Embed Size (px)
DESCRIPTION
Copyright (c) UWorld, Please do not save, print, cut, copy or paste anything while a test is active.
Citation preview

Official reprint from UpToDatewww.uptodate.com ©2016 UpToDate
AuthorJill P Karpel, MD
Section EditorTalmadge E King, Jr, MD
Deputy EditorHelen Hollingsworth, MD
Overview of pulmonary disease in injection drug users
All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Dec 2015. | This topic last updated: May 22, 2015. INTRODUCTION — Injection drug users (IDUs) are at increased risk for acute and chronic pulmonary complications. These sequelae may be due to pharmacodynamic properties of the drugs, effects of intravenous contaminants, or complications of the intravenous route of administration.The general pulmonary complications and drug-specific pulmonary diseases that may result from injection drug use will be reviewed here. Other complications of injection drug use, such as foreign body granulomatosis, infective endocarditis, opioid use disorder, cocaine intoxication, and methamphetamine intoxication, are reviewed separately. (See "Substance use disorder: Principles for recognition and assessment in general medical care" and "Foreign body granulomatosis" and "Infective endocarditis in injection drug users" and "Pharmacotherapy for opioid use disorder" and "Acute opioid intoxication in adults" and "Cocaine: Acute intoxication" and "Methamphetamine intoxication".)PULMONARY COMPLICATIONS — The pulmonary complications associated with intravenous injection of illicit drugs include pneumonia, septic embolization, noncardiogenic pulmonary edema, foreign body granulomatosis, emphysema, interstitial lung disease, pulmonary vascular disease, pneumothorax, and an increased incidence of fatal asthma [1-4].Pneumonia — Injection drug users (IDUs) have a 10-fold increased risk of community-acquired pneumonia compared with the general population [2]. This may be due to a number of factors:
The organisms that most commonly cause community-acquired pneumonia in this population include Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Klebsiella pneumoniae, and Escherichia coli, although it is difficult to separate out the pathogens associated with HIV-positive and HIV-negative injection drug use [5,6]. Antimicrobial therapy is initially empiric and based on the clinical situation, particularly whether the chest radiograph shows focal or diffuse opacities and whether the patient meets criteria for hospital admission. In patients presenting with typical symptoms of bacterial pneumonia with focal consolidation on chest radiograph, the initial antibiotic regimen will be directed at the most common community-acquired pathogens. (See "Diagnostic approach to community-acquired pneumonia in adults" and "Bacterial pulmonary infections in HIV-infected patients" and "Treatment of community-acquired pneumonia in adults in the outpatient setting" and "Treatment of community-acquired pneumonia in adults who require hospitalization".)If the etiology of community-acquired pneumonia is identified using reliable microbiologic methods, antimicrobial therapy can be focused on that pathogen (table 1). (See "Treatment of community-acquired pneumonia in adults who require hospitalization", section on 'Treatment regimens'.)
®®
Concurrent smoking of cigarettes or illicit drugs may impair local lung defenses, macrophage activity, and mucociliary clearance
●
The stupor induced by some injected drugs favors development of aspiration pneumonia or lung abscess (see "Aspiration pneumonia in adults" and "Lung abscess")
●
Bacteremia may follow injection and may hematogenously infect the lung●HIV-positive IDUs are at substantially higher risk for bacterial pneumonia than HIV-negative IDUs●

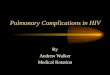
For patients who have progressive disease despite antibiotic therapy for bacterial pneumonia, other considerations include fungal and mycobacterial agents. Candida pneumonia has been reported in IDUs when the injection drug is contaminated [2].Tuberculosis (particularly multidrug-resistant tuberculosis) is more prevalent among IDUs than it is in the general population [7-9]. The excess risk largely relates to covariates which are more frequent among IDUs, such as poverty, homelessness, malnutrition, HIV infection, and poor medical care. Tuberculosis should be suspected in patients with a longer prodrome, particularly in the presence of fever or night sweats for more than a week prior to presentation, or weight loss. In addition, mycobacterial disease should be suspected in patients with nonresolving pneumonia. (See "Epidemiology of tuberculosis" and "Clinical manifestations and complications of pulmonary tuberculosis" and "Nonresolving pneumonia", section on 'Tuberculosis'.)The use of injection drugs is a strong risk factor for the acquisition of HIV infection. IDUs who present with pneumonia should be assessed for possible HIV infection. In the presence of known HIV infection, a variety of opportunistic pulmonary infections in addition to tuberculosis may occur. (See "Approach to the HIV-infected patient with pulmonary symptoms".)Septic emboli — Septic pulmonary emboli can originate in the peripheral veins at sites of thrombophlebitis or they can arise from heart valves that have been damaged and infected due to injection drug use. Right-sided valve (tricuspid) endocarditis is generally found to be more common among IDUs than left-sided. (See "Pathogenesis of vegetation formation in infective endocarditis" and "Infective endocarditis in injection drug users", section on 'Clinical evaluation'.)Patients typically present with fever, but generally do not have an audible murmur or peripheral stigmata of infective endocarditis. Blood cultures are usually positive. The radiographic manifestations of septic pulmonary emboli include ill-defined, nodular pulmonary opacities, cavities, abscesses, infarction, and pulmonary gangrene (image 1). The evaluation and treatment of infective endocarditis in IDUs is discussed separately. (See "Infective endocarditis in injection drug users".)Noncardiogenic pulmonary edema — Noncardiogenic pulmonary edema (NPE) refers to the radiographic evidence of alveolar fluid accumulation without hemodynamic evidence to suggest a cardiogenic etiology and is caused by increased pulmonary capillary permeability. NPE can occur following intravenous injection of cocaine and, more commonly, opioids [3,10-12]. Acute respiratory distress syndrome (ARDS) is a more severe form of NPE, associated with severe hypoxemia and the need for mechanical ventilatory support. (See "Noncardiogenic pulmonary edema" and "Acute respiratory distress syndrome: Epidemiology, pathophysiology, pathology, and etiology in adults", section on 'Etiologies and predisposing factors'.)The exact pathophysiology of NPE due to opioid overdose (eg, heroin or methadone) is unknown, but may include a direct effect of the drug, cerebral edema (neurogenic), or possibly negative pressure. Patients with central nervous system depression due to a drug overdose can develop upper airway obstruction. Breathing against the obstruction can create a strong negative pressure across the alveoli, which causes pulmonary capillary leakage. (See "Noncardiogenic pulmonary edema", section on 'Opioid overdose' and "Noncardiogenic pulmonary edema", section on 'Neurogenic pulmonary edema'.)Patients typically present with decreased mental status and evidence of respiratory insufficiency (eg, tachypnea, tachycardia, hypoxemia). Patients with NPE due to opiate intoxication typically have severe respiratory depression requiring naloxone reversal. Co-intoxication with alcohol or cocaine is present in approximately 50 percent [11]. The majority of these patients are hypoxemic on arrival in the emergency department [10,11].Imaging findings in IDUs with NPE were described in a series of 27 patients with opiate-related NPE: 74 percent had bilateral, ground-glass opacities suggestive of pulmonary edema, while unilateral pulmonary edema or focal opacities were noted in the remainder [10].

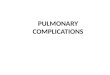
The diagnosis of NPE in IDUs is based on the clinical presentation and exclusion of processes in the differential diagnosis, which includes the other causes of ARDS that may complicate injection drug use, such as sepsis, pneumonia (bacterial, viral, fungal), aspiration, cardiogenic pulmonary edema, and pulmonary embolism. (See "Noncardiogenic pulmonary edema".)For most IDUs with NPE, treatment is supportive. Symptoms and signs typically resolve in 24 hours with supportive care (eg, supplemental oxygen), although approximately one-third of patients require mechanical ventilation for 24 to 48 hours. (See "Acute opioid intoxication in adults" and "Noncardiogenic pulmonary edema", section on 'Treatment'.)Foreign body granulomatosis — Drug users sometimes pulverize tablets intended for oral use, dissolve them in water, and inject them intravenously. Talc, starch, cotton, and cellulose are used as filler agents in these tablets and may be carried by the bloodstream until they lodge in the pulmonary capillary bed; chronic inflammation and multiple foreign body granulomas in the lungs may ensue.Patients may be asymptomatic or may present with nonspecific complaints such as dyspnea, cough, or an increase in sputum production. Computed tomography (CT) typically shows diffuse, small nodules (2 to 3 mm) or ground-glass opacities (image 2). Pulmonary hypertension, emphysema, and interstitial fibrosis can occur if the process is severe. The diagnosis and management of foreign body granulomatosis are discussed separately. (See "Foreign body granulomatosis".)Bullous lung disease and emphysema — Emphysema and bullous lung disease have been described in association with HIV infection, but HIV-negative IDUs can also develop these complications, particularly when methadone, methylphenidate, or talc-containing drugs are injected [13-15]. (See "Foreign body granulomatosis".)In one series, the prevalence of bullous lung damage and emphysema among intravenous drug users (as assessed by chest radiographs) was 2 percent [16]. The bullous cysts were noted predominantly in the upper lobes and in the lung periphery, with sparing of the central portions of the lungs [16,17]. Other reports of patients who injected talc-containing drugs have reported a predominance of bullous changes in the lower lobes [18,19]. Patients present with cough and dyspnea, and usually have combined obstructive and restrictive defects on pulmonary function testing.Interstitial lung disease — Interstitial lung disease in IDUs is generally associated with foreign body granulomatosis, but may also be a nonspecific finding due to previous episodes of infection, aspiration, or infarction. Lymphocytic interstitial pneumonia, a rare interstitial lung disease in the general population, is seen with increased frequency in HIV-infected individuals. In addition, organizing pneumonia, sarcoidosis, drug hypersensitivity, and immune reconstitution syndrome can develop in HIV-infected patients. (See "Foreign body granulomatosis" and "Approach to the adult with interstitial lung disease: Clinical evaluation" and "Approach to the adult with interstitial lung disease: Diagnostic testing" and "Approach to the HIV-infected patient with pulmonary symptoms", section on 'Pulmonary diseases and HIV'.)Pulmonary hypertension — Pulmonary hypertension may be induced by obstruction or obliteration of the pulmonary vascular bed from multiple causes, including foreign body granulomatosis, emphysema, or interstitial disease. Patients who are HIV-positive may develop pulmonary arterial hypertension (PAH) with plexiform lesions and medial hypertrophy. The evaluation and management of pulmonary hypertension associated with HIV infection is discussed separately. (See "Pulmonary arterial hypertension associated with human immunodeficiency virus" and "Overview of pulmonary hypertension in adults".)Drugs with sympathomimetic properties (eg, cocaine, methamphetamine) can produce transient pulmonary vasoconstriction. It also appears that chronic use of these drugs can lead to irreversible injury and production of a syndrome indistinguishable from primary pulmonary hypertension. In one retrospective study, patients with idiopathic PAH were ten times more likely to use stimulants (ie, amphetamines, methamphetamines, or cocaine) than patients with PAH due to known risk factors, such

as collagen vascular disease, congenital heart disease, or anorexigen use [20]. (See "Pathogenesis of pulmonary hypertension", section on 'Drugs and toxins'.)Pneumothorax and pneumomediastinum — Pneumothorax may result from unsuccessful attempts to inject drugs into the central circulation via the subclavian and jugular veins ("pocket shots"). It has also been reported as a complication of crack cocaine use, septic pulmonary emboli, and drug-related bullous disease [21,22]. (See 'Cocaine' below.)Pneumomediastinum is associated with inhalation of crack cocaine and, less commonly, intranasal cocaine [23]. It is most likely due to performance of a Valsalva maneuver after inhalation, rather than an effect of the drug. Approximately 20 percent also had a pneumothorax. (See "Pulmonary complications of cocaine abuse", section on 'Pneumothorax and pneumomediastinum'.)Asthma — IDUs with asthma appear to have an increased risk of fatal asthma [24-27] (see "Identifying patients at risk for fatal asthma", section on 'Minor risk factors'):
Amyloidosis — Bilateral pulmonary nodules containing amyloid (AA) protein have been reported in IDUs with HIV disease [28]. (See "HIV infection and malignancy: Management considerations", section on 'Plasma cell disorders'.)DRUG-SPECIFIC COMPLICATIONSCocaine — Cocaine is an alkaloid with anesthetic and central nervous system stimulant properties. It can be inhaled nasally or injected; a heat-stable form produced by boiling with bicarbonate can be smoked (“free-basing”). There is a higher incidence of clinically apparent pulmonary complications when cocaine is smoked versus used intravenously or intranasally. The pulmonary complications associated with the use of cocaine are multiple and can be divided into acute and chronic pulmonary disorders.
One toxicologic study of 92 cases of fatal asthma in Chicago found evidence of substance abuse, most commonly cocaine or opiates, in 32 percent of individuals [24]. It is unclear whether the drugs themselves or other unidentified factors are responsible for the increased asthma fatalities. Optimal use of asthma medicines is less frequent among drug users [25], and antiinflammatory medications were being utilized by just two patients in the Chicago series.
●
A retrospective review of 152 inner city asthma patients found that intubation and mechanical ventilation were required more often among patients presenting with an acute exacerbation if they use cocaine (31 versus 11.5 percent) or heroin (17 versus 2.3 percent), compared with nonusers [26].
●
Acute pulmonary complications – The acute complications of injection cocaine use overlap with those of inhaled crack cocaine; the most common are acute pulmonary edema and pulmonary hemorrhage.
●
Acute noncardiogenic pulmonary edema (NPE) presents with the rapid onset of dyspnea, hypoxemia, and diffuse opacities on chest radiograph; altered mental status is frequently also present in injection drug users (IDUs). Treatment is supportive and includes supplemental oxygen and ventilator support, if necessary. Clinical improvement generally occurs within 24 to 48 hours. (See 'Noncardiogenic pulmonary edema' above and "Noncardiogenic pulmonary edema".)
•
Pulmonary hemorrhage can occur with or without frank hemoptysis and is commonly found on autopsy in asymptomatic cocaine users [29]. The causes of hemorrhage are probably multifactorial and may include NPE, pulmonary infarction, infection, and pulmonary hypertension. Treatment is supportive. (See "Pulmonary complications of cocaine abuse".)
•
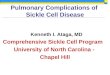
Cardiogenic edema may result from cocaine-induced coronary artery spasm, myocardial ischemia, and left ventricular dysfunction (image 3). The diagnosis is suspected in patients
•

Opioids — Opiates are naturally occurring alkaloids from the poppy plant; the term “opioids” includes natural opiates (eg, morphine, codeine) and synthetic derivatives that also bind to opioid receptors in the brain (eg, heroin, hydrocodone). Use of heroin (diacetyl morphine) is rising in the United States, and increasingly pure formulations of the drug are available. Most of the direct morbidity and mortality related to opiate use occur after acute intoxication and are due to anaphylaxis, noncardiogenic pulmonary edema, acute respiratory acidosis, and aspiration pneumonitis. (See "Acute opioid intoxication in adults".)
Methylphenidate and methamphetamine — Methylphenidate and methamphetamine are sympathomimetic stimulants that are sometimes injected intravenously by IDUs. General signs and symptoms of toxicity include restlessness, tachycardia, hypertension, diaphoresis, and confusion. Long-term use of methylphenidate can lead to bullous emphysema.
with dyspnea, diffuse pulmonary opacities on chest imaging, an elevated brain natriuretic peptide, and/or reduced left ventricular function by echocardiogram. The diagnosis and treatment are discussed separately. Of note, beta-adrenergic antagonists (ie, beta-blockers) are avoided in cocaine-related cardiovascular disease because they may create unopposed alpha-adrenergic stimulation. (See "Evaluation and management of the cardiovascular complications of cocaine abuse", section on 'Cardiovascular conditions associated with cocaine use' and "Cocaine: Acute intoxication", section on 'Cardiovascular complications' and "Treatment of acute decompensated heart failure: General considerations".)Pneumothorax and pneumomediastinum are also reported in association with cocaine inhalation. (See 'Pneumothorax and pneumomediastinum' above.)
•
Chronic pulmonary complications – The chronic pulmonary complications of injection cocaine use include foreign body granulomatosis, lung scarring due to repeated pulmonary infections and pulmonary infarction, and pulmonary arterial hypertension (PAH) [30]. (See 'Foreign body granulomatosis' above and 'Interstitial lung disease' above and 'Pulmonary hypertension' above.)
●
Massive release of histamine from mast cells and basophils may follow narcotic injection due to an anaphylactoid reaction to the narcotics themselves or to adulterants or contaminants. Shock, bronchospasm, and upper airway edema may ensue [31]. (See "Anaphylaxis: Rapid recognition and treatment".)
●
Heroin-induced noncardiogenic pulmonary edema usually develops rapidly within the first few hours following injection, but rarely occurs as late as 24 hours. This complication can also occur with other opiates such as codeine and methadone, as well as fentanyl-heroin mixtures [32]. Oxygen therapy and noninvasive positive pressure ventilation or intubation with mechanical ventilation may be required. Improvement can occur rapidly, but full resolution generally requires two to three days. (See 'Noncardiogenic pulmonary edema' above and "Noncardiogenic pulmonary edema".)
●
Narcotics powerfully suppress central respiratory drive. Acute administration may produce hypercapnia, acute respiratory acidosis, and if severe, cardiopulmonary arrest and death.
●
Narcotics also diminish the level of consciousness and depress the cough reflex. These actions render narcotic users less able to protect the airway and more likely to develop aspiration pneumonitis (due to infection or aspirated gastric contents) and lung abscess. Lower lobe bronchiectasis has been reported among heroin users and may result from prior episodes of aspiration or pulmonary infection [33]. (See "Aspiration pneumonia in adults" and "Lung abscess".)
●
In a case report, an intravenous heroin user developed respiratory failure due to organizing pneumonia; scattered, nonnecrotizing granulomata and multinucleated giant cells with foreign body particles were also noted [34].
●

The evaluation and management of acute methamphetamine intoxication are discussed separately. (See "Methamphetamine intoxication".)SUMMARY AND RECOMMENDATIONS
Methylphenidate – Intravenous methylphenidate has been associated with the development of hemoptysis, chest pain, and wheezing. One series of 22 patients hospitalized following methylphenidate use reported that 80 percent had one or more of these findings [35]. Excess adrenergic activity and vasospasm may underlie these complications.Habitual intravenous use of methylphenidate has been associated with the development of panlobar emphysema after one to six years [18,36]. Emphysema primarily involves the lower lobes of the lungs and has a similar radiographic appearance to alpha-1 antitrypsin deficiency. The relative contribution of methylphenidate, foreign body granulomatosis, and concomitant smoking in the genesis of emphysema among these patients is unclear, but one study compared the findings on chest computed tomography (CT) of patients with foreign body granulomatosis who abused intravenous methylphenidate with others who did not [37]. A significantly increased prevalence of lower lobe panacinar emphysema was demonstrated in patients abusing methylphenidate, and was frequently associated with a fine micronodular pattern and ground-glass attenuation. (See 'Bullous lung disease and emphysema' above.)
●
Methamphetamine – Methamphetamine ("speed" or "crank") is a stimulant drug that has similar effects to cocaine. It can be smoked or administered intravenously or intranasally. There are rare case reports of acute noncardiogenic pulmonary edema and pulmonary hypertension following the inhalation of methamphetamine, but complications of intravenous use are not well documented. Cardiogenic pulmonary edema can complicate methamphetamine intoxication, possibly related to fluid resuscitation in the setting of acute hypertension. (See "Methamphetamine intoxication", section on 'Clinical features' and "Methamphetamine intoxication", section on 'Fluid resuscitation'.)
●
Pulmonary complications associated with intravenous injection of illicit drugs include pneumonia, septic embolization, foreign body granulomatosis, emphysema, interstitial lung disease, organizing pneumonia, pulmonary vascular disease, pneumothorax, pneumomediastinum, and an increased incidence of fatal asthma. (See 'Pulmonary complications' above.)
●
Injection drug users (IDUs) have a 10-fold increased risk of community-acquired pneumonia compared with the general population; common causative organisms include Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Klebsiella pneumoniae, and Escherichia coli. In addition, those who develop HIV/AIDS are at risk for opportunistic pulmonary infections (eg, tuberculosis, atypical mycobacteria, Pneumocystis jirovecii, cytomegalovirus). (See 'Pneumonia' above.)
●
When tablets intended for oral use are pulverized and injected intravenously, the insoluble agents in the tablets (eg, talc, cotton, and cellulose) can be trapped in the pulmonary vasculature, migrate through the vessel walls, and initiate a granulomatous inflammatory response in the perivascular interstitium. This disease process, known as foreign body granulomatosis, can lead to development of progressive interstitial lung disease, emphysema, and pulmonary hypertension. (See 'Foreign body granulomatosis' above and "Foreign body granulomatosis".)
●
Emphysema and bullous lung disease may result from concomitant cigarette smoking, but are also associated with HIV infection and intravenous injection of methadone, methylphenidate, and talc-containing drugs. (See 'Pulmonary complications' above.)
●
Pneumothorax may result from unsuccessful attempts to inject drugs into the central circulation via the subclavian and jugular veins ("pocket shots"). It has also been reported as a complication of septic pulmonary emboli and drug-related bullous disease. (See 'Pneumothorax and pneumomediastinum' above.)
●

Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES1. Hind CR. Pulmonary complications of intravenous drug misuse. 1. Epidemiology and non-infective
complications. Thorax 1990; 45:891.2. Hind CR. Pulmonary complications of intravenous drug misuse. 2. Infective and HIV related
complications. Thorax 1990; 45:957.3. Todorović MS, Mitrović S, Aleksandrić B, et al. Association of pulmonary histopathological findings
with toxicological findings in forensic autopsies of illicit drug users. Vojnosanit Pregl 2011; 68:639.4. Passarino G, Ciccone G, Siragusa R, et al. Histopathological findings in 851 autopsies of drug
addicts, with toxicologic and virologic correlations. Am J Forensic Med Pathol 2005; 26:106.5. Caiaffa WT, Vlahov D, Graham NM, et al. Drug smoking, Pneumocystis carinii pneumonia, and
immunosuppression increase risk of bacterial pneumonia in human immunodeficiency virus-seropositive injection drug users. Am J Respir Crit Care Med 1994; 150:1493.
6. Madeddu G, Porqueddu EM, Cambosu F, et al. Bacterial community acquired pneumonia in HIV-infected inpatients in the highly active antiretroviral therapy era. Infection 2008; 36:231.
7. Reichman LB, Felton CP, Edsall JR. Drug dependence, a possible new risk factor for tuberculosis disease. Arch Intern Med 1979; 139:337.
8. Frieden TR, Sterling T, Pablos-Mendez A, et al. The emergence of drug-resistant tuberculosis in New York City. N Engl J Med 1993; 328:521.
9. Perlman DC, Salomon N, Perkins MP, et al. Tuberculosis in drug users. Clin Infect Dis 1995; 21:1253.
10. Sporer KA, Dorn E. Heroin-related noncardiogenic pulmonary edema : a case series. Chest 2001; 120:1628.
11. Sterrett C, Brownfield J, Korn CS, et al. Patterns of presentation in heroin overdose resulting in pulmonary edema. Am J Emerg Med 2003; 21:32.
12. Kissner DG, Lawrence WD, Selis JE, Flint A. Crack lung: pulmonary disease caused by cocaine abuse. Am Rev Respir Dis 1987; 136:1250.
13. O'Donnell AE, Pappas LS. Pulmonary complications of intravenous drug abuse. Experience at an inner-city hospital. Chest 1988; 94:251.
14. Paré JP, Cote G, Fraser RS. Long-term follow-up of drug abusers with intravenous talcosis. Am Rev Respir Dis 1989; 139:233.
15. Stern EJ, Frank MS, Schmutz JF, et al. Panlobular pulmonary emphysema caused by i.v. injection of methylphenidate (Ritalin): findings on chest radiographs and CT scans. AJR Am J Roentgenol 1994; 162:555.
Complications of intravenous injection of crack cocaine include noncardiogenic and cardiogenic pulmonary edema, acute and recurrent alveolar hemorrhage, and interstitial lung disease due to foreign body granulomatosis. (See 'Cocaine' above.)
●
Pulmonary complications related to opioid injection typically occur in the setting of acute intoxication and are due to anaphylaxis, noncardiogenic pulmonary edema, hypoventilation with acute respiratory acidosis, and aspiration pneumonitis. (See 'Opioids' above and "Acute opioid intoxication in adults" and "Opioid intoxication in children and adolescents".)
●
Intravenous injection of methylphenidate has been associated with hemoptysis, chest pain, and wheezing; excess adrenergic activity and vasospasm may underlie these complications. Foreign body granulomatosis and emphysema are complications associated with long-term use. Methamphetamine ("speed" or "crank") is a stimulant drug that has similar effects to cocaine and is rarely associated with noncardiogenic pulmonary edema and pulmonary hypertension. (See 'Methylphenidate and methamphetamine' above.)
●

16. Goldstein DS, Karpel JP, Appel D, Williams MH Jr. Bullous pulmonary damage in users of intravenous drugs. Chest 1986; 89:266.
17. Gurney JW, Bates FT. Pulmonary cystic disease: comparison of Pneumocystis carinii pneumatoceles and bullous emphysema due to intravenous drug abuse. Radiology 1989; 173:27.
18. Shlomi D, Shitrit D, Bendayan D, et al. Successful lung transplantation for talcosis secondary to intravenous abuse of oral drug. Int J Chron Obstruct Pulmon Dis 2008; 3:327.
19. Marchiori E, Lourenço S, Gasparetto TD, et al. Pulmonary talcosis: imaging findings. Lung 2010; 188:165.
20. Chin KM, Channick RN, Rubin LJ. Is methamphetamine use associated with idiopathic pulmonary arterial hypertension? Chest 2006; 130:1657.
21. Aguado JM, Arjona R, Ugarte P. Septic pulmonary emboli. A rare cause of bilateral pneumothorax in drug abusers. Chest 1990; 98:1302.
22. Fiorelli A, Accardo M, Rossi F, Santini M. Spontaneous pneumothorax associated with talc pulmonary granulomatosis after cocaine inhalation. Gen Thorac Cardiovasc Surg 2014.
23. Alnas M, Altayeh A, Zaman M. Clinical course and outcome of cocaine-induced pneumomediastinum. Am J Med Sci 2010; 339:65.
24. Levenson T, Greenberger PA, Donoghue ER, Lifschultz BD. Asthma deaths confounded by substance abuse. An assessment of fatal asthma. Chest 1996; 110:604.
25. National Asthma Education and Prevention Program: Expert panel report III: Guidelines for the diagnosis and management of asthma. Bethesda, MD: National Heart, Lung, and Blood Institute, 2007. (NIH publication no. 08-4051). www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm (Accessed on February 28, 2011).
26. Levine M, Iliescu ME, Margellos-Anast H, et al. The effects of cocaine and heroin use on intubation rates and hospital utilization in patients with acute asthma exacerbations. Chest 2005; 128:1951.
27. Doshi V, Shenoy S, Ganesh A, et al. Profile of Acute Asthma Exacerbation in Drug Users. Am J Ther 2014.
28. Shah SP, Khine M, Anigbogu J, Miller A. Nodular amyloidosis of the lung from intravenous drug abuse: an uncommon cause of multiple pulmonary nodules. South Med J 1998; 91:402.
29. Bailey ME, Fraire AE, Greenberg SD, et al. Pulmonary histopathology in cocaine abusers. Hum Pathol 1994; 25:203.
30. Yakel DL Jr, Eisenberg MJ. Pulmonary artery hypertension in chronic intravenous cocaine users. Am Heart J 1995; 130:398.
31. Edston E, van Hage-Hamsten M. Anaphylactoid shock--a common cause of death in heroin addicts? Allergy 1997; 52:950.
32. Algren DA, Monteilh CP, Punja M, et al. Fentanyl-associated fatalities among illicit drug users in Wayne County, Michigan (July 2005-May 2006). J Med Toxicol 2013; 9:106.
33. Banner AS, Rodriguez J, Sunderrajan EV, et al. Bronchiectasis: a cause of pulmonary symptoms in heroin addicts. Respiration 1979; 37:232.
34. Bishay A, Amchentsev A, Saleh A, et al. A hitherto unreported pulmonary complication in an IV heroin user. Chest 2008; 133:549.
35. Parran TV Jr, Jasinski DR. Intravenous methylphenidate abuse. Prototype for prescription drug abuse. Arch Intern Med 1991; 151:781.
36. Sherman CB, Hudson LD, Pierson DJ. Severe precocious emphysema in intravenous methylphenidate (Ritalin) abusers. Chest 1987; 92:1085.
37. Ward S, Heyneman LE, Reittner P, et al. Talcosis associated with IV abuse of oral medications: CT findings. AJR Am J Roentgenol 2000; 174:789.
Topic 4337 Version 7.0

GRAPHICSRecommended antimicrobial therapy for specific pathogens causing community-acquired pneumonia in adults
Organism Preferred antimicrobial(s)
Alternative antimicrobial(s)
Streptococcus pneumoniaePenicillin nonresistant; MIC <2 microgram/mL
Penicillin G, amoxicillin Macrolide, cephalosporins (oral [cefpodoxime, cefprozil, cefuroxime, cefdinir, cefditoren] or parenteral [cefuroxime, ceftriaxone, cefotaxime]), clindamycin, doxycyline, respiratory fluoroquinolone*
Penicillin resistant; MIC ≥2 microgram/mL
Agents chosen on the basis of susceptibility, including cefotaxime, ceftriaxone, fluoroquinolone
Vancomycin, linezolid, high-dose amoxicillin (3 g/day with penicillin MIC ≤4 microgram/mL)
Haemophilus influenzaeNon-beta-lactamase producing
Amoxicillin Fluoroquinolone, doxycycline, azithromycin, clarithromycin
Beta-lactamase producing Second- or third-generation cephalosporin, amoxicillin-clavulanate
Fluoroquinolone, doxycycline, azithromycin, clarithromycin
Mycoplasma pneumoniae/Chlamydophila pneumoniae
Macrolide, a tetracycline Fluoroquinolone
Legionella species Fluoroquinolone, azithromycin
Doxycyline
Chlamydophila psittaci A tetracycline MacrolideCoxiella burnetii A tetracycline MacrolideFrancisella tularensis Doxycycline Gentamicin, streptomycinYersinia pestis Streptomycin, gentamicin Doxycyline, fluoroquinoloneBacillus anthracis(inhalation)
Ciprofloxacin, levofloxacin, doxycycline (usually with second agent)
Other fluoroquinolones; beta-lactam, if susceptible; rifampin; clindamycin; chloramphenicol
Enterobacteriaceae Third-generation cephalosporin, carbapenem (drug of choice if extended-spectrum beta-lactamase producer)
Beta-lactam/beta-lactamase inhibitor , fluoroquinolone
Pseudomonas aeruginosa Antipseudomonal beta-lactam plus (ciprofloxacin or levofloxacin or aminoglycoside)
Aminoglycoside plus(ciprofloxacin or levofloxacin )
¶
¶
Δ◊
§¥ ¥

Burkholderia pseudomallei Carbapenem, ceftazidime Fluoroquinolone, TMP-SMXAcinetobacter species Carbapenem Cephalosporin-
aminoglycoside, ampicillin-sulbactam, colistin
Staphylococcus aureusMethicillin susceptible Antistaphylococcal penicillin Cefazolin, clindamycinMethicillin resistant Vancomycin or linezolid TMP-SMX
Bordetella pertussis Macrolide TMP-SMXAnaerobe (aspiration) Beta-lactam/beta-lactamase
inhibitor , clindamycinCarbapenem
Influenza virus Refer to associated topic reviews
Mycobacterium tuberculosis Isoniazid plus rifampin plus ethambutol plus pyrazinamide
Depends on susceptibility pattern. Refer to associated topic reviews.
Coccidioides species For uncomplicated infection in a normal host, no therapy generally recommended; for therapy, itraconazole, fluconazole.
Amphotericin B
Histoplasmosis Itraconazole** Amphotericin B**Blastomycosis Itraconazole** Amphotericin B**
Choices should be modified on the basis of susceptibility test results and advice from local specialists. Refer to local references for appropriate doses.Preferred agent may change over time due to changing resistance patterns and depends on many factors, including severity of illness. Refer to associated topic reviews for updated and detailed treatment recommendations for each pathogen.MIC: minimum inhibitory concentration; ATS: American Thoracic Society; CDC: Centers for Disease Control and Prevention; IDSA: Infectious Diseases Society of America; TMP-SMX: trimethoprim-sulfamethoxazole.* Levofloxacin, moxifloxacin, gemifloxacin (not a first-line choice for penicillin susceptible strains); ciprofloxacin is appropriate for Legionella and most gram-negative bacilli (including H. influenzae).¶ Azithromycin is more active in vitro than clarithromycin for H. influenzae.Δ Imipenem-cilastatin, meropenem, ertapenem.◊ Piperacillin-tazobactam for gram-negative bacilli, ticarcillin-clavulanate, ampicillin-sulbactam, or amoxicillin-clavulanate.§ Ticarcillin, piperacillin, ceftazidime, cefepime, aztreonam, imipenem, meropenem.¥ 750 mg daily.‡ Nafcillin, oxacillin, flucloxacillin.† Choice of antiviral regimen depends on type of influenza virus and expected resistance pattern. (Refer to the UpToDate topic on antiviral drugs for the treatment of influenza in adults.)** Preferred agent depends on severity of illness. Refer to associated topic reviews for full discussions.Adapted with permission from: Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thorac Society Consensus Guidelines on the Management of
‡
◊
†

Community-acquired Pneumonia in Adults. Clin Infect Dis 2007; 44:S27. Copyright © 2007 University of Chicago Press.Graphic 64816 Version 8.0

Septic embolization in an intravenous drug user with tricuspid valve endocarditis
Chest radiograph shows multiple ill-defined nodular opacities, some with cavitation. This is an example of multifocal patchy opacification.Courtesy of Paul Stark, MD.Graphic 59037 Version 4.0

Talc granulomatosis
Talc granulomatosis in an intravenous drug user with multiple, partially confluent, bilateral micronodules.Courtesy of Paul Stark, MD.Graphic 53000 Version 3.0

Disclosures: Jill P Karpel, MD Nothing to disclose. Talmadge E King, Jr, MD Consultant/Advisory Boards: InterMune [pulmonary fibrosis (pirfenidone)]; ImmuneWorks [pulmonary fibrosis]; Boehringer Ingelheim [IPF (nintedanib)]; GlaxoSmithKline [pulmonary fibrosis]; Daiichi Sankyo [pulmonary fibrosis]. Helen Hollingsworth, MD Nothing to disclose. Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through a multi-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content is required of all authors and must conform to UpToDate standards of evidence. Conflict of interest policy
Hydrostatic pulmonary edema
Pulmonary edema in a "butterfly distribution" due to left ventricular failure. Chest radiograph shows large perihilar opacities in patient with enlarged cardiac silhouette.Courtesy of Paul Stark, MD.Graphic 58394 Version 4.0
Disclosures