-
Clinical Pediatrics51(11) 1079 1086 The Author(s) 2012Reprints
and permission: sagepub.com/journalsPermissions.navDOI:
10.1177/0009922812461069http://cpj.sagepub.com
Introduction
The morbidity and mortality conference (MMC) has long been a
forum for discussing adverse outcomes in the academic medical
setting.1 The Accreditation Council for Graduate Medical Education
(ACGME) has recognized the educational value of resident
participa-tion in systematically analyzing practice and
imple-menting changes with the goal of practice improvement.2 The
format and methods by which cases are identified, presented, and
discussed vary widely among training programs and disciplines
across the United States and Canada3,4 and even within our own
institution.5
Although much has been published about both tradi-tional and
innovative uses of the MMC in internal medi-cine,1,3,6 emergency
medicine,7-11 surgery,12-25 and other disciplines as a forum for
highlighting the core compe-tencies of ACGMEs and quality
improvement,12-14,26-29 there is a paucity of literature about the
role of the MMC in pediatrics.4,30 At the Johns Hopkins Childrens
Center, the MMC had become very similar to the weekly case
management conference in which interesting and instructive cases
were discussed by faculty members with, primarily, residents and
medical students in atten-dance. The nature and source of the
morbidity and/or mortality were often difficult to ascertain.
Without a unifying philosophy, these sessions did not produce
effective or lasting solutions.
We hypothesized that by clearly identifying goals for the MMC
and empowering those involved to reach these goals, we could create
a constructive venue for quality improvement and a vehicle for
initiating system change. We restructured the conference to
encourage discussions
461069 CPJXXX10.1177/0009922812461069Clinical
PediatricsRabizadeh et al
1Cedars-Sinai Medical Center, Los Angeles, CA, USA2Wake Forest
School of Medicine, Winston-Salem, NC, USA 3Johns Hopkins School of
Medicine, Baltimore, MD, USA4Vanderbilt University, Nashville, TN,
USA
Corresponding Author:Shervin Rabizadeh, Cedars-Sinai Medical
Center, 8635 W 3rd Street, Suite 1165W, Los Angeles, CA 90077, USA
Email: [email protected]
Restructuring the Morbidity and Mortality Conference in a
Department of Pediatrics to Serve as a Vehicle for System
Changes
Shervin Rabizadeh, MD, MBA1, W. Adam Gower, MD2, Kurlen Payton,
MD1, Kathryn Miller, BS3, Kimberly Vera, MD, MSCI4, and Janet R.
Serwint, MD3
Abstract
Purpose. Morbidity and mortality conference (MMC) serves an
important role in medical care and education. We restructured our
Department of Pediatrics MMC to focus on multidisciplinary
participation and improved communication among disciplines, quality
improvement, and system changes for safer clinical care and
enhanced learning from adverse outcomes. Method. The structure and
philosophy of the Department of Pediatrics MMC was changed. We
present guiding principles for the restructuring process and
evaluation results postrestructuring, which examined achievement of
conference goals, including quality improvement. Results. The MMC
led to system changes within the Department of Pediatrics as well
as other parts of the hospital. Satisfaction with these changes was
high among conference participants, who felt that the conference
achieved its goals of including multiple disciplines and creating
system changes. Conclusions. The successful change in the focus of
the pediatric MMC conference resulted in significant hospital-wide
system changes, quality improvements, enhanced education, and
departmental satisfaction.
Keywords
morbidity, mortality, system changes, multidisciplinary
-
1080 Clinical Pediatrics 51(11)
about avoiding adverse events by focusing less on the roles of
individuals in the event and more on the system and team management
environment that enabled such events. We anticipated that shifting
the focus of discus-sion away from individual management would
encour-age increased attendance and participation at the conference
while providing a venue for initiating change through open
dialogue, with the goal of preventing future morbidity and
mortality (M&M). We emphasized the importance of including all
disciplines in discussions about enacting system changes. In
addition, we felt that this could be an effective way to empower
residents to take the lead in identifying areas for quality
improvement in the Childrens Center and marshalling the resources
necessary for enacting change. The purpose of this article is to
(1) describe how our department changed the format and philosophy
of our MMC to address systems issues, (2) describe content from the
conferences during the first 2 years following this change, and (3)
present evaluation data from surveys collected from faculty,
residents, and hospital staff about the perceived effectiveness and
satis-faction with this new approach.
MethodsNew Conference Format
The Johns Hopkins Department of Pediatrics MMC is an hour-long
continuing medical education (CME) approved twice monthly
conference. Our revised goals for this conference were to (1)
identify events resulting in adverse patient outcomes, (2) create
and participate in a forum in which health care providers
acknowledge and address reasons for medical errors, (3) modify
behavior and judgments by learning from past adverse events, (4)
address educational and systematic flaws that led to adverse
outcomes, and (5) identify a group to engineer the identified
needed changes and quality improvement. The conferences are
attended by Department of Pediatrics faculty, fellows, residents,
and medical students as well as representatives from other
disciplines, including nurs-ing, pharmacy, social work, child life,
pediatric surgical subspecialties, and other interested parties. If
the case involves other departments, such as surgery or obstetrics
and gynecology, invitations are extended to representa-tives from
these groups to attend and participate in the discussion.
Typically, a case with an adverse event is presented in detail by
one of the members of the M&M team (see below) followed by
discussions led by faculty members and additional staff (nursing,
pharmacy, etc) involved in the case. The conference ends with a
sum-mary of the identified system errors as well as a plan for
future actions toward quality improvement.
Morbidity and Mortality Team and Case Identification
The M&M team changes annually and is comprised of 6 senior
pediatric residents, the 2 pediatric chief resi-dents, and 4
faculty advisors, including the associate residency program
director. This team is charged with the task of identifying cases
with adverse outcomes that have occurred at the Johns Hopkins
Childrens Center. The members of the M&M team are identified at
the beginning of the academic year and health care providers are
encouraged to share ideas for cases with any member of the team. In
addition, team members solicit potential cases from faculty in
high-acuity units such as the pediatric emergency department,
pediatric intensive care unit, oncology, and the neona-tal
intensive care unit. Each M&M team resident is given primary
responsibility for developing several case presentations during the
year. Preparation for the conference presentation includes review
of all perti-nent medical records, in-depth interviewing of the
staff members involved with the case, and inviting speakers from
the various disciplines to present and participate in the
discussion. The team member pri-marily responsible for the case
develops a slide pre-sentation on case details and other pertinent
issues. At the end of the case presentation, the primary team
member summarizes key points addressed during the conference. From
this, 1 to 3 action items are gener-ated, and individuals are
assigned to follow up on discussed changes. The chief residents are
responsible for obtaining updates regarding progress made on the
action plans and system changes. The Department of Pediatrics Chair
and the Governing Executive Committee are updated, and their
involvement is solicited for systems changes that involve
depart-ments other than pediatrics.
Case OverviewsBiannually, a conference is devoted to reviewing
all the cases presented in the previous 6 months. The cases are
summarized, and updates on the progress toward pro-posed system
changes are reported. In addition, a sum-mary table, consisting of
a brief case presentation, identified system errors, and updates on
changes initi-ated by the case are distributed via e-mail to the
Department of Pediatrics faculty and residents and members of other
disciplines who had attended the conference. The primary types of
errors identified by each case were grouped into categories by 2 of
the authors (KP and JRS). Any disagreements were settled by group
consensus.
-
Rabizadeh et al 1081
Evaluation Process
A survey was developed to evaluate the change in the MMC format.
The 17-question survey included demo-graphics, responses to the
proposed goals of the confer-ence, and qualitative comments that
addressed reasons why participants attended, whether participants
had implemented system changes in their practice, the value of the
twice yearly MMC summary, and suggestions for improvement of the
conference. The survey was distrib-uted via e-mail during June of
2006 and 2007, at the end of each respective academic year. Data
from 2 years of evaluations were included to determine
sustainability of changes. Survey questions that addressed the MMC
goals used a standard 1 to 5 Likert response scale with 1 =
strongly disagree and 5 = strongly agree. Space was provided for
additional free text commentary. The sur-vey was sent to all
Department of Pediatrics faculty and residents as well as nurses,
pharmacists, social workers, and other interested individuals who
had attended the MMC. Survey reminders were also sent a total of 3
times over a 6-week period. The surveys were returned to the Senior
Academic Program Coordinator in the Department of Pediatrics (KM).
Institutional review board approval was obtained, and participants
consented by agreeing to complete the survey. Any identifying
information was removed prior to data extraction. Qualitative
comments were reviewed by 2 of the authors (KM and JRS), and
representative examples were selected.
Statistical AnalysisData analysis was performed using the
Statistical Program for the Social Sciences, SPSS, version 10 (SPSS
Inc, Chicago, IL). Frequencies were calculated, and 2 analysis was
performed comparing the 2 aca-demic years.
ResultsDemographicsA total of 18 MMCs were held during the
academic year 2005-2006 and 14 during 2006-2007. An additional 2
conferences during each academic year were devoted to the biannual
reviews. There were 10 different categories of error types leading
to M&M identified from the cases during the 2 academic years
(Table 1). The majority were a result of communication problems and
issues relating to medications and allergies. In reviewing the
survey results, the majority of the respondents were physicians
(Table 2). Other disciplines were represented and included nurses,
pharmacists, social workers, and other interested individuals or
staff who did not more specifically identify themselves.
Demographic analysis revealed no significant differences between
the 2 aca-demic years; hence data were combined. Almost two-thirds
of survey responders attended more than 4 sessions during an
individual academic year. Individuals who did not attend regularly
cited scheduling conflicts as the primary reason for
nonattendance.
Multidisciplinary ApproachGiven the wide range of services
involved in the care of patients, one of the successes of this
conference was drawing individuals from a variety of services and
backgrounds. There was active participation and pre-sentations by
individuals from pediatric subspecialties (36), nursing (13),
pharmacy (5), surgical subspecialties (4), ophthalmology (3),
hospitalist service (3), anesthe-sia (3), infection control (3),
hospital safety (3), radiol-ogy (2), pathology (2),
obstetrics/gynecology (1), adult emergency medicine (1), nutrition
(1), Child Life (1), and legal services (1). Survey respondents
agreed that the discussions were held in a nonthreatening
manner
Table 1. Types of Primary Errors and Number Per Year Identified
in the Conferences
Type of Error 2005-2006 Academic Year 2006-2007 Academic
Year
Communication between providers 3 2Communication with family 2
0Equipment failure 1 0Failure/Delayed diagnosis 3 1Infection
control 2 1Medication/Allergy 3 2Patient transport 0 1Primary
prevention 3 1Resuscitation 1 3Transfer of care 0 3
-
1082 Clinical Pediatrics 51(11)
with productive identification of problems and/or errors leading
to M&M as well as suggestions for implement-ing change. In
fact, 95% of survey responders felt that the MMC created a forum
for different disciplines to address reasons for medical
errors.
Case Description and Implemented ChangesExamples of cases
discussed and the system changes that occurred as a result of the
MMC are presented (Table 3). During the 2005-2006 academic year,
one of the most notable system changes involved a new hospi-tal
policy wherein positive pregnancy test results (besides those
obtained on the obstetrics unit) were deemed critical action
values, requiring immediate notification to the patients caretakers
with acknowl-edgement and documentation of the notification. The
impetus for this system change was secondary to a MMC in which a
group to champion the change was identified. This group
successfully lobbied for the new policy through various hospital
improvement commit-tees. Although this error was identified during
the MMC of the Department of Pediatrics, the system change was seen
as beneficial for the entire hospital, and an institu-tional policy
was amended. Another example of the MMC leading to hospital policy
change occurred in the 2006-2007 academic year. An insulin drip was
mistak-enly run in place of the ordered nalaxone drip secondary
to physical similarities in the medication bottles. The
pediatrics MMC was the impetus for forming a multi-disciplinary
group, including physicians, nurses, and pharmacists, that
successfully advocated a change in hospital policy. As a result,
nalaxone drips are now administered in a 60-cc syringe (no longer
in a bottle) via a preprogrammed syringe pump, with the medica-tion
name scrolling across the pump screen. The third case example
illustrates the effect of the multidisci-plinary approach of the
conference in promoting change. A large number of peripheral
intravenous (IV) catheter infiltrates were noted in Childrens
Center patients via data from the patient safety tracking system,
an online tool for all hospital caretakers for reporting safety
issues or adverse events in the hospital. The multidisciplinary
participation and discussion at the pediatric MMC pro-vided the
momentum for Childrens Center policy changes directed at decreasing
the number of peripheral IV catheter infiltrates.
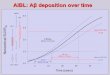
Survey ResultsAccording to the majority of individuals who
completed the annual surveys, the new MMC format achieved its goals
and objectives (Figure 1). A total of 98% of indi-viduals agreed or
strongly agreed that this conference allowed a practitioner to
modify behavior and judgments by learning from past adverse events,
whereas 95% felt that the conference was able to address
educational and systemic flaws that led to adverse outcomes.
Additionally, 80% agreed or strongly agreed that the discussions
were held in a nonthreatening manner, whereas 70% agreed or
strongly agreed that a group was identified to move for-ward with
needed changes and quality improvement. In all domains, the
positive responses were either sustained or improved during the
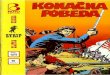
second year of study. Similar to the survey results, comments
showed appreciation and strong support for the new MMC format
(Figure 2). Respondents also expressed satisfaction with the
bian-nual summary. Suggestions for improvement centered on greater
participation of all disciplines, inclusion of nonmedical aspects
of the cases, and development of a systematic way to identify
cases.
DiscussionWe have successfully implemented a new system for the
Department of Pediatrics MMC and, in doing so, created a conference
focused on education and quality improvement. Our results indicate
that we had active participation from individuals with
multidisciplinary backgrounds engaged in nonthreatening discussions
about major patient-related M&M. Furthermore, system
Table 2. Demographics of Survey Participants
N Percentage
Attended 1 M&M conference
81/94 86%
Of those who attended 81 Discipline Physician 72 89% Faculty 23
32% Fellow 6 8% Resident 43 60% Other disciplinea 9 11%Male gender
25 31%Number of sessions
attended
1-3 29 36% 4-6 33 41% 7 19 23%Received biannual summary 59
73%
Abbreviation: M&M, morbidity and mortality.aIncludes
nursing, social work, pharmacist, bereavement coordinator, child
life worker.
-
Rabizadeh et al 1083
changes were proposed during the conference, and processes for
implementing those changes were initi-ated. The conference led to
hospital-wide system changes as exemplified by the new policy for
positive pregnancy test notification on nonobstetrics units and
change in the delivery apparatus of nalaxone drips to avoid
medication error. In addition, certain departmen-tal policies were
changed, such as appropriate use of peripheral IV access to reduce
catheter infiltrates. The annual survey demonstrated that
participants felt that the conference was effective in identifying
relevant system issues related to patient safety, fostering
dis-cussion of these issues and suggested changes, identi-fying
groups of individuals to address the potential changes, and
successfully implementing them. Scheduling conflicts, not a
perceived lack of value of the process, was the primary reason for
nonattendance, again supporting the overall satisfaction with the
new format of the conference.
The importance of didactic and case management conferences
cannot be overstated, but in changing the MMC, we were able to
transform an existing educa-tional vehicle in pediatrics that has
benefited not only the knowledge base of caretakers but also led to
system improvements translating to better and safer care. As
evident in the survey results, the nonthreatening,
multi-disciplinary approach to the MMC was a well-received adjunct
to more traditional resident education and CME.
Changing the culture of a conference such as the MMC is never a
static process and requires evolution with ongoing adaptation. One
of the most important aspects of the change in the MMC within our
depart-ment is the ability for future growth with ongoing
adjustments. To build on our success in terms of atten-dance,
multidisciplinary participation, problem identifi-cation, and
impetus for policy changes, the MMC will need to evolve based on
participant feedback. We seek to make this a dynamic process that
responds to the
Table 3. Examples of MMC Cases Extracted From the Yearly Summary
Table
Presenting Symptoms Issue Morbidity/Mortality System Changes
16-Year-old girl transferred in from outside hospital with
seizures, hypertension, and vision changes and presumed to have
venous sinus thrombosis
Pregnancy test obtained on admission not noted to be positive
for 5 hours, postresult availability. After noting result, patient
diagnosed with eclampsia and underwent emergent Cesarian
section
Delayed diagnosis of eclampsia because caretakers were unaware
of pregnancy test results
Newborn died in NICU secondary to respiratory failure
Patient fully recovered
Hospital-wide policy changed that positive pregnancy test
results (besides those obtained on obstetrics floor patients) made
critical action value requiring immediate notification to patients
caretakers
15-Year- old girl with history of lupus admitted with
pancreatitis and course complicated by significant pain and
hyperglycemia
Patient was treated with PCA and naloxone drip for her pain as
well as temporarily on an insulin drip, which was eventually
transitioned to SC regimen for hyperglycemia. During hospital
course, she developed hypoglycemia refractory to all interventions
(ie, stopping insulin). Required transfer to PICU
Though it had been discontinued, insulin was mistakenly hung
instead of naloxone, leading to the refractory hypoglycemia.
Insulin and naloxone drips were contained in identical bottles.
Furthermore, the bottle had correctly been labeled as insulin but
the IV tubing leading to the patient was marked as naloxone leading
to the medication error. The patient did well after the error was
discovered
Hospital-wide policy changed that naloxone would be administered
in a 60-cc syringe (no longer bottle) via a syringe pump that will
be programmed to have the medication name scroll across the pump
screen
A high number of peripheral IV catheter infiltrates were noted
after routine review of data in patient safety net (an online tool
for all hospital caretakers to report any safety issues or adverse
events)
In all, 36 IV infiltrate events were recorded, of which 24
caused significant morbidity and required additional treatment. The
majority of the 24 were receiving peripheral parenteral nutrition
via the infiltrating IV
High number of peripheral IV infiltrates, with two-thirds having
associated morbidity
Childrens Center policy changed that peripheral parenteral
nutrition will not be allowed unless approved by pediatric
gastroenterology, nutrition, and pharmacy after reviewing the need
and contents of the IV nutrition. Also the PICC line service will
get list of all admissions listed by diagnosis and touch base with
charge nurses on a daily basis, so as to be aware of patients who
may need longer-term IV access
Abbreviations: MMC, morbidity and mortality conference; NICU,
neonatal intensive care unit; PICU, pediatric ICU; OB, obstetrics;
PCA, patient-controlled anesthe-sia; SC, subcutaneous; IV,
intravenous; PICC, peripherally inserted central catheter.
-
1084 Clinical Pediatrics 51(11)
Figure 2. Representative comments made by conference
participants in the annual survey
Figure 1. Survey results
-
Rabizadeh et al 1085
changing conditions in both the patient care and medical
education environments. Our hope is that this will elicit a more
comprehensive cultural change in medical think-ing, especially in
pediatrics, where the most difficult casesthe ones in which harm
has occurred to the patientwill be discussed in a confidential,
nonthreat-ening manner with identification and initiation of
system-based changes that will make for safer patient care.
We recognize the limitations of evaluation using a postsurvey
study method. Our ability to quantify the impact of the change in
the conference format is limited because no baseline survey data
were collected prior to the implementation of this change.
Additionally, no objective data were collected to quantify whether
pro-posed changes led to increased patient safety or a decrease in
adverse events. Furthermore, the survey was susceptible to
responder bias.
Despite these limitations, survey results and com-ments suggest
that we have successfully reformatted the MMC in our pediatrics
department. The new conference format has promoted a nonthreatening
environment for multidisciplinary discussions of adverse events
and, most important, the nidus for promoting system changes that
can have significant effect across the entire medical center. This
is best exemplified by the following com-ment from an anonymous MMC
participant: A vast improvement over prior years during which [in
previous years] we would talk about cases in which the ball was
dropped, shake our heads forlornly and walk out of the room. Keep
up the good work! We hope to further improve the MMC and maintain
its new position as an important vehicle for identification of
errors, learning from errors, and promoting system changes.
Acknowledgments
We would like to acknowledge Dr George Dover and Dr Julia
McMillan for their support of the change in the MMC format and
their review of the manuscript. We would also like to acknowledge
Drs David Bundy, Elizabeth Hunt, Peter Rowe, and Allen Walker who
served as faculty advisors for the M&M team. In addition, we
would like to recognize the amaz-ing work of the residents on the
committee without whom these changes would not be possible: Drs
Naseem Amrasingham, Margaret Brewinski, Joshua Dishon, Doran Fink,
Raquel Hernandez, Michael Nemergut, and Patrick Wilson (2005-2006);
Drs Aaron Chambers, Joan Dunlop, Michelle Dunn, Rachel Johnson,
Michael McCrory, and David Shook (2006-2007).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with
respect to the research, authorship, and/or publication of this
article.
Funding
The authors received no financial support for the research,
authorship, and/or publication of this article.
References
1. Orlander JD, Barber TW, Fincke BG. The morbidity and
mortality conference: the delicate nature of learning from error.
Acad Med. 2002;77:1001-1006.
2. Accreditation Council of Graduate Medical Education Common
Program Requirements. http://www.acgme.org . Accessed August 11,
2009.
3. Orlander JD, Fincke BG. Morbidity and mortality confer-ence:
a survey of academic internal medicine departments. J Gen Intern
Med. 2003;18:656-658.
4. Friedman JN, Pinard MS, Laxer RM. The morbidity and mortality
conference in university-affiliated pediatric departments in
Canada. J Pediatr. 2005;146:1-2.
5. Aboumatar HJ, Blackledge CG, Jr, Dickson C, et al. A
descriptive study of morbidity and mortality conferences and their
conformity to medical incident analysis models: results of the
morbidity and mortality conference improve-ment study, phase 1. Am
J Med Qual. 2007;22:232-238.
6. Pierluissi E, Fischer MA, Campbell AR, Landefeld CS.
Discussion of medical errors in morbidity and mortality
conferences. JAMA. 2003;290:2838-2842.
7. Calabro JJ, Podrazik PM. Managed care morbidity and mortality
conference. Ann Emerg Med. 1995;26:531.
8. Hobgood CD, Ma OJ, Swart GL. Emergency medicine resident
errors: identification and educational utilization. Acad Emerg Med.
2000;7:1317-1320.
9. Vozenilek J, Wang E, Kharasch M, et al. Simulation-based
morbidity and mortality conference: new technologies augmenting
traditional case-based presentations. Acad Emerg Med.
2006;13:48-53.
10. Rosen P, Edlich RF, Rosen CL, Wolfe RE. Becom-ing a
specialist in emergency medicine. J Emerg Med. 2008;34:471-476.
11. Seigel TA, McGillicuddy DC, Barkin AZ, Rosen CL. Mor-bidity
and mortality conference in emergency medicine. J Emerg Med. In
press.
12. Rosenfeld JC. Using the morbidity and mortality confer-ence
to teach and assess the ACGME General Competen-cies. Curr Surg.
2005;62:664-669.
13. Hutter MM, Rowell KS, Devaney LA, et al. Identifica-tion of
surgical complications and deaths: an assessment of the traditional
surgical morbidity and mortality confer-ence compared with the
American College of Surgeons-National Surgical Quality Improvement
Program. J Am Coll Surg. 2006;203:618-624.
14. Miller DC, Filson CP, Wallner LP, et al. Comparing
per-formance of morbidity and mortality conference and National
Surgical Quality Improvement Program for
-
1086 Clinical Pediatrics 51(11)
detection of complications after urologic surgery. Urology.
2006;68:931-937.
15. Hurwitt ES, Schein CJ. Surgical mortality conference. Arch
Surg. 1965;91:1011-1013.
16. OConnell PR, Kirwan WO, Brady MP, ODonnell JA. Surgical
audit: the value of a morbidity and mortality con-ference. Ir J Med
Sci. 1988;157:100-103.
17. Thompson JS, Prior MA. Quality assurance and morbidity and
mortality conference. J Surg Res. 1992;52:97-100.
18. Harbison SP, Regehr G. Faculty and resident opinions
regarding the role of morbidity and mortality conference. Am J
Surg. 1999;177:136-139.
19. Seiler RW. Principles of the morbidity and mortality
con-ference. Acta Neurochir Suppl. 2001;78:125-126.
20. Veldenz HC, Dovgan PS, Schinco MS, Tepas JJ, III. Mor-bidity
and mortality conference: enhancing delivery of surgery residency
curricula. Curr Surg. 2001;58:580-582.
21. Risucci DA, Sullivan T, DiRusso S, Savino JA. Assessing
educational validity of the morbidity and mortality confer-ence: a
pilot study. Curr Surg. 2003;60:204-209.
22. Prince JM, Vallabhaneni R, Zenati MS, et al. Increased
interactive format for morbidity and mortality conference improves
educational value and enhances confidence. J Surg Educ.
2007;64:266-272.
23. Antonacci AC, Lam S, Lavarias V, et al. A morbidity and
mortality conference-based classification system for
adverse events: surgical outcome analysis: part I. J Surg Res.
2008;147:172-177.
24. Antonacci AC, Lam S, Lavarias V, et al. A report card
sys-tem using error profile analysis and concurrent morbidity and
mortality review: surgical outcome analysis, part II. J Surg Res.
2008;153:95-104.
25. Bender LC, Klingensmith ME, Freeman BD, et al. Anony-mous
group peer review in surgery morbidity and mortal-ity conference.
Am J Surg. 2009;198:270-276.
26. Esselman PC, Dillman-Long J. Morbidity and manage-ment
conference: an approach to quality improvement in brain injury
rehabilitation. J Head Trauma Rehabil. 2002;17:257-262.
27. Indresano AT. The morbidity and mortality conference: a case
assessment tool, quality control measure, and teach-ing method. J
Am Coll Dent. 2004;71:23-25.
28. Kravet SJ, Howell E, Wright SM. Morbidity and mortality
conference, grand rounds, and the ACGMEs core compe-tencies. J Gen
Intern Med. 2006;21:1192-1194.
29. Folcik MA, Kirton OC, Ivy ME. A two-tiered quality
management program: morbidity and mortality con-ference data
applied to resident education. Conn Med. 2007;71:471-478.
30. Carter BS, Guthrie SO. Utility of morbidity and mortality
conference in end-of-life education in the neonatal inten-sive care
unit. J Palliat Med. 2007;10:375-380.