Embed Size (px)
Citation preview

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 11
OklahomaOklahomaPrehospital Pediatric Prehospital Pediatric
SupplementSupplementDeveloped by the Oklahoma EMSC Resource Center for the:Developed by the Oklahoma EMSC Resource Center for the:
““Infants and Children Module of the Infants and Children Module of the 1994 EMT-Basic Curriculum”1994 EMT-Basic Curriculum”
PART 1: INTRODUCTORYPART 1: INTRODUCTORY

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 22
IntroductionIntroduction
• OSDH-EMS approvedOSDH-EMS approved– PAC’s course to include in EMT-B 1998’s NSC in PAC’s course to include in EMT-B 1998’s NSC in
19931993– USDOT-NHTSA: EMT-B 1994’s NSC in USDOT-NHTSA: EMT-B 1994’s NSC in 19951995– EMSC Pediatric Supplement (Revision of PAC’s) EMSC Pediatric Supplement (Revision of PAC’s)
to include in EMT-B 1994’s NSC in to include in EMT-B 1994’s NSC in 19961996
• Mandatory inclusion into EMT-B coursesMandatory inclusion into EMT-B courses

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 33
PART 1PART 1:: IntroductoryIntroductory
This section covers the following informational areas.This section covers the following informational areas.
- - Emergency Medical ServicesEmergency Medical Services for for ChildrenChildren
- Injury Prevention Methodology- Injury Prevention Methodology
- Anatomy and Physiology- Anatomy and Physiology
- Approaching Children- Approaching Children
- Vital Signs Assessment- Vital Signs Assessment
- Assessment Tools- Assessment Tools

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 44
ObjectivesObjectives
• Define Emergency Medical Services for Define Emergency Medical Services for Children Children ((EMSCEMSC).).– Objective: 6-1.0Objective: 6-1.0
• Discuss how an integrated EMSC system Discuss how an integrated EMSC system can affect patient outcome.can affect patient outcome.– Objective: 6-1.0 AObjective: 6-1.0 A
• Identify methods/mechanisms of injury Identify methods/mechanisms of injury prevention for Infants and Children.prevention for Infants and Children.– Objective: 6-1.0 BObjective: 6-1.0 B

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 55
Objectives Objectives ((ContinuedContinued))
• Identify two (2) anatomic and physiologic Identify two (2) anatomic and physiologic differences between children and adults differences between children and adults regarding skin and body surface.regarding skin and body surface.– Objective: 6-1.2 AObjective: 6-1.2 A
• Identify four (4) areas to consider when Identify four (4) areas to consider when taking the child’s history.taking the child’s history.– Objective: 6-1.3 AObjective: 6-1.3 A

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 66
Objectives Objectives ((ContinuedContinued))
• Describe important factors in taking and Describe important factors in taking and interpreting vital signs. interpreting vital signs. Objective: 6-1.3 BObjective: 6-1.3 B
– PulsePulse– RespirationsRespirations– Blood PressureBlood Pressure– TemperatureTemperature
• Identify a minimum of four (4) significant Identify a minimum of four (4) significant differences between the adult and pediatric differences between the adult and pediatric airway which affect ventilation.airway which affect ventilation.– Objective: 6-1.3 CObjective: 6-1.3 C

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 77
Emergency Medical Services Emergency Medical Services for Children for Children ((EMSCEMSC))
OBJECTIVE: 6-1.0OBJECTIVE: 6-1.0• DefinitionDefinition
– A program designed to reduce child and youth A program designed to reduce child and youth mortality and morbidity due to severe illness or mortality and morbidity due to severe illness or trauma.trauma.
• HistoryHistory– 1984 Legislation1984 Legislation
• National ManagementNational Management– MCHBMCHB– NHTSANHTSA
• Oklahoma ManagementOklahoma Management– OUHSCOUHSC

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 88
EMSC EMSC ((ContinuedContinued))
• National Resource CentersNational Resource Centers– National EMSC-NRCNational EMSC-NRC– National EMSC Resource Alliance National EMSC Resource Alliance ((NERANERA))
• Oklahoma Resource CenterOklahoma Resource Center– Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center
• Oklahoma Education and TrainingOklahoma Education and Training– Pediatric Specialty CoursesPediatric Specialty Courses
• PALSPALS• PEPPPEPP• PPCPPC• ENPCENPC

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 99
EMSC EMSC ((ContinuedContinued))
– Prehospital CurriculaPrehospital Curricula• Pediatric ’94 NSC SupplementPediatric ’94 NSC Supplement• Injury PreventionInjury Prevention• Bystander CareBystander Care
– Emergency 1Emergency 1stst Care for Childcare Providers Care for Childcare Providers– Childcare Health and Safety CoursesChildcare Health and Safety Courses– Other AreasOther Areas
• Pediatric Resource LibraryPediatric Resource Library– EducationEducation
– Assessment and Management ToolsAssessment and Management Tools
– Information CenterInformation Center
• Instructional Outcome Statistics and ImprovementInstructional Outcome Statistics and Improvement

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1010
EMSC EMSC ((ContinuedContinued))
OBJECTIVE 6-1.0 AOBJECTIVE 6-1.0 A• Integrated EMSC SystemsIntegrated EMSC Systems
– PreventionPrevention– PrehospitalPrehospital– E D’sE D’s– I C U’sI C U’s– RehabRehab– CommunityCommunity– PsychologicalPsychological– Trauma SystemsTrauma Systems– State AgenciesState Agencies

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1111
EMSC EMSC ((ContinuedContinued))
• Patient Outcome AffectPatient Outcome Affect– PreventionPrevention– ReductionReduction
• EmergenciesEmergencies• DisabilityDisability• DeathDeath• Negative ImpactNegative Impact
– FamilyFamily
– CommunityCommunity

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1212
Injury PreventionInjury Prevention
OBJECTIVE 6-1.0 BOBJECTIVE 6-1.0 B• Methodology and MechanismsMethodology and Mechanisms
– C P R and 1C P R and 1stst Aid Aid• TrainingTraining• CertificationCertification• RequirementRequirement
– Bicycle SafetyBicycle Safety– Community Injury Prevention ProgramsCommunity Injury Prevention Programs
• Data AnalysisData Analysis• Common Injury Specific EducationCommon Injury Specific Education

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1313
AnatomyAnatomy and and Physiology Physiology ((AA&&PP))
OBJECTIVE 6-1.2 AOBJECTIVE 6-1.2 A• Skin and Body Surface Area Skin and Body Surface Area ((BSABSA))
– Infants and Young ChildrenInfants and Young Children• Head = 20% BSAHead = 20% BSA• BSA Larger in Proportion to Body MassBSA Larger in Proportion to Body Mass
– Changes by Body Part through ChildhoodChanges by Body Part through Childhood– Assumes Adult as AdolescentAssumes Adult as Adolescent
• Thin Skin and Less Subcutaneous FatThin Skin and Less Subcutaneous Fat• Prone to Hypothermia and Deeper Burns than AdultProne to Hypothermia and Deeper Burns than Adult• Resuscitation and Drug Therapy Reduced in Resuscitation and Drug Therapy Reduced in
HyperthermiaHyperthermia
– Newborn Temperature Regulation Not Well Newborn Temperature Regulation Not Well DevelopedDeveloped

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1414
AA && P P ((ContinuedContinued))

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1515
Pediatric ApproachPediatric Approach
OBJECTIVE 6-1.3 AOBJECTIVE 6-1.3 A• Obtaining a HistoryObtaining a History
– Primary CaregiverPrimary Caregiver• InformationInformation• Reassures and CalmsReassures and Calms
– Elements Similar to AdultElements Similar to Adult– Additional ElementsAdditional Elements
• Birth WeightBirth Weight• Problems with PregnancyProblems with Pregnancy• Current Estimated WeightCurrent Estimated Weight

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1616
Pediatric Approach Pediatric Approach ((ContinuedContinued))
• Cooperation EnhancementCooperation Enhancement– Permit “Transition Phase”Permit “Transition Phase”– Level of ChildLevel of Child
• Calm and Friendly MannerismCalm and Friendly Mannerism
– Cooperation of ChildCooperation of Child– Uncooperative ChildUncooperative Child
• A-B-C’s Appropriate?A-B-C’s Appropriate?• Condition Known?Condition Known?• Don’t Waste Time!Don’t Waste Time!

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1717
Pediatric ApproachPediatric Approach ((ContinuedContinued))
• General Examination GuidelinesGeneral Examination Guidelines– Remain and Display CalmnessRemain and Display Calmness– AssessmentAssessment
• Life-Threatening = Head to ToeLife-Threatening = Head to Toe• Non-Life-Threatening = Toe to HeadNon-Life-Threatening = Toe to Head• Non-Traumatic = In Caregivers Lap/ArmsNon-Traumatic = In Caregivers Lap/Arms• Use Assessment ToolsUse Assessment Tools• Take Opportune AdvantagesTake Opportune Advantages
– Color and Moistness of Mucous MembranesColor and Moistness of Mucous Membranes
– Presence of TearsPresence of Tears
– Inspiratory Breath SoundsInspiratory Breath Sounds

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1818
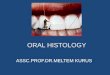
Pediatric Assessment Pediatric Assessment Triangle Triangle ((PATPAT))
APPEARANCEAPPEARANCEAPPEARANCEAPPEARANCE WORK WORK OF OF BREATHINGBREATHINGWORK WORK OF OF BREATHINGBREATHING
CIRCULATION CIRCULATION TO TO SKINSKINCIRCULATION CIRCULATION TO TO SKINSKIN
PPAATT does not exclude an initial or focused assessment, but by precluding does not exclude an initial or focused assessment, but by precluding it complements them giving opportunity for immediate interventions to be it complements them giving opportunity for immediate interventions to be established.established.

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 1919
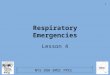
Pediatric Trauma Score Pediatric Trauma Score ((PTSPTS))
COMPONENTSCOMPONENTS +2+2 +1+1 -1-1
WEIGHTWEIGHT >20 kg>20 kg(>44 lbs)(>44 lbs)
10-20 kg10-20 kg(22-44 lbs)(22-44 lbs)
<10 kg<10 kg(<22 lbs)(<22 lbs)
AIRWAYAIRWAY PATENTPATENT MAINTAINABLEMAINTAINABLE NON – NON – MAINTAINABLEMAINTAINABLE
SYSTOLIC BP SYSTOLIC BP (AUSCULTATED)(AUSCULTATED)
>90 mmHg>90 mmHg 50-90 mmHg50-90 mmHg <50 mmHg<50 mmHg
(PALPATED PULSE)(PALPATED PULSE) RADIALRADIAL CAROTIDCAROTID NONENONE
MENTAL STATUSMENTAL STATUS Awake VERBALVERBAL OR OR PAINPAIN UNRESPONSIVEUNRESPONSIVE
FRACTURESFRACTURES NONENONE CLOSEDCLOSED OR OR
SUSPECTEDSUSPECTEDMULTIPLEMULTIPLEOPENOPEN OR OR
CLOSEDCLOSED
WOUNDSWOUNDS NONENONE MINORMINOR MAJORMAJOR
BURNS BURNS OROR
PENETRATINGPENETRATING

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2020
Other Assessment ToolsOther Assessment Tools
4 4 SPONTANEOUSSPONTANEOUS
3 3 SPEECHSPEECH
2 2 PAINPAIN
1 1 NONENONE
6 6 OBEYS COMMANDSOBEYS COMMANDS
5 5 LOCALIZED PAINLOCALIZED PAIN
4 4 WITHDRAWSWITHDRAWS TO TO PAINPAIN
3 3 DECORTICATE/FLEXIONDECORTICATE/FLEXION
2 2 DECEREBRATE/EXTENSIONDECEREBRATE/EXTENSION
1 1 NONENONE
5 5 ORIENTED/BABBLESORIENTED/BABBLES
4 4 CONFUSED/CRYINGCONFUSED/CRYING
3 3 CRYCRY TO TO PAINPAIN
2 2 INCOMPREHENSIBLEINCOMPREHENSIBLE
1 1 NONENONE
EYESEYES MOTORMOTOR VERBALVERBAL
GLASGOW COMA SCALE (GLASGOW COMA SCALE (GCSGCS))

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2121
AGEAGE kgkg H-RH-R R-RR-R SYS-BPSYS-BP DIAS-BPDIAS-BP TIDAL VOLUMETIDAL VOLUME
N-BN-B 33 120-160120-160 30-6030-60 74-10074-100 50-7050-70 30-45 mL30-45 mL
1 m1 m 44 120-160120-160 30-6030-60 74-10074-100 50-7050-70 40-60 mL40-60 mL
2 m2 m 55 120-160120-160 30-6030-60 74-10074-100 50-7050-70 50-75 mL50-75 mL
3 m3 m 66 120-160120-160 30-6030-60 74-10074-100 50-7050-70 60-90 mL60-90 mL
6 m6 m 77 120-160120-160 30-6030-60 74-10074-100 50-7050-70 70-105 mL70-105 mL
8 m8 m 88 110-150110-150 30-6030-60 74-10074-100 50-7050-70 80-120 mL80-120 mL
10 m10 m 99 110-150110-150 30-6030-60 74-10074-100 50-7050-70 90-135 mL90-135 mL
1 y1 y 1010 90-14090-140 20-4020-40 8282 5454 100-150 mL100-150 mL
1 y1 y 1111 90-14090-140 20-4020-40 8282 5454 110-165 mL110-165 mL
2 y2 y 1212 90-14090-140 20-4020-40 8484 5656 120-180 mL120-180 mL
2 y2 y 1313 90-14090-140 20-4020-40 8484 5656 130-195 mL130-195 mL
3 y3 y 1414 90-14090-140 20-4020-40 8686 5858 140-210 mL140-210 mL
3 y3 y 1515 90-14090-140 20-4020-40 8686 5858 150-225 mL150-225 mL
4 y4 y 1616 80-12080-120 20-4020-40 8888 6060 160-240 mL160-240 mL
4 y4 y 1717 80-12080-120 20-4020-40 8888 6060 170-255 mL170-255 mL
5 y5 y 1818 60-12060-120 16-3016-30 9090 6060 180-270 mL180-270 mL
5 y5 y 1919 60-12060-120 16-3016-30 9090 6060 190-285 mL190-285 mL
6 y6 y 2020 60-12060-120 16-3016-30 9292 6262 200-300 mL200-300 mL
7 y7 y 2222 60-12060-120 16-3016-30 9494 6262 220-330 mL220-330 mL
7 y7 y 2424 60-12060-120 16-3016-30 9494 6262 240-360 mL240-360 mL
8 y8 y 2626 60-12060-120 16-3016-30 9696 6464 260-390 mL260-390 mL
9 y9 y 2828 60-12060-120 16-3016-30 9898 6666 280-420 mL280-420 mL

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2222
Vital SignsVital Signs
OBJECTIVE 6-1.3 BOBJECTIVE 6-1.3 B• PULSEPULSE
– CENTRALCENTRAL• CarotidCarotid• FemoralFemoral
– PERIPHERALPERIPHERAL• RadialRadial• BrachialBrachial• PoplitealPopliteal• PedalPedal

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2323
Vital SignsVital Signs ((ContinuedContinued))
– Monitor PulseMonitor Pulse• 30 seconds minimum30 seconds minimum• Rate and QualityRate and Quality• Central and PeripheralCentral and Peripheral
– Tachycardia (Tachycardia (FastFast) and Triggers) and Triggers• Compensatory MechanismCompensatory Mechanism• ShockShock• AnxietyAnxiety• FeverFever• PainPain• Medical IllnessMedical Illness• Traumatic InjuryTraumatic Injury• Environmental InsultEnvironmental Insult

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2424
Vital SignsVital Signs ((ContinuedContinued))
– Bradycardia (Bradycardia (SlowSlow) and Triggers) and Triggers• End Stages ShockEnd Stages Shock• HypothermiaHypothermia• Hypoxia/HypoxemiaHypoxia/Hypoxemia• Cardiac PathologyCardiac Pathology• Congenital AnomaliesCongenital Anomalies• Certain MedicationsCertain Medications
– Rates Decrease through Childhood to Rates Decrease through Childhood to AdolescenceAdolescence

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2525
Vital SignsVital Signs ((ContinuedContinued))
• RESPIRATIONRESPIRATION– OBSERVATIONOBSERVATION
• Begins with P-A-TBegins with P-A-T• Prior to and During ExamPrior to and During Exam• For FollowingFor Following
– Tachypnea (Tachypnea (FastFast) or Bradypnea () or Bradypnea (SlowSlow))– Hyperpnea (Hyperpnea (DeepDeep) or Hypopnea () or Hypopnea (ShallowShallow))– Apnea (Apnea (AbsentAbsent))– Use of Accessory MusclesUse of Accessory Muscles
» Intercostal, Subcostal, Subclavicular, or DiaphragmaticIntercostal, Subcostal, Subclavicular, or Diaphragmatic
– NoisesNoises» Wheezing (Inspiratory and/or Expiratory), Grunting Wheezing (Inspiratory and/or Expiratory), Grunting
(Expiratory), Rhonchi (Upper Airway Rattling), Rales (Lower (Expiratory), Rhonchi (Upper Airway Rattling), Rales (Lower Airway Crackles)Airway Crackles)
– Nasal FlaringNasal Flaring

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2626
Vital SignsVital Signs ((ContinuedContinued))
– Tachypnea (Tachypnea (FastFast) and Triggers) and Triggers• Compensatory MechanismCompensatory Mechanism• ShockShock• AnxietyAnxiety• FeverFever• PainPain• Medical IllnessMedical Illness• Traumatic InjuryTraumatic Injury• Environmental InsultEnvironmental Insult
– MonitorMonitor• 30 seconds minimum30 seconds minimum• Rate, Depth, and QualityRate, Depth, and Quality

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2727
Vital SignsVital Signs ((ContinuedContinued))
• BLOOD PRESSUREBLOOD PRESSURE– Compensatory Mechanism Sustains Compensatory Mechanism Sustains
Normotension (Normal BP) Longer in PediatricsNormotension (Normal BP) Longer in Pediatrics– Hypotension (Low BP) Confirms Decompensated Hypotension (Low BP) Confirms Decompensated
ShockShock– Peripheral Pulse PresencePeripheral Pulse Presence
• Infants (Birth to 12 months) = Minimum Systolic Infants (Birth to 12 months) = Minimum Systolic Pressure of 60 mmHgPressure of 60 mmHg
• Children (1 year to 8 years) = Minimum Systolic Children (1 year to 8 years) = Minimum Systolic Pressure of 70 + (2 x Age in Years)Pressure of 70 + (2 x Age in Years)
– Normal Diastolic = 2/3 SystolicNormal Diastolic = 2/3 Systolic– Appropriate Size BP Cuff MandatoryAppropriate Size BP Cuff Mandatory

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2828
Vital SignsVital Signs ((ContinuedContinued))
• TEMPERATURETEMPERATURE– Protective MechanismProtective Mechanism
• Environmental (Environmental (Heat and ColdHeat and Cold) Regulator) Regulator• Microbial ProtectionMicrobial Protection
– AssessmentAssessment• Rectally Rectally ((Most AccurateMost Accurate)): Normal = 36: Normal = 36ºº C (96.8 C (96.8 ºº F) F)• Axillary or Tympanic: Normal = 36.5Axillary or Tympanic: Normal = 36.5ºº C (97.6 C (97.6 ºº F) F)• Orally: Normal = 37Orally: Normal = 37ºº C (98.6 C (98.6 ºº F) F)
– Fever: Most common cause of seizure in infantsFever: Most common cause of seizure in infants

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 2929
Vital SignsVital Signs ((ContinuedContinued))
• PULSE OXIMETRYPULSE OXIMETRY– PlacementPlacement
• Proximal to Central CirculationProximal to Central Circulation• Earlobe = Recommended SiteEarlobe = Recommended Site
– Administer OAdminister O22 if SAOif SAO22 << 95% 95%– CO binds with Hemoglobin 200 times faster than CO binds with Hemoglobin 200 times faster than
OO22
• Pulse Ox of NO VALUE in such casePulse Ox of NO VALUE in such case

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 3030
Airway: Pediatric vs AdultAirway: Pediatric vs Adult
OBJECTIVE 6-1.3 COBJECTIVE 6-1.3 C• Airway DifferencesAirway Differences
– PediatricPediatric• HeadHead
– Prominent OcciputProminent Occiput
• TongueTongue– LargerLarger
– More AnteriorMore Anterior
• EpiglottisEpiglottis– ““U” ShapedU” Shaped
– FloppierFloppier
– Protrudes more in LaryngopharynxProtrudes more in Laryngopharynx

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 3131
Airway Airway ((ContinuedContinued))
– Pediatric Pediatric ((ContinuedContinued))
• TracheaTrachea– ShorterShorter
» Infant: 4-5 cmInfant: 4-5 cm» Child: 8 cmChild: 8 cm
– More FlexibleMore Flexible– Rings Less Well DevelopedRings Less Well Developed
• Smallest Airway Diameter = Cricoid RingSmallest Airway Diameter = Cricoid Ring• LarynxLarynx
– More AnteriorMore Anterior– More CephaladMore Cephalad– Cords Shorter and ConcaveCords Shorter and Concave
• Lungs: Lungs: (Tidal Volume Dependent on Diaphragmatic Movement)(Tidal Volume Dependent on Diaphragmatic Movement)
– Adult Opposite that MentionedAdult Opposite that Mentioned

20032003 Oklahoma EMSC Resource CenterOklahoma EMSC Resource Center 3232
Summary: Section 1Summary: Section 1
• EMSC: Defined and IntegratedEMSC: Defined and Integrated• Pediatric Injury Prevention MethodologyPediatric Injury Prevention Methodology• Pediatric A&P vs AdultPediatric A&P vs Adult• Approach to Obtaining Medical HistoryApproach to Obtaining Medical History• Assessing and Interpreting Vital SignsAssessing and Interpreting Vital Signs• Pediatric vs Adult AirwayPediatric vs Adult Airway