Embed Size (px)
Citation preview

1
New inspection programme for CQC11 February 2015
KCHA 2015 Conference
Chris Day

2
Our purpose and role
Our purposeWe make sure health and social care services provide people with safe, effective, compassionate, high-quality care and we encourage care services to improve
Our roleWe monitor, inspect and regulate services to make sure they meet fundamental standards of quality and safety and we publish what we find, including performance ratings to help people choose care
We will be a strong, independent, expert inspectorate that is always on the side of people who use services

The landscape of care
Care homes
•565,000 residents
•165,000 going into care per year
•39,000 people with learning disabilities in residential care
•18,000 in a care home or care in their own home with no kith or kin
NHS hospitals
•90 million outpatient appointments / year
•11 million inpatients / year
•18 million A&E attendances
•5 million emergency admissions / year
•600k maternity users
•42,000 detained and treated against their will
Home-care
700,000 people receiving home-care support per year
General public
53 million (35 million adults)
Dentists
•22 million on a dentist list
•15 million NHS
•7 million private
Private hospital
1.4 million people receive treatment in a private hospital / year
GP practices
•52 million registered with a GP
•150m appointments / year
Health & social care staff
•1.7m NHS staff
•1.5m in adult social care
NB There is overlap between our different audiences – none are wholly distinct from the others
Stroke 1m Diabetes 3m Arthritis 8.5m Cancer 2m Dementia 0.7m25% by 2020 67% by 2025 100% by 2030 100% by 2032 100% by 2040

4
Independent of politics and the system
Covers all sectors
Clinically driven with expert teams, no guarantees
Evidence-based judgement, not regulatory compliance
Highlight excellence and expose poor care with transparent ratings
Always on the side of people who use services
Critical friend
Consistent and fair
What kind of regulator?

5
Recent facts and figures

6
Our new approach

Timeline
January 2014•First ‘wave’ of inspections of mental health, community health, and out of hours primary care•First ratings published for NHS acute trusts
October 2013•First ‘wave’ of NHS acute trusts•We published Intelligent Monitoring for all NHS acute trusts•Plans for ASC, GPs, mental health, and community health
April 2014•Regulation of NHS acute trusts now using new approach•First ‘wave’ of inspections of GP practices and adult social care•Regulatory handbooks published for consultation for all major providers
July/August 2014•First ‘wave’ of inspections of ambulance services•Guidance on legal regulations underpinning our work published for consultation•Plans for dentists and substance misuse services
October 2014•Regulation of adult social care providers using new approach – first ratings•Regulation of GPs using new approach•Regulation of community and mental health – new approach
Our New Approach
January 2015•Regulation of ambulances using new approach•First ‘wave’ of inspections of prison healthcare services, dentists, substance misuse services and independent doctors
April 2015•Regulation of all health and care providers using new model

8
What are we doing differently?
Larger inspection teams including specialist inspectors, clinical experts, and Experts by Experience
Intelligent monitoring to decide when, where and what to inspect
Inspections will focus on five key questions about services
We have developed services/groups and pathways that we focus on in each sector
KLOEs (key lines of enquiry) form the overall framework for a consistent and comprehensive approach
Ratings compare services and highlight where care is outstanding, good, requires improvement or inadequate

99
Our new approach
We ask these questions of all services:
Is it safe?Is it effective?Is it responsive?Is it caring?Is it well-led?

10
Four point scale
High level characteristics of each rating level
Innovative, creative, constantly striving to improve, open and transparent
Consistent level of service people have a right to expect, robust arrangements in place for when things do go wrong
May have elements of good practice but inconsistent, potential or actual risk, inconsistent responses when things go wrong
Severe harm has or is likely to occur, shortfalls in practice, ineffective or no action taken to put things right or improve

11
First ASC inspections and ratings
Outstanding
Good
Requires improvement
Inadequate
4
370
144
31As at 19January2015

12
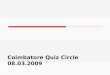
Q4 ratings 2014: by key question
Source: CQC ratings published October to December 2014

13
‘We were not assured that there were always sufficient staff available to meet people’s individual needs’ (Safe)
‘The provider had not taken steps to maintain and provide a safe environment for people to live in’ (Safe)
‘There were restrictions imposed on people that did not consider their ability to make individual decisions for themselves’ (Safe)
‘People were unoccupied for long parts of the day’ (Responsive)
‘People were not always supported to receive adequate nutrition and hydration’ (Effective)
‘Staff did not understand their responsibilities under the Mental Capacity Act 2005’ (Effective)
‘Staff felt they were not listened to and were blamed when things went wrong’ (Well-led)
Rating inadequate – sample findings so far

14
‘People and staff had high expectations of what each person could achieve and showed determination to succeed’ (Caring)
‘Staff skills, hobbies and interests were matched with the interests of the people they supported’ (Caring)
‘The management team provided strong leadership and led by example’ (Well-led)
‘Staff were encouraged to challenge and question practice and supported to change things’ (Well-led)
‘The environment had been arranged to promote people’s wellbeing. Staff worked creatively to best use the space to support people’s independence and personal identity’ (Effective)
Rating outstanding – sample findings so far

The importance of leadership: being well-led drives up quality
15
“It’s the leaders in organisations who really make a difference to the cultures of organisations – by what they attend to; what they value; what they monitor and what they model in their behaviours. The challenge for us is how can we ensure we have leadership, which ensures that there is a focus on the vision of providing high-quality, continually improving, and compassionate care at every level of the organisation? Not just in the vision or mission statements but in the behaviours throughout the organisation.”
Michael West, The King’s Fund

16
Have your say
www.cqc.org.uk/content/special-measures-adult-social-care-comment-our-proposals Until 30 Jan
www.cqc.org.uk/ascmarketoversight From 23 Jan to 20 Feb
New requirement to display CQC ratings www.cqc.org.uk From 26 Jan for 4 weeks
@CareQualityComm
#tellcqc

Join our team
Inspectors and Registration InspectorsPermanent and secondment opportunities now available - please email:[email protected]
Specialist Advisors If you have specialist experience in Adult Social Care you could assist us in inspections – please email:[email protected]
Experts by Experience CQC is committed to hearing the voices of people who use services. Our new approach uses experts by experience. Contact us here:[email protected]

www.cqc.org.uk
Chris DayDirector of Engagement
18
Thank you