Embed Size (px)
Citation preview
2018 Health Insurance Plans
For Retired SDCERA Members
Strength. Service. Commitment.
San Diego County Employees Retirement Association
Table of Contents
Eligibility ...........................................................................................1
Enrollment in a plan ...........................................................................1
Health Insurance Allowance ...............................................................2
2018 Monthly Premiums .....................................................................3
Medical Plans ....................................................................................4
Dental Plans .......................................................................................9
Notice of Creditable Coverage ..........................................................10
COBRA Continuation ......................................................................11
Legal Notices ...................................................................................13

2018 Health Insurance Plans for Retired Members
Who can enroll?
Retired Members, surviving spouses/partners, and eligible dependents
When can I enroll?
Annually during Open Enrollment, or within 30 days of an eligible event such as retirement
Do I need to re-enroll every year?
No, your current
SDCERA‑sponsored
plan election(s) will renew automatically if you take no action during Open Enrollment
If you are enrolled in an SDCERA-sponsored health plan, your current plan election(s) will automatically renew for the 2018 calendar year, unless you request a change.
Eligibility
SDCERA sponsors group medical and dental insurance plans for retired Members and their eligible dependents. In addition, if you are the surviving spouse/partner or dependent of a deceased SDCERA Member and you receive a monthly SDCERA retirement benefit, the plans are also available to you. Eligible dependents include a spouse or registered domestic partner and children under age 26.
Premium(s) and applicable fees for all SDCERA‑sponsored health plans, including coverage for your dependent(s), will be deducted from your monthly retirement benefit. If your monthly benefit does not cover the cost of the plan(s) you select, the SDCERA Retiree Health Program Service Center will contact you to set up automatic debit from your checking or savings account.
Plans provide coverage in both California and out‑of‑state service areas, but service areas vary by plan. Please contact the plan to verify that you live within its service area before enrolling. Premiums and types of medical plans vary based on Medicare eligibility. Dental plans are available to Members regardless of age and Medicare eligibility. SDCERA does not offer plans that provide coverage to Members living outside of the United States.
Enrollment in a plan
You may enroll or make changes to your current SDCERA‑sponsored plan selection during Open Enrollment from November 1 through November 22, 2017. Enrollment or changes outside of the annual Open Enrollment period are limited to qualifying life events (see Page 2). If you wish to continue your current election(s), you do not need to do anything during Open Enrollment; your current plan election(s) will renew automatically. If you change your plan, or enroll for the first time, allow 30 days from the effective date for the carrier to recognize your coverage. Plan ahead for any necessary prescriptions or care you may require.
2018 Health Insurance Plans1
Enrollment or changes outside of the annual Open Enrollment period are limited. You can cancel coverage for yourself or your dependents at any time. You may be eligible to enroll or make changes within 30 days if you have a qualifying life event noted below:
• retire
• become eligible for Medicare (or your dependent becomes eligible)
• add a dependent due to marriage, domestic partner registration, birth, adoption or placement for adoption
• move outside your plan’s service area
• lose eligibility for coverage, such as conclusion of COBRA or Cal‑COBRA
• lose eligibility for other coverage (or if the employer stops contributing toward your or your dependents’ other coverage), or
• lose eligibility (not due to termination for cause) for Medicaid, Medi‑Cal, Children’s Health Insurance Program (CHIP), Healthy Families Program, or Access for Infants and Mothers Program (you must request enrollment within 60 days)
If you are (or your dependent is) eligible for Medicare and the other is not, you can enroll in separate plans (Medicare and non‑Medicare) with the same carrier.
If you are (or your dependent is) turning 65 in 2018 and will become eligible for Medicare, the SDCERA Health Plans Service Center will send correspondence to your mailing address approximately 90 days prior to your 65th birthday outlining necessary steps to enroll in Medicare and providing information about SDCERA‑sponsored Medicare plans. In the meantime, you may enroll in a non‑Medicare plan through SDCERA.
To enroll in medical and/or dental plans, please visit www.sdcera.org, click on Retiree Health Program and then “Enrollment”, and follow the steps outlined to obtain a copy of the SDCERA Health Insurance Plans Enrollment form. This form is used to process your request, which includes enabling premium deductions to cover the cost of plan premiums and using your address for health zone coverage verification purposes. Please note, enrollment in some of the SDCERA‑sponsored Medicare plans requires a separate carrier‑specific form. More information is available on the Retiree Health Program page. You may submit your form requesting enrollment in an SDCERA‑sponsored plan online or by mailing or faxing your completed form to the SDCERA Health Plans Service Center.
Tier I and Tier II Members: Health Insurance Allowance
The Health Insurance Allowance (HIA) helps offset the cost of premiums for medical, dental and prescription plans. In addition to the allowance, $93.50 may be reimbursed to offset the cost of Medicare Part B. You are eligible for HIA if you are a retired Tier I or Tier II Member who has at least 10 years of SDCERA service credit or is receiving a disability retirement. Monthly allowance amounts range from $200 to $400. The HIA is not a vested SDCERA benefit and is not guaranteed. The allowance may be reduced or discontinued at any time.
To use your HIA towards the cost of a medical, dental and/or prescription plan not sponsored by SDCERA, complete the Health Insurance Allowance Request form. You must enroll in the program each year to be reimbursed.
2
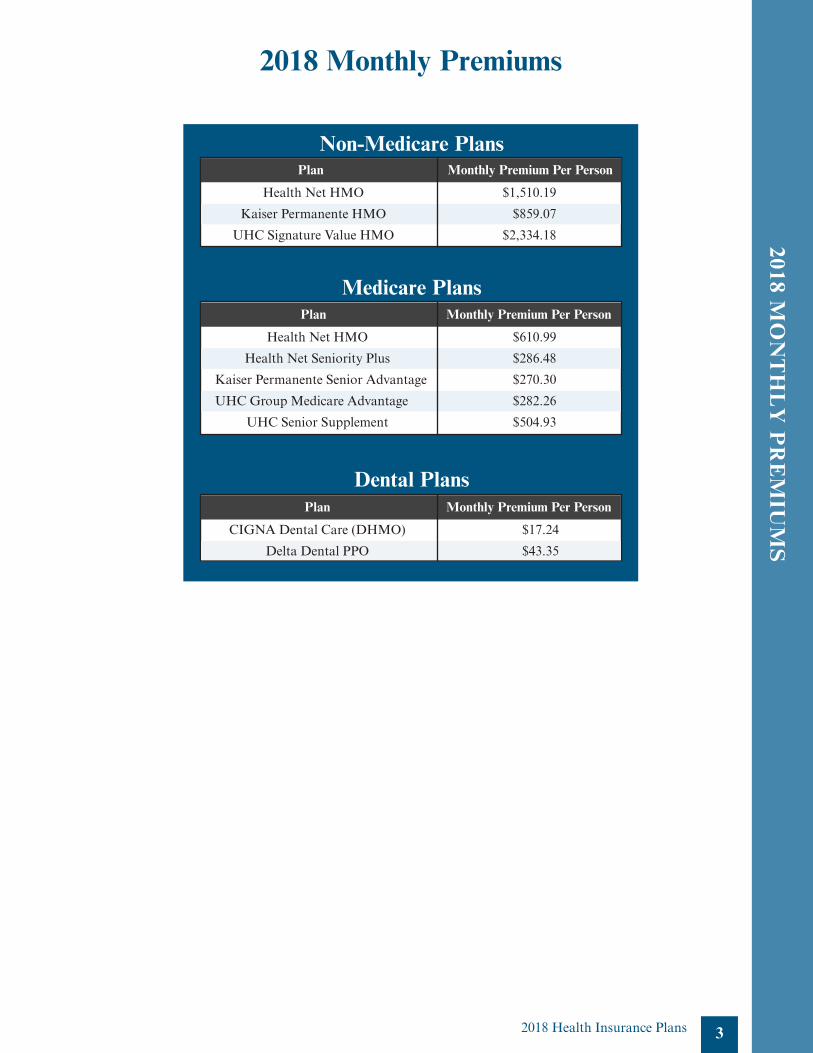
Medical plan coverage details and premiums begin on Page 4 of this booklet. Dental coverage details and premiums are on page 9. The premiums shown for medical and dental plans are per person, per month and do not include an administrative fee of $5.16.
2018 Health Insurance Plans
2018 Health Insurance Plans 3
2018 Monthly Premiums
Plan Monthly Premium Per Person
Health Net HMO $1,510.19
Kaiser Permanente HMO $859.07
UHC Signature Value HMO $2,334.18
Plan Monthly Premium Per Person
Health Net HMO $610.99
Health Net Seniority Plus $286.48
Kaiser Permanente Senior Advantage $270.30
UHC Group Medicare Advantage $282.26
UHC Senior Supplement $504.93
Non-Medicare Plans
Medicare Plans
Plan Monthly Premium Per Person
CIGNA Dental Care (DHMO) $17.24
Delta Dental PPO $43.35
Dental Plans
2018 MO
NT
HL
Y P
RE
MIU
MS
4
NO
N-M
ED
ICA
RE
PL
AN
S G
EN
ER
AL
LY
FO
R T
HO
SE
UN
DE
R 6
5
2018 Health Insurance Plans
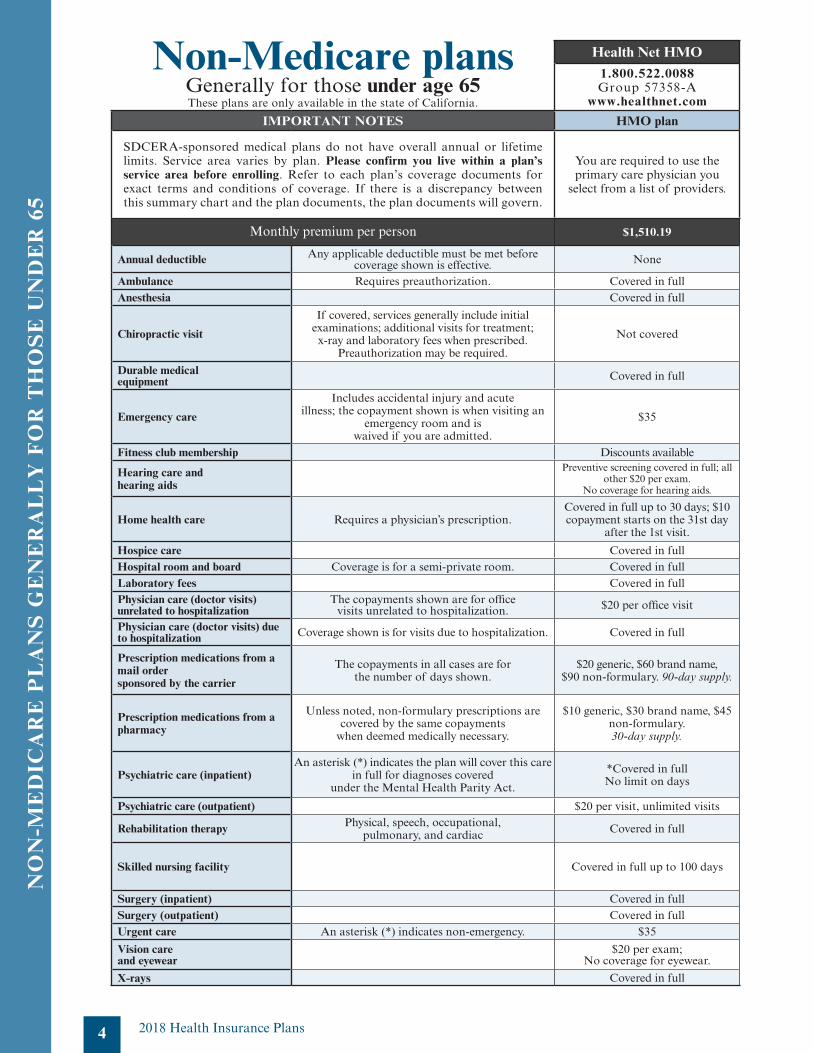
Non-Medicare plansGenerally for those under age 65These plans are only available in the state of California.
Health Net HMO
1.800.522.0088Group 57358‑A
www.healthnet.com
IMPORTANT NOTES HMO plan
SDCERA‑sponsored medical plans do not have overall annual or lifetime limits. Service area varies by plan. Please confirm you live within a plan’s service area before enrolling. Refer to each plan’s coverage documents for exact terms and conditions of coverage. If there is a discrepancy between this summary chart and the plan documents, the plan documents will govern.
You are required to use the primary care physician you
select from a list of providers.
$1,510.19
Annual deductible Any applicable deductible must be met before coverage shown is effective. None
Ambulance Requires preauthorization. Covered in fullAnesthesia Covered in full
Chiropractic visit
If covered, services generally include initial examinations; additional visits for treatment; x‑ray and laboratory fees when prescribed.
Preauthorization may be required.
Not covered
Durable medical equipment Covered in full
Emergency care
Includes accidental injury and acute illness; the copayment shown is when visiting an
emergency room and is waived if you are admitted.
$35
Fitness club membership Discounts available
Hearing care and hearing aids
Preventive screening covered in full; all other $20 per exam.
No coverage for hearing aids.
Home health care Requires a physician’s prescription.Covered in full up to 30 days; $10 copayment starts on the 31st day
after the 1st visit.
Hospice care Covered in fullHospital room and board Coverage is for a semi‑private room. Covered in fullLaboratory fees Covered in fullPhysician care (doctor visits) unrelated to hospitalization
The copayments shown are for office visits unrelated to hospitalization. $20 per office visit
Physician care (doctor visits) due to hospitalization Coverage shown is for visits due to hospitalization. Covered in full
Prescription medications from a mail order sponsored by the carrier
The copayments in all cases are for the number of days shown.
$20 generic, $60 brand name, $90 non‑formulary. 90‑day supply.
Prescription medications from a pharmacy
Unless noted, non‑formulary prescriptions are covered by the same copayments
when deemed medically necessary.
$10 generic, $30 brand name, $45 non‑formulary.30‑day supply.
Psychiatric care (inpatient)An asterisk (*) indicates the plan will cover this care
in full for diagnoses covered under the Mental Health Parity Act.
*Covered in fullNo limit on days
Psychiatric care (outpatient) $20 per visit, unlimited visits
Rehabilitation therapy Physical, speech, occupational, pulmonary, and cardiac Covered in full
Skilled nursing facility Covered in full up to 100 days
Surgery (inpatient) Covered in fullSurgery (outpatient) Covered in fullUrgent care An asterisk (*) indicates non‑emergency. $35
Vision care and eyewear
$20 per exam; No coverage for eyewear.
X-rays Covered in full
Monthly premium per person
2018 Health Insurance Plans
NO
N-M
ED
ICA
RE
PL
AN
S G
EN
ER
AL
LY
FO
R T
HO
SE
UN
DE
R 65
5
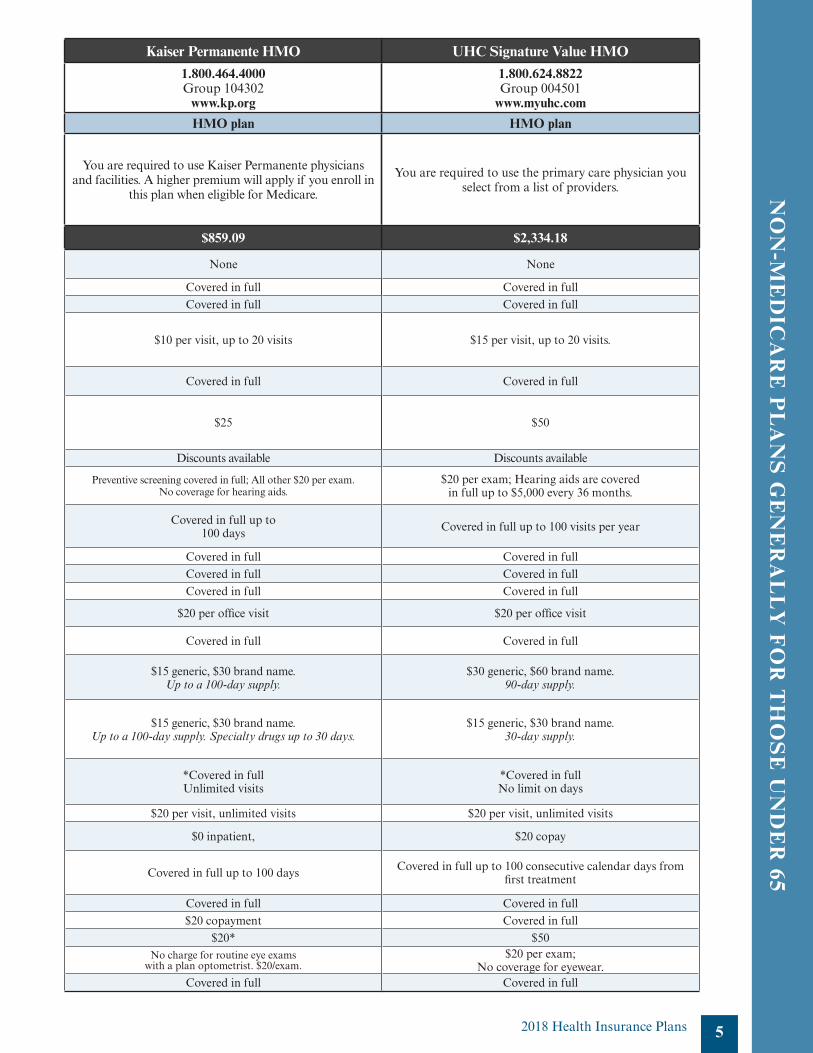
UHC Signature Value HMO1.800.624.8822Group 004501
www.myuhc.com
HMO plan
You are required to use the primary care physician you select from a list of providers.
$2,334.18
None
Covered in fullCovered in full
$15 per visit, up to 20 visits.
Covered in full
$50
Discounts available
$20 per exam; Hearing aids are covered in full up to $5,000 every 36 months.
Covered in full up to 100 visits per year
Covered in fullCovered in fullCovered in full
$20 per office visit
Covered in full
$30 generic, $60 brand name.90‑day supply.
$15 generic, $30 brand name.30‑day supply.
*Covered in fullNo limit on days
$20 per visit, unlimited visits
$20 copay
Covered in full up to 100 consecutive calendar days from first treatment
Covered in fullCovered in full
$50$20 per exam;
No coverage for eyewear.Covered in full
Kaiser Permanente HMO1.800.464.4000Group 104302
www.kp.org
HMO plan
You are required to use Kaiser Permanente physicians and facilities. A higher premium will apply if you enroll in
this plan when eligible for Medicare.
$859.09
None
Covered in fullCovered in full
$10 per visit, up to 20 visits
Covered in full
$25
Discounts available
Preventive screening covered in full; All other $20 per exam. No coverage for hearing aids.
Covered in full up to 100 days
Covered in fullCovered in fullCovered in full
$20 per office visit
Covered in full
$15 generic, $30 brand name. Up to a 100‑day supply.
$15 generic, $30 brand name. Up to a 100‑day supply. Specialty drugs up to 30 days.
*Covered in fullUnlimited visits
$20 per visit, unlimited visits
$0 inpatient,
Covered in full up to 100 days
Covered in full$20 copayment
$20*No charge for routine eye exams
with a plan optometrist. $20/exam.
Covered in full
SDCERA-sponsored Medicare plans
Although you may be enrolled in Medicare Part A and Part B, you may still have medical expenses not covered by Medicare; therefore, enrolling in an additional insurance plan such as an SDCERA‑sponsored medical plan may help pay for expenses that Medicare does not cover.
As long as you are covered by an SDCERA‑sponsored medical plan, you will have the option of joining a Medicare drug plan in the future—without a penalty. SDCERA‑sponsored medical plans meet the Centers for Medicare and Medicaid Services (CMS) creditable coverage guidelines. The Notice of Creditable Coverage on Page 10 of this booklet provides you with the documentation you need to prove that you have had creditable coverage through an SDCERA‑sponsored plan. This notice protects you from penalty charges and allows you to join a Medicare drug plan in the future (if you so decide).
SDCERA offers three types of Medicare health plans for Members covered by Medicare Part A and Part B. SDCERA‑sponsored plans include comprehensive medical coverage as well as the Medicare prescription drug coverage; therefore, if you enroll in an SDCERA‑sponsored plan, your drug coverage will be provided through the SDCERA‑sponsored plan you select. If you enroll in a separate Medicare prescription plan (Part D), you and your dependents will be disenrolled from the SDCERA-sponsored plan.
Medicare Supplement plans allow you to keep your Medicare benefits and use any physician or facility that accepts Medicare.
Medicare HMO plans coordinate their coverage with Medicare. You may also use your Medicare card to obtain services outside
your health plan.
Medicare Advantage plans require your Medicare Part A and Part B to be assigned to a health plan.
Refer to the Medicare Information page on the Retiree Health Program page of www.sdcera.org for more information about the types of Medicare health plans.
If you are eligible for Medicare, but your dependent is not (or if you are not eligible for Medicare and your dependent is), and you both want to enroll in SDCERA‑sponsored plans, you may enroll in separate plans with the same carrier.
You must submit a copy of both sides of your signed Medicare identification card to confirm your eligibility for enrollment in an SDCERA‑sponsored Medicare plan. If you have submitted a copy in the past, you do not need to submit another copy. If you are (or your dependent is) newly enrolled in Medicare Part A and Part B, please submit a copy of the signed card to the SDCERA Health Plans Service Center when you receive it.
If you are (or your dependent is) covered by Medicare Part A only or Medicare Part B only, different premiums may apply. If this situation affects you, contact the SDCERA Retiree Health Program Service Center at 1.866.751.0256 to confirm your monthly premium.
For information about the Medicare program, enrollment deadline or to contact Medicare, visit www.medicare.gov or call 1.800.633.4227.
6
Medicare information for SDCERA-sponsored plans
2018 Health Insurance Plans
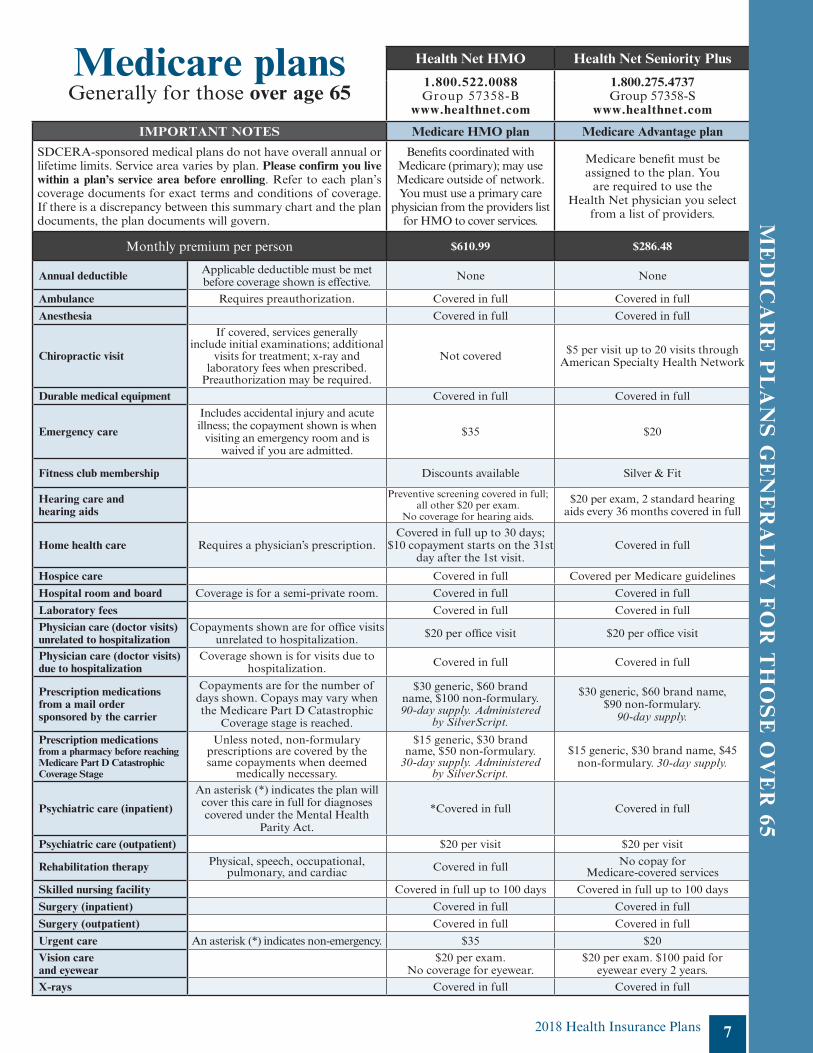
Medicare plansGenerally for those over age 65
Health Net HMO Health Net Seniority Plus Kaiser Permanente Senior Advantage
UHC Group Medicare Advantage UHC Senior Supplement
1.800.522.0088Group 57358‑B
www.healthnet.com
1.800.275.4737Group 57358‑S
www.healthnet.com
Customer service—1.800.457.8506Prospective Member—1.877.714.0178
Group CA: 004497; AZ: 060499; NV: 667201www.uhcretiree.com
Customer service—1.800.851.3802Prospective Member—1.800.698.0822
Group 05408www.uhcretiree.com
1.800.464.4000Group 104302‑00
www.kp.orgIMPORTANT NOTES Medicare HMO plan Medicare Advantage plan Medicare Advantage plan Medicare Advantage plan Medicare Supplement plan
SDCERA‑sponsored medical plans do not have overall annual or lifetime limits. Service area varies by plan. Please confirm you live within a plan’s service area before enrolling. Refer to each plan’s coverage documents for exact terms and conditions of coverage. If there is a discrepancy between this summary chart and the plan documents, the plan documents will govern.
Benefits coordinated with Medicare (primary); may use Medicare outside of network. You must use a primary care
physician from the providers list for HMO to cover services.
Medicare benefit must be assigned to the plan. You
are required to use the Health Net physician you select
from a list of providers.
Medicare benefit must be assigned to the plan, or a higher premium and traditional Kaiser HMO benefits
apply. You are required to use Kaiser Permanente physicians and facilities.
This plan provides coverage in California, Arizona and Nevada. Medicare benefit must be assigned to the plan. You are
required to use the primary care physician you select from a list of providers.
This plan is available nationwide. You may use any physician or facility
that accepts Medicare.
Monthly premium per person $610.99 $286.48 $270.30 $282.26 $504.93
Annual deductible Applicable deductible must be met before coverage shown is effective. None None None None None
Ambulance Requires preauthorization. Covered in full Covered in full Covered in full Covered in full Covered in full. No preauthorization required.
Anesthesia Covered in full Covered in full Covered in full Covered in full Covered in full
Chiropractic visit
If covered, services generally include initial examinations; additional
visits for treatment; x‑ray and laboratory fees when prescribed.
Preauthorization may be required.
Not covered $5 per visit up to 20 visits through American Specialty Health Network $10 per visit, up to 20 visits $5 per visit, up to 20 visits Spinal manipulation covered; $0 per visit.
Other services generally not covered.
Durable medical equipment Covered in full Covered in full Covered in full Covered in full Covered in full
Emergency care
Includes accidental injury and acute illness; the copayment shown is when
visiting an emergency room and is waived if you are admitted.
$35 $20 $20 $20Covered in full in the U.S.;
$250 deductible outside of the U.S.,
20% thereafter.
Fitness club membership Discounts available Silver & Fit Discounts available Silver Sneakers Fitness membership Silver Sneakers Fitness membership
Hearing care and hearing aids
Preventive screening covered in full; all other $20 per exam.
No coverage for hearing aids.
$20 per exam, 2 standard hearing aids every 36 months covered in full
$10 per examNo coverage for hearing aids.
$0 per exam; hearing aids covered up to $500 every 36 months.
Exams covered; $0 per visit for Medicare covered exams. Hearing aids not covered.
Home health care Requires a physician’s prescription.Covered in full up to 30 days;
$10 copayment starts on the 31st day after the 1st visit.
Covered in full Covered in full. Refer to evidence of coverage from the plan. Covered in full Covered in full
Hospice care Covered in full Covered per Medicare guidelines Covered in full Covered per Medicare guidelines Covered in full
Hospital room and board Coverage is for a semi‑private room. Covered in full Covered in full Covered in full Covered in full Covered in full
Laboratory fees Covered in full Covered in full Covered in full Covered in full Covered in full
Physician care (doctor visits) unrelated to hospitalization
Copayments shown are for office visits unrelated to hospitalization. $20 per office visit $20 per office visit $10 per office visit $20 per office visit Covered in full
Physician care (doctor visits) due to hospitalization
Coverage shown is for visits due to hospitalization. Covered in full Covered in full Covered in full Covered in full Covered in full
Prescription medications from a mail order sponsored by the carrier
Copayments are for the number of days shown. Copays may vary when the Medicare Part D Catastrophic
Coverage stage is reached.
$30 generic, $60 brand name, $100 non‑formulary. 90‑day supply. Administered
by SilverScript.
$30 generic, $60 brand name, $90 non‑formulary.
90‑day supply.
$10 generic, $20 brand nameUp to a100‑day supply.
$20 generic, $60 brand name, $60 non‑preferred brand formulary.
90‑day supply.
$20 generic, $70 brand name; $100 non‑preferred brand formulary.
90‑day supply.
Prescription medications from a pharmacy before reaching Medicare Part D Catastrophic Coverage Stage
Unless noted, non‑formulary prescriptions are covered by the same copayments when deemed
medically necessary.
$15 generic, $30 brand name, $50 non‑formulary.
30‑day supply. Administered by SilverScript.
$15 generic, $30 brand name, $45 non‑formulary. 30‑day supply.
$10 generic, $20 brand nameUp to a 100‑day supply.
$10 generic, $30 brand name, $30 non‑preferred brand formulary.
30‑day supply.
$10 generic, $35 brand name; $50 non‑preferred brand formulary.
30‑day supply.
Psychiatric care (inpatient)
An asterisk (*) indicates the plan will cover this care in full for diagnoses covered under the Mental Health
Parity Act.
*Covered in full Covered in full *Covered in fullUnlimited visits
Covered per Medicare guidelines up to 190 days per lifetime Covered in full up to 150 days
Psychiatric care (outpatient) $20 per visit $20 per visit $10 per visit, unlimited visits $20 per visit Covered in full
Rehabilitation therapy Physical, speech, occupational, pulmonary, and cardiac Covered in full No copay for
Medicare‑covered services $0 inpatient; $10 per visit outpatient $0 copay Covered in full
Skilled nursing facility Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days
Surgery (inpatient) Covered in full Covered in full Covered in full Covered in full Covered in full
Surgery (outpatient) Covered in full Covered in full $10 per procedure Covered in full Covered in full
Urgent care An asterisk (*) indicates non‑emergency. $35 $20 $10* $10 copay (in‑ and out‑of‑network) Covered in full
Vision care and eyewear
$20 per exam. No coverage for eyewear.
$20 per exam. $100 paid for eyewear every 2 years.
$10 per exam. $150 allowance for eyewear every 2 years.
$20 per exam.$75 per eyewear every 2 years.
$0 per Medicare‑covered exam. Medicare‑covered eyewear is reimbursed. Non‑Medicare is not covered.
X-rays Covered in full Covered in full Covered in full Covered in full Covered in full
7
ME
DIC
AR
E P
LA
NS
GE
NE
RA
LL
Y F
OR
TH
OS
E O
VE
R 65
2018 Health Insurance Plans
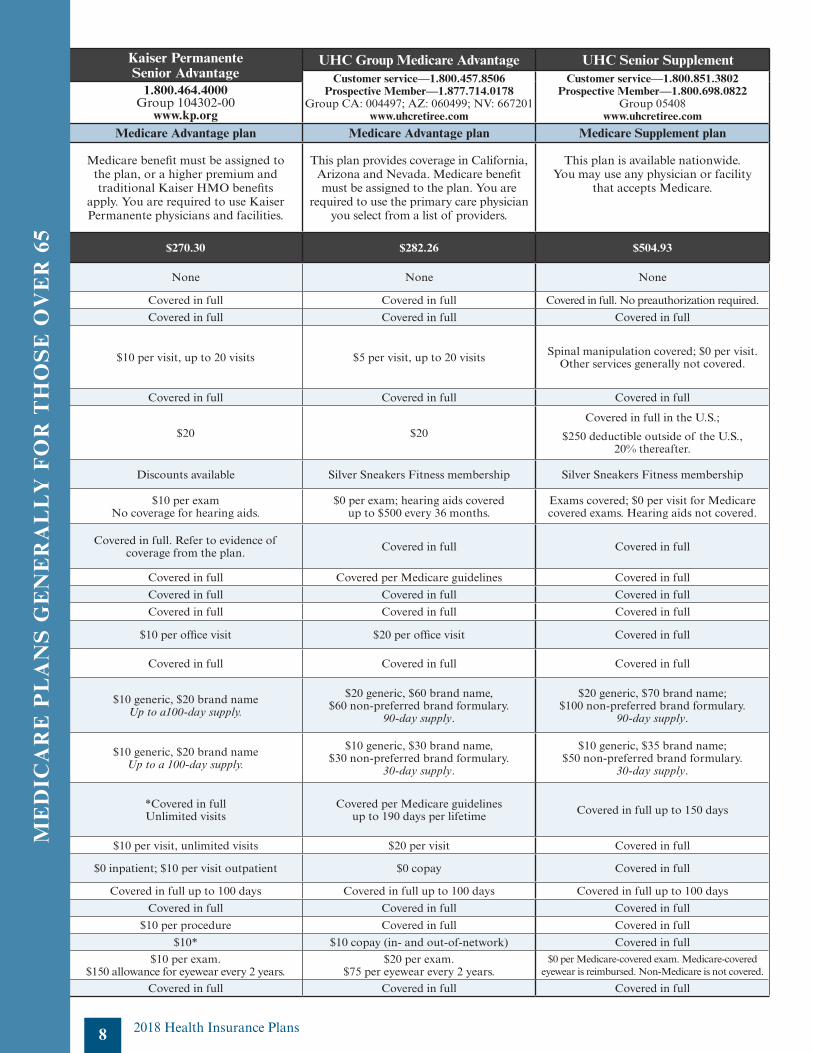
Medicare plansgenerally for those over age 65
Health Net HMO Health Net Seniority Plus Kaiser Permanente Senior Advantage
UHC Group Medicare Advantage UHC Senior Supplement
1.800.522.0088Group 57358‑B
www.healthnet.com
1.800.275.4737Group 57358‑S
www.healthnet.com
Customer service—1.800.457.8506Prospective Member—1.877.714.0178
Group CA: 004497; AZ: 060499; NV: 667201www.uhcretiree.com
Customer service—1.800.851.3802Prospective Member—1.800.698.0822
Group 05408www.uhcretiree.com
1.800.464.4000Group 104302‑00
www.kp.orgIMPORTANT NOTES Medicare HMO plan Medicare Advantage plan Medicare Advantage plan Medicare Advantage plan Medicare Supplement plan
SDCERA‑sponsored medical plans do not have overall annual or lifetime limits. Service area varies by plan. Please confirm you live within a plan’s service area before enrolling. Refer to each plan’s coverage documents for exact terms and conditions of coverage. If there is a discrepancy between this summary chart and the plan documents, the plan documents will govern.
Benefits coordinated with Medicare (primary); may use Medicare outside of network. You must use a primary care
physician from the providers list for HMO to cover services.
Medicare benefit must be assigned to the plan. You
are required to use the Health Net physician you select
from a list of providers.
Medicare benefit must be assigned to the plan, or a higher premium and traditional Kaiser HMO benefits
apply. You are required to use Kaiser Permanente physicians and facilities.
This plan provides coverage in California, Arizona and Nevada. Medicare benefit must be assigned to the plan. You are
required to use the primary care physician you select from a list of providers.
This plan is available nationwide. You may use any physician or facility
that accepts Medicare.
Monthly premium per person* $610.99 $286.48 $270.30 $282.26 $504.93
Annual deductible Applicable deductible must be met before coverage shown is effective. None None None None None
Ambulance Requires preauthorization. Covered in full Covered in full Covered in full Covered in full Covered in full. No preauthorization required.
Anesthesia Covered in full Covered in full Covered in full Covered in full Covered in full
Chiropractic visit
If covered, services generally include initial examinations; additional
visits for treatment; x‑ray and laboratory fees when prescribed.
Preauthorization may be required.
Not covered $5 per visit up to 20 visits through American Specialty Health Network $10 per visit, up to 20 visits $5 per visit, up to 20 visits Spinal manipulation covered; $0 per visit.
Other services generally not covered.
Durable medical equipment Covered in full Covered in full Covered in full Covered in full Covered in full
Emergency care
Includes accidental injury and acute illness; the copayment shown is when
visiting an emergency room and is waived if you are admitted.
$35 $20 $20 $20Covered in full in the U.S.;
$250 deductible outside of the U.S.,
20% thereafter.
Fitness club membership Discounts available Silver & Fit Discounts available Silver Sneakers Fitness membership Silver Sneakers Fitness membership
Hearing care and hearing aids
Preventive screening covered in full; all other $20 per exam.
No coverage for hearing aids.
$20 per exam, 2 standard hearing aids every 36 months covered in full
$10 per examNo coverage for hearing aids.
$0 per exam; hearing aids covered up to $500 every 36 months.
Exams covered; $0 per visit for Medicare covered exams. Hearing aids not covered.
Home health care Requires a physician’s prescription.Covered in full up to 30 days;
$10 copayment starts on the 31st day after the 1st visit.
Covered in full Covered in full. Refer to evidence of coverage from the plan. Covered in full Covered in full
Hospice care Covered in full Covered per Medicare guidelines Covered in full Covered per Medicare guidelines Covered in full
Hospital room and board Coverage is for a semi‑private room. Covered in full Covered in full Covered in full Covered in full Covered in full
Laboratory fees Covered in full Covered in full Covered in full Covered in full Covered in full
Physician care (doctor visits) unrelated to hospitalization
Copayments shown are for office visits unrelated to hospitalization. $20 per office visit $20 per office visit $10 per office visit $20 per office visit Covered in full
Physician care (doctor visits) due to hospitalization
Coverage shown is for visits due to hospitalization. Covered in full Covered in full Covered in full Covered in full Covered in full
Prescription medications from a mail order sponsored by the carrier
Copayments are for the number of days shown. Copays may vary when the Medicare Part D Catastrophic
Coverage stage is reached.
$30 generic, $60 brand name, $100 non‑formulary. 90‑day supply. Administered
by SilverScript.
$30 generic, $60 brand name, $90 non‑formulary.
90‑day supply.
$10 generic, $20 brand nameUp to a100‑day supply.
$20 generic, $60 brand name, $60 non‑preferred brand formulary.
90‑day supply.
$20 generic, $70 brand name; $100 non‑preferred brand formulary.
90‑day supply.
Prescription medications from a pharmacy before reaching Medicare Part D Catastrophic Coverage Stage
Unless noted, non‑formulary prescriptions are covered by the same copayments when deemed
medically necessary.
$15 generic, $30 brand name, $50 non‑formulary.
30‑day supply. Administered by SilverScript.
$15 generic, $30 brand name, $45 non‑formulary. 30‑day supply.
$10 generic, $20 brand nameUp to a 100‑day supply.
$10 generic, $30 brand name, $30 non‑preferred brand formulary.
30‑day supply.
$10 generic, $35 brand name; $50 non‑preferred brand formulary.
30‑day supply.
Psychiatric care (inpatient)
An asterisk (*) indicates the plan will cover this care in full for diagnoses covered under the Mental Health
Parity Act.
*Covered in full Covered in full *Covered in fullUnlimited visits
Covered per Medicare guidelines up to 190 days per lifetime Covered in full up to 150 days
Psychiatric care (outpatient) $20 per visit $20 per visit $10 per visit, unlimited visits $20 per visit Covered in full
Rehabilitation therapy Physical, speech, occupational, pulmonary, and cardiac Covered in full No copay for
Medicare‑covered services $0 inpatient; $10 per visit outpatient $0 copay Covered in full
Skilled nursing facility Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days Covered in full up to 100 days
Surgery (inpatient) Covered in full Covered in full Covered in full Covered in full Covered in full
Surgery (outpatient) Covered in full Covered in full $10 per procedure Covered in full Covered in full
Urgent care An asterisk (*) indicates non‑emergency. $35 $20 $10* $10 copay (in‑ and out‑of‑network) Covered in full
Vision care and eyewear
$20 per exam. No coverage for eyewear.
$20 per exam. $100 paid for eyewear every 2 years.
$10 per exam. $150 allowance for eyewear every 2 years.
$20 per exam.$75 per eyewear every 2 years.
$0 per Medicare‑covered exam. Medicare‑covered eyewear is reimbursed. Non‑Medicare is not covered.
X-rays Covered in full Covered in full Covered in full Covered in full Covered in full
ME
DIC
AR
E P
LA
NS
GE
NE
RA
LL
Y F
OR
TH
OS
E O
VE
R 6
5
8 2018 Health Insurance Plans
2018 Health Insurance Plans
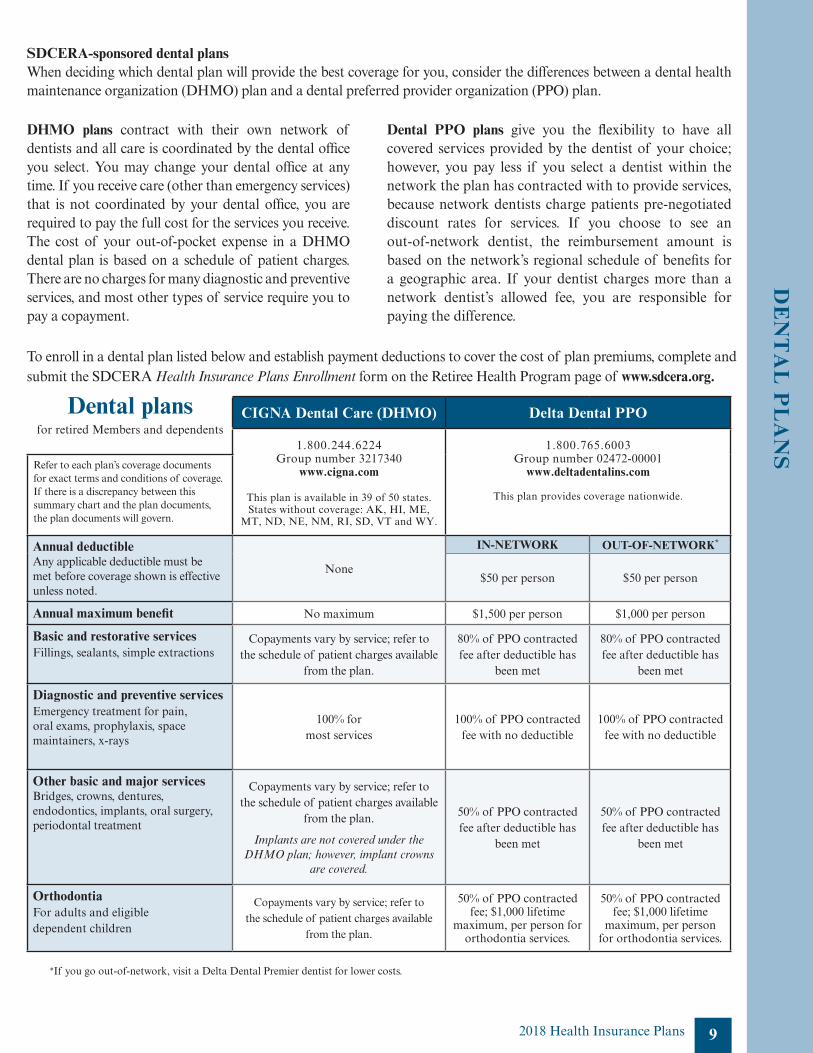
Dental plansfor retired Members and dependents
CIGNA Dental Care (DHMO) Delta Dental PPO
1.800.244.6224Group number 3217340
www.cigna.com
This plan is available in 39 of 50 states. States without coverage: AK, HI, ME,
MT, ND, NE, NM, RI, SD, VT and WY.
1.800.765.6003Group number 02472‑00001
www.deltadentalins.com
This plan provides coverage nationwide.
Refer to each plan’s coverage documents for exact terms and conditions of coverage. If there is a discrepancy between this summary chart and the plan documents, the plan documents will govern.
Annual deductibleAny applicable deductible must be met before coverage shown is effective unless noted.
None
IN-NETWORK OUT-OF-NETWORK*
$50 per person $50 per person
Annual maximum benefit No maximum $1,500 per person $1,000 per person
Basic and restorative servicesFillings, sealants, simple extractions
Copayments vary by service; refer to the schedule of patient charges available
from the plan.
80% of PPO contracted fee after deductible has
been met
80% of PPO contracted fee after deductible has
been met
Diagnostic and preventive servicesEmergency treatment for pain, oral exams, prophylaxis, space maintainers, x‑rays
100% for most services
100% of PPO contracted fee with no deductible
100% of PPO contracted fee with no deductible
Other basic and major servicesBridges, crowns, dentures, endodontics, implants, oral surgery, periodontal treatment
Copayments vary by service; refer to the schedule of patient charges available
from the plan.
Implants are not covered under the DHMO plan; however, implant crowns
are covered.
50% of PPO contracted fee after deductible has
been met
50% of PPO contracted fee after deductible has
been met
OrthodontiaFor adults and eligible dependent children
Copayments vary by service; refer to the schedule of patient charges available
from the plan.
50% of PPO contracted fee; $1,000 lifetime
maximum, per person for orthodontia services.
50% of PPO contracted fee; $1,000 lifetime
maximum, per person for orthodontia services.
SDCERA-sponsored dental plansWhen deciding which dental plan will provide the best coverage for you, consider the differences between a dental health maintenance organization (DHMO) plan and a dental preferred provider organization (PPO) plan.
DHMO plans contract with their own network of dentists and all care is coordinated by the dental office you select. You may change your dental office at any time. If you receive care (other than emergency services) that is not coordinated by your dental office, you are required to pay the full cost for the services you receive. The cost of your out‑of‑pocket expense in a DHMO dental plan is based on a schedule of patient charges. There are no charges for many diagnostic and preventive services, and most other types of service require you to pay a copayment.
Dental PPO plans give you the flexibility to have all covered services provided by the dentist of your choice; however, you pay less if you select a dentist within the network the plan has contracted with to provide services, because network dentists charge patients pre‑negotiated discount rates for services. If you choose to see an out‑of‑network dentist, the reimbursement amount is based on the network’s regional schedule of benefits for a geographic area. If your dentist charges more than a network dentist’s allowed fee, you are responsible for paying the difference.
To enroll in a dental plan listed below and establish payment deductions to cover the cost of plan premiums, complete and submit the SDCERA Health Insurance Plans Enrollment form on the Retiree Health Program page of www.sdcera.org.
9
DE
NT
AL
PL
AN
S
*If you go out‑of‑network, visit a Delta Dental Premier dentist for lower costs.

Notice of Creditable Coverage
Important notice about your prescription drug coverage and MedicareThe prescription drug coverage you have under your SDCERA‑sponsored medical plan for retired Members is expected to pay out, on average, at least as much as the standard Medicare prescription drug coverage will pay.
If you decide to join a Medicare drug plan, your current SDCERA-sponsored medical and prescription drug coverage will end for you and all covered dependents. If you decide to join a Medicare drug plan and drop your current SDCERA‑sponsored coverage, be aware that you and your dependents will be unable to get this coverage back until the next Open Enrollment period.
Members enrolled in an SDCERA‑sponsored prescription drug plan receive notice of creditable coverage annually. You may receive this notice at other times in the future, such as before the next period during which you may enroll in Medicare prescription drug coverage, if SDCERA‑sponsored plan coverage changes, or upon your request.
10 2018 Health Insurance Plans
11
COBRA Continuation Coverage
The Consolidated Omnibus Budget Reconciliation Act (COBRA) provides retired Members,
non‑Member payees, and their dependents who lose SDCERA‑sponsored coverage the
right to continue medical and dental coverage for limited periods of time due to certain
COBRA‑qualifying events.
Electing COBRA coverageIf you are eligible to elect COBRA continuation coverage due to a qualifying event, you have
60 days (from the date of the COBRA election notice or the date you lose coverage, whichever
is later) to elect COBRA continuation coverage.
COBRA Qualifying eventsCOBRA defines a qualifying event as the loss of health plan coverage that is attributable
to death of the Member, divorce, legal separation, annulment or dependent(s) ineligibility
(for instance, your dependent(s) no longer satisfies the requirements for coverage, such as
attainment of age 26).
Each individual who is affected by the qualifying event may independently elect continuation
coverage. This means that if you and your dependents are entitled to elect continuation
coverage, you each may decide separately whether to do so. The covered Member or the
spouse/registered domestic partner is allowed to elect on behalf of any dependent children or
on behalf of all qualified beneficiaries; COBRA coverage is limited to a maximum of 36 months
and the following terms and conditions apply:
• COBRA premiums are calculated based on current monthly medical or dental plan
rates plus a two percent administrative fee.
• You may only continue the coverage that was in effect on the date of the
qualifying event.
• Coverage is extended only to those individuals covered at the time of the
qualifying event.
2018 Health Insurance Plans
12
COBRA participants are subject to the same plan coverage levels and administrative
rules (e.g., adding dependents and changing or canceling coverage) that apply to
non‑COBRA participants.
COBRA is provided subject to your eligibility for coverage under the law and the plan.
SDCERA reserves the right to terminate your continuation coverage retroactively if you
are later determined to be ineligible.
Federal law places responsibility upon the Member or the Member’s eligible dependent(s)
to notify within 60 calendar days of death, divorce, legal separation, annulment or
dependent’s ineligibility. If you or your eligible dependent(s) do not notify the SDCERA
Health Plans Service Center of the qualifying event within the required time frame, you
and your dependents will be ineligible for COBRA. Other forms of notice will not bind
the plan.
COBRA Continuation Coverage (cont.)
You will be ineligible for COBRA coverage if you do not notify the SDCERA
Health Plans Service Center within 60 days of a qualifying event.
2018 Health Insurance Plans
13
SDCERA Retiree Health Program administration credit and fees
SDCERA Retiree Health Program administration feesThe administrative expenses of the health benefit program are paid by each plan participant. The health
benefit program expenses are divided equally among all participants, resulting in a monthly fee per person
for each plan in which they enroll (applicable to both medical and dental plans). This fee is applicable to
SDCERA‑sponsored plans and the Health Insurance Allowance program. The monthly administrative fee is
$5.16 for the 2018 plan year.
Patient Centered Outcomes Research Institute (PCORI)Federal law requires SDCERA to pay the Patient Centered Outcomes Research Institute (PCORI) fee
for each health plan participant. This fee, paid to the Internal Revenue Service (IRS), is intended to
fund a federal research institute that publishes guidelines for improving public health. Tier I and Tier II
members receiving the Health Insurance Allowance or Medicare Part B Reimbursement funds in 2017
will be charged this fee. The federal government determines the current‑year PCORI fee in October.
Once the fee is determined, SDCERA will deduct the fee from your retirement benefit.
Legal notices
2018 Health Insurance Plans
Legal Notices
14
CHIP/Medicaid NoticePremium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you are eligible for health
coverage from your employer, your state may have a premium assistance program that can
help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your
children aren’t eligible for Medicaid or CHIP, you may not be eligible for these premium
assistance programs but you may be able to buy individual insurance coverage through the
Health Insurance Marketplace. For more information, visit www.healthcare.gov.
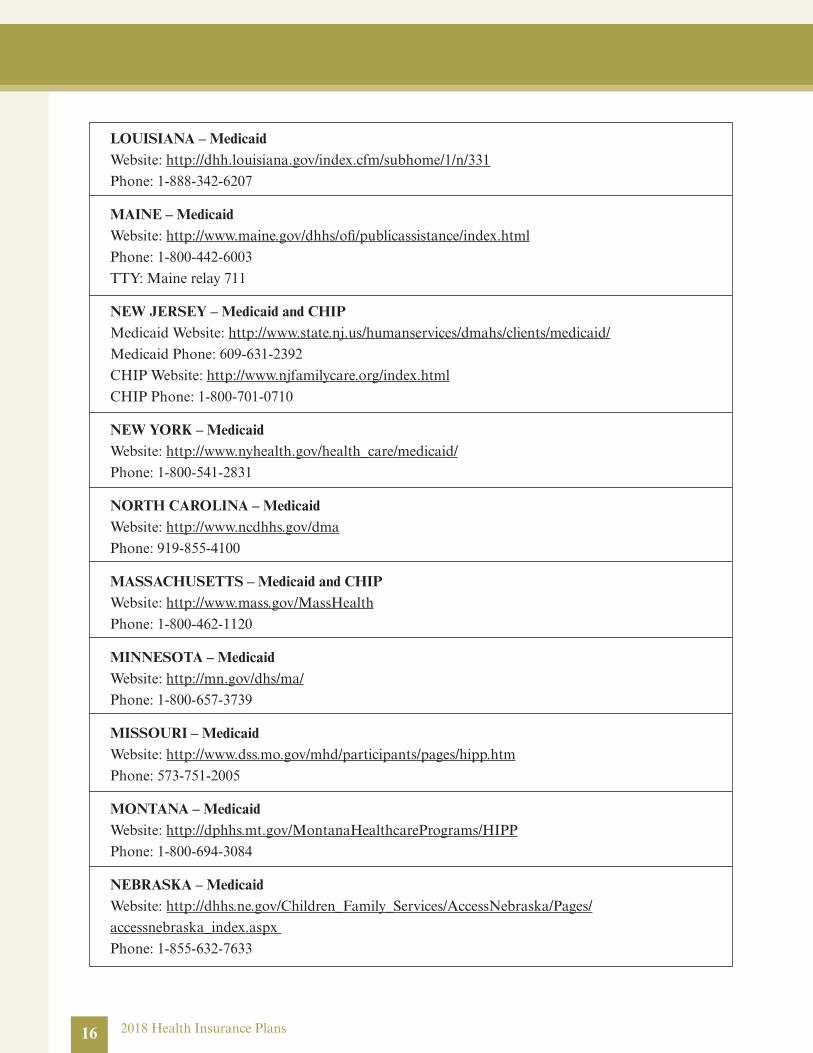
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a
state listed below on pages 15‑18, contact your state Medicaid or CHIP office to find out if
premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think
you or any of your dependents might be eligible for either of these programs, contact your
state Medicaid or CHIP office or dial 1.877.KIDS NOW or www.insurekidsnow.gov. If you
qualify, ask your state if it has a program that might help you pay the premiums for an
employer‑sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP,
as well as eligible under your employer plan, your employer must allow you to enroll in
your employer plan if you aren’t already enrolled. This is called a “special enrollment”
opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the
Department of Labor at www.askebsa.dol.gov or call 1.866.444.EBSA (3272).
2018 Health Insurance Plans
2018 Health Insurance Plans
Medicaid Contact List by State
ALABAMA – MedicaidWebsite: http://myalhipp.com/
Phone: 1‑855‑692‑5447
ALASKA – MedicaidWebsite: http://dhss.alaska.gov/dpa/Pages/medicaid/default.aspx
Phone (Outside of Anchorage): 1‑800‑780‑9972 / Phone (Anchorage): 907‑465‑2680
COLORADO – Medicaid Medicaid Website: http://www.colorado.gov/hcpf
Medicaid Customer Contact Center: 1‑800‑221‑3943
FLORIDA – MedicaidWebsite: http://flmedicaidtplrecovery.com/hipp/
Phone: 1‑877‑357‑3268
GEORGIA – Medicaid Website: http://dch.georgia.gov/medicaid ‑ Click on Health Insurance Premium Payment
(HIPP) Phone: 404‑656‑4507
INDIANA – Medicaid Healthy Indiana Plan for low‑income adults 19‑64 Website: http://www.hip.in.gov
Phone: 1‑877‑438‑4479
All other Medicaid Website: http://www.indianamedicaid.com
Phone 1‑800‑403‑0864
IOWA – Medicaid Website: http://www.dhs.state.ia.us/hipp/
Phone: 1‑888‑346‑9562
KANSAS – MedicaidWebsite: http://www.kdheks.gov/hcf/
Phone: 1‑785‑296‑3512
KENTUCKY – MedicaidWebsite: http://chfs.ky.gov/dms/default.htm
Phone: 1‑800‑635‑2570
15
16 2018 Health Insurance Plans
LOUISIANA – MedicaidWebsite: http://dhh.louisiana.gov/index.cfm/subhome/1/n/331
Phone: 1‑888‑342‑6207
MAINE – MedicaidWebsite: http://www.maine.gov/dhhs/ofi/publicassistance/index.html
Phone: 1‑800‑442‑6003
TTY: Maine relay 711
NEW JERSEY – Medicaid and CHIPMedicaid Website: http://www.state.nj.us/humanservices/dmahs/clients/medicaid/
Medicaid Phone: 609‑631‑2392
CHIP Website: http://www.njfamilycare.org/index.html
CHIP Phone: 1‑800‑701‑0710
NEW YORK – Medicaid Website: http://www.nyhealth.gov/health_care/medicaid/
Phone: 1‑800‑541‑2831
NORTH CAROLINA – Medicaid Website: http://www.ncdhhs.gov/dma
Phone: 919‑855‑4100
MASSACHUSETTS – Medicaid and CHIPWebsite: http://www.mass.gov/MassHealth
Phone: 1‑800‑462‑1120
MINNESOTA – MedicaidWebsite: http://mn.gov/dhs/ma/
Phone: 1‑800‑657‑3739
MISSOURI – MedicaidWebsite: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm
Phone: 573‑751‑2005
MONTANA – MedicaidWebsite: http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP
Phone: 1‑800‑694‑3084
NEBRASKA – MedicaidWebsite: http://dhhs.ne.gov/Children_Family_Services/AccessNebraska/Pages/
accessnebraska_index.aspx
Phone: 1‑855‑632‑7633
2018 Health Insurance Plans 17
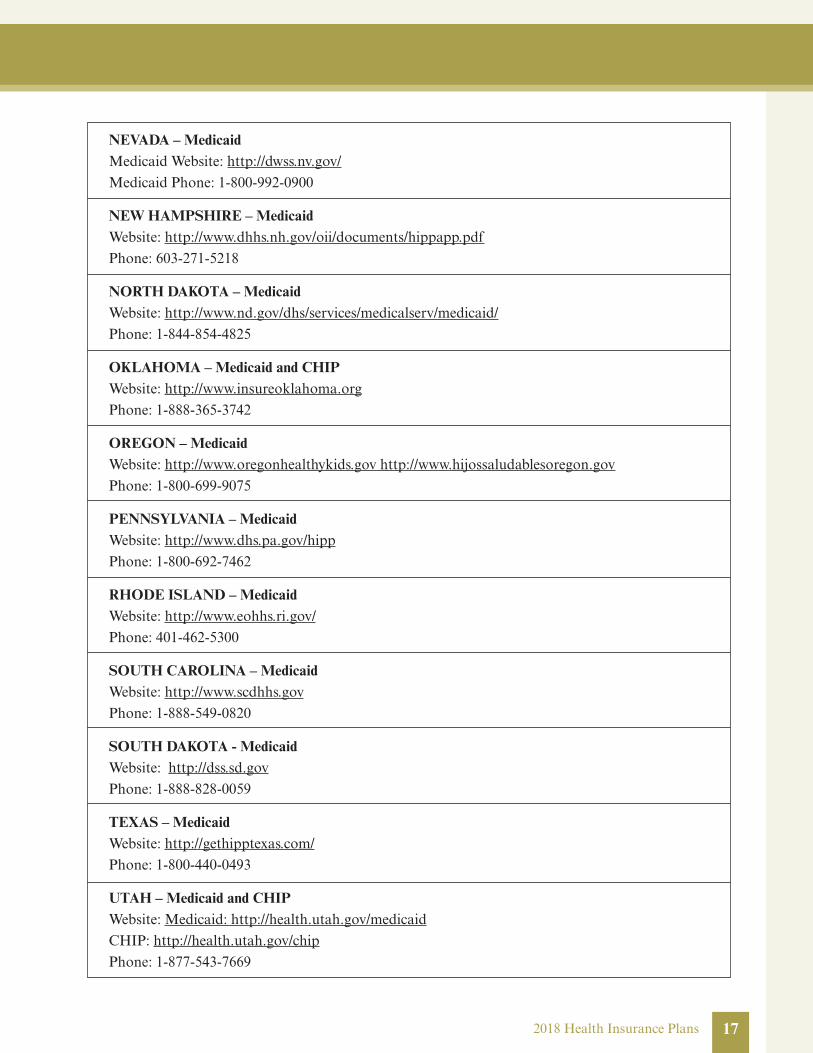
NEVADA – MedicaidMedicaid Website: http://dwss.nv.gov/
Medicaid Phone: 1‑800‑992‑0900
NEW HAMPSHIRE – MedicaidWebsite: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf
Phone: 603‑271‑5218
NORTH DAKOTA – MedicaidWebsite: http://www.nd.gov/dhs/services/medicalserv/medicaid/
Phone: 1‑844‑854‑4825
OKLAHOMA – Medicaid and CHIPWebsite: http://www.insureoklahoma.org
Phone: 1‑888‑365‑3742
OREGON – Medicaid Website: http://www.oregonhealthykids.gov http://www.hijossaludablesoregon.gov
Phone: 1‑800‑699‑9075
PENNSYLVANIA – MedicaidWebsite: http://www.dhs.pa.gov/hipp
Phone: 1‑800‑692‑7462
RHODE ISLAND – MedicaidWebsite: http://www.eohhs.ri.gov/
Phone: 401‑462‑5300
SOUTH CAROLINA – MedicaidWebsite: http://www.scdhhs.gov
Phone: 1‑888‑549‑0820
SOUTH DAKOTA - MedicaidWebsite: http://dss.sd.gov
Phone: 1‑888‑828‑0059
TEXAS – MedicaidWebsite: http://gethipptexas.com/
Phone: 1‑800‑440‑0493
UTAH – Medicaid and CHIPWebsite: Medicaid: http://health.utah.gov/medicaid
CHIP: http://health.utah.gov/chip
Phone: 1‑877‑543‑7669
18 2018 Health Insurance Plans
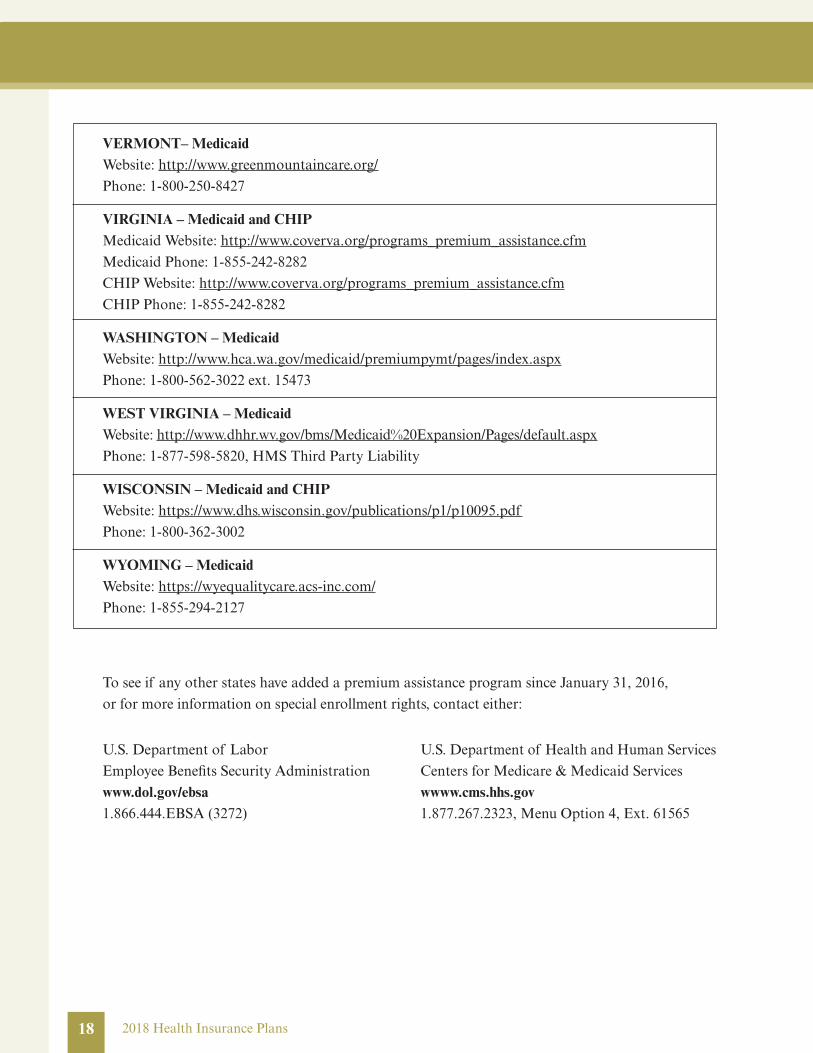
VERMONT– MedicaidWebsite: http://www.greenmountaincare.org/
Phone: 1‑800‑250‑8427
VIRGINIA – Medicaid and CHIPMedicaid Website: http://www.coverva.org/programs_premium_assistance.cfm
Medicaid Phone: 1‑855‑242‑8282
CHIP Website: http://www.coverva.org/programs_premium_assistance.cfm
CHIP Phone: 1‑855‑242‑8282
WASHINGTON – MedicaidWebsite: http://www.hca.wa.gov/medicaid/premiumpymt/pages/index.aspx
Phone: 1‑800‑562‑3022 ext. 15473
WEST VIRGINIA – MedicaidWebsite: http://www.dhhr.wv.gov/bms/Medicaid%20Expansion/Pages/default.aspx
Phone: 1‑877‑598‑5820, HMS Third Party Liability
WISCONSIN – Medicaid and CHIPWebsite: https://www.dhs.wisconsin.gov/publications/p1/p10095.pdf
Phone: 1‑800‑362‑3002
WYOMING – MedicaidWebsite: https://wyequalitycare.acs‑inc.com/
Phone: 1‑855‑294‑2127
To see if any other states have added a premium assistance program since January 31, 2016,
or for more information on special enrollment rights, contact either:
U.S. Department of Labor
Employee Benefits Security Administration
www.dol.gov/ebsa1.866.444.EBSA (3272)
U.S. Department of Health and Human Services
Centers for Medicare & Medicaid Services
wwww.cms.hhs.gov 1.877.267.2323, Menu Option 4, Ext. 61565

Physician Designation Notice
The SDCERA HMO retiree medical plans generally require the designation of a primary
care provider. You have the right to designate any primary care provider who participates in
the health plan’s network and who is available to accept you or your family members. Until
you make this designation, your HMO plan designates one for you. For information on how
to select a primary care provider, and for a list of the participating primary care providers,
contact:
Health Net Non‑Medicare HMO 1.800.522.0088
Health Net Medicare HMO 1.800.275.4737
UHC Non‑Medicare HMO 1.800.624.8822
UHC Medicare HMO 1.800.457.8506
For children, you may designate a pediatrician as the primary care provider. You do not need
prior authorization from Health Net or UHC or from any other person (including a primary
care provider) in order to obtain access to obstetrical or gynecological care from a health
care professional in the health plan’s network who specializes in obstetrics or gynecology.
The health care professional, however, may be required to comply with certain procedures,
including obtaining prior authorization for certain services, following a pre‑approved
treatment plan, or procedures for making referrals. For a list of participating health care
professionals who specialize in obstetrics or gynecology, contact your medical plan provider.
192018 Health Insurance Plans
20
SDCERA-sponsored health insurance plans
Access to SDCERA‑sponsored health insurance plans is not a vested right or guaranteed benefit. The
County Employees Retirement Law of 1937 and the California Public Employees’ Pension Reform
Act of 2013 do not require SDCERA to provide any post‑retirement health insurance plans. The
Board of Retirement annually determines whether to continue the health insurance plans.
Woman’s Health and Cancer Rights Act of 1998
Your (or your dependent’s) health plan will not restrict benefits if you (or your dependent) received
benefits for a mastectomy and elected breast reconstruction in connection with a mastectomy.
Benefits will not be restricted provided the breast reconstruction is performed in a manner determined
in consultation with your (or your dependent’s) physician and may include: (1) reconstruction of the
breast on which the mastectomy was performed, (2) surgery and reconstruction of the other breast to
produce a symmetrical appearance and (3) prostheses and treatment of physical complications for all
stages of mastectomy, including lymphedemas. Benefits for breast reconstruction may be subject to
appropriate annual deductibles and coinsurance provisions that are consistent with those established
for other benefits under the plan.
Medical and dental plan descriptions contained in this booklet
This booklet provides only a summary of the medical and dental plans offered to retired Members
and their eligible dependents. Please refer to each plan’s evidence of coverage documents for exact
terms and conditions of coverage. If there is a discrepancy between this summary and the plan
documents, the plan documents will govern in all cases.
2018 Health Insurance Plans

Strength. Service. Commitment.
SDCERA Retiree Health Program Service CenterPO Box 14464Des Moines, IA 50306‑34641.866.751.0256, Monday ‑ Friday 5:30 a.m. to 6:00 p.m. Pacific Time www.sdcera.org
81508 B11968 (9/17)