Embed Size (px)
Citation preview

www.mghcme.org
Buprenorphine 101
Sarah Wakeman, MD, FASAMMedical Director,
Mass General Substance Use Disorder InitiativeAssistant Professor, Harvard Medical School

www.mghcme.org
Disclosures
Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest
to disclose.
www.mghcme.org
Pharmacology of Treatments
Antagonist(naltrexone)

www.mghcme.org
4
H
������������
����
www.mghcme.org
5
B
�����������
�����������������������������������

www.mghcme.org
6
H
����
B
����������������������������������������������������������

www.mghcme.org
Goal of Medications for Addiction Treatment
Relieve withdrawal symptoms
Block effects of other opioids
Reduce cravings
Restore normal reward pathway

www.mghcme.org
Unique Properties of Buprenorphine Important to Understand for Treatment Initiation
High affinity + partial agonism = potential for….Precipitated withdrawal
www.mghcme.org
9
H
�����������
B
����

www.mghcme.org
Precipitated withdrawal
0
10
20
30
40
50
60
70
80
90
100
No drug Low dose High dose
Full Agonist
Antagonist
Partial Agonist
��� ����������������������������������������������������������� !�"� #$!�����

www.mghcme.org
Starting Buprenorphine
• Must be in mild to moderate withdrawal before taking initial dose
• This can be done in‐office or at home
• Many patients have taken buprenorphine before– patients can be our guide

www.mghcme.org
WHAT’S THE EVIDENCE?

www.mghcme.org
Kakko et al. The Lancet, Volume 361, Issue 9358, 2003, 662 - 668
Buprenorphine Maintenance More Effective than Detox + Counseling
Buprenorphine Maintenance75% retained in treatment75% abstinent by toxicology
Detoxification0% retained in treatment20% died

www.mghcme.org
Relapse Common After Taper
Sigmon et al. JAMA Psychiatry. 2013;70(12):1347‐1354.

www.mghcme.org
Most Patients Achieve Remission
Weiss et al. Drug Alc Depend. 2015;150:112‐9.
www.mghcme.orgHser et al. Addiction. 2016 Apr;111(4):695‐705.
Early Use During Treatment Expected

www.mghcme.org
High level of evidence found to support effectiveness of buprenorphine in improving treatment retention and decreasing illicit opioid use
When dosed appropriately, buprenorphine as effective as methadone in suppressing illicit opioid use, but may not be as effective in treatment retention
Inconclusive evidence on buprenorphine’s impact on non‐opioid drugs
Growing evidence that higher doses (>16mg) are more efficacious than lower doses
Effective for heroin users as well as prescription opioid users
Both buprenorphine and methadone improve pregnancy related outcomes

www.mghcme.orgLing et al. Addiction. 2013 October ; 108(10)
Buprenorphine Effective With or Without Behavioral Treatments
Mean Opioid Use, Withdrawal and Craving Scores by Treatment Condition

www.mghcme.org
Treatment Effective in Primary Care
No difference in self reported opioid use, opioid abstinence, study completion, or cocaine abstinence between the 2 groups
Fiellin DA et al. Am J Med 126:1 2013

www.mghcme.org
No Difference in Retention or Opioid Use for People who Also use Cocaine
Participants Who used Cocaine had: •Reduced self‐reported opioid use from 94% to 27% •6‐month treatment retention of 59%•No significant difference from those who didn’t use cocaine
Cunningham et al. Am J Addict. 2013 Jul‐Aug;22(4):352‐7.

www.mghcme.org
Prior Experience with Non‐Prescribed Buprenorphine Predicts Success

www.mghcme.org
Interim Buprenorphine Improves Outcomes
Sigmon et al. N Engl J Med. 2016 Dec 22;375(25):2504‐2505.

www.mghcme.org
Buprenorphine Implant Non‐inferior
• Responders:– 96.4% receiving
buprenorphine implants – 87.6% receiving sublingual
buprenorphine
• 85.7% receiving implants and 71.9% receiving sublingual maintained opioid abstinence
Rosenthal et al. JAMA. 2016;316(3):282‐290
www.mghcme.org
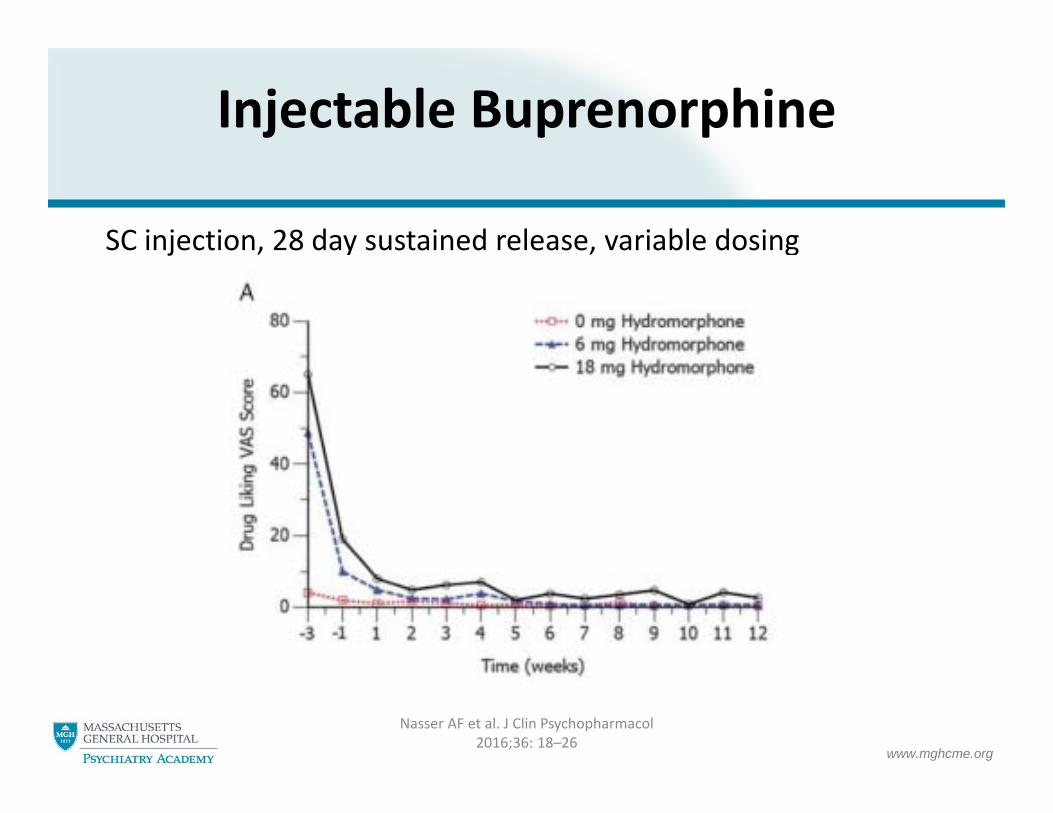
Injectable Buprenorphine
SC injection, 28 day sustained release, variable dosing
Nasser AF et al. J Clin Psychopharmacol2016;36: 18–26

www.mghcme.org
Lack of Access to Treatment
Ann Fam Med 2015;13:23‐26.
www.mghcme.org
The Need for Change
“For nearly a century, physicians were indoctrinated with the societal attitude that [people with addiction] brought upon themselves the suffering they deserve. Even after we began to regard [them] as having a disease, our policies continued to reflect our attitude: [they] are sick, they need help, but they also sin, so do not help them too much. Until the correct mindset is restored in the physician, the mere availability of an effective medication will not make a difference. To put it another way, for buprenorphine to succeed clinically, physicians themselves must first change before they can help patients change their lives.”
Ling. J Neuroimmune Pharmacol (2016) 11:394–400

www.mghcme.org
Rethinking Our Treatment Models






























