Embed Size (px)
Citation preview

RESULTS: Data for the moderate exercise session are in the table, strat-ified by baseline physical activity level. Age-predicted THRs werehigher than individually prescribed THRs in all women. Exercisersachieved higher METs.CONCLUSION: Although exercise testing provides an accurate THR, itmay not be practical for prescribing moderate exercise. However, pro-viding a THR using readily available age-predicted ranges (eg, healthclub charts) may be inappropriate, as it might cause women to workharder than necessary. RPE was not accurate. When exercising in in-dividualized THRs, average MET level was in the moderate range forall women. Thus, the simple recommendation to perform activitiesrequiring 3-5.9 METs (readily available information) may be a prac-tical method of conveying ‘moderate’ exercise to pregnant women.
132 Post-natal catch-up growth aftersuspected IUGR at termLinda van Wyk1
1Leiden University Medical Centre, Obstetrics & Gynecology, Leiden,NetherlandsOBJECTIVE: To study neonatal growth patterns of children born aftersuspected intra-uterine growth restriction at term.STUDY DESIGN: We performed a long-term follow-up of the DIGI-TAT-RCT (n�650). This nationwide trial compared in women with apregnancy with suspected IUGR at term induction of labor (IoL) withexpectant management (EM). We collected growth data of these chil-dren until the age of 2 years using a postal enquiry. Standard deviationscores (SDS) for height and weight were calculated at different ages.Subsequently we assessed the effects of IoL compared with EM and theeffects of a birthweight below or above the 10th centile on catch-upgrowth. Target height SDS were calculated using the height of bothparents.RESULTS: We approached 582 of the 650 randomized patients, ofwhom 267 (46 %) responded. At birth the average SDS was �1.8 forheight and �2.0 for weight. At 2 years of age the SDS for height was�0.9 and �1.1 for weight, significantly lower than in a normal pop-ulation and significantly lower than expected based on the parents’target height SDS (�0.3). We found a significant increase in SDS inthe first 2 years of life, suggesting neonatal catch-up growth. Whencomparing IoL to a policy of EM we found that at birth, the weightSDS in the EM group was significantly lower (�2.1 vs �1.9,p�0.004), but children in the EM group showed significantly morecatch-up growth in the first month after birth and the SDS were com-parable thereafter. The increase in SDS for weight from birth till 2years was 1.3 for children �p10 and for children �p10 it was 0.6(p�0.045).CONCLUSION: Children born after IUGR at term show catch-up growthin the first 2 years after birth. After an expectant management, chil-dren show more catch-up growth during the first month. Childrenborn with a birthweight �p10 show significantly more catch-upgrowth in weight than children born with a birthweight �p10. Basedon the fact that these children have not yet reached their target heightSDS, we can conclude that catch-up growth is incomplete at two yearsof age.
133 Labor progression in elderly parturientsLiron Kogan1, Uri Dior1, Yossef Ezra1, Neta Eisenberg3, RonitCalderon-Margalit2
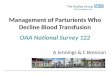
1Hebrew University, Department of Obstetrics and Gynecology, HadassahMedical Center, Jerusalem, Israel, 2Hebrew University, Epidemiology unit,School of Public Health, Jerusalem, Israel, 3Tel aviv university, The HelenSchneider Hospital for Women, Tel Aviv, IsraelOBJECTIVE: A major demographic trend of the last thirty years is in-creased mean age at first birth. Advanced maternal age has beenshown to be associated with obstetric complications. Yet, there is lim-ited data regarding labor progression of elderly parturients. Hence, weinvestigated the influence of maternal age on the labor curve.STUDY DESIGN: A retrospective cohort study of all singleton, term,cephalic, �1500 gram, spontaneous live vaginal deliveries between2003 and 2010 in a tertiary medical center. Detailed information wascollected on maternal demographics, cervical exams (enabling recon-struction of labor curves) and maternal and neonatal outcomes. Amixed models analysis of repeated measures were used to constructadjusted labor curves stratified by maternal age (�40, ��40 years)and parity (1, 2-5, �6). General linear models were used to comparedurations of the first and second stages of labor by maternal age, con-trolling for potential confounders (e.g. birthweight, oxytocin aug-mentation) and producing adjusted means.RESULTS: Of 44,121 births, maternal age was �40 years in 42,544, and��40 years in 1,577. Labor curves, stratified by age and parity, weresimilar (Figure). Duration of labor did not show a statistically signif-icant difference between the age groups. Mean durations from hospi-tal admissions to 10cm dilation for nulliparous parturients were 7.7and 7.5 hours for maternal age �40 and ��40 years, respectively(p�0.77); and for multiparous parturients, 4.5 and 4.7 hours for ma-ternal age �40 and ��40 years, respectively (p�0.27) [Table]. Meandurations of the second stage of labor for nulliparous parturients were81.9 and 94.2 minutes for maternal age �40 and ��40 years, respec-tively (P�0.08); and for multiparous parturients, 20.0 and 22.6 min-
Data from the moderate exercise session
Data are expressed as mean � standard deviation.* Age-predicted different from Individualized target heart rate (P � .05); † Non-exerciser different fromExerciser (P � .05.
SDS height and SDS weightfrom birth till 2 years of age
www.AJOG.org Clinical Obstetrics, Epidemiology, Fetus, Medical-Surgical Complications, Neonatology, Physiology/Endocrinology, Prematurity Poster Session I
Supplement to JANUARY 2013 American Journal of Obstetrics & Gynecology S69
utes for maternal age �40 and ��40 years of age, respectively(p�0.04).CONCLUSION: Progression of labor in the first and second stages is notsignificantly influenced by maternal age. This supports implementa-tion of similar clinical standards in the first and second stages of laborregardless of age.
134 WITHDRAWN
135 Is repeated shoulder dystocia a predictable event?M. Bas-Lando1, D. Goldberg1, V. Sery1, R. Farkash1,S. Grisaru-Granovsky1, A. Samueloff1
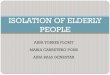
1Shaare Zedek Medical Center, Hadassah Hebrew University Hospital,Hebrew University Medical School, Deptartment of Obstetrics andGynecology, Jerusalem, IsraelOBJECTIVE: Shoulder dystocia (SD) is an event often followed by arecommendation for “preventive” CS in future births. We aimed toevaluate the risk factors for repeated SD and to set criteria for allowingsafe subsequent vaginal deliveries.STUDY DESIGN: Retrospective cohort review at a single center, between2005-2012, based on computerized database. All women with SD andsubsequent births were included. The primary event of SD was re-viewed for each case according to medical records and categorizedinto 2 groups: mild SD- less than a minute and no neonatal injury andsevere SD- more than a minute with neonatal injury. The subsequentvaginal deliveries were divided into 2 groups: Group A - repeat SD andGroup B- no recurrence. Group A & B were further compared fordemographic and risk factors (Table). Statistics: Descriptive,means�SDs , medians�IQR. Comparisons: chi-square, Fisher’s ex-act test, Mann-Whitney Test.RESULTS: Between 2005-2012 89,282 births were registered. SD wasrecorded for 235 women (0.26%) and 110 (46%) experienced deliv-eries following the event of SD: 84(76%) women were vaginal and 26(24%) were planned CS births. Ten (11.9%) women that delivered byvaginal route experienced repeat SD (Figure). Analysis showed thatthe main risk factors for repeated SD were macrosomia(p�0.02.OR�5 [1.3-19.3]), larger fetal weight at repeat birth(p�0.001), induction of labor (p�0.051) and longer interval betweenbirths (mean 5.1 �1.4 years vs 3.1�1.0 years, p�0.0001). However,all cases of repeated SD occurred in group of mild SD according to thefirst event description (0.068), 7 of them had mild SD and 3 severe SD.
CONCLUSION: The use of the classification of the SD severity is notpredictive of the risk for recurrent SD, thus even mild SD with noneonatal injury should be taken into account as a major risk factor forrecurrence in future vaginal birth, possibly with worse neonatal out-come. Furthermore, if vaginal birth is attempted, induction of laborshould be considered cautiously.
136 Duration of expulsive efforts and postpartumhemorrhage risk in nulliparous womenMarie-Danielle Dionne1, Catherine Deneux-Tharaux2, CorinneDupont3, Olga Basso1, René-Charles Rudigoz3, Marie-HélèneBouvier-Colle2, Camille Le Ray2
1McGill University, Obstetrics and Gynecology, Montréal, QC, Canada,2INSERM, u953, Paris, France, 3Réseau périnatal Aurore, Obstetrics andGynecology, Lyon, FranceOBJECTIVE: Several studies found an association between duration ofthe second stage of labor and postpartum hemorrhage (PPH). Most ofthese studies do not differentiate the passive and active (i.e. expulsiveefforts (EE)) phases of second stage. However, the intra uterine pres-sure is higher during the EE, thus the risk of PPH caused by atonymight be higher. Our study investigates the relationship between theduration of expulsive efforts (DEE) and risk of PPH.STUDY DESIGN: A case-control study was performed from the data ofPITHAGORE6 cluster randomized trial carried out in 106 Frenchmaternities (146 781 deliveries). All nulliparous women with a ce-phalic vaginal delivery were included. Exclusion criteria were: highrisk of PPH and contraindications to EE. Cases of PPH (n�3852) weredefined by a blood loss �500 ml and/or peripartum Hb decrease �2g/dl. Cases of severe PPH (n�1048) were defined by a peripartum Hbdecrease �4g/dl and/or the transfusion of �2 RBC units. The controlgroup (n�762) came from a representative sample of non-hemor-rhagic deliveries from the same population. The relationship betweenDEE and PPH was analyzed using multilevel logistic regression mod-els with adjustment on individual and organizational factors.
Duration of first stage of labor� stratified byage and parity groups�
�Admission to 10 cm; Adjusted for birthweight, oxytocin augmentation.
Poster Session I Clinical Obstetrics, Epidemiology, Fetus, Medical-Surgical Complications, Neonatology, Physiology/Endocrinology, Prematurity www.AJOG.org
S70 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2013