Embed Size (px)
Citation preview

SS
AT
Ab
stra
cts
1031
Survival After Proximal, Local and Distal Resection of ExtrahepaticCholangiocarcinoma: Analysis of Prognostic FactorsNiels Anthony Van Der Gaag, Jaap Kloek, Jacob de Bakker, Boudewijn Musters, Olivier R.Busch, Dirk J. Gouma, Thomas M. Van Gulik
Background/Aim: Differentiation between proximal, mid and distal extrahepatic cholangi-ocarcinoma (CCA) is primarily based on surgical approach, rather than differences in tumorbiology. The aim of the current study was to compare disease specific survival (DSS) betweenproximal, mid and distal CCA after resection and to identify prognostic factors. Methods:Clinicalpathological data of 175 patients with extrahepatic CCA who had undergone resectionwith curative intent between 1992 and 2007 were reviewed. Treatment consisted of proximalbile duct resection with concomitant hepatectomy, local bile duct resection (mid CCA,and radiologically defined Bismuth type I and II lesions), and distal resection as part ofpancreatoduodenectomy (PD). Follow-up data was analyzed for DSS. Results: Of 175 patients,48 (28%) had proximal CCA, 37 (21%) local, and 90 (51%) distal CCA. Median length offollow-up was 19 months (IQR 10-37) for the deceased patients and 54 months (IQR 34-99) for the 36 patients (21%) alive at last follow-up. Kaplan Meier estimate of 5-year DSS(overall 26%) was 42% in proximal CCA, 23% in local CCA and 19% in distal CCA (P0.055). Tumor positive nodes were present in 8 (17%) patients with proximal CCA ascompared to 13 (35%) and 45 (50%) patients with local and distal CCA, respectively (P<.001). Proximal CCA was also the least often associated with moderate to poor tumordifferentiation; ie 24 (50%) patients, compared to 22 (59%) and 80 (89%) in local anddistal CCA, respectively (P <.001). Nine patients (24%) with local CCA had tumor freeresection margins compared to 16 (33%) and 51 (57%) in proximal and distal CCA,respectively (P .001). Forward-entry multiple regression analysis demonstrated that lymphnode status (Hazard Ratio [HR] 1.75; 95%CI 1.19-2.58), tumor differentiation (HR 2.14;95% CI 1.32-3.47), and status of resection margin (HR 1.60; 95% CI 1.08-2.37) wereindependent prognosticators for worse DSS in the entire group. Conclusions: Patients withdistal CCA were associated with the worst DSS after resection, however, location was notan independent prognostic factor for survival. A margin negative resection was the onlyprognostic factor determined by the surgical procedure. In order to improve survival oflocal lesions the surgical procedure should be extended either with liver resection or withpancreatoduodenectomy, depending on site of the lesion.
1032
Fine Needle Aspiration Cytology from Pancreatic Cysts- Limited Utility inSurgical Decision MakingCraig P. Fischer, Bridget N. Fahy, Thomas A. Aloia, Isaac Raijman, Alberto O. Barroso,Peter J. Schwarz, Barbara L. Bass
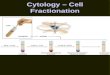
INTRODUCTION. Endoscopic Ultrasound (EUS) plays an important role in the diagnosisof cystic and solid pancreatic lesions. Fine needle aspiration cytology(FNAC) aids physiciansin determining which patients require surgical resection. We report the utility of EUS/FNACin the diagnosis of cystic and solid pancreatic lesions. METHODS. Fifty-eight patientsunderwent EUS/FNAC of pancreatic lesions between 7/2006- 7/2008. Fifty-two patientshad evaluable cytology, and 33 patients underwent surgical resection. FNAC results werecategorized into suspicious/positive for malignancy, negative and indeterminate, based onroutine hematoxylin and eosin staining performed by a single cytopathologist. The sensitivity(S), specificity (SP), positive predictive value (PPV), and negative predictive value (NPV) ofFNAC were determined based upon comparison to final surgical pathology. RESULTS. Ofthe 33 total pancreatic lesions reviewed, 17 were solid and 16 were cystic. Twenty-fourtotal lesions (12 solid, 12 cystic) were malignant or premalignant (73%). FNAC of solidlesions had a S of 100%, SP of 80% PPV of 92% and NPV of 100%. FNAC for cystic lesionshad a S of 58%, SP of 100%, PPV of 100%, and NPV of 44% (Table). While none of themalignant solid lesions had negative FNAC, 5/12 (42%) of malignant or premalignant cysticlesions were negative for malignancy on FNAC. CONCLUSIONS. FNAC demonstratedexcellent accuracy in the diagnosis of solid pancreatic lesions. FNAC of cystic pancreaticlesions was appreciably less accurate and alone does not appear to be an adequate meansof assessing the malignant potential of cystic pancreatic lesions.EUS-FNA Cytology (no. of patients)
A-886SSAT Abstracts
MCN - mucinous cystic neoplasia IPMN - intraductal papillary mucinous neoplasm
1033
Inhibition of IκB Kinase Attenuates Lipopolysaccharide Induced HepaticInjuryJeremy L. Ward, Jordan L. Pleitz, Daniel L. MacDougall, David W. Mercer
Background: Lipopolysaccharide (LPS) causes hepatic injury that may involve enhancedactivity of nuclear factor kappa B (NF-κB) and subsequent changes in expression of oxidativestress proteins such as inducible nitric oxide synthase (iNOS) and cyclo-oxygenase-2 (COX2).Translocation of inactive NF-κB from the cytosol to the nucleus is prevented by the inhibitoryprotein IκBα. NF-κB activation usually involves IκB kinase (IKK) phosphorylation of IκBαon two serine residues with resultant dissociation of IκBα from NF-κB. We hypothesizedthat inhibition of serine phosphorylation of IκBαwould diminish hepatic injury and modulatechanges in oxidative stress protein caused by LPS. Materials and Methods: Male Sprague-Dawley rats received Bay 11-7085 (10 mg/kg IP), an inhibitor of IκB kinase, or vehicle(DMSO) 1 hour before receiving saline or LPS (20 mg/kg IP). Rats were sacrificed 5 hoursafter LPS. Serum was collected to measure ALT as an index of hepatic injury. Liver wasassessed for iNOS and COX2 (Western blot) protein immunoreactivity (n > 5/group;ANOVA). Results: LPS significantly increased ALT levels and upregulated iNOS and COX2when compared to controls. Inhibition of IKK with Bay 11-7085 attenuated LPS inducedhepatic injury and blunted upregulation of iNOS and COX2 when compared to LPS treatedcontrols. Conclusions: These data indicate that LPS induced hepatic injury is mediated, atleast in part, through serine phosphorylation of IκBα which also modulates LPS inducedchanges in hepatic iNOS and COX2 expression.
1034
Frequency of CASH and Its Effect On Surgical Outcomes After NeoadjuvantFOLFOX Therapy for the Treatment of Colorectal Metastasis to the LiverKaye Reid Lombardo, Vishal Chandan, William S. Harmsen, Christina M. Wood, DavidNagorney
Background: Several studies have reported an increased risk of steatosis or chemotherapyassociated steatohepatitis (CASH) in the liver after treatment with FOLFOX for colorectalmetastasis (CRM). The primary aim of this study is to estimate the frequency of CASH inpatients treated with neoadjuvant FOLFOX compared to patients treated with 5-FU/Leucovo-rin and patients with benign hepatic pathologies. Methods: Retrospective analysis of 484patients who underwent hepatic resections from 2000-2005 at the institution was performedto identify 3 groups of patients, Group 1 underwent neoadjuvant chemotherapy with FOL-FOX for CRM (N=39), Group 2 underwent neoadjuvant chemotherapy with 5FU/Leucovorinfor CRM (n=134) and Group 3 did not receive neoadjuvant chemotherapy and had operativeresections for benign diseases (n=51). Data were adjusted for age, gender and BMI. Theassociation of group status with CASH was assessed using Fishers exact test for an orderedcontingency table. Survival was assessed using Kaplan Maier and Cox proportional hazardsregression. Results: Nontumorous liver was available in 187 of 224 patients for pathologicanalysis. Fifty percent of patients were males and the median age was 59(21-80) years.Median follow-up time was 2.4 years. The median duration of chemotherapy treatment was151 days in Group 1 and 153 days in Group 2. The frequency of CASH in Group 1, 2 and3 was 9%, 11% and 6%, respectively (p =0.89). The frequency of steatosis was not differentamong Groups 1, 2 and 3 (p= 0.99). Both operative duration (p=0.007) and blood loss (p=0.003) were greater for patients receiving any chemotherapy compared to benign controls.However, there was no difference in operative duration or blood loss between chemotherapygroups. There was a trend towards greater (>Grade 4) post-operative complications (Claviengrading scheme) in Group 1 compared to Group 2 (p=0.08).Overall 30 day mortality was2.2% and there was no difference in 30 day or 60 day mortality. The one and five yearsurvival was 96.9% and 26.3%, respectively in Group 1. The one and five year survival was96.4% and 43.7%, respectively in Group 2. The HR was 1.6 (0.9-2.86) for patients treatedwith FOLFOX when compared to 5FU. Conclusion: Folfox neoadjuvant chemotherapy wasnot associated with an increased frequency of CASH or steatosis compared to patients'receiving 5FU or patients with benign disease. Folfox therapy was not associated withincreased EBL or operative time when compared to those receiving 5FU but there was atrend to higher grades of complications when compared to patients receiving 5FU. OS wassignificantly less in patients undergoing neoadjuvant FOLFOX therapy.