Embed Size (px)
Citation preview

Salvage Cryotherapy
Bernard Malavaud MD, PhD, FEBU Institut Universitaire du Cancer
Toulouse (France)
lowed for a better evaluation of the prostate, its surrounding struc-tures, and for better percutaneous placement of the catheters.44
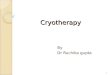
During this procedure performed under general anaesthesia, sixcathethers are inserted into the prostate and this allows a flow ofArgon and Helium gases (Fig. 2). These gases cool down the pros-tate to a temperature of minus 40 !C, and destroy cancerous cellsthroughout formation of ice balls. Salvage cryotherapy has a rolein the management of localized PC failure following RT, especiallyin older patients and those with some comorbidities.1,45,46 The 5-year biochemical DFS of salvage cryotherapy as reported in the lit-erature ranges between 23% and 58%44,50–54 (Table 2). Side effectsof salvage cryablation are more prevalent and serious comparedwith those noticed in case of primary intent.47 Indeed, prior studiesreported rates of 73% and 72% for urinary incontinence and erectiledysfunction, respectively, as well as more severe complicationsrequiring major operative interventions.48 Contemporary series re-ported lower urinary incontinence rates ranging between 4.3% and6.7%.44,49 The risk of complications seems to be higher in presenceof bulky disease or prior transurethral surgery.44 In order to de-crease the rates of morbidity, Eisenberg et al.46 proposed to reducethe prostate treated volume applying a partial salvage procedure.With improvements in technique, serious complications of salvagecryotherapy are less frequent but still occur, and salvage cryother-apy should be offered to patients presenting with organ confineddisease (excluding bulky disease) and low risk of complication(excluding prior transurethral surgery).
Radical brachytherapy
Salvage prostate brachytherapy may provide another attractiveoption for attaining disease control in patients with PC local failure.This procedure is performed under general or spinal anesthesia.Using a perineal template, radioactive seeds (low-dose rate brach-ytherapy) or catheters (high dose rate brachytherapy) are insertedinto the prostate. A transrectal ultrasound allows for visualization
of the prostate, the urethra and the surrounding tissue. It alsoguides catheter and needle insertion. Assessment and optimizationof dose distribution can be obtained intra-operatively using radio-active seeds (iodine-125 or palladium-103) (Fig. 3A) or postopera-tively, using CT planning, by dwell location and time variation ofthe high dose rate source (Fig. 3B and C). Dose distribution optimi-zation help to maximize radiation dose to the prostate while spar-ing the rest of organ at risk tissues. Multiple studies of salvagebrachytherapy have been reported in the post-PSA era, althoughthe published reports comprise fewer than 100 patients. Grado etal.55 presented the results of the largest clinical experience re-ported to date (49 patients) using radioactive seeds. With a medianfollow-up of 64 months, 3 and 5-year biochemical control rateswere 48% and 34%, respectively. Late complications included grosshematuria (4%), dysuria (6%) and rectal ulcers (4%). The rate ofhematochezia requiring surgical intervention was of 2% and therate of urinary incontinence requiring a prostate transurethralresection was of 6%. Lee et al.56 used a high dose rate salvagebrachytherapy procedure, delivering a total dose of 36 Gy in 6 frac-
Fig. 2. Prostate catheter placement guided by endorectal ultrasonography during the cryotherapy procedure.
Table 2Results of salvage cryosurgery for prostate cancer local recurrence after definitiveradiation therapy.
Authors aPatients Median FU(months)
Five year DFS(%)
Incontinence rate(%)
Izawa et al.50 131 57 23–57 72Chin et al.44 125 19 34 20Benoit et al.51 87 60 58 10.3Bahn et al.52 59 82 59b 4.3Donneelly
et al.5346 20 44c 6.5
Ghafar et al.54 38 21 74c 7.9
a Patients: number of patients; FU: follow-up; and DFS: disease-free survival.b Seven-year DFS.c Two-year DFS.
4 C. Boukaram, J.-M. Hannoun-Levi / Cancer Treatment Reviews xxx (2010) xxx–xxx
ARTICLE IN PRESS
Please cite this article in press as: Boukaram C, Hannoun-Levi J-M. Management of prostate cancer recurrence after definitive radiation therapy. CancerTreat Rev (2010), doi:10.1016/j.ctrv.2009.06.006
TRUS positioning & monitoring
Argon decompression -40°/-60°C
Urethra protection
Ice Ball
temperature monitoring of the
rectal wall
17G hollow needles

1.Mechanisms of action and limitations (geometry)
2.Adverse effects (historical series)
3.Guidelines on radiorecurrent PCa
4.Pre-operative management
5.Efficacy
6.Prognostic factors

Cryotherapy adresses cancer simultaneously at the cellular (membranes, organites) and the stromal support (microvasculature) levels
It then engages the cascade of apoptosis in injured but surviving cells
There is no known -possible- mechanisms of resistance to cryotherapy when the appropriate temperature was reached for a sufficient length of time.
©
2 0 0 5 B J U I N T E R N A T I O N A L | 9 5 , 11 8 7 – 11 9 1 | doi:10.1111/j.1464-410X.2005.05502.x
11 8 7
Blackwell Science, LtdOxford, UKBJUBJU International1464-410XBJU InternationalJune 2005959
Mini-rev Article
THE MOLECULAR BASIS OF CRYOSURGERYBAUST and GAGE
The molecular basis of cryosurgery
JOHN G. BAUST and ANDREW A. GAGE*
Institute of Biomedical Technology, State University of New York, Binghamton, and *School of Medicine and Biomedical Sciences, State University of New York at Buffalo, Buffalo, New York, NY, USA
Accepted for publication 21 February 2005
generally defined as arising from two major mechanisms. These are the direct injury to cells caused by ice crystal formation and the microcirculatory failure which occurs in the thawing period [2]. The relative importance of these two mechanisms has long been debated, but both are clearly major effects. Ice-crystal formation removes water from the biological system, which produces a host of deleterious effects. Intracellular ice is particularly lethal for cells. Cells closely packed in a tissue may sustain damage from ice crystals by purely mechanical means, as from the shearing forces of the crystals. The vascular effect, i.e. the microcirculatory failure that follows thawing, is evident in any experiments
in vivo
. The loss of blood supply deprives the cells of any chance of survival. The importance of this mechanism of injury, featuring vascular stasis in the thawed tissue, has long been stressed, including in recent investigations [3]. Nevertheless, from the molecular perspective, the most important advance in basic research related to cryosurgery is the recognition that apoptosis is a mechanism of cell death after cold injury [4].
CELL DEATH BY APOPTOSIS
Apoptosis is recognized as a mechanism of cell death which occurs in normal tissues. Apoptotic cells are characterized by nonrandom DNA cleavage, blebbing of membranes, phospholipid inversion in the membranes, and caspase activation [5]. This mode of cell death is seen also in diverse pathological conditions, including cancers, cytotoxic chemotherapy, heat injury, hormone ablation and irradiation. Apoptosis is seen also in freezing injury; apoptotic cells after freezing are found primarily in the peripheral zone of the cryogenic lesion, where the temperature was not sufficiently cold to kill all the cells. In the periphery, some cells would live and others would die. Some cells linger for days, then die, showing signs of apoptosis, as described by Hollister
et al.
[6] in experiments with prostate cancer cells. Apoptotic cells in human colon carcinoma
were identified by Hanai
et al.
[7] after exposure to modest freezing temperatures (
-
6 to
-
36
∞
C). Kinetic studies showed that the cells were susceptible to entering the apoptotic state up to 8 h after re-warming; similar findings were reported by Yang
et al.
[8]. The relatively recent discovery of apoptosis in cells adds a new dimension to potential therapy [9], as will be described later.
THE TISSUE RESPONSE TO FREEZING
The response to freezing injury varies from inflammatory to destructive, depending upon the severity of freezing. Minor freezing injury features only inflammatory responses, which have some therapeutic uses. Severe freezing injury destroys cells and tissues, which is the prime requirement for treating tumours, producing coagulation necrosis in the frozen tissue in the days after thawing. Some differences in the sensitivity of different types of cells exist, and these are the basis of selective cryotherapy, in which the therapeutic goal is to preserve some cells while destroying others [10]. However, cancer cells in most organs, such as the prostate gland, kidney and liver, require that techniques be used to ensure destruction.
THE CRYOGENIC LESION
This is characterized by a central uniform coagulation necrosis surrounded by a peripheral zone in which only partial cell death has occurred. This tissue change develops several days after freezing. Soon after thawing, the tissue appears congested and hypereamic, and becomes oedematous. The extent of necrosis becomes evident in about 2 days. In the central zone, near the cryoprobe/cryoneedle, cell death is uniform, but in the border zone at the periphery of the previously frozen tissue, where the tissue temperature was 0 to
-
20
∞
C, some cells survive, other cells are dead, and others are in the balance between life and death. Apoptotic cells are seen in this peripheral zone.
KEYWORDS
cryosurgery, apoptosis, prostate, kidney
INTRODUCTION
Recent molecular research has the potential to substantially broaden the efficacy of cryosurgery, especially in the treatment of tumours. The critical facet of this research is the recognition that apoptosis is a mechanism of cell death in cryogenic injury. This newly defined characteristic of freezing injury may provide an opportunity to manipulate the course of injury and repair so that it would be beneficial to therapy. This review explores the manner in which this goal may be achieved, defining the possible new directions that may be taken in the cryosurgical treatment of tumours, especially those of the prostate and kidney.
Freezing kills cells, a response that has long been evident in frostbite injury. In the last 50 years the therapeutic uses of freezing, whether for preserving or destroying cells and tissues, have increased interest in cold injury. In these years substantial progress has been made in preserving cells and tissues by freezing, but organ preservation by cryogenic techniques remains a challenge. This progress has been paralleled by the development of techniques for cell destruction, commonly termed cryosurgery or cryotherapy. Cryosurgical techniques have developed over the years as technological advances were made [1]. At the same time, the need for a better understanding of the mechanisms of injury and for better control of the therapeutic procedure became evident, and led to considerable research directed at these concerns. This article reviews the cryobiological basis of cryosurgery and defines the technical practices that should increase the efficacy of the freezing techniques.
THE MECHANISMS OF INJURY
The characteristics of tissue injury from freezing have been known for many years and
Baust & Gage, BJU Int 2005

Gage & Baust, Cryobiology
REVIEW
Mechanisms of Tissue Injury in Cryosurgery
Andrew A. Gage*,1 and John Baust†,2
*The Department of Surgery, State University of New York, Buffalo, New York 14214, U.S.A.; and †The Center forCryobiological Research, State University of New York, Binghamton, New York 13902, U.S.A.
As the modern era of cryosurgery began in the mid 1960s, the basic features of cryosurgical technique wereestablished as rapid freezing, slow thawing, and repetition of the freeze–thaw cycle. Since then, new applicationsof cryosurgery have caused numerous investigations on the mechanism of injury in cryosurgery with the intentto better define appropriate or optimal temperature–time dosimetry of the freeze–thaw cycles. A diversity ofopinion has become evident on some aspects of technique, but the basic tenets of cryosurgery remain unchanged.All the parts of the freeze–thaw cycle can cause tissue injury. The cooling rate should be as fast as possible, butit is not as critical as other factors. The coldest tissue temperature is the prime factor in cell death and this shouldbe 250°C in neoplastic tissue. The optimal duration of freezing is not known, but prolonged freezing increasestissue destruction. The thawing rate is a prime destructive factor and it should be as slow as possible. Repetitionof the freeze–thaw cycle is well known to be an important factor in effective therapy. A prime need incryosurgical research is related to the periphery of the cryosurgical lesion where some cells die and others live.Adjunctive therapy should influence the fate of cells in this region and increase the efficacy of cryosurgicaltechniques. © 1998 Academic PressKey Words: cryosurgery; mechanisms, tissue injury; cryogens.
As the modern era of cryosurgery began withthe development of automated cryosurgicalequipment in the 1960s, Cooper wrote that atissue temperature of220°C held for 1 min wassufficient to produce necrosis of tissue (13). Atthat time, a considerable body of information onthe effects of freezing tissue was available fromstudies in vitro directed at cryopreservation andfrom experimental and clinical work on frost-bite (49, 63, 69, 87, 107). Cooper’s statementwas based on this information and on his animalexperimentation. In cryosurgical literature dur-ing the next few years, it was commonly statedthat 220°C was lethal for cells and that thistemperature should be produced in the tissue toachieve a destructive effect (12, 34, 37, 40, 71,93, 110, 125). Nevertheless, at that time therewere no experiments in vivo that supported the
view that 220°C was an appropriate goal incryosurgical treatment.On the technical aspects of cryosurgery, a
measure of agreement was evident in the earlyreports. In the mid 1960s, the basic features ofcryosurgical technique, i.e., rapid freezing, slowthawing, and repetition of the freeze–thaw cy-cle, were established (11, 14, 27). Since then,the nature of the cryosurgical injury has beenthe subject of numerous investigations in aneffort to define the appropriate temperature–time dosimetry of the freeze–thaw cycles ofcryosurgery. A diversity of opinion has becomeevident. This review focuses on the nature oftissue injury under cryosurgical conditions andcomments on the relevance to clinical practice.Cryosurgery, whether experimental or thera-
peutic, requires that a volume of tissue be fro-zen, using appropriate techniques and instru-ments to control the freezing process. The rapidand intense freezing of tissue in situ, as done incryosurgical procedures, produces a localized,sharply demarcated wound. The nature of thetissue response varies with the intensity of the
Received March 16, 1998; accepted July 21, 1998.1 Consultant to Cryomedical Sciences, Inc.2 Vice President for Research and Development for Cryo-
medical Sciences, Inc., Rockville, MD.
CRYOBIOLOGY 37, 171–186 (1998)ARTICLE NO. CY982115
1710011-2240/98 $25.00Copyright © 1998 by Academic PressAll rights of reproduction in any form reserved.
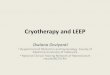
two cycles of -20°C for 10 minutes at the outer limit of the target, interspeded by passive thaw

Freezing point of a 0.9% w/v solution (saline solution) is -3.3°C- that is the temperature reached at the outer limit of the iceball -
1.2 mm 1.2 mm
-3°C
1.5 Cryoablation Needles 3
ENGL
ISH
1.4 Needle Performance - CryoablationIn vivo iceball dimensions and resulting ablation zone are determined by the
selected cryoablation needle, number of needles placed, tissue and tumor
characteristics, thermal heat sink from surrounding vasculature, and treatment
duration. Monitoring iceball formation provides direct control throughout the
procedure and is key to cryotherapy success.
NOTE: Using ultrasound or CT visualization, monitor iceball formation throughout
the cryotherapy procedure.
1.4.1 Laboratory TestingIceball shapes and dimensions are specific to the needle brand. The following
laboratory model of iceball dimensions is provided to assist users in selecting the
cryoablation needle(s) and needle placement to appropriately ablate the target
area. Typically, in vivo dimensions are smaller than the dimensions generated in
the laboratory.
Laboratory testing was performed in room temperature (21°C) gel; measurements
were made after two 10-minute Freeze cycles separated by a 5-minute passive
Thaw cycle. Accuracy is ±3 mm width, ±4 mm length.
Fig 3. 1.5 Cryoablation Needle Isotherm Data
ISOTHERMDATA
Hei
gh
t in
mill
imet
ers
0° C-20° C-40° C
20
10
0
10
20
30
40
50
IceSeed® 1.51.5 mm (17G)
33 mm x 38 mm20 mm x 27 mm11 mm x 20 mm
IceSphere® 1.51.5 mm (17G)
39 mm x 45 mm26 mm x 32 mm16 mm x 24 mm
IceRod® 1.5 PLUS1.5 mm (17G)
43 mm x 60 mm30 mm x 48 mm18 mm x 42 mm
PLUSIceRod® 1.51.5 mm (17G)
41 mm x 60 mm27 mm x 50 mm16 mm x 41 mm
Galil 2018 Manual
-8°C
Ice Sphere: 11mL/-20°C Ice Rod: 19 mL/-20°C

Limitations therefore pertain to our ability to extend the ice ball beyond the tumor margins
Porcine Kidney, 1 week after CA

literature, a wide variation of papers describes treatment
outcome and toxicity after different salvage modalities,preceded by different primary therapies. To our knowl-
edge, there are few reports on salvage outcome from large
populations, and no previous article has presented outcomeof three different treatment groups from one population. A
comparison from the literature is summarized in Table 3
(FFF) and Table 4 (toxicity). Comparison, however, ishampered by the small and divergent study populations and
the different definitions for BF.Although this study population is not comparable
regarding patient and tumor characteristics and follow-up,
a comparison could be made regarding toxicity. Grade 3GU and GI toxicity occurred in 32 % of SRP patients,
29 % of SBT patients and 30 % of SCS patients. Further-
more, toxicity rates in this study are equivalent to the datapresented in the literature.
The 5-year FFF was 27 % following SRP and 15 %
following SBT (Phoenix definition). After 36 months, theFFF following cryosurgery was 19 %. These figures are
lower compared to those found in the literature (Table 3,
4). This could be due to incomplete salvage procedures,but dissemination before salvage is more probable.
Patients with high PSA levels and a short PSADT prior to
salvage have a high risk of dissemination at the time of
salvage. Especially, the cryosurgery group contained high-risk cases like cT3 and Gleason 8–10 tumors. The litera-
ture shows that the pre-salvage PSA concentration,
PSADT after primary radiation treatment and the primarytumor stage are important in the prediction of a bio-
chemical recurrence. In one SRP study, patients with a
pre-salvage PSA \2 ng/ml and PSADT [12 monthsshowed better biochemical survival rates than patient with
PSA [2 ng/ml and PSADT \12 months ([80 % bDFSafter 80 months in the most favorable risk group com-
pared with 0 % bDFS after 20 months in the group with
the highest risk factors) [11]. Other data indicate morefavorable results for primary T1 and T2 tumors in com-
parison with T3 and T4 tumors (100 % bDFS after 5 years
in T2 tumors compared with 35 % in T3 and 0 % inN ? tumors) (9,22). In the brachytherapy group, pre-sal-
vage PSA [10 ng/ml, pre-salvage Gleason scores C7 and
PSADT \10 months show poorer biochemical controlrates [9, 12]. For the SCS group, these risk factors for
salvage treatment failure have also been recognized.
Patients with a pre-salvage PSA [10 ng/ml, Gleasonscores C8 before primary treatment, clinical T3/T4 tumors
and poor response to hormonal treatment show decreased
Table 3 Comparison with results from literature–freedom from biochemical failure
Salvage procedure No. studies [references] N Follow-up FFF (%) Follow-up present study FFF present study (%)
Radical prostatectomy 5 [9, 11, 20–22] 377 5 years 31–71 5 years 27
125-I implantation 3 [9, 23, 24] 66 5 years 34–53 5 years 15
Cryosurgery 3 [9, 25, 26] 467 5 years 44–55 3 years 19
FFF freedom from biochemical failure
Table 4 Comparison withresults from previous literature–toxicity
GU genitourinary; GIgastrointestinal; NA notavailablea 44 % of patients had pre-existent erectile dysfunction
Salvage procedure Radical prostatectomy 125-Iimplantation
Cryosurgery
Literature
No. studies[references]
5 [9, 11, 20, 22, 27] 3 [9, 23, 24] 6 [9, 25, 28–31]
N 308 66 707
% GU toxicity 20–68 % incontinence 12 % grade 1–2 4–83 % incontinence
22–41 % bladder neckstricture
38 % grade 3–4 7–55 % bladder neck stricture/retention
% GI toxicity 2–7 % rectal injury 0–12 % grade1–2
6–37 % perineal pain
0–2 % grade3–4
1–11 % fistula
Erectile dysfunction 72 %—Nearly uniform NA 72–86 %
Present study
% GU toxicity 23 % grade 3 23 % grade 3 22 % grade 3
% GI toxicity 9 % grade 3 6 % grade 3 7 % grade 3
Erectile dysfunction 86 % 45 % 93 %a
World J Urol (2013) 31:403–409 407
123
ORIGINAL ARTICLE
Patterns of outcome and toxicity after salvage prostatectomy,salvage cryosurgery and salvage brachytherapy for prostatecancer recurrences after radiation therapy: a multi-centerexperience and literature review
Max Peters • Maaike R. Moman • Henk G. van der Poel •
Henk Vergunst • Igle Jan de Jong • Peter L. M. Vijverberg •
Jan J. Battermann • Simon Horenblas • Marco van Vulpen
Received: 23 April 2012 / Accepted: 27 July 2012 / Published online: 18 August 2012! Springer-Verlag 2012
AbstractPurpose Current salvage treatments for recurrent prostate
cancer after primary radiation therapy include radical
prostatectomy, cryosurgery and brachytherapy. Becausetoxicity and failure rates are considerable, salvage treat-
ments are not commonly performed. As most centers per-
form only one preferred salvage technique, the literatureonly describes single-center outcomes from a single sal-
vage technique with a limited number of patients. In this
overview, five high-volume Dutch centers describe theirtoxicity and outcome data using different salvage tech-
niques. This provides a view on how salvage is performed
in clinical practice in the Netherlands.
Methods A total of 129 patients from five different cen-ters in the Netherlands were retrospectively analyzed.
Biochemical failure (BF) was defined as PSA [0.1 ng/ml
for the salvage prostatectomy group (n = 44) and PSAnadir ? 2.0 ng/ml (Phoenix definition) for the salvage
cryosurgery (n = 54) and salvage brachytherapy group
(n = 31). Toxicity was scored according to the CommonToxicity Criteria for Adverse events (CTCAE v3.0).
Results BF occurred in 25 (81 %) patients in the brach-
ytherapy group (mean follow-up 29 ± 24 months), 29(66 %) patients in the prostatectomy group (mean follow-
up 22 ± 25 months) and 33 (61 %) patients in the cryo-
surgery group (mean follow-up 14 ± 11 months). Severe(grade [3) genitourinary and gastrointestinal toxicity was
observed in up to 30 % of patients in all three groups.
Conclusion This overview shows clinical practice ofprostate cancer salvage. Significant failure and toxicity
rates are observed, regardless of salvage technique.
Patients should be selected with great care before offeringthese salvage treatment strategies.
Keywords Salvage ! Prostatectomy ! Cryosurgery !Brachytherapy ! Toxicity ! Outcome ! Prostate cancer
Introduction
A significant proportion of prostate cancer patients treated
with primary radiotherapy develop a recurrence. Estima-tions of risks exceeding 60 % have been presented for the
highest risk groups [1–4]. The recurrence risk is dependent
on various risk factors such as initial PSA level (iPSA),PSA doubling time (PSADT), Gleason score and PSA nadir
after initial treatment.
M. Peters (&) ! M. R. Moman ! J. J. Battermann !M. van Vulpen (&)Department of Radiation Oncology,University Medical Center Utrecht,Heidelberglaan 100, 3584 CX Utrecht, The Netherlandse-mail: [email protected]
M. van Vulpene-mail: [email protected]
H. G. van der Poel ! S. HorenblasDepartment of Urology, Netherlands Cancer Institute,Amsterdam, The Netherlands
H. VergunstDepartment of Urology, Canisius-Wilhelmina Hospital,Nijmegen, The Netherlands
I. J. de JongDepartment of Urology, University Medical Center Groningen,Groningen, The Netherlands
P. L. M. VijverbergDepartment of Urology, St. Antonius Hospital,Nieuwegein, The Netherlands
123
World J Urol (2013) 31:403–409
DOI 10.1007/s00345-012-0928-8
Peters, World J Urol 213
The Dutch experience (4 centers) and review of the literature
A reputation of a somewhat morbid procedure driven by historical series

Review – Prostate Cancer
Salvage Cryoablation for Locally Recurrent Prostate CancerFollowing Primary Radiotherapy
Vladimir Mouraviev a,*, Philippe E. Spiess b, J. Stephen Jones c
a Division of Urology, Department of Surgery, Medical College of Cincinnati, Cincinnati, OH, USA; b Department of Genitourinary Oncology, Moffitt Cancer
Center, Tampa, FL, USA; c Cleveland Clinic Department of Regional Urology, Glickman Urological and Kidney Institute, Cleveland Clinic Lerner College of
Medicine at Case Western Reserve University, Cleveland, OH, USA
E U R O P E A N U R O L O G Y 6 1 ( 2 0 1 2 ) 1 2 0 4 – 1 2 1 1
avai lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted February 29, 2012Published online ahead ofprint on March 8, 2012
Keywords:Radiorecurrent prostate cancerFocal salvage treatmentSalvage whole-glandcryoablation
Abstract
Context: The purpose of this paper is to review current salvage cryoablation (SCA)outcomes in patients with locally recurrent prostate cancer (PCa) following primaryradiation therapy.Objective: The objectives of this review are (1) to analyze the eligibility criteria forcareful patient selection for these salvage modalities and (2) to evaluate the oncologicresults and reported complication rates for these respective modalities.Evidence acquisition: A Medline/PubMed literature search was performed of peer-reviewed scientific articles published from 1991 to 2012 regarding salvage therapyfor radiorecurrent PCa. The following search terms and various permutations were used:radiorecurrent prostate cancer, local salvage treatment, salvage radical prostatectomy,salvage cryoablation, salvage brachytherapy, and salvage high-intensity focused ultrasound.Only articles written in English were included.Evidence synthesis: SCA is a feasible and efficacious treatment modality, especiallyusing third-generation technology, whereby the biochemical disease-free survival isestimated to be between 50% and 70% at 5-yr follow-up in properly selected patients.Severe complications such as rectourethral fistulas are significantly less common overthe last decade than was reported in the past. Because there are no prospective,randomized studies and the definitions of PSA failure vary among many studies,comparisons between these different salvage modalities are limited in terms of cancer-specific outcomes. Nevertheless, in recent years, tertiary care referral centers forprostate cryotherapy have reported their treatment outcomes using rigorous treat-ment end points and morbidity grading systems, dramatically improving the quality ofreported clinical data. Consequently, favorable predictors of treatment outcomes havebeen identified.Conclusions: The inability to effectively salvage patients with locally recurrent PCafollowing radiation therapy has in large part resulted from the lack of sufficientlysensitive and specific diagnostic tools to detect local recurrences at an early, potentiallycurable stage. Consequently, a more stringent definition of biochemical failure, im-proved imaging techniques, and accurate PCa mapping imaging technology is greatlyneeded within our diagnostic armamentarium. Additional research and randomizedclinical trials are required to determine which salvage modality is superior in terms ofoncologic efficacy and reduced morbidity.# 2012 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. 231 Albert Sabin Way, ML 0589, Cincinnati, OH 45267, USA.Tel. +1 513 558 0983; Fax: +1 513 558 3575.E-mail address: [email protected] (V. Mouraviev).
0302-2838/$ – see back matter # 2012 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2012.02.051
positive cores to prostate volume were significant prognosticfactors of favorable biochemical outcomes [54].
Ng et al. [31] reported the pattern of local recurrenceafter SCA in 122 patients. At a mean follow-up of 56 mo, 23%of patients were diagnosed with locally recurrent PCa basedon the presence of positive post-treatment prostate biopsy.Interestingly, most recurrences were located in the apex(51.5%), in the base (21.2%), and in the SVs (18.2%). Theauthors postulated that it was truly the location of lessaggressive freezing (ie, cryoablation) used in close proximi-ty to vital structures such external sphincter and rectumthat was predictive of treatment failure. The presence ofcancer at the base of the prostate was a significantprognostic factor ( p = 0.014) of SCA success, probably dueto more extensive disease among patients with SVinvolvement.
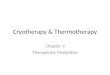
Reiterating the concept of incomplete ablation of radio-recurrent PCa, Huang et al. demonstrated the distribution oftumor lesions on whole-mount sections at final pathologyassessment after salvage RP for failed primary RT [55]. Theauthors found periurethral tumors in 67% cases, with 7%located in direct contact with the urethra (Fig. 2). In anadditional 17.4%, tumors were revealed within 2 mm of theurethra. This is the exact area where cryosurgeons attemptto protect the urethral wall from deep freezing (and henceavoid sloughing) using the urethral warmer with 43 8Cirrigation throughout the procedure. Extracapsular exten-sion was noted in 43% of cases and SV involvement in 28%.Lastly, the apex contained cancer foci in 93% of cases. Thesedata may initially appear worrisome regarding the ability toachieve a complete ablation of tumor with SCA, but thebDFS rate of SCA is significantly more encouraging.Nevertheless, one of the possible directions for increasingthe ‘‘killing effect’’ (ie, efficacy of the freezing) is the localuse of cryosensitizers (eg, peritumoral injection of vitaminD3 before cryoablation) that significantly enhance the
tissue destruction in vitro and in vivo with more softfreezing while preserving vital surrounding structures [56].
3.6. Complications of salvage cryoablation
Unfortunately, there is still negative sentiment amongmany urologic oncologists that SCA causes serious sideeffects such as post-treatment urinary incontinence, rectalfistula formation, and impotence in most cases. Thisperception largely results from the early results ofrudimentary first- and second-generation cryotherapydevices from which a substantial proportion of patientsexperienced voiding and bowel difficulties, perineal pain,and urethral sloughing. In one early study, the incontinencerate following SCA was reportedly as high as 73% [45].
[(Fig._1)TD$FIG]
Fig. 1 – Pretreatment nomogram to predict biochemical failure after salvage cryoablation (adopted from Spiess et al. [39]).PSA = prostate-specific antigen.
[(Fig._2)TD$FIG]
Urethra
< 2 mm
2 – 5 mm
5 – 10 mm
> 10 mm
No. of Specimens (%)
3 (6.5%)
8 (17.4%)
20 (43.5%)
14 (30.4%)
1 (2.2%)
Fig. 2 – Minimal distance from radiorecurrent cancer and urethra inmillimeters (adopted from Huang et al. [55]).
E U R O P E A N U R O L O G Y 6 1 ( 2 0 1 2 ) 1 2 0 4 – 1 2 1 11208
Mouraviev, Eur Urol 2012
Urethral warmer is instrumental in reducing the risks of fistula but may promote
recurrence in the close vicinity of the urethra

Guidelines
EAU Guidelines on Prostate Cancer. Part II: Treatment ofAdvanced, Relapsing, and Castration-Resistant Prostate Cancer
Axel Heidenreich a,*,y, Patrick J. Bastian b, Joaquim Bellmunt c, Michel Bolla d, Steven Joniau e,Theodor van der Kwast f, Malcolm Mason g, Vsevolod Matveev h, Thomas Wiegel i,Filiberto Zattoni j, Nicolas Mottet k,z
a Department of Urology, RWTH University, Aachen, Germany; b Department of Urology, Klinikum Golzheim, Dusseldorf, Germany; c Department of Medical
Oncology, University Hospital Del Mar, Barcelona, Spain; d Department of Radiation Therapy, CHU Grenoble, Grenoble, France; e Department of Urology,
University Hospital, Leuven, Belgium; f Department of Pathology, Erasmus Medical Center, Rotterdam, The Netherlands; g Department of Oncology and
Palliative Medicine, Velindre Hospital, Cardiff, UK; h Department of Urology, Russian Academy of Medical Science, Cancer Research Center, Moscow, Russia;i Department of Radiation Oncology, University Hospital, Ulm, Germany; j Department of Urology, Santa Maria Della Misericordia Hospital, Udine, Italy;k Department of Urology, University Hospital St Etienne, France
E U R O P E A N U R O L O G Y 6 5 ( 2 0 1 4 ) 4 6 7 – 4 7 9
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted November 1, 2013Published online ahead ofprint on November 12, 2013
Keywords:Prostate cancerEAU guidelinesReviewFollow-upSalvage radiation therapySalvage radical prostatectomyAndrogen deprivationChemotherapyEnzalutamideAbirateroneDocetaxelZoledronic acidDenosumab
Abstract
Objective: To present a summary of the 2013 version of the European Association ofUrology (EAU) guidelines on the treatment of advanced, relapsing, and castration-resistant prostate cancer (CRPC).Evidence acquisition: The working panel performed a literature review of the new data(2011–2013). The guidelines were updated, and levels of evidence and/or grades ofrecommendation were added to the text based on a systematic review of the literaturethat included a search of online databases and bibliographic reviews.Evidence synthesis: Luteinising hormone-releasing hormone (LHRH) agonists are thestandard of care in metastatic prostate cancer (PCa). LHRH antagonists decrease testos-terone without any testosterone surge, and they may be associated with an oncologicbenefit compared with LHRH analogues. Complete androgen blockade has a smallsurvival benefit of about 5%. Intermittent androgen deprivation results in noninferioroncologic efficacy when compared with continuous androgen-deprivation therapy(ADT) in well-selected populations. In locally advanced and metastatic PCa, earlyADT does not result in a significant survival advantage when compared with delayedADT. Relapse after local therapy is defined by prostate-specific antigen (PSA) values>0.2 ng/ml following radical prostatectomy (RP) and>2 ng/ml above the nadir and afterradiation therapy (RT). Therapy for PSA relapse after RP includes salvage RT (SRT) at PSAlevels <0.5 ng/ml and SRP or cryosurgical ablation of the prostate in radiation failures.Endorectal magnetic resonance imaging and 11C-choline positron emission tomogra-phy/computed tomography (PET/CT) are of limited importance if the PSA is <1.0 ng/ml;bone scans and CT can be omitted unless PSA is >20 ng/ml. Follow-up after ADT shouldinclude analysis of PSA and testosterone levels, and screening for cardiovascular diseaseand metabolic syndrome. Treatment of CRPC includes sipuleucel-T, abiraterone acetateplus prednisone (AA/P), or chemotherapy with docetaxel at 75 mg/m2 every 3 wk.Cabazitaxel, AA/P, enzalutamide, and radium-223 are available for second-line treat-ment of CRPC following docetaxel. Zoledronic acid and denosumab can be used in menwith CRPC and osseous metastases to prevent skeletal-related complications.
* Corresponding author. Tel. +49 241 808 9374; Fax: +49 241 808 2441.E-mail address: [email protected] (A. Heidenreich).y Chair of the EAU Prostate Cancer Guidelines Group, 2008 to March 2013.z Chair of the EAU Prostate Cancer Guidelines Group since March 2013.
0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.eururo.2013.11.002
Heidenreich, Eur Urol 2014
3. Diagnosis and treatment of relapse after curativetherapies
3.1. Definition of recurrence
Following RP, a confirmed PSA value >0.2 ng/ml (ie, twoconsecutive increases) represents recurrent cancer [36].Following RT, a PSA value of 2 ng/ml above the nadir after RTrepresents recurrent cancer (Phoenix classification [37]).
Local failure following RP might be predicted with an80% probability by a PSA increase >3 yr after RP, a PSADT >11 mo, a Gleason score <7, and stage !pT3a pN0, pTxR1. Systemic failure following RP might be predicted with>80% accuracy by a PSA increase <1 yr after RP, a PSA DT of4–6 mo, a Gleason score of 8–10, and stage pT3b, pTxpN1. Ina cohort of 148 men with rising PSA and a PSA DT <12 mofollowing local treatment, the PFS was associated withGleason grade ( p = 0.006), PSA at time of treatment( p < 0.001), and PSA DT ( p < 0.001) [38]. The median PFSwas 19 mo, with a 3- and 5-yr metastasis PFS of 32% and16%, respectively.
Prostatic biopsy after RT is necessary only if localprocedures such as SRP are indicated in an individualpatient. Treatment can then be guided by the presumed siteof failure, the patient’s general condition, and personalpreferences (Table 3; sect. 3.2).
Imaging studies such as bone scintigraphy or computedtomography (CT) to determine the site of recurrence are ofno additional diagnostic value with a positive finding in<5% unless the PSA serum levels are >20 ng/ml or the PSAvelocity is >2 ng/ml per year [39,40]. Endorectal coilimaging might represent a useful technique to detect localrecurrences after RP if PSA serum levels exceed 2 ng/ml [41].Similar data were achieved in a cohort of 64 patients withPSA progression following external-beam radiation therapy(EBRT) [42]. The diagnostic accuracy to detect locallyrecurrent PCa was highest at a PSA level >2 ng/ml butonly for 18F-choline PET/CT.
Positron emission tomography (PET) has been usedsuccessfully in many human cancers for early identificationof local, locoregional, or systemic recurrences. In PCa, thereare few, even if promising, published data on the clinical
efficacy of PET in detecting local recurrences after RP,especially when an increased PSA value >1.0 ng/ml isdetected [42,43]. As reported by Giovacchini et al. [44] in2012, the accuracy of PET correlates with PSA values, PSADT, and other pathologic features. A PSA DT <3 mo cancertainly be regarded as a strong predictor of PET positivityas does a PSA serum level >1.5 ng/ml. In addition, imagingstudies such as 11C-choline PET/CT should only beperformed if therapeutic consequences such as salvagelymphadenectomy, SRP, or salvage RT to lymph nodes arebeing considered as a therapeutic option.
3.2. Management of prostate-specific antigen relapse following
radical prostatectomy
There have been many studies on the use of RT for PSA-onlyrecurrence following RP. As confirmed by various studies,the preradiation PSA level is critically important for optimaltreatment results. Stephenson et al. [45] identified asignificant relationship between PSA serum concentrationat the time of RT and therapeutic outcome. The 6-yr BCR-FSwas 48% in men with PSA <0.5 ng/ml, whereas it was only40%, 28%, and 18% in men with PSA levels of 0.51–1 ng/ml,1.01–1.5 ng/ml, and >1.5 ng/ml, respectively.
In a subanalysis of the SWOG 8974 trial, Swanson et al.[46] showed that men in all categories of post-RP PSA level(<0.2, 0.2–1.0, >1.0 ng/ml) showed an improvement withSRT in metastasis-free survival. However, the therapeuticbenefit was most evident in the presence of minimal PSAserum levels. Even in men with PSA DT!6 mo, SRT has beenreported to improve PCa-specific survival if it is givenwithin 2 yr following a rise in the PSA level [47].
Currently, local recurrences after RP are best treated bySRT with 64–66 Gy at a PSA serum level !0.5 ng/ml.Siegmann et al. tried to define ‘‘what is the best time totreat’’ in 301 patients with biochemical recurrences after RPby evaluating the biochemical response to SRT and with amedian follow-up of 30 mo [48]. In the multivariate logisticregression analysis evaluating factors influencing anundetectable PSA following SRT, only the pre-SRT PSA level(odds ratio [OR]: 2.62; p = 0.001) and infiltration of theseminal vesicles (OR: 2.53; p = 0.02) were found to be
Table 3 – Guidelines on treatment options for prostate-specific antigen relapse following local treatment
Recommendations GR
" Local recurrences are best treated by salvage RT with 64–66 Gy at a PSA serum level !0.5 ng/ml. B
" Expectant management is an option for patients with presumed local recurrence who are too unfit or unwilling to undergo RT. B
" PSA recurrence indicative of systemic relapse is best treated by early ADT, resulting in decreased frequency of clinical metastases if poor prognostic
risk factors such as PSA DT <12 mo or Gleason score 8–10 are present.
B
" Luteinising hormone-releasing hormone analogues/antagonists/orchiectomy or bicalutamide 150 mg/d when hormonal therapy is indicated. A
Local recurrences can be treated with salvage RP in carefully selected patients, who presumably have organ-confined disease, that is, PSA <10 ng/mL,
PSA DT >12 mo, low-dose brachytherapy, biopsy Gleason score <7.
B
Cryosurgical ablation of the prostate and interstitial brachytherapy are alternative procedures in patients not suitable for surgery. B
HIFU may be an alternative option. However, patients must be informed about the experimental nature of this treatment modality due to the short
follow-up periods reported.
B
In patients with presumed systemic relapse, ADT may be offered. C
ADT = androgen deprivation therapy; GR = grade of recommendation; HIFU = high-intensity focused ultrasound; PSA DT = prostate-specific antigen doubling
time; RP = radical prostatectomy; RT = radiation therapy.
E U R O P E A N U R O L O G Y 6 5 ( 2 0 1 4 ) 4 6 7 – 4 7 9472
PRad: PSA <10, PSAdT>12M, GS<7 and
LDR brachytherapy failure
Salvage cryotherapy when not suitable for surgery
experimental nature of salvage HIFU

1990- 2000: PSA recurrence in one patient out of three (Phoenix definition)
10% of good pronostic patients,
up to 60% in the poor prognostic group
Better results (DFSR) since IMRT and adjuvant ADT
Grossfeld CAPSURE J.Urol 2002, Bolla Lancet 2002, Jones, Eur Urol 2011
Platinum Priority – EditorialReferring to the article published on pp. 405–410 of this issue
Radiorecurrent Prostate Cancer: An Emerging and LargelyMismanaged Epidemic
J. Stephen Jones *
Cleveland Clinic Lerner College of Medicine at Case Western Reserve University, Department of Regional Urology, Glickman Urological and Kidney Institute,
9500 Euclid, Desk A100, Cleveland, OH 44120, USA
Radiation as primary treatment for organ-confined prostatecancer (PCa) is widely and increasingly utilized throughoutmuch of the world via both external-beam radiation therapy(EBRT) and brachytherapy. Tremendous variations in itsutilization exist both within and across countries and arelargely unsupported by data to explain such discrepancies.
Controversy remains regarding the efficacy of radiationtherapy (RT) for PCa, especially considering that at least 25%of patients will have a positive biopsy following therapy.Nevertheless, local failure as defined by a postradiationbiopsy showing histologic evidence of persistent cancercorrelates with disease-free survival and metastasis, so thetemptation to ignore biopsy findings in otherwise healthypatients appears to be imprudent [1]. Unfortunately, up toone-third of radiation patients will receive secondarytreatment for cancer recurrence, indicating that long-termefficacy for RT is far from assured [2]. Compared to radicalprostatectomy, RT is associated with a more than two-foldlikelihood of cancer-specific mortality in the nonrandom-ized but well-controlled Cancer of the Prostate StrategicUrologic Research Endeavor (CaPSURE) data [3].
Despite this, the lower immediate morbidity of RTcompared to prostatectomy, combined with physician andpatient choice, led approximately one-fourth of patients toundergo either EBRT or brachytherapy in that representa-tive American registry. One-fourth of the 217 730 new casesof PCa in the United States predicted by the AmericanCancer Society in 2010 [4] would translate into 54 433American patients radiated (with EBRT, brachytherapy, ortheir combination) annually. Furthermore, a conservativecalculation of a 25% failure rate means that there are at least13 608 new radiorecurrent PCa patients in the United Statesannually and many times that throughout the world. In
other words, radiorecurrent PCa is the fourth most commongenitourinary malignancy in men, following primary PCa,bladder cancer, and kidney cancer.
Radiorecurrent PCa represents an emerging epidemic inmany developed countries. Nevertheless, the phenomenonremains largely ignored by the urologic community,probably because most patients remain under the care ofradiation oncologists who may not be keen to emphasize itsprevalence or who may not be aware of available curativeoptions such as salvage cryoablation, prostatectomy, orhigh-intensity focused ultrasound (HIFU). Its existence isoften veiled by antiandrogen therapy, which suppressesprostate-specific antigen (PSA) levels but has absolutely nochance of cure. Disturbingly, >90% of patients undergoingsecondary therapy following radiation are treated withandrogen deprivation therapy (ADT) in the CaPSUREpopulation, despite a total lack of evidence for efficacyfor ADT in this setting as well as the growing understandingof its own morbidity and the complete inability of androgendeprivation to cure patients who often have local recur-rences that are amenable to curative local therapy.
A report in this issue of European Urology from Williamsand colleagues from Canada adds to a growing body ofevidence supporting the use of cryoablation for patients withlocalized disease following RT [5]. Furthermore, their workhelps identify which patients are unlikely likely to benefit,and this information can allow us to avoid morbidity forthose patients who are unlikely to be cured. Consistent withprior reports [6], Williams et al identified that large numbersof patients can be ‘‘salvaged’’ despite failure of primary RT,but salvage therapy must be administered before canceradvances beyond where local treatment can reach. The bestpredictor of salvage success identified so far is serum PSA.
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 1 1 – 4 1 2
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
DOI of original article: 10.1016/j.eururo.2010.12.012* Tel. +1 216 839 3666; Fax: +1 216 839 3660.E-mail address: [email protected].
0302-2838/$ – see back matter # 2011 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2011.01.007

Local Recurrence
Cancer extension
Cryo feasibility
Informed consent
Cryotherapy
Surveillance
mpMRI Koelis° EF guided Bx Path
Bone Scan PET Choline
DRE Flexible HD-videoscopyTRUS
Alternatives Adverse effects
MRI 3M,12M PSA 3M, 12M,..
Adjuvant ADT 6-12M

Salvage Therapies for Radiorecurrent Prostate Cancer
Kamran Zargar-Shoshtari, Pranav Sharma and Julio Pow-Sang*
From the Department of Genitourinary Oncology, H. Lee Moffitt Cancer Center, Tampa, Florida
Abstract
Introduction: We report available salvage options in patients with biochemical recurrence after radiationtherapy for prostate cancer.Methods: We performed MEDLINE! searches for various salvage options and reviewed the most recentpublications on each modality.Results: Salvage radical prostatectomy, brachytherapy, cryotherapy and high intensity focused ultrasoundare the main therapeutic options available for men with biochemical recurrence after radiation therapy.These modalities have different side effect profiles. There is also wide variability in followup and reportingof oncologic outcomes. Androgen deprivation therapy remains the most common form of therapy afterbiochemical recurrence.Conclusions: No standard salvage therapy exists. Treatments are best administered at specialist centers wherethere is expertise with managing potential complications.
Key Words: prostatic neoplasms; radiotherapy; neoplasm recurrence, local; salvage therapy; prostate-specific antigen
Various options are available for the pri-mary treatment of PCa, although not everymodality is suitable in all patients. Success isdictated by clinical and pathological variables,and disease eventually recurs in certain pa-tients. A proportion of these patients may becandidates for salvage therapy.
Method
We reviewed the current status of salvage op-tions available for BCR after radiation therapyfor PCa (see figure). This is not a systematicreview of this topic. MEDLINE searches wereperformed for the terms surgery, radiationtherapy, brachytherapy, cryotherapy and highintensity focused ultrasound combined with
“key word and salvage and prostate.” Emphasiswas placed on the most recent review articlesand studies done in the last 10 years. Subse-quently we also searched the reference lists ofthese publications for other relevant articles.
Diagnosis
Recurrence can be classified based on clinicalsign, symptoms or location (local or systemic).However, after RT with curative intent BCR isoften the first sign of disease relapse. TheASTRO Phoenix definition of BCR followingRT is PSA greater than 2 ng/ml above the post-RT nadir with or without neoadjuvant ADT.1
The same definition is also often used aftercryotherapy, although no standardized defini-tion exists in this setting. After BCR is suspectedhistological confirmation is essential in patientswho are candidates for local salvage therapy.
Relevant Investigations
Confirmation of local recurrence and absentmetastatic disease is the first step when
Submitted for publication August 10, 2014.No direct or indirect commercial incentive associated
with publishing this article.* Correspondence: Genito-Urinary Oncology Program,
H. Lee Moffitt Cancer Center, 12902 Magnolia Dr., Tampa,Florida 33612 (telephone: 813-745-2226; FAX: 813-745-8494; e-mail address: [email protected]).
Abbreviationsand Acronyms
ADT = androgen deprivationtherapy
ASTRO = American Society forRadiation Oncology
BCR = biochemical recurrence
EBRT = external beamradiation therapy
HIFU = high intensity focusedultrasound
mMRI = multiparametricmagnetic resonance imaging
PCa = prostate cancer
PET/CT = positron emissiontomography/computerizedtomography
PSA = prostate specific antigen
RP = radical prostatectomy
RT = radiotherapy
SRP = salvage RP
SV = seminal vesicle
urologypracticejournal.com
2352-0779/15/23-126/0UROLOGY PRACTICE" 2015 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH, INC.
http://dx.doi.org/10.1016/j.urpr.2014.10.004Vol. 2, 126-132, May 2015
Published by Elsevier
Zargar, Urology Practice, 2015planning salvage therapy. Men with widely disseminated dis-ease are best treated with systemic therapies. Clinical andlaboratory variables can be used to stratify patients who maybenefit from further investigations and staging information.After failed treatment with EBRT or brachytherapy PET/CTand mMRI may be helpful to differentiate local vs systemicrecurrence. The detection rate depends on the PSA value andon kinetics, although imaging, including 11C choline PET/CT,is not sensitive for detecting micrometastatic disease. mMRIwith an endorectal coil is highly sensitive to detect recurrentPCa after RT. It can be used for accurate local staging andguiding biopsy but it cannot replace confirmatory tissue diag-nosis. While mMRI is operator dependent, after RT biopsyconfirmed recurrence the sensitivity of mMRI was reported tobe 80% to 94% in the PSA range of 0.4 to 6 ng/ml.2 Ata median PSA of 3.2 ng/ml 11C choline PET/CT has 93%sensitivity and can alter management in up to a third of pa-tients.3,4 Bone scan may be considered in cases of post-RTrecurrence. Although 18F-fluoride PET/CT has higher sensi-tivity than traditional technetium bone scintigraphy (93% vs51%), it is less specific (52% vs 82%) and can be positive whenthere is benign bone disease.5
Biopsy after RT has an important role in planning salvagetreatment. However, histological changes following RT usuallyrequire an 18 to 24-month delay before biopsy. False-negativeand false-positive results were observed in 19% and 30%of cases, respectively, when early biopsy was performed at12 months.6,7
Patients with SV involvement and more locally advanceddisease have a higher likelihood of harboring occult metastaticdisease. Some clinicians consider these men unsuitable candi-dates for local salvage therapy because the efficacy of a numberof local salvage options is decreased in the presence ofSV infiltration. SV biopsy can be considered in cases in
which the confirmation of SV involvement could impactmanagement. This may be based on mMRI findings or onclinical examination.
A 70% to 80% disease-free survival rate was reportedin patients with localized disease compared to 40% to 60% inthose with more advanced disease.8,9 Therefore a proportion ofmen with clinically nonmetastatic disease who show features ofhigh risk disease such as high PSA, brief PSA doubling time,cT3 or greater, high volume and high Gleason scores on bi-opsy, may not benefit from salvage therapy. Careful patientconsultation and selection should be essential parts of thetreatment algorithm.
Recurrence after RT
Salvage Radical Prostatectomy
SRP after RT has an extended history as a treatment alternativebut the morbidity associated with SRP has limited widespreaduse. Earlier detection, improved surgical technique and betterpatient selection have led to SRP being considered a viableoption at specialized centers.
When considering SRP after RT, metastatic disease shouldbe ruled out. Bone assessment for metastatic disease andabdominopelvic computerized tomography or magnetic reso-nance imaging are recommended. Additionally, biopsy shouldbe done to confirm disease recurrence. Ideal candidates arethose with biopsy proven local recurrence, T1-T2 diseasebefore initial radiation, PSA less than 10 ng/ml and no evi-dence of metastatic disease. PSA at salvage surgery is a strongpredictor of BCR-free and overall survival. Patients should alsohave adequately long life expectancy to benefit from salvagetherapy. A review of SRP data showed a decreased positivesurgical margin rate in more contemporary studies (0% to
Radiation Therapy
Biochemical RecurrencePSA>2 ng/ml above Nadir
Repeat StagingHistological Confirmation
Local Recurrence andCandidate for Salvage Therapy
Systemic Recurrence orNot candidate for Salvage
HIFUTreatment for
Oligometastatic disease
Surgery Brachytherapy Cryotherapy Androgen Deprivation
Figure. Study outline
127Salvage Therapies for Radiorecurrent Prostate Cancer
Quite a few large series

The variability in results probably reflected the heterogeneity in outcome definition, which significantlylimits the comparability of the results.
Sexual dysfunctionUsing different definitions of sexual dysfunction, the sexual dysfunction rate for salvage cryotherapy212 was68.8% at 1 year and 51.9% at 2 years. The figures for salvage RP (based on different definitions) were81% at 1 year215 and 74% at a median of 18 months.213
Quality of lifeOnly one study on salvage ablative therapy reported on quality of life outcomes; this was Robinson 2006212
on salvage cryotherapy. One study on salvage RP reported on quality of life outcomes.214 The data werelimited by heterogeneity of the different quality of life measures used, different time points of outcomemeasurement and different means of reporting (e.g. total score vs. individual component score).
Adverse eventsOnly three studies on salvage ablative therapies reported on adverse events: two studies on salvagecryotherapy208,212 and one on salvage HIFU.120 Six studies of salvage RP reported on adverse events.209–211,213–215
For salvage cryotherapy, at a median follow-up of 18.6 months, the incidence of adverse events was relativelylow, ranging from 2% (bladder neck stenosis) to 3% (rectourethral fistula). The corresponding figure forsalvage RP, within a similar period of follow-up, was 4.8–6% (rectovesical fistula) and 3–25% (bladder neckstenosis or anastomotic stricture). For salvage HIFU, at 15 months follow-up, the incidence of rectourethralfistula was 6% and that of bladder neck stenosis was 17%. The data were limited by the relatively lownumber of patients and low event rates.
Summary and conclusions from the evidence of thecomparative effectiveness of salvage ablative therapy
This review considered data from 400 participants treated with salvage therapy following primary EBRT acrossnine studies,120,208–215 all of which were single-arm case series. Six studies involved salvage RP,209–211,213–215 twoinvolved salvage cryotherapy208,212 and one involved salvage HIFU.120 All of the studies were considered ashaving a high risk of bias. Consequently, the findings should be interpreted cautiously to reflect the extremelypoor quality of the evidence base and the heterogeneity of outcome definition, different time points ofoutcome measurement and different means of outcome reporting. Data on the long-term effectivenessof salvage therapy were limited, with the majority of studies reporting on short-term data only.
In the short term, there was no robust evidence that mortality or other cancer-specific outcomes(biochemical disease-free survival or failure) differed between salvage cryotherapy and salvage RP.There were no data on cancer-specific outcomes for salvage HIFU.
With regard to functional outcomes, including urinary and sexual dysfunction and quality of life outcomes,the limited data prevented any valid conclusions from being made.
For adverse event outcomes, therewas a general trend for salvage cryotherapy to have fewer procedure-relatedcomplications, especially for bladder neck stenosis (up to 2% at amedian of 18.6months), in comparison withsalvage HIFU (up to 17%at amedian of 15months) and salvage RP (up to 25%at amedian of 20months).However, the data limitations render these findings uncertain at best.
In conclusion, the results of this review on salvage therapies were associated with large uncertainty owingto the quality and quantity of the evidence base. There was a lack of long-term direct measures ofeffectiveness and a lack of prospective comparative studies. There was no evidence to suggest that salvageablative therapy was either better or worse than salvage RP following primary EBRT for any outcomes.
EFFECTIVENESS OF SALVAGE ABLATIVE THERAPY FOLLOWING PRIMARY EXTERNAL BEAM RADIOTHERAPY
NIHR Journals Library www.journalslibrary.nihr.ac.uk
70
HEALTH TECHNOLOGY ASSESSMENTVOLUME 19 ISSUE 49 JULY 2015
ISSN 1366-5278
DOI 10.3310/hta19490
Ablative therapy for people with localised prostate cancer: a systematic review and economic evaluation
Craig R Ramsay, Temitope E Adewuyi, Joanne Gray, Jenni Hislop, Mark DF Shirley, Shalmini Jayakody, Graeme MacLennan, Cynthia Fraser, Sara MacLennan, Miriam Brazzelli, James N’Dow, Robert Pickard, Clare Robertson, Kieran Rothnie, Stephen P Rushton, Luke Vale and Thomas B Lam
Ramsay, Health Technology Assessment 2015
« There was no evidence that salvage ablative therapy was either better or worse than salvage RP following primary EBRT for any outcomes »

Platinum Priority – Prostate CancerEditorial by J. Stephen Jones on pp. 411–412 of this issue
Disease-Free Survival Following Salvage Cryotherapy forBiopsy-Proven Radio-Recurrent Prostate Cancer
Andrew K. Williams a, Carlos H. Martınez a, Chen Lu a, Chee Kwan Ng b,Stephen E. Pautler a, Joseph L. Chin a,*a Departments of Urology and Oncology, University of Western Ontario, London, Ontario, Canadab Department of Urology, Tan Tock Seng Hospital, Singapore
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 0 5 – 4 1 0
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted December 10, 2010Published online ahead ofprint on December 21, 2010
Keywords:Prostate cancerCryotherapyRadiationRecurrence
Abstract
Background: The optimum treatment of prostate cancer recurrence followingradiation therapy (RT) remains controversial due to the lack of long-term data.Objective: Our aim was to review the survival of patients who underwent salvagecryotherapy to the prostate gland for biopsy-proven recurrent prostate cancer andestablish prognostic indicators.Design, setting, and participants: A retrospective analysis was performed on allpatients undergoing salvage cryotherapy at an academic urology unit for biopsy-proven locally recurrent prostate cancer after RT from 1995 to 2004. Patients’preoperative, perioperative, and postoperative data were reviewed and recorded.Intervention: Two freeze-thaw cycles of transperineal cryotherapy were per-formed under transrectal ultrasound guidance by a single surgeon.Measurements: The primary outcome was survival. Secondary outcomes weredisease-free survival (DFS), metastasis-free survival, and progression to andro-gen-deprivation therapy.Results and limitations: Of 187 patients, 176 had records available for follow-up(follow-up rate: 94%). Mean follow-up was 7.46 yr (range: 1–14 yr). Fifty-twopatients were followed for>10 yr. DFS at 10 yr was 39%. Risk factors for recurrencewere presalvage prostate-specific antigen (PSA), preradiation, and presalvageGleason score. A PSA nadir >1.0 ng/dl was highly predictive of early recurrence.Conclusions: Salvage cryotherapy led to an acceptable 10-yr DFS. Presalvage PSAand Gleason score were the best predictors of disease recurrence. A PSA nadir >1ng/dl following cryotherapy indicated a poor prognosis, and recurrence of diseasewas universal in these patients.# 2010 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Urology, London Health Sciences Centre, 800 CommissionersRd, London, Ontario, Canada N6AAG5. Tel. +1 519 685 8451; Fax: +1 519 685 8455.E-mail address: [email protected] (J.L. Chin).
0302-2838/$ – see back matter # 2010 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2010.12.012
Williams, Eur Urol 2011be palatable to patients. It could be argued it would beunethical in the context of documented 10-yr biochemicalrecurrence-free survival rates of 39%.
Salvage cryotherapy was shown to have incontinencerates of 36% and fistula rates of 2.6% across studies incomparison with salvage RP with incontinence rates of 41%and rectal injury rates of 2–15% [3]. The complication ratesof the current cohort were previously described [4] and areconsistent with the literature [9,10]. This cohort had 37%mild and 3% severe incontinence rates, along with a 2%fistula rate that we find acceptable in a salvage setting. Webelieve that just as primary treatment needs to be tailoredto the individual, so does salvage treatment. Although norandomized head-to-head comparison exists, this studyreaffirms that salvage cryotherapy is a reasonable alterna-tive to salvage RP, particularly in patients with significantmedical comorbidity but a significant life expectancy. Webelieve that RP still plays a role in the management of radio-recurrent prostate cancer. However, it requires a motivatedand younger patient with few comorbidities who is willingto accept the associated morbidity.
It has become increasingly apparent that ADT is associatedwith a significant increase in non–prostate-related diseasessuch as cardiovascular disease and osteoporosis [11], albeitnot without some debate [12–14]. These results show thatwith a mean follow-up of nearly 8 yr, only 38.6% of patientswent on to ADT, which leads to a well-documented reductionin quality of life. Keating et al [15] demonstrated thatgonadotropin-releasing hormone agonist treatment led to anincreased rate of myocardial infarction, stroke, diabetes, andsudden cardiac death in a cohort of 37 443 patients. It isimportant to note that these data only had a short medianfollow-up of 2.6 yr, and it would be reasonable to suggest therisk of cardiovascular disease continues with ongoing ADT. Inaddition to the obvious financial benefit, we also speculate
that we may delay the development of androgen resistance. Itis unlikely there will ever be randomized studies to comparemortality rates between patients undergoing salvage treat-ment (who we must acknowledge are likely to have fewercomorbidities) with patients receiving ADT, and therefore itis observational data we must rely on.
This study has shown that patients with presalvage PSA>10 ng/dl had very high recurrence rates and tended to recurearly, and we do not believe they are good candidates forsalvage cryotherapy. This concurs with other salvage studiesthat have shown this effect at the 5-yr mark [9,16]. Our dataalso highlight the role of rebiopsy and Gleason score inpredicting response to subsequent salvage cryotherapy.Presalvage biopsies obviously must be viewed with somecaution, given the changes induced by radiation. However,these were able to predict prognosis, whereas preradiationGleason scores had no predictive value in our cohort. Patientswith Gleason !7 disease on presalvage biopsy had a higherrisk of recurrence that was not statistically different frompatients with Gleason !8 disease. The recurrence rates inpatient with Gleason 7, 8, or 9 disease was still acceptable at33%. Given the theoretical benefit of cryotherapy beingcytocidal regardless of tumor grade, we believe the presenceof high-grade cancer should not exclude a patient withotherwise favorable features, most notably a low PSA, fromsalvage treatment.
We therefore believe patients should not be excludedbased on a higher Gleason score on preradiation biopsy butshould be counseled about a higher risk of recurrence. Wesuggest any patient with a presalvage PSA >10 ng/dl is apoor candidate for salvage cryoablation, and patients with aPSA between 5 and 10 ng/dl should be counseled abouttheir increased risk of recurrence. We found no correlationin the time between initial and salvage treatment to higherrecurrence rates.
[()TD$FIG]
% S
urvi
ving
0
20
40
60
80
100
Time (Months)
0 12 24 36 48 60 72 84 96 108 120
Overall SurvivalDisease Free Survival
Mo 0 24 48 72 96 120
No. of patients 176 156 134 113 88 52
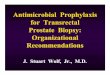
Fig. 4 – Kaplan-Meier curve for overall and disease-free survival with corresponding n values.
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 0 5 – 4 1 0 409
Single institution London (Ontario) 2nd generation cryo. (1994-2004)
176 radio-recurrent PCa
10 year Overall survival: 90%
10 year Disease-free survival: 40%

Gleason!6 disease (Fig. 3). However, patients with Gleason7 disease had similar 10-yr survival to those with Gleason"8 disease (both 33%).
Postsalvage PSA nadir was strongly associated withdisease recurrence. A PSA nadir of>1 ng/dl had a RR ratio of6.63 ( p < 0.001) for recurrence (95% confidence interval,4.1–10.6) and was associated with disease-free rates of 3%,0%, and 0% at 5, 8, and 10 yr, respectively. In contrast, PSAnadir <1 ng/dl was associated with a DFS of 56%, 46%, and46%, respectively (Fig. 4).
4. Discussion
This study reports the intermediate-term results in patientswith biopsy-proven local recurrence of prostate cancerfollowing RT. We are limited as always by the retrospectivenature of studies such as this and the evolution to newertechnologies that inevitably occurs over a period of follow-up. It is likely that morbidity has reduced and efficacy hasincreased with newer technologies, but it will take at least10 yr for validation.
It is difficult to correlate our work with the onlypreviously large cohort of salvage cryotherapy patients[5] due to the heterogeneity in a multi-institutionaldatabase. Our study was limited to patients with biopsy-proven cancer who underwent a method of standardizedscreening for localized disease, and follow-up biopsies wereperformed in 95.7% versus 16.5% from the Cyro On-LineDatabase registry.
As demonstrated in the Kaplan-Meier curves, this studyindicates DFS rates with very little change to the survivalbetween 8 and 10 yr despite the fact that median follow-upof the 176 patients was nearly 8 yr and 52 patients werefollowed >10 yr.
A recent HIFU study on establishing a definition forrecurrence [6] highlighted the high sensitivity and lowspecificity of the American Society for Therapeutic Radiol-ogy and Oncology (ASTRO) definition versus the lowsensitivity and high specificity of the Phoenix definition.This likely applies in analyzing cryotherapy data. Pisterset al [7] describe inferior recurrence-free survival withcryotherapy using a variety of definitions. However, notably
[()TD$FIG]
_
Fig. 1 – Kaplan-Meier curve for presalvage prostate-specific antigen (PSA; nanograms per deciliter) with corresponding n values.
Table 2 – Presalvage characteristics
PresalvageGleason score
Before RT Relative risk for recurrence(95% confidence interval)
!6 38 1
7 50 1.69 (0.91–3.11)
"8 57 1.92 (1.06–3.49)
Presalvage PSA, ng/dl
<5 84 1
5–10 56 2.8 (1.7–4.7)
>10 34 5.1 (3.0–8.7)
Age at time of salvage treatment, yr
<70 83 1.45 (0.96–2.2)
>70 92 1
Range: 54–82, IQR: 65–74
Time between primary and salvage treatments, yr
<5 85 1.05 (0.81–1.13)
>5 56 1
IQR = interquartile range; PSA = prostate-specific antigen; RT, radiation
therapy.
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 0 5 – 4 1 0 407
no analysis was shown using the Phoenix definition of PSAnadir plus 2 ng/ml, and they described recurrence rates thatare significantly higher than our series. From our experiencewe have seen significantly higher biochemical recurrencerates in this cohort using the ASTRO definition [8] that donot seem to translate to an increased recurrence rate withtime under the Phoenix definition. This highlights the factthat with a lack of a validated standard definition of failure,
long-term follow-up is required. Comparisons betweentreatment modalities can be heavily influenced by thedefinitions used. Regardless, we have demonstrated asignificant overall recurrence-free survival that can beoptimized with appropriate stringent patient selection. Weacknowledge that we have not proven any survival benefitfor this treatment given the absence of any control arm. Atrial of salvage versus observation, however, is unlikely to
[()TD$FIG]
Fig. 2 – Kaplan-Meier curve for prostate-specific antigen (PSA) nadir (nanograms per deciliter) with corresponding n values.
[()TD$FIG]
% D
isea
se F
ree
0
20
40
60
80
100
Time (Months)
0 12 24 36 48 60 72 84 96 108 120
< 7 7 > 7
Mo 0 24 48 72 96 120
Gleason <7 38 36 34 30 18 8
Gleason 7 50 47 39 33 28 18
Gleason >7 57 46 39 35 29 18
Fig. 3 – Kaplan-Meier curve for presalvage Gleason scores with corresponding n values.
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 0 5 – 4 1 0408
Pre-salvage PSA (5 or 10ng/mL) Pre Salvage Bx Gleason score
Williams, Eur Urol 2011
Two pre-salvage prognostic factors
It’s therefore important to refer patients as early as possible after failure (Phoenix)

no analysis was shown using the Phoenix definition of PSAnadir plus 2 ng/ml, and they described recurrence rates thatare significantly higher than our series. From our experiencewe have seen significantly higher biochemical recurrencerates in this cohort using the ASTRO definition [8] that donot seem to translate to an increased recurrence rate withtime under the Phoenix definition. This highlights the factthat with a lack of a validated standard definition of failure,
long-term follow-up is required. Comparisons betweentreatment modalities can be heavily influenced by thedefinitions used. Regardless, we have demonstrated asignificant overall recurrence-free survival that can beoptimized with appropriate stringent patient selection. Weacknowledge that we have not proven any survival benefitfor this treatment given the absence of any control arm. Atrial of salvage versus observation, however, is unlikely to
[()TD$FIG]
Fig. 2 – Kaplan-Meier curve for prostate-specific antigen (PSA) nadir (nanograms per deciliter) with corresponding n values.
[()TD$FIG]
% D
isea
se F
ree
0
20
40
60
80
100
Time (Months)
0 12 24 36 48 60 72 84 96 108 120
< 7 7 > 7
Mo 0 24 48 72 96 120
Gleason <7 38 36 34 30 18 8
Gleason 7 50 47 39 33 28 18
Gleason >7 57 46 39 35 29 18
Fig. 3 – Kaplan-Meier curve for presalvage Gleason scores with corresponding n values.
E U R O P E A N U R O L O G Y 6 0 ( 2 0 1 1 ) 4 0 5 – 4 1 0408
PSA nadir <1ng/ml as post-salvage prognostic indicator

T
Thank You

![Dramatic Reduction of CEA Post Spray Cryotherapy in a Patient … · 2018-06-09 · chemotherapy with cryotherapy [2-5]. Standard, slow-energy transfer cryotherapy or cryosurgery](https://img.pdfslide.net/doc/110x75/5e852869e78a231248157db5/dramatic-reduction-of-cea-post-spray-cryotherapy-in-a-patient-2018-06-09-chemotherapy.jpg)






![Cryotherapy: Physiological Considerations and Applications ...cdn.intechopen.com/pdfs/35000.pdf · Rokita 2006]. Cryogenic liquids, ... Cryotherapy: Physiological Considerations and](https://img.pdfslide.net/doc/110x75/5a9e4c127f8b9a077e8b53ef/cryotherapy-physiological-considerations-and-applications-cdn-2006-cryogenic.jpg)