Embed Size (px)
Citation preview

1
Toxicology,Alcohol & Drug Abuse
2008

2
Types of Toxicological Emergencies
Unintentional• Dosage errors• Idiosyncratic reactions• Childhood poisoning• Environmental exposure• Occupational exposure• Neglect and exposure

3
Intentional poisoning/overdose• Chemical warfare
• Assault/homicide
• Suicide attempts

4
Use of poison control centers Oregon Poison Control
1-800-452-7165 Evaluation of the poisoned patient

5
Scene Size-up
Where are you? Who’s around you? Is there any potential danger? Any evidence of pill bottles, used
needles, etc.

6
History
• Provides a working diagnosis; notoriously unreliable
• What - samples• How much• How• When• Why• What else

7
Physical exam Vitals
• Airway• Stridor
• Snoring
• Vomitus
• Gag reflex
• Risk of aspiration
8
• Breathing evaluation• Baseline RR
• Quality of respirations
–Shallow; need early ventilatory support
–Deep; underlying hypoxemia or metabolic acidosis
• Early - noncardiogenic pulmonary edema
• Later - ARDS

9
• Circulation• Baseline pulse rate and BP
–Hypotension common–Hypertension occasionally; serious ie
CVA
• ECG monitoring–Tachyarrhythmias common; not
usually serious perfusion problem–Bradyarrhythmias uncommon; more
serious underlying metabolic problem

10
Temperature• Baseline temp.
• Hypothermia and hyperthermia frequently accompany poisons

11
Neuro complications• Altered level of consciousness
(AMS) frequent• Seizures one of most common• Mild drowsiness• Agitation• Hallucinations• Confused, combative• Coma• Medullary depression• Cardiopulmonary depression• Death

12
Underlying disease states• Asthma, COPD etc. increased risk for resp.
compromise
• Underlying cardiac disease increased risk for severe arrhythmias.

13
Supportive care
• Prevent or limit respiratory, cardiac, neurologic complications
• Oxygen,
• IV
• ECG

14
Respiratory complications• Airway protection• ET or NT intubation• Bronchodilator therapy prn• Positive pressure ventilation prn

15
Cardiovascular complications
• Appropriate antiarrhythmics
• Atropine
• Pacing
• Fluid challenge for hypotension
• Vasodilators for hypertension

16
Neurologic complications
• Anticonvulsants; diazepam/versed prn
• Chemical restraints only compounds
intoxication and may precipitate
catastrophic cardiopulmonary
complications

17
Routes of absorption
• Ingestion
• Inhalation
• Injection
• Absorption
18
Ingestion
Most common route• Assessment findings
• What?• When?• Quantity?• Alcohol?• Self-treatment?• Psychiatric care?• Weight?

19
Physical examination
• Skin
• Eyes
• Mouth
• Chest
• Circulation
• Abdomen

20
General management considerations
• Prevent Aspiration • Intubation/RSI?
• Fluids & Drugs• GI decontamination
• Syrup of Ipecac–Reduces absorption by @ 30%–Interferes with activated charcoal
• Gastric lavage–36-40 Fr. orogastric tube–After 1-2 hrs post ingestion
questionable

21
• Activated charcoal
• Agent of choice
• Adsorbs molecules of chemicals on its surface
• Reduces absorption by @ 50%
• Dose 1 g/kg

22
Cathartics• Sorbitol, mag sulfate, mag citrate• Speed up motility• Studies show they don’t positively
affect patient outcome• Liquid stools• Dehydration, electrolyte imbalances
occur• Administration of activated charcoal
20-30 min. prior to gastric lavage doubles effectiveness
23
How do people poison themselves?

24
They Inhale it
• Paint, other hydrocarbons• Carbon monoxide• Ammonia• Chlorine• Freon• Toxic vapors, fumes, aerosols• Mace, mustard gas

25
What do they look like? Primarily respiratory
• Tachypnea, cough, hoarseness, stridor, dyspnea, retractions, wheezing, chest pain or tightness, rales, rhonchi
Cardiac:• Dysrhythmias
CNS• Dizziness, H/A, confusion, seizures,
hallucinations, coma

Carbon Monoxide
Inadvertant• Faulty furnace• Indoor heating source
Purposeful• Suicide

Poisonous Gases
Oxygen robbing Chlorine Warfare
• Chlorine• Mustard gas• Bromine

28
29
Now what?
Be safe! Remove patient from environment Exam Provide supportive care Contact Poison Control and follow
directions
30
They inject it
• IV drug abuse – more later
• Venomous bites and stings• Bees, hornets, yellow jackets, wasps,
ants (only females)
• Spiders, ticks, other arachnids; scorpions
• Snakes
• Marine animals; jelly fish, stingrays, anemones, coral, fish
31
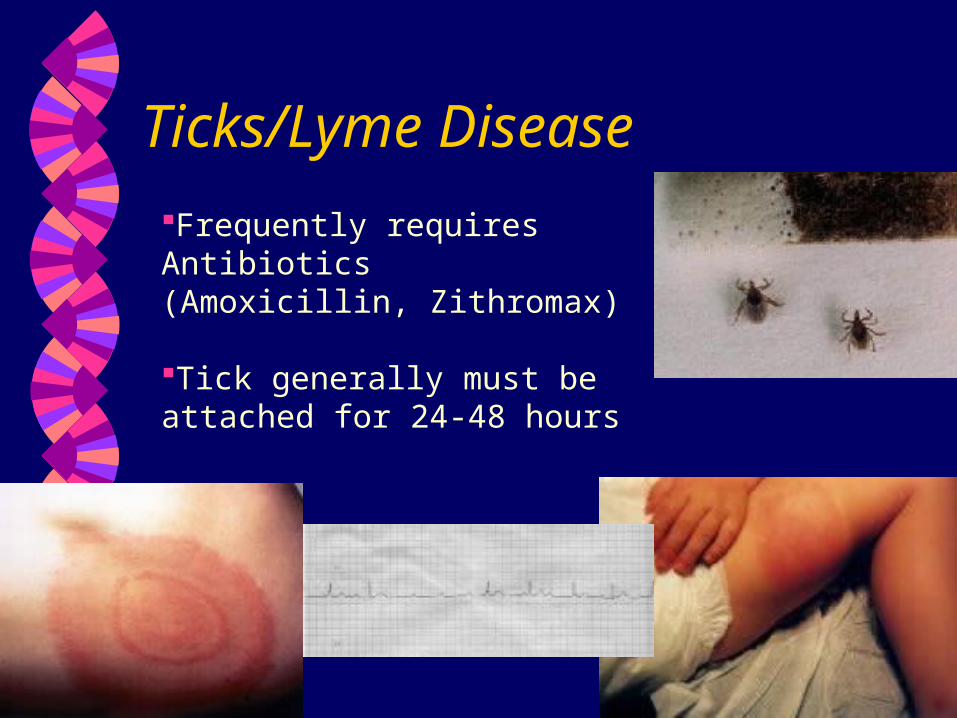
Ticks/Lyme Disease
Frequently requires Antibiotics (Amoxicillin, Zithromax)
Tick generally must be attached for 24-48 hours

32
Results in immediate & delayed reactions• Immediate reaction
• Rash• Fever• Malaise• Fatigue• H/A• Muscle & joint aches• Sore throat• Sinus infection

33
Delayed reaction• Chronic malaise/fatigue• Muscle pain/joint pain with/without arthritis• Neuropathy• Tremor• Bell’s palsy• Meningitis• Vision problems (double vision, photophobia)• Vestibular problems• Seizures• Cardiac symptoms• N/V• Immune suppression

34
Hymenoptera (Bee stings, Wasp stings, Ants)• Bumblebees, Sweat bees, Honeybees;
Hornets, Yellow jackets; Fire ants, Harvester ants
• Type of reaction• Local; • Toxic; 10 or more stings
– N/V/D, light-headedness, syncope, H/A, fever, drowsiness, muscle spasms, edema, seizures
– Sx subside w/in 48 hrs

35
Systemic/anaphylactic:• The shorter the onset, more severe the
reaction• Initial sx: itching eyes, facial flushing,
generalized urticaria, dry cough• Sx intensify; chest or throat constriction,
wheezing, dyspnea, cyanosis, abdominal cramps, N/V/D, vertigo, chills, fever, shock, loss of consciousness
• Reaction can be fatal in 30 min.
Bees and Bugs

36
Delayed reaction• Serum-sickness-like sx; fever, malaise, H/A,
urticaria, lymphadenopathy appears 10-14 days later.
Dx: difficult• Honeybees; leaves it’s stinger with venom sac
attached• Yellow Jackets: nest in ground • Wasps: under eaves or windowsills • Southern US Fire Ants; groupings of 3-4
stings and pustules
Bees and Bugs

37
Tx:• Scrape honeybees stinger out; don’t
squeeze; remove quickly
• Wash sting sites with soap and water
• Ice packs
• Benadryl, Prednisone
• Epinephrine 1:1000 0.3 - 0.5 mg sq IF SYSTEMIC
Bees and Bugs
38
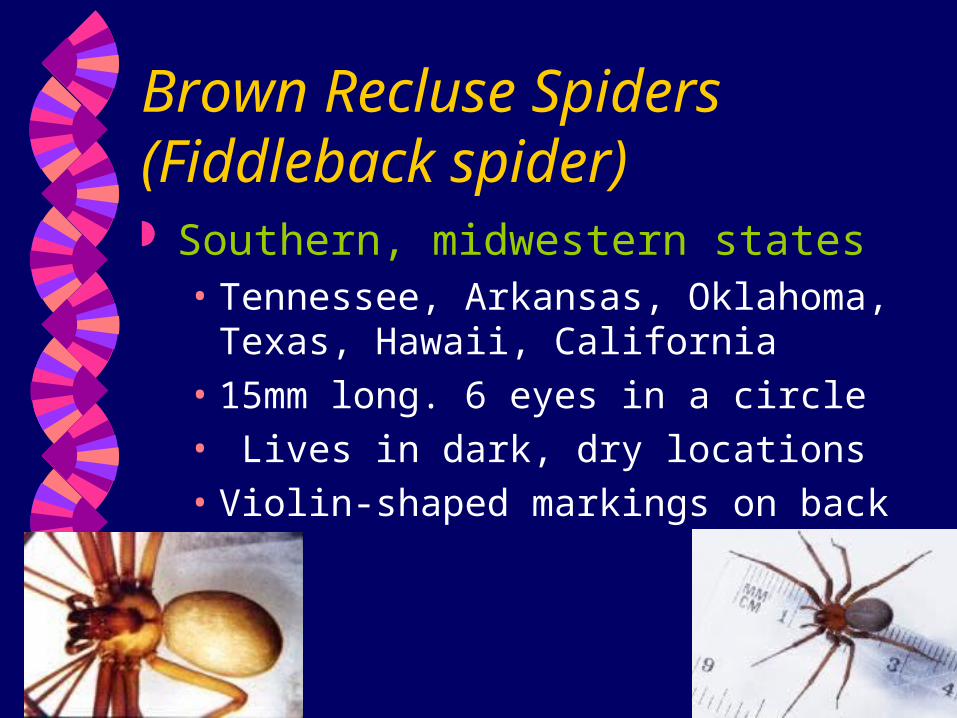
Brown Recluse Spiders (Fiddleback spider) Southern, midwestern states
• Tennessee, Arkansas, Oklahoma, Texas, Hawaii, California
• 15mm long. 6 eyes in a circle• Lives in dark, dry locations• Violin-shaped markings on back

39
Does it hurt?
Usually painless Bites occur at night Local reaction
• Initially, small erythematous macule surrounded by a white ring
• Over next 8 hours, localized pain, redness, swelling
• Tissue necrosis over days > weeks
Chills, fever, N/V, joint pain, DIC Tx: Diphenhydramine; supportive

40
41
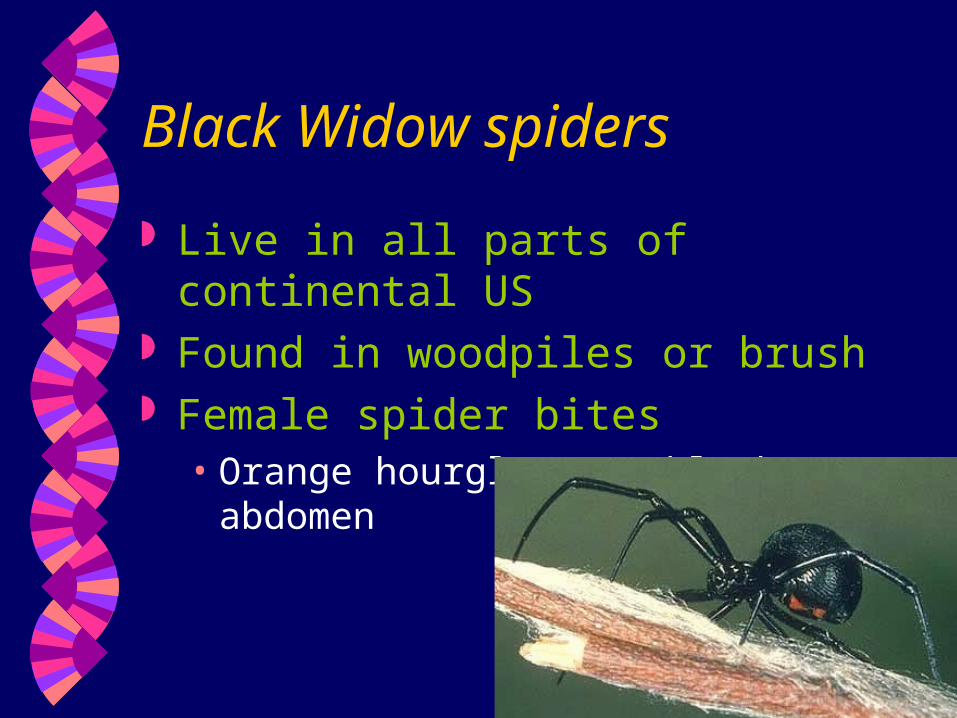
Black Widow spiders
Live in all parts of continental US Found in woodpiles or brush Female spider bites
• Orange hourglass on black abdomen

42
Does it hurt? Immediate localized pain, redness, swelling. Progressive muscle spasms of all large muscle
groups can occur N/V, sweating, seizures, paralysis, decreased
level of consciousness. Management: Supportive care;
• Consider Diazepam• 2 – 10 mg IVP
• or Calcium gluconate• 0.1 – 0.2 mg/kg of 10% solution.
• Monitor B/P• Antivenin is available

43
Scorpion stings All species can sting, =
localized pain Only bark scorpion has
caused fatalities• Mostly in Arizona,
California, Nevada, New Mexico, Texas.
• Move mostly at night• Venom stored in bulb at
end of tail

44
Does it hurt? Venom acts on nervous system
• Burning, tingling effect • Gradually progresses to numbness.
Systemic effects • Slurred speech, restlessness• Hyperactivity in 80% of children• Muscle twitching, seizures• Salivation, abdominal cramping, N/V
Management: Supportive• Apply constricting band above wound site –
watch band – occludes lymphatic flow only• Avoid analgesics; may increase toxicity

45
Snakebite• 8000 bites/yr - mortality is
@ 50/yr• N. Carolina has highest %• Peak months July, August
6am - 9 pm

46
Pit Vipers
Cottonmouth, rattlesnake, copperhead• Indentation 1/2-way between eye and
nostril• Hollow, retractable fangs• Vertical pupils• Triangular head

47
Venom contains enzymes that may destroy proteins, other tissue components; destroys RBCs, affects blood clotting
Death from shock possible in 30 minutes • Most occur 6-30 hours
Pit Vipers (cont.)

48
S/S: Fang marks, swelling and pain• Weakness, dizziness, faintness• Sweating/chills• Thirst, N/V, Diarrhea, • Tachycardia, hypotension• Bloody urine
Tx: Keep pt. Supine• Immobilize limb• Maintain extremity in neutral position• DO NOT apply constricting bands, Ice, etc.
Pit Vipers (cont.)

49
Coral snakes Distinct pattern of red
and black bands wider than interspaced yellow rings
“Red on yellow, kill a fellow”/coral snake
“Red on black, venom lack”/harmless snake
•Venom•Affects coagulation•Affects endothelium of vessels•Paralyzes activity of white blood cells•Neurotoxins A & B affect nervous system; esp. cardiorespiratory centers

50
May be NO effects for 12-24 hours
• Localized numbness, weakness, drowsiness
• Ataxia, slurred speech, excessive salivation
• Paralysis of tongue, larynx
• Drooping eyelids, double vision, dilated pupils
• Abdominal pain, N/V
• Hypotension, Respiratory failure
• Seizures
Coral Snakes (cont.)

51
Size of victim important; condition of victim will seriously affect outcome
Location very important; bites on head and trunk 2-3x more dangerous; bites on upper extremities more serious than lower.
Coral Snakes (cont.)

52
Tx:• Wash wound with copious amounts of water• Apply compression bandage, keep extremity
at level of heart• Immmobilize limb• Transport for antivenin• Do NOT apply ice, cold pack, freon sprays,
or incise wound
Coral Snakes (cont.)
53
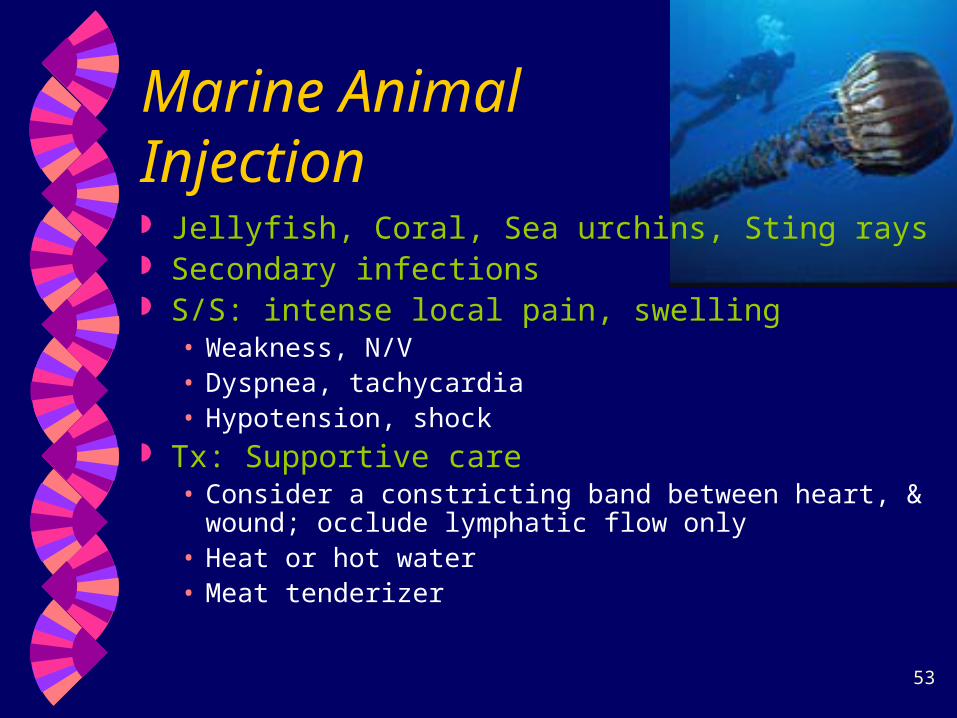
Marine Animal Injection Jellyfish, Coral, Sea urchins, Sting rays Secondary infections S/S: intense local pain, swelling
• Weakness, N/V• Dyspnea, tachycardia• Hypotension, shock
Tx: Supportive care• Consider a constricting band between heart, & wound;
occlude lymphatic flow only• Heat or hot water• Meat tenderizer

54
Poisoning By Absorption
Surface absorption
• Poisonous plants; ivy, sumac, oak
• Organophosphates

55
Now What? Management considerations
• Remove patient from environment• Wear protective clothing• Remove pt. clothing• Initiate supportive measures• Contact poison control• Soap and water• Decontaminate eyes with 15-30 min. Water
flush• Supportive care

56
Cholinergics
Pesticides (organophosphates, carbamates)
Nerve agents (sarin, Soman)

57
Findings• SLUDGE• Headache, Dizziness, Weakness, Nausea• Bradycardia, wheezing, bronchoconstriction,
myosis, coma, convulsions, diaphoresis
Management• Decontamination• Airway and ventilation
• Aggressive airway management
• Circulation
Cholinergics (cont.)
58
• Pharmacological• Atropine 2 – 5 mg IV q 15-30 min. until vitals
improve• Pralidoxime chloride (2-PAM)• Diazepam 2 – 10 mg IV for seizure control• Activated charcoal – if ingested & gag reflex
intact
• Transport considerations• Protect self • Notify receiving hospital• May require decontamination outside ED
Cholinergics (cont.)

59
Caustic substances Acids, alkalis
• 12,000 exposures/yr• 150 major complications/deaths
• Plumbing liquids• Cause tissue coagulation, necrosis• S/S - Acids: pH <2
• Eschar at burn site• Local burns to mouth, throat• Esophagus usually not damaged• Stomach lining injured• Immediate, severe pain• Acidemia

60
Alkali's: pH > 12.5• Induce liquefaction necrosis• Pain often delayed• Cause perforation, bleeding,
inflammation of central chest structures• W/in 2-3 days, complete loss of
protective mucosal tissue• S/S:
• Facial burns, pain in lips, tongue, throat, gums
• Drooling, trouble swallowing• Hoarseness, stridor, SOB• shock

61
Tx:• Aggressive, rapid
• Prevent injury to rescuers
• Airway management critical
• Cricothyrotomy
• Don’t use activated charcoal
• Rapid transport

62
Hydrofluoric Acid
Used to etch glass Extremely toxic Penetrates deeply into tissues; inactivated only
by contact with calcium; settles in tissues as salt• Causes total disruption of cell functioning, bone
destruction S/S: burning at site of contact, SOB, confusion,
palpitations, muscle cramps Tx: Supportive: Immerse affected limb in ice
water with Mag. Sulfate or calcium salts

63
Hydrocarbons Organic compounds;
• Kerosene, turpentine, mineral oil, chloroform, etc.• Lighter fluid, paint, glue, lubricants, solvents,
aerosol propellants.
S/S:• Burns, wheezing, dyspnea, slurred speech, ataxia,
obtundation• Foot and wrist drop with numbness, tingling• Cardiac dysrhythmias
Tx: Rarely serious – call poison control
64
Tricyclic antidepressants Narrow therapeutic index
• Amitrriptyline, Elavil, amoxapine, clomipramine, doxepin, imipramine, nortriptyline
S/S: dry mouth, blurred vision, urinary retention, constipation, confusion, hallucinations, hyperthermia, respiratory depression, seizures, tachycardia, hypotension, heart block, wide QRS, Torsades de pointes
Tx: Sodium Bicarbonate, 1 mEq/kg

65
MAO Inhibitors
Atapryl, Eldepryl Relatively unpopular
• Narrow therapeutic index• Serious interactions with red wine, cheese
Symptoms may not appear for up to 6 hours• Headache, agitation, restlessness, tremor• Nausea, palpitations, tachycardia, hypertension,
hyperthermia, bradycardia, hypotension, coma, death
No antidote available; tx life-threatening sx.

66
Hallucinogens
LSD, PCP, peyote, mushrooms, jimson weed, mescaline• “Psychedelic” - visual or tactile
PCP• Ketamine still used• Powdered or solution; added to tobacco or
marijuana• Onset in 2-5 min.; Peak effect in 15 min.• Elimination half-life about 7 h - 3 days.
67
LSD• Blotter acid, sugar cubes, gelatin• Sx in 1/2 - 1 hr; peak in 2 hrs (paranoia may
occur), acute psychosis may persist for days
68
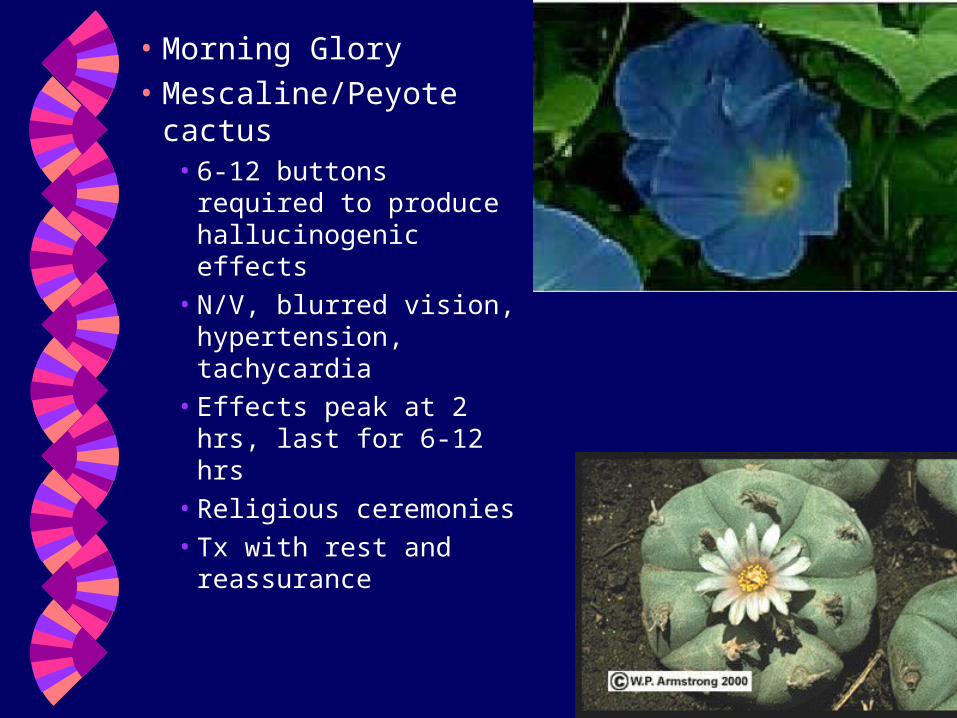
• Morning Glory• Mescaline/Peyote
cactus• 6-12 buttons required
to produce hallucinogenic effects
• N/V, blurred vision, hypertension, tachycardia
• Effects peak at 2 hrs, last for 6-12 hrs
• Religious ceremonies• Tx with rest and
reassurance

69
Mushrooms; psilocybin or ibotenic acid- magic mushrooms
• Common in US; pacific NW, texas, florida,
hawaii
• Religious ceremonies since aztec
• Eaten raw, brewed in soup or tea, or dried
• GI discomfort in 15-30 min. N/V
• Effects last from 4-12 hrs
70
Nutmeg; common in foods and herbal remedies• Myristicin is major
component• 10-50 g of fresh nutmeg
(2-9 whole nutmegs)• Sx in 3-6 hrs; N/V,
abdominal pain• Cold extremities with
weak pulses shallow respirations; sx resolve in 24 hr with supportive care

71
Designer amphetamines• Adam, Eve, Ecstasy
• Effects are drug and dose dependent
• Severe psychomotor agitation
• Disorders of thought process
• Hypertension, seizures, DIC, ARDS, death
• Management supportive

72
Marijuana• Cannabis sativa; marijuana and
hashish• Medicinal qualities in china > 4000
years ago• Today; glaucoma and chronic pain• Most commonly used illicit substance
after alcohol and tobacco• THC levels peak about 8 min after
inhalation, and 45 min. after ingestion. Effects last 2-6 hrs.

73

74
Narcotics Heroin, methadone,
morphine, codeine, meperidine, hydromorphone (Dilaudid), hydrocodone (Percodan)• Street heroin cut with
quinine, lactose, sucrose, mannitol, talc, procaine, baking soda.
• Effects include drowsiness, euphoria, miosis, decreased respiration, N/V, respiratory arrest

75

76
Withdrawal
• Piloerection, lacrimation, yawning,
rhinorrhea, sweating, nasal stuffiness,
myalgia, vomiting, abdominal
cramping, diarrhea, irritable,
hyperactive, confused

77
Narcotic overdose• Cardinal findings; pinpoint pupils,
hypoventilation Tx: Airway, ventilation, circulation Naloxone, 0.4-2.0 mg/0.01 mg/kg in
child, SQ, IM, IV, ET; effective in 1-2 min. • Naloxone acts as antagonist at opiate
receptor sites• Overdose often mixed• Serum half-life of Narcan is 1 hr with
action duration of 2-3 hr. (methadone half-life 72 hr).

78
Complications of narcotic abuse
• Skin ulcers or lesions
• nonpitting edema of extremities
• Infection
• Abscesses, Cellulitis, Thrombophlebitis
• Endocarditis
• Malaria (1929)
• Tetanus (1876) esp. female, subcu
injectors

79
• Hepatic complications; most common• GI complications
• Ilius• Fecal impaction
• CNS complications• Meningitis• Spinal abscess
80
Cocaine Most common cause of drug related
deaths• Plant alkaloid found in coca plant. Leaves
are crushed with a hydrocarbon solvent followed by extraction of alkaloid with sulfuric acid
• Smoked, snorted, or injected• Crack is almost pure cocaine vaporizes at
high temp.• Absorbed from all sites; mucous
membranes, GI tract, respiratory tree.

81
Cocaine
Smoked, injected, snorted, swallowed Intensity & duration depends on route 1997 – 1.5 million Americans use Drug most frequently involved in ED visits Often used with Valium, Ativan, Heroin as
upper/downer combo Adolescents combine Cocaine, Marijuana,
Alcohol

82
Short-term effects
Pleasure Increased alertness Paranoia Vasoconstriction Myocardial damage Dysrhythmias Death

83
Long term effects Severe
depression Loss of energy Damage to
• Heart• Lung• Brain• Kidneys

84

85
86
• Intranasal admin peak effect in 1/2 hr• GI peak effect in 90 min.• IV and inhalation peak at 30 seconds to 2
min.• Tachycardia, hypertension, hyperthermia,
agitation, seizures are common.
Cocaine (cont.)

87
AMI common; onset immediate > 24 hr.• Coronary artery spasm, thrombosis, atrial and
ventricular arrhythmias, aortic rupture, CHF, QRS widening
Spontaneous pneumothorax and pneumomediastinum possible 2ndary to deep breath holding
CVA OB risks Renal failure
Cocaine (cont.)
88
Topical cocaine
Management• Sedation, control of hyperthermia and
seizures, fluids.
Cocaine (cont.)

89
Amphetamines & Amphetaminie-like Drugs
• Benzedrine• Dexedrine• Ritalin• Midol• Vicks inhaler• Bronkaid tabs• Alka-Seltzer plus, Allerest, Contac, Dexatrim,
Dimetapp, Novahistine tabs, Extra-strength Sinutab, Triaminic
• Actifed, Drixoral, Novahistine, Sudafed

90
• First synthesized in 1887, but not commercially available until 1932
• Similar to epinephrine, norepinephrine Effects:
• Restlessness, hyperactivity, repetitive behavior, anorexia, sleep reduction
• Rapidly absorbed from GI tract; peak levels within 1 hr.
Amphetamines (cont.)

91
Toxicity:
• Diaphoresis, extreme restlessness,
repetitive and bizarre behavior, coma,
intracranial hemorrhage, flushing,
tachycardia, hypertension, arrhythmias, MI,
N/V/D
• Abrupt withdrawal rarely life-threatening.
Depression, increased appetite, cramps,
N/D, HA.
• Care supportive
Amphetamines (cont.)

92
Methamphetamines






80% children in foster care are Meth related

100
Barbiturates
• First introduced as sedative in 1903. Currently used to treat seizures, induction of anesthesia, treatment of ICP
• Methohexital• Phenobarbital• Secobarbital• Primadone

101
Barb. intoxication mimics alcohol intoxication. Rule of thumb; 10x hypnotic dose can produce severe toxicity.
Treatment: ET, gastric lavage, IV, diuresis, Hemodialysis
Barbiturates (cont.)

102
Benzodiazepines Commonly used for anxiety,
insomnia, seizures, Alcohol withdrawal, conscious sedation, general anesthesia.
• Xanax• Librium• Klonopin• Tranxene• Valium• Dalmane• Ativan• Versed• Halcion

103
Predominantly CNS effects, well
absorbed from GI tract. IM injection is
unpredictable
Benzodiazepines (cont.)
104
Most serious toxicity occurs in ingestion of other agents or parenteral administration.
CNS effects;• Drowsiness, dizziness, slurred speech, confusion,
ataxia, intellectual impairment. Managment:
• Dextrose, thiamine, naloxone• Do not induce vomiting• Give activated charcoal• Gastric lavage• Monitor closely
Benzodiazepines (cont.)

105
Cyanide
Potent cellular toxin; as little as 50 mg may cause death.• Extract of bitter almonds/cherry laurel leaves,
extracts of apricot, cherry, peach pits• Silver polish• Prolonged exposure to IV nitroprusside• Burning of synthetics and wool, silk, vinyl,
polyurethane
Several hours exposure (<50 ppm) can cause sx
Recovery is rapid after removal.

106
Exposure to 100 ppm may be fatal in 30 min.
Sx: • Severe dyspnea, • Loss of consc., Seizures, • Arrhythmias, • HA, • Drowsiness, • Paralysis, • Pulmonary edema,
Bright red retinal vessels, smell of bitter almonds important clues.
Tx: amyl nitrite for inhalation, 10 ml of 3% solution of sodium nitrite for IV infusion.; Give 300 mg, followed by 12.5 g of sodium thiosulfate.
107
Drug abuse• Epidemiology
• Incidence
• Morbidity/mortality
• Risk factors
• Prevention
• Psychological issues
• Psycho-social issues

108
Pathophysiology of long term drug abuse• End-organ damage
• Brain, liver, heart
• Malnutrition
• Habituation/dependence/addiction
• Tolerance
• Withdrawal syndromes
Drug abuse (cont.)
109
Alcoholism - Ethanol• Incidence
• Morbidity/mortality– 42% traffic fatalities, 69% drownings, 23%
suicides
– 100,000+ deaths/yr
• Risk factors
• Prevention
• Psychological issues
• Psycho-social issues

110
End-organ damage• Brain
• Liver
• Heart
• Bone
• Pancreas
Alcoholism (cont.)

111
Alcoholism –Clinical Manifestations
Altered Immunity Anorexia Dysrhythmias Coma Irritability and disorientation Muscle cramps Poor wound healing Seizures Tremor and ataxia

112
Malnutrition Withdrawal syndrome Wernicke’s encephalopathy (disorder
of the brain)
Alcoholism (cont.)

113
Alcoholism –Body System Disturbances
Fluid and electrolyte from diuresis
GI disorders (bleeds, esophageal varices)
Liver (cirrhosis)
Pancreatitis
Cardiac and skeletal muscle myopathy
Immune suppression
Trauma (suppressed clotting factors)

114
Prehospital concerns
Delirium Tremens (DT’s)• Treat symptomatically
• Valium/Versed• Rehydration
115
Wernicke-Korsakoff’s syndrome
• Personality; psychosis, polyneuritis,
disorientation, muttering delirium,
insomnia, illusions, hallucinations
• Classic triad; ataxia, ophthalmoplegia
(nystagmus and 6th nerve palsy), and
altered mental status; also, hypothermia,
coma, hypotension
116
Methanol
• Antifreeze, paint solvent, Sterno, gasoline additives
• Life-threat even with small amount; 30 ml of 100% methanol lethal;
• Converted in liver to formaldehyde to formate = cellular hypoxia.
• S/S: visual sx-photophobia, blurred vision, dilated pupils; CNS depression; abd. Pn; N/V; metabolic acidosis. Onset 1 hr - 72 hrs

117
Ethylene Glycol
• Colorless, oderless, sweet-tasting, nonvolatile liquid
• Detergents, paints, pharmaceuticals, polishes, antifreeze, lysol spray, coolants
• Toxicity due primarily to accumulation of toxic metabolites.
• CNS sx 1-12 hr later: Ataxia, nystagmus, seizures, hallucination, coma

118
Cardiopulmonary sx 12-72 hrs later: Tachycardia, tachypnea, mild HTN, pneumonia, pulmonary edema, cardiac failure
Renal failure w/in 24-72 hrs Tx: Gastric lavage, Alcohol, calcium
chloride
Ethylene Glycol (cont.)

119
Salicylates - aspirin (acetylsalicylic acid)
• Oil of Wintergreen (methyl salicylate)• Darvon, Percodan, Fiorinal
Directly stimulates respiratory centers
in brainstem, = respiratory alkalosis.
Causes mobilization of glycogen
stores and inhibits gluconeogenesis,
= hyperglycemia, normoglycemia,
hypoglycemia

120
S/S: • GI irritation, Upper GI bleeding, persistant
vomiting• Mixed respiratory and metabolic acidosis
• Confusion, lethargy, convulsions,
respiratory arrest, coma, brain death,
cardiac toxicity, significant hyperthermia,
pulmonary edema
Salicylates - ASA

121
Toxic doses• Peak serum levels in 18-24 hrs, although
toxic levels within 6 hours.• Therapeutic levels, salicylate mainly
cleared by hepatic metabolism• Toxic levels, renal excretion is major
route of elimination • 150-300 mg/kg = mild-moderate toxicity;
hyperpnea, vomiting, diaphoresis, tinnitus, acid/base disturbances
Salicylates - ASA

122
Tx: • Activated charcoal
• IV fluids
• D50
• Hemodialysis
Salicylates - ASA

123
Acetaminophen poisoning (APAP)• Tylenol, Datril
• Poisoning may result in fatal hepatic necrosis
• Therapeutic dose 15 mg/kg q 4-6h (children)
max daily dose 80 mg/kg
• 325-1000 mg q 4 h (adults) max daily dose 4 g
• Eliminated primarily by hepatic metabolism
• Mechanism of toxicity unclear; a highly reactive
metabolite is thought to cause hepatic necrosis
by binding to protein macromolecules

124
Toxic doses• 140 mg/kg in children• 7/5 g in adults
Toxicity:• Stage I: 1/2 - 24 h
• N/V, Anorexia, malaise, pallor, diaphoresis• Stage II: 24-48 h
• Transient clinical improvement• RUQ pain with liver enlargement, tenderness• Pancreatitis• Oliguria
Acetaminophen poisoning (APAP)

125
Toxicity: • Stage III: 72-96 h
• GI sx reappear, persist, or worsen• Jaundice• SGOT, SG
• Stage IV: 4 d - 2 weeks• Resolution or progressive hepatic failure
Acetaminophen poisoning (APAP)

Overdose guidelines Alcohol – thiamine, D50W
Cocaine – Benzodiazepines• Beta blockers absolutely contraindicated
Narcotics/opiates – naloxone
Amphetamines – benzodiazepines, haldol
Hallucinogens – benzodiazepines, haldol
Benzodiazepines – flumazenil
Barbiturates – forced diuresis, alkalinization
of urine 126

127

128

129
Bye-Bye now~