Embed Size (px)
Citation preview

25EPOETIN ALFA AND DARBEPOETIN ALFA COSTS BY DOMINANT DOSING INTERVAL IN CHRONIC KIDNEY DISEASE NOT ON DIALYSISRobert Bailey1,Ozgur Tunceli2,Joseph Singer2,Judith Stephenson2, Mekre Senbetta1, Scott McKenzie1 1Centocor Ortho Biotech Services,LLC, Horsham, PA 2HealthCore,Inc, Wilmington, DE To examine epoetin alfa(EPO) and darbepoetin alfa(DARB) treatment patterns and costs in patients with chronic kidney disease not on dialysis(CKD). The HealthCore Integrated Research Database from 1/1/2004-7/31/2009 was used to identify CKD patients treated with EPO or DARB. Patients with cancer, receiving chemotherapy or dialysis were excluded. Drug cost was calculated using January 2010 Wholesale Acquisition Cost. Dominant dosing interval was stratified by <15 or >15 days. 1,660 EPO- and 1,175 DARB-treated CKD patients were identified. Mean (SD) cumulative dose was 300,596 (468,371) units for EPO and 1,205(1,824) mcg for DARB. Dose ratio (EPO units ÷ DARB mcg) was 249:1. DARB was 38% higher in cost compared to EPO. When stratified by dominant dosing intervals of <15 days or >15 days, dose ratios and DARB cost premium were similar between groups and similar to the total population. In CKD, DARB costs were higher compared to EPO in the total population. Observations were similar when stratified by dominant dosing interval.
26PERCUTANEOUS KIDNEY BIOPSIES IN A SOUTHEASTERN TEACHING HOSPITAL: INDICATIONS, BIOCHEMICAL PROFILES, AND RECOVERED HISTOLOGICAL DIAGNOSES. Justin Bain, David Pruett, Lajos Zsom, Albert Dreisbach, T. Fulop. University of Mississippi Medical Center, Jackson, MS. Indications for procedures may evolve over time and display a regional pattern of variation as well. We sought to review our current experience with percutaneous kidney biopsy (PKB) in our institution. We have performed a retrospective data review of PKB obtained via renal trainees over a 3-year period (01/2007 - 12/2009) at the University of Mississippi Medical Center. We collected information on baseline parameters, underlying diagnoses, PKB indications and the recovered diagnoses. Data was analyzed with PAWS Statistics 18 and results expressed as either percents (%) or means with standard deviation (SD). The study was reviewed and approved by the University of Mississippi Human Research Office. Results from 70 PKB (71.4% native, 24.3% deceased donor) were analyzed; main indications for biopsy were impaired renal function in 37 (52.9%) and proteinuria in 33 (47.1%) patients. Baseline Blood Urea Nitrogen was 38 (29.8) mg/dL, creatinine 3.15 (3.09) mg/dL, and random urine protein/creatinine (UPC) ratio 5.85 (7.27). Mean platelet count was 274,770 (101,301)/mm3, PT 10.4 (1.1) sec, PTT 25.9 (3.1) sec. Major recovered histological diagnoses included lupus nephritis (23.5%), focal sclerosis (20.6%), chronic scarring (20.6%), acute tubular necrosis (11.8%), diabetes (7.4%), acute cellular or humoral rejection (7.4%) and membranous nephropathy (4.4%). Diabetes and lupus on biopsy correlated closely with proceeding history (r 0.580 and 0.847; p<0.001 for both). Only 3 specimens returned with “No diagnostic changes”. Thus, in this Southeast cohort of patients, indications for PKB remained vigorous and a large array of significant diagnoses were recovered.
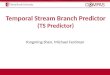
27GDS-15 AS A PREDICTOR OF MORTALITY IN ELDERLY HEMODIALYSIS PATIENTS. Rasheed A Balogun 1, Seki A Balogun2, Alyson L Kepple1, Jennie Ma1, Faruk Turgut 1 Csaba P Kovesdy 1,3 and Emaad M Abdel-Rahman1
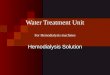
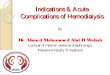
1 Div. of Nephrology, 2 Div. of Gen. Med., Geriatrics & Pallia�ve Care, Dept of Medicine Univ. of Virginia, Charlo�esville, Virginia, USA and3Div. of Nephrology, Salem VA Med. Ctr. Depression is common and ass ociated with increased morbidity and mortality in elderly (≥65yrs) hemodialysis (HD) pa�ents. We recently validated the use of th e 15-item Geriatric Depression scale (GDS-15) as a screening test for depression in elderly HD pa�ents. (Nephron, in press, NKF SCM10). Ques�on: Can GDS-15 assess mortality risk related to depression? Methods: 77 elderly HD pa�ents were divided into 2 groups by results of their GDS-15, Depressed, score ≥ 5: D (n=26), Non-Depressed score ≤ 4: ND (n=51). Outcome is 5-yr survival. Results: (Figure): There is a significant difference in Kaplan-Meier survival (log-rank p=0.042), with 84% increased risk of death for depressed pa�ents (hazard ra�o=1.84, 95% CI (1.01, 3.33)). Median survival �me is 23.15 months with 95% CI (13.02, 46.59)for D, and is 45.18 months with 95% CI (23.38, 66.29) for ND. Conclusion: GDS-15 can be used as a tool to iden�fy elderly HD pa�ents with increased mortality risk related to depression.
Kaplan-Meier survival estimate by GDS
Sur
viva
l Dis
tribu
tion
Func
tion
0.00
0.25
0.50
0.75
1.00
surtime0 10 20 30 40 50 60 70
STRATA: GDS=D Censored GDS=DGDS=ND Censored GDS=ND
28HAZING INDUCED RHABDOMYOLYSIS AND ACUTE KIDNEY INJURY (AKI). Khalid Bashir, Anju Oommen, Alsadek Sultan, Dept. of Medicine, Morehouse School of Medicine, Atlanta, GA, USA; Suhail Akbar, Saghir Ahmed, CGKS, GA, USA. Hazing practices have become increasingly prevalent in schools within fraternities, sororities and athletic teams, as well as in nonacademic settings including the military and street gangs. Hazing is used for an individual to be initiated into an organization. Some of these acts can put the individual at risk for injury. Scant information about renal involvement from hazing is available in the literature. A 19 year old man with no past medical problems presented with complaints of generalized aches, chills, back pain, right hand pain, and urine discoloration after suffering “an accident”. On further questioning, patient stated that he had joined a “membership until fraternity” upon admission to a state college. For the last three months he had been subjected to hazing by receiving 700 to 1000 hard blows to his buttock areas and back with wooden paddles. This was done between hours of 10 pm and 3 am in off-campus secluded wooden areas. Physical examination revealed a well built male, blood pressure of 133/92, temperature of 99.5º F, with extensive bruising on the lower back, both buttocks and upper thighs. Laboratory abnormalities revealed BUN 89 mg/dl, serum creatinine 13.7 mg/dl, calcium 7.8 mg/dl, phosphorus 9.7 mg/dl, magnesium 2.5 mg/dl, CPK 367.3 u/L, aldolase 13.3 u/L, and moderate hematuria. Renal ultrasound showed normal sized kidneys with increased echotexture. Percutaneous renal biopsy revealed 10% focal acute tubular injury with occasional muddy red-brown casts, with no chronicity and no immune complex disease. Patient required intermittent hemodialysis for 8 days with subsequent recovery of renal function. Hazing can cause traumatic rhabdomyolysis and AKI. A common misconception exists among college students (as in our case) that once admitted, the fraternity would do its part to protect the individual from acts including hazing. Thorough education at community grass root level, in addition to utilization of legislation and institutional policies may prevent hazing and its associated severe traumatic injuries.
NKF 2011 Spring Clinical Meetings Abstracts
Am J Kidney Dis. 2011;57(4):A1-A108 A23