Embed Size (px)
Citation preview

Intracranial Cysts: Radiologic-Pathologic Correlation and ImagingApproach1
Anne G. Osborn, MDMichael T. Preece, MD Cysts and cystic-appearing intracranial masses have a
broad imaging and pathologic spectra. The authors reviewthe pathologic findings, origin, radiologic appearance, anddifferential diagnosis of many different intracranial cysts.A diagnostic algorithm based on most common anatomiclocations is presented that helps narrow the differentialdiagnosis.
� RSNA, 2006
1 From the Department of Radiology, University of UtahMedical Center, Salt Lake City, Utah. Received May 13,2005; revision requested June 17; revision received July25; accepted September 1; final version accepted De-cember 8. Address correspondence to M.T.P., 266East 4th Ave #501, Salt Lake City, Utah 84103(e-mail: [email protected]).
� RSNA, 2006
REVI
EWS
AND
COM
MEN
TARY
�RE
VIEW
FOR
RESI
DENT
S
650 Radiology: Volume 239: Number 3—June 2006
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

Cysts are common findings at mag-netic resonance (MR) and com-puted tomographic (CT) brain im-
aging. Their histopathologic spectrum isbroad, and differentiation of these cystson the basis of imaging findings alonecan be problematic. In this article, wewill first review the pathologic and im-aging spectra of nonneoplastic and tu-mor-associated nonneoplastic cysts (Ta-ble 1). We will discuss the major differ-ential diagnoses for each cyst. We willthen present an algorithmic location-based diagnostic approach for thesecysts. Cystic and necrotic neoplasms, aswell as brain abscesses, are excludedfrom the discussion.
Choroid Plexus Cysts
Pathologic FindingsChoroid plexus cysts (CPCs) are non-neoplastic epithelial-lined cysts of thechoroid plexus (1,2) (Fig 1). They arethe most common of all intracranialneuroepithelial cysts, occurring in up to50% of autopsy cases. Most are bilat-eral and located in the lateral ventricu-lar atria. The third ventricle is a rarebut reported location (1). Most CPCsare asymptomatic and are found inci-dentally, typically in neonates and olderadults. Symptomatic lesions are rare
since the atria typically enlarge to ac-commodate the cyst (2,3).
CPCs occur when lipid accumulatesin the choroid plexus from degeneratingand/or desquamating choroid epithe-lium (1). CPCs can be almost entirelycystic, nodular, or partially cystic. Theyappear as nodular, yellowish graymasses within the glomus of the choroidplexus. Most are small, measuring 2–8mm in diameter. Cysts greater than 2cm are rare.
Microscopic analysis of CPCs revealsneuroepithelial microcysts containingnests of foamy lipid-laden histiocytes.Chronic inflammatory lymphocytic andplasma cell infiltrates, cholesterol clefts,hemosiderin, and peripheral psammo-matous calcium are part of the CPCspectrum (1).
ImagingCPCs are iso- to slightly hyperattenu-ated on nonenhanced CT scans com-pared with CSF. Peripheral calcificationis common. The cysts show enhance-ment that varies from none to striking.Signal intensity on MR images is vari-able. Most are iso- or hyperintense onprecontrast T1-weighted MR imagescompared with CSF and show rim ornodular contrast enhancement. CPCsare usually hyperintense to CSF on T2-weighted images, especially with longrepetition/short echo time sequences.The majority do not become completelyhypointense (suppress) on fluid-attenu-ated inversion-recovery (FLAIR) imagesand remain slightly or moderately hy-perintense to CSF. Two-thirds show re-striction (high signal intensity) on diffu-sion-weighted images (1,2,4). Real-timeprenatal ultrasonographic (US) findingsdemonstrate a cyst greater than 2 mmsurrounded by echogenic choroid.
Differential DiagnosisThe major differential diagnosis isependymal cyst and villous hyperplasiaof the choroid plexus. Ependymal cystsdo not enhance. Villous hyperplasia isvery rare and, when present, enhancesstrongly and relatively uniformly. Dis-turbed CSF flow and pseudolesions canalso be seen on US images but are moststriking around the foramen of Monro
(interventricular foramen) and withinthe ventricular body, not the atria. Col-loid cysts should not be mistaken forCPCs since they typically occur only atthe foramen of Monro (see below).
Enlarged PVSs
Pathologic FindingsEnlarged PVSs, also known as Virchow-Robin spaces, are pial-lined interstitialfluid-filled structures that accompanypenetrating arteries and veins (Fig 2).They do not communicate directly withthe subarachnoid space (5,6). They arecommon, incidental, “leave me alone”lesions that should not be mistaken formore ominous disease (5). They fre-quently appear in the inferior basal gan-glia, clustering around the anteriorcommissure and surrounding the lentic-ulostriate arteries as they superiorlycourse through the anterior perforatedsubstance. Other common locations in-clude the midbrain, deep white matter,and subinsular cortex. They can also befound in the region of the thalami, den-tate nuclei, corpus callosum, and cingu-late gyrus (5,6).
Microscopically, PVSs consist of asingle or double layer of invaginated pia.They are typically very small or inappar-ent as they pass through the cortex, en-larging in the subcortical white matter.They are typically not associated with gli-osis in the surrounding parenchyma (5).
ImagingProminent PVSs are considered a nor-mal variant. Most appear as smoothlydemarcated fluid-filled cysts, typicallyless than 5 mm in diameter, and oftenoccur in clusters in the basal ganglia ormidbrain. They are isointense to CSF at
Published online10.1148/radiol.2393050823
Radiology 2006; 239:650–664
Abbreviations:CPC � choroid plexus cystCSF � cerebrospinal fluidFLAIR � fluid-attenuated inversion recoveryPVS � perivascular space
Essentials
� Cysts are common findings at MRand CT brain imaging.
� Enlarged perivascular spaces arecommon incidental “leave mealone” lesions that should not bemistaken for more ominous dis-ease.
� Tumor-associated nonneoplasticcysts with trapped CSF or inter-stitial fluid occur, usually with be-nign neoplasms.
� Diffusion-weighted and FLAIR MRsequences are helpful in narrow-ing the differential diagnosis ofcystic brain lesions.
� A location-based approach to in-tracranial cysts is helpful in estab-lishing an appropriate differentialdiagnosis.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 651

all sequences, including FLAIR. Mostshow normal signal intensity in the adja-cent brain; 25% may have a small rim ofslightly increased signal intensity. Theydo not enhance, cause focal mass effect,or restrict on diffusion-weighted im-ages. In older patients, basal gangliaPVSs sometimes become prominentand sievelike, a condition known as etatcrible, or cribriform state.
Occasionally PVSs may become verylarge and appear bizarre. They areprobably caused by the accumulation ofinterstitial fluid between the penetratingvessels and the pia. If interstitial fluid
egress is blocked, fluid accumulates andthe PVSs dilate (5). These lesions causefocal mass effect and occasionally evenhydrocephalus. Rarely, so-called giantor tumefactive PVSs may be mistakenfor more ominous disease (7).
Differential DiagnosisEnlarged PVSs are often mistaken formultiple lacunar infarcts, cystic neo-plasms, and infectious cysts. Lacunarinfarcts can usually be distinguishedfrom PVSs since many exhibit adjacent
Figure 1
Figure 1: (a) Transverse graphic representa-tion shows multiple cystic masses in the choroidplexus glomi (arrows). Most CPCs are actuallydegenerative xanthogranulomas. (Image courtesyof Amirsys, Salt Lake City, Utah.) (b) Transversecontrast-enhanced T1-weighted MR image in ahealthy 52-year-old man shows bilateral CPCswith peripheral and nodular enhancement(arrows).
Figure 2
Figure 2: (a) Coronal gross slice of autopsiedbrain with postmortem gas in bilateral enlargedPVSs. (Image courtesy of E. T. Hedley-Whyte, MD,Massachusetts General Hospital, Boston, Mass.)(b) Transverse contrast-enhanced T1-weighted MRimage shows typical nonenhancing enlarged PVSs inright basal ganglia. The cluster of variably sized cystsis a common appearance. (c) Transverse T2-weightedMR image shows multiple bizarre-appearing cysts(arrows) in centrum semiovale and subcortical whitematter of both hemispheres. The cysts vary in sizeand focally expand but otherwise spare the overlyingcortex.
Table 1
Classification of Intracranial Cysts according to Origin or Pathogenesis
Origin or Pathogenesis Cyst
Normal and/or variant Choroid plexus (xanthogranuloma), enlarged perivascular spaces(PVSs), ependymal, neuroglial, pineal
Congenital Arachnoid, colloid, epidermoid, dermoid, neurenteric, Rathke cleftTraumatic and/or vascular infectious Porencephalic, neurocysticercosis, hydatid, other parasitic cystsTumor-associated nonneoplastic Meningioma (with trapped cerebrospinal fluid [CSF]),
schwannoma (with arachnoid cyst), pituitary adenoma (withenlarged PVSs), craniopharyngioma (with enlarged PVSs)
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
652 Radiology: Volume 239: Number 3—June 2006

parenchymal hyperintensity (so-calledetat lacunaire). Cystic neoplasms rarelyexhibit signal intensity exactly like theCSF. Neurocysticercosis cysts may havea scolex (parasite head), and the cystwalls often enhance. Neurocysticercosiscysts may be multiple but do not typi-cally occur in clusters within the brainparenchyma.
Ependymal Cysts
Pathologic FindingsEpendymal cysts are rare, benign,ependymal-lined cysts of the lateral ven-tricle or juxtaventricular region of thetemporoparietal region and frontal lobe(Fig 3). They have been infrequentlyidentified in the subarachnoid spaces,brainstem, and cerebellum (3,8,9).Most are incidental, but symptomaticcysts may manifest with headache, sei-zure, and/or obstructive hydrocepha-lus. Fewer than 25 symptomatic cystshave been reported in the literature (8).
Ependymal cysts are thought toarise from sequestration of developingneuroectoderm during embryogenesis.They are thin walled and filled withclear serous fluid secreted from ependy-mal cells. Columnar cells, with or with-
out cilia, line ependymal cysts. Theyhave vesicular nuclei and eosinophiliccytoplasm (10).
ImagingThe best diagnostic clue is a nonenhanc-ing thin-walled CSF-containing cyst ofthe lateral ventricle (8).
Differential DiagnosisThe differential diagnosis for an ependy-mal cyst includes CPC, arachnoid cyst,neurocysticercosis, and asymmetric ven-
tricles (8,10). Part or all of a ventricle(most often the temporal horn, atria oflateral ventricles, or fourth ventricle)may also enlarge if it is “trapped” byneoplasm or infection. CPCs are usuallynot identical to CSF at all imaging se-quences, are typically bilateral, and of-ten enhance. Arachnoid cysts occur inthe subarachnoid spaces. Intraventricu-lar neurocysticercosis cysts have a hy-perintense rim and scolex on FLAIR im-ages. Large CSF-appearing cysts mayoccur along the choroid fissure and canbe either ependymal or lined witharachnoid (Fig 4b).
Neuroglial Cysts
Pathologic FindingsNeuroglial (also called glioependymal)cysts are benign epithelial-lined lesionsthat occur anywhere in the neuraxis(Fig 4). They are uncommon, repre-senting fewer than 1% of intracranialcysts (11). While they may occur inmyriad locations, the frontal lobe is themost typical location (11). Also, intra-parenchymal neuroglial cysts are morecommon than extraparenchymal cysts.
Intraparenchymal neuroglial cystsare congenital lesions, arising from em-bryonic neural tube elements that be-come sequestered within the developingwhite matter. They are rounded, smooth,and unilocular and contain clear fluid thatresembles CSF. They are lined byependymal (columnar epithelium) orchoroid plexus cells (low cuboidal epi-thelium) (11).
ImagingThe best diagnostic clue to a neuroglialcyst is a nonenhancing CSF-like paren-chymal cyst with minimal to no sur-rounding signal intensity abnormality.The cysts are benign-appearing lesionswith smooth, rounded borders (11).Size is variable.
Differential DiagnosisOther lesions that may be mistakenfor a neuroglial cyst include an en-larged PVS, infectious cyst, porence-phalic cyst, and arachnoid cyst. En-larged PVSs are typically multiple and
Figure 3
Figure 3: Transverse FLAIR MR image showsependymal cyst within enlarged atrium of the leftlateral ventricle (open arrow). Signal intensity wasisointense to CSF at all pulse sequences. Notelateral displacement of choroid plexus (solidarrow).
Figure 4
Figure 4: (a) Transverse FLAIR MR imageshows typical neuroglial cyst (straight arrow) adja-cent to left temporal horn. The cyst appears welldemarcated without surrounding gliosis and hasthe same appearance as CSF at all sequences. Thiscyst does not communicate with the ventricle(curved arrow). (b) Transverse FLAIR MR imagedemonstrates neuroglial cyst in the choroid fissure(arrow).
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 653

cluster around the basal ganglia. Infec-tious cysts, such as neurocysticerco-sis, are typically smaller than 1 cm andcan partially enhance. Porencephaliccysts communicate with the lateralventricle and show surrounding glio-sis. Arachnoid cysts are typically ex-traaxial (11).
Pineal Cysts
Pathologic FindingsPineal cysts and cystic degeneration ofthe pineal gland with some residual pi-neal parenchyma are common; they areseen in up to 10% of cases at routineimaging and in 20%–40% of cases atautopsy (12–14) (Fig 5). Microscopi-cally, benign pineal cysts exhibit threedistinct layers. The outer layer consistsof a delicate layer of fibrous connectivetissue. The middle layer is composed ofpineal parenchyma with or without cal-cium. The inner layer is composed offinely fibrillar glial tissue that often con-tains hemosiderin deposits (12,15,16).
Theories regarding the origin of pi-neal cysts and/or cystic degeneration ofthe pineal gland include ischemic glialdegeneration with or without hemor-rhagic expansion, preexisting cysts thatenlarge under hormonal influence, andenlargement of the embryonic pinealcavity (2,12). At surgery, they aresmooth unilocular cysts with a soft tanto yellow wall. Contents vary from clearto yellow (most common) to hemor-rhagic. Eighty percent are smaller than1 cm in diameter (12). Cysts larger than1.5 cm may result in hydrocephalus bycausing compression of the tectum andaqueduct (14,15).
ImagingThe best diagnostic clue is unilocular fluid-filled mass within the pineal gland. Attenua-tion or signal intensity varies with cyst con-tent. One-fourth have rim or nodular cal-cium in the cyst wall on nonenhanced CTscans. Rim or nodular enhancement is alsocommon. On T1-weighted MR images,55%–60% are slightly hyperintense toCSF. Most do not appear hypointense onFLAIR images, and 60% enhance with useof contrast material (12).
Differential DiagnosisPineal cysts are most often mistaken for—and may be indistinguishable from—a be-nign pineal parenchymal neoplasm calleda pineocytoma. Pineocytomas are morelikely to have solid components, but itmay be impossible to distinguish the twowith imaging studies alone. Both benignnonneoplastic pineal cysts and the typicalpineocytoma grow extremely slowly, sofollow-up scans are often not helpful. CT-or MR-guided stereotactic biopsy may beneeded for the evaluation and manage-ment of symptomatic cases. Other cystsin the quadrigeminal cistern that mimicpineal cysts include arachnoid cysts (nocalcium) and, rarely, epidermoid cysts(2,12).
Arachnoid Cysts
Pathologic FindingsArachnoid cysts are benign, congenital,intraarachnoidal space-occupying le-sions that are filled with clear CSF (Fig6). They do not communicate with theventricular system (17,18). The cyststend to be unilocular, smoothly margin-ated expansile lesions that are moldedby the surrounding structures. They arecommon, representing 1% of all intra-cranial masses. The incidence is some-what higher in men (15).
Most arachnoid cysts are supraten-torial. Fifty to 60% are found in themiddle cranial fossa, anterior to thetemporal lobes. Other locations includethe suprasellar cistern and posteriorfossa (10%), where they occur mostcommonly in the cerebellopontine anglecistern. Less common locations arewithin the interhemispheric fissure;over the cerebral convexity; or in thechoroidal fissure, cisterna magna, quad-rigeminal cistern, and the vermian fis-sures (15–18).
The precise mechanism for the for-mation of arachnoid cysts is not known(15,18). It is possible that they are sec-ondary to “splitting” or a diverticulum ofthe developing arachnoid. A newer con-cept for the middle fossa arachnoid cystis the failure of temporal embryonicmeninges to merge as the sylvian fis-sure forms. These two layers remain
separate, forming duplicate arachnoid.Other mechanisms might include activefluid secretion by the cyst wall, slow dis-tention by CSF pulsations, or one-wayball-valve flow of CSF (17). The cause hasalso been attributed to trauma, mastoid-itis, meningitis, and subarachnoid hemor-rhage (19). Arachnoid cysts are generallystable over time, although cases of sud-den or progressive enlargement, as wellas spontaneous resolution, have been re-ported (20,21).
Arachnoid cysts collapse on inci-sion. Therefore, surgical specimens areusually limited to a portion of the outerwall. The transparent cyst wall is sepa-rate from the inner dural layer and theunderlying pia-arachnoid. Most are filledwith clear colorless fluid. The size varies,from small and incidental to a large space-
Figure 5
Figure 5: (a) Sagittal gross postmortem slicedemonstrates cystic pineal gland (arrow) with thincyst wall. (Image courtesy of E. Tessa Hedley-Whyte, MD, Massachusetts General Hospital,Boston, Mass.) (b) Sagittal contrast-enhancedT1-weighted MR image shows classic benignpineal cyst (straight arrows) with rim enhancementand mild mass effect (note slight compression,displacement of tectal plate [curved arrow]). (Im-age courtesy of L. Rudolf, MD, Barrett MemorialHospital, Dillon, Mont.)
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
654 Radiology: Volume 239: Number 3—June 2006

occupying lesion with extensive compres-sion of the underlying brain (15,17,18).
Microscopically, the cyst wall is madeof a vascular collagenous membrane linedby flattened arachnoid cells (3,18).Arachnoid cysts lack a glial-limiting mem-brane or an epithelial lining (2).
ImagingThe best diagnostic clue is a sharplydemarcated extraaxial cyst that candisplace or deform adjacent brain.Scalloping of the adjacent calvarium isoften seen. The classic arachnoid cysthas no identifiable internal architec-ture and does not enhance. The cysttypically has the same signal intensityas CSF at all sequences. Occasionally,however, hemorrhage, high proteincontent, or lack of flow within the cystmay complicate the MR appearance(15,17,18). Arachnoid cysts have anincreased prevalence of coexistingsubdural hematomas, especially whenthey occur in the middle cranial fossa.
Differential DiagnosisThe most difficult lesion to distinguishfrom the arachnoid cyst is an epider-moid cyst. Epidermoid cysts can appearnearly identical to CSF on CT scans. OnMR images, epidermoid cysts appear
isointense to CSF, although close in-spection often shows they are not pre-cisely identical in signal intensity toCSF. Arachnoid cysts typically suppresscompletely on FLAIR images and do notrestrict on diffusion-weighted images.Occasionally an arachnoid cyst can beslightly hyperintense on images ob-tained with a long repetition time and ashort echo time. Arachnoid cysts dis-place adjacent arteries and cranialnerves rather than engulf them, as epi-dermoid cysts often do (17–19).
Chronic subdural hematoma andporencephalic cyst can also be confusedfor an arachnoid cyst. Chronic subduralhematomas do not typically show CSFsignal intensity on MR images and oftenhave an enhancing membrane. Porence-phalic cysts often follow a history oftrauma or stroke. The cysts are nor-mally surrounded by gliotic brain (17).
Colloid Cysts
Pathologic FindingsApproximately three people per millionper year receive a diagnosis of a colloidcyst (22) (Fig 7). Colloid cysts are be-nign mucin-containing cysts and ac-count for 0.5%–1% of primary brain
tumors and 15%–20% of intraventricu-lar masses (16,22,23). More than 99%are found wedged in the foramen ofMonro. The cysts are typically attachedto the anterosuperior portion of thethird ventricular roof. The pillars of thefornix straddle the cyst. The posterioraspect of the frontal horns is oftensplayed laterally. Rarely, cysts arefound at other sites, including the lat-eral ventricles, cerebellar parenchyma,and various extraaxial locations (22,23).Even relatively small colloid cysts mayproduce sudden acute hydrocephalus.Occasionally brain herniation with rapidclinical deterioration and even death en-sue (22,23).
Like neurenteric and Rathke cleftcysts, colloid cysts are derived from em-bryonic endoderm (not neuroectoderm)(15). Colloid cysts originate when ec-topic endodermal elements migrate intothe velum interpositum during embryo-genesis (23,24). Contents slowly accu-mulate from epithelial secretory andbreakdown products (23). The cystsare smooth and spherical, varying insize from 0.3 cm to more than 4 cm indiameter (16,22). The mean size is 1.5cm. The cysts are filled with viscousgelatinous material that consists ofmucin, blood degradation products,
Figure 6
Figure 6: (a) Submentovertex view of autopsied brain with large middle fossa arachnoid cyst, which is contained within split layers of arachnoid. (Image courtesy of J.Townsend, MD, University of Utah School of Medicine.) (b) Transverse T2-weighted MR image shows extraaxial CSF-like arachnoid cyst in anterior middle cranial fossa(straight arrow). The temporal lobe is hypoplastic with posteriorly displaced temporal horn (curved arrow). (c) Transverse diffusion-weighted MR image shows no re-striction (an epidermoid cyst would not suppress completely on FLAIR image and would restrict on diffusion-weighted image) and a classic arachnoid cyst (arrows).
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 655

foamy cells, and cholesterol crystals(18,23).
Colloid cysts are characterized by asimple to pseudostratified epithelial lin-ing with interspersed mucous gobletcells and occasional scattered cilia (22).The epithelial layer rests on a delicatelayer of collagen and fibroblasts (18).
ImagingThe best diagnostic clue to a colloid cystis its location at the foramen of Monro.The classic colloid cyst appears as awell-delineated hyperattenuated masson nonenhanced CT scans. Attenuationcorrelates inversely with hydrationstate. On T1-weighted MR images, two-thirds of colloid cysts are hyperintense.The majority are isointense to brain onT2-weighted images. Some demonstrate
peripheral rim enhancement (22,23). Oc-casionally, colloid cysts expand rapidly.These colloid cysts typically have a higherwater content, which reflects ongoingcyst expansion. Thus, it is hypothesizedthat potentially the most “dangerous” le-sions are hypointense on T1- and hyperin-tense on T2-weighted images (24).
Differential DiagnosisThe imaging appearance of a colloid cystis almost pathognomonic. The mostcommon “lesion” mistaken for a colloidcyst is CSF flow artifact (MR pseudo-cyst) caused by pulsatile turbulent CSFflow around the foramen of Monro. Oc-casionally, a neurocysticus cyst may oc-cur at the foramen of Monro. Neo-plasms such as subependymoma or cho-roid plexus papilloma that may occur at
the foramen of Monro are much lesscommon and typically enhance (23).
Epidermoid Cysts
Pathologic FindingsIntracranial epidermoid cysts are con-genital inclusion cysts (Fig 8). Epider-moid cysts comprise 0.2%–1.8% of pri-mary intracranial tumors and are fourto nine times as common as dermoidcysts (18,25). The most common loca-tion for epidermoid cysts is the cerebel-lopontine angle cistern (40%–50%),where they are the third most commonoverall cerebellopontine angle cistern–internal auditory canal mass (afteracoustic schwannoma and meningi-oma). Epidermoid cysts also occur in
Figure 7
Figure 7: (a) Coronal gross specimen showscolloid cyst at the foramen of Monro. Note displace-ment ofseptumpellucidumandfornices(whitearrow)around the cyst (black arrow). Moderate hydrocepha-lus is present. (Image courtesy of J. Townsend, MD,University of Utah School of Medicine.) (b) Trans-verse nonenhanced CT scan shows classic hyperat-tenuated colloid cyst at foramen of Monro (arrow).
Figure 8
Figure 8: (a) Sagittal graphic representationshows posterior fossa epidermoid cyst (arrow) wrap-ping around basilar artery and displacing the brain-stem posteriorly. (Image courtesy of Amirsys, SaltLake City, Utah.) (b) Transverse nonenhanced CTscan shows slightly lobulated low-attenuation massin posterior fossa (arrows). (c) Transverse diffusion-weighted image shows markedly restricted diffusion(arrows). Epidermoid cyst was confirmed at surgery.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
656 Radiology: Volume 239: Number 3—June 2006

the fourth ventricle (17%) and the sellarand/or parasellar regions (10%–15%).Less common locations include the ce-rebral hemispheres or brainstem. Tenpercent of epidermoid cysts are extra-dural, located in the skull or spine. Allare located off the midline (25,26).Most are asymptomatic but may occa-sionally result in mass effect, cranialneuropathy, or seizure (26). Occa-sionally, epidermoid cysts rupture andmay excite a granulomatous meningi-tis (16,27).
Epidermoid cysts arise from ecto-dermal inclusion during neural tubeclosure in the 3rd–5th week of embryo-genesis. Epithelial cell rests may betransplanted to regions such as the cer-ebellopontine angle by the laterally mi-grating otic capsule or developing neu-rovasculature (19). Acquired epider-moid cysts may develop as a result oftrauma but are uncommon in the brain(25).
To the surgeon or pathologist, theirregular lobulated surface of the epi-dermoid glistens with the sheen ofmother-of-pearl. This so-called “beau-tiful tumor” has an irregular cauli-flower-like outer surface that grows toencase vessels and nerves (15,18,25).The cyst interior is filled with “un-
pleasant” soft, waxy, or flaky kerato-hyalin material that results from theprogressive desquamation of the cystwall (18).
The microscopic cyst lining consistsof stratified squamous epithelium sup-ported by an outer layer of collagenousconnective tissue. Cystic contents usu-ally include debris, keratin, water, andcholesterol laid down in a lamellar fash-ion. Epidermoid cysts do not containdermal appendages.
ImagingThe best diagnostic clue is a CSF-likemass that insinuates within cisterns, en-casing adjacent nerves and vessels (25).On CT scans, most epidermoid cysts arewell-defined hypoattenuated massesthat resemble CSF and do not enhance.Calcification is present in 10%–25% ofcases. Most epidermoid cysts are isoin-tense or slightly hyperintense to CSF onboth T1- and T2-weighted MR images.They do not suppress completely onFLAIR images and restrict (show highsignal intensity) on diffusion-weightedimages. Most epidermoid cysts do notenhance, although some minimal rimenhancement occurs in approximately25% of cases.
Rare “white epidermoids” have highprotein content and may appear hyperat-tenuated on CT scans. Compared withthe classic epidermoid cyst, these “dense”or white epidermoids show reversed sig-nal intensity on MR images, with high sig-nal intensity on T1- and low signal inten-sity on T2-weighted images (25).
Differential DiagnosisThe major differential consideration forthe epidermoid cyst is an arachnoidcyst. Arachnoid cysts are isointense toCSF at all sequences, including FLAIR.They displace rather than invade struc-tures such as the epidermoid. Finally,arachnoid cysts do not restrict on diffu-sion-weighted images (18).
Other epidermoid cyst mimics in-clude dermoid cyst, neurocysticercosis,and cystic neoplasm (25). Dermoidcysts are typically located along the mid-line and resemble fat, not CSF. Cysticneoplasms often enhance and do not re-semble CSF. Neurocysticercosis cysts
often enhance and demonstrate sur-rounding edema or gliosis.
Dermoid Cysts
Pathologic FindingsLike epidermoid cysts, dermoid cysts arecongenital ectodermal inclusion cysts (28)(Fig 9). They are extremely rare, consti-tuting fewer than 0.5% of primary intra-cranial tumors and are four to nine timesless common than epidermoid cysts(18,25). They tend to occur in the midlinesellar, parasellar, or frontonasal regions(18,28). Other dermoid cysts are midlinein the posterior fossa, where they occureither as vermian lesions or within thefourth ventricle (15,18,28). These cystsincrease in size by means of glandularsecretion and epithelial desquamation.Growth can lead to rupture of the cystcontents, causing a chemical meningitisthat may lead to vasospasm, infarction,and even death (29). Malignant transfor-mation into squamous cell carcinoma hasalso been described (28).
A common misconception is thatdermoid cysts arise from both ectodermaland mesodermal elements. They do not:Their origin is strictly ectodermal (18).Dermoid cysts arise from the inclusion ofectodermally committed cells at the timeof neural tube closure (3rd–5th week ofembryogenesis [16,28,29]). The capsuleof dermoid cysts consists of simple epi-thelium supported by collagen. Inthicker parts, the lining is supplementedwith dermis containing hair follicles, se-baceous glands, and apocrine glands(16,28). The active production of hairand oils by the dermal appendages hasbeen implicated in the earlier rupturewhen compared with keratin-producingepidermoid cysts (16).
The dermoid cyst is a well-defined,lobulated, “pearly” mass of variable size.The capsule is thicker than that of theepidermoid cyst and often containsplaques of calcification. Characteristi-cally, the cyst contains thick, disagree-able, foul-smelling, yellow material due tothe secretion of sebaceous glands anddesquamated epithelium. The cysts mayalso contain hair and/or teeth (15,16,18,28).
Figure 9
Figure 9: Sagittal T1-weighted MR imageshows mixed-signal-intensity lesion in the pinealregion (straight arrow) with multiple hyperintensedroplets scattered through the subarachnoidspace (curved arrows). Moderate hydrocephalusis present. Ruptured dermoid cyst was confirmedat surgery.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 657

ImagingImaging findings vary, depending onwhether the cyst has ruptured. Unrup-tured cysts have the same imaging char-acteristics as fat because they containliquid cholesterol (26). All are hyperin-tense on T1-weighted images and do notenhance. The masses have heteroge-neous signal intensity on T2-weightedMR images and vary from hypo- to hy-perintense (28,29). The best diagnosticclue of a ruptured dermoid cyst is fatlikedroplets in the subarachnoid cisterns, sulci,and ventricles (28). Extensive pial enhance-ment can be seen from chemical meningitiscaused by ruptured cysts (28).
Differential DiagnosisDermoid cysts may be confused with anepidermoid, craniopharyngioma, tera-toma, or lipoma. Epidermoid cysts typi-cally resemble CSF (not fat), lack der-mal appendages, and are usually locatedoff midline. Like dermoid cysts, cranio-pharyngiomas are suprasellar, with amidline location, and demonstrate nod-ular calcification. However, most cra-niopharyngiomas are strikingly hyperin-tense on T2-weighted images and en-hance strongly. Teratomas may alsohave a similar location but usually occurin the pineal region. Lipomas demon-strate homogeneous fat attenuationand/or signal intensity and show achemical shift artifact, which typicallydoes not occur with dermoid cysts.
Neurenteric Cysts
Pathologic FindingsNeurenteric cysts are congenital, be-nign, malformative endodermal lesionsin the central nervous system (Fig 10).They are approximately three times ascommon in the spine, compared withthe brain (30). Most intracranialneurenteric cysts are found in the poste-rior fossa. They are typically in the mid-line, anterior to the brainstem. Theycan also be found in the cerebellopon-tine angle or clivus. Supratentorial cystshave rarely been reported (30).
While the precise origin is un-known, neurenteric cysts probably ariseat the time of notochordal development
during the transitory existence of theneurenteric canal. The notochord andforegut fail to separate, causing primi-tive endodermal cells to be incorpo-rated into the notochord. These dis-placed alimentary cells ultimately be-come the cyst (18,30,31).
The size of the cysts is variable, usu-ally measuring less than 2 cm. Gross cystsare smooth, thin-walled, and transparentstructures. The contents vary from clearto mucoid or xanthochromic (30).
Microscopic examination of the cystwall demonstrates endothelium-linedstructures of cuboidal to columnar cells(partially ciliated). The epithelium may bepseudostratified in places and typicallyhas ciliated and goblet cells (31,32). Thecysts contain only endodermal elementsand closely resemble gastrointestinaltract mucosa (31).
ImagingThe best diagnostic clue for a neuren-teric cyst is a round and/or lobulated,nonenhancing, slightly hyperintensemass in front of the medulla. The signalintensity characteristics vary dependingon the protein content of the cysts.Most are proteinaceous with a T1-weighted imaging appearance that isiso- to slightly hyperintense comparedwith the CSF and a T2-weighted imagingappearance that is very hyperintense(30,33–35). Neurenteric cysts are hy-perintense on FLAIR images and mayshow mild restriction on diffusion-weighted images. They very rarely showrim enhancement.
Differential DiagnosisThe differential diagnosis of a neurentericcyst includes epidermoid cyst, arachnoidcyst, and other endodermal cysts (Rathkeand colloid) (30). The rare white epider-moid is most like the neurenteric cyst be-cause it is hyperintense on T1-weightedimages and can be difficult to distinguish iflocated along the midline (30). Epider-moid cysts usually restrict on diffusion-weighted images (34). Arachnoid cystshave the same appearance as CSF at allsequences. Other endodermal-derivedcysts such as Rathke and colloid can bedifferentiated from neurenteric cysts onthe basis of location.
Rathke Cleft Cysts
Pathologic FindingsRathke cleft cysts are congenital non-neoplastic cysts arising from remnantsof the embryonic Rathke cleft (36) (Fig11). They are common incidental intra-and/or suprasellar lesions and are foundin 13%–33% of routine autopsy series(36,37). Forty percent are completelyintrasellar, while 60% have some supra-sellar extension (36). Completely supra-sellar cysts are rare (18). Symptoms oc-cur from compression of the optic chi-asm, hypothalamus, or pituitary gland(15).
Rathke cleft cysts probably arisefrom the failure of obliteration of theRathke pouch, which develops as a ros-tral outpouching of the primitive oralcavity during the 3rd or 4th week ofembryogenesis (37). This rostral elon-gation of the pouch forms the cranio-pharyngeal duct. The proximal portionof the duct closes early during develop-ment, but a remnant may persist be-tween the pars distalis and pars ner-vosa. Occasionally, this remnant givesrise to the macroscopic Rathke cleft cyst(18).
Rathke cleft cysts are smoothly mar-ginated cysts that vary in size from a fewmillimeters to 1–2 cm. The contents vary
Figure 10
Figure 10: Sagittal T1-weighted MR imageshows small well-delineated ovoid mass in front ofpontomedullary junction (arrow). Mass is hyperin-tense compared to CSF. Location and configurationare typical foraneurentericcyst,confirmedatsurgery.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
658 Radiology: Volume 239: Number 3—June 2006

from clear CSF-like fluid to thick mucoidmaterial (36). Microscopically they aresimilar to other endodermal cysts (neu-renteric and colloid). They are lined bypseudostratified or single-layered colum-nar or cuboidal epithelium. Cilia and scat-teredmucin-secretinggobletcellsarecom-mon. Many cysts have squamous differen-tiation, and cornified squamous pearlsare occasionally identified (18). The intra-cystic nodule consists of mucinous mate-rial at histologic examination. Biochemi-cal analysis of this material is consistentwith cholesterol and protein (37).
ImagingThe best imaging clue is a nonenhancingnoncalcified intra- and/or suprasellar cystwith an intracystic nodule (36,37). Whilethis is the typical picture, the imagingcharacteristics vary widely. Approxi-mately half are hyperintense on T1-weighted images, while half are hypoin-tense. On T2-weighted images, 70% arehyperintense and 30% are iso- or hypoin-tense (36). A small nonenhancing intra-cystic nodule is considered a virtually pa-thognomonic sign of a Rathke cleft cyst.These nodules show high signal intensityon T1-weighted images and low signal in-
tensity on T2-weighted images, and theydo not enhance (37). Rathke cleft cysts donot enhance after contrast material ad-ministration, although an enhancing rimof displaced compressed pituitary gland ispresent in approximately half of the cases(18).
Differential DiagnosisThe differential diagnosis for Rathkecleft cysts includes craniopharyngioma,cystic pituitary adenoma, or other non-neoplastic cysts (36). Unlike Rathkecleft cysts, craniopharyngiomas typi-cally demonstrate calcification and ap-proximately 90% have nodular, globu-lar, or rim enhancement. The presenceof solid enhancing nodules in the cystwall also favors the diagnosis of cranio-pharyngioma (37,38). The rare noncal-cified cystic nonenhancing craniophar-yngioma, a finding more common inadults than in children, may be impossi-ble to distinguish from Rathke cleft cystwith imaging findings alone.
Porencephalic Cysts
Pathologic FindingsPorencephalic cysts are congenital oracquired cavities within the cerebral
hemisphere that usually—although notinvariably—communicate directly withthe ventricular system (1). They can becortical or subcortical, unilateral or bi-lateral (39). The location often corre-sponds to territories supplied by the ce-rebral arteries.
Congenital porencephalic cysts orig-inate from a fetal or perinatal encepha-loclastic process that results from intra-uterine vascular or infectious injury. Ac-quired cysts are secondary to injurylater in life and are usually secondary totrauma, surgery, ischemia, or infection(Fig 12a).
Porencephalic cysts vary greatly insize. They are typically CSF-filled cavi-ties with a smooth wall and are linedwith gliotic or spongiotic white matter.The adjacent skull may demonstrate re-modeling due to chronic CSF pulsations(39).
ImagingThe typical porencephalic cyst is a cysticspace in the brain parenchyma thatcommunicates with an enlarged adja-cent ventricle. The cysts have the sameappearance as CSF at all MR sequences(39). Adjacent white matter typicallyshows hyperintensity on T2-weightedand FLAIR images.
Figure 11
Figure 11: Sagittal postcontrast T1-weightedMR image shows rounded mass (solid arrow)separate from and just above the pituitary gland(open arrow). This cyst has moderately high pro-tein content and is isointense with brain, not CSF.Location is typical for a Rathke cleft cyst, con-firmed at surgery. (Image courtesy of J. Rees, MD,MedTell International, McLean, Va.)
Figure 12
Figure 12: (a) Close-up of autopsy brain specimen shows large acquired porencephalic cyst in the tempo-ral lobe that communicates with temporal horn of the lateral ventricle (arrows). (Image courtesy of E. Ross,MD, Loyola University School of Medicine, Chicago, Ill.) (b) Coronal T1-weighted MR image in another caseshows enlarged left temporal horn (black arrow) that communicates with peripherally located porencephaliccyst (white arrows). Cyst extends to the brain surface.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 659

Differential DiagnosisThe differential diagnosis for the poren-cephalic cyst includes arachnoid cyst,schizencephaly, ependymal cyst, en-cephalomalacia, and hydranencephaly.Arachnoid cysts are extraaxial and dis-place the brain cortex away from theadjacent skull. Schizencephaly is a CSF-filled cavity that is lined with hetero-topic gray matter and extends all theway from the ventricle to the brain sur-face. Ependymal cysts are typically in-traventricular with normal surroundingbrain tissue (39).
Neurocysticercosis
Pathologic FindingsCysticercosis is the most common, mostwidely disseminated parasitic infectionin the world (40,41) (Fig 13). Neurocys-ticercosis occurs in 60%–90% of allcases of systemic cysticercosis. Mostneurocysticercosis cysts are found inthe subarachnoid spaces, typically thebasal cisterns and deep within the sulci.Inflammatory reaction provoked by thecyst may cause adhesion of the adjacentgyral surfaces, giving the mistaken im-pression that the cyst is intraparenchy-mal. Other common locations includethe hemispheric parenchyma at the graymatter–white matter interface and inthe ventricles (fourth ventricle is mostcommon) (40). Rarely, cysts are foundin the sella, orbit, or spinal cord (41).Seizures are the common manifestationof neurocysticercosis (40,42).
ImagingImaging findings in neurocysticercosisvary with the stage of cyst development.The early vesicular stage is typified by asmooth thin-walled cyst that is CSF-likeon CT and MR images. Edema and con-trast enhancement are rare. A muralnodule is often present that representsthe viable larval scolex, the “cyst with adot” appearance (40,41). When cyst de-generation begins (colloidal-vesicularstage) and host inflammatory responseensues, pericystic edema and cyst wallenhancement are present. Cyst fluid ishyperintense to CSF on MR images dur-ing this stage (41).
In the healing, or granular nodular,stage, nonenhanced CT scans show anisoattenuated cyst with a hyperattenuatedcalcified scolex. Surrounding edema isstill present, and enhancement followingcontrast material administration persists.The residual cyst is isointense to the brainon T1-weighted images and it is iso- tohypointense on T2-weighted images.Nodular or micro-ring enhancement iscommon at this stage, suggesting granu-loma. Occasionally, a “target” or “bull’seye” appearance is seen with the calcifiedscolex in the center of the mass (41).
In the quiescent or residual stage,small calcified nodules without mass ef-fect and usually without enhancementare seen (40,41). Multifocal lesions andlesions in different stages of develop-ment are common.
Differential DiagnosisThe differential diagnosis for neuro-cysticercosis includes abscess, tuber-culosis, neoplasm (primary or meta-static), enlarged PVSs, and otherparasitic infections. Abscesses have aT2-hypointense rim, whereas neuro-cysticercosis cysts are typically isoin-tense except when they are in the ven-tricles where the rim is hyperintenseon FLAIR images. Tuberculomas often
occur with meningitis, are rarely cys-tic, and are often profoundly hypoin-tense on T2-weighted images. En-larged PVSs have the same appear-ance as CSF at all MR sequences anddo not enhance. None of these cysticlesions has the characteristic “cystwith dot” appearance (40).
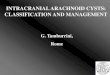
Figure 13
Figure 13: (a) Multiple neurocysticercosis cysts of various sizes. Some contain visible scolices (arrows).(Image courtesy of E. Ross, MD, Loyola University School of Medicine, Chicago, Ill.) (b) Transverse T1-weighted MR image shows innumerable tiny low-signal-intensity neurocyticercosis cysts in brain paren-chyma and subarachnoid spaces. Most contain small “dot” that represents the scolex (arrows).
Figure 14
Figure 14: Hydatid cyst. Transverse contrast-enhanced CT scan in a 5-year-old child shows avery large nonenhancing cystic mass without sur-rounding edema (arrows). (Image courtesy of R.Ramakantan, MD, King Edward Memorial Hospi-tal, Bombay, India.)
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
660 Radiology: Volume 239: Number 3—June 2006

Hydatid Cysts
Pathologic FindingsIntracranial hydatid cysts are parasiticinfections caused by the larval stage of
Echinococcus granulosus (41) (Fig14). The cysts preferentially affect theliver but may also involve the lungs,bone, and brain. Cerebral hydatidcysts are rare, seen in only 2% of
cases (41,43). The most common loca-tion for intracranial hydatid cysts isthe hemispheric parenchyma, particu-larly in the perfusion territory of themiddle cerebral artery (41,44). Thesubarachnoid spaces are another com-mon site of involvement.
Hydatid cysts are usually spherical,solitary, and unilocular. They growslowly and are typically large, averaging4–10 cm in diameter (45). The cystscontain translucent fluid and may alsocontain daughter cysts with an appear-ance resembling small white grapes.Protoscolices within cysts form a granu-lar deposit known as hydatid sand (44).
ImagingThe best diagnostic clue of a hydatidcyst is a single, large, thin-walled,spherical, nonenhancing CSF-attenua-tion cyst in the parietal region of thebrain. Perilesional edema is usually ab-sent. The two visible imaging compo-nents are the cyst and the pericyst. Thepericyst is a peripheral capsule of thecyst. While MR imaging is more sensi-tive in demonstrating the pericyst, CT ismore sensitive in depicting cyst calcifi-cation (43). Multilocular or multiple le-sions occur but are rare (43).
Differential DiagnosisThe differential diagnosis for hydatidcysts includes arachnoid cyst, epider-moid cyst, and neurocysticercosis (41).
Other Parasitic Cysts
Pathologic FindingsA number of parasites may occasionallyinfect the central nervous system andappear at least partially cystic (Fig 15a).Amebiasis, paragonimiasis, schistoso-miasis, and sparganosis can cause bothunilocular and complex intraparenchy-mal cysts with or without accompany-ing meningoencephalitis. Perilesionaledema and petechial hemorrhage arecommon.
ImagingComplex conglomerate cysts with thickenhancing rims and striking adjacentedema are common.
Figure 15
Figure 15: (a) Sagittal precontrast T1-weighted MR image in a patient presenting to the emergency roomwith seizure shows partially cystic mixed-signal-intensity subcortical mass (arrow). (b) Transverse postcon-trast T1-weighted MR image demonstrates some enhancement around complex cystic mass (arrow). Surgerydisclosed multiloculated amebic abscess. (Image courtesy of R. Hewlett, MD, Stellenbosch University Schoolof Medicine, Cape Town, South Africa.)
Figure 16
Figure 16: (a) Transverse postcontrast T1-weighted MR image shows facial schwannoma associated withlarge arachnoid cyst (open arrow). Note enhancing cerebellopontine angle cistern–internal auditory canalportion of the mass as it extends into labyrinthine segment of facial nerve canal (curved arrow). Incidentallynoted is a filling defect in the left transverse sinus, which was a large arachnoid granulation (black arrow).(b) Coronal postcontrast T1-weighted MR image in another case shows large pituitary macroadenoma withmultiple cysts (arrows) surrounding the suprasellar component. Cysts appear slightly hyperintense to CSF.Fluid in enlarged trapped PVSs was confirmed at surgery.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 661

Differential DiagnosisComplex conglomerated parasitic cystsof any origin may mimic primary ormetastatic brain tumor. The patient’spersonal and travel history, as well asserologic findings, are key to the diag-nosis.
Neoplasm-associated Benign Cysts
Pathologc FindingsExtraaxial tumors such as meningioma,schwannoma, craniopharyngioma, andpituitary macroadenoma may be associ-ated with large nonneoplastic cysts (Fig16). These peritumoral cysts appear tocontain CSF. Some, such as cysts thatoccur adjacent to vestibular schwan-noma, are true arachnoid cysts. Others,such as meningioma, trap CSF withinthe cleft between the expanding tumorand the adjacent brain. Craniopharyngi-omas and pituitary macroadenomaswith suprasellar extension may obstruct
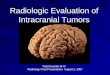
Figure 17
Figure 17: Diagnostic algorithm for intracranial cyst with common location: Rathke cleft cyst (RCC), suprasellar arachnoid cyst (SSAC), arachnoid cyst (AC), neuro-cysticercosis (NCC), neurenteric cyst (NE), and enlarged PVSs.
Table 2
Classification of Intracranial Cysts according to Most Common Location
Cyst Location
Arachnoid Middle cranial fossaChoroid plexus Lateral ventricle (atria)Colloid Third ventricle (foramen of Monro)Craniopharyngioma (with enlarged PVSs) SuprasellarDermoid Sellar, parasellar, frontonasal (midline)Enlarged PVS Basal ganglia/midbrainEpidermoid Cerebellopontine angle cisternEpendymal Lateral ventricleHydatid Parietal lobeMeningioma (with trapped CSF) Convexity or planum sphenoidaleNeurenteric PrepontineNeurocysticercosis Convexity or basal subarachnoid spacesNeuroglial Frontal lobePineal Pineal glandPituitary adenoma (with enlarged PVSs) ParasellarPorencephalic Cerebral hemispheresRathke cleft Sellar or suprasellarSchwannoma (with arachnoid cyst) Cerebellopontine angle cistern
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
662 Radiology: Volume 239: Number 3—June 2006

and enlarge adjacent PVSs. Interstitialfluid is retained within the enlargedPVSs and may result in edema along theoptic tracts. Occasionally, large peritu-moral cysts can be identified.
ImagingTumor-associated arachnoid cysts andcystic PVSs do not enhance. Most paral-lel CSF in signal intensity. If protein con-tent is elevated within the trapped poolsof CSF, the arachnoid cysts may appearslightly hyperintense to normal CSF onMR images.
Differential DiagnosisTrue arachnoid cyst associated withneoplasm may be impossible to distin-guish from enlarged PVSs with trappedinterstitial fluid unless biopsy is per-formed.
Location-based Diagnostic Approach
A location-based approach to intracra-nial cysts is helpful in establishing anappropriate differential diagnosis. Manyintracranial cysts occur in characteristiclocations (Table 2). Some locations arevirtually pathognomonic for certain le-sions (eg, colloid cyst in anterosuperioraspect of the third ventricle), while othersare suggestive of—but not specific for—aparticular diagnosis (eg, middle cranialfossa and arachnoid cyst).
A series of imaging questions, posedin the following order, results in a usefuldiagnostic algorithm (Fig 17): (a) Is thecyst intra- or extraaxial? (b) Is it supra-or infratentorial? (c) If extraaxial, is itmidline or off midline? (d) If intraaxial,is it intraparenchymal or intraventricu-lar? (e) If intraventricular, what is thespecific location? (f) Is the cyst CSF-likeon CT and/or MR images or is it differ-ent? (g) Are there any special distin-guishing imaging features (eg, calcifica-tion, enhancement, diffusion restric-tion)?
Conclusion
A broad spectrum of diseases can causeintracranial cysts. The combination of alocation-based algorithm with specificimaging findings, such as presence or
absence of calcification, enhancement,MR signal intensity at different se-quences, and presence or absence ofrestriction on diffusion-weighted im-ages, permits a narrowed differential di-agnosis when an intracranial cyst isidentified on imaging studies.
References1. Osborn AG. Choroid plexus cyst. In: Diag-
nostic imaging: brain. Salt Lake City, Utah:Amirsys, 2004; I-7-30.
2. Osborn AG. Brain tumors and tumorlikemasses: classification and differential diag-nosis. In: Diagnostic neuroradiology. StLouis, Mo: Mosby, 1994; 408–430.
3. Boockvar JA, Shafa R, Forman MS,O’Rourke DM. Symptomatic lateral ventricu-lar ependymal cysts: criteria for distinguish-ing these rare cysts from other symptomaticcysts of the ventricles—case report. Neuro-surgery 2000;46(5):1229–1233.
4. Kadota T, Mihara N, Tsuji N, Ishiguro S,Nakagawa H, Kuroda C. MR of xanthogran-uloma of the choroid plexus. AJNR Am JNeuroradiol 1996;17(8):1595–1597.
5. Osborn AG. Enlarged perivascular spaces.In: Diagnostic imaging: brain. Salt Lake City,Utah: Amirsys, 2004; I-7-22.
6. Osborn AG. Acquired metabolic, white mat-ter, and degenerative diseases of the brain.In: Diagnostic neuroradiology. St Louis, Mo:Mosby, 1994; 751–752.
7. Salzman KL, Osborn AG, House P, et al.Giant tumefactive perivascular spaces.AJNR Am J Neuroradiol 2005;26:298–305.
8. Salzman KL. Ependymal cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-34.
9. Gherardi R, Lacombe MJ, Porer J, et al.Asymptomatic encephalic intraparenchyma-tous neuroepithelial cysts. Acta Neuropathol1984;63:264.
10. Pawar SJ, Sharma RR, Mahapatra AK, DevEJ. Giant ependymal cyst of the temporalhorn: an unusual presentation—case reportwith review of the literature. Pediatr Neuro-surg 2001;34:306–310.
11. Osborn AG. Neuroglial cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-20.
12. Osborn AG. Pineal cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-26.
13. Engel U, Gottschalk S, Niehaus L, et al. Cys-tic lesions of the pineal region: MRI and pa-thology. Neuroradiology 2000;42:399–402.
14. Barboriak DP, Lee L, Provenzale JM. SerialMR imaging of pineal cysts: implications fornatural history and follow-up. AJR Am JRoentgenol 2001;176:737–743.
15. Burger PC, Scheithauer BW, Vogel FS. In-tracranial meninges. In: Surgical pathologyof the brain and its coverings. 4th ed. Phila-delphia, Pa: Churchill Livingstone, 2002;89–93.
16. McLendon RE, Tien RD. Tumors and tumor-like lesions of maldevelopmental origin. In:Russell and Rubinstein’s pathology of tumorsof the nervous system. 6th ed. New York,NY: Oxford University Press, 1998; 327–352.
17. Osborn AG. Arachnoid cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-4.
18. Osborn AG. Miscellaneous tumors, cysts,and metastases. In: Diagnostic neuroradiol-ogy. St Louis, Mo: Mosby, 1994; 631–649.
19. Dutt SN, Mirza S, Chavda SV, Irving RM.Radiologic differentiation of intracranial epi-dermoids from arachnoid cysts. Otol Neuro-tol 2002;23:84–92.
20. Rao G, Anderson R, Feldstein NA, Brock-meyer DL. Expansion of arachnoid cysts inchildren: report of two cases and review ofthe literature. J Neurosurg 2005;102(3suppl):314–317.
21. Falcone C, Tinelli E, Pierallini A, et al. Spon-taneous disappearance of juxta-sylvian cyst:MRI study and clinical evaluations [in Ital-ian]. Riv Neuroradiol 2005;18:54–58.
22. Armao D, Castillo M, Chen H, Kwock L.Colloid cyst of the third ventricle: imaging-pathologic correlation. AJNR Am J Neurora-diol 2000;21:1470–1477.
23. Osborn AG. Colloid cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-8.
24. Pollock BE, Schreiner SA, Huston J 3rd. Atheory on the natural history of colloid cystsin the third ventricle. Neurosurgery 2000;46(5):1077–1081.
25. Katzman GL. Epidermoid cyst. In: Diagnos-tic imaging: brain. Salt Lake City, Utah:Amirsys, 2004; I-7-16.
26. Castillo M. Intracranial tumors. In: The corecurriculum: neuroradiology. Philadelphia,Pa: Lippincott Williams & Wilkins, 2002;166–172.
27. Timmer FA, Sluzewski M, Treskes M, vanRooij WJ, Teepen JL, Wijnalda D. Chemicalanalysis of an epidermoid cyst with unusualCT and MR characteristics. AJNR Am J Neu-roradiol 1998;19:1111–1112.
28. Katzman GL. Dermoid cyst. In: Diagnostic
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
Radiology: Volume 239: Number 3—June 2006 663

imaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-12.
29. Brown JY, Morokoff AP, Mitchell PJ, Gonza-les MF. Unusual imaging appearance of anintracranial dermoid cyst. AJNR Am J Neu-roradiol 2001;22:1970–1972.
30. Osborn AG. Neurenteric cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; I-7-40.
31. Harris CP, Dias MS, Brockmeyer DL,Townsend JJ, Willis BK, Apfelbaum RI.Neurenteric cysts of the posterior fossa: rec-ognition management, and embryogenesis.Neurosurgery 1991;29:893–897.
32. Chaynes P, Thorn-Kany M, Sol JC, Arrue P,Lagarrigue J, Manelfe C. Imaging in neuren-teric cysts of the posterior cranial fossa.Neuroradiology 1998;40(6):374–376.
33. Shakudo M, Inoue Y, Ohata K, Tanaka S.Neurenteric cyst with alteration of signal in-tensity on follow-up MR images. AJNR Am JNeuroradiol 2001;22:496–498.
34. Evans A, Stoodley N, Halpin S. Magneticresonance imaging of intraspinal cysticlesions: a pictorial review. Curr Probl DiagnRadiol 2002;31(3):79–94.
35. Hayashi Y, Tachibana O, Muramatsu N, etal. Rathke cleft cyst: MR and biomedicalanalysis of cyst content. J Comput Assist To-mogr 1999;23:34–38.
36. Osborn AG. Rathke cleft cyst. In: Diagnosticimaging: brain. Salt Lake City, Utah: Amir-sys, 2004; II-2-16.
37. Byun WM, Kim OL, Kim D. MR imagingfindings of Rathke’s cleft cysts: significance ofintracystic nodules. AJNR Am J Neuroradiol2000;21:485–488.
38. Shin JL, Asa SL, Woodhouse LJ, Smyth HS,Ezzat S. Cystic lesions of the pituitary: clini-copathological features distinguishing cra-niopharyngioma, Rathke’s cleft cyst, andarachnoid cyst. J Clin Endocrinol Metab1999;84(11):3972–3982.
39. Osborn AG. Porencephalic cyst. In: Diagnos-
tic imaging: brain. Salt Lake City, Utah:Amirsys, 2004; I-7-36.
40. Salzman KL. Parasites, miscellaneous. In:Diagnostic imaging: brain. Salt Lake City,Utah: Amirsys, 2004; I-8-53.
41. Osborn AG. Infections of the brain and itslinings. In: Diagnostic neuroradiology. StLouis, Mo: Mosby, 1994; 709–713.
42. Garcia HH, Gonzalez AE, Evans CA, GilmanRH. Taenia solium cysticercosis. Lancet2003;362(9383):547–554.
43. Tsitouridis J, Dimitriadis AS, Kazana E. MRin cisternal hydatid cysts. AJNR Am J Neuro-radiol 1997;18:1586–1587.
44. Ellison D, Love S, Chimelli L, Harding BN,Lowe J, Vinters H. Parasitic infections. In:Neuropathology: a reference text of CNS pa-thology. 2nd ed. Philadelphia, Pa: Mosby,2004; 379–381.
45. Taratuto AL, Venturiello SM. Echinococco-sis. Brain Pathol 1997;7:663–672.
REVIEW FOR RESIDENTS: Intracranial Cysts Osborn and Preece
664 Radiology: Volume 239: Number 3—June 2006