Embed Size (px)
DESCRIPTION
Bones
Citation preview
A Video Review of Skull and Mandible Anatomy
Gives information on skull structures
Gives information on certain endocrine and metabolic disorders, metastasis and fractures
no value for patients suspected of having neurological disease
PLAIN SKULL RADIOGRAPHY
Routine Method of Study of Skull Radiographs… WHAT TO TAKE NOTE?
shape of the skull as a whole
especially the relationship of the vault to the base in all views
outline of the skull as a whole
noting the thickness of the inner and outer tables
lines, impressions, channels and sutures
Routine Method of Study of Skull Radiographs… WHAT TO TAKE NOTE?
Check for calcifications
Carefully define the sella turcica, its anterior and posterior clinoid processes and tuberculum sellae
Examine the petrous ridges, orbits, sphenoid ridges, temporal bones and facial bones
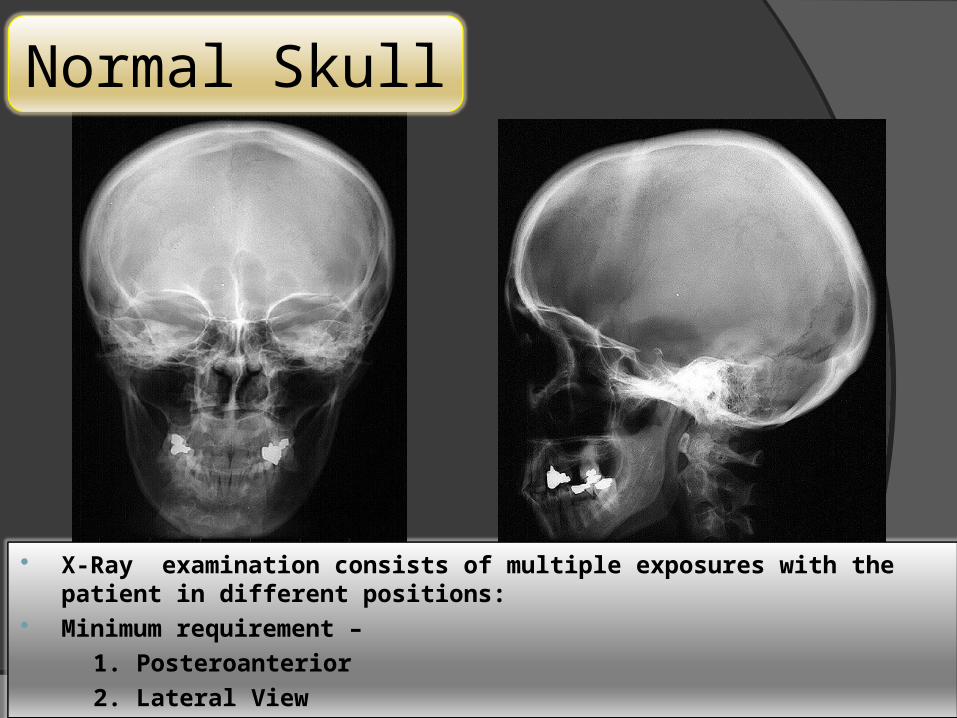
X-Ray examination consists of multiple exposures with the patient in different positions:
Minimum requirement –
1. Posteroanterior
2. Lateral View
Normal Skull
Routine Radiographic Procedures of Skull
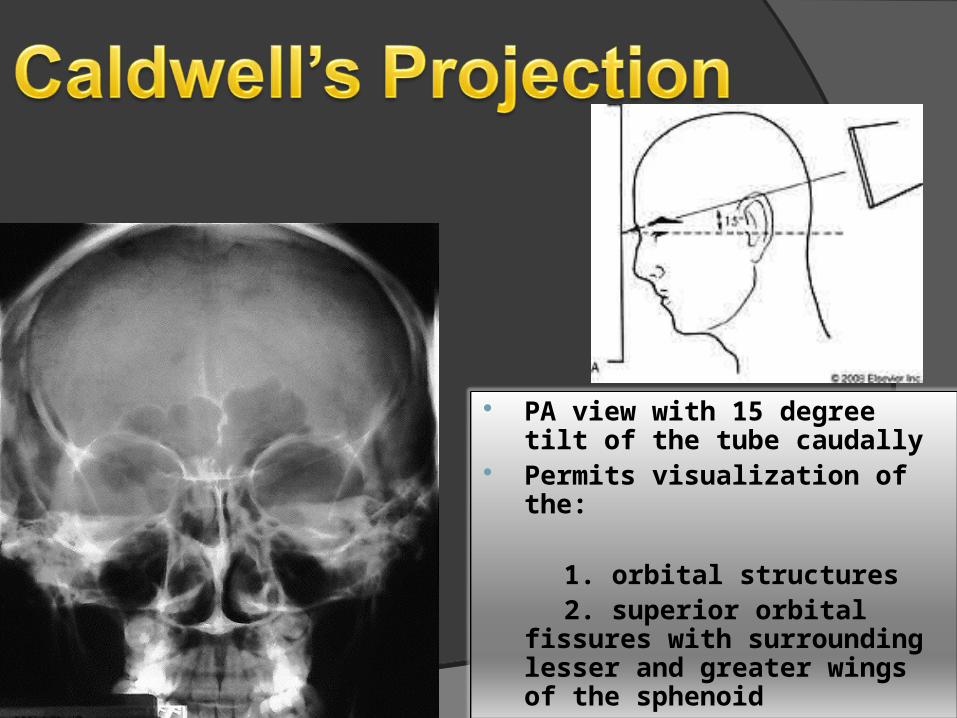
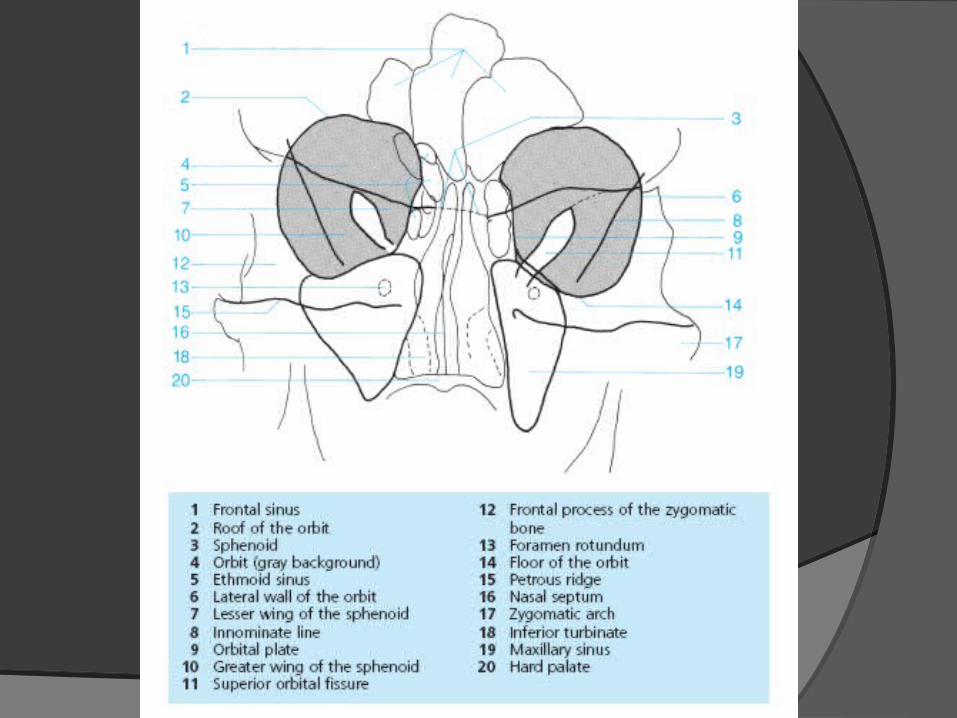
PA view with 15 degree tilt of the tube caudally
Permits visualization of the:
1. orbital structures 2. superior orbital fissures with
surrounding lesser and greater wings of the sphenoid
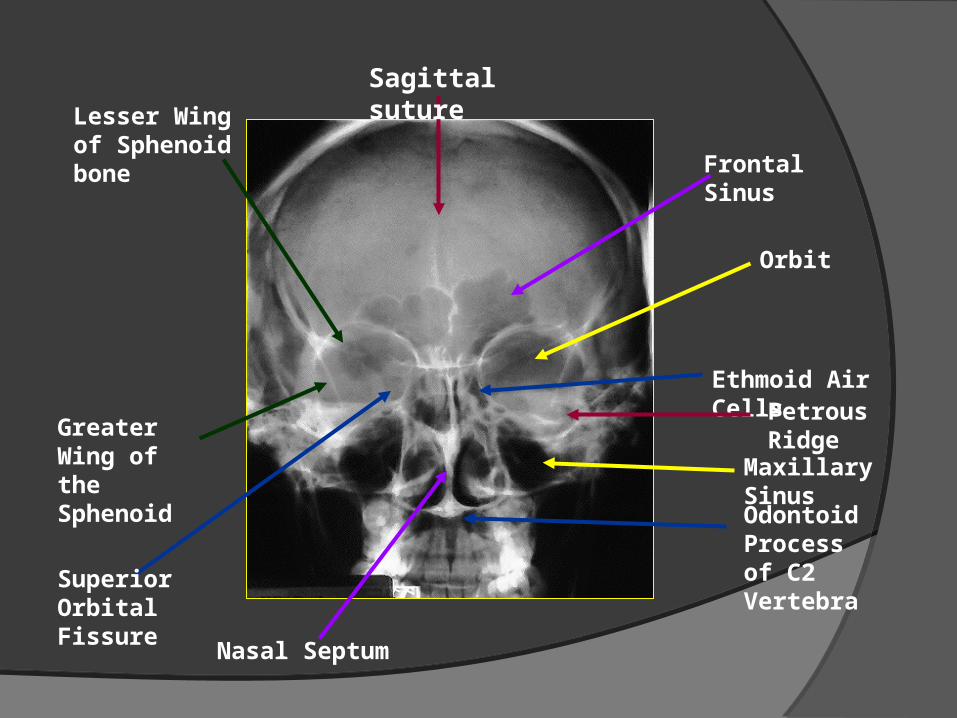
Sagittal suture
Frontal Sinus
Orbit
Maxillary Sinus
Odontoid Process of C2 Vertebra
Lesser Wing of Sphenoid bone
Greater Wing of the Sphenoid
Superior Orbital Fissure
Ethmoid Air Cells
Nasal Septum
Petrous Ridge
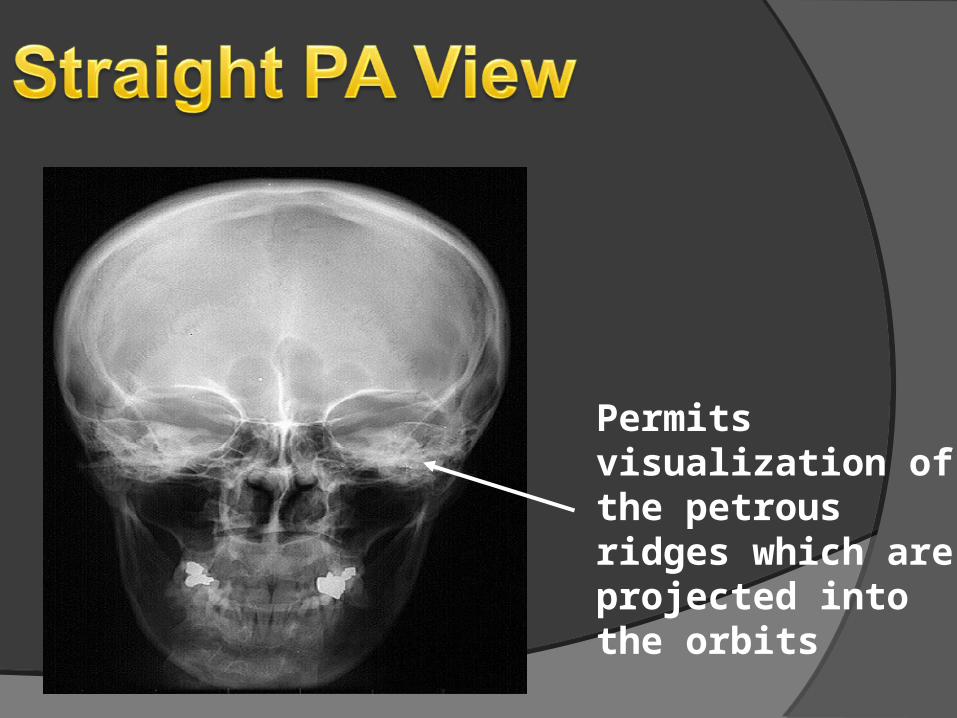
Permits visualization of the petrous ridges which are projected into the orbits
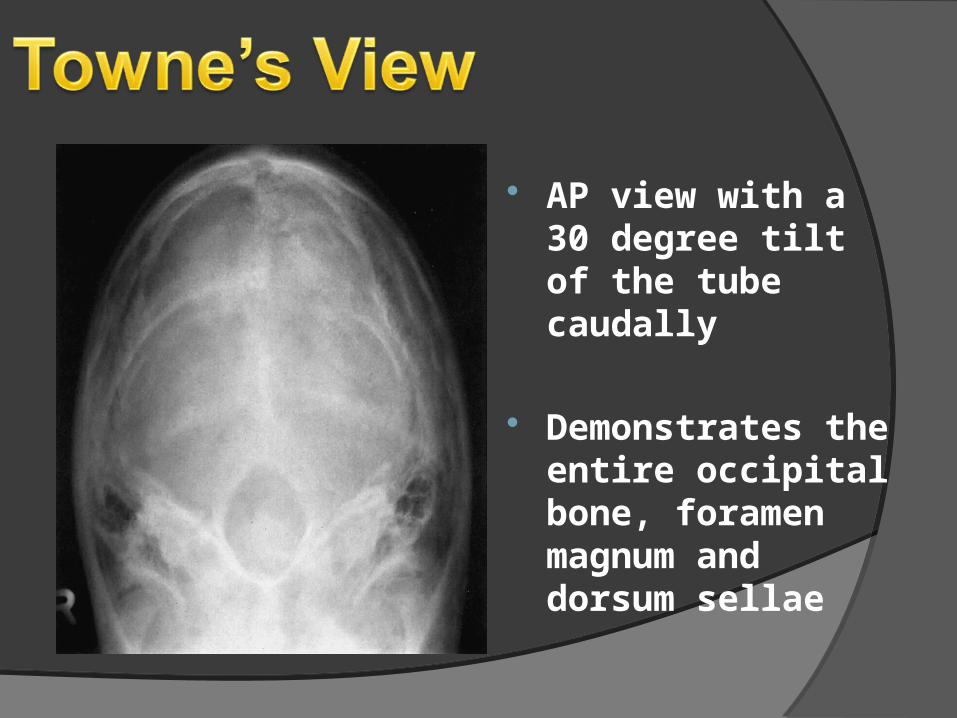
AP view with a 30 degree tilt of the tube caudally
Demonstrates the entire occipital bone, foramen magnum and dorsum sellae
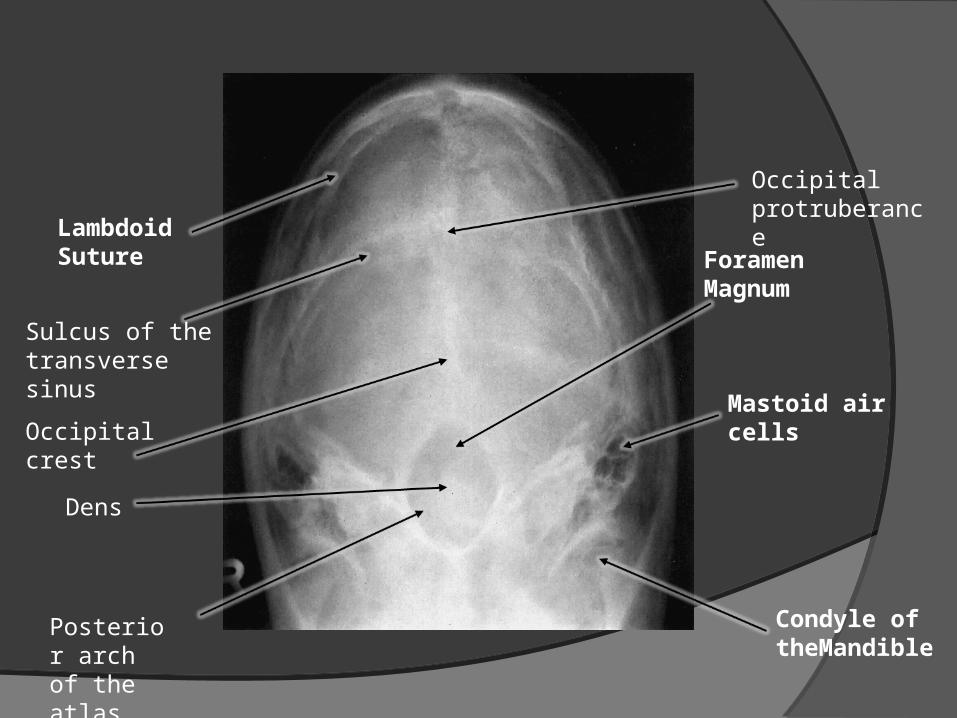
Lambdoid Suture Foramen
Magnum
Mastoid air cells
Condyle of theMandible
Dens
Posterior arch of the atlas
Occipital crest
Occipital protruberance
Sulcus of the transverse sinus
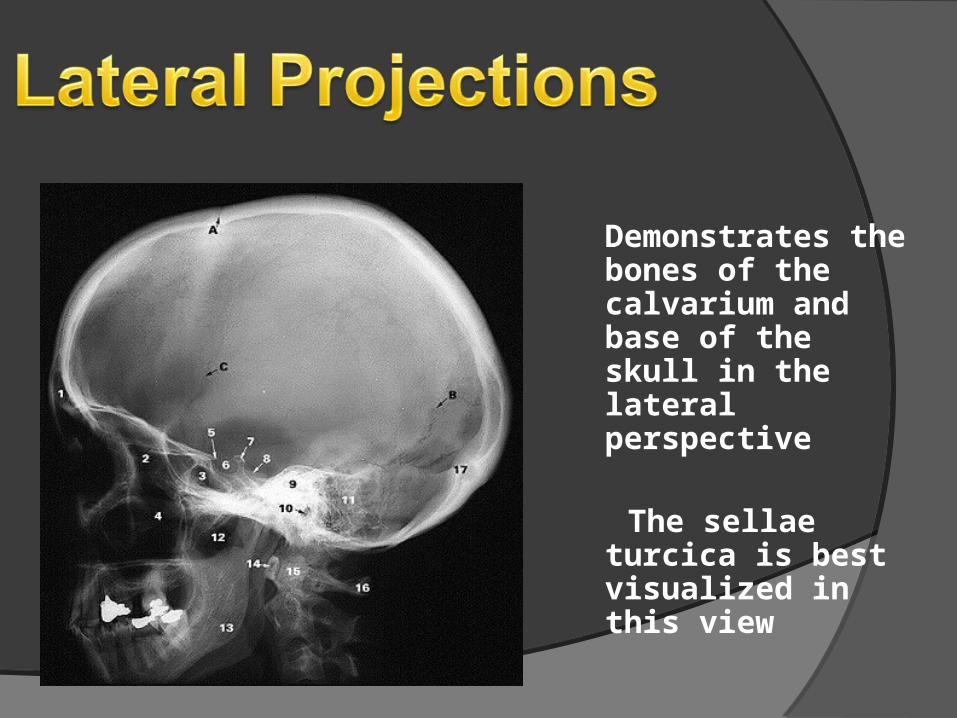
Demonstrates the bones of the calvarium and base of the skull in the lateral perspective
The sellae turcica is best visualized in this view
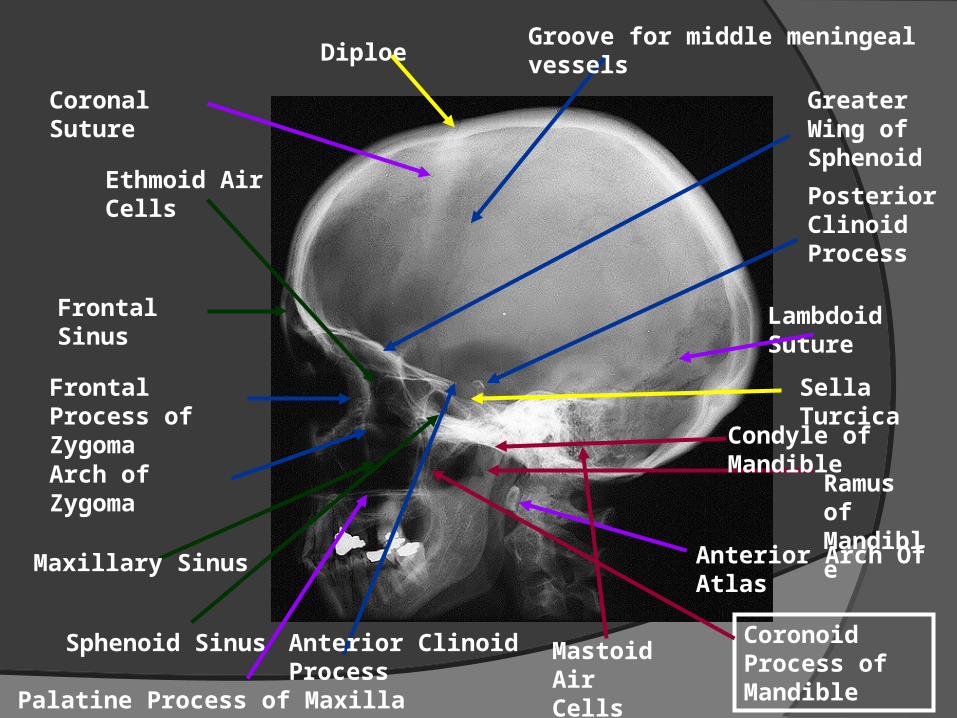
Diploe Groove for middle meningeal vessels
Lambdoid Suture
Frontal Sinus
Frontal Process of Zygoma
Arch of Zygoma
Ethmoid Air Cells
Sphenoid Sinus
Maxillary Sinus
Coronal Suture
Ramus of Mandible
Sella Turcica
Posterior Clinoid Process
Anterior Clinoid Process
Anterior Arch Of Atlas
Condyle of Mandible
Coronoid Process of Mandible
Greater Wing of Sphenoid
Mastoid Air Cells
Palatine Process of Maxilla
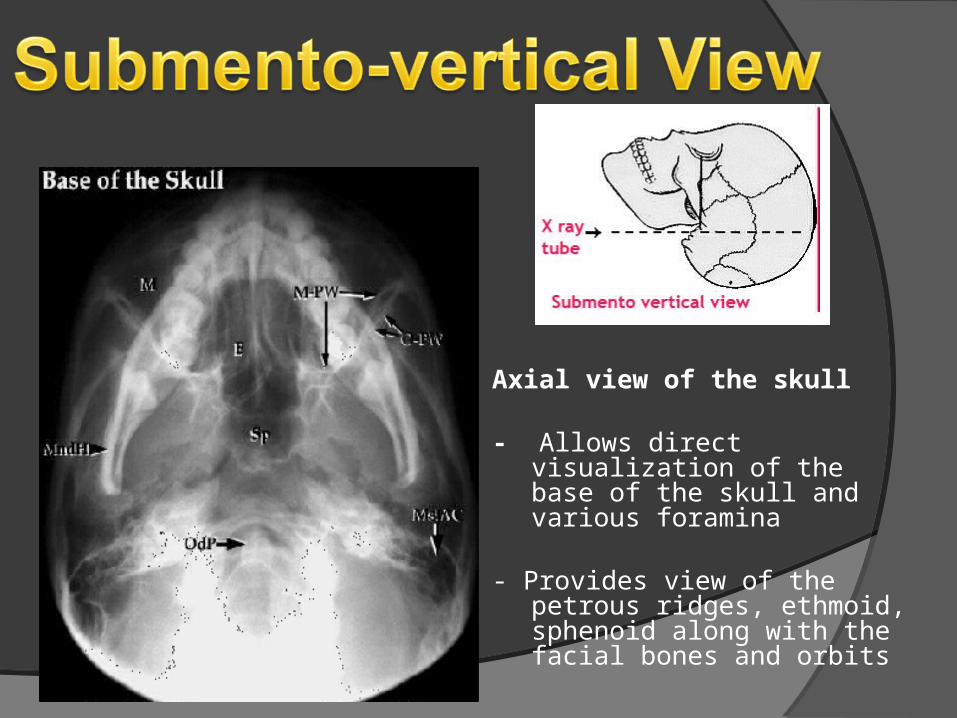
Axial view of the skull
- Allows direct visualization of the base of the skull and various foramina
- Provides view of the petrous ridges, ethmoid, sphenoid along with the facial bones and orbits
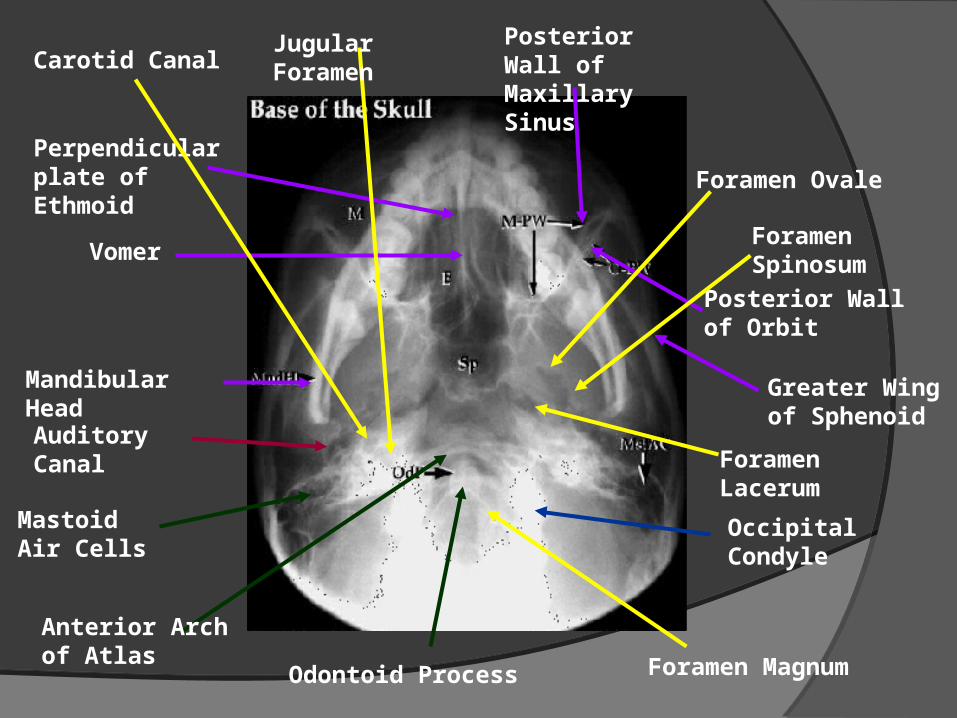
Occipital Condyle
Mastoid Air Cells
Posterior Wall of Maxillary Sinus
Posterior Wall of Orbit
Greater Wing of Sphenoid
Anterior Arch of Atlas
Odontoid Process Foramen Magnum
Perpendicular plate of Ethmoid
Vomer
Mandibular Head
Foramen Ovale
Foramen Spinosum
Foramen Lacerum
Auditory Canal
Carotid Canal Jugular Foramen
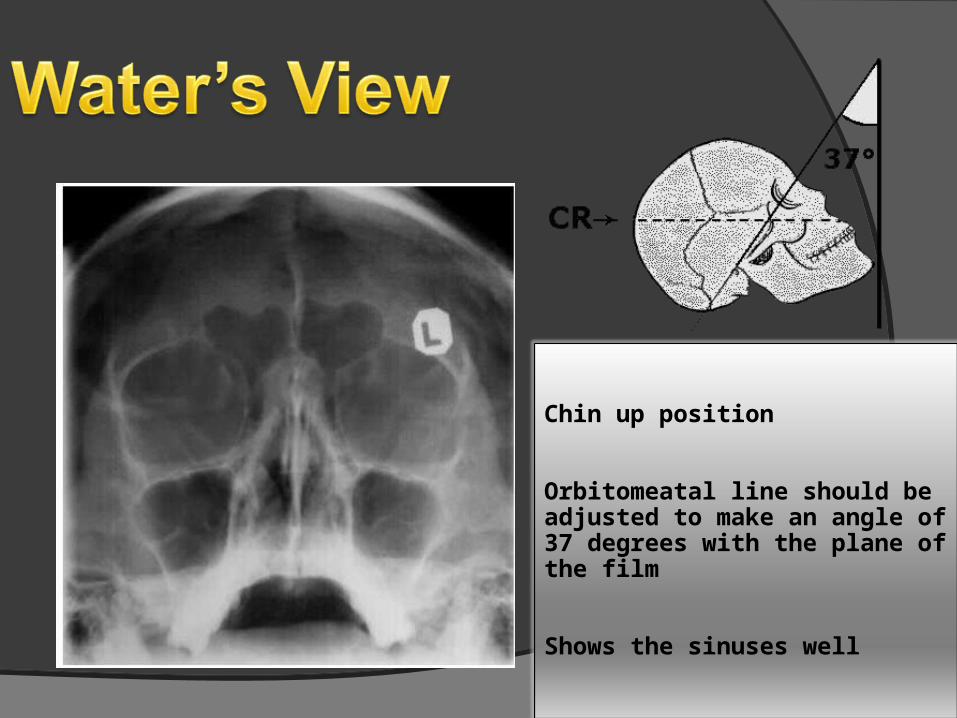
Chin up position
Orbitomeatal line should be adjusted to make an angle of 37 degrees with the plane of the film
Shows the sinuses well
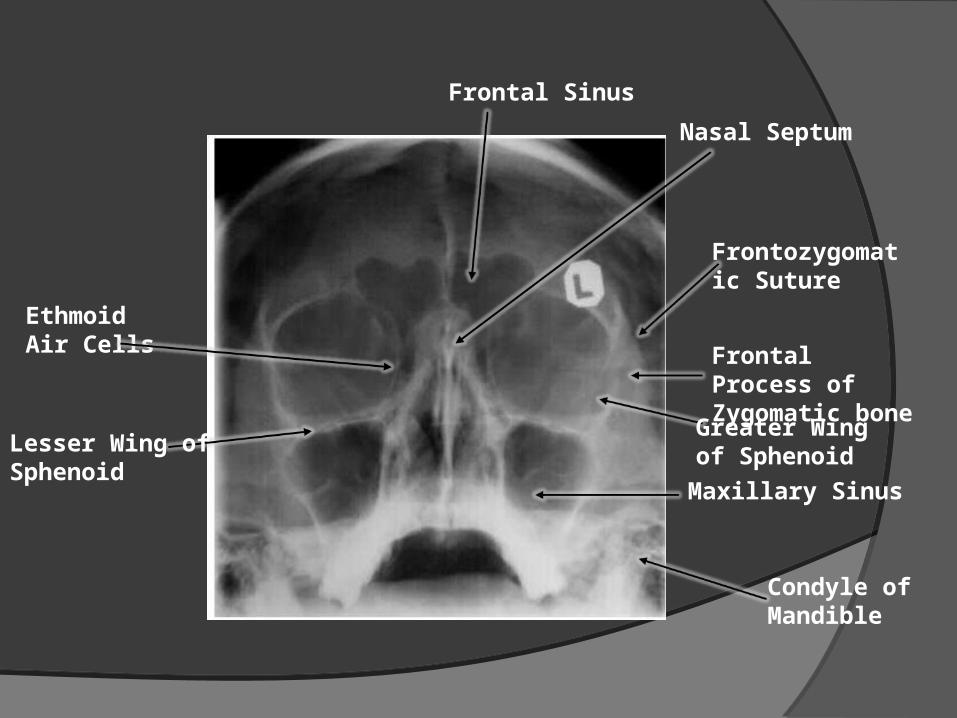
Frontal Sinus
Nasal Septum
Ethmoid Air Cells
Maxillary Sinus
Lesser Wing of Sphenoid
Greater Wing of Sphenoid
Frontal Process of Zygomatic bone
Frontozygomatic Suture
Condyle of Mandible
The Paranasal Sinuses
Paranasal Sinuses- are paired cavities lined by mucous
membrane (mucoperiosteum)
- arise as outpouchings from the nasal fossa
- extends into the maxillary, ethmoid, sphenoid and frontal bones
- named according to the bones in which they develop
Paranasal SinusesMethods of Examination:• Standard Positions
- Water’s (occipitomental) projection- Caldwell’s (occipitofrontal) position- Lateral position- Submentovertical (SMV) projection
• Special Methods– Contrast studies– Tomography– Computerized Tomography
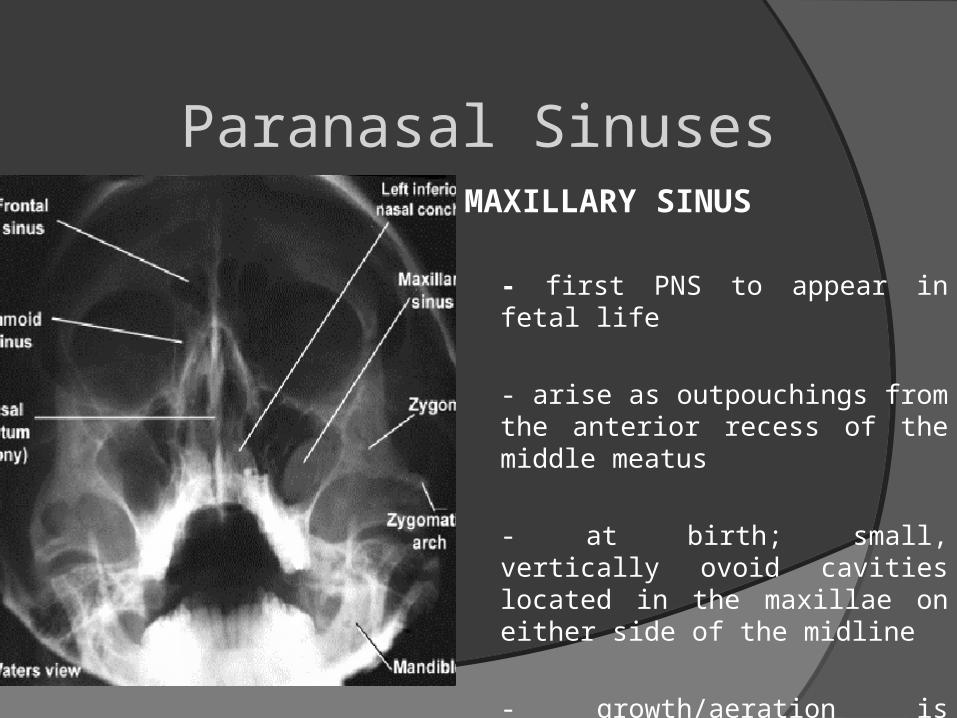
Paranasal SinusesMAXILLARY SINUS
- first PNS to appear in fetal life
- arise as outpouchings from the anterior recess of the middle meatus
- at birth; small, vertically ovoid cavities located in the maxillae on either side of the midline
- growth/aeration is complete at 12 years of age
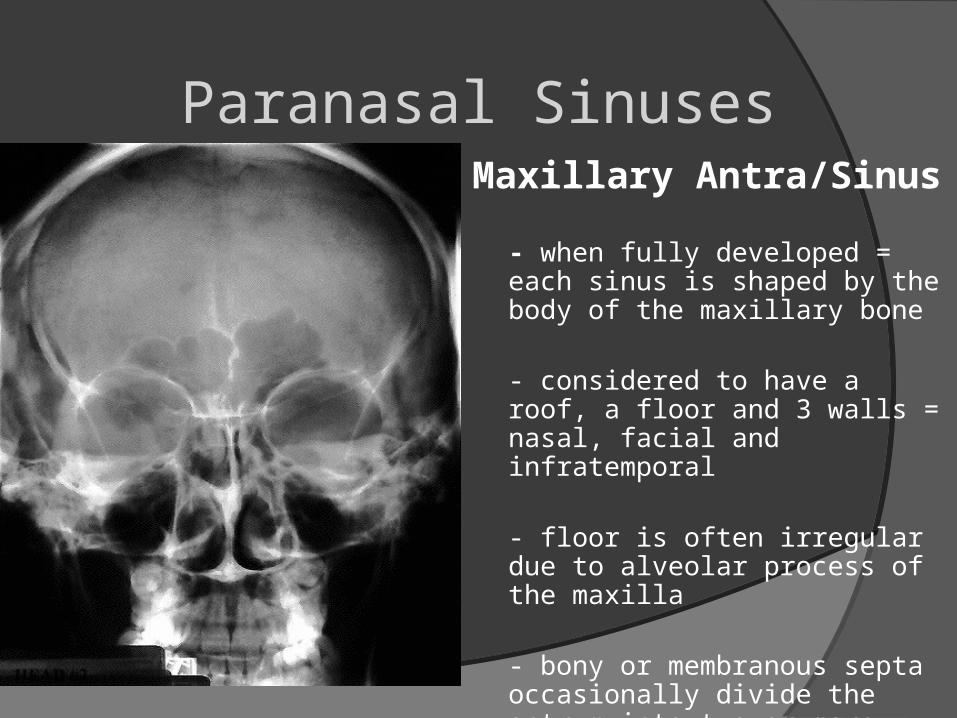
Paranasal SinusesMaxillary Antra/Sinus
- when fully developed = each sinus is shaped by the body of the maxillary bone
- considered to have a roof, a floor and 3 walls = nasal, facial and infratemporal
- floor is often irregular due to alveolar process of the maxilla
- bony or membranous septa occasionally divide the antrum into two or more compartments
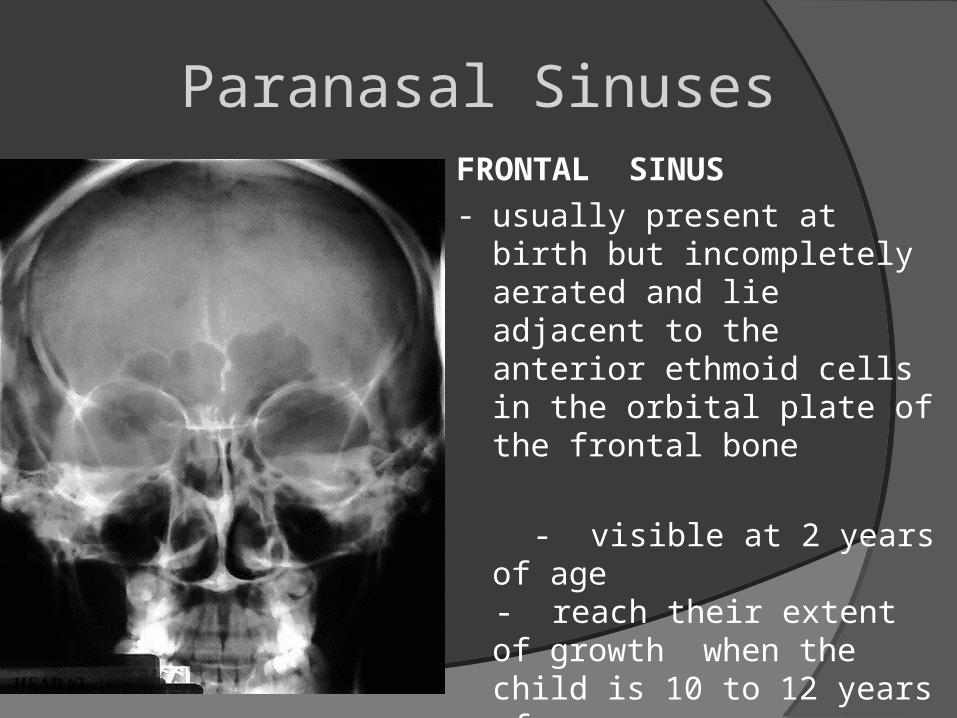
Paranasal SinusesFRONTAL SINUS- usually present at birth but
incompletely aerated and lie adjacent to the anterior ethmoid cells in the orbital plate of the frontal bone
- visible at 2 years of age - reach their extent of growth
when the child is 10 to 12 years of age
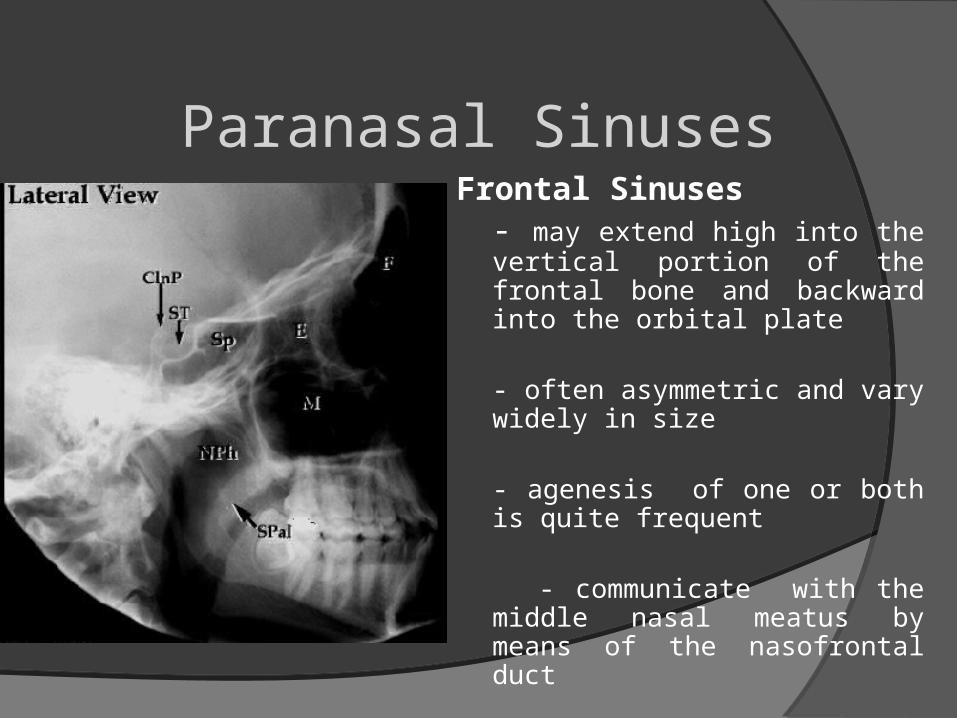
Paranasal SinusesFrontal Sinuses
- may extend high into the vertical portion of the frontal bone and backward into the orbital plate
- often asymmetric and vary widely in size
- agenesis of one or both is quite frequent
- communicate with the middle nasal meatus by means of the nasofrontal duct
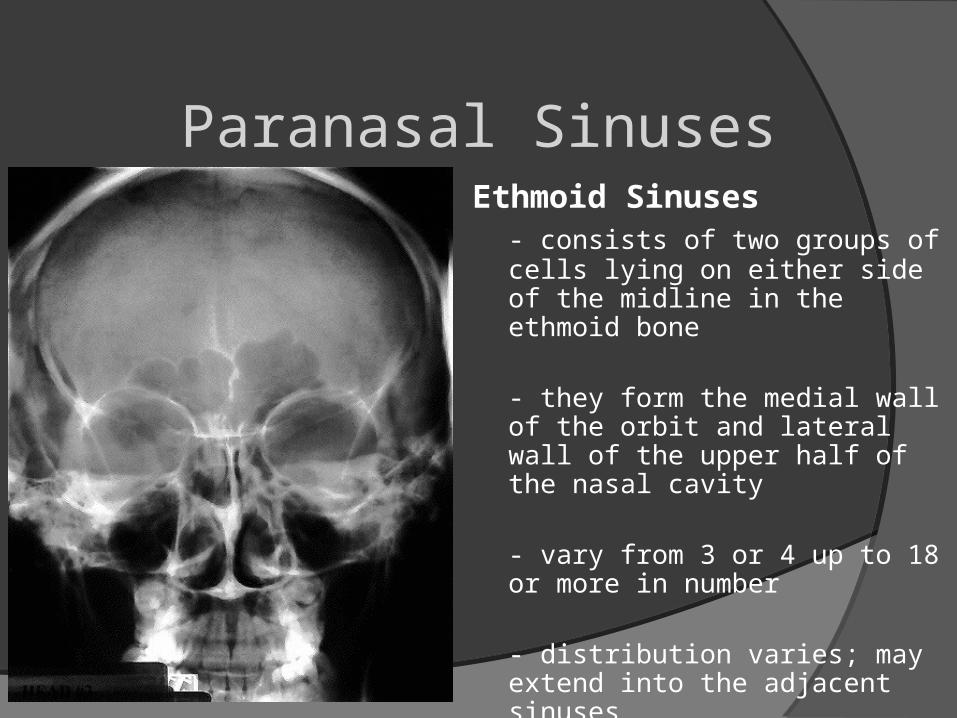
Paranasal SinusesEthmoid Sinuses
- consists of two groups of cells lying on either side of the midline in the ethmoid bone
- they form the medial wall of the orbit and lateral wall of the upper half of the nasal cavity
- vary from 3 or 4 up to 18 or more in number
- distribution varies; may extend into the adjacent sinuses
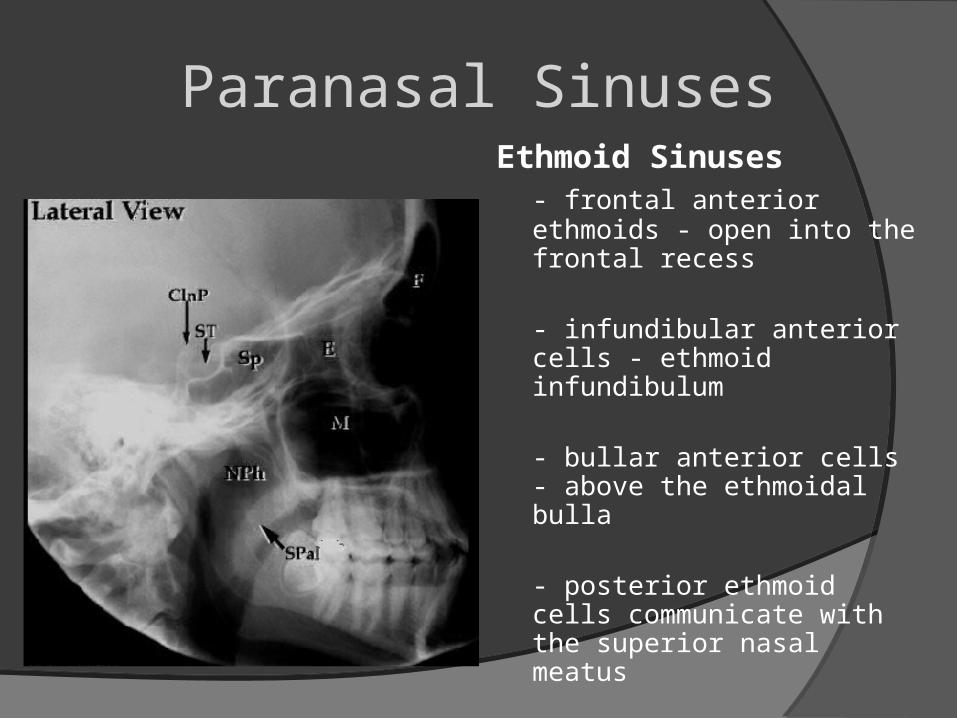
Paranasal SinusesEthmoid Sinuses
- frontal anterior ethmoids - open into the frontal recess
- infundibular anterior cells - ethmoid infundibulum
- bullar anterior cells - above the ethmoidal bulla
- posterior ethmoid cells communicate with the superior nasal meatus
- fully developed at 10 to 12 years of age
Paranasal Sinuses
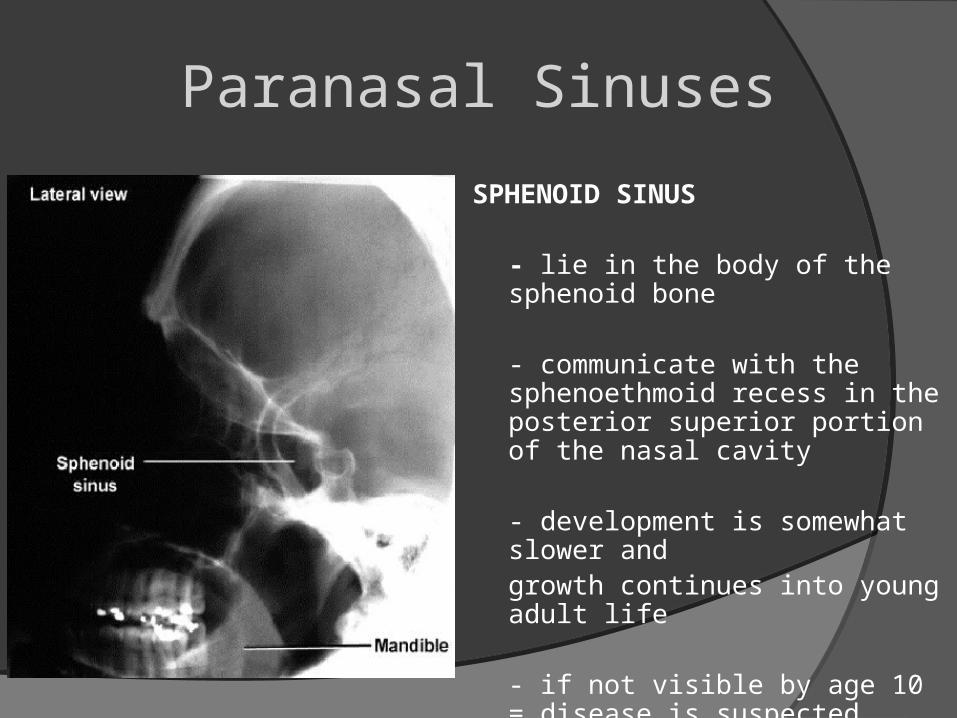
SPHENOID SINUS
- lie in the body of the sphenoid bone
- communicate with the sphenoethmoid recess in the posterior superior portion of the nasal cavity
- development is somewhat slower andgrowth continues into young adult life
- if not visible by age 10 = disease is suspected

The Mastoids
Mastoids
- important in the diagnosis of middle ear and mastoid diseases
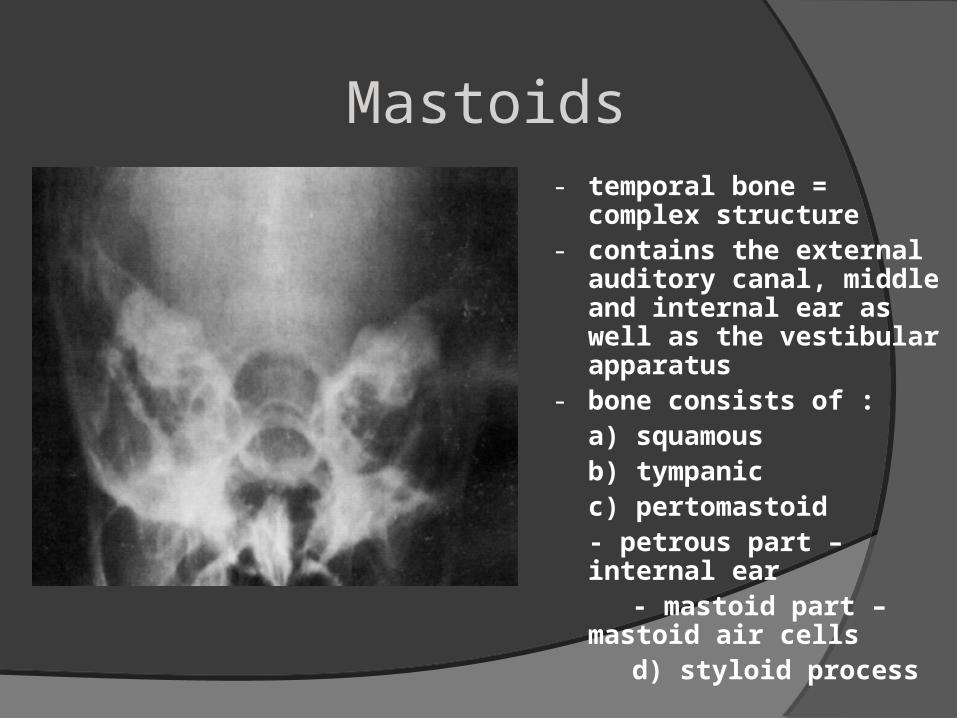
Mastoids- temporal bone = complex
structure- contains the external
auditory canal, middle and internal ear as well as the vestibular apparatus
- bone consists of : a) squamousb) tympanicc) pertomastoid- petrous part – internal ear
- mastoid part – mastoid air cells
d) styloid process
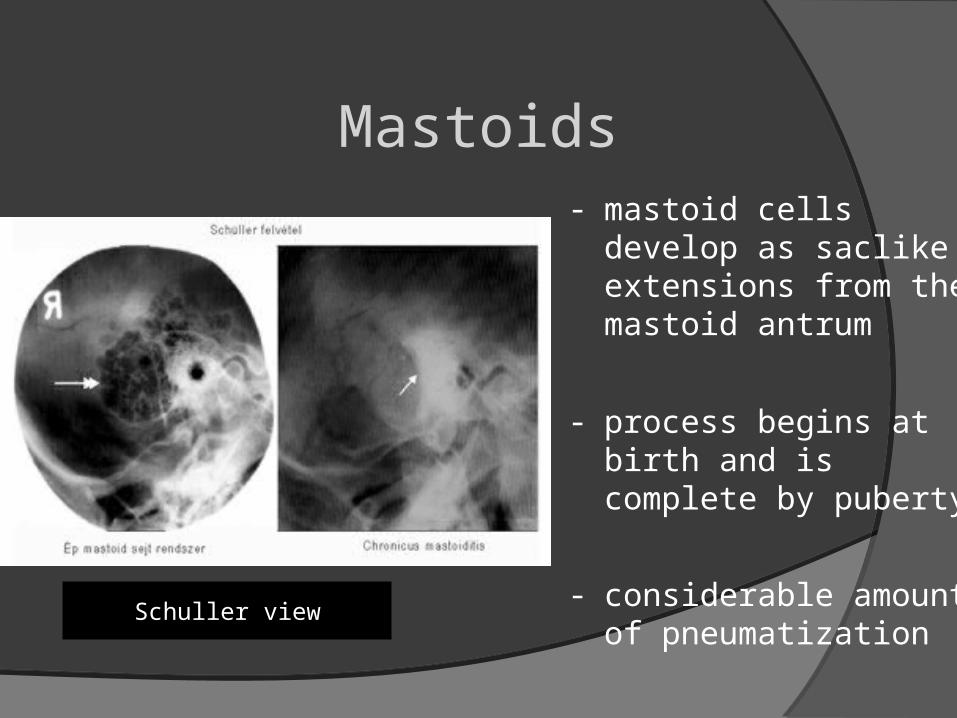
Mastoids- mastoid cells develop as
saclike extensions from the mastoid antrum
- process begins at birth and is complete by puberty
- considerable amount of pneumatization
Schuller view
Xray of the Orbits
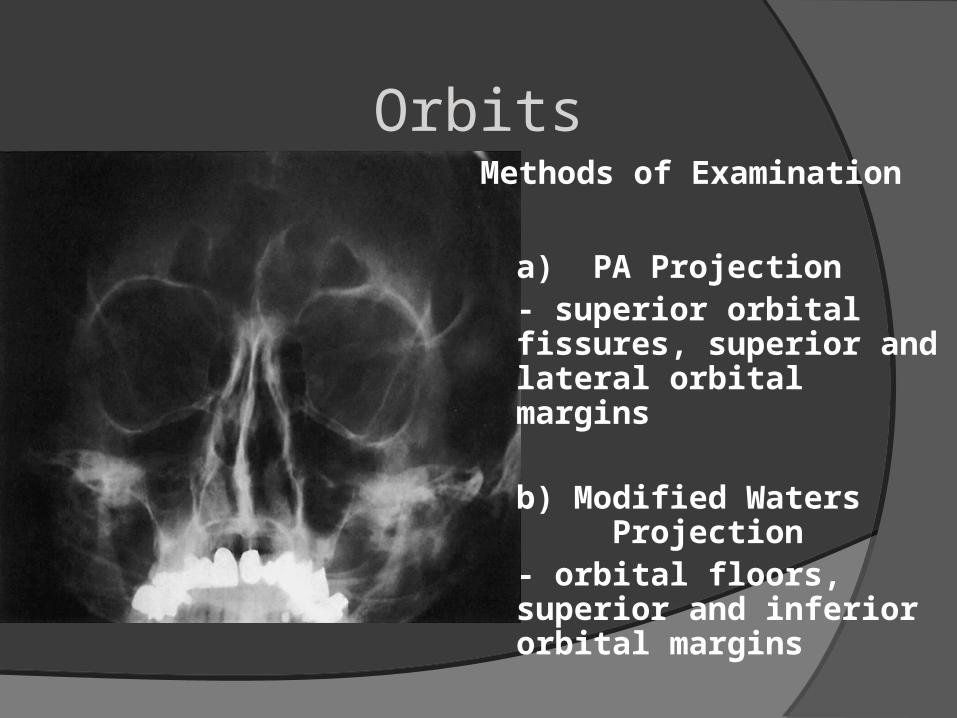
OrbitsMethods of Examination
a) PA Projection - superior orbital fissures, superior and lateral orbital margins
b) Modified Waters Projection- orbital floors, superior and inferior orbital margins
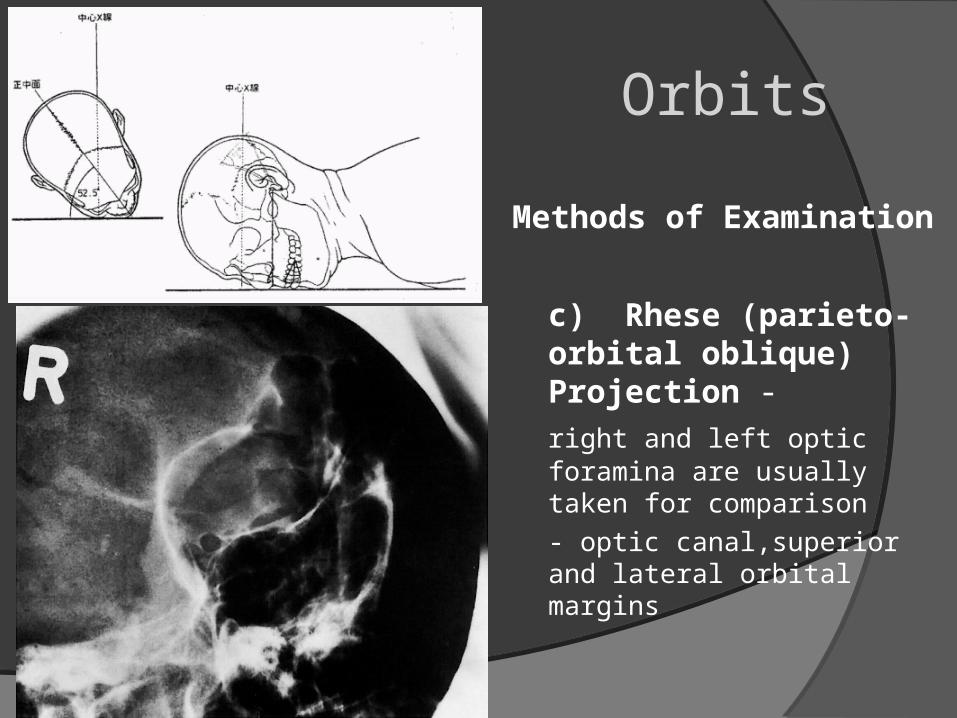
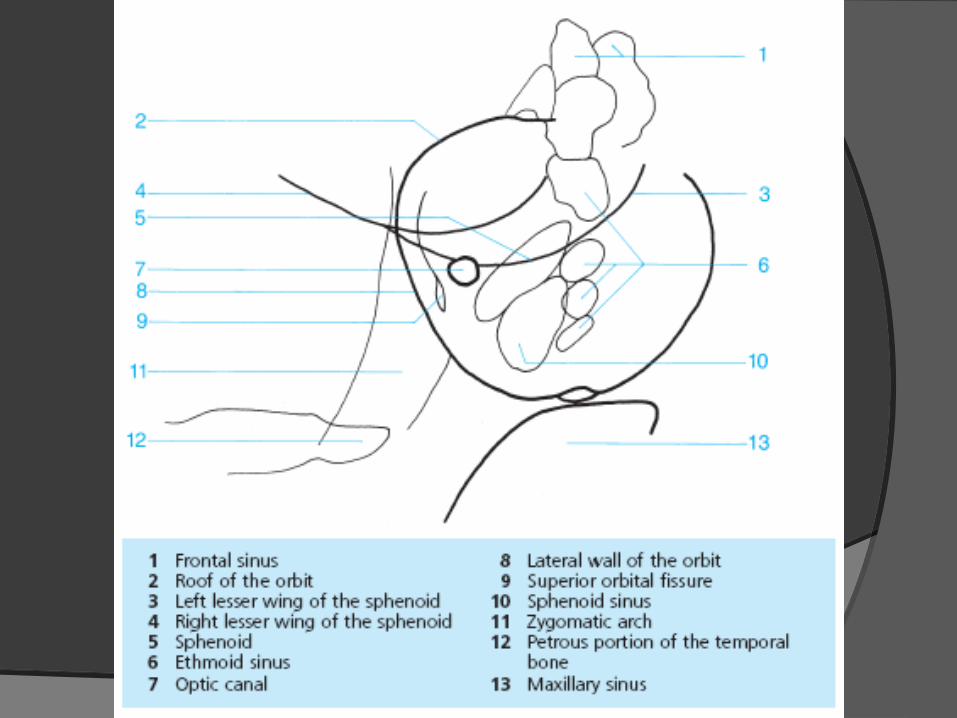
Orbits
Methods of Examination
c) Rhese (parieto-orbital oblique) Projection -
right and left optic foramina are usually taken for comparison
- optic canal,superior and lateral orbital margins

THE Nasal Bone
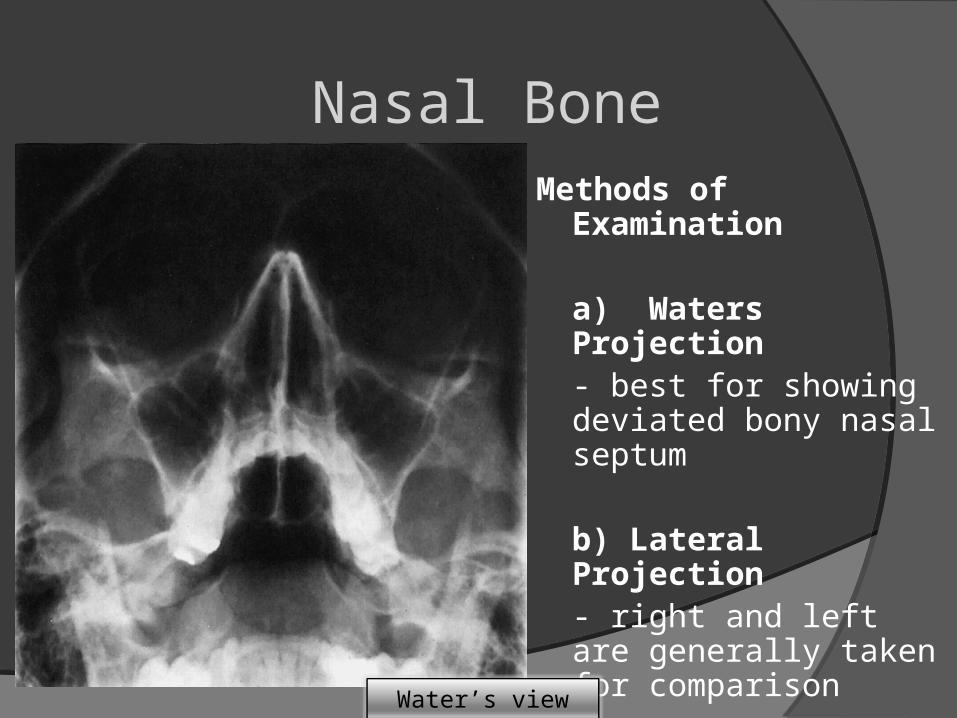
Nasal BoneMethods of Examination
a) Waters Projection - best for showing deviated bony nasal septum
b) Lateral Projection- right and left are generally taken for comparison
Water’s view
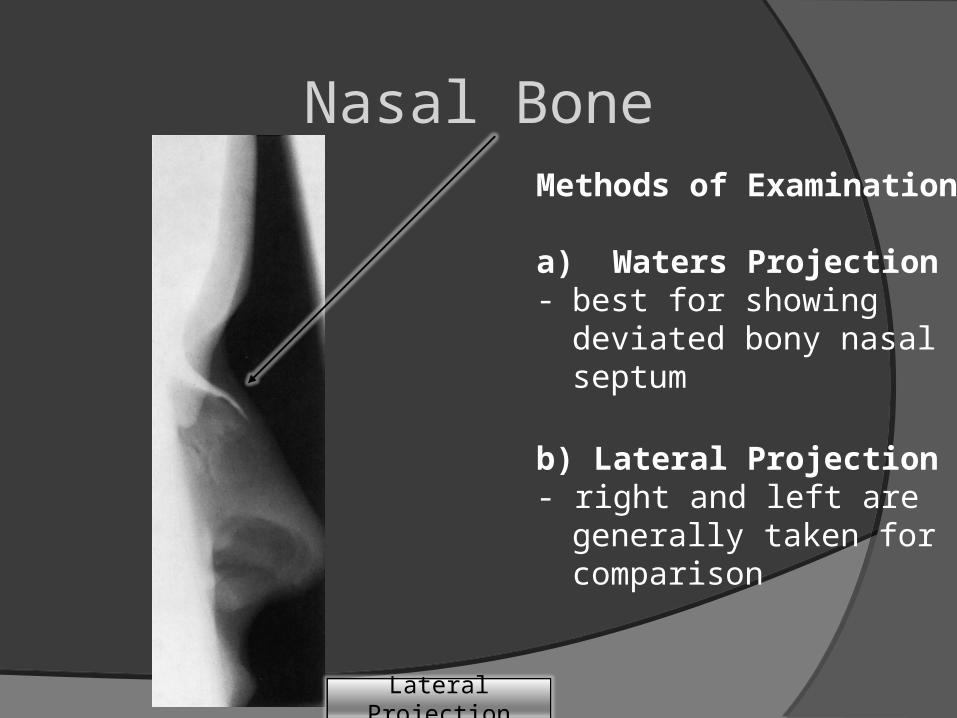
Nasal BoneMethods of Examination
a) Waters Projection - best for showing deviated
bony nasal septum
b) Lateral Projection- right and left are generally
taken for comparison
Lateral Projection
The Facial Bones
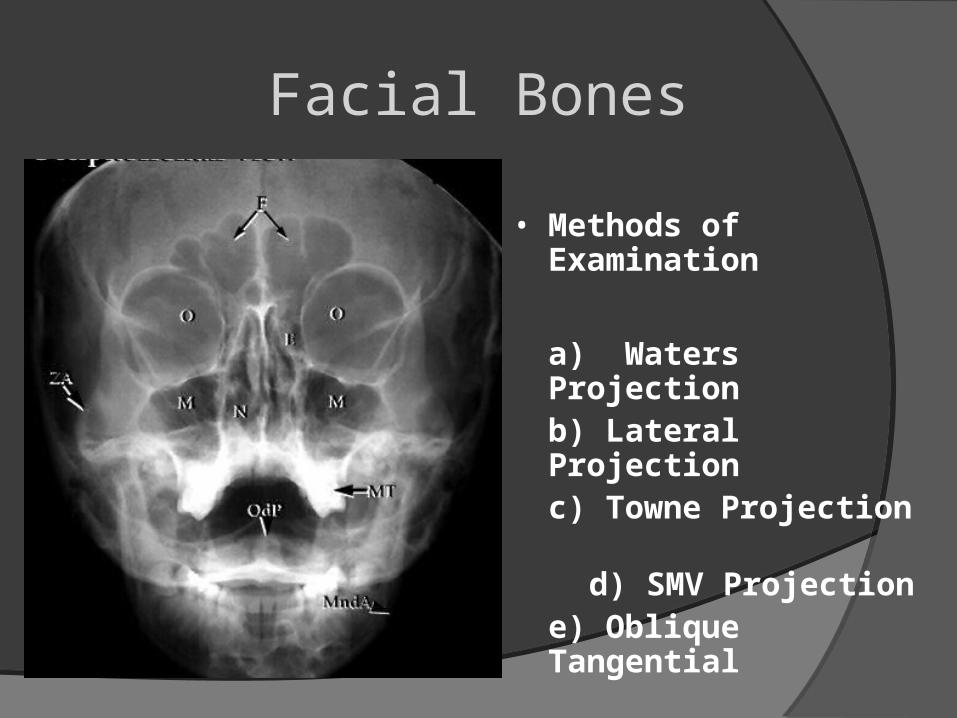
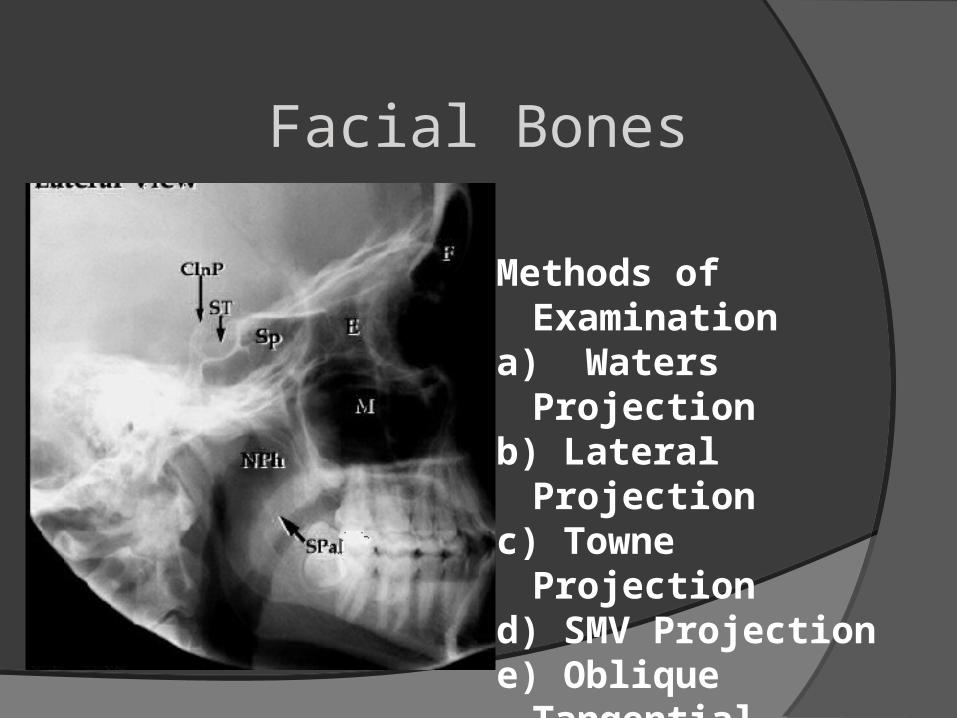
Facial Bones
• Methods of Examination
a) Waters Projection b) Lateral Projectionc) Towne Projection
d) SMV Projectione) Oblique Tangential
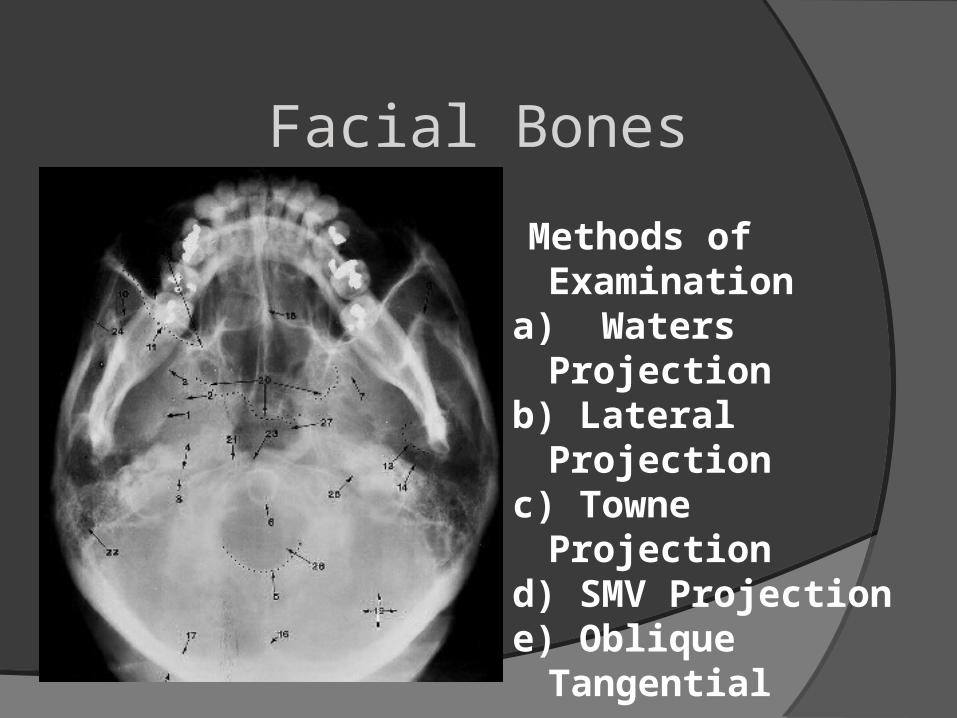
Facial Bones
Methods of Examination
a) Waters Projection b) Lateral Projectionc) Towne Projection d) SMV Projectione) Oblique Tangential
Facial Bones
Methods of Examination
a) Waters Projection b) Lateral Projectionc) Towne Projection d) SMV Projectione) Oblique Tangential
Facial Bones
Methods of Examinationa) Waters Projection b) Lateral Projectionc) Towne Projection d) SMV Projectione) Oblique Tangential
The Mandible
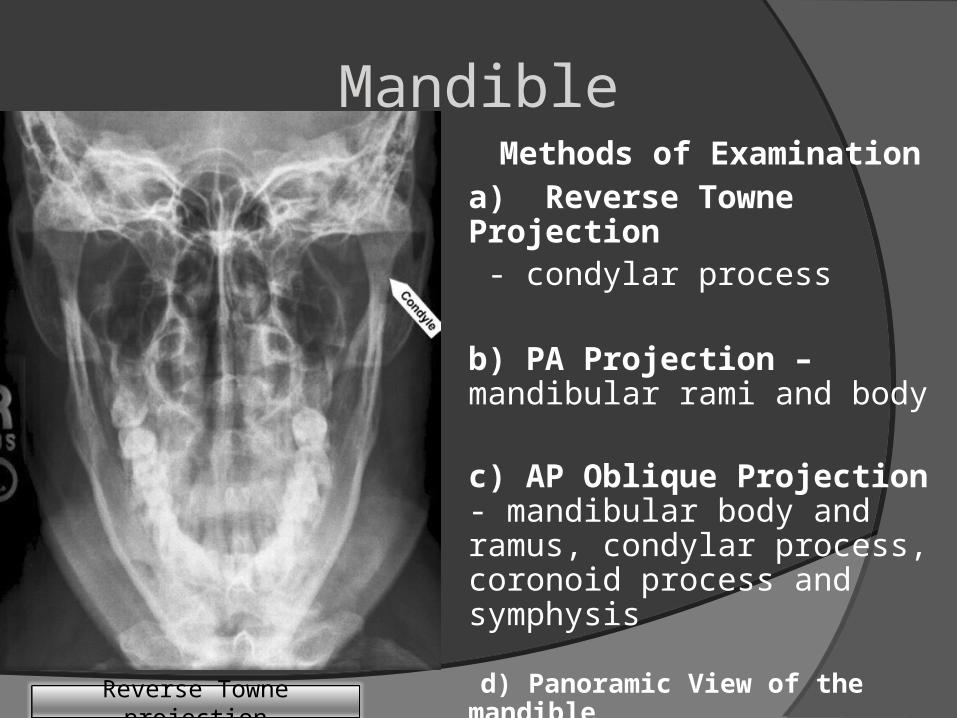
Mandible Methods of Examination
a) Reverse Towne Projection - condylar process
b) PA Projection – mandibular rami and body
c) AP Oblique Projection - mandibular body and ramus, condylar process, coronoid process and symphysis
d) Panoramic View of the mandible
Reverse Towne projection
Mandible
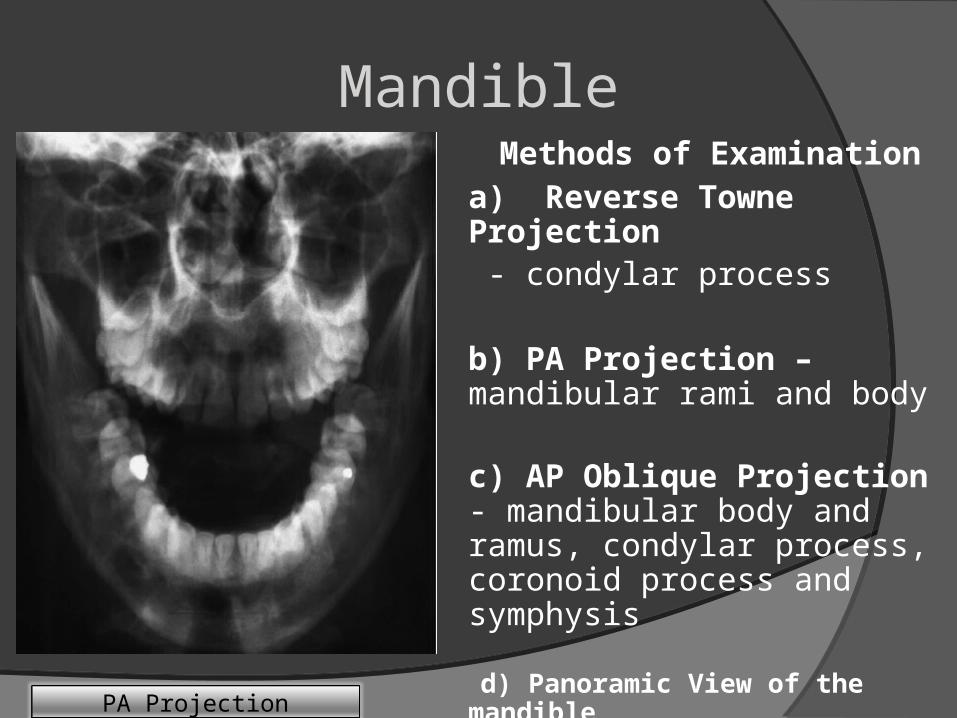
PA Projection
Methods of Examinationa) Reverse Towne Projection - condylar process
b) PA Projection – mandibular rami and body
c) AP Oblique Projection - mandibular body and ramus, condylar process, coronoid process and symphysis
d) Panoramic View of the mandible
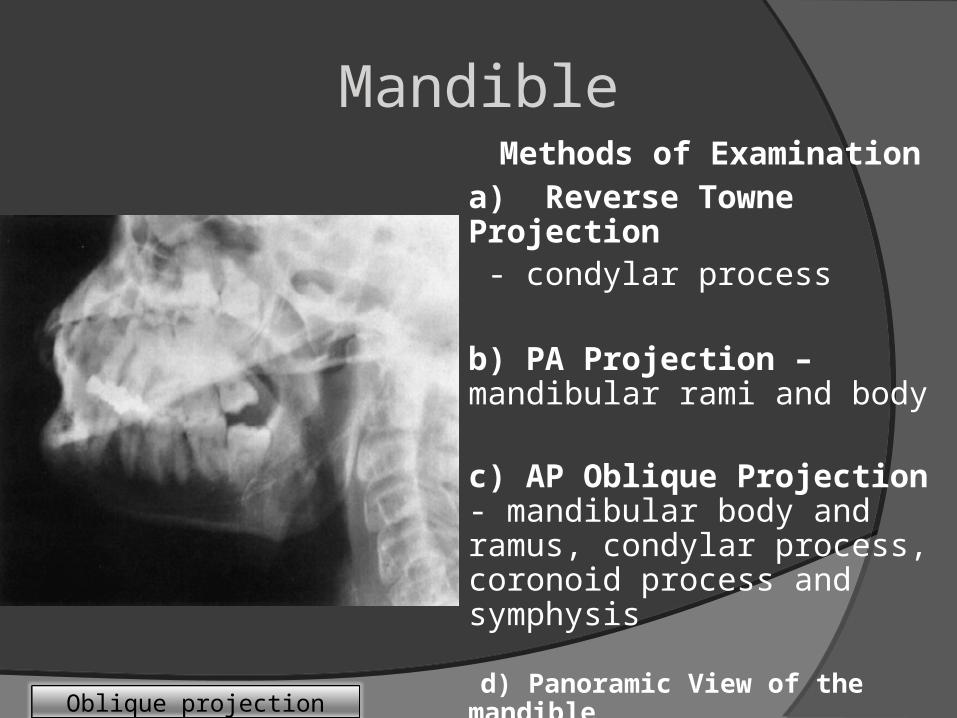
Mandible
Oblique projection
Methods of Examinationa) Reverse Towne Projection - condylar process
b) PA Projection – mandibular rami and body
c) AP Oblique Projection - mandibular body and ramus, condylar process, coronoid process and symphysis
d) Panoramic View of the mandible
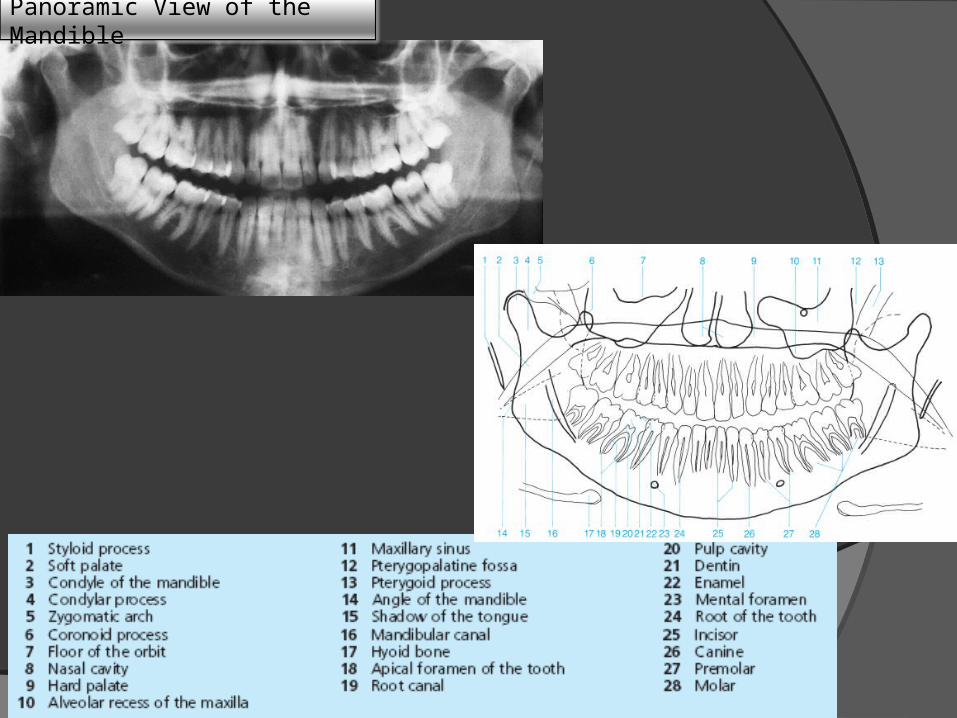
Panoramic View of the Mandible
The Temporomandibular Joints
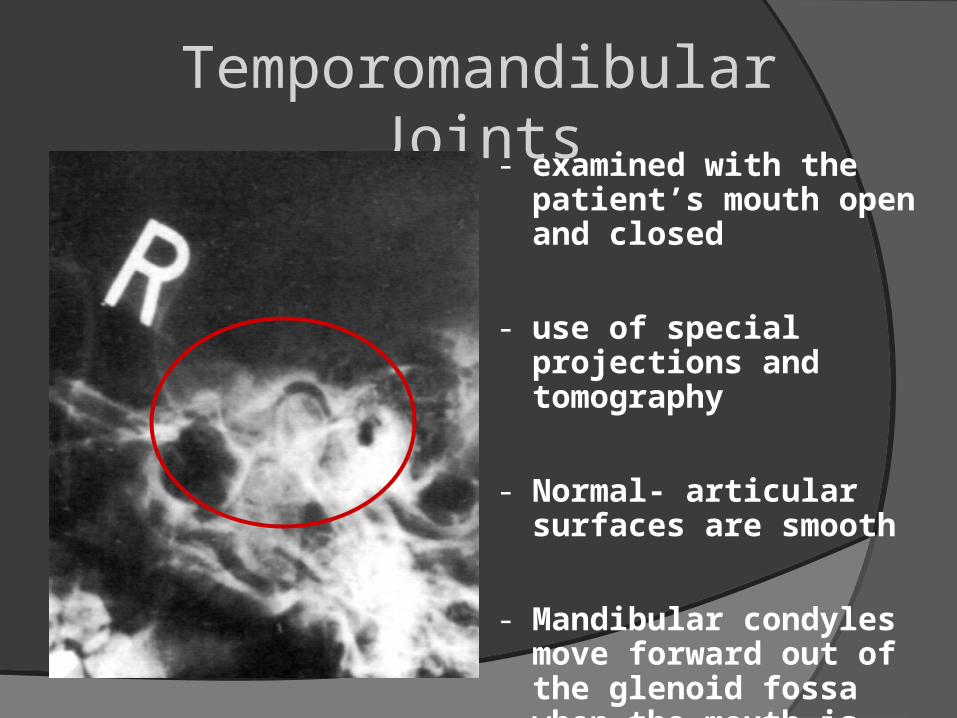
Temporomandibular Joints- examined with the
patient’s mouth open and closed
- use of special projections and tomography
- Normal- articular surfaces are smooth
- Mandibular condyles move forward out of the glenoid fossa when the mouth is open
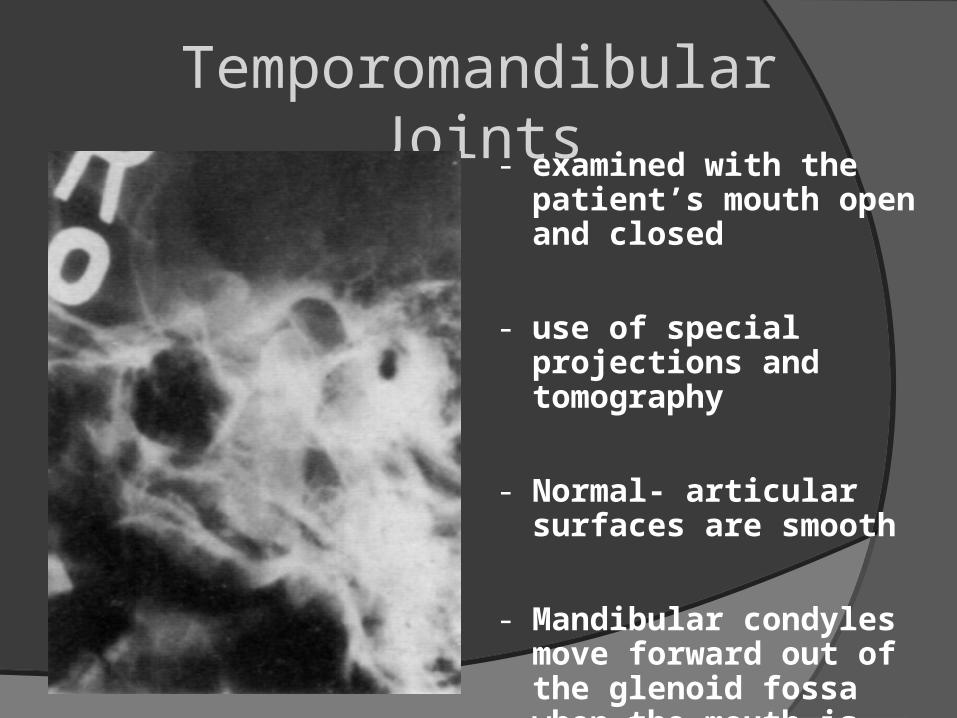
Temporomandibular Joints- examined with the
patient’s mouth open and closed
- use of special projections and tomography
- Normal- articular surfaces are smooth
- Mandibular condyles move forward out of the glenoid fossa when the mouth is open
This 11-month old infant fell and struck his head on a hard surface This 11-month old infant fell and struck his head on
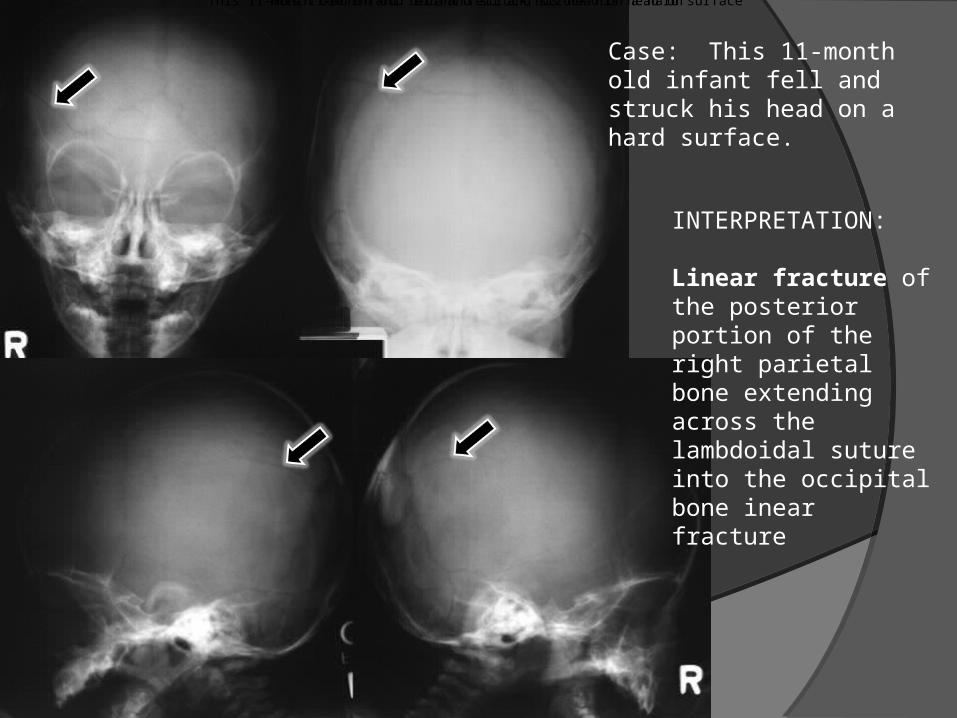
Case: This 11-month old infant fell and struck his head on a hard surface.
INTERPRETATION:
Linear fracture of the posterior portion of the right parietal bone extending across the lambdoidal suture into the occipital bone inear fracture
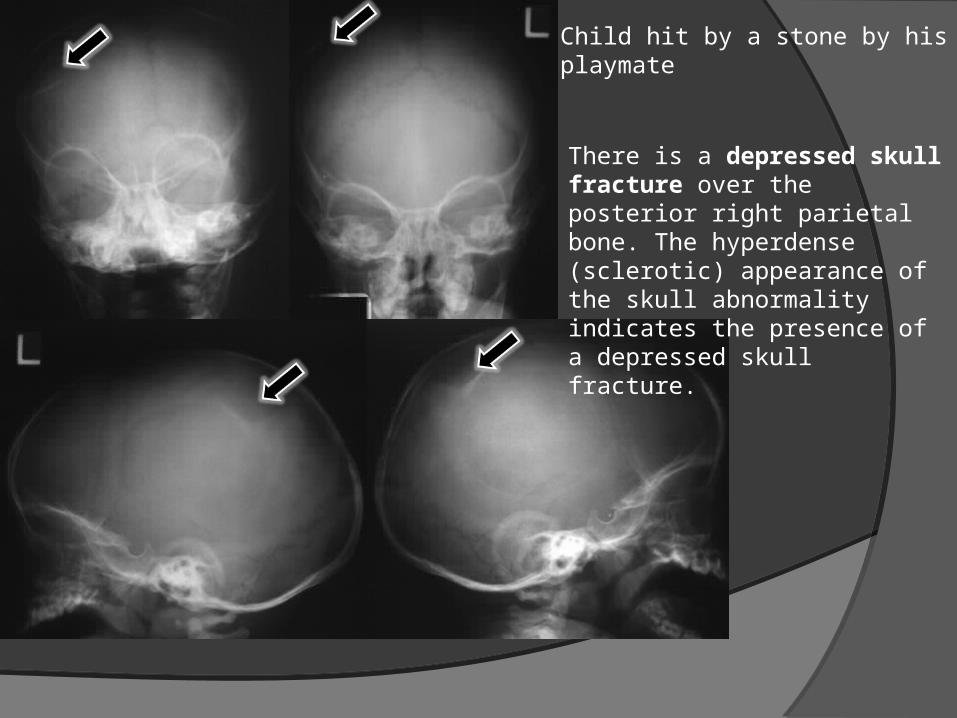
There is a depressed skull fracture over the posterior right parietal bone. The hyperdense (sclerotic) appearance of the skull abnormality indicates the presence of a depressed skull fracture.
Child hit by a stone by his playmate
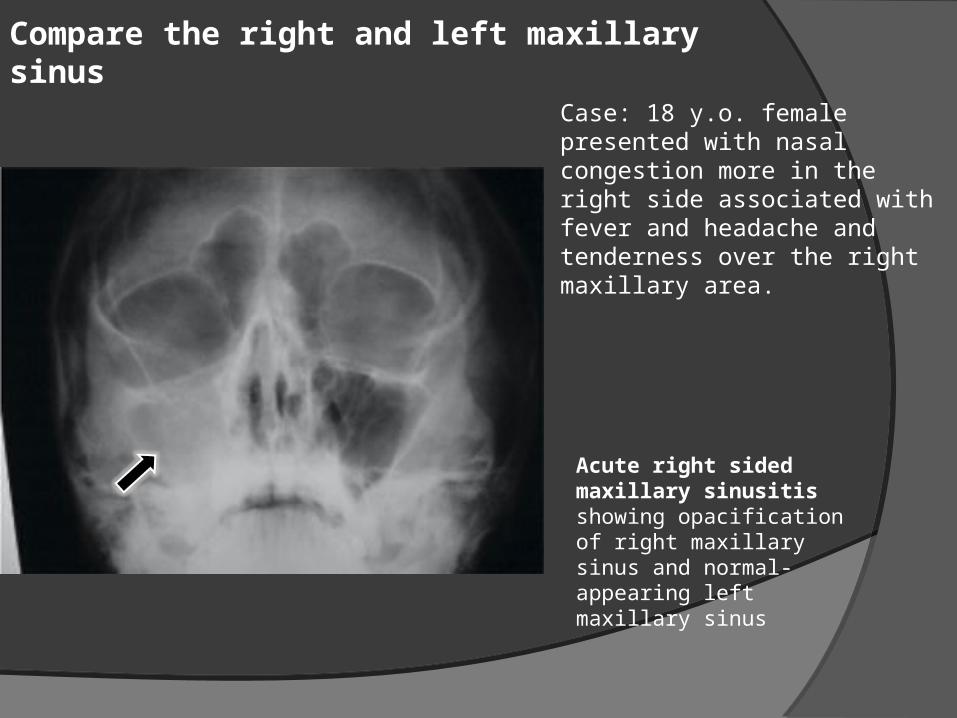
Case: 18 y.o. female presented with nasal congestion more in the right side associated with fever and headache and tenderness over the right maxillary area.
Acute right sided maxillary sinusitis showing opacification of right maxillary sinus and normal-appearing left maxillary sinus
Compare the right and left maxillary sinus

Case: 22 y.o. male involved in a motorcycle accident (no helmet). Identify the fractured parts of the mandible?
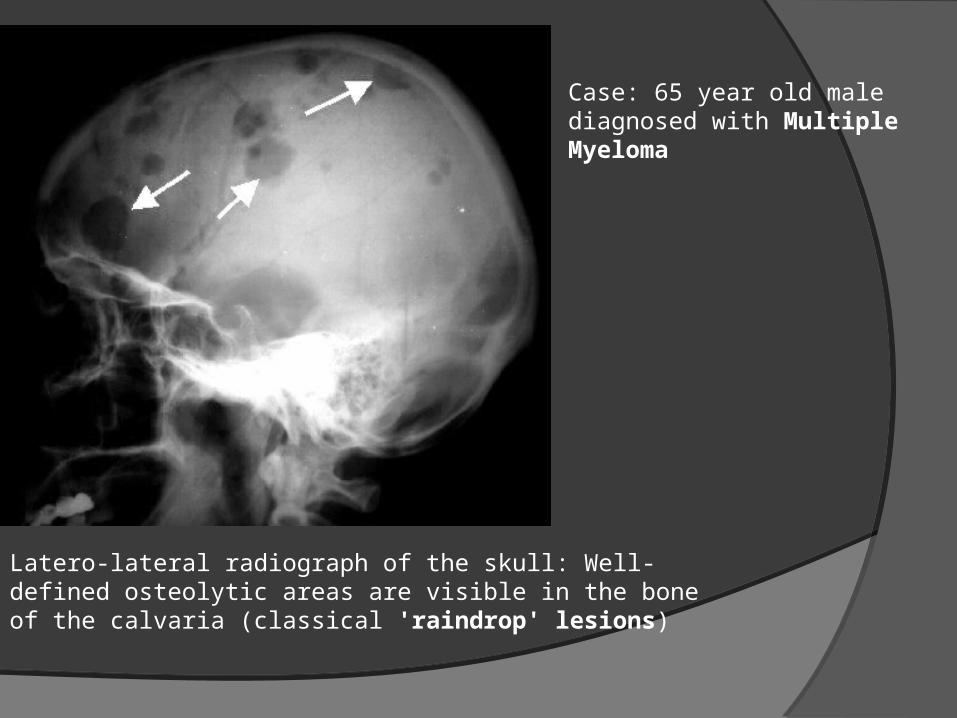
Latero-lateral radiograph of the skull: Well-defined osteolytic areas are visible in the bone of the calvaria (classical 'raindrop' lesions)
Case: 65 year old male diagnosed with Multiple Myeloma
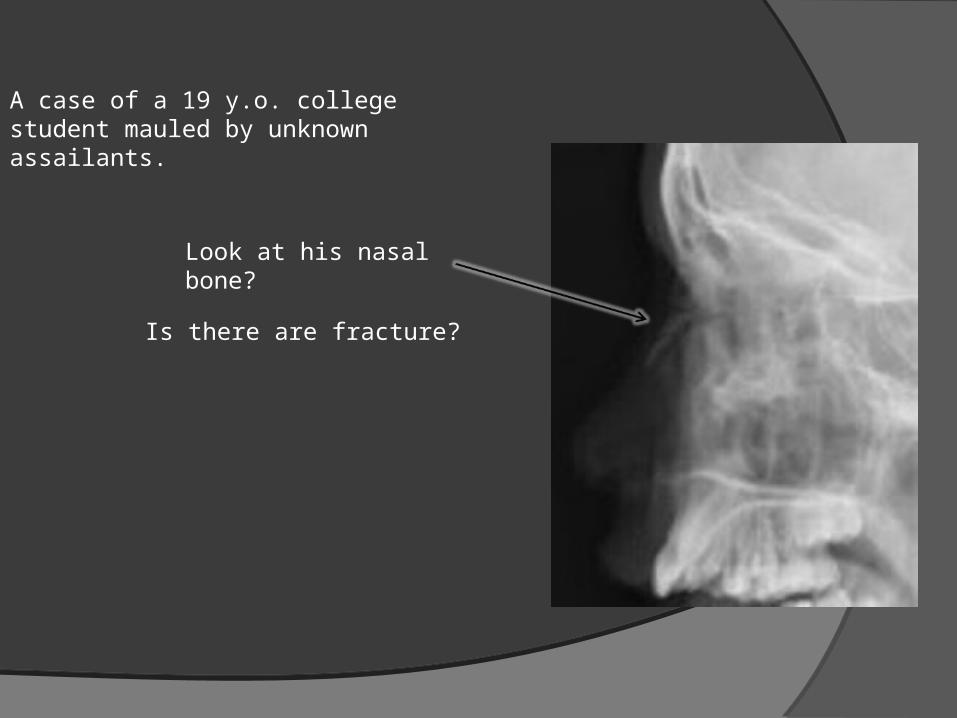
A case of a 19 y.o. college student mauled by unknown assailants.
Look at his nasal bone?
Is there are fracture?