5-HT administered in seven depressive patients who failed to 1A 2
respond to citalopram (40 mg/day) for three weeks. All receptors, resulting in manifestations of the serotonin 53patients responded. It was found that plasma S- syndrome. Visual hallucination occurred in a 90-year-
citalopram levels rose to two to threefolds due to old woman taking hydrocodone when her antidepressant
stereoselective inhibition of the metabolism of S- was changed from citalopram 10 mg daily to 44 54 citalopram by fluvoxamine. In non-responding escitalopram 10 mg daily. The seizures or myoclonus
depressive patients, the interaction of SSRIs results in the associated with citalopram treatment appeared to be
beneficial outcome. decreased in the threshold when concurrently 55
Lithium Carbonate administered with dextropropoxyphene. In all the above
cases, the symptoms of serotonin syndrome and A study conducted in healthy individuals concluded that
hallucination have stopped on discontinuing the there was no pharmacokinetic change when citalopram 54 45 administration of the opioids. Meperidine, fentanyl and and lithium carbonate were co-administered. But, the
other opioids are weak serotonin reuptake inhibitors. On depressive patients who did not respond to citalopram
co-administration of these drugs with citalopram may alone have responded well in combination with 46 produce higher levels of serotonin in the synaptic cleft, lithiumcarbonate without any signs of adverse effects.
which may result in the development of serotonin Even then the manufacturers cautioned the patients about 53
syndrome and other adverse outcome.excessive serotonin effects with the co-administration of 10,47
citalopram and lithium. Lithium may enhance the Antipsychotic Drugs
pharmacologic effects of citalopram through the Both pharmacokinetic and pharmacodynamic
hyperstimulation of the brainstem 5-HT1A and 5-HT2A interactions were observed between the typical and 48
receptors. atypical classes of antipsychotics and citalopram.
Levomepromazine increased the initial steady-state
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

5
plasma levels of desmethylcitalopram, the primary rifampicin 600 mg twice daily. His condition improved
metabolite of citalopram, between 10 and 20%. This when the rifampicin was stopped. Rifampicin is a potent
pharmacokinetic interaction was due to potent inhibition inducer of the hepatic CYP450 enzymes system,
o f t h e C Y P 2 D 6 i s o e n z y m e s a c t i v i t y b y particularly CYP3A4 isoenzymes involved in the
levomepromazine. CytochromeP4502D6 isoenzymes metabolism of citalopram. Induction of the CYP 56 enzymes may have decreased citalopram plasma levels to are involved in metabolism of desmethylcitalopram.
64 result in the therapeutic failure. Concomitant Urinary obstruction was observed in a 65 year old
administration of citalopram with fluconazole, an schizophrenic woman under treatment of aripiprazole
antifungal produces serotonin syndrome which may be of when co administered with citalopram. The mechanism
life threatening intensity. This interaction is concluded as of urinary retention has been attributed to its cholinergic
the outcome of fluconazole's potent CYP3A4 isoenzyme and central serotonergic effects. Aripiprazole is a partial 65
inhibiting property.agonist of dopamine D receptors and 5-HT serotonin 2 1A
DISCUSSIONreceptors. It blocks 5-HT serotoninergic, á -adrenergic 2 1
57 All selective serotonin reuptake inhibiting anti-and histamine-H receptors.1
depressants interact with many drugs. Of these The serotonin syndrome developed in a patient with antidepressants, interaction potential of citalopram is bipolar affective disorder who was taking lithium
2less. Nevertheless, citalopram was found to interact with carbonate and citalopram when olanzapine was added. many drugs. Reviewing of such drug interactions helps The syndrome was due to serotonergic side effects of psychiatrists to take the precautionary steps while olanzapine together with serotonergic effects of treating the patients with such interacting combinations. citalopram. These symptoms resolved on cessation of
58 Citalopram increases serotonin levels in the brain to olanzapine administration. Similarly, serotonin 1
produce antidepressant effect. It is prescribed either syndrome was reported in a 42 year old woman who was alone or in combination with drugs of different taking citalopram along with quitapine. It was mentioned therapeutic classes to treat the patients with depression that serotonin syndrome was a consequence of increased with or without co-morbid illnesses. Citalopram acts by brainstem and spinal cord 5-HT receptor modulation 1A
59 elevating serotonin levels in the synapse and it inhibits occurring with 5-HT receptor antagonism. These 2A
the cytochrome isoenzymes like CYP2C19, CYP2D6 reports suggest that the psychiatrists are required to be
and CYP3A4 involved in the metabolism of many drugs. alert about the adverse outcome associated with the
This may leads to pharmacodynamic and combination of antipsychotics and citalopram.
pharmacokinetic drug interactions due to citalopram. In Tricyclic antidepressants
contrast, other drugs also potentially interact with In a study conducted in 18 patients who were taking
citalopram by pharmacodynamic and pharmacokinetic citalopram and tricyclic antidepressants, the serum levels mechanisms. These reports suggest that the citalopram
60 of citalopram was found increased by 44%. This behaves like a precipitant and/or index drug to result in interaction was related to the ability of tricyclic drug-drug interactions. antidepressants to inhibit mildly CYP2C19 enzymes
Pharmacokinetically, citalopram affects the plasma 61
involved in the metabolism of citalopram. concentrations of other drugs. It has increased the plasma Chemotherapeutic agents levels of atypical antipsychotics, trazodone and â-
In another case report, 85-year-old woman taking adrenergic receptor blockers to the different extent by
citalopram developed the symptoms of serotonin inhibiting the CYP450 isoenzymes mentioned
syndrome after linezolid was started. Symptoms were elsewhere. Citalopram elevated the plasma levels of 62 16 resolved over 72 hours upon discontinuing citalopram. aripiprazole up to 34% in six patients. And metoprolol
13 Linezolid is a reversible non-selective inhibitor of plasma levels were increased by twofold. But, the monoamine oxidase. It has the potential to interact with patients from both the studies did not report any side
63adrenergic and serotonergic agents. effects. Citalopram (40mg daily), on co-administration
In 55-year-old man who was taking citalopram 40 to 60 with clozapine in schizophrenics reported sedation,
mg daily reported a decrease in therapeutic efficacy hypersalivation and confusion with the clozapine serum
(increased crying and panic attacks) after starting levels of 1097 ng/ml. And the symptoms resolved when
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

6
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
the dose is reduced to 20mg daily with clozapine serum three weeks. The plasma concentration of citalopram was 19 increased by two to three folds due to selective inhibition levels of 792 ng/ml. In another case study, initiation of
44 treatment with citalopram in a man who was regularly of CYP3A4 and CYP2C19 enzymes by fluvoxamine.
taking resperidone, resperidone plasma levels were These reports suggest that the drugs that interact with 20 citalopram by inhibiting CYP450 enzymes from mild to elevated and resulted in idiopathic priapism. Similarly,
severe extent may produce excessive serotonergic citalopram increased the plasma concentrations of
reactions. These reactions may be life-threatening for trazodone up to 30% in depressive patients and produced 11 many patients but, sometimes, beneficial to non-serotonin syndrome. These reports suggest the
responsive depressive patients. Hence, psychiatrists pharmacodynamic changes due to pharmacokinetic
must be cautious and reduce the doses of index drug, if interaction with certain drugs.
needed, while prescribing such interacting drug In contrast, the bioavailability of selegiline was combinations. decreased by 30% in presence of citalopram in a study
12 In contrast, the dose of citalopram is required to be involving 18 healthy subjects. In another study,
increased in patients who are also prescribed with citalopram delayed the time to maximum alprazolam
CYP450 enzymes inducers such as carbamazepine and concentration by 30 minutes perhaps by affecting its 1 5 rifampicin. Carbamazepine and rifampicin potently a b s o r p t i o n . N e v e r t h e l e s s , t h e r e w a s n o
induces CYP3A4 isoenzyme involved in the metabolism pharmacodynamic change or therapeutic failure (N-demethylation) of citalopram. Carbamazepine was observed in such patients. These drug interactions were found to decrease (30%) the plasma levels of considered as clinically insignificant.
49 citalopram. Less therapeutic efficacy (increased crying The drugs that alter the activity of CYP3A4, CYP2D6 and panic attacks) of citalopram (40 to 60 mg daily) was and CYP2C19 enzymes involved in the metabolism of observed in a 55-year-old depressive man when citalopram can thus alter the plasma levels of citalopram. rifampicin (600 mg twice daily) was co-administered. Buspirone and alprazolam have increased the plasma The depressive condition improved when rifampicin concentrations of citalopram in depressive patients by
64administration was stopped. inhibiting CYP3A4 isoenzyme. In an isolated case,
Pharmacodynamically, citalopram interacts potentially buspirone and citalopram co-administration lead to 35,38 with many drugs from different therapeutic classes. serotonin syndrome and hyponatraemia. In another
Conversely, other drugs also interact with citalopram study, concomitant administration of citalopram with
through the same mechanism. Serotonin reuptake fluconazole produced serotonin syndrome of life
inhibiting property of citalopram is responsible for such threatening intensity. Because, fluconazole potently 65 interactions. Citalopram including other SSRIs increase inhibits CYP3A4 isoenzymes.
the risk of bleeding when administered with NSAIDS In a patient citalopram 10 mg daily for three years and oral anticoagulants by inhibiting serotonin levels and showed the symptoms of serotonin syndrome when
8,9 thus causing decreased platelet aggregation.started taking tramadol 50 mg daily for pain relief
Meperidine, fentanyl and other opioids weakly inhibit following a surgical operation. Tramadol inhibits 5 1 serotonin reuptake. Serotonin syndrome, visual CYP2D6 and CYP2C19 enzymes. Similarly,
hallucinations and decrease in the threshold of the levomepromazine increased the initial steady-state myoclonous were observed when the opioids were plasma levels of desmethylcitalopram (10 to 20%), the
.52, 53, 54, 55 concurrently administered with citalopramprimary metabolite of citalopram, by potently inhibiting
Appetite suppressants like sibutramine, dexfenfluramine CYP2D6 isoenzymes activity. The interaction was not 56 and fenfluramine have nonspecific serotonin agonistic considered as clinically significant. The serum levels of
activity that enhance the release of serotonin and also citalopram was found raised by 44% in eighteen patients
inhibit serotonin reuptake. These drugs produce who were taking combination of citalopram and tricyclic 60 serotonin syndrome when administered with antidepressants (example imipramine). Imipramine
32,33,34 citalopram. Patients who did not respond to reportedly inhibits CYP2C19 enzymes to a milder
61 citalopram alone responded well with lithium carbonate extent. Depressive patients who did not respond to 45,46
combination. It was related to hyperstimulation of the citalopram (40 mg/day) alone responded when
5-HT and 5-HT receptors by lithium in the fluvoxamine (50 to100 mg/day) co-administered for 1A 2A

7
48 interactions and reducing the time of hospitalization. The brainstem. Similarly, olanzapine and quitapine with
interaction capacity of citalopram was less compared to citalopram produced serotonin syndrome as a
consequence of increased brainstem and spinal cord 5- other SSRIs in concurrent treatment with some
HT receptor modulation occurring with 5-HT receptor antihypertensives, tricyclic antidepressants and 1A 2A
58,59 antipsychotics. The interaction consequences of antagonism. Fatal serotonergic effects were observed
citalopram are some time manageable and even some when citalopram was co-administered with monoamino
times it gives an outcome which is beneficial. But oxidase inhibitor moclobemide and chemotherapeutic
pharmacodynamic interactions cannot be managed as the agent linezolid due to activation of 5-HT receptor. 1A
40,41,42,62,63 consequences of it were very severe which may even
cause death. So close monitoring of the symptoms of These findings indicate that the outcome of
pharmacodynamic interaction was required and even it pharmacodynamic interactions of citalopram is clinically
wil l be bet ter i f these combinations with significant. The consequences of excessive serotonergic
pharmacodynamic interactions is avoided.effects may even produce death in the affected patients or
prolonged hospital stay. Long hospital stay due to ACKNOLWLEDMENT
adverse interaction consequences may increase The authors sincerely thank Dr. H.G. Shivakumar,
economic burden for the affected patients. To avoid such Principal, J.S.S. College of Pharmacy, Mysore, for his
adverse consequences awareness about patient's support and encouragement. Our gratitude also goes to
conditions, adverse interactions including their J.S.S. University, Mysore, for providing all the necessary
management is required. In addition, withdrawal of an facilities.offending drug may be necessary to resolve exaggerated REFERENCESseroninergic symptoms.
1. Karin H, Norio Y, Gunnel T, Jolanta W, Lars LG, Leif In spite of the adversities which are mentioned above, B. Metabolism of citalopram enantiomers in citalopram was found to be safest of its class. It was found CYP2C19/CYP2D6 phenotyped panels of healthy to be safe in the treatment of hypertension as it is a weaker Swedes. Br J Clin Pharmacol 2003;56:415-21.
15 inhibitor of CYP2C19. It was found to be a substitute for
2. Andre FJ, Connie S, Frank L. Citalopram. Human the treatment of paroxetine in tricyclic antidepressant
Psychopharmacology: Clinical and Experimental 27
toxicity. Citalopram did not affect the plasma levels of 2000;15(6):439–51.
antipsychotic olanzapine which was found in case of 3. Olesen Ole V, Linnet Kristian. Studies on the
22 fluoxetine, sertraline and paroxetine. Overall intensity
Stereoselective Metabolism of Citalopram by Human of pharmacokinetic interactions of citalopram is
Liver Microsomes and cDNA-Expressed minimum and which can be managed clinically. But, the
Cytochrome P450 Enzymes. Pharmacology pharmacodynamic interactions which were observed
1999;59:298-09.with drugs with serotonergic activity were found
4. Rochat, Amey B, Gillet M, Meyer M. Identification of sometimes fatal. So, it is necessary that close monitoring
three cytochrome P450 isozymes involved in N-of serotonin syndrome symptoms is required when these
demethylation. Pharmacogenetics.1997;7(1):1-10.drugs are co administered and it is better to avoid this
5. Skop BP, Brown TM. Potential vascular and bleeding combination. Citalopram is producing some interaction complications of treatment with selective serotonin on co administered with some drugs the outcome of reuptake inhibitors. Psychosomatics 1996;37:12-16.which is its increased therapeutic efficacy.
6. Brunton Laurence L, Lazo John S, Parker Keith L. CONCLUSIONGoodman & Gilman's: The Pharmacological Basis Of Citalopram has the potential to interact with many drugs
thTherapeutics. 11 ed. McGraw Hill; 2006. p.302.by pharmacokinetic and pharmacodynamic mechanisms.
7. Priskorn M, Sidhu JS, Larsen F, Davis JD, Khan AZ, Many drugs similarly interact with citalopram. The
Rolan PE. Investigation of multiple dose citalopram nature of these interactions may vary from mild to severe.
on the pharmacokinetics and pharmacodynamics of Close monitoring of these drug interactions
r a c e m i c w a r f a r i n . B r J C l i n consequences is required. This helps to avoid or manage
Pharmacol.1997;44:199–202.the citalopram implicated interactions in the affected
patients and thus reducing the cost associated with these 8. Borrás-Blasco J, Marco-Garbayo JL, Bosca-Sanleon
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

8
B, Navarro-Ruiz A. Probable interaction between 20.Borba CP, Henderson DC. Citalopram and clozapine:
citalopram and acenocoumarol. Ann Pharmacother. potential drug interaction. J Clin Psychiatry.
2002;36:345. 2000;61:301–2.
9. Maurer-Spurej E, Pittendreigh C, Solomons K. The 21.Freudenreich O. Exacerbation of idiopathic priapism
influence of selective serotonin reuptake inhibitors on with risperidone-citalopram combination. J Clin
human platelet serotonin. Thromb Haemost. Psychiatry. 2002;63:249–50.
2004;91(1):119-128. 22.Chiu C-C, Lu M-L, Huang M-C, Chen K-P. Heavy
10.Celexa (Citalopram hydrobromide). Forest smoking, reduced olanzapine levels, and treatment
Pharmaceuticals, Inc. US Prescribing information, effects. A case report. Ther Drug Monit
May 2007. 2004;26:579–81.
11.Prapotnik M, Waschgler R, König P, Moll W, Conca 23.Baettig D, Bondolfi G, Montaldi S, Amey M, A. Therapeutic drug monitoring of trazodone: Are Baumann P. Tricyclic antidepressant plasma levels there pharmacokinetic interactions involving after augmentation with citalopram: a case study. Eur citalopram and fluoxetine? Int J Clin Pharmacol J Clin Pharmacol. 1993;44:403–5.Ther.2004;42:120–4. 24.Gram LF, Hansen MG, Sindrup SH. Citalopram:
12.Laine K, Anttila M, Heinonen E. Lack of adverse interaction studies with levomepromazine, interactions between concomitantly administered imipramine and lithium. Ther Drug Monit. selegiline and citalopram. Clin Neuropharmacol. 1993;15:18–24.1997;20:419–33.
25.Haffen E, Vandel P, Broly F. Citalopram: an 13.Drug interactions between Celexa and metoprolol.. interaction study with clomipramine in a patient
Drugs.com [online] 2010 Feb [cited 2010 Feb 28]; [3 h e t e r o z y g o u s f o r C Y P 2 D 6 g e n o t y p e . screens]. Available from: URL:http://www.drugs. Pharmacopsychiatry 1999;32:232–4.com/drug-interactions/celexa-with-metoprolol-679-
26.Haffen E, Vandel P, Bonin B, Vandel S. Citalopram 335-1615-0.html.
pharmacokinetic interaction with clomipramine. 14. Karin Nyfort-Hansen. erhexiline toxicity related to
UDP-glucuronosyltransferase inhibition? A case citalopram use. Med J Aust 2002; 176 (11):560-61.
report. Therapie. 1999;54:768–70.15.Belpaire FM, Wijnant P, Temmerman A, Rasmussen
27.Ashton AK. Lack of desipramine toxicity with BB, Brøsen K. The oxidative metabolism of
citalopram. J Clin Psychiatry 2000;61: 144.metoprolol in human liver microsomes: inhibition by
28.Richards S, Umbreit JN, Fanucchi MP, Giblin J, the selective serotonin reuptake inhibitors. Eur J Clin
Khuri F. Selective serotonin reuptake inhibitor- Pharmacol 1998;54:261–4.
induced rhabdomyolysis associated with irinotecan. 16.Hall J, Naranjo CA, Sproule BA, Herrmann N.
South Med J. 2003;96: 1031–33.Pharmacokinetic and pharmacodynamic evaluation
29.FDA ALERT [07/2006]: Potentially Life-of the inhibition of alprazolam by citalopram and
Threatening Serotonin Syndrome with Combined Use f l u o x e t i n e . J C l i n P s y c h o p h a r m a c o l .
of SSRIs or SNRIs and Triptan Medications.2003;23:349–57.
30.Prod Info Axert(TM), 2001.17.Castberg I, Spigset O. Effects of comedication on the
31.US Food and Drug Administration, 2006.serum levels of aripiprazole: evidence from routine 32.Prod Info Meridia(R), 1997.t h e r a p e u t i c d r u g m o n i t o r i n g s e r v i c e .
33.Schenck CH, Mahowald MW. Potential hazard of Pharmacopsychiatry. 2007;40:107–10.
serotonin syndrome associated with dexfenfluramine 18.Taylor D, Ellison Z, Ementon Shaw L, Wickham H, hydrochloride (Redux). J Am Med Assoc. Murray R. Co-administration of citalopram and 1996;276(15):1220-1.clozapine: effect on plasma clozapine levels. Int Clin
34.Benazzi F. Organic hypomania secondary to Psychopharmacol. 1998;13:19–21.
sibutramine-citalopram interaction. J Clin Psychiatry. 19.Avenoso A, Facciolà G, Scordo MG. No effect of
2002;63:165.citalopram on plasma levels of clozapine, risperidone
and their active metabolites in patients with chronic 35.Spigset O, Adielsson G. Combined serotonin
schizophrenia. Clin Drug Invest. 1998;16:393–8. syndrome and hyponatraemia caused by a
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

9
citalopram–buspirone interaction. Int Clin 2007.
Psychopharmacol 1997;12:61–3. 48.Drug interactions between Celexa and metoprolol.
Drugs.com [online] 2010 Feb [cited 2010 Feb 28]; [3 36.Cipramil (Citalopram hydrobromide). Lundbeck Ltd.
s c r e e n s ] . Av a i l a b l e f r o m U R L : h t t p : / / UK Summary of product characteristics, January
www.drugs.com/drug-interactions/citalopram-with-2007.
lithium-679-0-1477-0.html 37.Celexa (Citalopram hydrobromide). Forest
49.Steinacher L, Vandel P, Zullino DF, Eap CB, Pharmaceuticals, Inc. US Prescribing information,
Brawand-Amey M, Baumann P. Carbamazepine May 2007.
augmentation in depressive patients non-responding 38.Leinonen E, Lepola U, Koponen H, Kinnunen I. The to citalopram: a pharmacokinetic and clinical pilot effect of age and concomitant treatment with other study. Eur Neuropsychopharmacol. 2002;12:255–60.psychoactive drugs on serum concentrations of
50.Leinonen E, Lepola U, Koponen H. Substituting citalopram measured with a nonenantioselective
carbamazepine with oxcarbazepine increases method. Ther Drug Monit. 1996;18:111–17.citalopram levels. A report on two cases. 39.Gumà M, Clemente F, Segura A, Costa J. Síndrome Pharmacopsychiatry. 1996;29: 156–8.serotoninérgico: moclobemida y citalopram. Med
51.Mahlberg R, Kunz D, Sasse J, Kirchheiner J. Clin (Barc). 1999;113:677–8.Serotonin syndrome with tramadol and citalopram. 40.Neuvonen PJ, Pohjola-Sintonen S, Tacke U, Vuori E. Am J Psychiatry. 2004;161:1129.Five fatal cases of serotonin syndrome after
52.Altman Evan M, Manos Gail H. Serotonin Syndrome moclobemide-citalopram or moclobemide-Associated With Citalopram and Meperidine. clomipramine overdoses. Lancet. 1993;342:1419.Psychosomatics 2007;48(4):361-62.41.Höjer J, Personne M, Skagius A-S, Hansson O.
53.Ailawadhi S, Sung KW, Carlson LA, Baer MR. Serotoninergt syndrom: flera allvarliga fall med Serotonin syndrome caused by interaction between denna ofta förbisedda diagnos. Lakartidningen. citalopram and fentanyl. Journal of Clinical 2002;99:2054–5, 2058–60.Pharmacy and Therapeutics 2007;32:199–202.
42.Dams R, Benijts THP, Lambert WE. A fatal case of 54.Gnanadesigan N, Espinoza RT, Smith R, Israel M, serotonin syndrome after combined moclobemide
Reuben DB. Interact ion of serotonergic ci talopram intoxication. J Anal Toxicol. antidepressants and opioid analgesics: is serotonin 2001;25:147–51.syndrome going undetected? J Am Med Dir Assoc.
43.Hiremagulur J, Keshavan Hrishi , Gurbani Nirmal K, 2005;6:265–9.Dandiya Prem C. Effect of citalopram (Lu 10-171) on
55.Spigset O, Hedenmalm K, Dahl ML, Wiholm BE, tranylcypromine and tryptophan-induced wet-dog shakes in rats. Psychopharmacology.1980;70:209-12. Dahlqvist R. Seizures and myoclonus associated with
44.Bondolfi G, Chautems C, Rochat B, Bertschy G, antidepressant treatment: assessment of potential risk Baumann P. Non-response to citalopram in depressive
factors, including CYP2D6 and CYP2C19 patients: pharmacokinetic and clinical consequences
polymorphisms, and treatment with CYP2D6 o f a f l u v o x a m i n e a u g m e n t a t i o n . inhibitors. Acta Psychiatr Scand. 1997;96:379–84.Psychopharmacology 1996;128:421–5.
45.Gram LF, Hansen MG, Sindrup SH. Citalopram: 56.Gram LF, Hansen MG, Sindrup SH. Citalopram:
interaction studies with levomepromazine, interaction studies with levomepromazine,
imipramine and lithium. Ther Drug Monit i m i p r a m i n e a n d l i t h i u m . T h e r D r u g
1993;15:18–24. Monit.1993;15:18–24.
46.Baumann, Pierre, Nil R. A double-blind, placebo- 57.Padala, Prasad R, Sadiq, Hasnain J, Padala, Kalpana.
controlled study of citalopram with and without Urinary obstruction with citalopram and aripiprazole
lithium in the treatment of therapy-resistant combination in an elderly patient. Journal of Clinical
depressive patients: a clinical, pharmacokinetic, and Psychopharmacology; December 2006;26 (6):667-
p h a r m a c o g e n e t i c i n v e s t i g a t i o n . J C l i n 68.
Psychopharmacol. 1996;16:307–14. 58.Haslett CD, Kumar S. Can olanzapine be implicated
47.Cipramil (Citalopram hydrobromide). Lundbeck Ltd. in causing serotonin syndrome? Psychiatry.Clin
UK Summary of product characteristics, January Neurosci. 2002;56:533–5.
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

59.Marlowe Karl, Schirgel Dorothea. Quetiapine and
citalopram: aetiological significance in serotonin
syndrome. NMJ;119:1237.
60.Leinonen E, Lepola U, Koponen H, Kinnunen I. The
effect of age and concomitant treatment with other
psychoactive drugs on serum concentrations of
citalopram measured with a nonenantioselective
method. Ther Drug Monit. 1996;18:111–17.
61.Shin JG, Park JY, Kim MJ, Shon JH, Yoon YR, Cha IJ,
et.al. Inhibitory effects of tricyclicantidepressants
(TCAs) on human cytochrome P450 enzymes in vitro:
mechanism of drug interaction between TCAs and
phenytoin. Drug Metab Dispos 2002;30:1102–07.
62.Tahir N. Serotonin syndrome as a consequence of
drug-resistant infections: an interaction between
linezolid and citalopram. J Am Med Dir Assoc.
2004;5:111–13.
63.Hendershot PE, Antal EJ, Welshman IR, Batts DH,
Hopkins NK. Linezolid: pharmacokinetic and
pharmacodynamic evaluation of co-administration
with pseudoephedrine HCl, phenylpropanolamine
HCl, and dextromethorphan HBr. Journal of Clinical
Pharmacology 2001;41:563–72.
64.Kukoyi O, Argo TR, Carnaham RM. Exacerbation of
panic disorder with rifampin therapy in a patient
r e c e i v i n g c i t a l o p r a m . P h a r m a c o t h e r a p y
2005;25:435–7.
65.Levin Tomer T, Cortes-Ladino Alberto, Mark Weiss,
M. Lia Palomba, Life-threatening serotonin toxicity
due to a citalopram-fluconazole drug interaction: case
reports and discussion. General Hospital Psychiatry
2008;30:372–77.
10
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

AbstractTo evaluate the prescription pattern in terms of essentiality and rationality and assessment of Hospital pharmacy
services utilization in tertiary care teaching rural hospital. A Prospective Observational Study was conducted. Total
100 patients attending various outpatient departments of Shree Krishna Hospital, a tertiary care teaching hospital
were interviewed at their exit from the hospital and necessary information was gathered. Average time taken for
interview with patient was 8.3 minutes with range of 7 to 10 minutes. All the prescriptions collected were analyzed for
different parameters. Total 350 drugs were prescribed and average number of drugs per prescription was 3.5. Out of
these 350 drugs, 60 (17.14%) were prescribed by generic name and the rest 290 (82.86%) were prescribed by brand
name. Only 18 (5.14%) drugs were not prescribed from hospital formulary. 264 (75.43%) drugs were dispensed from
the hospital pharmacy. On the basis of rationality score 53% prescriptions were rational, 30% semi rational and 17%
irrational. Average rationality score was 20.56. In a hospital, where hospital formulary is based on WHO Essential
medicine list, hundred percent utilization of hospital pharmacy services by doctors and patients would ensure
rational prescribing for the benefit of the patients. Key words: prescription, out-patient, WHO, formulary
11
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
2INTRODUCTION less attractive cost-effectiveness in a variety of settings .
Essential medicines are the drugs which satisfy health WHO Essential drug list helps in promotion of Rational care need of majority of population and they should be Drug Therapy. Rational drug therapy means right drug to available within the context of functioning health system the right patient in a right manner (dose, duration, at all time in adequate amount in appropriate dosage form frequency and route of administration) at affordable
1with assured quality and adequate information with cost . Our hospital is a rural based tertiary care teaching 1
affordable price . hospital and the Hospital Formulary is based on WHO The WHO essential core list presents a list of minimum Essential drug list. Establishing the hospital formulary medicine needs for a basic health care system, listing the based on essential medicine list is not enough, assessing
most efficacious, safe and cost-effective medicines for adherence of clinicians to the formulary is equally
priority conditions. Priority conditions are selected on important.
the basis of current and estimated future public health This study aims to check the compliance of doctors with
hospital formulary, evaluation of utilization of hospital relevance, and potential for safe and cost-effective 2 pharmacy services by doctors and patients, and treatment .
evaluation of rationality of prescribing.The WHO essential complementary list presents METHODOLOGYessential medicines for priority diseases, for which
A Prospective Observational Study was conducted in the specialized diagnostic or monitoring facilities, and/or
Shree Krishna Hospital during the month of Jan-Feb specialist medical care, and/or specialist training are
2009. The study was conducted under the aegis of needed. In case of doubt medicines may also be listed as
Pharmacy Committee as a measure of audit. Permission complementary on the basis of consistent higher costs or
from CEO was obtained prior to study. Ethics Committee
approval was also taken. Written informed consent was
taken from all participants after explaining detailed
APTI
Indian Journal of Pharmacy Practice Received on 20/03/2010
Accepted on 24/03/2010 © APTI All rights reserved
APTI ijopp
Evaluation of prescription pattern in terms of essentiality and
rationality and assessment of Hospital pharmacy services utilization
in tertiary care teaching rural hospital.
Shah AM *, Dhanani JV, Shah RB, Agrawal A, Gajjar BM
Department of Pharmacology, Pramukh Swami Medical College, Karamsad (Gujarat), PIN 388325
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /0
Accepted on / © APTI All rights reserved
ijopp

12
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
4methodology to them. Total 100 patients attending Health Association of India, 1996, updated in 2003) .
various outpatient departments of Shree Krishna Based on above mentioned criteria for analysis, net score
Hospital, a tertiary care teaching hospital were was calculated and each prescription was graded
interviewed at their exit from the hospital and necessary accordingly as mentioned below:
information was gathered. Average time taken for (a) 0 to 14 points- Irrationalinterview with patient was 8.3 minutes with range of 7 to (b) 15 to 24 points- Semi rational10 minutes. All the prescriptions collected were analyzed
(c) 25 to 30 points- Rational for following parameters.
RESULTS?Extent of utilization of hospital pharmacy services by
Total 100 prescriptions from various outpatient doctors and patients.
departments were collected. In these prescriptions, total ?Reasons in cases of non-utilization of hospital
350 drugs were prescribed. Average no. of drugs per pharmacy services.
prescription was 3.5. Department wise distribution of ?Prescription pattern in terms of essentiality and
these prescriptions and average no. of drugs prescribed rationality.
are shown in Table 1. Maximum number of drugs per ?Whether medicines prescribed from Hospital prescription (4.58) was in medicine and ENT
Formulary. departments while lowest number per prescription (2) ?Whether medicines prescribed by generic or brand was in dental, ophthalmology and superspeciality clinics.
names. Out of these 350 drugs only 60 (17.14%) were prescribed ?Appropriateness of drugs prescribed. by generic name and rest 290 (82.86%) were prescribed
For assessment of appropriateness of prescribing we by brand name. 3
have followed Phadke's criteria . According to this Out of 350 drugs prescribed, 332 (94.86%) drugs were criteria maximum 30 points score system was assigned as prescribed from hospital formulary and only 18 (5.14%) follows: drugs were not prescribed from hospital formulary. 264
?Main drugs – 20 points (75.43%) drugs were dispensed from the hospital
? Complementary drugs – 10 points pharmacy and rest 86 (24.57%) were not dispensed from
hospital pharmacy (figure 1). Total 38 patients had not Out of these total points, half the points for each of these
taken some or all of the medicines prescribed, from the two categories of the drugs were allocated for the
hospital pharmacy. We also tried to evaluate reasons for correctness of the type of drug chosen for the condition
not purchasing drugs from hospital pharmacy, as shown and half for the correctness of the dose given, including
in Table 2. route and frequency of administration and the duration of st nd
therapy. So for the 1 choice 100% points, 2 choice 60% On evaluating the prescriptions for appropriateness of rd prescribing 53% prescriptions were rational, 30% semi points & 3 choice 30% points were allocated. If more
rational and 17% irrational (figure 2). Average rationality than two drugs were needed to be given in a condition, the
score was 20.56. points allocated were subdivided accordingly.
Negative points were given for use of (a) irrational drug DISCUSSION
or irrational drug combination: -5; (b) unnecessary drug Rational prescribing is essential part of patient care.
or injection: -5; (c) hazardous or banned drug: -10. WHO has developed an essential drug list for promotion
These categories were defined as follows: of rational drug therapy. Hospitals should have a
formulary based on essential drug list. In our study we (a) Irrational drug or irrational drug combination: a drug
found that majority of prescriptions (94.86%) were from not recommended in the standard textbook of
hospital formulary which is based on WHO essential pharmacology or other established scientific
drug list.literature.
In our study average no. of drugs per prescription was 3.5 (b) Unnecessary drug or injection: a category of drug or
which is almost similar to 3.52 reported by a similar study formulation not recommended for that particular 5
condition in the standard textbooks. done by Ansari et al . One of the studies conducted
inTaiwan by Lai MS has reported average 4.3 drugs per (c) Hazardous or banned drug: drug listed under the 6
heading 'Banned and bannable drugs' (Voluntary prescription. Inappropriate polypharmacy and potential

13
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Table.1: Department wise distribution of prescriptions co llected
Sl.No. Name of department No. of prescriptions
Total No. of drugs prescribed
No. of drugs per prescription
1 Medicine 31 143 4.58 2 Surgery 15 43 2.86
3 Skin 14 64 4.57 4 Orthopedics 11 26 2.36
5 ENT 8 37 4.58 6 Obs & Gyn 6 13 2.16
7 Paediatrics 5 12 2.4 8 TB chest 4 17 4.25
9 Psychiatry 2 7 3.50 10 Dental 2 4 2
11 Ophthalmology 1 2 2 12 superspeciality 1 2 2
Total 100 350 3.5
Table.2: Reaso ns for not purchasing drugs from hospital pharmacy (n=38)
Sl. No. Reason No. of patients (%)
1 Drugs not available in pharmacy store 14 (36.84%)
2 Drugs already present at home 12 (31.57%)
3 Long queue 7 (18.42%)
4 Cheaper drugs/ brands available outside 4 (10.52%)
5 Free drugs available from drug bank/ samples/ other sources 3 (7.89%)
6 Advised by doctor to take from outside 1 (2.63%)
7 ADR with brand available in hospital pharmacy 1 (2.63%)

14
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
5drug therapeutic problems showed strong positive near to 59.2% reported in a study done by Ansari et al . In 7
our study 17% of prescriptions were irrational which is correlation with the number of drug per prescription . The
comparable to the nationwide multicentre study done by less no. of drugs per prescription carries less risk of
Krishnanangshu R et al which reported 4 to 26% of adverse drug reactions and drug interactions.8
prescriptions as irrational . In our study 17.14% of drugs were prescribed by generic
This type of study is helpful in assessing adherence of name and 82.86% by brand name. This suggests that
doctors to the hospital formulary as well as compliance of there is a need for encouragement for prescribing
both patients and doctors with the hospital pharmacy medicines by generic name, particularly in a hospital
services. Further it is also helpful in finding out the issues attached to medical college.
responsible for noncompliance to the hospital pharmacy In this study 94.86% of drugs were prescribed from services.hospital formulary and only 18 (5.14%) drugs were not
In conclusion, in a hospital, where hospital formulary is from hospital formulary. As our hospital formulary is
based on WHO Essential medicine list, hundred percent based on WHO essential medicine list, it has direct
utilization of hospital pharmacy services by doctors and impact on number of rational prescriptions. 86 drugs
patients would ensure rational prescribing for the benefit were not purchased from hospital pharmacy. Various of the patients. reasons were given by patients for not purchasing drugs REFERENCES
from the hospital pharmacy. Out of those, reasons like 1. Sharma HL, Sharma KK. Principles of pharmacology.
long queue, drugs out of stock and availability of cheaper st1 ed. Hyderabad: Paras medical publisher; 2007. p.
brands outside are the issues which can be taken care of 108-114
by the hospital authority for improving the compliance to 2. World Health Organization. WHO Model list of hospital pharmacy. Steps can be taken for improvement Essential Medicines. 15th list. (last cited 2008 Nov2). like keeping enough stock and increasing pharmacy Available from URL: http://www.who.int/ windows. medicines/publications/EML15.pdfIn our study 53% of prescriptions were rational, which is 3. Phadke A. Drug supply and use: Towards rational
Fig.2: Rationality score

15
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
stpolicy in India. 1 ed. New Delhi: Sage publications;
1998. p. 85-100.
4. Community Development Medicinal Unit
Documentation Centre. Banned and Bannable Drugs
thin India. 4 ed. (last cited 2008 dec 24). Available from
URL: http://www.cdmubengal.org/other_info/
Banned Drugs India.pdf
5. Ansari KU, Singh S, Pandey RC. Evaluation of
prescribing pattern for rational drug therapy. Ind J
Pharmacol; 1998: 30: 408-410.
6. Lai MS, Chu CS, Lin SH, Lin MS. Prescribing pattern
in primary health care in Taiwan. Int J Clin Pharmacol:
1995: 33: 437-441.
7. Muazu J , Ikunaiye NY , Abubakar A , Sadiq GU ,
Zarma SY and Umar YH. Assessment of Quality of
Out-patient Prescriptions in the National Health
Insurance Scheme Unit of a Tertiary Hospital in
Nigeria. Res J Pharm Biol Chem Sci;2010: 1(1): 557-
561.
8. Krishnangshu R, Ghosh JM, Chandhri SB, Mandal A,
Prasad S. Prescription audit analysis-A study of drug
prescription practices in India. Calcutta: Voluntary
Consumer Action Network (V-CAN), Consumer
Utility &Trust Society, 1996.

16
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
INTRODUCTION
Rational pharmacotherapy involves the appropriate use that prescription error is the most common type of
of medications for the patients to their clinical needs, in medication error and accounted for 20-40% of all
doses that meet their own individual requirements, for an medication error (Sangtawesin et al, 2003, Barker et al.,
adequate period of time and at the lowest cost to them and 2002).
their community (World Health Organization, 1987). A A study from United States of America (USA) suggested
medication error is defined as any preventable event that that around 44000 to 98000 hospitalized patients die due
may cause or lead to in appropriate use or patient harm to medication errors in USA every year and number of
while the medication is in the control of healthcare death due to medication error is increasing day by day.
professional, patient or consumer (Institute of Medicine, (Institute of Medicine, 2000 and Phillips et al., 1998).
2000). Pharmacotherapy is a complex process which Similarly in Australia 2-4% of all hospital admissions
requires the involvement of wide variety of healthcare and up to 30% for patients aging more than 75 years are
professional including doctor, pharmacist, nurses etc. It due to medication related out of which 75% are
is evident that error in the pharmacotherapy is quite potentially preventable (Runciman et al., 2003). Further,
common and can occurs at the any stage of medication a study conducted in the neighboring country, India in
process like prescribing, dispensing, administration and 304 patients in public hospital found that 34% patients
monitoring (Gandhi et al., 2005, Runciman et al., 2003). were having at least one medication error (Pote et al., Studies from Thailand and Georgia, and Colorado found 2007).
Nepal is a developing country with poor healthcare status
with a large number of drug use problem. Some of them
are irrational prescribing and dispensing, polypharmacy,
APTI
Indian Journal of Pharmacy Practice Received on 24/04/2010
Accepted on 30/04/2010 © APTI All rights reserved
APTI ijopp
Pattern of potential medication errors in a tertiary care hospital in Nepal.
1, 2, 3 1,2 1 1Kadir A , Subish P , Anil K , Ram B
1. Department of Hospital and Clinical Pharmacy, Manipal Teaching Hospital, Pokhara, Nepal; 2. Department of
Pharmacology, Manipal College of Medical Sciences, Pokhara, Nepal; 3. Department of Social and Administrative
Pharmacy, Faculty of Pharmaceutical Sciences, Chulalongkorn University, Bangkok, Thailand
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /0
Accepted on © APTI All rights reserved
ijopp
AbstractIn the process of treating a patient errors may occur at any stage of pharmacotherapy starting from the prescription
writing, dispensing, administration and monitoring. The present study was conducted to identify the potential
medication errors among the outpatients and to categorize them based on the onset, underlying cause, medication
error index and severity of medication error. A cross-sectional study was conducted in Manipal Teaching Hospital,
Pokhara, Nepal between July 2007 to October 2008. The prescriptions having medication error was photocopied
and used as the data source. The encountered medication errors were classified based on their onset, underlying
cause, medication error index and severity of medication errors. Altogether 66 medication errors were recorded in
59 prescriptions. Medication errors were noticed more in prescribed medication of male patients and with anti-rd
microbial class of drugs. All (100%; n=66) the errors had latent onset. More than 2/3 (68.18% n=45) of errors had rd
underlying cause as wrong dose. Similarly, more than 2/3 (72.73%; n=48) of errors were found to be medication
error index of 'Category B' which suggests an error occurred, but medication did not reach to the patients and the
degree of severity of most of the medication errors (69.70%; n=46) were 'B' on severity scale means clinically
significant error which can increase need for patient monitoring. Conclusively, the proper communication between
pharmacists and prescribers prevented majority of potential errors which is appreciable and should be continued. Key words: Medication Error, Nepal, Outpatients, Pharmacovigilance.
,
;

17
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
misuse of antibiotic, irrational drug promotion, adverse Western Nepal. It is 700 bedded multidisciplinary
drug reaction, drug interaction etc (Blum, 2000). hospital having clinical departments such as Medicine,
Moreover, status of hospital pharmacy is very poor and Surgery, Pediatric, Psychiatry, Orthopedic, Obstetrics
most of the hospital does not have their own hospital and gynecology, Ophthalmology, Dermatology,
pharmacy. In addition, there is lack of drug information Otorhinolaryngology and Dental. On an average 600
(DI) services in the most of hospital. Further more, there patients visit the hospital everyday. Outpatient pharmacy
is lack of package insert in the pharmaceutical is one of the units of Hospital and Clinical Pharmacy
Department situated at the ground floor of the hospital. preparation manufactured by Nepalese pharmaceutical
company which is supposed to be one of cheap source of Duration: The study was conducted during July 2007 to
DI in the developing country. This suggests the lack of October 2008.
vigilance to the medicine and high risk of medication Inclusion Criteria: Prescriptions having at least one
errors. To improve the vigilance, pharmacovigilance medication error were included in this study.
program was recently started to monitor the drug related Source of data: Photocopy of the prescriptions was the problem (Uppsala Report, 2007). Currently, there are five sources of data.regional pharmacovigilance centers in the country. Drug Operation modality: Pharmacists working in the Information and Pharmacovigilance Center in Manipal outpatient pharmacy department whenever encountered Teaching Hospital is one among them. The center is the error in the prescription, he/she photocopied the regional center for western region of Nepal. The center is prescription. Further the clarification with the prescriber located in Manipal Teaching Hospital which tertiary care was done before dispensing the prescription. After teaching hospital in Western Nepal. The hospital also has clarification the correction made by the prescriber was a drugs and therapeutics committee (DTC). The recorded in the backside of the photocopied prescription. committee has also taken several steps to ensure the safe The photocopied prescription is studied for the use of medicines (Palaian and Mishra, 2005). In the past, categorization of error in this study. Categorization of there were several initiatives taken to minimize the medication error was done based on published literatures medication error which include drug information (Jackson and Reines, 2003; Allan and Barker, 1990; services for healthcare providers, medication counseling Hartwig et al 1991 and Lustig, 2000).to the patients, continue pharmacy education to the Result analysis: The data obtained from the prescription hospital pharmacists, triplet billing system, batch were entered in the Microsoft excel spread sheet and dispensing, telephonic queries to prescribers, envelope analyzed.system for dispensing drugs, computer billing system,
Results: Altogether 59 prescriptions encountering separation of inpatients from outpatients, dispensing
medication error were photocopied. only with prescription, dispensing by qualified
Demography: The demography of the patients whose pharmacists and arrangements of medicine in pharmacy
prescription encountered potential medication error (Dubey et al., 2006). After such initiative there is need to
revealed that number patients were male (42.37%, n=25) know the pattern of medication error in the hospital.
as compared to female (28.81%, n=17), where as in Moreover, the study in this area is lacking in Nepal. The
28.81% (n=17) sex was not mentioned. The Age present study was conducted with the following
distribution of patients encountering potential mediation objectives:
error shows that more number of patients was in the age 1. To identify the potential medication errors among the
group 21-30 years (18.64%, n=11), followed by age outpatient prescriptions
group years 11-20 (13.56%, n=8), age group 41-50 years 2. To categorize the identified medication errors based on (10.17%, n=6), age group 31-40 years (8.47%, n=5), age their onset, underlying cause, medication error index and group 61-70 years (6.78%, n=4), age group 0-10 years severity of the medication errors. (3.39%, n=2), age group 51-60 years (1.69%, n=1) and Material and Methods age group >70 years (1.69%, n=1). However, in 35.59%
Study type: Cross-sectional Study (n=21) of prescription age of the patients were not
Study site: The study was conducted in the Outpatient mentioned. The department wise distribution of the
Pharmacy of Manipal Teaching Hospital. Manipal prescription encountering potential medication error is
Teaching Hospital is a tertiary care teaching hospital in given in Table 1.

18
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Table.1: Department distribution (n=59)
Department No. of prescription Percentage
Medicine 11 18.64 Surgery 10 16.95
Orthopedics 7 11.86 Pediatrics 7 11.86
Obstetrics and gynecology 5 8.47 Dermatology 4 6.78
Ophthalmo logy 3 5.08 Psychiatry 3 5.08
Dental 2 3.39 Otorhinolaryngology 2 3.39
Unknown 5 8.47
Categorization of medication errors: Altogether 169 recorded (n=66) was latent.
drugs were prescribed in 59 prescriptions encountering Categorization of medication error based on
66 medication errors. While classifying the medication underlying cause: The classification of medication error
error based on onset it was found that all the error based on underlying cause is shown in Table 2.
Table.2: Classification of medication error based on underlying cause (n=66)
Underlying cause No. of Error Percentage
Wrong dose error 45 68.18
Wrong T ime error 7 10.61 Extra dose error 6 9.09
Wrong dosage form error 3 4.55 Wrong dose preparation error 3 4.55
Wrong route of administration error 1 1.52 Others 1 1.52
Categorization of medication error based on medication error index: The classification based on medication error index is given in Figure 1.
Fig.1: Classification based on medication error index (n=66)
23%
72%
3%
2%
Category A
Category B
Category C
Category D

19
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Categorization of medication error based o n severity: The classification based on severity is given in Figure 2.
Fig.2: Classification based on Severity Index
9%
70%
21%
A
B
C
Classification of drugs involved in medication error: Similarly the classification of drugs which was involved in medication error is classified in Table 3.
Table.3: Class of drugs involved in medication erro r (n=66)
Class of drugs Number of drugs Percentage
Anti-microbial agents 27 40.91
Gastrointestinal agents 14 21.21
Drugs acting on central nervous system (CNS) 7 10.61
Non-steroidal anti-inflammato ry drugs 5 7.58
Anti-allergic drugs 4 6.06
Corticosteroids 2 3.03
Non-opiodal analgesics 2 3.03
Anticancer drugs 1 1.52
Drugs acting on cardiovascular system 1 1.52
Drugs acting on resp iratory system 1 1.52
Vitamins 1 1.52
Others 1 1.52

20
Table.3 : Site of Infection Diagnosed
Sl. No. SITE OF INFECTION % OF CASES n=482
1 Gastro-intestinal 26.86
2 Respiratory 22.39
3 Others 50.74
The prescriptions were also evaluated for their rationality antibiotics prescribed in each prescription. When
and irrationality. Based on the number of antibiotics prescriptions were evaluated based on the drug
prescribed in each prescription 71.64% prescriptions interaction 58.21% prescriptions were found to be
were found to be rational, the remaining of 28.36% rational and 41.79% prescriptions were irrational, the
prescriptions were found irrational with two or three data have been represented in Table-4.
Table.4: Rationality and Irrationality of Prescriptions
Sl. No. PATTERN RATIONAL
(%)
IRRATIONAL
(%)
1 Number of antibiotics prescribed 71.64 28.36
2 Drug interaction 58.21 41.79
DISCUSSION
The inappropriate utilization of antibiotics, especially in contradict to the previous observation it was found that
infants and children, forced many researchers to evaluate the most widely used antibiotics belong to class of
the consumption of this class of antimicrobial agent in quinolones and penicillins (Pn). Norfloxacin,
order to control the risk and its misuse. Studying the ciprofloxacin, ofloxacin and amoxicillin are found to be
antimicrobial prescribing pattern in an Indian tertiary most frequently used antibiotics in pediatrics. Resistance
against quinolones such as norfloxacin, ciprofloxacin, hospital has showed that two antimicrobials per
etc. develops quite slowly and hence they are widely prescription was maximum in pediatrics, while one 11
antimicrobial was maximum in surgery, urology and used .Amoxicillin is active against all organisms
internal medicine departments. Amikacin, ciprofloxacin, sensitive to Pn G, in addition it inhibits many gram
cefotaxime and cloxacillin were the most preferred negative bacilli, its oral absorption is better and is not 10 interfered by food along with this higher and more drugs . The result of present study demonstrates that
12 antibiotics are frequently used in infants and children. In sustained blood levels are produced . Amoxicillin with
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

21
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Steps taken to prevent the medication errors: Majority of times (89.39%, n=59) after encountering mediation error pharmacists clarified the errors with the prescribers. Whereas in few instances (7.58%, n=5) action taken after
encountering the medication error are not recorded. However, in one instances (1.52%, n=1) the drugs were wrongly dispensed by the pharmacists and in one instances (1.52%, n=1) correction was done after few doses.
Example of potential medication error: Some of the potential medication errors are described in Table 4.
Table.4: Example of potential medication error
Name of drugs
Medication errors
Secnidazole Tab Secnidazole was prescribed as 2 gm two tab HS single dose which after clarification
with prescriber it was dispensed as Tab Secnidazole 1 gm two tab HS. Cloxacillin Cap Cloxacillin was prescribed as 500 mg three times daily for 7 days which after
clarification with prescriber, it was dispensed as Cap Cloxacillin 500 mg four times daily for 7 days
Azithromycin Tab. Azithromycin was prescribed as 500 mg four times daily for 7 day which after clarification with prescriber, it was dispensed as Tab. Azithromycin 500 mg once daily for
7 days Tramadol Tab. Tramadol was prescribed as 500 mg whenever necessary which after clarification with
prescriber it was modified as Tab Tramadol 50 mg whenever necessary.
Ranitidine Tab. Ranitidine was prescribed as 40 mg daily 7 day which after consultation with prescriber it was modified as Tab. Ranitidine 150 mg twice daily for 7 days.
DISCUSSION
Altogether 66 medication errors were identified in 59 (Pote et al., 2007). This suggests that wrong dose and
prescriptions. The study found that all the medication wrong timing are the common underlying cause involved
error has latent onset. In most of the cases (68.18%) in medication error.
underlying cause for medication error was found to be We found that medication error was more with the anti-
wrong dose. Similarly, most of the medication errors microbial class of drugs (40.91%) followed by GI agents
were found to be medication error index of 'Category B' (21.21%), CNS agents (10.61%). This is because anti-
which suggests an error occurred, but medication did not microbial are the class of drugs used commonly in
reach to the patients. The degree of severity of most of the different specialties. A study conducted in India by Pote S
medication error was found to be 'B' on severity scale et al. also found anti-microbial class of drugs were more
means clinically significant error which can increase involved in medication error (Pote et al., 2007) and
need for patient monitoring. Medication error was found Similar result was found in study conducted in Israel
more with anti-microbial class of drugs. where anti-infective class of drugs were involved in
38.7% of medication error (Lustig A, 2000). It suggests There are several underlying cause involved in
that anti-microbial class of drugs need special focus.medication error which include wrong dosing interval,
wrong dose, wrong route, wrong drug, wrong dosage A study suggests that more than 75% of potential
form etc. We found that most promising underlying cause medication errors can be prevented (Runciman et al.,
for medication error was wrong dose (68.18%) followed 2003). In our study we found that more than two-third of
by wrong time (10.61%) and extra doses (9.09%). medication error (72.73%) were found to be medication
Similarly in a study conducted in 36 healthcare facilities error index of 'Category B' means an error occurred, but
in Georgia and Colorado found most frequent types of medication did not reach to the patients which is very
error were wrong time (43%), omission (30%), wrong good from the patients point of views followed by
dose (17%) (Barker et al., 2002). Whereas in another 22.73% of 'Category A' in medication error index which
study conducted in India found most common types were suggest circumstances or events that have the capacity to
drug interaction (68%) followed by incorrect interval cause error. Similarly in a study conducted in Thailand,
(12.1%) and incorrect dose [over and under dose] (9.6%) 76.71% of medication errors were prevented

(Sangtawesin et al, 2003). This suggests that reporting prevention initiatives in a teaching hospital in
medication error is not a fault finding process rather it is a Western Nepal. Pak. J. Pharm. Sci 2006;19(3):244-
preventing of its incidence. Hence, reporting of 51.
5. Gandhi TK, Weingart SN, Seger AC, Borus J, Poon medication error should be encouraged. rd EG. Outpatient prescribing errors and the impact of More than 2/3 of the Medication error found clinically
computerized prescribing. J. Gen. Intern. Med significant error which can increase need for patient
2005;20:837-41.monitoring. Similarly a study conducted in Israel found 6. Har twig SC, Dener SD, Schne ider PJ . that 11%, 16%, 34% and 80% of clinically significant
Severityindexed, incident report-based medication error occurs per day in Internal Medicine, Intensive Care, error-reporting program. Am. J. Hosp. Pharm Surgery and Hemato – Oncology Departments 1991;48:2611-6.respectively (Lustig A, 2000).
7. Institute of Medicine, committee on quality Several strategies have been recommended to prevent the
healthcare in America. To err is human: building a medication errors in the health care setting. Some of them
safer health system. Kohn LT, Corrigan JM, are computerized physician order, clinical pharmacist
Donaldson MS, editors. In: Report of the institute of monitoring order, improved communication between medicine 2000. Washington DC: National academy healthcare practitioners etc. In this study majority of time press; 2000.(89.39%) pharmacists clarify their doubt with the
8. Jackson MA, Reines WG. A systematic approach to prescribers to prevent the medication errors. Hence, it is
preventing medication errors. US Pharm evidence that proper communication between healthcare
2003;28(6):69-76.professionals can prevent the majority of potential errors.
9. Lustig A. Medication error prevention by CONCLUSION
pharmacists- an Israeli solution. Pharm World Sci Medication error in the healthcare setting is a common
2000;22(1): 21-5.phenomenon. Medication error is more common with 10.Phillips DP, Christenfeld N, Glynn LM. Increase in anti-microbial class of drugs and the most common US medication-error deaths between 1983 and 1993. underlying cause behind medication error is wrong dose. The Lancet 1998;351:643-44.Most of the errors are clinically significant and it can be
11. Palaian S, Mishra P. Role of drug and therapeutics prevented by working together in a healthcare team. We
committee towards drug safety: experiences from experienced that most of the medication error was mainly
wes tern Nepal . Kathmandu. Univ. Med due to poor prescription writing. Since, we prevent most
2005;3(9):79-80.of the potential medication errors through proper
12.Pote S, Tiwari P, D'cruz S. Medication prescribing communication with prescriber which is highly
errors in a public teaching hospital in India: a appreciable. But the matter should be discussed in DTC
prospective study. Pharm. Pract 2007;5(1):17-21.meeting to minimize the risks.13.Runciman WB, Roughead EE, Semple SJ, Adams RJ. ACKNOWLEDGEMENT
Adverse drug events and medication errors in Authors acknowledge Mr. Pradip Ojha, Hospital
Australia. Int. J. Qual. Health Care 2003;15(I):i49-Pharmacist, Manipal Teaching Hospital for his help i59.during data collection.
14.Sangtawesin V, Kanjanapattanakul W, Srisan P, REFERENCESNawasiri W, Ingchareonsunthorn P. Medication 1. Allan EL, Barker KN. Fundamentals of medication errors at Queen Sirikit National Institute of Child error research. Am. J. Hosp. Pharm 1990;47: 555-71.Health. J. Med. Assoc.Thai 2003;86(Suppl 3): S570-
2. Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal 5.RL. Medication errors observed in 36 health care
15.Uppsala Reports 2007. Nepal joins the programme. facilities. Arch. Intern. Med 2002;162:1897-903.36: 5-6. Available from: URL:<www.who-3. Blum NL. Drug Information Development-a case
study Nepal. Rational Pharmaceutical Management umc.org/graphics/10205.pdf
Project. United States Pharmacopeia 2000. 16.World Health Organization. The rational use of drugs: 4. Dubey AK, Palaian S, Shankar PR, Mishra P, Prabhu report of the conference of experts1987. Nairobi,
M. Introduction to medication errors and the error 1985 Nov 25
22
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

INTRODUCTION
In the last 2 decades, the treatment of psychosis has been is primarily based on a similar practice for treating adults.1–3
revolutionized by the widespread adoption of ATAs. The more acceptable side effect profile and the safety of
These agents, presently available in India include ATAs have broadened the indications for their use. ATAs
risperidone, olanzapine, quetiapine, and clozapine, have are being used increasingly to treat various nonpsychotic
fewer propensities to cause extrapyramidal side effects disorders, not only in adults but also in children and 8–14 and carry a significantly lower risk of tardive dyskinesia adolescents. As is often the case, controlled trials are
4than do typical agents. For adults, monitoring guidelines rare and are characterized by small sample sizes,
and established indications for the use of these diagnostically heterogeneous samples, retrospective
medications exist, but not for children, with some designs, short follow-up, and the lack of control 15–18exceptions. Some data exist to support the use of groups. Some data support short-term, sustained
19–24 25 26,27clozapine to treat refractory schizophrenia in patients efficacy in reducing aggression, tics, and mania. 5
aged under 18 years and to reduce aggression in this Other uses for ATAs, for example, as adjunctive 6 7
population ; the review by Kranzler and colleagues cites treatment for anxiety and depression, are only supported it as the drug of choice for this indication. Olanzapine has by data for adults. Unfortunately, these medications are been reported to provide good response in early-onset not without their shortcomings. Most studies of adults
schizophrenia. The adoption of ATA's as first-line drugs and children find weight gain to be a side effect of 28–31
ATAs. Although this is to some extent a class effect,
weight gain is generally more common and greater with 31
olanzapine and clozapine. Prior to treatment, adults
23
APTI
Indian Journal of Pharmacy Practice Received on 28/03/2010
Accepted on 31/03/2010 © APTI All rights reserved
APTI ijopp
Study of prescription practice for Antipsychotic drugs by
Psychiatrists- A Survey1 2 3
Mukesh Ratnaparakhi* Guru Prasad Mohanta , Lokesh Upadayay
1. Marathwada Mitra Mandal's College of Pharmacy, Thergaon, Pune- 411033, India; 2. Annamalai University,
Annamalai Nagar - 608 002, India; 3. CARISM, Sastra University, Tanjavur -613 402, India.
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /
Accepted on / © APTI All rights reserved
AbstractThis study was revealed with prescribing patterns of antipsychotic and monitoring practices of psychiatrists in Pune
region. We were surveyed 100 psychiatrists in Pune region out of that 50 gave a positive response. This survey
includes the study of antipsychotic types prescribed its frequency, the age of the patients and the diagnosis of patients
for whom they prescribed these medications. We were prepared a questionnaires format and were distributed to
various psychiatrists in the form of hard copy within the Pune region. Questionnaires formats were collected after
fulfillment by psychiatrics in the form of hard copy. In that 88 % of psychiatrics prescribed ATAs, most commonly
(67 %). Patients diagnosis was include psychotic, mood, anxiety, externalizing, and pervasive
developmental disorders. Symptoms persist in patients were aggression, low frustration tolerance, and affect
dysregulation was also common. Percent of all prescriptions were for years. Most clinicians monitored patients, but
there were wide variations in the type and frequency of tests performed. Our study reveals that there exists
considerable variation in patterns of prescribing psychotropic medications and a significant increase in the number
of patients suffering from psychiatric illnesses seeking treatment. Prescribing patterns vary due to differences in
diagnosis, the discomfort that some psychiatrists feel toward prescribing, differing levels of awareness and
recognition due to cultural variances, the perceived negative stigma of mental illness, and insufficient education
regarding the etiology and management of psychiatric disorders.
Key words: Anti-psychotic drugs, prescribing pattern, mental illness
risperidone
ijopp
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

24
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
with psychosis have a higher risk of glucose intolerance hard copy within the Pune region. Questionnaires were
than do control subjects without psychosis; these collected from the psychiatrics after their fulfillment as a 32,33 hard copy. medications increase that risk. Medications such as
olanzapine and clozapine, which cause more weight gain Analysis
in adults, are generally more likely to disturb glucose Student t test was used to compare differences in
metabolism, but this change has been found with use of categorical outcome variables. Instat software was used
all these medications in adult populations to differing for analysis.
extents. Finally, undesirable effects on lipid metabolism RESULT33–35
have also been identified in adults. Weight gain with The survey of antipsychotic agent prescribing by ATA use is by no means universal or inevitable. psychiatrists was conducted in a 100 psychiatrists out of Awareness of this side effect, warning patients about it, them 50 gave a positive response. The survey was and early intervention with diet and exercise have been conducted on questionnaire basis. Questionnaire formats
36advised. The use of ATAs in treating psychotic disorder was given to psychiatrics and collected in the form of has been increasing exponentially, raising concerns as to hard copy. The survey was conducted from August to
37the appropriateness of this practice. , Evidence-based January on a weekly basis. Some of the questions were guidelines on frequency and type of monitoring do not found to be ineligible due to misinterpretation.exist. To better appreciate current practices, we surveyed Respondents were asked, which dosage forms you psychiatric to quantify their prescribing of this class of generally preferred. The most commonly used dosage medications, the disorders and symptoms being treated, forms are injectables, depot injections, oral dosage and the type and frequency of monitoring being used forms, liquid preparations out of which 34% were currently. With respect to this in present study we had injectables, 58% of oral dosage forms, 2% of liquid surveyed the psychiatrists to study the use of atypical preparations and 6% of depot injections were generally antipsychotic, their patient compliance to different preferred by psychiatrists. The various types of formulations. psychiatric patients were visited to hospital as, Neurosis, METHOD depression, mood disorders, anxiety, bipolar disorders,
We surveyed child and adolescent psychiatrists, and schizophrenia. Out of which 61% of the patients
developmental pediatricians after obtaining approval suffered from schizophrenia 9% of the patients suffered
from their professional organizations. from depression, 1 % of the patients suffered from
Questionnaire neurosis, 13 % from anxiety and 7% from mood
We developed a questionnaire asking whether the disorders. Regarding long acting dosage form only 10%
physicians prescribed these medications, for which of psychiatrist prefers long acting preparations and in
indications, and in which age groups. Questionnaires contrast to that 80% of the psychiatrists think that mouth
format were given to various psychiatrics in the form of dissolving tablet is the best option for psychotic patients
Fig.1: Percentage of Prescribers by Age of Patients
Percentage of Prescribers by Age of Patients
0%
5%
10%
15%
20%
25%
30%
35%
40%
20-30 30-40 40-50 50-60
Age in years
Pre
cen
tage

25
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Table.1: Percentage of prescribers by medication
Medication Percentage
Risperidone 67
Olanzapine 23 Quetiapine 24
Clozapine 0.5
Table.2: Percentage of prescribers by indication
Indication Percentage
Schizophrenia 79
Bipolar mood disorder 80 Depression 28
Tourette syndrome 72 Eating disorder 24
Obsessive–compulsive disorder 53 Posttraumatic stress disorder 33
Other anxiety disorders 29 Pervasive developmental disorder 88
Mental retardation 48 Attention-deficit hyperactivity disorder 51
Oppositional defiant disorder 51 Conduct disorder 59
Impulsivity 65 Poor frustration tolerance 73
Affective dysregulation 83 Insomnia 33
as a drug delivery medium. 30 % of patients have age proportion of these prescriptions are given to children
more than 50 year. 79% the psychiatrists answered that aged under the age of 9 years. These medications are
they use tranquilizers before giving anti- psychotic currently being used off-label without clear guidelines
agents while 21% answered that they are not used for indications, dosing, and monitoring. Subjects report
tranquilizers before giving anti- psychotic agents. The that they monitor patients extensively and frequently, but
most commonly used methods for reducing catatonia in the practices are not uniform. This situation may be due to
patients were ECT, Anti-psychotic agents and exercise lack of data and guidelines.
show that 60% use of ECT, 25% use of antipsychotic A 43.9% rate of AIMS testing is impressive; however,
agents, 14% use of benzodiazepines and 1% exercise this means that 56.1% of patients under the age of 18
helped in reducing catatonia as reported by the years who are being prescribed this medication are not
psychiatrists. 79% the psychiatrists answered that they being monitored in this way. Further, there are significant
use tranquilizers before giving anti- psychotic agents discrepancies in the timing of follow-up (3 months, 6
while 21% answered that they are not used tranquilizers months, or 12 months.) Although these survey results do
before giving anti-psychotic agents. The drug abuse was not establish the total number of patients being treated
found to be 30% and drug dependence 70% as reported with ATAs, they do establish that the prescribing of ATAs
by the psychiatrists. by psychiatrics in Pune India is ubiquitous. There is an
DISCUSSION urgent need for more data regarding safety. reports
These data suggest a high rate of prescribing ATAs for suggests that most of the doctors found long acting
various indications and symptoms. A significant preparations and oral dosage forms more compatible as

26
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
compared to injectables and liquid dosage forms. Can J Psychiatry. 2003;48(2 Suppl 1):3S–12S.
CONCLUSION 6. Kumra S, Frazier JR, Jacobsen LK. Childhood-onset
schizophrenia. A double-blind clozapine-This study reveals that there has been a significant
haloperidol comparison. Arch Gen Psychiatry increase in the number of patients suffering from
psychiatric illnesses seeking treatment, which has 1996;53(12):1090 –97.
precipitated an increase in the number of prescriptions 7. Kranzler H, Roofeh D, Gerbino-Rosen G.
written by psychiatrists for antipsychotic agents. Clozapine: its impact on aggressive behaviour
However, there exists considerable variation in patterns among children and adolescents with schizophrenia.
of prescribing psychotropic medications, as well as a J Am Acad Chi ld Adolesc Psychia t ry. general lack of concordance between diagnosis and 2005;44(1):55–63.psychotropic medications prescribed in the medical field 8. Kranzler HN, Kestor HM, Gerbino-Rosen G. as a whole. Prescribing patterns vary due to differences in Treatment-refractory schizophrenia in children and diagnosis, the discomfort that some psychiatrists feel adolescents: an update on clozapine and other toward prescribing, differing levels of awareness and pharmacological interventions. Child Adolesc recognition due to cultural variances, the perceived
Psychiatr Clin N Am 2006;15(1):135–159.negative stigma of mental illness, and insufficient
9. Aman MG, De Smedt G, Derivan A. Double-blind, education regarding the etiology and management of
placebo-controlled study of risperidone for the psychiatric disorders.
treatment of disruptive behaviors in children with These variations are particularly evident in the
subaverage intelligence. Am J Psychiatry. prescribing trends of primary care physicians with
2002;159(8):1337–46.antipsychotic medications. In order to have a positive
10. Hanna GL, Fluent TE, Fischer DJ. Separation impact on patient populations, it is important for
anxiety in children and adolescents treated with psychiatrist to make use of various newly introduced
risperidone. J Child Adolesc Psychopharmacol medications to manage the spectrum of these disorders
1999;9(4):277–83.that are so frequently appearing in their practices.
11. Muller-Vahl KR. The treatment of Tourette's ACKNOWLEDGEMENT
syndrome: current opinions. Expert Opinion The authors are thankful to Dr. M. J. Patil Principal
Pharmacotherapy 2002;3(7):899–14.Marathwada Mitra Mandals College of Pharmacy for
12. Wozniak J, Biederman J, Richards JA. Diagnostic providing the necessary support. and therapeutic dilemmas in the management of
REFERENCESpediatric onset bipolar disorder. J Clin Psychiatry.
1. Lambert M, Conus P, Lambert T. Pharmacotherapy of 2001;62(Suppl 14):10–15.
first-episode psychosis. Expert Opin Pharmacother. 13. Frazier JA, Meyer MC, Biederman J. Risperidone 2003;4(5):717–50.
treatment for juvenile bipolar disorders: a 2. Pappadopulos E, Macintyre Ii JC, Crismon ML.
retrospective chart review. J Am Acad Child Adolesc Treatment recommendations for the use of Psychiatry. 1999;38(8):960–65.antipsychotics for aggressive youth (TRAAY) Part
14. Steele M, Fisman S. Bipolar disorder in children and II. J Am Acad Child Adolesc Psychiatry. adolescents: current challenges. Can J Psychiatry. 2003;42(2):145–61.1997;42(6):632–36.3. Curran S, Harris L, Macdonald A. Antipsychotics in
15. Fava M. Psychopharmacologic treatment of clinical practice: guidelines for safe and effective
pathological aggression. Psychiatr Clin North Am. use. Hum Psychopharmacol. 2002;17(2):75–82.
1997;20(2):427–51.4. Varghese Sunny T. Antipsychotic drug prescription
16. Saito E, Kafantaris V. Can diabetes mellitus be in postgraduate psychiatry training programs in
induced by medication? J Child Adolesc India: Time to reflect. Ind J Psychiatry
Psychopharmacol. 2002;12(3):231–6. 2007;49(3):225.
17. Domon SE, Webber JC. Hyperglycemia and 5. Lalonde P. Evaluating antipsychotic medications:
predictors of clinical effectiveness. Report of an hypertriglyceridemia secondary to olanzepine. J
expert review panel on efficacy and effectiveness. C h i l d A d o l e s c P s y c h o p h a r m a c o l .

27
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
2001;11(3):285–88. 28. Delbello MP, Kowatch RA, Adler CM, et al. A
double-blind randomized study comparing 18. Nguyen M, Murphy T. Olanzepine and
quetiapine and divalproex for adolescent mania. J hypertriglyceridemia. J Am Acad Child Adolesc
Psychiatry. 2001;40(2):133. A m A c a d C h i l d A d o l e s c P s y c h i a t r y.
2006;45(3):305–13.19. Martin A, L'Ecuyer S. Triglyceride, cholesterol and
weight changes among risperidone-treated youths. A 29. Addington J, Mansley C, Addington D. Weight gain
retrospective study. Eur Child Adolesc Psychiatry. in first-episode psychosis. Can J Psychiatry.
2002;11(3):129–33. 2003;48(4):272–76.
20. Reyes M, Olah R, Csaba K. Long-term safety and 30. Allison DB, Casey DE. Anti-psychotic-induced
efficacy of risperidone in children with disruptive weight gain: a review of the literature. J Clin
behaviour disorders. Results of a 2-year extension Psychiatry. 2001;62(Suppl 17):22–31.s t u d y. E u r C h i l d A d o l e s c P s y c h i a t r y. 31. Theisen FM, Linden A, Geller F. Prevalence of 2006;15(2):97–104. obesity in adolescent and young adult patients with
21. Aman MG. Management of hyperactivity and other and without schizophrenia and in relationship to acting-out problems in patients with autism antipsychotic medication. J Psychiatr Res. spectrum disorder. Semin Pediatr Neurol. 2001;35(6):339–45.2004;11(3):225–28.
32. Survey of Atypical Antipsychotic Prescribing by 22. Findling RL, McNamara NK, Branicky LA. A
Canadian Child Psychiatrists and Developmental double-blind pilot study of risperidone in the
Pediatricians for Patients Aged Under 18 Years The treatment of conduct disorder. J Am Acad Child
C a n a d i a n J o u r n a l o f P s y c h i a t r y 2 0 0 7 Adolesc Psychiatry. 2000;39(4):509–16.
June;52(6):367.23. Shea S, Turgay A, Carroll A. Risperidone in the
33. Wirshing DA, Wirshing WC, Kysar L. Novel treatment of disruptive behavioral symptoms in
antipsychotics: comparison of weight gain liabilities. children with autistic and other pervasive
J Clin Psychiatry. 1999;60(6):358–63. d e v e l o p m e n t a l d i s o r d e r s . P e d i a t r i c s .
34. Meyer JM. A retrospective comparison of weight, 2004;114(5):634–41.
lipid, and glucose changes between risperidone- and 24. Troost PW, Lahuis BE, Steenhuis MP. Long-term
olanzapine-treated inpatients: metabolic outcomes effects of risperidone in children with autism
after 1 year. J Clin Psychiatry. 2002;63(5):425–33.spectrum disorders: a placebo discontinuation study.
35. Lund BC, Perry PJ, Brooks JM. Clozapine use in J Am Acad Chi ld Adolesc Psychia t ry. patients with schizophrenia and the risk of diabetes, 2005;44(11):1137–44. hyperlipidemia, and hypertension: a claims-based 25. McCracken JT, McGough J, Shah B. Risperidone in approach. Arch Gen Psychiatry. 2001;58(12): children with autism and serious behavioral 1172–76.problems. N Engl J Med. 2002;347(5):314–21.
36. Meyer JM. Novel antipsychotics and severe 26. Scahill L, Leckman JF, Schultz RT. A placebo-
hyperlipidemia. J Clin Psychopharmacol. controlled trial of risperidone in Tourette's
2001;21(4):369–74.syndrome. Neurology. 2003;60(7):1130–35.
37. Koro CE, Fedder DO, L'Italien GJ. An assessment of 27. Delbello MP, Schwiers ML, Rosenberg HL. A
the independent effects of olanzapine and risperidone double-blind, randomized, placebo-controlled study
exposure on the risk of hyperlipidemia in of quetiapine as adjunctive treatment for adolescent
schizophrenic patients. Arch Gen Psychiatry. mania. J Am Acad Child Adolesc Psychiatry.
2002;41(10):1216–23. 2002;59(11):1021–26.

28
INTRODUCTION
Malaria is one of the most common infectious diseases Ninety percent of malaria-related deaths occur in Sub-
and an enormous public health problem. Malaria has Saharan Africa. Malaria is commonly associated with 5infected humans for over 50,000 years, and has been a poverty, but is also a cause of poverty . As per WHO latest
1human pathogen for the entire history of the species . estimation, there are 300-500 million cases globally and
Each year, there are approximately 350–500 million 1.5- 2.7 million deaths occur due to malaria each year, 2
cases of malaria , killing between one and three million 90% of which are in Africa. In India, The National
people, the majority of whom are young children in Sub- Malaria Eradication Programme (NMEP) was started in 3 1958 and achieved near complete disappearance of Saharan Africa .There are sixty three species of
6mosquitoes still today reported worldwide. Among them, disease in 1960s . In 1995, NMEP has reported 2.3
four species are very active in India, namely, million proven cases out of which 0.8 million were by
Plasmodium falciparum (pf), Plasmodium vivax (pv), Plasmodium falciparum and there were 1012 deaths.
Plasmodium ovale(po) and Plasmodium culex (pc). The However, the actual incidence of malaria in India is 7parasites multiply within red blood cells, causing estimated to be between 15-35 million cases per year .
symptoms that include anemia (light-headedness, For diagnosis of malarial parasites, direct microscopy of shortness of breath, tachycardia, etc.), as well as other peripheral smear is widely used. Other processes general symptoms such as fever, chills, nausea, flu-like involved dip stick/ Quantitative Buffy coat technique illness, and, in severe cases, coma, and death. Malaria (QBC).To study the epidemiological distribution of transmission can be reduced by preventing mosquito falciparum with its positive rate, Hbgm% label is used as
8bites with mosquito nets and insect repellents, or by a parameter . Based on direct microscopy of peripheral mosquito control measures such as spraying insecticides blood smear, 7,490 patients having history of fever were inside houses and draining standing water where registered in outpatient department of Agartala
4mosquitoes lay their eggs . Government Medical college hospital (G. B. Pant
hospital) during March 2003 - 2005. Blood was collected
aseptically in EDTA vial, smear was prepared of all 7,490
registered cases and leishman stain was done.
APTI
Indian Journal of Pharmacy Practice Received on 03/05/2010
Accepted on 11/05/2010 © APTI All rights reserved
APTI ijopp
A retrospective review on Malaria and Antimalarial drugs in Tripura, India – A Survey Report
1 1 1Mallik Santanu* , Kumar Nilesh , Gautam Rajesh
1 Department of Pharmacy, Lovely Professional University, Phagwara, Punjab-144402
2Regional Institute of Pharmaceutical Science and Technology, Abhoynagar, Agartala, Tripura-799105
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /
Accepted on / © APTI All rights reserved
AbstractThis study reveals the status of disease malaria in Indian hilly areas with respect to availability of drugs and to
identify the common causative parasites of malaria. The work was carried out in urban and rural areas of Tripura. In
both cases 500 indoor patients' bed tickets were surveyed to find out the causative parasite, recovery period,
antimalarial drug used and again to compare the facilities, diagnostic procedure and clinical status. In this study it
was observed that the clinical pharmacy strategies were not well maintained in hospitals of both the areas but the
disease was well handled in semi rural areas. The self medication, magic remedies /mantras are still in practice
among rural peoples .In this survey it was observed that; in primary cases of malaria, patient recovered within 5-7
days; whereas in severe cases it took 25-30 days, if proper medication is provided. But 25% of patients come to
hospital only when disease is in chronic situation. In both the places two types of parasites were mainly found -
Plasmodium falciparum & Plasmodium vivax .In acute cases of malaria, chloroquine group of drugs were widely
prescribed and in normal cases the proguanil group was the choice of drug by the physicians. Key words: Malaria, Anti-malarial drugs, Malaria parasite, Plasmodium
ijopp
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

Hemoglobin estimations were done by acid hematin Total 500 nos. of bed tickets of both male medical ward 1
method for all 36 positive cases in the department of and 2, female medical ward 1 and 2 were studied.
clinical microbiology. Out of 7,490 smears 36 were Approval of Study
positive. Among the 36 positive patients, males were The approval of the study was forwarded to the hospitals more than females with 66.66% and 33.33% respectively. by the Head of the Institution and procured on 18.11.2005 Smear showed Plasmodium falciparm positive rate in as per NO. F. 11(33)-RIPSAT/DEG/2003-2004/5225-27.86.11%, others vivax in 8.33% and gametocyte in Materials included in the study5.55%. Hemoglobin pattern was markedly decreased
All the bed tickets were thoroughly checked and the below 8% in 66.66% and below 10% and above 8% in
following information was documented. Patients name, 36.11% cases only. Mostly were treated at home and
age, sex, BP and pulse, date of admission, date of 9
detailed drug history was not known . discharge, symptoms, primary medication, diagnosis, In Tripura Anopheles dirus & minimus, Culex species post medication, duration of treatment and treatment were also seen. In order to improve detection of result. In diagnosis, the blood testing methods (smear hemoparasites, QBC Assay was introduced in Tripura in test/QBC technique), were also documented with its private laboratory since July, 2000. During these 5 year identified malarial parasite.period, total no of 6449 blood samples were examined by
Planning and Procedure followed for the studyQBC Assay. Samples were received from patients with
The study was planned in such a way that, for each City pyrexia of acute onset as well as PUO patients. QBC
hospital, three weeks and for each rural hospital one and capillaries processed as per standard protocol. Giemsa
half week scheduled. All the prescriptions were stain was done in thin smear for confirmation of species.
fragmented into two groups according to the gender. Out of 6449 samples, 1349 (21%) were positive for
Further among those prescriptions selection was made malaria. Among them, 1072 (79%) P.falciparum 197
based on how many of them were malarial parasite (15%) P.vivax, 80 (6%) mixed infection. Surprisingly, in
positive and if positive, then what type of malaria parasite 4 patients Microfilaria was detected where clinical
it was. The first line and follow up medication provided suspision was for malaria though not in indigenous
by the doctors were recorded systematically. The drugs people. This was first time in Tripura Microfilaria could
prescribed were categorized according to their generic be detected from day time samples because of using
class. Finally, the ratio of mortality due to malaria was sensitive diagnostic tool. Incidence of malaria in Tripura
calculated.9, 10is quite high, P.falciparum is the predominant species .
RESULTS AND DISCUSSIONSA number of anti malarial drugs are prescribed by the
During the study period 500 nos. of bed tickets of fever doctors globally, like Chloroquine, Quinine and
reported prescription were observed and among them mefloquine, Primaquine, Antifols and Quinghaosu
328 nos. (65.6%) had positive parasitic test. There were (Artemisinine)
237 (72.25%) male patient and 91(27.74%) female MATERIALS AND METHODS
patients admitted. Out of 328(Fig.1), 271 (82.62%) were Study site
Plasmodium falciparum, 37 (11.28%) were Plasmodium The study was conducted in five different hospitals,
vivax, 13 (6.09%) were Plasmodium culex positive cases situated in three different locations, one is Agartala Govt,
(Fig.2). Among the 328 patients, 191 (58.47%) were Medical College and G.B.P. Hospital, Indira Gandhi
from urban hospitals and 137 (41.53%) were from rural Memorial Hospital, B.R. Ambedkar Teaching Hospital,
hospitals. In case of medication, a generalized rule was Agartala; Tripura Sundari Hospital, Udaipur; Santir
followed, whenever a patient (adult) was admitted with Bazar Public Health Center, Santir Bazar, South Tripura
fever, Quinine di HCl with 5% Dextrose I.V. was were selected.
administered at every 8 hrs. Paracetamol was given orally Study Period twice daily. In management of positive malarial patients, The study was carried out for the period of three months orally, first line medication, Primaquines were preferred from November 2005 to January 2006. mostly with sulfadoxines or quinines as a follow up Study Design medication (62%) and in case of I.V. medication, á, â-
Retrospective- Observational study. Arteether or â- Arteether were drug of choice as a first
Selection of Prescriptions (Bed Tickets) line dosing, followed by quinine or chloroquine
29
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

phosphate injection (31%). For critical cases, Artisunate local market and the same were prescribed, Chloroquine
injection was given intramuscularly (7%). About five (35%), Antifols (26%), Primaquine (17%), Quinine and
categories of anti malarial drugs were available in the mefloquine (13%) and Quinghaosu (9%).
Male
72%
Female
28%
Frequency of malaria attack according to gender
Quinghaosu
Antifols
Primaquine
Quinine and Mefloquine
Chloroquine
9%
26%
17%
13%
35%
Percentage frequency of prescribed antimalarial
drugs
Fig.1: Frequency of Malaria attack according to gender
Fig.2: Percentage frequency of prescribed antimalarial drugs
30
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

83%
11%
6%
0% 20% 40% 60% 80% 100%
PV
PF
PC
Ratio of Malarial Parasites found in bed tickets
Intravenous
36%
Oral
64%
Choice of dosage form as per bed tickets
Fig.3: Ratio of Malarial Parasites found in bed tickets
Fig.4: Choice of dosage form as per bed tickets
31
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

Rural
42%Urban
58%
Ratio of Malaria attack on urban and rural area
Winter
Season
23%
Rainy
Season
77%
Frequency of attack- Seasonwise
Fig.5: Ratio of Malaria attack on urban and rural area
Fig.6: Frequency of attack-Seasonwise
32
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

CONCLUSION
From the above study, it was concluded that the overview. Trends Parasetol 2001, 17:507-509
frequency of malarial attack by species Plasmodium 11)Basco LK, Ramiliarisoa O, Le Bras J: Invitro activity
falciparum was maximum. The frequency of malaria of pyrimethamine, cycloguanil and other antimalerial
attack is much more in urban area due to stack water of drugs against African isolates and clones of
the drains and also a huge number of malarial patients Plasmodium falciparum.Arn J Trop Med Hyg 1994,
were admitted to the hospitals during the rainy season. 50:193-199
The doctors prescribed the medications for malaria
depending on various factors like types of malaria
parasites, severity of parasite attack, patient age and most
obviously they look the economical soundness of the
patients. Drugs were given mainly through oral route
rather the intravenous. Beside all these things, a bi-month
health camp was organized by the health department in
the rural areas to create the awareness among the rural
population about the disease and how they can safeguard
themselves.
REFERENCES
1) Joy D, Feng X, Mu J, et.al. "Early origin and recent
expansion of Plasmodium falciparum". Science
2003; 300(5617):318–321.
2) Malaria Facts. Centers for Disease Control and
Prevention.
3) Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI.
"The global distribution of clinical episodes of
Plasmodium falciparum malaria". Nature 2005;434
4) Yoshida S, Shimada Y, Kondoh D, et al (2007).
"Hemolytic C-type lectin CEL-III from sea cucumber
expressed in transgenic mosquitoes impairs malaria
parasite development". PLoS Pathog. 3 (12): e192.
doi:10.1371/journal.ppat.0030192. PMID 18159942.
http://www.plospathogens.org/article/info:doi/10.13
71/journal.ppat.0030192.
5) "Malaria: Disease Impacts and Long-Run Income
Differences" (PDF). Institute for the Study of Labor.
http://ftp.iza.org/dp2997.pdf. Retrieved on 2008-12-
10(7030): 214–7. doi:10.1038/nature03342. PMID
15759000.
6) World Health Report 2001Annex Table 3
[http://www.who.int/whr/2001/main/en/annex/anne
x3.htm] 2001
7) www.whoindia.org/LinkFiles/Malaria_Country_
Profile-Malaria.pdf
8) Global coordination of Malaria Control Efforts:
Annex A.The malaria Consortium July 1998
9) www.mrcindia.org/conf/abstracts/3.pdf
10)Aultmann KS, Beaty BJ, Walker ED: Genetically
Manipulated Vectors of Human Disease: a practical
33
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

34
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
INTRODUCTION
detected, as they emerge and actions are taken to contain Antimicrobial resistance is currently the greatest
them, the world could be faced with resistant bacterial challenge to the effective treatment of infections
strains with no known or newer antibiotics available to globally. Resistance adversely affects both the clinical 3
combat them . Several epidemiological studies have and financial therapeutic outcomes with effects ranging
shown that the type and frequency of resistance from the failure of an individual patient to respond to mechanism varies in regions and even among different therapy and need for expensive alternative drugs to the hospitals in the same community and such differences social costs of higher morbidity and mortality rates, have been related to qualitative and quantitative longer duration of hospitalisation, and the need for the
41 differences in antibiotic use . It is important to regularly
changes in the empirical therpay . Multi resistant monitor the pattern of susceptibility of microorganisms
organisms are diminishing our ability to treat and control 5
to antiiotics . This will improve the quality of prescribing the spread of infections. Abuse and misuse of antibiotics
and may help in overcoming the problems associated have been known to contribute to the development of
with the emergence of resistant bacteria. Hospital antibiotic resistance. Clinicians also frequently
antibiograms can be a useful means of guiding empiric commence antibiotic therapy before sending samples to
therapy and tracking the emergence of bacterial the microbiology laboratory for culture sensitivity
resistance among bacterial isolates and such data will 2
analysis . Unless antibiotic resistance problems are 6have better day to day application . Thus the purpose of
the study is to conduct a detailed retrospective and
prospective study about the prevalence of
microorganisms and their sensitivity pattern against
APTI
Indian Journal of Pharmacy Practice Received on 25/01/2010
Accepted on 29/01/2010 © APTI All rights reserved
APTI ijopp
Comparative Study on the Sensitivity Pattern of MicroorganismsVidhya D, Sriram S, Manjula Devi A.S, Rajalingam B, Shivashankar S, Chitra B, Rajeswari R
Department of Pharmacy Practice, Sri Ramakrishna Institute of Paramedical Sciences,
Sarojini Naidu Road, Siddhapudur, Coimbatore – 641 044
Address for correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /0
Accepted on / © APTI All rights reserved
AbstractAntimicrobial resistance is an issue of great significance for public health at global level. The purpose of the study is
to determine the susceptibility patterns of microorganisms to antibiotics and the prevalence of antibiotic resistance
among common pathogens in a tertiary care hospital. The study was conducted in a 500- bedded multi- specialty
hospital in South India (for a period of six months from May 2009 to October 2009 in four different phases). A total of
4321 records were analyzed during the retrospective study (May 2006 to April 2009) which revealed that the major
organisms isolated were E.coli (33.3%), Klebsiella (21.4%), S.pneumoniae (16%), S. aureus (10.7%), Pseudomonas
(8.9%). The sensitivity pattern showed that E.coli, Klebsiella, S.pneumoniae, and Pseudomonas were highly
sensitive to Imipenem and Piperacillin/ Tazobactam. S. aureus was sensitive to Linezolid (80%). In the prospective
study (May 2009 to October 2009) a total of 956 records were screened which showed that the major organisms
isolated were E.coli (37.7%), Klebsiella (24.6%), S.pneumoniae (12%), S. aureus (9.6%), Pseudomonas (7.8%). The
sensitivity pattern studies revealed that E.coli was highly sensitive to Piperacillin/ Tazobactam (92.2%), Klebsiella
to Cephazolin/ Sulbactam (91.5%), S.pneumoniae to Imipenem (91.3%), and Pseudomonas to Sparfloxacin (90.7%)
and S. aureus to Linezolid (91.3%). On comparing the retrospective and prospective data it was seen that
S.pneumoniae had developed resistance to Carbenicillin, Klebsiella to Ofloxacin, Citrobacter to Netilmicin, E.coli
to Amikacin and S.aureus to Methicillin. Key words: Antibiotics, resistance, retrospective, sensitivity pattern
ijopp

35
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
antibiotics which helps the health care professionals to microorganisms for antibiotics during the period May
decrease the irrational antibiotic therapy and also to 2006 to April 2009. The necessity of the study was 7
explained to the physician, pathologist and minimize the development of resistant strains .
microbiologist of the study hospital. A total of 4321 MATERIALS AND METHODS
records were analyzed during the retrospective study. Study site
Major organisms isolated were E.coli (33.3%), The study was in a 500 bedded multi specialty tertiary Klebsiella (21.4%), S.pneumoniae (16%), S. aureus care teaching and one of the largest hospitals in (10.7%), Pseudomonas (8.9%) [Table no. 1]. Similar Coimbatore.study conducted by Odusanya M D in 2002 revealed that Study Periodthe common organisms isolated were S. aureus, E.coli,
The study was carried out fro a period of six months from Klebsiella and S.pneumoniae. The retrospective
May 2009 to October 2009.sensitivity pattern studies showed that E.coli was more
Study designsensitive to Imipenem (96.3%), Piperacillin/ Tazobactam
Retrospective – Prospective study.(92.8%) and Amikacin (81.9%) [Fig. no. 1]. Klebsiella,
Selection criteriaS.pneumoniae, and Pseudomonas were highly sensitive
All the inpatients, outpatients and intensive care patients to Imipenem and Piperacillin/ Tazobactam. S. aureus was
for whom a culture sensitivity test was done were sensitive to Linezolid (80%) [Table no. 2]. Similar study
included in both retrospective and prospective analysis. 9conducted by Aroma Oberoi et al in the year 2006 in 233
Study approvalisolates showed that third generation cephalosporins,
The protocol of the study that includes the objectives and Fluoroquinolones and Aminoglycosides showed the best methodology was submitted to the Dean of the study sensitivity. The major multiple organisms isolated were hospital. The authorization from the Dean was procured Pseudomonas and E.coli, followed by Pseudomonas and as per SRH/ DEAN/F.19/2009-2010. Klebsiella [Table no. 3]. In the prospective study Study material (May 2009 – October 2009) a total of 956 records were A specially designed format was used for entering the screened which showed that the major organisms isolated prevalence and sensitivity pattern of microorganisms were E.coli (37.7%), Klebsiella (24.6%), S.pneumoniae among the patients during the study period. (12%), S. aureus (9.6%) and Pseudomonas (7.8%) [Fig.
METHODOLOGY no. 2]. The sensitivity pattern studies revealed that E.coli
The study was carried out in four phases. The first phase was highly sensitive to Piperacillin/ Tazobactam
involves the retrospective analysis on the sensitivity (92.2%), Klebsiella to Cephazolin/ Sulbactam (91.5%),
pattern of microorganisms for antibiotics for a period of S.pneumoniae to Imipenem (91.3%), and Pseudomonas
three years from May 2006 to April 2009. to Sparfloxacin (90.7%) and S. aureus to Linezolid
The second phase pf the study is the prospective study for (91.3%) [Fig. no. 3]. From the comparison of the
a period of six months from May 2009 to October 2009. retrospective and prospective data it was seen that E.coli
The third phase involves the comparison of data obtained developed resistance to Amikacin, Klebsiella to
from retrospective and prospective study to look for Ofloxacin, S.aureus to Methicillin and S.pneumoniae to 10changes in the sensitivity pattern of microorganisms to Carbenicillin [Table no. 4]. Similar study by Akira
antibiotics, since the sensitivity pattern varies from time (1995) reported strains of Methicillin resistant S.aureus.
to time. Sensitivity pattern studies reflect the major Another study by Ron Dagan revealed that the resistance
organism to be treated and also help to choose the developed by S.pneumoniae varied during the warm and
appropriate antibiotics resulting in rational antibiotic cold months which were 20% and 29% respectively. 8
therapy . During the final phase of the study antibiotic E.coli was present more in urine samples (77%),
usage guidelines for the antibiotics prescribed in the followed by pus (8%), catheter tip (3.4%), tracheal
hospital were prepared and submitted to the physicians. (3.3%) and semen (2.4%). Klebsiella species were
RESULTS AND DISCUSSION present more in urine (50%) and sputum (22.5%).
The study was conducted in four different phases. During S.pneumoniae (63.8%) and Pseudomonas (36.3%) were
the first phase of the study a retrospective analysis was majorly seen in sputum. S.aureus was found more in pus
conducted to check the sensitivity pattern of cells (47.6%) [Table no. 5].

ORGANISM RETROSPECTIVE (n= 4321)
PROSPECTIVE (n= 956)
E.coli Imipenem – 1387
(96.3%)
Piperacillin/ Tazobactam – 332
(92.2%) Klebsiella Imipenem – 848
(91.8%)
Ceftriaxone/ Sulbactam – 215
(91.5%)
S.pneumoniae Imipenem – 631 (91.1%)
Imipenem – 105 (90.7%)
S.aureus Imipenem – 414
(89.1%)
Sparfloxacin – 68
(90.7%)
Pseudomonas Imipenem – 428 (92.2%)
Linezolid – 84 (91.3%)
36
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
ORGANISM
RETROSPECTIVE
(May 2006 – April 2009) (n= 4321)
PROSPECTIVE
(May 2009 – October 2009) (n= 956)
NO. OF PATIENTS
INFECTED
PERCENTAGE (%)
NO. OF PATIENTS
INFECTED
PERCENTAGE (%)
E.coli 1440 33.3 360 37.7
Klebsiella 924 21.4 235 24.6
S.pneumoniae 693 16 115 12
Pseudomonas 386 8.9 75 7.8
S.aureus 464 10.7 92 9.6
S.pyogenes 052 1.2 8 0.8
S.epidermidis 102 2.4 - -
Proteus 108 2.5 30 3.1
Enterobacter 068 1.6 12 1.4
Actinobacter 066 1.5 16 1.7
Citrobacter 006 0.1 9 0.9
a-Hemolytic
streptococci 010 0.2 - -
Salmonella 002 0.05 4 0.4
Table.1: Percentage Prevalence of Microorganism- A Comparison
Table.2: Sensitivity pattern of microorganisms

ORGANISM
ANTIBIOTIC
DEVELOPMENT OF RESISTANCE
RETROSPECTIVE (%) PROSPECTIVE (%)
E.coli Amikacin 18.1 41
Klebsiella Ofloxacin 49 70
S.pneumoniae Carbenicillin 52 84
S.aureus Methicillin 70.3 98.7
Citrobacter Netilmicin 50 88.9
37
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
ORGANISMS RETROSPECTIVE
(n= 26) PROSPECTIVE
(n=14)
Pseudomonas + E.coli 6 1
Pseudomonas + Klebsiella 4 2
Pseudomonas + S. aureus 3 1
S.pneumoniae + Klebsiella 3 3
S.pneumoniae + S. aureus 3 1
Klebsiella + E.coli 2 1
Klebsiella + S. aureus 1 2
S. aureus + S.pyogenes 1 1
S. aureus + E.coli 3 2
Table.3: Multiple Orga nisms Isolated
Table.4: Emergence of Resistance

38
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Table.5: Specimen vs. Organism – Retro spective
ORGANISM URINE TRACHEAL PUS CELLS THROAT
SWAB WOUND SPUTUM
E.coli 71.1 5.8 6.4 21.1 3.9 2 .5
Klebsiella 80 5.1 6.4 4.7 0.4 1 .7
S.pneumoniae 1.7 2.6 1.7 10.4 - 77.4
S.aureus 13 3.3 53.3 2.2 5.4 4 .3
Pseudomonas 20 14.7 14.7 18.7 - 29.3
Fig.1: Percentage sensitivity pattern of microorganisms - Retrospective
% SENSITIVITY PATTERN OF MICROORGANISM - RETROSPECTIVE
81.9
68
60.858.2
74.4
92.888.1 88.7
83.786.9
71
6063.5
55.9
48.1
96.391.8 91.1 89.1
92.2
40
51.1
69.3
29.8
43.3
0
20
40
60
80
100
120
E.coli Klebsiella S.pneumoniae Pseudomonas S.aureus
ORGANISM
%SE
NSITIV
ITY
Amikacin Pieracillin/Tazobactam Ceftriaxone/ Sulbactam
Imipenem Ofloxacin
Fig.1: Shows the percentage sensitivity pattern of microorganisms retrospectively (from May 2006 to April 2009). A total of 4321 records are studied and this shows that all the organisms were highly sensitive to Imipenem i.e., E.coli (96.3%), Klebsiella (91.8%), S.pneumoniae (91.8%), and Pseudomonas (89.1%) and S. aureus (92.2%). The other antibiotics which show better sensitivity are Piperacillin/ Tazobactam and Amikacin.

39
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
Fig.2: Retrospective vs Prospective organism prevalence (%)
RETROSPECTIVE vs PROSPECTIVE ORGANISM PREVALENCE (%)
33.3
21.4
16
8.9
10.7
37.7
24.6
12
7.8
9.6
0
5
10
15
20
25
30
35
40
E.coli
Klebsiella
S.p
neu
moniae
Pse
udomon
as
S.a
ureu
s
ORGANISM
PATIE
NTS
INFECTED
RETROSPECTIVE
PROSPECTIVE
Fig.3: Sensitivity pattern of microorganism prospective
% SENSITIVITY PATTERN OF MICRO ORGANISM PROSPECTIVE
92.2 90.2
76.5
8488
83.6
88.991.3
81.3
87
0
10
20
30
40
50
60
70
80
90
100
E.coli Klebsiella S.pneumoniae Pseudomonas S.aureus
ORGANISM
PE
RC
EN
TAG
E
Amikacin
Pieracillin/Tazobactam
Ceftriaxone/
SulbactamImipenem
Ofloxacin
Fig.2: shows the comparative prevalence (retrospective and prospective) of organisms in the study hospital. It may be seen both in the retrospective and prospective study that E.coli is the most commonly found organism, ie 33.3% and 37.7% respectively, followed by Klebsiella 21.4% and 24.6%. The other organisms commonly prevailing are S.pneumoniae, and Pseudomonas and S. aureus.
Fig.3: Shows the percentage sensitivity pattern of microorganisms prospectively fir a six month period (May 2009 to October 2009). A total of 956 records are studied and this shows that all the organisms are highly sensitive to Imipenem, Ceftriaxone, Piperacillin/ Tazobactam and Amikacin.

40
CONCLUSION microorganisms from community acquired
pneumonia. JK Science 2006;8:79-82.As there is increasing international concern regarding the
escalating antibiotic resistance, periodical study on the 10.Akira W, Kotaro O, Kazuhiro M, Takeshi N, 12 Masakichi M, Toshihiro N. Antibiotic susceptibility control of antibiotic resistance is necessary . This can be
of the sputum pathogens and throat swab pathogens achieved only when proper sensitivity pattern data are
isolated from the patients undergoing treatment in available. The pharmacist's role in advising prescribers
twenty-one private clinics in Japan. Tohoku J Exp on antibiotic prescribing issues gained more importance
Med 1995;175:235-247.in adhering to rational drug therapy and complete patient 13
care . The study revealed that clinical pharmacists play 11. Ron D, Galia B, Noga G, Amir ZS, Daniel V, Ted C, et.
an important role in promoting optimal antibiotic al. Seasonality of antibiotic resistant S.pneumoniae
prescribing practice among physicians, during their that causes acute otitis media: A clue for an antibiotic 14 restriction policy. J Infect Diseas 2008;197(8):1094-routine daily visit to wards .
1102.REFERENCES
12.Ravi PS, Praveen P, Nagesh KS, Joshy M, Narayanan 1. Essack SY, Connolly C, Strum AW. Antibiotic use and K. Prescribing patterns of antibiotics and sensitivity resistance in public sector hospitals KwaZulu – Natal. patterns of common microorganisms in the internal S Afr Med J 2005;95:865-870.medicine ward of a teaching hospital in Western 2. Odusanya OO. Antibiotic susceptibility of Nepal: a prospective study. Ann Clin Microbiol microorganisms at a general hospital in Nigeria. J Antimicrob [serial online] 2008 [cited 2007 Feb Natl Med Assoc 2007;94:994-998. 1];16:2-7. Available from: URL:http://www.ann-3. Lakshmi V. Need for National/ Regional guidelines clinmicrob.com/content/2/1/7and policies in India to combat antibiotic resistance.
13.Shlaes DM, Gerding DN, John JF. Optimizing Ind J Med Microbiol 2009;26(2):105-107.antibiotic use in hospitals: Methods of data collection 4. Jacobs Michael, Flemingham David, Appelbaum and analysis. Pharmacotherapy [serial online] 2008 Peter C, Gruneberg Reuben N. Susceptibility to [cited 2008 Oct 5];23(12):152-157. Available from: pathogens isolated from CARTI to commonly used URL:http://www. pharmacother.org.antimicrobial agents. J of Antimicrobial
14. Cole O. Combating resistance to antibiotics. Hosp chemotherapy 2003;52:229-246.Pharmacist 2002;9(1):21-22.5. Ozumba Uchenna Chinedu. Antimicrobial resistance
problem in a University hospital. J Natl Med Assoc
2005;97:1714-1718.
6. Shoba KL, Rao PS, Thomas J. Survey of
Staphylococcus isolates among hospital personnel,
environment and their antibiogram with special
emphasis on methicillin resistance. Ind J Med
Microbiol [serial online] 2005 [cited 2009 Oct
30];23:186-88. Available from URL:http://
www.ijmm.org/text.asp?2009/23/3/186/ 16592.
7. Agalar C, Aydin S, Yaris F, Ozcakir A. Most common
infections and antibiotic prescribing habits of
residents: experience of three university hospitals.
Turk J Med Sci 2005;35:169-173.
8. Serena P, Akhilesh CJ. A study of antibiotics used in
adult respiratory disorders in Kathmandu and
Bhaktapur. J Nepal Med Assoc 2008;43:31-35.
9. Oberoi Aroma, Agarwal Aruna. Bacteriological
profile, serology and antibiotic sensitivity pattern of
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

Counterfeit drugs are a menacing and deadly problem and is exploited by counterfeiters. Counterfeit medicines
worldwide contributing to morbidity, mortality, toxicity, contain wrong ingredients, insufficient ingredients and
and drug resistance among the individuals. The sometimes no active ingredients at all. The consequences
proliferation of fake drugs is astounding, with over 100 of taking counterfeit medicines include treatment failure,
countries reporting incidents of fake drugs according to a drug resistance and sometimes death. It is the right of
2008 report from the Pharmaceutical Security Institute. every patient to receive quality medicines. To achieve
The incidents of drug counterfeiting show no evidence of this, changes are needed in the existing Indian regulations
declining: some industry people suggest that the number to preserve a medicine's integrity and stop intermediaries
of counterfeit medicines in market has increased to as tampering with them. We therefore strongly urge the
much as 25% each year over the past several years. Indian Commissions to consider the benefits to all
Counterfeiting medicines is not a new issue, in Graham stakeholders of medicines traceability and authentication
Greene's 1948 novel The Third Man was a story about a through its review of medicines distribution in India as
search for a smuggler of counterfeit penicillin in postwar o ther developed na t ions l ike Europe e tc .
Vienna. Although the literatures on counterfeit medicines In order to check the adulteracy an industry-wide
in the medical and scientific communities aren't vast, solution has been proposed in the form of barcode to
there's a lot in newspapers and magazines because protect patient safety through a more transparent
journalists have picked up high-profile stories. medicine supply chain, thereby attempting to tackle the
A counterfeit medicine is a compound that is not made by rise in counterfeit duplicate medicines entering the
an authorized manufacturer but is presented to the market. Championing 2D Data-Matrix Bar Coding
consumer as if it were. The global estimates of drug should be done on the wrapper of the medicines as a
counterfeiting are somewhat ambiguous, depending on technological solution to support its call for tighter
geographic region, but proportions range from 1% of regulation and better enforcement in the supply chain to
sales in developed countries to >10% in developing protect patient safety.
countries. Medicines counterfeiting is highly There is need for a transparent and secure medicines
sophisticated and it is almost impossible for patients and supply chain that puts the patient first and where all
dispensing healthcare professionals to spot the fakes. stakeholders take responsibility for guaranteeing the
There is also a lack of transparency in the legitimate integrity of medicines. “A unique bar-coding should be
medicines supply chain, which makes it vulnerable to done on every medicine pack before it leaves its
infiltration by counterfeiters. This puts lives at risk. From manufacturer”. This way, at every stage of its
the manufacturer to the dispensing healthcare distribution, up to the point at which it reaches the patient,
professional, the safe supply of medicines can only be the medicine can be authenticated to make sure it is
achieved if each and every stage of the supply chain genuine.” DataBar Barcode is a type of linear barcode
enforces safe practice. This is not currently the case. The symbol. DataBar when linked with 2D barcode,
existing system makes it almost impossible to establish especially Micro PDF barcode with linkage character is
the pedigree of a medicine dispensed to a patient. This is called 2D Data-Matrix Bar-Code. When linkage
made worse by repackaging and re-labelling medicines character is turned on, scanner will read both barcode one
within the supply chain which contributes to uncertainty after another.
The encrypted 2D Data Matrix Bar-Code can also carry a
randomized number unique to the individual pack,
making it even harder for counterfeiters to successfully
41
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
APTI ijopp
Counterfeiting of medicine is no more incurable now
Sayed Aliul Hasan Abidi
J.S.S. College of Pharmacy, Mysore, Karnataka
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on 21/01/2010
Accepted on 28/01/2010 © APTI All rights reserved

42
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
copy and bring their fakes to market. By using a hand Integrity of manufacturers packaging
held bar-code reader which very common in most Removing or interfering with manufacturers packaging
European pharmacies, Indian markets should also can never be in the interests of patient safety. Parallel
employ such technology so that the dispenser will be free traders repackage and over-label medicines. These
to scan the encrypted 2-D data matrix code and check practices may have to be reviewed with the introduction
vital data including recall information and the details of of a new, safer medicines tracing and authentification
every trader who has handled that pack in the supply system.
chain. The introduction of unique coding for each pack of The consequences of counterfeiting: medicine, together with authentication, track and trace Counterfeiting is of grave concern for consumers, systems and physical security in the form of tamper governments, and legitimate manufacturers as well. It resistant packaging will dramatically improve the safety has significant social and economic consequences. The of medicines supply. This involves the integration of four important one is that the consumers don't get the safe and key elements. effective products they pay for and, instead, may be put at Tamper resistant packaging significant risk. On the economic point of view, Medicines currently lack the type of tamper resistant legitimate manufacturers of pharmaceuticals suffer from devices now taken for granted in other sectors such as the patent and copyright infringement. Counterfeiting, in food and drinks industry. All medicines should possess reality, "hijacks" the brand. For these reasons, this should special features to show whether the packaging has been be strictly handled by employing science and technology opened. This includes bottles with external seals or and in this context 'Bar coding' seems to be a highly tampers evident screw caps, and boxes with seals or promising and reliable solution to fight away this perforated panels. menace.
2D Bar Codes REFERENCES 2D data matrix bar codes printed on packaging during 1. Counterfeit Medicines: a New Update on Estimates. manufacture can provide each medicine with a unique Position statement by the International Medical identity before it enters the supply chain. Significant Products Anti-Counterfeiting Taskforce (WHO). quantities of encrypted information can be stored this 2006, Nov.way to support pharmacists, regulators and government
2. Available- from: URL:www.usp.org/worldwide/ authorities in the authentication and tracing of individual
dqi/drugQuality.htmlmedicines. 2D data matrix bar codes help prevent
3. Shepherd M. Beef up international cooperation on dispensing errors and make counterfeit medicines easily
counterfeits. Nature Medicine 2010;16:366.identifiable. Existing scanners found in most pharmacies
4. Newton PN. Counterfeit anti-infective drugs. Lancet can read the bar codes and no additional work is required
Infectious disease 2006;6:602-13.by the pharmacist. Scanned information is transmitted to
5. Mukhopadhyay R. The hunt for counterfeit an independent electronic data hub and a verification
medicine. 2007;10:2622-27.message is quickly returned to the dispensing
6. World Health Organization 2006. Fact Sheet No. pharmacist.275. Available fro: URL:www.who.int/mediacentre/ Dispensing authentication and transparencyfactsheets/fs275/en
No part of the supply chain should accept medicines 7. Nyadong L. Analytical Chemistry 2007.without validation. With tamper resistant packaging and 8. Eliasson C, Matousek P. Non-invasive detection of 2D data matrix bar codes in place, a unified system with
counterfeit drugs using spatially offset Raman agreed responsibilities across the country will allow each spectroscopy (SORS). Central Laser Facility Annual individual medicine pack to be traced. This will take the Report 2007.place of existing systems which is not of much
9. Tipke. Substandard anti-malarial drugs in Burkina significance in preventing counterfeiting and do not
Faso. Malaria Journal 2008;7:95.allow the pedigree of medicines imported across national
boundaries to be checked. A safe medicine supply is one 10. Sharp J. Quality in the Manufacture of Medicines and
in which every stakeholder is able to trace and other HealthCare Products. London: Pharmaceutical
authenticate the medicine back to the manufacturer. Press; 2000.

43
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
INTRODUCTION
Medicines are perhaps the most important medical priorities and reduce the quantities of less cost effective
medicines. Though the decentralized system of health intervention in health care delivery systems. Thus the
care- shifting the responsibility for managing health care availability and easy accessibility to quality medicines
services from central level to intermediate and by the public is an important component in health care
community levels is favoured, the pooled procurement services. The non-availability of medicines demoralise
process (centralized procurement) is proved to be more the health work force and the health system looses
beneficial in cutting cost and ensuring quality and credibility. The people will not use the system and the
quantity. Pooled procurement of medicines has been system may fail. Health system can not succeed unless
remarkably successful reducing the expenditure on the continuing availability of quality medicines is
purchase of medicines in Tamil Nadu. The National ensured. The component of the medicines in the overall
Rural Health Mission review views the Tamil Nadu health budget of the central and state governments is just
system of Drug Procurement (full Medicine supply around 12 % and 10% respectively. Often the drug management system) is one of the best in the country and expenditure as percentage of health expenditure is as low is a role model for other states.as less than 2 % in some states. Such small percentage of
Procurement plansmoney allotment or spent on medicines requires careful
Procurement plans are usually based on requirement planning on drug supply management in order to
estimates derived mathematically from the following optimise the utilization of resources for ensuring
data: (i) forecasts, (ii) stock on hands at all levels of availability of quality medicines in public health system.
distribution system, (iii) previous procurement quantities Procurement is an important step in overall drug
ordered or deliveries expected, (iv) losses expected to management cycle which primarily determines cost
occur due to damage or expiry, (v) transfer to or from containment. Procurement or purchasing is the
other logistic system and (vi) desired stock at the end of identification of suitable source of supply and the
each planning period (including safety stocks and acquisition of supply according to the procurement plan,
working stocks at all levels). The estimated quantity of as economically as possible, within established quality
medicine required in a given planning period, usually an standards. Regardless of how medicines are procured, year, can be calculated as: Quantities required = (Stock the goal should be to make procurement process as on hand + Quantities already ordered + Transfer expected effective and efficient as possible. Effective procurement from any other source - Estimated consumption for the enables the government or procurement agency to make period - Losses - Desired stock at the end of period).necessary medicines available based on quality, timing,
Procurement Processand quantity specifications in the procurement plan.
The core principles of medicines procurement are:Efficient procurement means that medicines are
purchased at least possible cost to the system. In budget · Procurement of most cost effective medicines in the
constraint situation, VEN (vital, essential and non- right quantities;
essential) analysis, Therapeutic category analysis and · Selection of reliable suppliers of quality products;
ABC analysis techniques may be utilized to select · Assurance of timely delivery; and
· Use of lowest possible cost.
The following general procurement methods are
followed in procurement practices in public health
APTI
Indian Journal of Pharmacy Practice
Received on 02/06/2010
Accepted on 04/06/2010 © APTI All rights reserved
APTI ijopp
Medicines Procurement Practices in Public SectorMohanta GP, Veena R*
Department of Pharmacy, Annamalai University, Annamalai Nagar – 608 002, *School of Pharmacy, Mahatma
Gandhi University, Kottayam, Kerala)
Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice
Received on /
Accepted on / © APTI All rights reserved
ijopp

system. Their advantages and disadvantages given in
the tabular form:
Method Criteria Advantages Disadvantages
Open Tender Quotations are invited from
potential manufactures or suppliers
Many bids some with low
prices; New suppliers can be
identified
High workload required in
evaluating bids and selecting suppliers
Restricted Tender
Open only to pre-qualified suppliers
Fewer bids; Pre-qualified suppliers;
Quality easier to ensure
Fewer bids; More limited options; A
system for prequalification needs to be in place.
Competitive
Negotiation
Approaching a few selected
manufacturers or suppliers and requesting price
quotations
Suppliers are generally well
known; Less evaluation work
Generally higher prices
Direct Procurement
Direct purchase from a single supplier either at
quoted prices or negotiated prices
Easy and Quick High prices; Transparency is in question
A restricted tender, open to pre-qualified suppliers, pharmacists are knowledgeable and skilled on
should be the method of choice. The World Health determining the quality of medicines, their presence in
board would likely to ensure quality consideration in Organization follows pre-qualification of products for
addition to price in awarding the tender. The procurement by International Agencies. The pre-
Procurement system should have in built mechanism for qualification criteria are often in built into the tender
monitoring the supplier's performance. The suppliers' document. The pre-qualification of suppliers can be
compliance with terms and conditions of the contract made obtaining supplier information through
must be recorded. Quality of supply is also to be checked questionnaires, evaluating product samples, evaluating
through visual inspection following standard operating the past performance etc.
procedure with pre-determined criteria.In the tender invitation, the terms and conditions of the Tamil Nadu Model of Procurement
procurement are laid down. The document must specify In order to redress the chronic non-availability of
at least the following:essential medicines in most of the health facilities, the
· How the quotations should be submitted.government of Tamil Nadu in 1994 set up a government · Terms of payment.procurement and distribution agency, Tamil Nadu · Delivery period.
· Delivery schedule. Medical Service Corporations Limited (TNMSCL). It · Product specification. was entrusted with the responsibility for streamlining · Labelling. procedure for procurement, distribution and storage of · Packaging.
medicines within the entire health care network of Tamil · Shelf life.
Nadu.The tender invitation document must lay down the The system procures drugs on International
technical and basic requirements for obtaining products Nonproprietary name (Generic Name) for all health
of acceptable quality. This also serves as a reference in facilities, called pooled procurement. The salient
the event of problems or disputes with the supplier. After features of the procurement process:
thorough evaluation of bids, the tender board usually · Updating the essential drugs list.
awards the tender. It is important that the pharmacist · Procurement by generic name only.with knowledge and expertise of pharmaceutical · Open tender system inviting bidding only from
products or medicines must be part of the board. As manufacturers.
44
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

· Pre-qualification criteria: CONCLUSION
· GMP certification for manufacturer. Procurement in public health system involves a · Market standing of at least three years.
competitive bidding process where the lowest qualifying · Minimum turn over.
bidder unconditionally wins the contract. Tendering or · Two lower suppliers are also approved.
Competitive bidding for drug procurement has been · Outer and inner package of all items bear the logo of
TNMSC and labels with “For state government (TG) accepted as being positive in terms of making the process
only & Not for Sale”.as fair and transparent as possible. But it has few negative
· Quality Control: Coded samples are analysed in private aspects too. Though competitive bidding reduced the
approved laboratories.possibilities of collusion, fraud and corruption practices, · 90% of the medicines requirement (in terms of budget)
are supplied by TNMSCL and remaining 10% budget it has not completely prevented these to occur. The
meant for local purchase by individual health facility. competitive bidding (especially in case of high volume Pooled procurement with transparent tender system with
and price contracts) is time-consuming process which well-defined pre-qualification criteria and efficient
may take at least 6 often more than 12 months. A new distribution and storage system helped in improving the
drug availability in health systems. approach or mechanism may arise with time which
Other states like Kerala, Andhra Pradesh and Karnataka would perhaps make the system of procurement methods are following similar procedures for Medicine
further efficient with better transparency.Procurement for the respective states through
REFERENCESestablishment of procurement agencies in line of Tamil
Nadu Model. The procurement agency as part of quality 1. Managing Drug Supply, Second Edition, assurance programme as well for monitoring the
Management Sciences for Health in Collaboration performance of suppliers often publicly disclose the
with the World Health Organization, 1997.name of banned and disqualified suppliers. This helps
other procurement agencies eliminating them from 2. Operational Principles for Good Pharmaceutical prospective list. One can find the list of such suppliers at
Procurement, WHO, 1999.JIPMER website.
3. Practical Guidelines on Pharmaceutical Procurement Hospital Pharmacy in Drug procurement
for Countries with Small Procurement Agencies, As procurement being centralized in most of the states
following successful model of Tamil Nadu, the hospital WHO, Manila, 2002.pharmacy department of hospitals will have little options
4. Ranjit RC, Nirmal KG. Enhancing Acess to Quality for directly participating in drug procurement. However,
Medicines for the Undeserved, Delhi Society for its expertise on estimating drug requirement for the
health facility is important feed back for finalizing the Promotion of Rational Use of Drugs, 2003.quantity to be procured by the central agency. As most
5. The Medicines Scenario in India: Perceptions and health facilities would have provisions for local purchase
Perspectives, Delhi Society for Promotion of Rational to some extent to cater local needs, the hospital pharmacy
continues to involve in drug procurement, but only to the Use of Drugs.
extent of direct purchasing. But in private or corporate 6. Mohanta GP , Manna PK, Manavalan R, Veena R.
hospitals, the hospital pharmacy continues to be involved Quality Assurance Programme in Procurement of in procurement process for procuring drugs and other
supplies for the hospitals. Even in private charitable Medicines, The Pharma Review, October 2006.
institutions with several health facilities adopted pooled 7. Mohanta GP, Manna PK, Manavalan R, Veena R,
procurement process with delivery at different locations. nd
Procurement of Medicines, Pharmabiz, 02 August One example of this type is: Emmanuel Hospital
Association. 2006.
45
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010

46
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
INTRODUCTION
Erythema Multiforme in about 1 in 1000 adult patients. The main risk factors
appear to be concomitant with use of valproate and
exceeding the recommended initial dose of lamotrigine
or the recommended rate of dose escalation (Sachs et al., 5
possibly mediated by deposition of 1997). These skin rashes reactions usually occur within
immune complex (mostly IgM) in the superficial 8 weeks of starting the therapy with Lamotrigine, but
microvasculature of the skin and oral mucous membrane onset as early as the first day and as late as 2 years has 2 6that usually follows an infection or drug exposure. been noted.
Lamotrigine is a novel anti-epileptic drug that has been The commonly seen severe forms of dermatologic
proven effective as an adjuvant medication in children reactions with lamotrigine therapy are erythema
and adults with refractory partial seizures, in Lennox- multiforme, Steven Johnson syndrome and toxic
Gastaut syndrome and in tonic-clonic seizures that are epidermal necrolysis. The pathogenesis of these severe
not satisfactorily controlled by other anti-epileptic cutaneous ADR's is unknown, although a metabolic basis
agents. Lamotrigine is also found to be effective in has been hypothesized. Anticonvulsants like lamotrigine 3
bipolar depression with minimal risk of inducing mania. are metabolized to toxic metabolites which are
It mainly acts by prolonging the sodium channel subsequently detoxified in most individuals. However in
inactivation and suppression of high frequency firing. In predisposed patients with genetic defect, the metabolite
addition it also bocks the voltage sensitive sodium may bind covalently to proteins. In some of these
channels, thus stabilizing the presynaptic membrane and patients, the metabolite- protein adduct may trigger an
preventing release of the excitatory neurotransmitters, immune response, which may lead to a cutaneous 4 7mainly glutamate and aspartate. adverse reaction.
Adverse effects reported with the use of Lamotrigine Treatment of erythema multiforme, Steven Jhonson
include angioedema, photosensitivity, diplopia, blurred syndrome and Toxic epidermal necrolysis includes
vision, discontinuation of the drug and supportive measures,
conjunctivitis, dizziness, insomnia, headache, ataxia, such as careful wound care, hydration and nutritional 7tiredness, nausea, vomiting, aggression, tremor, support.
confusion and Skin rashes. Rashes account for CASE REPORT
withdrawal from the therapy in about 2% of those given The patient was 34 year old male who was a known case lamotrigine and serious skin reactions including Steven of bipolar disorder and on lamotrigine 50 mg once daily Johnson syndrome and toxic epidermal necrolysis occur (OD) along with magnesium valproate 200mg since
month and a half. Apart from his psychiatric history, he
was on tamsulosin hydrochloride since one year for
benign prostrate hyperplasia and urinary incontinence,
is an acute mucocutaneous
inflammatory and hypersensit ivi ty reaction
characterized by a skin eruption, with symmetric
erythematous edematous or bullous lesions of the skin or 1
mucous membranes
APTI
Indian Journal of Pharmacy Practice Received on 21/04 /201 0
Accepted on 28/04/2010 © APTI All rights reserved
APTI ijopp
Lamotrigine Induced Erythema Multiforme: A Case ReportMahvash Iram*, Shobha Rani.R.H, Megha Bhat.Y
Dept of Pharmacy Practice, Al-Ameen College of Pharmacy, Bangalore.Address for correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /
Accepted on / © APTI All rights reserved
ijopp
AbstractThe prototypical lesion of Erythema Multiforme is a targetoid dusky erythematous patch, found predominantly on the
extremities, although many different morphologies may be observed. Lamotrigine is an anti epileptic drug found to
be effective to treat bi polar disorder, however it is reported to cause various hypersensitivity reactions ranging from
a simple rash to life threatening reactions like Steven Johnsons Syndrome. A case of Lamotrigine induced Erythema
Multiforme is discussed herewith. Key words: Erythema Multiforme, Lamotrigine, Anti-epileptic drugs

47
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
no known drug or food allergies were reported DISCUSSION
previously. Patient was admitted to hospital with fever Erythema Multiforme
and moderate degree rash (maculo papular) centrifugal in characterized by a dense dermal inflammatory
distribution, first noticed over arms and abdomen which cell infiltrate and keratinocyte necrosis. Erythema
then spread to face, extremities and scalp. Rashes were Multiforme
associated with itching and scaling of skin, bleeding of
gums and skin was not reported. Patient was emotionally
unstable and extremely uncomfortable with his new Erythema Multiforme
found problem, more so considering his psychiatric
condition. Patient was isolated since he was not
comfortable with the other people around.
Hematological, Urine, Renal as well as Liver function
tests were carried out which were normal, suggesting
clearly that it was a hypersensitivity reaction induced by
lamotrigine and valproate. The drugs lamotrigine and Erythema Multiforme
valproate were discontinued immediately. Treatment was Lamotrigine and one
done with Hydroxyzine (anti-histaminic agent) and of the other AED exhibited hypersensitivity with rashes
prednisolone (steroid) prescribed to subside the itching indicating that LTG-induced rash is more likely to occur
and rashes of the skin. Escitalopram and Alprazolam with polytherapy. The reason of the latter finding has not
were considered for psychiatric problem of the patient, been known till date. In addition several researches
however tamsulosin was continued.Apart from the pointed out that higher starting dose and rapid increment 9, 10, 11
pharmacotherapy, supportive care including proper skin of dose are risk, factors for Lamotrigine induced rash.
care, fluid therapy, liquid paraffin were started. Patient Hypersensitivity reaction with lamotrigine typically
was better after 3 days of admission with reduced itching develops between 2 and 8 weeks after starting therapy but th
and redness of skin and was discharged on 5 day of can occur after 12 weeks or longer. Although lamotrigine
treatment with the same discharge medication as can be added to valproic acid with an acceptable
mentioned above. incidence of side effects; reports suggest that 60% of the
is caused by various insults from
a drug,
minor which typically affects a single
mucosa is the most common form and may be associated
with symmetrical target lesions on the extremities.
major is more severe, typically
involving 2 or more mucous membranes with more
variable skin involvement. This feature is used to
distinguish it from Stevens–Johnson syndrome, where
there is extensive skin involvement, significant
morbidity, and a mortality rate. Although it is more
frequently seen in males, the incidence of drug-related 8
is similar in males and females.
Many reports have mentioned that
Fig.1:

48
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
patients with hypersensitivity related to lamotrigine were lamotrigine is essential, and the patient should be closely 12
monitored over the next several weeks for the taking valproic acid. Although prolonged symptoms
and fatalities have been reported, early recognition and development of other systemic problems, such as
discontinuation of offending agents often result in rapid hepatitis and renal failure, as residual symptoms can
improvement, as with our patient. persist for weeks. Intravenous steroids may also have 13
After the hypersensitivity reaction is seen cessation of utility in slowing the progression of the syndrome. With
Fig.2:
Fig.2:

49
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
the proper recognition of lamotrigine-associated 388- 395.
hypersensitivity, the risk of morbidity and mortality of 8. Isik SR, Karakaya G, Erkin G, Kalyoncu AF.
this rare condition can be reduced.Multidrug-Induced Erythema Multiforme. J Investig
CONCLUSIONAllergol Clin Immunol 2007;17(3):196-198
Since lamotrigine is known to cause hypersensitivity skin 9. Thome-Souza S, Freitas A, Fiore LA, Valente KD.
reactions, it must be used with care and in the appropriate Lamotrigine and valproate: efficacy of co-dose recommended instead of using a higher dose at the administration in a pediatric population. Pediatr outset. In our case the initial dose of lamotrigine was 50 Neurol 2003 May; 28(5):360-364.
mg/day, higher than the recommended starting dose of 25 10.Culy CR, Goa KL. Lamotrigine. A review of its use in
childhood epilepsy. Paediatr Drugs 2000 Jul-Aug; mg/day for bipolar disorder which could be the possible 2(4):299-330.reason to trigger the hypersensitivity reaction. Another
11. Rogvi-Hansen B, Gram L. Adverse effects of major factor could be the concomitant use of magnesium established and new antiepileptic drugs: an attempted
valproate with lamotrigine suggestive of the reaction. comparison. Pharmacol Ther 1995; 68(3):425-434.
The risk can be minimized with appropriate use of drugs, 12.Rahman M, Haider N, Fargo, ND. Anticonvulsant
it is recommended to inform all patients about skin Hypersensitivity Syndrome from Addition of
complications that are not uncommon, especially in the Lamotrigine to Divalproex. Am J Psychiatry May initial two months and to avoid polytherapy as far as 2005;162:5.possible.
13.Blondin NA, Zahedi S, Hale MS. A Case of ACKNOWLEDGEMENT
L a m o t r i g i n e - A s s o c i a t e d A n t i c o n v u l s a n t Authors wish to thank medical superintendent,
Hypersensitivity Syndrome. J Clin Psychiatry consultants and nursing staff of St. Martha's Hospital,
Bangalore for their support and encouragement. The 2008;10(3): 249–250
authors are also thankful to the Principal and
management of Al-Ameen College of Pharmacy,
Bangalore for their support.
REFERENCES
1. Carder RK. Hypersensitivity reactions in neonates
and infants. Dermatol Ther 2005;18:160-75.
2. Farthing P, Bagan JV, Scully C. Mucosal Disease
Series. Number IV. Erythema multiforme. Oral Dis
2005;11(5):261-7.3. Sogut A, Yilmaz A, Kilinc M, Sogut AG, Demiralay
E, Uzar H. Suspected lamotrigine-induced toxic
epidermal necrolysis. Acta neurol belg 2003;103:95-
984. Tripati KD. Antiepileptic drugs In: Essentials of
thMedical Pharmacology. 5 ed, New Delhi. 2001:376
– 377.
5. Sachs B, Ronnau AC, Schmiedeberg S, Ruzicka T,
Gleichman E, Schuppe HC. Lamotrigine-induced
Stevens - Johnson syndrome: Demonstration of
specific lymphocyte reactivity in vitro. Dermatology
1997;195: 60-64.
6. Sweetman SC. Martindale- The complete drug rd
reference. 33 ed; 351
7. Knowles S, Shapiro L, Shear N H: Serious
dermatologic reactions in children. Dermatology

50
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
INTRODUCTION
Stevens Johnson Syndrome (SJS) is a hypersensitivity Among the drugs used for longer periods, the increased
reaction characterized by skin rashes with hyper risk is confined largely to the first two months. The
pigmentation and cutaneous target lesions involving commonly implicated drugs in this category include 1 carbamezapine, phenobarbital, phenytoin, valproic acid blistering/erosions over face, trunk & limbs. The
etc. Such kinds of reactions are independent on dose of incidence of SJS ranges from 7 to 49 cases per million 4,5
persons per year with higher incidence in male compare drug and are idiosyncratic. Ibupofen is widely used non
to female. SJS presents in three different forms which steroidal anti-inflammatory drug for pain relief and 6reflect the same condition: a mild form, called erythema fever. A literature search revealed very few previously
multiforme (EM) (where <10% Total Body Surface Area reported cases of mucocutaneous drug reactions 7is affected), the main form (between 10 and 30%), and the secondary to non-steroidal anti-inflammatory therapy.
severe form, called toxic epidermal necrolysis We report a case of ibuprofen induced Stevens Johnson
(TEN).Stevens-Johnson syndrome (SJS) is a serious Syndrome.
systemic disorder with the potential for severe morbidity CASE REPORTand even death. SJS has the mortality rate is A 22 year old male patient from rural area of Gujarat was approximately 1-5%. However, when more than 30% admitted in emergency department of the Sheth Vadilal Body Surface Area sloughing is present, the mortality Sarabhai General Hospital, Ahmedabad (India) with
2,3 rate is between 25% and 35%. chief complaint of congestion of eyes since 3 days with Various etiologic factors have been implicated as a cause involvement of tongue and oral mucosa and skin lesions of SJS, including infection, vaccination, drugs, systemic since two days.(See Figure 1) Mucosal involvement diseases, physical agents, and food. Stevens-Johnson included erythema, edema, sloughing, blistering, etiology is mainly a reaction to medication with more ulceration, and necrosis. He had history of sneezing, than 80% of cases of SJS/TEN related to drug only. cough and generalized body pain for the last three days
prior taking any medication. He took the medication pain
killer ibuprofen and Vick VapoRub ointment for the rd
treatment of the same for last four days. On the 3 day of
APTI
Indian Journal of Pharmacy Practice Received on 14/04 /201 0
Accepted on 20/04/2010 © APTI All rights reserved
APTI ijopp
Ibuprofen Induced Stevens Johnson Syndrome -A Case Report1 2 1*
Tapan Shah , Yogesh B. Shah , Amit Raval1 2Department of Pharmacology, Institute of Pharmacy, NIRMA University; Department of Dermatology, Sheth
Vadilal Sarabhai Hospital;Address for Correspondence: [email protected]
Indian Journal of Pharmacy Practice Received on /
Accepted on / © APTI All rights reserved
ijopp
AbstractThe Stevens-Johnson syndrome (SJS) is a rare immune-complex-mediated hypersensitivity disorder which affects 7
cases per million persons per year. This article describes a case study of a 22 year old male patient who was admitted
to the Sheth Vadilal Sarabhai General Hospital, Ahmedabad, with chief complaints of congestion of eyes with
mucosal involvement included erythema, edema, sloughing, blistering, ulceration for last three days prior to
admission. He had multiple purpuric macular lesions on face, neck, upper limb and lower limb. Past history of
medication revealed intake of non steroidal anti-inflammatory drug (Ibuprofen) and Vicks VapoRub ointment for
sneezing, cough and overall body pain for last five days prior to admission to the hopsital. Based on signs and
symptoms, with causality assessment analysis diagnosis of drug induced Stevens Johnson syndrome was confirmed.
In the scarcity of evidence of effective treatment, patient was managed with symptomatic therapy. As Stevens-
Johnson syndrome is a potentially fatal multiorgan disease with a strong etiologic link to some medications, one must
have a high index of suspicion to be able to diagnose and treat patients with SJS in time and must therefore consider
Stevens-Johnson syndrome as a potential complication of treatment. Key words: Ibuprofen, Non-steroidal anti-inflammatory drug, Stevens Johnson Syndrome, Erythema

51
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
the administration of ibuprofen, reaction in the eye impairment except ibuprofen. Renal function test was
appeared with congestion followed by redness in the eye normal. Other test for diabetes, malaria, HIV infections,
on the 5th day. hepatitis infections were normal. In the absence of
etiology of infections, other concomitant medications On physical examination, it was observed that patients
and timing of occurrence of the Stevens Johnson had multiple purpuric macular lesions on face, neck,
Syndrome, it can be inferred that it is a case of drug upper limb and lower limb.(See Figure 2) Trunk showed
induced SJS with hepatic impairment. multiple, purpuric, macular lesions with few
vesiculobullous lesions on base of purpuric macules. During the hospital administration, patient was managed
Purpuric lesions were confluent covering majority of symptomatically for pain control, skin, mouth blistering
trunk and few types of erosion present. Few erythema and ulceration. After the withdrawal of ibuprofen
multiforme (EM) form lesions were also present. In following which the lesions gradually resolved. Patient's
conjunctiva, congestion was present. Patients had symptoms began to improve after initiation of
erosion over lips with crusting with single well-defined intravenous dexamethasone and hydroxizine in
erosion over dorsum of tongue with few vesicule with no conjunction with fluid replacement as supportive
genital involvement. therapy. Corticosteroid dose was gradually tapered after
the 4th day of treatment. Ceftriaxone and metronidazole Laboratory investigations revealed patients elevated
was given to cover infections and also topical cream of level of white blood cells showed etiology of infectious
fusidic acid to cover gram positive infections. For disease after the administration in the hospital. Patients
congestion of eyes, tobramycin eye drops with lubricant had elevated level of Serum glutamate pyruvic acid
were adminstred. Xylocaine for symptomatic transferase and Serum oxaloacetate transferase which
improvement in mouth ulcer with vitamin B were showed hepa ta to tox ic i ty and fur ther wi th
administered. Patient gradually recovered and ultrasonography, intrahepatic cholestasis was confirmed. th
There were no drug which can cause the hepatic discharged on the 9 day of admission with a specific
rdFig.1: Congestion with conjunctivitis of eyes on the 3 day of admission

52
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
warning card for sensitivity to drug and with a list of cross derivatives appeared to have the greatest association with
reactive medicine to avoid such incidence in future. SJS and TEN in USA. The relative risks reported with
Discharge medication included the Discharge other NSAIDs are much lower. The risk of SJS or TEN
medications include hydroxyzine, fucidic acid cream, caused by NSAIDs is extremely low (less than 2 per 1
ciprofloxacin eye drop and acetaminophen. million users per week for oxicam derivatives, less than 1
per 1 million users per week for other NSAIDs, and 6 DISCUSSION7
cases per 1 million person-years for celecoxib). Patients' safety is paramount importance while treating
Mahboob et al had repoted 19 cases of ibuprofen induced the patients. Physicians writing prescriptions for their 11
drug eruption cases in Pakistan. . By our knowledge patients must warn them about possible side effects.
from literature search, this is the forth case report of Stevens Johnson syndrome is potentially fatal condition
adverse reaction of Stevens Johnson Syndrome due to of skin & mucus membrane but can also affect other vital 12
organs. Stevens-Johnson syndrome (SJS) associated ibuprofen in India.
with the use of nonsteroidal antiinflammatory drugs SJS/TEN is a rare and unpredictable reaction to
(Ibuprofen) is described here. Sternlieb et al reported the medication. However, the mechanism has still not been
first case report on Stevens Johnson syndrome with understood and is complex, evidence has shown various 8
hepatitis secondary to Ibuprofen in the USA in 1978. In pathological mechanism like drug specific CD8+
1984, Sterrn et reported case series of 135 cutaneous cytotoxic lymphocytes, natural killer cell activation,
reactions secondary to use of non steroidal anti- cytokines including perforin/granzyme, Fas-L and 13 inflammatory agents to NSAIDs in USA. The study Tumour Necrosis Factor (TNF) alpha. Cytokines play a
showed high incidence of fixed drug eruption secondary role in the immunopathological and molecular 9
to ibuprofen first time. mechanisms of drug-induced hypersensitivity reactions
A study with adverse reactions of SJS due to NSAIDS (HSR). A study of ibuprofen-induced SJS showed that in
revealed that of the available NSAIDs, oxicam the patient with SJS, high lymphocyte level,and high
Fig.2: Multiple purpuric macular lesions on face, neck, upper limb and lower limb in the patient

Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
cytokine secretion in the patient's sera with the high level 5. Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS,
of tumor necrosis factor alpha (TNF-alpha) as high as in Anderson T, et al. Medication use and the risk of 14
patients found to have TEN. Stevens-Johnson syndrome or toxic epidermal
Finally, the presented case reinforce that Stevens- necrolysis. N Engl J Med. 1995 .14;333(24):1600-7.
Johnson syndrome is a potentially fatal multiorgan 6. I b u p r o f e n D r u g disease with a strong etiologic link to some medications.
Information[www.nlm.nih.gov/medlineplus/druginfOne must have a high index of suspicion to be able to
o/med /a682159 .htm]diagnose and treat patients with SJS in time and must
7. Ward KE, Archambault R, Mersfelder TL. Severe therefore consider Stevens-Johnson syndrome as a
adverse sk in reac t ions to nons te ro ida l potential complication of treatment, especially when use antiinflammatory drugs:A review of the literature. of medication is questionable. Affected patients and their
Am J Health Syst Pharm 2010.1;67(3):206-13. first-degree relatives should be instructed to avoid any
identified drugs or chemicals that may be responsible. 8. Sternlieb P, Robinson RM. Stevens-Johnson
This is critical for the subsequent survival of these syndrome plus toxic hepatitis due to ibuprofen. N Y patients. Intensive treatment must also be done together State J Med. 1978;78(8):1239-43with specialist physicians, where available. Treatment
9. Stern RS, Bigby M. An expanded profile of cutaneous with steroid agents may be helpful, but this option
reactions to nonsteroidal anti-inflammatory drugs. remains controversial.
Reports to a specialty-based system for spontaneous CONSENT
reporting of adverse reactions to drugs. JAMA. 1984 Written informed consent was obtained from the patient
21;252(11):1433-7.for publication of this case report. A copy of the written
10. Nirken MH. Stevens-Johnson syndrome and toxic consent is available for review from the journal's Editor-
e p i d e r m a l n e c r o l y s i s i n in-Chief.
adults.[http://uptodateonline.com/patients/content/tREFERENCES
opic.do?topicKey=~KMM0KgcQUwSCr8z].1. Castana O., Rempelos G., Anagiotos G.,
Apostolopoulou C., Dimitrouli A., Alexakis D. 11. Mahboob A, Haroon TS. Drugs causing fixed
Stevens Johnson Syndrome: A case report. Annals of eruptions: a study of 450 cases. Int J Dermatol. 1998
Burns and Fire Disasters 2009; 22(3): 147-151. Nov;37(11):833-8
2. French LE. Toxic epidermal necrolysis and Stevens 12. Patel R, Marfatia Y. Clinical study of cutaneous drig Johnson syndrome: our current understanding.
eruptions in 200 patients. Indian Journal of Dermatol Allergol Int. 2006;55(1):9-16.
Venereol Leprol 2008; 74:803. Bastuji-Garin S, Fouchard N, Bertocchi M, et al.
13. Stevens Johnson Syndrome & Toxic Epidermal SCORTEN: a severity-of-illness score for toxic
Necrolysis[http://dermnetnz.org/reactions/sjs-epidermal necrolysis. J Invest Dermatol.
ten.html]2000;115(2):149-53.
14. Neuman M, Nicar M. Apoptosis in ibuprofen-4. Stevens Johnson Syndrome. [http://www.
induced Stevens-Johnson syndrome. Transl Res. s k i n a s s n . o rg / c a u s e s - o f - s t e v e n s - j o h n s o n -
syndrome.html] 2007 May;149(5):254-9.)
53

Indian Journal of Pharmacy Practice (ijopp) is official numbered consecutively with arabic numbers, beginning
journal of Association of Pharmaceutical Teachers of with title page, ending with the (last) page of figure
India (APTI). Indian Journal of Pharmacy Practice, a legends. The length of an Review/ Science Education
quarterly publication is devoted to publishing reviews article should not exceed 25 manuscript pages to include
and research articles in the area of Pharmacy Practice. figures, tables and references. No abbreviations or
Articles in the areas of clinical pharmacy, hospital acronyms shall be used in the Title or Abstract acronyms,
pharmacy, community pharmacy, pharmaceutical care, except for measurements. All the references, figures
pharmacovigilance, pharmacoeconomics, clinical (Fig.) and tables (Table) in the text shall be numbered
research, clinical pharmacokinetics and other related consecutively as they first appear. No sentence shall start issues can be sent for publication in ijopp. All with a numeral. Abbreviations like “&” and “etc” shall be manuscripts should be submitted in triplicate along with avoided in the paper. There shall not be any decorative 'Authorship Responsibility Undertaking', signed by all borders anywhere in the text including the title page. The the authors of the paper to, entire MS Word document with graphs and illustrations The Editor,
pasted in it shall not exceed 2 MB. Manuscripts must Indian Journal of Pharmacy Practice,
conform to the “Uniform Requirements for Manuscripts Association of Pharmaceutical Teachers of India, Submitted to Biomedical Journals” http://www.icmje.org/. H.Q.: Al-Ameen College of Pharmacy, Hosur Road, The Content of the manuscript shall be organized in the Opp. Lalbagh Main Gate, Bangalore- 560 027.following sequence and shall start on separate pages: title Authors should retain a copy of all materials submitted to
page (including author's name, affiliations and address the journal; the editor cannot accept responsibility for
loss or damage to submitted materials. for correspondence), abstract (including atleast 4 key Manuscripts will be subjected to peer review process to words), text (consisting of introduction, materials and determine their suitability for publication, provided they methods, results, discussion, conclusion and fulfilled the requirements of the journal. After the review, acknowledgements), references, figure legends, tables manuscript will be returned for revision along with and figures. Titles should be short, specific, and clear. reviewer's and /or editor's comments. One original copy Beginning with the first page of text, each page should be of the final revised manuscript should be submitted for consecutively numbered.publication within one month after receiving the For the Review Articles, the author(s) is absolutely free
comments. It is also desirable to submit the final revised to design the paper. The Abstract section is needed for
manuscript on a CD prepared in MS word version 6.0/95 review articles too. The article should not exceed 15 or a higher version. manuscript pages including figures, tables and Submission of a manuscript to ijopp for publication
references. References, figures, and legends shall follow implies that the same work has not been either
the general guidelines described below. For all other published or under consideration for publication in
Articles, the following format shall be strictly another journal.
followed.Author/s publishing results from in-vivo experiments
Title Page. The following information should appear: involving animal or humans should state whether due
title of article (A running title or short title of not more permission for conduct of these experiments was
than 50 characters), authors' name, and last name. The obtained from the relevant authorities /Ethics
author to whom all correspondence be addressed should committee/Institutional Review Board.
be denoted by an asterisk mark. Full mailing address with Manuscript preparation:pin-code numbers, phone and fax numbers, and Manuscripts should be concisely typewritten in double
functional e-mail address should be provided of the space in A4 sized sheets, only on one side with a 2 cm
author for correspondence. Names of the authors should margin on all sides. The manuscript shall be prepared in
appear as initials followed by surnames for men and one Times New Roman font using a font size of 12. Title
given-name followed by surname for women. Full names shall be in a font size 14. All section titles in the
may be given in some instances to avoid confusion. manuscript shall be in font size 12, bold face capitals.
Subtitles in each section shall be in font size 12, bold face Names should not be prefixed or suffixed by titles or
lower case followed by a colon. The pages shall be degrees.
INSTRUCTIONS TO AUTHORS -2010INDIAN JOURNAL OF PHARMACY PRACTICE (ijopp)
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
54

Abstract: The abstract is limited to 250 words, and fit in portrait form of A4 size paper, then, it can be
should describe the essential aspects of the investigation. prepared in the landscape form. Authors will be asked to
In the first sentence, the background for the work should revise tables not conforming to this standard before the
be stated; in the second sentence the specific purpose or review process is initiated. Tables should be numbered as
hypothesis shall be provided; followed sequentially by Table No.1 Title…., Table No.2 Title…. Etc. Tables
summary of methods, results and conclusion. No inserted in word document should be in tight wrapping
references should be cited. style with alignment as center.Introduction: A brief background information on what Figures, Photographs and Images: Graphs and bar
has been done in the past in this area and the importance graphs should preferably be prepared using Microsoft
of the proposed investigation shall be given. Introduction Excel and submitted as Excel graph pasted in Word.
shall end with a statement of the purpose or hypothesis of These graphs and illustrations should be drawn to
the study. approximately twice the printed size to obtain Material and Methods: This section may be divided satisfactory reproduction. into sub-sections if it facilitates better reading of the Specification of Legends/values in Graphs Font
paper. The research design, subjects, material used, and Arial, size- 10 pt, Italics- None] Diagrams made with
statistical methods should be included. Results and Indian ink on white drawing paper, cellophane sheet
discussion shall not be drawn into this section. In human or tracing paper with hand written captions or titles experimentation, ethical guidelines shall be will not be accepted. Photographs should be submitted acknowledged. only on photo-glossy paper. Photographs should bear the Results: This section may be divided into subsections if
names of the authors and the title of the paper on the back, it facilitates better reading of the paper. All results based
lightly in pencil. Alternatively photographs can also be on methods must be included. Tables, graphic material
submitted as 'jpeg/TIFF with the resolution of 600 dpi and figures shall be included as they facilitate
or more' images. Figure and Table titles and legends understanding of the results.
should be typed on a separate page with numerals Discussion: Shall start with limited background
corresponding to the illustrations. Keys to symbols, information and then proceed with the discussion of the
abbreviations, arrows, numbers or letters used in the results of the investigation in light of what has been
illustrations should not be written on the illustration itself published in the past, the limitations of the study, and
but should be clearly explained in the legend. The potential directions for future research. The figures and
complete sets of original figures must be submitted. graphs shall be cited at appropriate places.
Legends should be in the present tense (e.g., 'Illustration Conclusion: Here, the major findings of the study and shows ...'). Subjects' names must not appear on the
their usefulness shall be summarized. This paragraph figures. Labels should contrast well with the background.
should address the hypothesis or purpose stated earlier in Images should be uniform in size and magnification. the paper.Illustrations should be free of all identifying information Acknowledgments. Acknowledgments should appear
relative to the subject and institution. Written permission on a separate page.Tables. Each table should be given on a separate page. for use of all previously published illustrations must be
Each table should have a short, descriptive title and included with submission, and the source should be
numbered in the order cited in the text. Abbreviations referenced in the legends. Written permission from any
should be defined as footnotes in italics at the bottom of person recognizable in a photo is required. Legends must
each table. Tables should not duplicate data given in be double spaced, and figures are numbered in the order
the text or figures. Only MS word table format should be cited in the text. Color prints shall be submitted only if
used for preparing tables. Tables should show lines color is essential in understanding the material presented.
separating columns with those separating rows. Units of Label all pertinent findings. The quality of the printed
measurement should be abbreviated and placed below figure directly reflects the quality of the submitted figure. Figures not conforming to acceptable standards will be the column headings. Column headings or captions
returned for revision. Figures should be numbered as should not be in bold face. It is essential that all tables
have legends, which explain the contents of the table. Fig.1, Fig.2 etc. ; Figures inserted in word document
Tables should not be very large that they run more than should be in square wrapping style with horizontal
one A4 sized page. If the tables are wide which may not alignment as center.
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
55

Resolution: Drawings made with Adobe Illustrator and Please put all primary section titles in UPPER CASE
CorelDraw (IBM/DOS) generally give good results. letters (Example INTRODUCTION, MATERIALS
Drawings made in WordPerfect or Word generally have AND METHODS, RESULTS, DISCUSSION,
too low a resolution; only if made at a much higher ACKNOW-LEDGEMENT, REFERENCES) and
resolution (1016 dpi) can they be used. Files of scanned subheading in both Upper and Lower Case letters
line drawings are acceptable if done at a minimum of (Italics). Do not number your subtitles (for example, 1.0
1016 dpi. For scanned halftone figures a resolution of 300 Introduction; 2.0 Background; 2.1.1 are not acceptable).
dpi is sufficient. Scanned figures cannot be enlarged, but Do not use the tab key to indent blocks of text such as
only reduced. Figures/Images should be submitted as paragraphs of quotes or lists because the page layout
photographic quality scanned prints, and if possible program overrides your left margin with its own, and the
attach an electronic version (TIFF/ JPEG). tabs end up in mid-sentence.Chemical terminology - The chemical nomenclature References
Literature citations in the text must be indicated by used must be in accordance with that used in the chemical Arabic numerals in superscript. Each reference abstracts.
Symbols and abbreviations - Unless specified separately in the order it appears in the text. The
otherwise, all temperatures are understood to be in references should be cited at the end of the manuscript in
degrees centigrade and need not be followed by the letter the order of their appearance in the text. In case of formal
'C'. Abbreviations should be those well known in acceptance of any article for publication, such articles
scientific literature. In vitro, in vivo, in situ, ex vivo, ad can be cited in the reference as “in press”, listing all author's involved. References should strictly adhere to libitum, et al. and so on are two words each and should be Vancouver style of citing references.written in italics. None of the above is a hyphenated Format: Author(s) of article (surname initials). Title of word. All foreign language (other than English) names article. Journal title abbreviated Year of publication; and words shall be in italics as a general rule.volume number (issue number):page numbers. General Guidelines for units and symbols - The use of Standard journal article (If more than six authors, the the International System of Units (SI) is recommended. first three shall be listed followed by et al.) You CH, Lee For meter (m), gram (g), kilogram (kg), second (s), KY, Chey WY, Menguy R. Electrogastrographic study of minute (m), hour (h), mole (mol), liter (l), milliliter (ml), patients with unexplained nausea, bloating and vomiting. microliter (µl). No pluralization of symbols is followed. Gastroenterology 1980;79:311-4.There shall be one character spacing between number Books and other monographsand symbol. A zero has to be used before a decimal. Format:Author(s) of book (surname initials). Title of
Decimal numbers shall be used instead of fractions.book. Edition. Place of publication: Publisher; Year of Biological nomenclature - Names of plants, animals and publication.bacteria should be in italics.Personal author(s)Enzyme nomenclature - The trivial names Eisen HN. Immunology: an introduction to molecular
recommended by the IUPAC-IUB Commission should and cellular principles of the immune response. 5th ed.
be used. When the enzyme is the main subject of a paper, New York: Harper and Row; 1974.
its code number and systematic name should be stated at Editor, compiler, as authorits first citation in the paper. Dausser J, Colombani J, editors. Histocompatibility Spelling - These should be as in the Concise Oxford testing 1972. Copenhagen: Munksgaard; 1973.Dictionary of Current English. Organisation as author and publisherPAGE LAYOUT GUIDELINES Indian Journal of Institute of Medicine (US). Looking at the future of the Pharmacy Practice Medicaid program. Washington: The Institute; 1992.___________________________________________ Conference proceedingsPage size Letter Portrait 8.5” X 11.0”
Kimura J, Shibasaki H, editors. Recent advances in Margins All Margins, 1”Page numbers Numbered as per the assigned page clinical neurophysiology. Proceedings of the 10th /Absolutely no break or Missed sectionsIndent None, Absolutely, No Tab International Congress of EMG and Clinical Footer / Headers None
Neurophysiology; 1995 Oct 15-19; Kyoto, Japan. Title 14pt Times New Roman, bold, centered followed by a single blank line. Amsterdam: Elsevier; 1996.Text 12pt Times New Roman, full
Dissertation justification1.5 line spacing between paragraph. No indentation Kaplan SJ. Post-hospital home health care: the elderly's Tables At the end of context with rows and columns active; tables should have individual rows and columns for access and utilization [dissertation]. St. Louis (MO):
each value expressed. All text should be fully justified. Washington Univ.; 1995.
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
56

Patent Develop Ind Pharm)
Larsen CE, Trip R, Johnson CR, inventors; Novoste Helvitica Chimica Acta- (Helv Chim Acta)
Corporation, assignee. Methods for procedures related to Indian Journal of Medical Sciences- (Indian J Med Sci)
the electrophysiology of the heart. US patent 5529 067. Indian Journal of Pharmaceutical Sciences- (Indian J
1995 Jun 25. Pharm Sci)
Chapter or article in a book Journal of the American Chemical Society, The- (J Amer
Format: Author(s) of chapter (surname initials). Title of Chem Soc)
chapter. In: Editor(s) name, editors. Title of book. Place Journal of Biological Chemistry- (J Biol Chem)
of publication: Publisher; Year of publication. page Journal of Organic Chemistry, The- (J Org Chem)
numbers. Journal of Pharmacology and Experimental
Electronic journal article Therapeutics- (J Pharmacol Exp Ther)
Morse SS. Factors in the emergence of infectious New England Journal of Medicine- (N Engl J Med)diseases. Emerg Infec Dis [serial online] 1995Jan-Mar Pharmaceutical Journal, The (Pharm J)[cited 1996 Jun 5];1(1):[24 screens]. Available from: Pharmacologica lResearch Communica t ions- URL: http://www.cdc.gov/ ncidod/EID/eid.htm (Pharmacol Res Commun)World Wide Web AUTHOR's CHECKLIST FOR SENDING PROOFS Format: Author/editor (surname initials). Title [online]. TO EDITORIAL OFFICEYear [cited year month day]. Available from: URL: In order to maintain quality and consistency in Indian World Wide Web page McCook A. Pre-diabetic Journal of Pharmacy Practice, we ask you to perform the Condition Linked to Memory Loss [online]. 2003 [cited following items prior to submitting your final proof for 2003 Feb 7]. Available from: URL: http:// publication:www.nlm.nih.gov/medlineplus/news/fullstory_11531
?Include the original, hard copy of Author's .html
Transfer of Copyright signed by each authorAbbreviations for Journals For More information on
?Thoroughly check the article for typographic errors, medline indexed journals : Download list of medline
format errors, grammatical errors, in particular: journals: ftp://ftp.ncbi.nih.gov/pubmed/J_Medline.zip
spelling of names, affiliations, any symbols, American Journal of Pharmacy- (Amer J Pharm)
equations in the context, etc.Analytical Chemistry- (Anal Chem)
?Provide graphs and figures in excel format, Pictures British Journal of Pharmacology and Chemotherapy- are required as high resolution images (300 dpi).(Brit J Pharmacol)
?Provide laser printed hard copies of all figures and Canadian Journal of Pharmaceutical Sciences- (Can J
graphics in black and white or scanned copies can Pharm Sci)
also be sent to [email protected] Pharmacokinetics- (Clin Pharmacokinet)
Drug Development and Industrial Pharmacy- (Drug ?Submit a proof corrected with RED INK ONLY.
Send the Corrected Proof, Copyright Transfer Form, with covering letter in a single envelope to the Following AddressAuthors are required to send their contributions or manuscripts through post or courier services.
Dr. Shobha Rani R HiremathEditor, Indian Journal of Pharmacy Practice (ijopp).C/o. Association of Pharmaceutical Teachers of India (APTI),H.Q: Al-Ameen College of Pharmacy,Opp. Lalbagh Main gate, Hosur Road, Bangalore 560 027, Karnataka, INDIA.
All enquiries can be made through e-mail: [email protected]
Indian J. Pharm. Pract. 3(2), Apr-Jun, 2010
57





![Characterising malaria connectivity using malaria ......Arucial and legitimate concern of malaria control pro-grammes is the threat of malaria importation˜[1].It has long been acknowledged](https://img.pdfslide.net/doc/110x75/5f64a26f577ec557b52b4778/characterising-malaria-connectivity-using-malaria-arucial-and-legitimate.jpg)






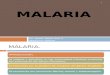









![NormaTecnica Malaria VersionFinal Set[1]](https://img.pdfslide.net/doc/110x75/5572004449795991699f1e24/normatecnica-malaria-versionfinal-set1.jpg)
![Manual Malaria Ultima 200209[1]](https://img.pdfslide.net/doc/110x75/5572003349795991699efe48/manual-malaria-ultima-2002091.jpg)