Embed Size (px)
Citation preview

C. Theda, MD - final version shown in Vienna 1
33rdrd International Neonatal International Neonatal Brain Monitoring ConferenceBrain Monitoring ConferenceVienna, AustriaVienna, AustriaPlatform Presentation: January 18Platform Presentation: January 18thth, 2008., 2008.
AmplitudeAmplitude--Integrated EEG Monitoring Integrated EEG Monitoring in Patients with Metabolic Disordersin Patients with Metabolic DisordersC. Theda (1,2), C AygC. Theda (1,2), C Aygüün (3), M Toet (4), D Azzopardi (5), M n (3), M Toet (4), D Azzopardi (5), M DiFazio (6), A Hamosh (1), L DeVries (4), L HellstromDiFazio (6), A Hamosh (1), L DeVries (4), L Hellstrom--Westas Westas (7) and E Shany (8)(7) and E Shany (8)(1)(1) Johns Hopkins University School of Medicine, Baltimore, MarylandJohns Hopkins University School of Medicine, Baltimore, Maryland, USA;, USA;(2)(2) Frederick Memorial Hospital, Frederick, Maryland, USA;Frederick Memorial Hospital, Frederick, Maryland, USA;(3)(3) Ondokuz Mayis University, Samsun, Turkey;Ondokuz Mayis University, Samsun, Turkey;(4)(4) Wilhelmina ChildrenWilhelmina Children’’s Hospital, Utrecht, The Netherlands;s Hospital, Utrecht, The Netherlands;(5)(5) Imperial College, London, United Kingdom;Imperial College, London, United Kingdom;(6)(6) Uniformed Services University of the Health Sciences, Bethesda, Uniformed Services University of the Health Sciences, Bethesda, MD, USA;MD, USA;(7)(7) Uppsala University, Uppsala, Sweden;Uppsala University, Uppsala, Sweden;(8)(8) BenBen--Gurion University of the Negev, BeerGurion University of the Negev, Beer--Sheva, Israel.Sheva, Israel.
What is the role of amplitudeWhat is the role of amplitude--integrated integrated Electroencephalography (aEEG) in Electroencephalography (aEEG) in patients with metabolic disorders?patients with metabolic disorders?
Metabolic disorders with ENCEPHALOPATHY:Metabolic disorders with ENCEPHALOPATHY:•• diagnose/confirmdiagnose/confirm the encephalopathy the encephalopathy
through detection of its EEG correlatethrough detection of its EEG correlate•• assess assess severityseverity of the encephalopathyof the encephalopathy•• evaluate changes in the severity and evaluate changes in the severity and
characteristics of the encephalopathy characteristics of the encephalopathy over time over time (with or without treatment)(with or without treatment)

C. Theda, MD - final version shown in Vienna 2
For metabolic disorders with SEIZURES:For metabolic disorders with SEIZURES:•• detect detect seizure activity (with or without seizure activity (with or without
clinical correlates)clinical correlates)•• assess seizure assess seizure frequencyfrequency•• assess assess response to treatment response to treatment (or lack (or lack
thereofthereof……))
What is the role of amplitudeWhat is the role of amplitude--integrated integrated Electroencephalography (aEEG) in Electroencephalography (aEEG) in patients with metabolic disorders?patients with metabolic disorders?
In addition aEEG may have a role in In addition aEEG may have a role in nonnon--metabolic genetic disorders:metabolic genetic disorders:
Patients with nonPatients with non--metabolic genetic metabolic genetic conditions often experience seizures:conditions often experience seizures:
oo Search of POSSUM (a computer based Search of POSSUM (a computer based system that allows search for genetic system that allows search for genetic syndromes by traits) reveals:syndromes by traits) reveals:
oo 588 syndromes with 588 syndromes with ““seizures of any typeseizures of any type””
oo including 376 syndromes with including 376 syndromes with ““abnormal nervous system structureabnormal nervous system structure””

C. Theda, MD - final version shown in Vienna 3
Previous Previous published reportspublished reports of aEEG use of aEEG use in patients with metabolic disordersin patients with metabolic disorders
WhatWhat’’s known about aEEG in s known about aEEG in metabolic disorders:metabolic disorders:
Request for collaboration made after a Request for collaboration made after a presentation at last years presentation at last years 22ndnd Neonatal Neonatal Brain Monitoring Conference in FloridaBrain Monitoring Conference in Florida(Glycine encephalopathy: Characteristics of (Glycine encephalopathy: Characteristics of amplitudeamplitude--integrated EEG tracing in a patient with integrated EEG tracing in a patient with early symptoms of disease)early symptoms of disease)
Background of this presentation:Background of this presentation:
9 Contributors from 9 Contributors from six Countries!six Countries!
23 aEEG 23 aEEG tracings tracings submittedsubmitted
Countries in alphabetical orderCountries in alphabetical order
over 12 different diagnosesover 12 different diagnoses

C. Theda, MD - final version shown in Vienna 4
Metabolic conditions with several Metabolic conditions with several patient tracings available:patient tracings available:
Glycine encephalopathy (GE/NKH)Glycine encephalopathy (GE/NKH)(non(non--ketotic hyperglycinemia) ketotic hyperglycinemia) n=4n=4Inborn error of glycine degradationInborn error of glycine degradationleading to accumulation of large leading to accumulation of large quantities of glycine in all body tissues quantities of glycine in all body tissues
Glycine is a neurotransmitter with part Glycine is a neurotransmitter with part inhibitory and part excitatory effectsinhibitory and part excitatory effects
Typical EEG changes are seen in this patient:Typical EEG changes are seen in this patient:burst suppression like patternburst suppression like pattern characterized by characterized by high voltage complexes separated by low high voltage complexes separated by low amplitude sequences amplitude sequences –– short interburst intervalsshort interburst intervals
GE/NKH Patient 1GE/NKH Patient 1

C. Theda, MD - final version shown in Vienna 5
This patient with a This patient with a similar aEEG tracingsimilar aEEG tracing –– again again short interburst interval.short interburst interval.Note appearance of tracing at time of Note appearance of tracing at time of hiccups hiccups (which are typically seen in patients with GE/NKH).(which are typically seen in patients with GE/NKH).
GE/NKH Patient 2GE/NKH Patient 2
This patient also with This patient also with similar aEEG tracingsimilar aEEG tracing but but baseline not as suppressed: baseline not as suppressed: 32.5% of individual 32.5% of individual EEG segments analyzed do not show burst EEG segments analyzed do not show burst suppression suppression (early tracing at 46 hours of age)(early tracing at 46 hours of age)
GE/NKH Patient 3GE/NKH Patient 3

C. Theda, MD - final version shown in Vienna 6
Some patients with NKH survive and stabilize Some patients with NKH survive and stabilize ––long term outcome extremely guardedlong term outcome extremely guarded though. though. Note: Note: changed amplitude range later in coursechanged amplitude range later in course
Patient 2: aEEG DOL 15Patient 2: aEEG DOL 15
Patient 2: aEEG DOL 2Patient 2: aEEG DOL 2
This patient also shows burst suppression when This patient also shows burst suppression when monitoring started at day of life (DOL) 4:monitoring started at day of life (DOL) 4:Note transient increases in baseline also.Note transient increases in baseline also.Later tracingLater tracing shows shows slight improvementslight improvement but but still still appears discontinuousappears discontinuous……
GE/NKH Patient 4GE/NKH Patient 4

C. Theda, MD - final version shown in Vienna 7
Metabolic conditions with several Metabolic conditions with several patient tracings available:patient tracings available:
Peroxisomal disordersPeroxisomal disordersn=4n=4Group of genetic conditions with Group of genetic conditions with defects defects of peroxisome assembly and functionof peroxisome assembly and function;;most disorders in this group with most disorders in this group with elevation elevation of very long chain fatty acids.of very long chain fatty acids.
3 patients with 3 patients with Zellweger SyndromeZellweger Syndrome
Zellweger Syndrome:Zellweger Syndrome:
Disorder of Disorder of Peroxisome biogenesis.Peroxisome biogenesis.Multiple biochemical markers abnormal.Multiple biochemical markers abnormal.Can be clinically diagnosed at birth.Can be clinically diagnosed at birth.Seizures due to Seizures due to neuronal migration defects.neuronal migration defects.
Photo courtesy Dr. G. RaymondPhoto courtesy Dr. G. Raymond

C. Theda, MD - final version shown in Vienna 8
Patient with Zellweger Syndrome (DOL 5):Patient with Zellweger Syndrome (DOL 5):Normal voltage background pattern;Normal voltage background pattern;Multiple seizuresMultiple seizures are marked.are marked.
Zellweger Syndrome: Patient 1Zellweger Syndrome: Patient 1
Patient with Zellweger Syndrome (DOL 5):Patient with Zellweger Syndrome (DOL 5):Treatment with Treatment with lidocaine and midazolamlidocaine and midazolam resulted resulted in intubation for recurrent apneas;in intubation for recurrent apneas;aEEG backgroundaEEG background becomes becomes more discontinuous.more discontinuous.
Zellweger Syndrome: Patient 1Zellweger Syndrome: Patient 1

C. Theda, MD - final version shown in Vienna 9
Zellweger Syndrome: Patient 2Zellweger Syndrome: Patient 2
Another patient with Zellweger Syndrome:Another patient with Zellweger Syndrome:Intermittent seizure activityIntermittent seizure activity notednoted Zellweger Syndrome (Patient 3):Zellweger Syndrome (Patient 3):
First aEEGFirst aEEG done early in course when seizures done early in course when seizures clinically suspected: continuous with sleep cycling. clinically suspected: continuous with sleep cycling. Second aEEGSecond aEEG at age three months: again at age three months: again continuous with sleep wake cycling. Two continuous with sleep wake cycling. Two conventional EEGs on DOL 1 and a week later:conventional EEGs on DOL 1 and a week later:no electrical seizures documentedno electrical seizures documented
Patient 4: Peroxisomal biogenesis disorder:Patient 4: Peroxisomal biogenesis disorder:Clinical seizures with EEG correlateClinical seizures with EEG correlate

C. Theda, MD - final version shown in Vienna 10
Metabolic conditions with several patient Metabolic conditions with several patient tracings available:tracings available:
Disorders with HyperammonemiaDisorders with Hyperammonemian=4n=4Urea cycle converts Urea cycle converts ammonia to urea.ammonia to urea.An intact urea cycle is essential for the An intact urea cycle is essential for the excretion of excess nitrogen produced during excretion of excess nitrogen produced during the metabolic breakdown of amino acids.the metabolic breakdown of amino acids.HyperammonemiaHyperammonemia results in severe results in severe encephalopathy.encephalopathy.
DOL 3: Clinical seizuresDOL 3: Clinical seizures
Patient with Patient with Urea Cycle Defect:Urea Cycle Defect:aEEG tracings covering DOL 3 to 13aEEG tracings covering DOL 3 to 13
DOL 7: Ammonium levels decreased after treatment with DOL 7: Ammonium levels decreased after treatment with peritoneal dialysis and arginine but clinically not much improveperitoneal dialysis and arginine but clinically not much improvedd
Hyperammonemia: Patient 1Hyperammonemia: Patient 1

C. Theda, MD - final version shown in Vienna 11
Patient with Patient with Urea Cycle Defect:Urea Cycle Defect:aEEG tracings tracings covering DOL 3 to 13:aEEG tracings tracings covering DOL 3 to 13:Seizures, encephalopathy, then inactive tracingSeizures, encephalopathy, then inactive tracing
DOL 13: Inactive tracing. Patient died later that day.DOL 13: Inactive tracing. Patient died later that day.
Hyperammonemia: Patient 1Hyperammonemia: Patient 1
DOL 11: No clinical improvement. DOL 11: No clinical improvement.
Patient with Patient with Ornithine Transcarbamylase Deficiency:Ornithine Transcarbamylase Deficiency:Severe encephalopathySevere encephalopathy
Patient improved and hyperammonemia resolved after dialysis Patient improved and hyperammonemia resolved after dialysis --but he died at a later time.but he died at a later time.
Hyperammonemia: Patient 2Hyperammonemia: Patient 2

C. Theda, MD - final version shown in Vienna 12
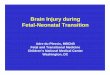
Patient with Patient with HMGHMG--CoA Lyase Deficiency:CoA Lyase Deficiency:Enzyme deficiency interferes with leucine Enzyme deficiency interferes with leucine degradation and fatty acid oxidation and results in degradation and fatty acid oxidation and results in accumulation of 3accumulation of 3--OHOH--methylmethyl--glutarylglutaryl--CoACoA –– which which inhibits gluconeogenesisinhibits gluconeogenesis (leads to hypoglycemia) (leads to hypoglycemia) and and inhibits the urea cycleinhibits the urea cycle (thus resulting in (thus resulting in hyperammonemia)hyperammonemia)
This patient presented DOL 3 with This patient presented DOL 3 with respiratory respiratory distress, hypotonia and convulsionsdistress, hypotonia and convulsions -- ammonia 359 mmol/l;ammonia 359 mmol/l;
also in renal failure also in renal failure –– received received peritoneal dialysisperitoneal dialysis..
Treated with special diet and eventually discharged Treated with special diet and eventually discharged home.home.Hyperammonemia Patient 3Hyperammonemia Patient 3 Hyperammonemia: Patient 3Hyperammonemia: Patient 3
(A)
(A)
(C)(B)
(C)
(B)
(C)
At the time the aEEG tracing below was obtained At the time the aEEG tracing below was obtained on DOL 3, the patient on DOL 3, the patient had received midazolam and had received midazolam and chloralhydratechloralhydrate and was and was without without clinical seizuresclinical seizures..

C. Theda, MD - final version shown in Vienna 13
Patient with Patient with NN--Acetyglutamate synthase deficiency:Acetyglutamate synthase deficiency:
NN--Acetylglutamate (NAG) Acetylglutamate (NAG) activates Carbamyl activates Carbamyl phosphate synthase Iphosphate synthase I, the enzyme that catalyzes the , the enzyme that catalyzes the first committed step of the urea cycle (regulatory effect first committed step of the urea cycle (regulatory effect on the urea cycle). on the urea cycle).
NAG is synthesizedNAG is synthesized from glutamate and acetylfrom glutamate and acetyl--CoA CoA by by NAG synthase.NAG synthase. Deficiency leads to hyperammonemia.Deficiency leads to hyperammonemia.
This patient This patient presented on DOL 1 with convulsions.presented on DOL 1 with convulsions.
Treatment included Treatment included peritoneal dialysis.peritoneal dialysis.
Final discharge home in neonatal period on DOL 20.Final discharge home in neonatal period on DOL 20.
Hyperammonemia Patient 4Hyperammonemia Patient 4 Hyperammonemia Patient 4Hyperammonemia Patient 4
NN--Acetyglutamate synthase deficiency:Acetyglutamate synthase deficiency:Patient at DOL 16:Patient at DOL 16:Readmission to hospital with seizuresReadmission to hospital with seizures

C. Theda, MD - final version shown in Vienna 14
Metabolic conditions with several patient Metabolic conditions with several patient tracings available:tracings available:
Disorders affecting Energy MetabolismDisorders affecting Energy Metabolismn=6n=6Affected metabolic pathways include:Affected metabolic pathways include:••Deficient mitochondrial fatty acid oxidationDeficient mitochondrial fatty acid oxidation••Deficient mitochondrial respiratory chainDeficient mitochondrial respiratory chain••Deficiencies to transport substrate across theDeficiencies to transport substrate across the
mitochondrial membranemitochondrial membrane••Decreased conversion of substrate for entry into Decreased conversion of substrate for entry into
Krebs Cycle / Citric Acid CycleKrebs Cycle / Citric Acid Cycle
Patient with Patient with long chain 3long chain 3--ketothiolase deficiency:ketothiolase deficiency:
35 week infant; consanguineous parents. Did 35 week infant; consanguineous parents. Did not feed not feed wellwell. Clinical picture complicated by bloody stool, . Clinical picture complicated by bloody stool, presumed NEC, surgery for presumed bowel presumed NEC, surgery for presumed bowel perforation. perforation. Acidotic with elevated lactate.Acidotic with elevated lactate. Initial ECHO Initial ECHO normal but after infant continued to be acidotic, repeat normal but after infant continued to be acidotic, repeat ECHO revealed ECHO revealed very poor contractility.very poor contractility.DiedDied despite full intensivedespite full intensive--care support.care support.
Monitoring initiated after surgery: discontinuous patternMonitoring initiated after surgery: discontinuous pattern

C. Theda, MD - final version shown in Vienna 15
Flattened tracingafter phenobarbitone
Patient with Patient with long chain 3long chain 3--ketothiolase deficiency:ketothiolase deficiency:
Deterioration from discontinuous to burst suppression patternDeterioration from discontinuous to burst suppression pattern
Left sided seizures due to IVHLeft sided seizures due to IVH
SZ
SZ
pink shaded area:loose electrode
Patient with fatty acid oxidation defectPatient with fatty acid oxidation defect
Less impressive aEEG findings despite clinical Less impressive aEEG findings despite clinical manifestations:manifestations:
Infant presented DOL 3 for jaundice but was severely Infant presented DOL 3 for jaundice but was severely hypoglycemichypoglycemic (5 mg/dl). Apneic spell leads to (5 mg/dl). Apneic spell leads to intubation. intubation. Clinical convulsionsClinical convulsions. Patient with . Patient with fatty acid fatty acid oxidation defectoxidation defect –– no specific enzyme identified.no specific enzyme identified.
Conventional EEGConventional EEGdone later during done later during hospital stay hospital stay showed showed epileptic epileptic activityactivity and and abnormal posterior abnormal posterior baseline activitybaseline activity..
Discharge on Discharge on ““special formulaspecial formula””and Carnitine.and Carnitine.

C. Theda, MD - final version shown in Vienna 16
Despite clinical seizures Despite clinical seizures -- no clear seizure correlate identified on aEEGno clear seizure correlate identified on aEEG
Patient with Patient with respiratory chain defect:respiratory chain defect:
42 week infant; consanguineous parents. Sibling of 42 week infant; consanguineous parents. Sibling of patient with Complex I Deficiency. patient with Complex I Deficiency. Apneic spellsApneic spellswithin 1 hours after birth. Severe within 1 hours after birth. Severe cardiomyopathycardiomyopathy. . Lactic acidosis. Lactic acidosis. DiedDied on DOL 2.on DOL 2.
* = clinical seizure sa = desaturation episode
Depression after midazolamDepression after midazolam Later aEEG pattern suggestive of seizure activityLater aEEG pattern suggestive of seizure activity* = clinical seizure
No aEEG abnormalities may be found when patient No aEEG abnormalities may be found when patient asymptomatic:asymptomatic:
Patient with Patient with Carnitine Palmitoyl Transferase Deficiency Carnitine Palmitoyl Transferase Deficiency (a defect that results in an (a defect that results in an inability to transport certain inability to transport certain fatty acids across the outer mitochondrial membrane).fatty acids across the outer mitochondrial membrane).
Patient presented DOL 2 with Patient presented DOL 2 with hypotonia hypotonia was found to be was found to be hypoglycemichypoglycemic. Treated with glucose infusion and diet.. Treated with glucose infusion and diet.
aEEG obtained 3 days later:aEEG obtained 3 days later:

C. Theda, MD - final version shown in Vienna 17
Disorders affecting energy metabolism:Disorders affecting energy metabolism:E3 pyruvate dehydrogenase deficiencyE3 pyruvate dehydrogenase deficiency
Two patients born to consanguineous parents Two patients born to consanguineous parents with a with a previous child diagnosed with previous child diagnosed with E3 pyruvate dehydrogenase deficiencyE3 pyruvate dehydrogenase deficiency
E3 pyruvate dehydrogenase is part of an E3 pyruvate dehydrogenase is part of an enzyme complex that converts enzyme complex that converts pyruvate to pyruvate to acetylacetyl--CoACoA –– the the ““entry reactionentry reaction”” to the Krebs to the Krebs cycle / Citric Acid Cycle cycle / Citric Acid Cycle (a pathway with ATP (a pathway with ATP production)production)
Older sibling: Older sibling: With With acidosisacidosis, admitted to NICU, , admitted to NICU, clinical clinical convulsionsconvulsions were treated with were treated with Phenobarbital:Phenobarbital:
Younger sibling: Younger sibling: With With acidosisacidosis, , admitted to NICU, admitted to NICU, nono convulsionsconvulsions
Phenobarbital

C. Theda, MD - final version shown in Vienna 18
Other metabolic conditions:Other metabolic conditions:Disorders of Amino Acid MetabolismDisorders of Amino Acid Metabolismn=2n=2Patient 1:Patient 1:Methylmalonic acidemiaMethylmalonic acidemiaPatient 2:Patient 2:Maple syrup diseaseMaple syrup disease
aEEG tracings analyzed but not included in aEEG tracings analyzed but not included in this presentationthis presentation for the following conditions:for the following conditions:Sulfite oxidase deficiencySulfite oxidase deficiency (unremarkable)(unremarkable)Pyridoxine dependent seizuresPyridoxine dependent seizures (cessation of (cessation of seizures with pyridoxine treatment)seizures with pyridoxine treatment)
Patient with Methylmalonic Acidemia:Patient with Methylmalonic Acidemia:
Typical presentation with increasingTypical presentation with increasing lethargy, lethargy, acidosis, leukopenia, thrombocytopenia.acidosis, leukopenia, thrombocytopenia.
aEEG started after aEEG started after ““staring episodestaring episode”” and and apnea;apnea;PhenobarbitalPhenobarbital was given.was given.
Next slide:panel A
Next slide:panel B

C. Theda, MD - final version shown in Vienna 19
Patient with Methylmalonic Acidemia:Patient with Methylmalonic Acidemia:
Multiple areas with ictal dischargesMultiple areas with ictal discharges
A
B
Patient with Maple Syrup Urine Disease:Patient with Maple Syrup Urine Disease:
Infant with Infant with hypotonia, failure to gain weight, hypotonia, failure to gain weight, hepatomegaly, compensated metabolic acidosishepatomegaly, compensated metabolic acidosis, , urine ketones positiveurine ketones positive. No clinical seizures. . No clinical seizures.
PatientPatient’’s clinical status improved on diet.s clinical status improved on diet.
aEEG obtained 10 days after presentation;aEEG obtained 10 days after presentation;conventional EEG obtained 6 days later with paroxysmal activitieconventional EEG obtained 6 days later with paroxysmal activities:s:mainly generalized sharp, slow waves.mainly generalized sharp, slow waves.

C. Theda, MD - final version shown in Vienna 20
SUMMARY AND CONCLUSIONS (1):SUMMARY AND CONCLUSIONS (1):aEEG monitoring is abnormal in a number of aEEG monitoring is abnormal in a number of metabolic disorders with metabolic disorders with discontinuous tracing, discontinuous tracing, burst suppression patterns and / or seizures.burst suppression patterns and / or seizures.
Disorders with most pronounced changes are Disorders with most pronounced changes are often characterized by presence of often characterized by presence of toxic toxic metabolites metabolites or or severe energy failure.severe energy failure.
SUMMARY AND CONCLUSIONS (2):SUMMARY AND CONCLUSIONS (2):Seizures in certain metabolic disorders and Seizures in certain metabolic disorders and other genetic conditions may alternatively other genetic conditions may alternatively be due to be due to dysgenesis of the central nervous dysgenesis of the central nervous system, including neuronal migration system, including neuronal migration defects.defects.
To summarize and interpret the aEEG To summarize and interpret the aEEG findings in metabolic disorders beyond findings in metabolic disorders beyond ““individual observationsindividual observations”” is hinderedis hindered by by their their low occurrence ratelow occurrence rate and the and the use of use of aEEG in a aEEG in a ““nonnon--standardized fashionstandardized fashion””..

C. Theda, MD - final version shown in Vienna 21
SUMMARY AND CONCLUSIONS (3):SUMMARY AND CONCLUSIONS (3):
Protocols should be developed that Protocols should be developed that would would encourage a more uniform encourage a more uniform approach to monitoring and collection approach to monitoring and collection of other data of other data in the aEEG monitoring of in the aEEG monitoring of patients with metabolic disorders and patients with metabolic disorders and other genetic conditions.other genetic conditions.
SUMMARY AND CONCLUSIONS (4):SUMMARY AND CONCLUSIONS (4):
Establishment of an Establishment of an International RegistryInternational Registryto collect data of patients with metabolic to collect data of patients with metabolic disorders and other genetic conditions disorders and other genetic conditions seems desirable.seems desirable.
The authors eThe authors e--mail address is:mail address is:[email protected]@jhmi.edu