Embed Size (px)
Citation preview

Journal of Electromyography and Kinesiology 31 (2016) 96–103
Contents lists available at ScienceDirect
Journal of Electromyography and Kinesiology
journal homepage: www.elsevier .com/ locate/ je lek in
The influence of knee alignment on lower extremity kinetics duringsquats
http://dx.doi.org/10.1016/j.jelekin.2016.10.0041050-6411/� 2016 Elsevier Ltd. All rights reserved.
⇑ Corresponding author at: University of Virginia, 210 Emmet Street South, Suite203, PO Box 400407, Charlottesville, VA 22904, USA.
E-mail address: [email protected] (L.V. Slater).
Lindsay V. Slater MA, CSCS ⇑, Joseph M. Hart PhD, ATCDepartment of Kinesiology, University of Virginia, Charlottesville, VA, USA
a r t i c l e i n f o a b s t r a c t
Article history:Received 18 February 2016Received in revised form 27 September2016Accepted 10 October 2016
Keywords:Knee injuryMovement assessmentKnee valgusBiomechanics
The squat is an assessment of lower extremity alignment during movement, however there is little infor-mation regarding altered joint kinetics during poorly performed squats. The purpose of this study was toexamine changes in joint kinetics and power from altered knee alignment during a squat. Thirty partic-ipants completed squats while displacing the knee medially, anteriorly, and with neutral alignment (con-trol). Sagittal and frontal plane torques at the ankle, knee, and hip were altered in the descending andascending phase of the squat in both the medial and anterior malaligned squat compared to the controlsquat. Ankle and trunk power increased and hip power decreased in the medial malaligned squat com-pared to the control squat. Ankle, knee, and trunk power increased and hip power decreased in the ante-rior malaligned squat compared to the control squat. Changes in joint torques and power duringmalaligned squats suggest that altered knee alignment increases ankle and trunk involvement to executethe movement. Increased anterior knee excursion during squatting may also lead to persistent alteredloading of the ankle and knee. Sports medicine professionals using the squat for quadriceps strengtheningmust consider knee alignment to reduce ankle and trunk involvement during the movement.
� 2016 Elsevier Ltd. All rights reserved.
1. Introduction
Sports medicine and performance professionals commonly usethe squat exercise as a quadriceps strengthening exercise. Squatsare also used to visually evaluate knee alignment during move-ment in a bilateral stance (Kritz et al., 2009; Noda andVerscheure, 2009) because it requires mobility and stability atthe ankle, knee, hip, and trunk for optimal performance (Cooket al., 2014). Performance on a squat assessment is also predictiveof performance on an entire movement screen (Clifton et al., 2015),indicating that the bilateral squat may be appropriate to identifyindividuals who may be at increased risk of injury. Despite thegrowing popularity of the use of bilateral squat assessment, thereis little information regarding changes in lower extremity kineticsduring commonly observed technique deviations.
Two commonly observed technique deviations during squatperformance include excessive medial and anterior knee displace-ment (Kritz et al., 2009). Medial knee displacement has been asso-ciated with altered lower extremity muscle activation patterns(Padua et al., 2012; Slater and Hart, in press), however little is
known about the consequences of increased anterior knee dis-placement. Some have noted increased trunk motion and flexiontorque at the hip when anterior knee displacement is restrictedduring squatting (Fry et al., 2003; List et al., 2013), however thereis no current literature examining the way the lower extremity andtrunk attenuates the ground reaction forces with excessive kneeexcursion. Changes in joint power absorption have been notedbetween soft and stiff landings, indicating that knee position alterslower extremity force attenuation (Devita and Skelly, 1992).Increased anterior or medial knee displacement may result inaltered lower extremity joint kinetics and increased involvementof distal and proximal joints to execute the squat movement.
Changes in lower extremity alignment during bilateral squatsare also important given the potential for increased patellofemoralcontact forces during squatting (von Eisenhart-Rothe et al., 2004;Besier et al., 2005; Mesfar and Shirazi-adl, 2005; Trepczynskiet al., 2012). Previous researchers have noted decreased quadricepsactivation and increased gastrocnemii activation with medial kneedisplacement during bilateral squats (Padua et al., 2012). Theincreased gastrocnemii activation stabilizes the ankle during peakknee flexion and decreases strain at the anterior cruciate ligament(Hsu et al., 1993; Kvist and Gillquist, 2001; Morgan et al., 2014),which may indicate an unstable knee position with altered lowerextremity alignment. Although lower extremity muscle activation

L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103 97
patterns change from altered knee alignments, little attention hasbeen given to changes in joint torque and power distribution. Cur-rent literature suggests that changes in knee alignment duringweighted squats decreases internal knee extension torque andincreases internal hip extension torque at peak knee flexion, sup-porting that varying knee alignments may increase proximal jointcontribution (Fry et al., 2003). There is no current study, however,identifying changes in lower extremity joint torque and power dis-tribution over the entire squat cycle during a bilateral bodyweightsquat. Understanding the way the lower extremity attenuatesground reaction forces with excessive knee excursion is importantto appreciate the consequences and behavior of surrounding jointsduring the movement. Furthermore, a better understanding oflower extremity torque and power distribution with altered kneealignments during the squat will provide clinicians an evidencebased approach when evaluating the bilateral squat assessment,similar to the single leg squat and landings (Hewett et al., 2005;Crossley et al., 2011). Therefore, the purpose of this study was tocompare changes in joint torque and joint power resulting fromaltered knee alignment during a bilateral squat. We hypothesizedthat medial and anterior knee displacement would increase lowerextremity torques and joint power in the ankle and trunk duringboth the descending and ascending phase of the squats comparedto a control squat.
2. Methods
2.1. Design
A descriptive, repeated measures laboratory design was used tocompare three different squat techniques. The independent vari-able in this study was squat technique (control, anterior mala-ligned, and medial malaligned). The dependent variablesincluded lower extremity joint moments and lower extremityand trunk joint power from 0% to 100% of the squat cycle.
2.2. Subjects
Thirty healthy, recreationally active subjects (19 females, 11males, 21.4 ± 3 years, 170.9 ± 8.8 cm, 66.5 ± 11.9 kg) without self-reported history of lower extremity injury within the past6 months and no surgical history volunteered. All subjects pro-vided informed consent prior to participating. Study methods wereapproved by the university’s institutional review board for healthscience research.
2.3. Instrumentation
Kinematic data were collected using an electromagnetic motionanalysis system (Ascension Technology Corporation, Burlington,VT) and sampled at 144 Hz, which has been used previously insquat research (Padua et al., 2012; Slater and Hart, in press) andprovides accurate and reliable three-dimensional movement ofbody segments (Milne et al., 1996). Ground reaction forces werecollected using a single forceplate (Bertec, Columbus, OH) and sam-pled at 1000 Hz. Mass-normalized internal joint moments and jointpowers were calculated using MotionMonitor software (InnovativeSports Training, Chicago, IL) (Houck et al., 2007). All data were syn-chronized and exported using MotionMonitor software.
2.4. Procedures
Subjects reported to the laboratory for a single session wearingathletic shoes and athletic clothing. Electromagnetic sensors wereplaced bilaterally on the dorsum, midshank, and midthigh, the
sacrum and T2. Bony landmarks were digitized using the endpointof a stylus with a fixed electromagnetic sensor. Digitized bonylandmarks included left and right anterior superior iliac spines,medial and lateral malleoli, medial and lateral knee joint lines,and L5/S1, T12/L1, C7/T1. Left and right anterior superior iliacspines of the pelvis were digitized to determine the hip joint centerof rotation using the Bell method (Bell et al., 1989). Medial and lat-eral malleoli and knee joint lines were digitized to determine theankle and knee joint centers. Spinal landmarks were defined asthe digitized space between the associated processes (Blackburnand Padua, 2009).
Subjects placed the dominant foot within a single force plateembedded in the floor and the contralateral foot outside of theforce plate (Escamilla et al., 2009a,b). The dominant leg wasdefined as the preferred kicking leg (Brophy et al., 2010). The sub-ject practiced bilateral squats to parallel to become accustomed tothe wires from the electromagnetic motion capture system. Thesubject stood with feet shoulder width apart, toes pointing forwardand performed 5 trials of 3 different squat techniques in the fol-lowing order: A squat with knees intentionally malaligned in thefrontal plane (medial malaligned), a squat with the knees inten-tionally malaligned in the sagittal plane (anterior malaligned),and a squat with the knees in line with the feet (control). Subjectswere instructed to squat in a slow, controlled manner, until thighswere parallel with the floor for all 3 squat conditions. Feedback onknee alignment and squat performance was only given during thecontrol squat and included the following statements: Sit back atyour heels like you’re sitting in a chair; push your knees out inthe bottom of the squat; keep your toes pointing forward (Slaterand Hart, in press). The order of the squats was predetermined tolimit feedback during squat performance until malaligned squatswere completed.
2.5. Data processing and statistical analyses
Kinematic and kinetic data were filtered using a zero-lagfourth-order Butterworth filter at 14.5 Hz then synchronized andreduced to 50 points from full knee extension to peak knee flexionand 50 points from peak knee flexion returning to full knee exten-sion. Combining these two phases represents 100% of the squatcycle so that 50% represents peak knee flexion and 0% and 99% rep-resent full knee extension (Robertson et al., 2008; Padua et al.,2012). Descending phase of the squat cycle was defined as 0–49%and ascending phase of the squat cycle was defined as 50–99%.Internal joint moments were calculated using inverse dynamics.Sagittal and frontal internal joint moments and net joint powersfor the dominant limb were calculated using inverse dynamics inMotionMonitor software (Houck et al., 2007) and were mass nor-malized. Negative joint powers were interpreted as power absorp-tion while positive joint powers were interpreted as powergeneration (Williams et al., 2012; Nagano et al., 2015). Meansand 90% confidence intervals were calculated for each squat tech-nique. Areas in which confidence intervals did not overlap for threeor more consecutive percentage points were considered statisti-cally significant (Drewes et al., 2009; Kuenze et al., 2014). Cohen’sd effect sizes were calculated using mean differences and associ-ated pooled standard deviations during periods of the squat cyclewhen squat techniques (malaligned and control condition) weresignificantly different.
3. Results
Anterior and lateral knee displacement relative to the startingposition (full knee extension) during the different squat techniquesare shown in Fig. 1.

Fig. 1. Peak knee excursion during medial, anterior, and control squats from full knee extension.
98 L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103
3.1. Internal joint moments
3.1.1. Medial malaligned squatThe medial malaligned squat significantly increased internal
ankle plantarflexion moment from 9% to 99% of the squat cyclecompared to the control squat (Fig. 2). Internal knee extensionmoment decreased in the medial malaligned squat from 89% to99% of the squat cycle compared to the control squat (Fig. 2). Inter-nal hip extension moment decreased in the medial malalignedsquat from 45% to 52% of the squat cycle and increased 89–94%of the squat cycle compared to the control squat. The medialmalaligned squat increased internal ankle eversion moment from19–40% and 52–60% of the squat cycle and decreased internalankle eversion moment from 88% to 99% of the squat cycle com-pared to the control squat (Fig. 2). Internal knee adduction moment
Fig. 2. Differences in joint moments during the medial malaligned squat (grey line), antecycle with 90% confidence intervals. Areas in which confidence intervals did not overlainternal moments were mass normalized.
increased in the medial malaligned squat from 5% to 99% of thesquat cycle compared to the control squat (Fig. 2). Internal hipabduction increased in the medial malaligned squat from 29% to71% and decreased from 83% to 99% of the squat cycle comparedto the control squat (Fig. 2). Effect sizes were large for all differ-ences during the squat cycle (Fig. 3).
3.1.2. Anterior malaligned squatThe anterior malaligned squat significantly increased internal
ankle plantarflexion moment from 2% to 99% of the squat cyclecompared to the control squat (Fig. 2). Internal knee extensionmoment decreased from 9% to 25% and 74–99% of the squat cycleand increased from 33% to 66% of the squat cycle compared to thecontrol squat (Fig. 2). Internal hip extension moment decreased inthe anterior malaligned squat from 19% to 70% of the squat cycle
rior malaligned squat (vertical lines), and control squat (black line) across the squatp for three or more consecutive points were considered statistically significant. All
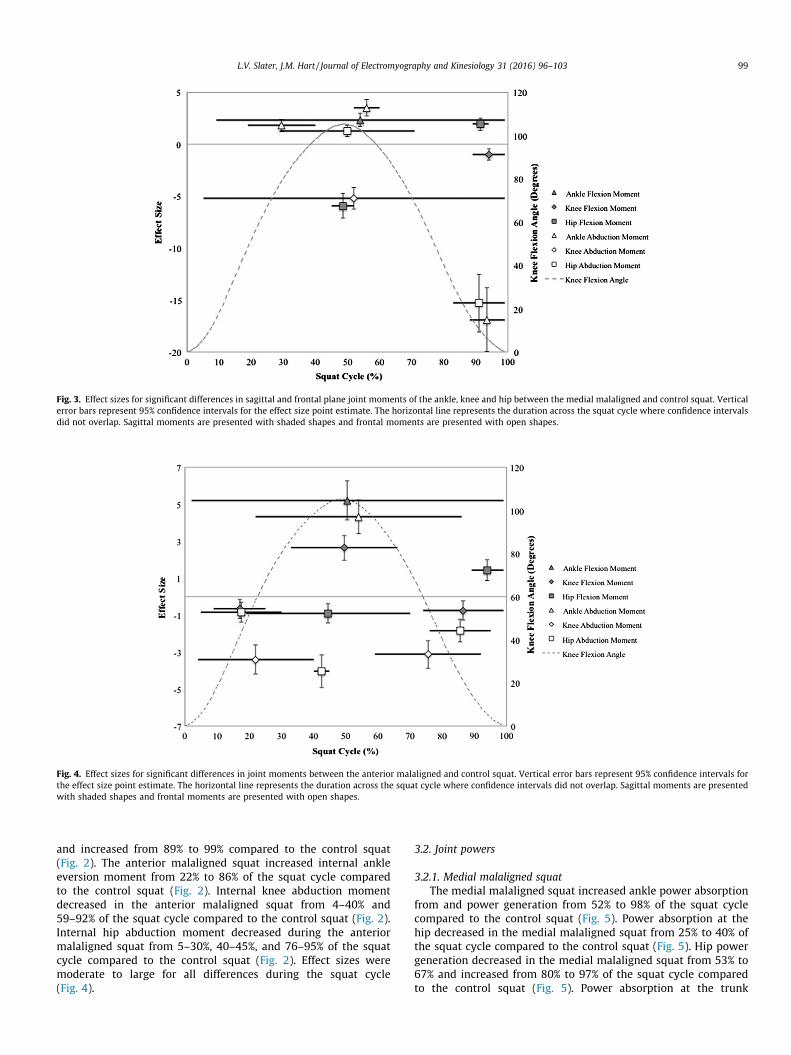
Fig. 3. Effect sizes for significant differences in sagittal and frontal plane joint moments of the ankle, knee and hip between the medial malaligned and control squat. Verticalerror bars represent 95% confidence intervals for the effect size point estimate. The horizontal line represents the duration across the squat cycle where confidence intervalsdid not overlap. Sagittal moments are presented with shaded shapes and frontal moments are presented with open shapes.
Fig. 4. Effect sizes for significant differences in joint moments between the anterior malaligned and control squat. Vertical error bars represent 95% confidence intervals forthe effect size point estimate. The horizontal line represents the duration across the squat cycle where confidence intervals did not overlap. Sagittal moments are presentedwith shaded shapes and frontal moments are presented with open shapes.
L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103 99
and increased from 89% to 99% compared to the control squat(Fig. 2). The anterior malaligned squat increased internal ankleeversion moment from 22% to 86% of the squat cycle comparedto the control squat (Fig. 2). Internal knee abduction momentdecreased in the anterior malaligned squat from 4–40% and59–92% of the squat cycle compared to the control squat (Fig. 2).Internal hip abduction moment decreased during the anteriormalaligned squat from 5–30%, 40–45%, and 76–95% of the squatcycle compared to the control squat (Fig. 2). Effect sizes weremoderate to large for all differences during the squat cycle(Fig. 4).
3.2. Joint powers
3.2.1. Medial malaligned squatThe medial malaligned squat increased ankle power absorption
from and power generation from 52% to 98% of the squat cyclecompared to the control squat (Fig. 5). Power absorption at thehip decreased in the medial malaligned squat from 25% to 40% ofthe squat cycle compared to the control squat (Fig. 5). Hip powergeneration decreased in the medial malaligned squat from 53% to67% and increased from 80% to 97% of the squat cycle comparedto the control squat (Fig. 5). Power absorption at the trunk

MEDIAL MALALIGNED ANTERIOR MALALIGNED
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0 10 20 30 40 50 60 70 80 90
Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0 10 20 30 40 50 60 70 80 90
Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
ANKLE
KNEE
-1.5
-1
-0.5
0
0.5
1
1.5
2
0 10 20 30 40 50 60 70 80 90
Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
-1.5
-1
-0.5
0
0.5
1
1.5
2
0 10 20 30 40 50 60 70 80 90 Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
-1.5
-1
-0.5
0
0.5
1
1.5
2
0 10 20 30 40 50 60 70 80 90 Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
-1.5
-1
-0.5
0
0.5
1
1.5
2
0 10 20 30 40 50 60 70 80 90 Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
HIP
TRUNK
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0 10 20 30 40 50 60 70 80 90
Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0 10 20 30 40 50 60 70 80 90
Pow
er (W
/kg)
Squat Cycle (%)
Ascending Phase Descending Phase
Fig. 5. Net joint powers during the medial malaligned squat (grey line), anterior malaligned squat (vertical lines), and control squat (black line) across the squat cycle with90% confidence intervals. Areas in which confidence intervals did not overlap for three or more consecutive points were considered statistically significant. The horizontal axisrepresents 100% of the squat cycle, with 50% representing peak knee flexion and 0% and 99% representing full extension. The vertical axis represents mass normalized netjoint power.
100 L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103
increased in the medial malaligned squat from 25% to 31% andpower generated at the trunk increased 73–90% of the squat cyclecompared to the control squat (Fig. 5). Effect sizes were moderateto large for all differences during the squat cycle (Fig. 6).
3.2.2. Anterior malaligned squatThe anterior malaligned squat increased ankle power absorp-
tion from 8–26% and 88–99% of the squat cycle compared to thecontrol squat (Fig. 5). Ankle power generation increased in theanterior malaligned squat from 52% to 86% of the squat cycle com-pared to the control squat (Fig. 5). Power absorbed at the kneedecreased in the anterior malaligned squat from 8% to 24% andpower generated at the knee decreased from 77% to 99% of the
squat cycle compared to the control squat (Fig. 5). Knee power gen-eration increased in the anterior malaligned squat from 54% to 70%of the squat cycle (Fig. 5). Power absorbed at the hip decreased inthe anterior malaligned squat from 12% to 32% of the squat cycleand power generated at the hip decreased from 66% to 73% ofthe squat cycle compared to the control squat (Fig. 5). Power gen-erated at the hip increased in the anterior malaligned squat from83% to 99% of the squat cycle compared to the control squat(Fig. 5). Power absorbed at the trunk increased in the anteriormalaligned squat from 14% to 25% and decreased from 31% to44% of the squat cycle compared to the control squat (Fig. 5). Powergenerated at the trunk decreased from 52% to 59% and increasedfrom 75% to 86% of the squat cycle compared to the control squat

Fig. 6. Effect sizes for significant differences in joint powers between the medial malaligned and control squat. Vertical error bars represent 95% confidence intervals for theeffect size point estimate. The horizontal line represents the duration across the squat cycle where confidence intervals did not overlap.
Fig. 7. Effect sizes for significant differences in joint powers between the anterior malaligned and control squat. Vertical error bars represent 95% confidence intervals for theeffect size point estimate. The horizontal line represents the duration across the squat cycle where confidence intervals did not overlap.
L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103 101
(Fig. 5). Effect sizes were moderate to large for all differences dur-ing the squat cycle (Fig. 7).
4. Discussion
The purpose of this study was to examine changes in joint tor-que and power resulting from medial and anterior knee displace-ment during a bilateral squat. The results of this study indicatethat sagittal and frontal plane knee alignment influences lowerextremity joint moments and powers during a squat exercise.Medial knee excursion increased internal plantarflexion torque,ankle eversion torque, knee adduction torque, and hip abductiontorque while decreasing knee and hip extension torque. Medialknee excursion also increased ankle and trunk joint power anddecreased joint power at the hip. Increased anterior knee excursion
increased internal plantarflexion torque and ankle eversion torqueand decreased knee and hip abduction torques. Anterior kneeexcursion also increased ankle joint power and decreased hip jointpower compared to a control squat. When knee joint powerdecreased with anterior knee displacement, trunk joint powerincreased and when knee joint power increased, trunk jointpower decreased.
Increased knee excursion during squatting increased ankle con-tribution to the movement. Both medial and anterior knee excur-sion increased internal plantarflexion moment and ankle jointpower. Although subjects with dynamic knee valgus often displaydecreased dorsiflexion range of motion (Bell et al., 2008), theseassessments are often completed in unilateral stance or with min-imal knee flexion, such as the single leg squat. Previous researchers(Padua et al., 2012; Slater and Hart, in press) investigating bilateralsquats have noted increased gastrocnemii activation during squats

102 L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103
with medial knee displacement, supporting increased ankle contri-bution with knee malalignment. This increased gastrocnemii acti-vation during flexed knee stance may be an effort to decreaseanterior tibial translation and stabilize the lower extremity (Hsuet al., 1993; Kvist and Gillquist, 2001,; Morgan et al., 2014). Alter-natively, knee malalignments during squats may be due to gastroc-nemii tightness (Bell et al., 2012). Furthermore, ankle joint powerabsorption and generation increased during both malaligned squatconditions compared to the control condition. Similar increases inankle power absorption have been noted during gait when movingfrom a rearfoot to forefoot strike (Williams et al., 2012). Thisincreased power absorption during malaligned squats may bedue to the altered center of pressure location at the foot. Changesin knee alignment move center of pressure towards the forefootduring the squat (Koh et al., 2015) increasing the moment arm tothe ankle and increasing internal plantarflexion torque (Fig. 2)and power absorption (Fig. 5) at the ankle. Malaligned squatsmay be a consequence of poor knee extensor strength, displacingjoint torque and power absorption to the ankle joint.
Along with increased ankle contribution, knee malalignmentsalso increased trunk contribution to the squat movement. Restrict-ing anterior knee displacement during a bilateral squat mayincrease shear forces at the trunk from the vertical trunk positionmaintained throughout the squat cycle (Fry et al., 2003; Listet al., 2013), however the results of this study suggest that toomuch anterior displacement of the knee may be disadvantageous.The anterior malaligned squat increased joint power absorptionat the ankle and trunk while decreasing the power absorption atthe knee and hip. The decreased knee and hip joint power duringsquats with knee excursion may be the result of decreased quadri-ceps activation (Padua et al., 2012; Slater and Hart, in press), caus-ing an increase in joint power production at the trunk. This trade-off between knee and trunk joint power is particularly evident dur-ing the anterior malaligned squat; as knee joint power decreases,trunk joint power increases (Fig. 5). Although these changes inpower distribution are small, the difference in malaligned and con-trol squat trunk power had very large effect sizes (Figs. 6 and 7).This supports that the change in distribution of joint power altersthe nature of the squat from a primarily quadriceps dominantexercise (Isear et al., 1997; Escamilla et al., 1998; Caterisanoet al., 2002; Dionisio et al., 2008) to increased trunk contributionto execute the movement (Escamilla et al., 2001; Dionisio et al.,2008).
Sports medicine professionals may need to consider the poten-tial for excessive loading on the knee joint with knee excursion inthe sagittal or frontal plane. The increased internal knee extensionmoment coupled with increased knee joint power generation nearpeak knee flexion with anterior knee excursion may lead toincreased patellofemoral contact forces (Mesfar and Shirazi-adl,2005; Shalhoub and Maletsky, 2014; van den Tillaar et al., 2014).Patellofemoral forces are highest around 90–100 degrees of kneeflexion (Escamilla et al., 2009a,b; Fekete et al., 2014), when hipand trunk power decreased while ankle and knee power increasedin the anterior malaligned squat compared to the control squat.These kinetic changes are similar to those seen in individuals withpatellofemoral pain syndrome with abnormal patellar tracking(Powers, 1999; Fulkerson, 2002). Furthermore, increased Q-anglehas been associated with a more laterally shifted patella resultingin increased contact forces during knee flexion (Huberti and Hayes,1984; Mizuno et al., 2001), which suggests that frontal planemalalignments increases contact forces at the knee. Althoughrestricting anterior displacement may increase forces at the trunk,the results of this study suggest that sagittal plane malalignmentduring closed chain exercise may also increase knee contact forces(Mesfar and Shirazi-adl, 2005; Trepczynski et al., 2012; Shalhouband Maletsky, 2014). Furthermore, commonly observed technique
deviations in during a common exercise may lead to persistentaltered loading of the ankle and knee. Persistent altered loadingpatterns during squatting may result in similar cartilaginousdegeneration (Lee et al., 2001) seen with altered gait kinematicsin people with osteoarthritis (Andriacchi et al., 2009). Futureresearch should continue to explore the consequences of anteriorknee excursion in order to establish safe guidelines for anteriorknee displacement during squatting.
Some limitations were present in the current study. The sub-jects in this study purposefully collapsed their knees mediallyand anteriorly while squatting, however the findings in this studyagree with previous researchers who have noted increased anklecontribution during passive medial knee displacement (Paduaet al., 2012). Knee flexion angle and squat velocity were also notstandardized in the current study, however all participantsreceived the same instructions which best simulates the way thesquat would be taught in a clinic or gym (Czaprowski et al.,2012). Furthermore, subjects likely used the same timing for eachsquat. Although squat velocity was not standardized, the descend-ing and ascending phases of the squat were reduced to 50 points tostandardize the squat cycle based on kinematic events. Center ofpressure was also not reported in the current study. Changes incenter of pressure, such as anterior displacement during anteriormalaligned squats, would result in an increased moment armand torque at the ankle joint. Future research regarding lowerextremity alignment during the squat should consider changes incenter of pressure to better interpret changes in joint torques.
5. Conclusion
The results of the study support that excessive knee excursionin the frontal and sagittal planes alters joint moments, powerabsorption, and power generation in the lower extremity andtrunk. The increased ankle and trunk joint power during mala-ligned squatting indicates that increased sagittal and frontal planeknee excursion during squats may change the nature of the exer-cise from a predominantly knee and hip strengthening exerciseto distal and proximal contribution to execute the movement.Sports medicine professionals using the bilateral squat for quadri-ceps strengthening must consider knee alignment to reduce ankleand trunk involvement during the movement.
Funding
There was no funding source for this paper.
Conflict of interest
The authors declare that they have no conflict of interest.
References
Andriacchi, T.P., Koo, S., Scanlan, S.F., 2009. Gait mechanics influence healthycartilage morphology and osteoarthritis of the knee. J. Bone Joint Surg. Am. 91(Suppl. 1), 95–101.
Bell, A.L., Pedersen, D.R., Brand, R.A., 1989. Prediction of hip joint center locationfrom external landmarks. Hum. Movement Sci. 8 (1), 3–16.
Bell, D.R., Padua, D.A., Clark, M.A., 2008. Muscle strength and flexibilitycharacteristics of people displaying excessive medial knee displacement. Arch.Phys. Med. Rehabil. 89 (7), 1323–1328.
Bell, D.R., Vesci, B.J., DiStefano, L.J., Guskiewicz, K.M., Hirth, C.J., Padua, D., 2012.Muscle activity and flexibility in individuals with medial knee displacementduring the overhead squat. Athletic Train. Sports Health Care 4 (3), 117–125.
Besier, T.F., Draper, C.E., Gold, G.E., Beaupre, G.S., Delp, S.L., 2005. Patellofemoraljoint contact area increases with knee flexion and weight-bearing. J. Orthop.Res. 23, 345–350.
Blackburn, J.T., Padua, D.A., 2009. Sagittal-plane trunk position, landing forces, andquadriceps electromyographic activity. J. Athl. Train. 44 (2), 174–179.

L.V. Slater, J.M. Hart / Journal of Electromyography and Kinesiology 31 (2016) 96–103 103
Brophy, R., Jacinda Silvers, H., Gonzales, T., Mandelbaum, B.R., 2010. Genderinfluences: the role of leg dominance in ACL injury among soccer players. Br. J.Sports Med. 44, 694–697.
Caterisano, A., Moss, R.F., Pellinger, T.K., Woodruff, K., Lewis, V.C., Booth, W., Khadra,T., 2002. The effect of back squat depth on the EMG activity of 4 superficial hipand thigh muscles. J. Strength Cond. Res. 16 (3), 428–432.
Clifton, D.R., Grooms, D.R., Onate, J.A., 2015. Overhead deep squat performancepredicts functional movement screen score. Int. J. Sports Phys. Ther. 10 (5), 622–627.
Cook, G., Burton, L., Hoogenboom, B.J., Voight, M., 2014. Functional movementscreening: the use of fundamental movements as an assessment of function –Part 1. Int. J. Sports Phys. Ther. 9 (3), 396–409.
Crossley, K.M., Zhang, W.-J., Schache, A.G., Bryant, A., Cowan, S.M., 2011.Performance on the single-leg squat task indicates hip abductor musclefunction. Am. J. Sports Med. 39 (4), 866–873.
Czaprowski, D., Biernat, R., Kendra, A., 2012. Squat - rules of performing and mostcommon mistakes. Polish J. Sport Tourism 19 (1), 3–12.
Devita, P., Skelly, W.A., 1992. Effect of landing stiffness on joint kinetics andenergetics in the lower extremity. Med. Sci. Sport Exer. 24 (1), 108–115.
Dionisio, V.C., Almeida, G.L., Duarte, M., Hirata, R.P., 2008. Kinematic, kinetic, andEMG patterns during downward squatting. J. Electromyogr. Kinesiol. 18 (1),134–143.
Drewes, L.K., McKeon, P.O., Paolini, G., Riley, P., Kerrigan, D.C., Ingersoll, C.D., Hertel,J., 2009. Altered ankle kinematics and shank-rear-foot coupling in those withchronic ankle instability. J. Sport Rehab. 18 (3), 375–388.
Escamilla, R.F., Fleisig, G.S., Lowry, T.M., Barrentine, S.W., Andrews, J.R., 2001. Athree-dimensional biomechanical analysis of the squat during varying stancewidths. Med. Sci. Sports Exerc. 33 (6), 984–998.
Escamilla, R.F., Fleisig, G.S., Zheng, N., Barrentine, S.W., Wilk, K.E., Andrews, J.R.,1998. Biomechanics of the knee during closed kinetic chain and open kineticchain exercises. Med. Sci. Sports Exerc. 30 (4), 556–569.
Escamilla, R.F., Zheng, N., Imamura, R., Macleod, T.D., Edwards, W.B., Hreljac, A.,Fleisig, G.S., Wilk, K.E., Moorman 3rd, C.T., Andrews, J.R., 2009a. Cruciateligament force during the wall squat and the one-leg squat. Med. Sci. SportsExerc. 41 (2), 408–417.
Escamilla, R.F., Zheng, N., Macleod, T.D., Edwards, W.B., Imamura, R., Hreljac, A.,Fleisig, G.S., Wilk, K.E., Moorman 3rd, C.T., Andrews, J.R., 2009b. Patellofemoraljoint force and stress during the wall squat and one-leg squat. Med. Sci. SportsExerc. 41 (4), 879–888.
Fekete, G., Csizmadia, B.M., Wahab, M.A., De Baets, P., Vanegas-Useche, L.V., Biro, I.,2014. Patellofemoral model of the knee joint under non-standard squatting.Dyna 81 (183), 60–67.
Fry, A.C., Smith, C., Schilling, B.K., 2003. Effect of knee position on hip and kneetorques during the barbell squat. J. Strength Cond. Res. 17 (4), 629–633.
Fulkerson, J.P., 2002. Diagnosis and treatment of patients with patellofemoral pain.Am. J. Sports Med. 30 (3), 447–456.
Hewett, T.E., Myer, G.D., Ford, K.R., Heidt, R.S.J., Colosimo, A.J., McLean, S.G., van denBogert, A.J., Paterno, M.V., Succop, P., 2005. Biomechanical measures ofneuromuscular control and valgus loading of the knee predict anteriorcruciate ligament injury risk in female athletes. Am. J. Sports Med. 33 (4),492–501.
Houck, J.R., De Haven, K.E., Maloney, M., 2007. Influence of anticipation onmovement patterns in subjects with ACL deficiency classified as noncopers. J.Orthop. Sports Phys. Ther. 37 (2), 56–64.
Hsu, A.-T., Perry, J., Gronley, J.K., Hislop, H.J., 1993. Quadriceps force and myoelectricactivity during flexed knee stance. Clin. Orthop. Relat. Res. 288, 254–262.
Huberti, H.H., Hayes, W.C., 1984. Patellofemoral contact pressures. The influence ofq-angle and tendofemoral contact. J. Bone Joint Surg. Am. 66 (5), 715–724.
Isear Jr., J.A., Erickson, J.C., Worrell, T.W., 1997. EMG analysis of lower extremitymuscle recruitment patterns during an unloaded squat. Med. Sci. Sports Exerc.29 (4), 532–539.
Koh, D.H., Lee, J.D., Kim, K., 2015. Plantar pressures in individuals with normal andpronated feet according to static squat depths. J. Phys. Ther. Sci. 27 (9), 2833–2835.
Kritz, M., Cronin, J., Hume, P., 2009. The bodyweight squat: a movement screen forthe squat pattern. Strength Condition. J. 31 (1), 76–85.
Kuenze, C., Hertel, J., Weltman, A., Diduch, D.R., Saliba, S., Hart, J.M., 2014. Joggingbiomechanics after exercise in Individuals with ACL-reconstructed knees. Med.Sci. Sport Exer. 46 (6), 1067–1076.
Kvist, J., Gillquist, J., 2001. Sagittal plane knee translation and electromyographicactivity during closed and open kinetic chain exercises in anterior cruciateligament-deficient patients and control subjects. Am. J. Sports Med. 29 (1), 72–82.
Lee, T.Q., Yang, B.Y., Sandusky, M.D., McMahon, P.J., 2001. The effects of tibialrotation on the patellofemoral joint: assessment of the changes in situ strain inthe peripatellar retinaculum and the patellofemoral contact pressures andareas. J. Rehabil. Res. Dev. 38 (5), 463–469.
List, R., Gulay, T., Stoop, M., Lorenzetti, S., 2013. Kinematics of the trunk and thelower extremities during restricted and unrestricted squats. J. Strength Cond.Res. 27 (6), 1529–1538.
Mesfar, W., Shirazi-Adl, A., 2005. Biomechanics of the knee joint in flexion undervarious quadriceps forces. Knee 12, 424–434.
Milne, A.D., Chess, D.G., Johnson, J.A., King, G.J., 1996. Accuracy of anelectromagnetic tracking device: a study of the optimal range and metalinterference. J. Biomech. 29 (6), 791–793.
Mizuno, Y., Kumagai, M., Mattessich, S.M., Elias, J.J., Ramrattan, N., Cosgarea, A.J.,Chao, E.Y.S., 2001. Q-angle influences tibiofemoral and patellofemoralkinematics. J. Orthop. Res. 19 (5), 834–840.
Morgan, K.D., Donnelly, C.J., Reinbolt, J.A., 2014. Elevated gastrocnemius forcescompensate for decreased hamstrings forces during the weight-acceptancephase of a single-leg jump landing: implications for anterior cruciate ligamentinjury rink. J. Biomech. 47 (13), 3295–3302.
Nagano, H., Tatsumi, I., Sarashina, E., Sparrow, W.A., Begg, R.K., 2015. Modellingknee flexion effects on joint power absorption and adduction moment. Knee 22(6), 490–493.
Noda, T., Verscheure, S., 2009. Individual goniometric measurements correlatedwith observations of the deep overhead squat. Athletic Train. Sports Health Care1 (3), 114–119.
Padua, D.A., Bell, D.R., Clark, M.A., 2012. Neuromuscular characteristics ofindividuals displaying excessive medial knee displacement. J. Athl. Train. 47(5), 525–536.
Powers, C.M., 1999. The influence of altered lower-extremity kinematics onpatellofemoral joint dysfunction: a theoretical perspective. J. Orthop. SportsPhys. Ther. 33 (11), 639–646.
Robertson, D.G., Wilson, J.M., St Pierre, T.A., 2008. Lower extremity muscle functionsduring full squats. J. Appl. Biomech. 24 (4), 333–339.
Shalhoub, S., Maletsky, L.P., 2014. Variation in patellofemoral kinematics due tochanges in quadriceps loading configuration during in vitro testing. J. Biomech.47 (1), 130–136.
Slater, L.V., Hart, J.M., in press. Muscle activation patterns during different squattechniques. J. Strength Cond. Res. (in press).
Trepczynski, A., Kutzner, I., Kornaropoulos, E., Taylor, W.R., Duda, G.N., Bergmann,G., Heller, M.O., 2012. Patellofemoral joint contact forces during activities withhigh knee flexion. J. Orthop. Res. 30 (3), 408–415.
van den Tillaar, R., Anderson, V., Saeterbakken, A.H., 2014. Comparison of muscleactivation and performance during 6 RM, two-legged free-weight squats.Kinesiol. Slovenica 20 (2), 5–16.
von Eisenhart-Rothe, R., Siebert, M., Bringmann, C., Vogl, T., Englmeier, K.H.,Graichen, H., 2004. A new in vivo technique for determination of 3D kinematicsand contact areas of the patello-femoral and tibio-femoral joint. J. Biomech. 37(6), 927–934.
Williams III, D.S.B., Green, D.H., Wurzinger, B., 2012. Changes in lower extremitymovement and power absorption during forefoot striking and barefoot running.Int. J. Sports Phys. Ther. 7 (5), 525–532.
Lindsay V. Slater is a doctoral candidate at theUniversity of Virginia in Sports Medicine inthe Department of Kinesiology. Her research focuses onthe neuromuscular adaptations to high-intensityexercise after knee injury.
Joseph M. Hart is an Associate Professor of Kinesiologyat the University of Virginia. He is also the Director ofClinical Research for Orthopaedic Surgery. His researchfocus is neuromuscular consequences of joint injury, inparticular neuromuscular factors that contribute to theprogression of osteoarthritis following ACL reconstruc-tion.





























