-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
1/12
review article
T he n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082254
Mechanisms of Disease
Pulmonary Complications of Sickle CellDisease
Mark T. Gladwin, M.D., and Elliott Vichinsky, M.D.
From the Division of Pulmonary, Allergy,and Critical Care
Medicine and the Hemo-stasis and Vascular Biology Research
In-stitute, University of Pittsburgh, Pitts-burgh, (M.T.G.); and
Childrens Hospitaland Research Center at Oakland, Oakland,CA
(E.V.). Address reprint requests to Dr.
Gladwin at the Division of Pulmonary,Allergy, and Critical Care
Medicine, Uni-versity of Pittsburgh, NW 168 MontefioreHospital, 354
Fifth Ave., Pittsburgh, PA,15213, or at [email protected].
N Engl J Med 2008;359:2254-65.Copyright 2008 Massachusetts
Medical Society.
The inheritance of two copies of a mutant -globin gene, one
from each parent, is the underlying cause of sickle cell
disease. The muta-tion, GAGGTG, substitutes valine for glutamic
acid at position 6 in the
-globin chain of hemoglobin A, resulting in a hemoglobin called
hemoglobin S.1-3Sickle cell disease is one of the most common
autosomal recessive disorders in theworld. Approximately 8% of
black Americans are heterozygous and have the sickle
cell trait, whereas approximately 1 in 600 is homozygous and has
sickle cell dis-ease. In certain areas of sub-Saharan Africa, an
estimated 40 to 60% of the popu-lation is heterozygous, suggesting
that 1 to 4% of babies born in this region havethe disease.4
Hemoglobin S polymerizes on deoxygenation. The polymers make the
erythro-cyte rigid, distort its shape, and cause structural damage
in the red-cell membrane,all of which alter the rheologic
properties of the cell, impair blood flow through
themicrovasculature, and lead to hemolysis and vaso-occlusive
episodes.2,5The extentof hemoglobin S polymerization is a primary
determinant of the severity of sicklecell disease6and is
proportional to the degree and duration of hemoglobin
deoxy-genation and to the concentration of intracellular hemoglobin
S raised to approxi-mately the 15th power.2The presence of fetal
hemoglobin in the erythrocyte re-duces the concentration of
hemoglobin S and thereby inhibits its polymerization.7
The complications of sickle cell disease are myriad, but the two
most commonacute events are vaso-occlusive pain crisis, caused by
physical and adhesive entrap-ment of red cells containing
hemoglobin S in the microcirculation, and the acutechest syndrome,
a lung injury syndrome.8,9In addition, affected adults are at
riskfor a progressive vasculopathy, characterized by systemic and
pulmonary hyperten-sion, endothelial dysfunction, and proliferative
changes in the intima and smoothmuscle of blood vessels.10-16With
increasing age, chronic end-organ complicationsbegin to appear.
These include chronic renal failure, hemorrhagic and
nonhemor-rhagic stroke, avascular necrosis of bone, and pulmonary
hypertension, which hasa remarkably high prevalence among adults
with sickle cell disease.12,17From a
clinical perspective, pulmonary complications namely, the acute
chest syndromeand pulmonary hypertension are the most common causes
of death in patientswith sickle cell disease.8,9,12,18
Advances in our understanding of the mechanism of vaso-occlusion
and thesequelae of chronic intravascular hemolysis have led to
insights into the highlyvariable clinical manifestations of sickle
cell disease. We present a new formulationof sickle cell disease
and propose that certain of its complications are driven bythe
vaso-occlusive process, whereas others result from the deleterious
effects ofintravascular hemolysis on endothelial-cell and vascular
function.
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
2/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2255
Phenotypes of Sickle Cell
Disease
All patients with sickle cell disease have the sameGAGGTG
substitution, but the penetrance andseverity of specific
complications arising from themutant hemoglobin S gene, as well as
the risk
factors for these complications and the age atwhich they occur,
are highly variable. For exam-ple, the major laboratory risk
factors for bothvaso-occlusive pain crisis and the acute chest
syn-drome are high, steady-state leukocyte counts andhigh
hemoglobin levels.1,8,9In contrast, chole-lithiasis, cutaneous leg
ulceration, priapism, andpulmonary hypertension are associated with
lowsteady-state hemoglobin levels and an increasedrate of
intravascular hemolysis.12,17,19-23These lat-ter complications also
occur in other hemolyticdiseases. For example, pulmonary
hypertension
is common in thalassemia even though the acutechest syndrome
does not occur in that disorder,which is not caused by hemoglobin
S.24-28Pria-pism and cutaneous leg ulceration also occur inother
hemolytic disorders, although to a lesser ex-tent than in sickle
cell disease.21,29-34
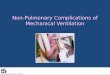
Given the divergent clinical manifestations ofand epidemiologic
risk factors for vaso-occlusivepain crisis and the acute chest
syndrome (as com-pared with other vasculopathic complications,such
as sudden death, pulmonary hypertension,cutaneous leg ulceration,
and priapism), sicklecell disease may be best understood as the
inter-action of two overlapping subphenotypes drivenby two major
mechanisms: vaso-occlusion andhemolytic anemia (Fig. 1).
Vaso-occlusion
Vaso-occlusive crises are recurrent episodes ofsevere pain in
sickle cell disease. The cause ofthese events is microvascular
entrapment of eryth-rocytes and leukocytes, which obstruct blood
flow
and bring about organ ischemia. In the microcir-culation of
transgenic mouse models of sicklecell disease, hypoxia or
inflammatory agents,such as tumor necrosis factor or
lipopolysac-charide, increase adhesive interactions
betweenendothelium, leukocytes, and erythrocytes in
thepostcapillary venules, thereby initiating
vascularocclusion.35-39This model indicates that cycles ofischemia
and reperfusion, in addition to intra-
vascular hemolysis, cause oxidant stress, in whichthere is
activation of vascular oxidases,40-42andinflammatory stress, which
is characterized by theexpression of endothelial-cell adhesion
moleculesand inflammatory cytokines and by
leukocyto-sis.35,37,43-45Precapillary obstruction by rigid,
de-formed erythrocytes with a high content of hemo-
globin S polymer probably also contributes toocclusion of the
microcirculation (Fig. 1).46
Bone marrow and periosteal ischemia andreperfusion instigate
cellular injury, infarction,tissue necrosis, edema, and
inflammation. Theclinical manifestations of these
microvascularevents are explosive episodes of pain and inf
lam-mation, often accompanied by fever and leuko-cytosis and
sometimes by bone marrow necrosis,with pulmonary emboli consisting
of necroticmarrow fat and cellular elements.1,8,9Epidemio-logic
studies of the frequency and severity of vaso-
occlusive crises indicate an association with highconcentrations
of hemoglobin S, low concentra-tions of fetal hemoglobin, and high
steady-stateleukocyte counts and hemoglobin
levels.8Theseepidemiologic data point to polymerized hemo-globin S,
inflammation, and hyperviscosity as ma-jor determinants of the
severity of erythrocytevaso-occlusion.
The Acute Chest Syndrome
The acute chest syndrome is a common form oflung injury in
sickle cell disease. When severe, thissyndrome is analogous to the
acute respiratorydistress syndrome. In a patient with sickle cell
dis-ease it is generally defined by the development ofa new
pulmonary infiltrate that is consistent withalveolar consolidation
but not atelectasis, involv-ing at least one complete lung segment.
The radio-graphic abnormality is usually accompanied bychest pain,
fever, tachypnea, wheezing, or cough.9The acute chest syndrome is
the second most com-mon cause of hospitalization among patients
with
sickle cell disease and the leading cause of ad-mission to an
intensive care unit and prematuredeath in this patient
population.8
Causes of the Acute Chest Syndrome
Three major causes of the acute chest syndromehave been
proposed: pulmonary infection, em-bolization of bone marrow fat,
and intravascu-lar pulmonary sequestration of sickled eryth-
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
3/12
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082256
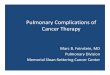
rocytes, resulting in lung injury and infarction(Fig. 2).
Pulmonary Infection
The most common cause of the acute chest syn-drome in children
and adults is pulmonary infec-tion by a community-acquired
pathogen, whichincites an excessive inflammatory response towhat
often should have been a mild upper respi-ratory infection. Studies
have shown that trans-genic mice that express human hemoglobin S
aresusceptible to inf lammatory triggers such as lipo-
polysaccharide and episodic exposure to environ-mental hypoxia,
with the development of lung
injury at doses of endotoxin or degrees of hypoxiathat do not
adversely affect wild-type mice.47,48
The National Acute Chest Syndrome StudyGroup analyzed 671
episodes of the acute chestsyndrome in 538 patients with sickle
cell diseaseto determine the cause, outcome, and responseto
therapy.9Respiratory airway sputum and bron-choalveolar-lavage
specimens were analyzed forviral and bacterial infect ions, and an
infectiousagent was identified in 54% of patients who
Hemolysis, endothelial dysfunction
Precapillary arteriole
Smooth-musclecells
Postcapillary venule
Capillary
Erythrocyte
Monocyte
PlateletsVCAM-1
41
Endothelialcells
Hb
Viscosity, vaso-occlusion
NOS
Arg
ET-1
NO O2-
XO
NOx
x
Pulmonary hypertensionLeg ulcerationPriapismStroke
Pain crisisAcute chest syndrome
Osteonecrosis
Decreased NObioactivity
Increasedvaso-occlusion
Figure 1.Hypothetical Mechanisms of Clinical Subphenotypes of
Sickle Cell Disease.
It is hypothesized that many of the complications of sickle cell
disease can be divided into two overlapping subtypes, each driven
by dis-
tinct mechanisms. Cutaneous leg ulceration, priapism, pulmonary
hypertension, sudden death, and stroke are associated with low
steady-
state hemoglobin (Hb) levels and an increased rate of
intravascular hemolysis, shown on the left side of the figure.
These vasculopathiccomplications probably result from endothelial
dysfunction, mediated by both inactivation of nitric oxide (NO) by
free-plasma hemoglo-bin and vascular reactive oxygen species as
well as arginine (Arg) catabolism by plasma arginase. This process
of hemolysis-associated
endothelial dysfunction may also cause hemostatic activation and
intimal and smooth-muscle proliferation. Such clinical
complications
as vaso-occlusive pain crisis, the acute chest syndrome,
avascular necrosis of bones, and retinal vasculopathy are
associated with highsteady-state leukocyte counts and high
hemoglobin levels. These complications are likely to result from
obstruction of capillaries and
postcapillary venules by erythrocytes containing polymerized
hemoglobin S and by leukocytes (a monocyte is shown), as shown on
theright side of the figure. ET-1 denotes endothelin 1, NOS nitric
oxide synthase, O2
superoxide, VCAM-1 vascular-cell adhesion molecule 1,
and XO xanthine oxidase.
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
4/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2257
were admitted to a hospital. Most of the agentswere atypical
bacteria and viruses. Community-acquired encapsulated bacteria were
isolated inless than 10% of cases, even though normalsplenic
phagocytic function is rare in sickle celldisease.
Fat Emboli
The second major cause of the acute chest syn-drome is the fat
emboli syndrome. It is associated
with a severe vaso-occlusive pain crisis involvingmultiple
bones, especially the pelvis and femur,which results in infarction
and edema of thebone marrow. The bone marrow undergoes ne-crosis,
and its contents, including fat, cells, andeven bony spicules, are
released into the blood-stream and travel to the lung, where they
causeacute pulmonary hypertension, severe lung in-f lammation, and
hypoxemia.49-51Secretory phos-pholipase A2is thought to convert
bone marrow
il ll
Increased polymerizationand erthyrocyte rigidity
Increased endothelialVCAM-1 expression
and adhesion
Increased erythrocyteadhesion in lung causing
pulmonary infarction
Acute chest syndrome
Vaso-occlusive crisis
Secretoryphospholipase
Pulmonaryinfection
Hypoventilaton and
atelectasis resulting fromrib and vertebral infarction
Fat
Microvasculature occlusion
and bone marrow infarction
Erythrocyte
NO
Shunt
Desaturatedhemoglobin
Decreasedoxygen delivery
Regionalhypoxia
NO
41
VCAM-1
Figure 2.The Vicious Cycle of the Acute Chest Syndrome.
The acute chest syndrome is a lung injury syndrome initiated by
three major triggers, all related to vaso-occlusion
by sickle cells: infection, embolization of bone marrow fat, and
intravascular sequestration of red cells, all of whichcause lung
injury and infarction. Lung injury results in ventilationperfusion
mismatch and hypoxemia, which leads
to increased deoxygenation of hemoglobin S, followed by
hemoglobin polymerization and erythrocyte vaso-occlu-sion, which in
turn promote bone marrow infarction and pulmonary vaso-occlusion.
NO denotes nitric oxide, and
VCAM-1 vascular-cell adhesion molecule.
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
5/12
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082258
phospholipids to free fatty acids, which initiatean inflammatory
response and lung injury in aprocess analogous to that triggered by
intravenousadministration of oleic acid in mouse models ofthe acute
respiratory distress syndrome.52
Oil red O staining of lipid accumulationswithin alveolar
macrophages is diagnostic of the
fat emboli syndrome, and the lipid accumula-tions can be
identified in more than 16% of casesof the acute chest syndrome in
adults and chil-dren.9A study compared induced sputum sam-ples of
alveolar macrophages with samples ob-tained using bronchoalveolar
lavage and found amodest but significant correlation between thetwo
methods (r = 0.65).53 In this study, patientswith lipid-laden
macrophages in induced sputumsamples had significantly greater
extrathoracicpain, more neurologic symptoms, lower plateletcounts,
and higher aminotransferase levels than
patients without evidence of fat emboli. The acutechest syndrome
can be part of the spectrum ofdisorders in the systemic fat emboli
syndrome.This latter syndrome should be suspected in pa-tients with
abrupt multiorgan failure, rapid de-velopment of the acute
respiratory distress syn-drome, acute increases in pulmonary
arterialpressures, evidence of hepatic injury, alterationsin mental
status, seizures, prominent thrombo-cytopenia, and in rare cases,
coagulopathy.54,55
Pulmonary Infarction
Pulmonary infarction, or vaso-occlusion, may alsocontribute to
the development of the acute chestsyndrome. In a small number of
patients, wedge-shaped lung infarction, sometimes followed
bycentral cavitation, develops.9,56
Clinical Aspects of the Acute Chest Syndrome
In most adults with sickle cell anemia, the acutechest syndrome
develops 24 to 72 hours after theonset of severe pain in the arms,
legs, or chest.The acute chest syndrome is associated with
marked systemic inflammation, with a mean peaktemperature of
38.9C and a mean white-cellcount of 23,000 per cubic
millimeter.9Althougha high steady-state hemoglobin level (without
paincrisis) is a major risk factor for the acute chestsyndrome, in
hospitalized patients with vaso-occlusive pain crisis, an abrupt
drop in the hemo-globin level (a mean decrease of 0.78 g per
deci-liter from steady-state levels) and an increase in
markers of hemolysis often precede the develop-ment of the acute
chest syndrome. The plateletcount also falls before the onset of
the acutechest syndrome; a platelet level of 200,000 percubic
millimeter or less is an independent riskfactor for severe
manifestations of the syndromeand is associated with increased
risks of neuro-
logic complications and the need for mechanicalventilation.
The mean length of hospitalization for adultswith the acute
chest syndrome is 10.5 days, ascompared with only 3 to 4 days for
uncomplicat-ed vaso-occlusive pain crisis. Mechanical ventila-tion
is required in 13% of patients with the syn-drome, and 3% die. The
outcome for patients onmechanical ventilation is actually quite
good, witha mortality rate of only 19%, as compared withthe outcome
for all patients with the acute chestsyndrome, for whom the
mortality rate is approx-
imately 30%.9Rapid simple or exchange transfu-sion, ideally with
antigen-matched blood, removesthe trigger for acute lung injury
sickled erythro-cytes allowing rapid recovery in young
pa-tients.
Sickle cell disease is often accompanied byasthma. Reactive
airway disease occurs in 13% ormore of patients with the acute
chest syndromeand in up to 53% of children between birth andthe age
of 9 years.9,57 Although a number ofstudies suggest that asthma is
a risk factor forthe acute chest syndrome and stroke in
patientswith sickle cell disease,58-60it remains uncertainwhether
there is an increase in the prevalence ofasthma among children with
sickle cell diseasein the steady state, as compared with
matchedcontrols.59,61During steady-state sickle cell dis-ease, the
major abnormality in pulmonary func-tion is a restrictive
ventilatory impairment, char-acterized by a mild reduction in total
lungcapacity, and reduced diffusion capacity for car-bon
monoxide.62,63These abnormalities worsenwith age and are associated
with increases in
pulmonary-artery pressures.63,64
Hemolysis, Endothelial-Cell
Dysfunction, a nd Vasculopathy
Catabolism of Hemoglobin
A complex biochemical and cellular system clearsand detoxifies
the hemoglobin that red cells re-lease into the plasma during
normal oxidative and
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
6/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2259
mechanical stress.65The hemoglobin dimer bindswith an unusually
high proteinprotein aff inityto haptoglobin.66The resulting complex
exposes aneoepitope recognized by the hemoglobin scaven-ger protein
CD163, a transmembrane glycopro-tein that initiates the uptake of
hemoglobin intomacrophages and monocytes. The uptake of he-
moglobin by these cells activates interleukin-10and induces
expression of heme oxygenase-1 andbiliverdin reductase.67-69These
enzymes catabo-lize heme and signal potent antiproliferative,
anti-oxidant, and antiinflammatory reactions.68-70Thedownstream
activities of these molecules takeplace in response to the
oxidative and inflamma-tory effects of free heme, iron, and oxygen:
thebinding of haptoglobin to hemoglobin limitsheme-mediated lipid
peroxidation,71biliverdin re-ductase catalytically generates NADPH
and reduc-es glutathione,69and heme oxygenase-1 generates
carbon monoxide and biliverdin, both of whichlimit proliferative
and thrombotic vascular inju-ry.68New therapeutic approaches, such
as hapto-globin infusions, inhaled carbon monoxide gasand carbon
monoxidereleasing compounds, andgenetic or pharmacologic induction
of heme oxy-genase are being studied in animal models for
thetreatment of vascular injury in sickle cell disease.72
Hemolysis
Effect on Nitric Oxide
In sickle cell disease, the hemoglobin and hemescavenging
systems are saturated and over-whelmed, even in the steady
state.73,74Free plasmahemoglobin, in addition to generating
reactiveoxygen species, such as the hydroxyl and super-oxide
radicals (through the Fenton and peroxidaseand auto-oxidation
chemical reactions),75,76is alsoa potent scavenger of nitric
oxide.74,77Nitric oxide,which is normally produced by the
endothelium,regulates basal vasodilator tone; inhibits plateletand
hemostatic activation; inhibits transcriptionalexpression of
nuclear factor Bdependent adhe-
sion molecules, such as vascular-cell adhesionmolecule 1,
intercellular adhesion molecule 1,and the selectins; and reduces
superoxide levelsthrough radicalradical scavenging.78-82The
half-life of nitric oxide in the blood is extremely shortbecause of
its rapid reaction with hemoglobin toform methemoglobin and
nitrate.83Actually, thevasodilator activity of nitric oxide is
possible onlybecause most hemoglobin is normally compart-
mentalized within erythrocytes. Flowing bloodproduces a
cell-free zone along the endotheli-um; this zone and an area of
nonflowing bloodaround the outside of the erythrocyte (called
theunstirred layer) constitute major diffusion barriersagainst
nitric oxide entry into red cells.84-86Thesebarriers reduce the
rate at which nitric oxide reacts
with intracellular hemoglobin by two to threeorders of
magnitude. The release of hemoglobininto plasma during hemolysis
circumvents thesediffusion barriers and serves as a potent
inhibi-tor of all nitric oxide bioactivity, leading to aclinical
state of endothelial-cell dysfunction andnitric oxide
resistance.14,74,77,87-92
Effect on Arginine
Hemolysis also releases erythrocyte arginase 1 intoplasma.
Arginase metabolizes plasma arginineinto ornithine, reducing the
required substrate for
nitric oxide synthesis and compounding the re-duction in the
bioavailability of nitric oxide insickle cell disease (Fig. 1).93
In one study, theplasma levels and enzymatic activity of arginase1
were significantly increased in 228 patients withsickle cell
disease as compared with black controlsubjects; moreover, arginase
1 modulated themetabolic profile of arginine by reducing argi-nine
levels and increasing the production of orni-thine relative to that
of citrulline.93These abnor-malities were associated with severe
pulmonaryhypertension and an increased risk of death.
Intra-vascular hemolysis has also been shown to beassociated with
reduced availability of nitric oxideand arginine in animal models
and in humanswith severe falciparum malaria.94,95In the studyof
malaria, impairment of nitric oxidedependent,flow-mediated
vasodilatation developed and wasassociated with hemolysis and high
levels of ar-ginase and lactate dehydrogenase.95
The Hypercoagulable State
Chronic depletion of nitric oxide and arginine
may also contribute to the hypercoagulable statein hemolytic
diseases. Since nitric oxide is a po-tent inhibitor of platelet
activation, the depletionof nitric oxide and arginine (the
substrate for ni-tric oxide synthesis) in sickle cell disease
allowsfor platelet activation.96Arginine consumption iscompounded
by increased intracellular plateletexpression of arginase.97
Recent studies of sickle cell disease showed
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
7/12
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082260
correlations between the intrinsic rate of hemo-lysis and the
levels of procoagulant factors inblood.98-100 In addition to the
release of freehemoglobin, hemolysis is associated with the
for-mation of red-cell microvesicles containing
phos-phatidylserine, an activator of tissue factor.100,101Patients
with sickle cell disease who have func-
tional asplenia and patients with thalassemiawho have undergone
surgical splenectomy haveincreased levels of plasma hemoglobin and
red-cell microvesicles, which are potential mecha-nisms for the
hypercoagulability associated withboth diseases, with possible
exacerbation by asple-nia.100
Additional support for the idea that hemolysisimpairs nitric
oxide signaling comes from trans-genic mouse models of sickle cell
disease andspherocytosis and from mouse models of allo-immune
hemolysis and malaria.42,94,102In these
models, there is impaired vasodilatation in re-sponse to nitric
oxide donors and endothelial-dependent vasodilators, and pulmonary
hyperten-sion and right heart failure develop.42,102
Pulmonary Hypertension
in Sickle Cell Disease
A major risk factor for pulmonary hypertensionin sickle cell
disease is the severity of hemolyticanemia, which can be determined
by measuringsteady-state hemoglobin levels and levels of lac-tate
dehydrogenase, indirect bilirubin, and
retic-ulocytes.12,19,23,103,104An association between
thedevelopment of pulmonary hypertension and theintensity of
hemolytic anemia has been observedin three prospective screening
studies of adultswith sickle cell disease12,103,104and in a
growingnumber of pediatric studies.105-108 Pulmonaryhypertension is
a reported complication of otherforms of chronic hereditary or
acquired hemo-lytic anemia, including thalassemia intermediaand
thalassemia major, paroxysmal nocturnal
hemoglobinuria, spherocytosis, stomatocytosis,pyruvate kinase
deficiency, alloimmune hemo-lytic anemia, glucose-6-phosphate
dehydrogenasedeficiency, unstable hemoglobin variants, and
themicroangiopathic hemolytic anemias.65,109 Al-though data from
cohort screening studies areavailable only for sickle cell disease
and thalas-semia, there are growing numbers of case reportsand case
series involving pulmonary hypertension
in other chronic hereditary and acquired hemo-lytic anemias.
Echocardiography
Three prospective screening studies using echo-cardiography have
shown that 20% of adults withsickle cell disease have borderline or
mild pul-
monary hypertension, defined by a pulmonaryartery systolic
pressure greater than 35 mm Hg;10% of these adults have moderate to
severe pul-monary hypertension, defined by a pressure great-er than
45 mm Hg.12,103,104Despite pulmonaryartery systolic pressures that
are much lower thanthose in idiopathic or hereditary pulmonary
hyper-tension, in sickle cell disease borderline or mildpulmonary
hypertension is associated with anextremely high risk of
death.12,103,104,110-112It re-mains to be determined whether
elevations inpulmonary pressures are a marker for vasculopa-
thy and a risk factor for cardiovascular death orwhether the
elevations contribute directly to deathdue to progressive or acute
right heart failure.The implications of borderline elevations in
pul-monary artery systolic pressure in the pediatricpopulation
remain unknown.
Adults with sickle cell disease should bescreened for pulmonary
hypertension with trans-thoracic Doppler echocardiography.12 The
thinbody habitus of these adults, along with dilatedand
hyperdynamic heart chambers, allows easydetection of the
regurgitation of blood backwardacross the tricuspid valve during
right ventricu-lar systole (Fig. 3). The tricuspid regurgitant
jetvelocity is used to estimate the right ventricularand
pulmonary-artery systolic pressures (whichare approximately four
times the tricuspid regur-gitant jet velocity squared) after the
addition ofan estimate of the central venous pressure. Insickle
cell disease, these estimated pulmonarysystolic pressures correlate
well with measure-ments obtained by means of right heart
catheter-ization.12A value of 2.5 m per second or more
corresponds to an estimated pulmonary-arterysystolic pressure of
35 mm Hg, which is approxi-mately 2 SD above the normal mean value;
forpatients less than 40 years of age, the referencevalue for the
mean pulmonary-artery systolicpressure, estimated with the use of
Doppler echo-cardiography, is 27.514.2 mm Hg (95% confi-dence
interval [CI], 19.3 to 35.5).113Although amore traditional
definition of pulmonary hyper-
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
8/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2261
tension would be a tricuspid regurgitant jet veloc-
ity of 3.0 m per second or more, values between2.5 and 2.9 m per
second are associated with anincreased risk of death among patients
withsickle cell disease.12,103,104A follow-up analysisof the
National Institutes of Health (NIH) pulmo-nary-hypertension
screening cohort12showed thatwith a tricuspid regurgitant jet
velocity of 2.5 to2.9 m per second, as compared with a velocity
ofless than 2.5 m per second, the rate ratio for death
was 4.4 (95% CI, 1.6 to 12.2; P
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
9/12
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082262
pulmonary hypertension.64,110The mean pulmo-nary-artery pressure
in patients with sickle celldisease and pulmonary-artery
hypertension is ap-proximately 40 mm Hg, and pulmonary
vascularresistance is approximately 250 dyn sec cm5.The relatively
low pulmonary vascular resistanceis caused by the high cardiac
output that is char-
acteristic of anemia. Approximately 60% of cath-eterized
patients with a tricuspid regurgitant jetvelocity that is 3.0 m per
second or more meetthe definition of pulmonary-artery
hypertension,indicating that vasculopathy primarily involves
thepulmonary arterial system. In the other 40% ofpatients, the left
ventricular end diastolic pres-sures are greater than 15 mm Hg,
indicating acomponent of left ventricular diastolic
dysfunc-tion.64Patients with both pulmonary vascular dis-ease and
echocardiographic evidence of diastolicdysfunction are at
particularly high risk for death
(relative risk ratio, 12.0; 95% CI, 3.8 to 38.1;P
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
10/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2263
are the leading complications associated withdeath in adults
with sickle cell disease. In patientswho die of the acute chest
syndrome, abrupt in-creases in pulmonary pressures and right
heartfailure are common, indicating a major interac-tion between
these clinical entities. The currenttreatment of these
complications is based on lim-
ited evidence or expert opinion, highlighting thecritical need
for randomized clinical trials in thisarea. Identification,
prevention, and expert man-
agement of these complications by hematologistsand
pulmonologists will be a challenge as thepopulation of patients
with sickle cell diseaseages and increases worldwide.
Dr. Gladwin reports receiving grant support from the
U.S.government and INO Therapeutics in the form of a
CollaborativeResearch and Development Agreement, from the
Intramural
Research Division of the National Heart, Lung, and Blood
Insti-tute, and from the Institute for Transfusion Medicine and
theHemophilia Center of Western Pennsylvania. No other
potentialconflict of interest was reported.
References
Platt OS. The acute chest syndrome of1.sickle cell disease. N
Engl J Med 2000;342:1904-7. [Erratum, N Engl J Med
2000;343:591.]
Bunn HF. Pathogenesis and treatment2.of sickle cell disease. N
Engl J Med 1997;337:762-9.
Steinberg MH. Management of sickle3.cell disease. N Engl J Med
1999;340:1021-
30.Aliyu ZY, Gordeuk V, Sachdev V, et al.4.
Prevalence and risk factors for pulmonaryartery systolic
hypertension among sicklecell disease patients in Nigeria. Am J
He-matol 2008;83:485-90.
Noguchi CT, Schechter AN, Rodgers5.GP. Sickle cell disease
pathophysiology.Baillieres Clin Haematol 1993;6:57-91.
Brittenham GM, Schechter AN, Nogu-6.chi CT. Hemoglobin S
polymerization:primary determinant of the hemolytic andclinical
severit y of the sickling syndromes.Blood 1985;65:183-9.
Noguchi CT, Rodgers GP, Serjeant G,7.Schechter AN. Levels of
fetal hemoglobinnecessary for treatment of sickle cell dis-ease. N
Engl J Med 1988;318:96-9.
Platt OS, Brambilla DJ, Rosse WF, et al.8.Mortality in sickle
cell disease: life ex-pectancy and risk factors for early death.N
Engl J Med 1994;330:1639-44.
Vichinsky EP, Neumayr LD, Earles AN,9.et al. Causes and outcomes
of the acutechest syndrome in sickle cell disease.N Engl J Med
2000;342:1855-65. [Erratum,N Engl J Med 2000;343:824.]
Pegelow CH, Colangelo L, Steinberg M,10.et al. Natural history
of blood pressure insickle cell disease: risks for stroke anddeath
associated with relative hyperten-
sion in sickle cell anemia. Am J Med
1997;102:171-7.Ohene-Frempong K, Weiner SJ, Sleeper11.
LA, et al. Cerebrovascular accidents insickle cell disease:
rates and risk factors.Blood 1998;91:288-94.
Gladwin MT, Sachdev V, Jison ML, et12.al. Pulmonary hypertension
as a risk fac-tor for death in patients with sickle celldisease. N
Engl J Med 2004;350:886-95.
Gladwin MT, Schechter AN, Ognibene13.FP, et al. Divergent nitric
oxide bioavail-
ability in men and women with sickle celldisease. Circulation
2003;107:271-8.
Eberhardt RT, McMahon L, Duffy SJ,14.et al. Sickle cell anemia
is associated withreduced nitric oxide bioactivity in periph-eral
conduit and resistance vessels. Am JHematol 2003;74:104-11.
Haque AK, Gokhale S, Rampy BA, Ad-15.egboyega P, Duarte A,
Saldana MJ. Pulmo-
nary hypertension in sickle cell hemoglo-binopathy: a
clinicopathologic study of 20cases. Hum Pathol 2002;33:1037-43.
Kato GJ, Hsieh M, Machado R, et al.16.Cerebrovascular disease
associated withsickle cell pulmonary hypertension. Am JHematol
2006;81:503-10.
Kato GJ, Gladwin MT, Steinberg MH.17.Deconstructing sickle cell
disease: reap-praisal of the role of hemolysis in the de-velopment
of clinical subphenotypes. BloodRev 2007;21:37-47.
Perronne V, Roberts-Harewood M,18.Bachir D, et al. Patterns of
mortality insickle cell disease in adults in France andEngland.
Hematol J 2002;3:56-60.
Kato GJ, McGowan V, Machado RF, et19.al. Lactate dehydrogenase
as a biomarkerof hemolysis-associated nitric oxide resis-tance,
priapism, leg ulceration, pulmonaryhypertension, and death in
patients withsickle cell disease. Blood 2006;107:2279-85.
Nolan VG, Adewoye A, Baldwin C, et20.al. Sickle cell leg ulcers:
associations withhaemolysis and SNPs in Klotho, TEK andgenes of the
TGF-beta/BMP pathway. Br JHaematol 2006;133:570-8.
Nolan VG, Baldwin C, Ma Q, et al.21.Associat ion of single
nucleotide polymor-phisms in klotho with priapism in sickle
cell anaemia. Br J Haematol 2005;128:266-72.Nolan VG, Wyszynski
DF, Farrer LA,22.
Steinberg MH. Hemolysis-associated pri-apism in sickle cell
disease. Blood 2005;106:3264-7.
Kato GJ, Onyekwere OC, Gladwin MT.23.Pulmonary hypertension in
sickle cell dis-ease: relevance to children. Pediatr Hema-tol Oncol
2007;24:159-70.
Aessopos A, Farmakis D, Karagiorga24.M, et al. Cardiac
involvement in thalas-
semia intermedia: a multicenter study.Blood 2001;97:3411-6.
Du ZD, Roguin N, Milgram E, Saab K,25.Koren A. Pulmonary
hypertension in pa-tients with thalassemia major. Am HeartJ
1997;134:532-7.
Aessopos A, Stamatelos G, Skoumas V,26.Vassilopoulos G,
Mantzourani M, Louko-poulos D. Pulmonary hypertension and
right heart failure in patients with beta-thalassemia
intermedia. Chest 1995;107:50-3.
Derchi G, Fonti A, Forni GL, et al. Pul-27.monary hypertension
in patients withthalassemia major. Am Heart J 1999;138:384.
Morris CR, Kuypers FA, Kato GJ, et al.28.Hemolysis-associated
pulmonary hyper-tension in thalassemia. Ann N Y Acad
Sci2005;1054:481-5.
Burnett AL, Bivalacqua TJ. Glucose-6-29.phosphate dehydrogenase
def iciency: anetiology for idiopathic priapism? J Sex
Med2008;5:237-40.
Prabhakaran K, Jacobs BL, Smaldone30.MC, Franks ME. Stuttering
priapism asso-ciated with hereditary spherocytosis. CanJ Urol
2007;14:3702-4.
Thuret I, Bardakdjian J, Badens C, et al.31.Priapism following
splenectomy in an un-stable hemoglobin: hemoglobin Olmstedbeta 141
(H19) LeuArg. Am J Hematol1996;51:133-6.
Mohamed N, Jackson N. Severe thalas-32.saemia intermedia:
clinical problems inthe absence of hypertransfusion. BloodRev
1998;12:163-70.
Taher A, Ismaeel H, Cappellini MD.33.Thalassemia intermedia:
revisited. BloodCells Mol Dis 2006;37:12-20.
Vanscheidt W, Leder O, Vanscheidt E,34.et al. Leg ulcers in a
patient with sphero-cytosis: a clinicopathological report.
Der-matologica 1990;181:56-9.
Frenette PS. Sickle cell vaso-occlusion:35.multistep and
multicellular paradigm. CurrOpin Hematol 2002;9:101-6.
Turhan A, Weiss LA, Mohandas N,36.Coller BS, Frenette PS.
Primary role foradherent leukocytes in sickle cell
vascularocclusion: a new paradigm. Proc Natl AcadSci U S A
2002;99:3047-51.
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
11/12
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 359;21 www.nejm.org november 20, 20082264
Belcher JD, Bryant CJ, Nguyen J, et a l.37.Transgenic sickle
mice have vascular in-flammation. Blood 2003;101:3953-9.
Belcher JD, Marker PH, Weber JP, Heb-38.bel RP, Vercellotti GM.
Activated mono-cytes in sickle cell disease: potential rolein the
activation of vascular endotheliumand vaso-occlusion. Blood
2000;96:2451-9.
Osarogiagbon UR, Choong S, Belcher39.
JD, Vercellott i GM, Paller MS, Hebbel RP.Reperfusion injury
pathophysiology insickle transgenic mice. Blood 2000;96:314-20.
Aslan M, Ryan TM, Adler B, et al.40.Oxygen radical inhibition of
nitric oxide-dependent vascular function in sickle celldisease.
Proc Natl Acad Sci U S A 2001;98:15215-20.
Wood KC, Hebbel RP, Granger DN.41.Endothelial cell NADPH oxidase
mediatesthe cerebral microvascular dysfunction insickle cell
transgenic mice. FASEB J 2005;19:989-91.
Hsu LL, Champion HC, Campbell-Lee42.SA, et al. Hemolysis in
sickle cell mice
causes pulmonary hypertension due toglobal impairment in nitric
oxide bioavail-ability. Blood 2007;109:3088-98. [Erratum,Blood
2008;111:1772.]
Kaul DK, Hebbel RP. Hypoxia/reoxy-43.genation causes
inflammatory responsein transgenic sickle mice but not in nor-mal
mice. J Clin Invest 2000;106:411-20.[Erratum, J Clin Invest
2000;106:715.]
Belcher JD, Mahaseth H, Welch TE, et44.al. Critical role of
endothelial cell activa-tion in hypoxia-induced vasoocclusion
intransgenic sickle mice. Am J Physiol HeartCirc Physiol
2005;288:H2715-H2725.
Platt OS. Sickle cell anemia as an in-45.flammatory disease. J
Clin Invest 2000;106:
337-8.Hiruma H, Noguchi CT, Uyesaka N,46.
Schechter AN, Rodgers GP. Contributionsof sickle hemoglobin
polymer and sicklecell membranes to impaired filterability.Am J
Physiol 1995;268:H2003-H2008.
Holtzclaw JD, Jack D, Aguayo SM, Eck-47.man JR, Roman J, Hsu LL.
Enhanced pul-monary and systemic response to endo-toxin in
transgenic sickle mice. Am JRespir Crit Care Med
2004;169:687-95.
Sabaa N, de Franceschi L, Bonnin P, et48.al. Endothelin receptor
antagonism pre-vents hypoxia-induced mortality and mor-bidity in a
mouse model of sickle-celldisease. J Clin Invest
2008;118:1924-33.
Case Records of the Massachusetts49.General Hospital (Case
34-1997). N Engl JMed 1997;337:1293-301.
Case Records of the Massachusetts50.General Hospital (Case
52-1983). N Engl JMed 1983;309:1627-36.
Gladwin MT, Rodgers GP. Pathogene-51.sis and treatment of acute
chest syndromeof sickle-cell anaemia. Lancet 2000;355:1476-8.
Styles LA, Schalkwijk CG, Aarsman52.AJ, Vichinsky EP, Lubin BH,
Kuypers FA.Phospholipase A2 levels in acute chest
syndrome of sickle cell disease. Blood1996;87:2573-8.
Lechapt E, Habibi A, Bachir D, et al.53.Induced sputum versus
bronchoalveolarlavage during acute chest syndrome insickle cell
disease. Am J Respir Crit CareMed 2003;168:1373-7.
Vichinsky E, Williams R, Das M, et al.54.Pulmonary fat embolism:
a distinct cause
of severe acute chest syndrome in sicklecell anemia. Blood
1994;83:3107-12.Castro O. Systemic fat embolism and55.
pulmonary hypertension in sickle cell dis-ease. Hematol Oncol
Clin North Am 1996;10:1289-303.
Bellet PS, Kalinyak KA, Shukla R, Gel-56.fand MJ, Rucknagel DL.
Incentive spirom-etry to prevent acute pulmonary compli-cations in
sickle cell diseases. N Engl JMed 1995;333:699-703.
Bryant R. Asthma in the pediatric sick-57.le cell patient with
acute chest syndrome.J Pediatr Health Care 2005;19:157-62.
Boyd JH, Macklin EA, Strunk RC, De-58.Baun MR. Asthma is
associated with acute
chest syndrome and pain in children withsickle cell anemia.
Blood 2006;108:2923-7.
Knight-Madden JM, Forrester TS, Lewis59.NA, Greenough A. Asthma
in childrenwith sickle cell disease and its associationwith acute
chest syndrome. Thorax 2005;60:206-10.
Nordness ME, Lynn J, Zacharisen MC,60.Scott PJ, Kelly KJ. Asthma
is a risk factorfor acute chest syndrome and cerebralvascular
accidents in children with sicklecell disease. Clin Mol Allerg y
2005;3:2.
Sylvester KP, Patey RA, Broughton S,61.et al. Temporal
relationship of asthma toacute chest syndrome in sickle cell
disease.
Pediatr Pulmonol 2007;42:103-6.Field JJ, Glassberg J, Gilmore A,
et al.62.
Longitudinal analysis of pulmonary func-tion in adults with
sickle cell disease. AmJ Hematol 2008;83:574-6.
Klings ES, Wyszynski DF, Nolan VG,63.Steinberg MH. Abnormal
pulmonary func-tion in adults with sickle cell anemia. AmJ Respir
Crit Care Med 2006;173:1264-9.
Anthi A, Machado RF, Jison ML, et al.64.Hemodynamic and
functional assessmentof patients with sickle cell disease
andpulmonary hypertension. Am J Respir CritCare Med
2007;175:1272-9.
Rother RP, Bell L, Hil lmen P, Gladwin65.MT. The clinical
sequelae of intravascularhemolysis and extracellular plasma
hemo-globin: a novel mechanism of human dis-ease. JAMA
2005;293:1653-62.
Nagel RL, Gibson QH. The binding of66.hemoglobin to haptoglobin
and its rela-tion to subunit dissociation of hemoglo-bin. J Biol
Chem 1971;246:69-73.
Kristiansen M, Graversen JH, Jacob-67.sen C, et al.
Identification of the haemo-globin scavenger receptor. Nature
2001;409:198-201.
Ryter SW, Otterbein LE, Morse D, Choi68.AM. Heme
oxygenase/carbon monoxide
signaling pathways: regulation and func-tional significance. Mol
Cell Biochem2002;234-235:249-63.
Baranano DE, Rao M, Ferris CD, Sny-69.der SH. Biliverdin
reductase: a majorphysiologic cytoprotectant. Proc Natl AcadSci U S
A 2002;99:16093-8.
Otterbein LE, Bach FH, Alam J, et al.70.Carbon monoxide has
anti-inflammatory
effects involving the mitogen-activatedprotein kinase pathway.
Nat Med 2000;6:422-8.
Melamed-Frank M, Lache O, Enav BI,71.et al. Structure-function
analysis of theantioxidant properties of haptoglobin.Blood
2001;98:3693-8.
Belcher JD, Mahaseth H, Welch TE,72.Otterbein LE, Hebbel RP,
Vercellotti GM.Heme oxygenase-1 is a modulator of in-flammation and
vaso-occlusion in trans-genic sickle mice. J Clin Invest
2006;116:808-16.
Bensinger TA, Gillette PN. Hemolysis73.in sickle cell disease.
Arch Intern Med1974;133:624-31.
Reiter CD, Wang X, Tanus-Santos JE,74.et al. Cell-free
hemoglobin limits nitricoxide bioavailability in sickle-cell
disease.Nat Med 2002;8:1383-9.
Hebbel RP. Auto-oxidation and a mem-75.brane-associated Fenton
reagent: a possi-ble explanation for development of mem-brane
lesions in sickle erythrocytes. ClinHaematol 1985;14:129-40.
Repka T, Hebbel RP. Hydroxyl radical76.formation by sickle
erythrocyte mem-branes: role of pathologic iron depositsand
cytoplasmic reducing agents. Blood1991;78:2753-8.
Reiter CD, Gladwin MT. An emerging77.role for nitric oxide in
sickle cell disease
vascular homeostasis and therapy. CurrOpin Hematol
2003;10:99-107.
Furchgott RF, Zawadzki JV. The oblig-78.atory role of
endothelial cells in the relax-ation of arteria l smooth muscle by
acetyl-choline. Nature 1980;288:373-6.
Ignarro LJ, Buga GM, Wood KS, Byrns79.RE, Chaudhuri G.
Endothelium-derived re-laxing factor produced and released
fromartery and vein is nitric oxide. Proc NatlAcad Sci U S A
1987;84:9265-9.
Palmer RM, Ashton DS, Moncada S.80.Vascular endothelial cells
synthesize nitricoxide from L-arginine. Nature 1988;333:664-6.
Panza JA, Casino PR, Kilcoyne CM,81.Quyyumi AA. Role of
endothelium-derivednitric oxide in the abnormal
endothelium-dependent vascular relaxation of patientswith essential
hypertension. Circulation1993;87:1468-74.
De Caterina R, Libby P, Peng HB, et al.82.Nitric oxide decreases
cytokine-inducedendothelial activation: nitric oxide selec-tively
reduces endothelial expression ofadhesion molecules and
proinflammatorycytokines. J Clin Invest 1995;96:60-8.
Doherty DH, Doyle MP, Curry SR, et al.83.Rate of reaction with
nitric oxide deter-
Copyright 2008 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org at UNIVERSITY OF PITTSBURGH
on January 6, 2009 .
-
8/10/2019 2009 Pulmonary Complications of Sickle Cell
12/12
Mechanisms of Disease
n engl j med 359;21 www.nejm.org november 20, 2008 2265
mines the hypertensive effect of cell-freehemoglobin. Nat
Biotechnol 1998;16:672-6.
Butler AR, Megson IL, Wright PG.84.Diffusion of nitric oxide and
scavengingby blood in the vasculature. Biochim Bio-phys Acta
1998;1425:168-76.
Liu X, Mil ler MJ, Joshi MS, Sadowska-85.Krowicka H, Clark DA,
Lancaster JR Jr.
Diffusion-limited reaction of free nitricoxide with
erythrocytes. J Biol Chem 1998;273:18709-13.
Schechter AN, Gladwin MT. Hemo-86.globin and the paracrine and
endocrinefunctions of nitric oxide. N Engl J
Med2003;348:1483-5.
Yu B, Raher MJ, Volpato GP, Bloch87.KD, Ichinose F, Zapol WM.
Inhaled nitricoxide enables artificial blood transfusionwithout
hypertension. Circulation 2008;117:1982-90.
Minneci PC, Deans KJ, Zhi H, et al.88.Hemolysis-associated
endothelial dysfunc-tion mediated by accelerated NO inactiva-tion
by decompartmentalized oxyhemo-
globin. J Clin Invest 2005;115:3409-17.Gladwin MT.
Deconstructing endo-89.
thelial dysfunction: soluble guanylyl cy-clase oxidation and the
NO resistancesyndrome. J Clin Invest 2006;116:2330-2.
Nath KA, Shah V, Haggard JJ, et al.90.Mechanisms of vascular
instability in atransgenic mouse model of sickle cell dis-ease. Am
J Physiol Regul Integr CompPhysiol 2000;279:R1949-R1955.
Kaul DK, Liu XD, Chang HY, Nagel91.RL, Fabry ME. Effect of fetal
hemoglobinon microvascular regulation in sickle
trans-genic-knockout mice. J Clin Invest 2004;114:1136-45.
Kaul DK, Liu XD, Fabry ME, Nagel RL.92.
Impaired nitric oxide-mediated vasodila-tion in transgenic
sickle mouse. Am J Phy-siol Heart Circ Physiol
2000;278:H1799-H1806.
Morris CR, Kato GJ, Poljakovic M, et al.93.Dysregulated arginine
metabolism, hemo-lysis-associated pulmonary hypertension,and
mortality in sickle cell disease. JAMA2005;294:81-90.
Gramaglia I, Sobolewski P, Meays D,94.et al. Low nitric oxide
bioavailability con-tributes to the genesis of experimentalcerebral
malaria. Nat Med 2006;12:1417-22.
Yeo TW, Lampah DA, Gitawati R, et95.al. Impaired nitric oxide
bioavailability andL-arginine reversible endothelial dysfunc-tion
in adults with falciparum malaria.J Exp Med 2007;204:2693-704.
Villagra J, Shiva S, Hunter LA, Macha-96.do RF, Gladwin MT, Kato
GJ. Platelet ac-tivation in patients with sickle
disease,hemolysis-associated pulmonary hyperten-sion, and nitric
oxide scavenging by cell-free hemoglobin. Blood
2007;110:2166-72.
Raghavachari N, Xu X, Harris A, et al.97.Amplified expression
profiling of platelet
transcriptome reveals changes in argininemetabolic pathways in
patients with sick-le cell disease. Circu lation
2007;115:1551-62.
Ataga KI, Moore CG, Hillery CA, et al.98.Coagulation activation
and inf lammationin sickle cell disease-associated pulmo-nary hyper
tension. Haematologica 2008;93:20-6.
van Beers EJ, Spronk HM, Ten Cate H,99.et al. No association of
the hypercoagu-lable state with sickle cell disease
relatedpulmonary hypertension. Haematologica2008;93(5):e42-e44.
Westerman M, Pizzey A, Hirschman100.J, et al. Microvesicles in
haemoglobinopa-
thies offer insights into mechanisms ofhypercoagulability,
haemolysis and theeffects of therapy. Br J Haematol
2008;142:126-35.
Setty BN, Rao AK, Stuart MJ. Throm-101.bophilia in sickle cell
disease: the red cellconnection. Blood 2001;98:3228-33.
Frei AC, Guo Y, Jones DW, et al. Vas-102.cular dysfunction in a
murine model ofsevere hemolysis. Blood 2008;112:398-405.
De Castro LM, Jonassaint JC, Gra-103.ham FL, Ashley-Koch A,
Telen MJ. Pulmo-nary hypertension associated with sicklecell
disease: clinical and laboratory end-points and disease outcomes.
Am J Hema-
tol 2008;83:19-25.Ataga KI, Moore CG, Jones S, et al.104.
Pulmonary hypertension in patients withsickle cell disease: a
longitudinal study.Br J Haematol 2006;134:109-15.
Ambrusko SJ, Gunawardena S, Saka-105.ra A, et al. Elevation of
tricuspid regurgi-tant jet velocity, a marker for
pulmonaryhypertension in children with sickle celldisease. Pediatr
Blood Cancer 2006;47:907-13.
Liem RI, Young LT, Thompson AA.106.Tricuspid regurgitant jet
velocity is associ-ated with hemolysis in children and youngadults
with sickle cell disease evaluatedfor pulmonary hypertension.
Haemato-logica 2007;92:1549-52.
Pashankar FD, Carbonella J, Bazzy-107.Asaad A, Friedman A.
Prevalence and risk
factors of elevated pulmonary artery pres-sures in children with
sickle cell disease.Pediatrics 2008;121:777-82.
Onyekwere OC, Campbell A, Teshome108.M, et al. Pulmonary
hypertension in chil-dren and adolescents with sickle cell
dis-ease. Pediatr Cardiol 2008;29:309-12.
Machado RF, Gladwin MT. Chronic109.sickle cell lung disease: new
insights into
the diagnosis, pathogenesis and t reatmentof pulmonary
hypertension. Br J Haema-tol 2005;129:449-64.
Castro OL, Hoque M, Brown BD. Pul-110.monary hypertension in
sickle cell dis-ease: cardiac catheterization results andsurvival.
Blood 2003;101:1257-61.
Ataga KI, Sood N, De Gent G, et al.111.Pulmonary hypertension in
sickle cell dis-ease. Am J Med 2004;117:665-9.
Machado RF, Anthi A, Steinberg112.MH, et al. N-terminal
pro-brain natriuret-ic peptide levels and risk of death in sick-le
cell disease. JAMA 2006;296:310-8.
McQuillan BM, Picard MH, Leavitt113.M, Weyman AE. Clinical
correlates and
reference intervals for pulmonary arterysystolic pressure among
echocardiograph-ically normal subjects. Circulation
2001;104:2797-802.
Machado RF, Kyle Mack A, Martyr S,114.et al. Severity of
pulmonary hypertensionduring vaso-occlusive pain crisis and
exer-cise in patients with sickle cell disease. BrJ Haematol
2007;136:319-25.
Mekontso Dessap A, Leon R, Habibi115.A, et al. Pulmonary
hypertension and corpulmonale during severe acute chest syn-drome
in sickle cell disease. Am J RespirCrit Care Med
2008;177:646-53.
Sachdev V, Machado RF, Shizukuda Y,116.et al. Diastolic
dysfunction is an indepen-
dent risk factor for death in patients withsickle cell disease.
J Am Coll Cardiol 2007;49:472-9.
Hayag-Barin JE, Smith RE, Tucker117.FC Jr. Hereditary
spherocytosis, thrombo-cytosis, and chronic pulmonary emboli:a case
report and review of the literature.Am J Hematol 1998;57:82-4.
Vichinsky EP. Pulmonary hyperten-118.sion in sickle cell
disease. N Engl J Med2004;350:857-9.
Taylor JG IV, Nolan VG, Mendelsohn119.L, Kato GJ, Gladwin MT,
Steinberg MH.Chronic hyper-hemolysis in sickle cell ane-mia:
association of vascular complicationsand mortality with less
frequent vasooc-clusive pain. PLoS One 2008;3(5):e2095.Copyright
2008 Massachusetts Medical Society.
COLLECTIONSOFARTICLESONTHEJOURNALSWEBSITE
TheJournals Web site (www.nejm.org) sorts published articles
intomore than 50 distinct clinical collections, which can be used
as convenient
entry points to clinical content. In each collection, articles
are cited in reversechronologic order, with the most recent
first.
Downloaded from www nejm org at UNIVERSITY OF PITTSBURGH on
January 6 2009