Embed Size (px)
DESCRIPTION
Case Study on Appendicitis
Citation preview
I. INTRODUCTION
A. OVEVIEW OF THE CASE The appendix is a closed-ended, narrow tube up to several inches in length that attaches to the cecum the 1st part of the colon like a worm. The anatomical name for the appendix, vermiform appendix, means worm like appendage. The inner lining of the appendix produces a small amount of mucus that flows through the open center of the appendix and into the cecum. The wall of the appendicitis contains lymphatic tissue that is part of the immune system for making antibodies. Like the rest of the colon, the wall of the appendix also contains a layer of muscle but the muscle is fully developed. The appendicitis is the inflammation of the vermiform appendix and was 1st described as a pathologic condition by Reginald Fitz in 1886; it was caused by an obstruction attributed to infection, stricture, fecal mass, foreign body or tumor. Appendicitis can affect either gender at any age, but most common in male ages 10-30. Appendicitis is the most common disease requiring surgery and one of the most commonly misdiagnosed diseases. Appendectomy removal of the appendicitis, is the standard treatment for acute appendicitis, it is important to immediately remove the appendix after the diagnosis to prevent the occurrence of life threatening complications of appendix can lead to periappendiceal abscess(a collection of infected pus) or diffuse peritonitis (infection of the entire lining of the abdomen and the pelvis). The major reason for appendiceal perforation is delay in diagnosis and treatment. In general, the longer the delay between diagnosis and surgery, the more likely is perforation. The risk of perforation is 36hour after the onset of symptoms at least 15 percent. Therefore once appendicitis is diagnosed surgery should be done with out unnecessary delay
B. OBJECTIVE OF THE STUDY
The objectives of this study are as follows;
Know how it is manifested and how it is diagnosed.
Trace the disease process which is related to the actual condition of the
patient.
Recognize the medical care of the client and know the significance of
the medical managements rendered.
Recognize the significance of all diagnostic tests given to the client.
Formulate and implement an effective nursing care plan especially
designed for client’s problems as identified in the nursing assessment.
Encourage empathy and compassion to dealing with these patients
To widen and enhance the students nurse’s knowledge and skill’s
through additional research about the nature of the disease, its sign and
symptoms, its phatophysiology, its diagnosis and treatment.
Provide appropriate health teachings to patients with these disease
conditions
C. SCOPE AND LIMITATIONS OF THE STUDY
This case presentation involves patient Patricio Pardillo who was
diagnosed with acute appendicitis. The scope and limitation of this case study are
as follows:
- Patient’s history and background
- Predisposing and precipitating factors as manifested by the patient
- Anatomy, Physiology and Pathophysiology of appendicitis Nursing
and Medical management during the confinement period
- Discharge plan, referrals and evaluation of the study
- Assessment of patient is inclusive only from January 14-19, 2010
- Sources of information were limited only to the patient himself
II. HEALTH HISTORY
A. PATIENT'S PROFILE
Name: Pardillo, Patricio
Age: 38 years old
Address: District 8 upper Canitoan
Gender: Male
Civil Status: Married
Date of Birth: June 25, 1927
Place of Birth: Bukidnon City
Religion: Roman Catholic
Nationality: Filipino
Occupation: maintenance at Xavier state
Educational Attainment: High school level
Height: 5'4''
Weight: 64 kg
Date of Admission: January 14, 2010
Time Admitted: 09:00 pm
Chief Complaint: Abdominal Pain
Admitting Physician: Dr. Hudiries
Admitting Diagnosis: acute appendicitis
Father's Name: Mr. Teodoro Pardillo
Occupation: Decease
Mother's Name: Mrs. Luisa Pardillo
Occupation: Decease
B. FAMILY AND PERSONAL HEALTH HISTORY
The patient denies allergies to any medications, foods or
animals. The patient claims that he only suffered from two common childhood
illnesses, chicken pox and measles, when she was a kid. According to him he was
completely immunized when he was a child as evidence by scars on the patient’s
left and right deltoid. The patient admits a family history of hypertension,
according to the patient her father died of heart attack.
C. HISTORY OF PRESENT ILLNESS
This is the case of Guillermo H. Jayme, age 82 years old, male, Filipino, Roman
Catholic who lives in Zone 5 Mantibugao Manolo Fortich Bukidnon and was admitted at
Northern Mindanao Medical Center on December 30, 2009 at 09:00 pm with chief
complaints of community acquired pneumonia with cough and fever episode. The patient
felt severe coughing and take Robitusin as a method to resolve the problem, but it was
still having an onset of severe coughing. Four Days prior to admission the patient had
already felt the severe coughing, he seeks medical consultation.
D. CHIEF COMPLAINT
Four days prior to admission because of cough and fever
III. DEVELOPMENT DATA
IV. MEDICAL MANAGEMENT
A. Medical Order and Rationale
B. Drug study
1. General Name of ordered drug: Acetylcysteine
Brand Name: Mucomyst
Date Order: January 4, 2010
Classification: Mucolytic
Dose/Frequency/Route: 600mg > Tab >70cc
Mechanism of Action: Decrease viscosity of secretions in respiratory
tract by breaking disulfide links of mucoproteins.
Specific Indication: Drug is given because patient had diagnosed of
pneumonia and relief of the symptoms of pneumonia.
Contraindication: Hypersensitivity
Side Effect/Toxic Effect: This medication can cause drowsiness,
headache, tooth damage, and constipation.
Nursing Precaution: Dilute oral doses with cola, fruit juice, or water
before administering.
2. Generic Name of Ordered Drug: Omeprazole
Brand Name: Omeprazole
Date Ordered: January 3, 2010
Classification: Therapeutic – Antiulcer agent
Pharmacologic – Proton – Pump Inhibitors
Dose/Frequency/Route: 40mg ┬ cap BID
Mechanism of Action: Inhibits the activity of the acid (proton). This
blocks the formation gastric acid.
Specific Indication: Treatment of anemia secondary to upper gastric
intestinal bleeding.
Contraindication: Hypersensitivity
Side Effect/Toxic Effect: Dizziness, fatigue, and headache.
Nursing Precaution: Asses the patient routinely for epigastric or
abdominal pain and occult blood in the stool.
3. Generic Name of Ordered Drug: Dig
V. PATHOPHYSIOLOGY WITH ANATOMY AND PHYSIOLOGY
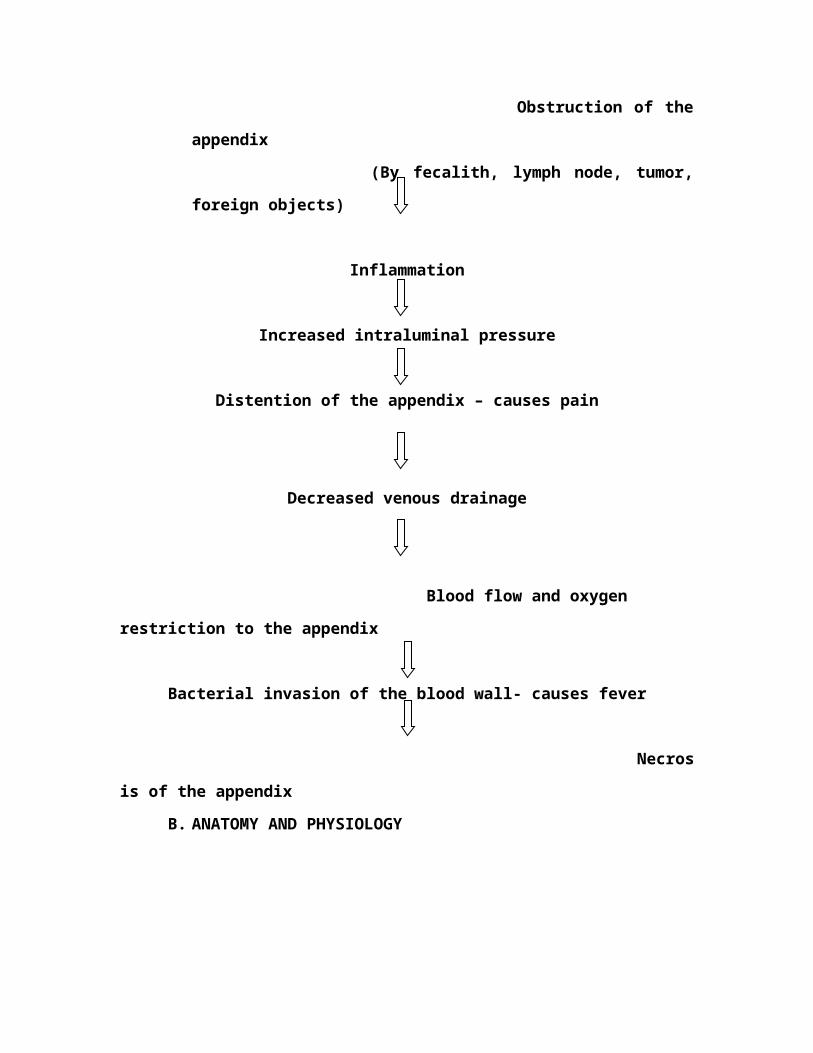
A. Pathophysiology of Acute Appendicitis
Obstruction of the appendix
(By fecalith, lymph node, tumor, foreign objects)
Inflammation
Increased intraluminal pressure
Distention of the appendix – causes pain
Decreased venous drainage
Blood flow and oxygen restriction to the appendix
Bacterial invasion of the blood wall- causes fever
Necrosis of the appendix
B. ANATOMY AND PHYSIOLOGY
The pathophysiology of appendicitis is the constellation of process that leads to the
Dev. Of acute appendicitis from a normal appendix. The man thrust of events
leading to the dev. Of acute appendicitis lies innthe appendix developing a
compromised blood supply due to obstruction of its lumen and becoming very
vulnerable to inasion by bacteria found in gut normally.
Obstruction of the appendix lumen by fecalth, enlarge lymph rode, worms
tumor, or indeed foreign objects, brings about a raised intra-luminal pressure, w/c
Cause the wall of the appendix to become distended. Normal mucus secrations con-
w/in the lumen of the appendix, thus causing further build up of intralumenal
pressures. This in turn leads to the ocelusion of the lymphatic channels, then the
various return, and finally the arterial supply become undermined. Reduce blood
supply to wall of appendix gets little or nonutrion and O2. H also means a lil or no
supply and other natural fighters of infection found in the blood being mode
available to the appendix within 36 hours from the point of luminal obstruction,
worsening the process of a appendiatis. This leads to necrosis and perforation of the
appendix pus formation occurs when nearby wbc are requited to fight the bacterial
invation. A combination of deal wbc bacterial . and dead tissue makes up pus. The
content of the appendix (fecalith,pus and macus see) are then released into the gen.
abdominal cavity, brining causing peritonitis. So in acute appendicitis, bacterial
colonization folous only when the process have commended.
These events occur so rapidly, that the complete pathoof appendicitis takes about
one to three days. This is why delay can be deadly. Pain in appendicitis is thus
caused, initially by the distention of the wall of the appendix and later when the
grossly inflamed
VI. NURSING MANAGEMENT
NURSING SYSTEM REVIEW CHART
Name: Jayme, Guillermo H. Date: January 4, 2009Temp.:37°C Pulse Rate: 66 BPM Resp. Rate: 26CPM BP: 120/80 mmHg Height: 5’4’’ Weight: 70kg
INSTRUCTIONS: Place an [X] in the area of abnormality. Comment at the space provided. Indicate the location of the problem in the figure using [X].
EENT:[x] impaired vision [ ] blind [ ] pain[ ] reddened [ ] drainage [ ] gums [x] hard of hearing [x] deaf [ ] burning IMPAIRED VISION[ ] edema [ ] lesion [ ] teeth HARD OF HEARIHG Assess eyes, ears, nose throat for abnormalities. [ ] No problem
RESPIRATORY:[ ] asymmetric [ ] tachypnea [ ] apnea [ ] rales [x] cough [ ] barrel chest[ ] bradypnea [ ] shallow [ ] rhonchi Pain scale (6-10) [ ] sputum [ ] diminished [ ] dyspnea abnormal[ ] orthopnea [ ] labored [ ] wheezing abdominal pain prior to [ ] pain [ ] cyanotic surgery ongoingAssess resp. rate, rhythm, pulse blood breath sounds, comfort nf of DSLR11
[ ] No problem 8 40ts/min
W(L) hand infusingCARDIOVASCULAR: well
[ ] arrhythmia [ ] tachypnea [ ] numbness[ ] diminished pulses [ ] edema [ ] fatigue[ ] irregular [ ] bradycardia [ ] murmur[ ] tingling [ ] absent pulses [ ] painAssess heart sound, rate, rhythm, pulse, blood pressure.Circulation, fluid retention, comfort[x] No problem
GASTROINTESTINAL TRACT:[ ] obese [ ] distention [ ] mass[ ] dysphagia [ ] rigidity [x] painAssess abdomen, bowel habits, swallowing bowel sounds, comfort.[x] no problem
GENITO-URINARY AND GYNE:[ ] pain [ ] urine color [ ] vaginal bleeding[ ] hematuria [ ] discharge [ ] nocturiaAssess urine frequency, control, color, odor,Comfort, gyne bleeding, discharge [x] No problem
NEURO:[ ] paralysis [ ] stuporous [ ] unsteady [ ] seizures [ ] lethargic [ ] comatose [ ] vertigo [ ] tremors [ ] confused [ ] vision [ ] gripAssess motor, function, sensation, LOC, strengthGrip, gait, coordination, speech[x] No problem
MUSCULOSKELETAL AND SKIN:[ ] appliance [ ] stiffness [ ] itching [ ] petechiae [ ] hot [ ] drainage [ ] prosthesis [ ] swelling [ ] lesion [ ] poor turgor [ ] cool [ ] deformity[ ] wound [ ] rash [ ] skin color [ ] flushed [ ] atrophy [ ] pain[ ] ecchymosis [ ] diaphoretic [ ] moistAssess mobility, motion, gait, alignment, joint functionSkin color, texture, turgor, integrity [x] No problem
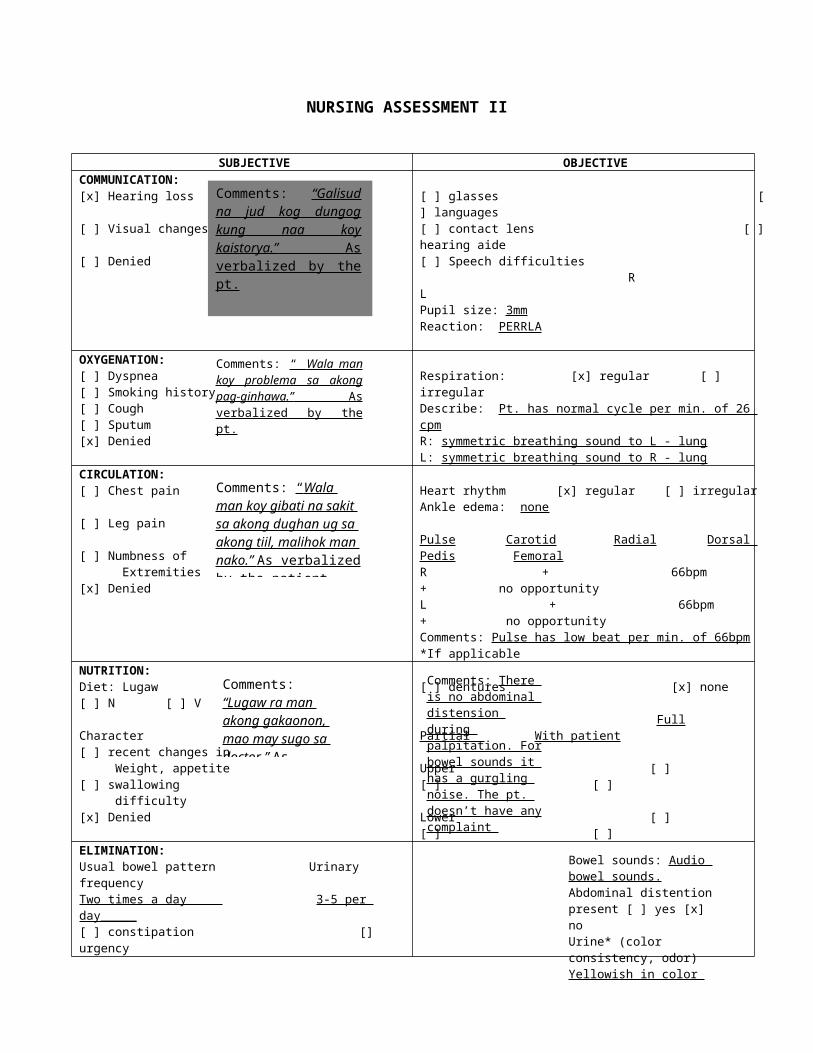
NURSING ASSESSMENT II
SUBJECTIVE OBJECTIVECOMMUNICATION:[x] Hearing loss [ ] Visual changes [ ] Denied
[ ] glasses [ ] languages [ ] contact lens [ ] hearing aide[ ] Speech difficulties R LPupil size: 3mmReaction: PERRLA
OXYGENATION:[ ] Dyspnea [ ] Smoking history [ ] Cough [ ] Sputum [x] Denied
Respiration: [x] regular [ ] irregular Describe: Pt. has normal cycle per min. of 26 cpmR: symmetric breathing sound to L - lungL: symmetric breathing sound to R - lung
CIRCULATION:[ ] Chest pain [ ] Leg pain [ ] Numbness of Extremities [x] Denied
Heart rhythm [x] regular [ ] irregular Ankle edema: none
Pulse Carotid Radial Dorsal Pedis Femoral R + 66bpm + no opportunityL + 66bpm + no opportunity Comments: Pulse has low beat per min. of 66bpm*If applicable
NUTRITION:Diet: Lugaw [ ] N [ ] V Character [ ] recent changes in Weight, appetite [ ] swallowing difficulty [x] Denied
[ ] dentures [x] none
Full Partial With patient
Upper [ ] [ ] [ ]
Lower [ ] [ ] [ ]
Comments: “Galisud na jud kog dungog kung naa koy kaistorya.” As verbalized by the pt.
Comments: “ Wala man koy problema sa akong pag-ginhawa.” As verbalized by the pt.
Comments: “ Wala man koy gibati na sakit sa akong dughan ug sa akong tiil, malihok man nako.” As verbalized by the patient.
Comments: “Lugaw ra man akong gakaonon, mao may sugo sa doctor.” As verbalized by the pt.
Comments: There is no abdominal distension during palpitation. For bowel sounds it has a gurgling noise. The pt. doesn’t have any complaint regarding on difficulty on
maturation symmetric contour also at the abdomen.
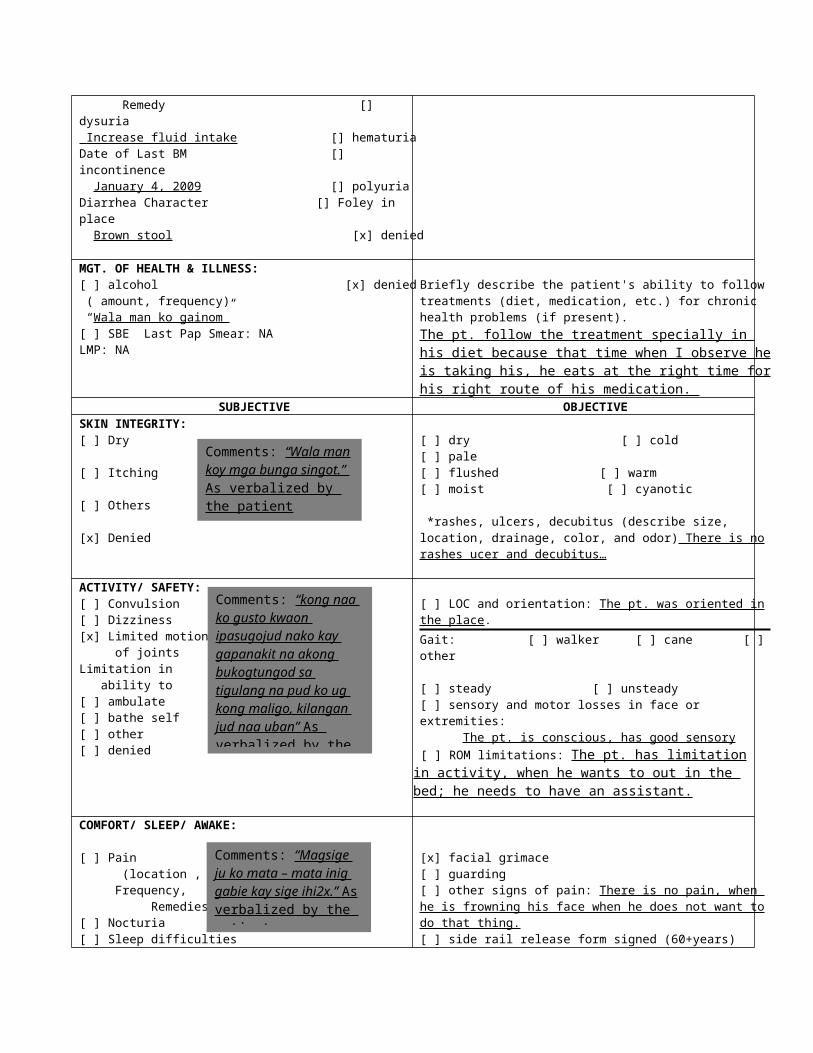
ELIMINATION:Usual bowel pattern Urinary frequencyTwo times a day 3-5 per day_____[ ] constipation [] urgency Remedy [] dysuria Increase fluid intake [] hematuriaDate of Last BM [] incontinence January 4, 2009 [] polyuriaDiarrhea Character [] Foley in place Brown stool [x] denied
MGT. OF HEALTH & ILLNESS:[ ] alcohol [x] denied ( amount, frequency) “Wala man ko gainom”[ ] SBE Last Pap Smear: NALMP: NA
Briefly describe the patient's ability to follow treatments (diet, medication, etc.) for chronic health problems (if present).The pt. follow the treatment specially in his diet because that time when I observe he is taking his, he eats at the right time for his right route of his medication.
SUBJECTIVE OBJECTIVESKIN INTEGRITY:[ ] Dry [ ] Itching [ ] Others [x] Denied
[ ] dry [ ] cold [ ] pale[ ] flushed [ ] warm[ ] moist [ ] cyanotic
*rashes, ulcers, decubitus (describe size, location, drainage, color, and odor) There is no rashes ucer and decubitus…
ACTIVITY/ SAFETY:[ ] Convulsion [ ] Dizziness [x] Limited motion of joints Limitation in ability to [ ] ambulate [ ] bathe self [ ] other [ ] denied
[ ] LOC and orientation: The pt. was oriented in the place.
Gait: [ ] walker [ ] cane [ ] other
[ ] steady [ ] unsteady [ ] sensory and motor losses in face or extremities: The pt. is conscious, has good sensory
[ ] ROM limitations: The pt. has limitation in activity, when he wants to out in the bed; he needs to have an assistant.
COMFORT/ SLEEP/ AWAKE:
[ ] Pain (location , Frequency, Remedies) [ ] Nocturia [ ] Sleep difficulties [ ] Denied
[x] facial grimace[ ] guarding [ ] other signs of pain: There is no pain, when he is frowning his face when he does not want to do that thing.[ ] side rail release form signed (60+years)
Bowel sounds: Audio bowel sounds.Abdominal distention present [ ] yes [x] noUrine* (color consistency, odor)Yellowish in color and odorless, aromatic odor.*if Foley is in place?
Comments: “Wala man koy mga bunga singot.” As verbalized by the patient
Comments: “kong naa ko gusto kwaon ipasugojud nako kay gapanakit na akong bukogtungod sa tigulang na pud ko ug kong maligo, kilangan jud naa uban” As verbalized by the patient
Comments: “Magsige ju ko mata – mata inig gabie kay sige ihi2x.” As verbalized by the patient
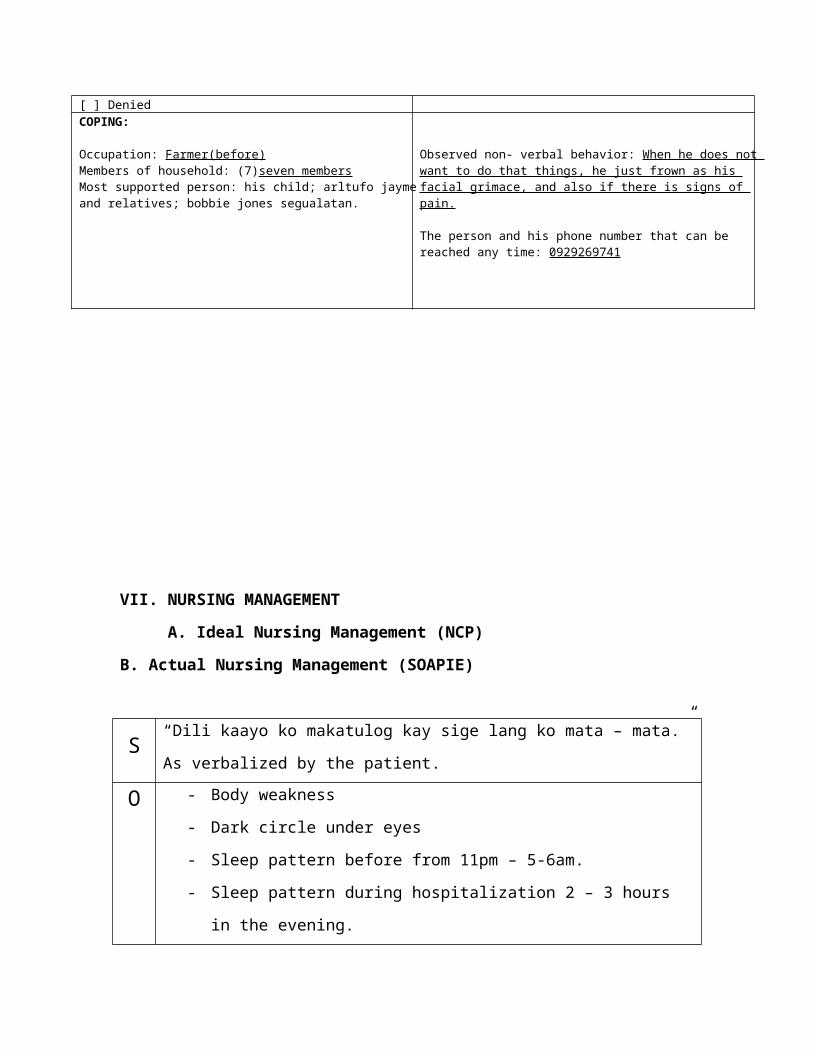
COPING:
Occupation: Farmer(before)Members of household: (7)seven membersMost supported person: his child; arltufo jayme and relatives; bobbie jones segualatan.
Observed non- verbal behavior: When he does not want to do that things, he just frown as his facial grimace, and also if there is signs of pain.
The person and his phone number that can be reached any time: 0929269741
VII. NURSING MANAGEMENT
A. Ideal Nursing Management (NCP)
B. Actual Nursing Management (SOAPIE)
S“Dili kaayo ko makatulog kay sige lang ko mata – mata.” As verbalized by
the patient.
O
- Body weakness
- Dark circle under eyes
- Sleep pattern before from 11pm – 5-6am.
- Sleep pattern during hospitalization 2 – 3 hours in the evening.
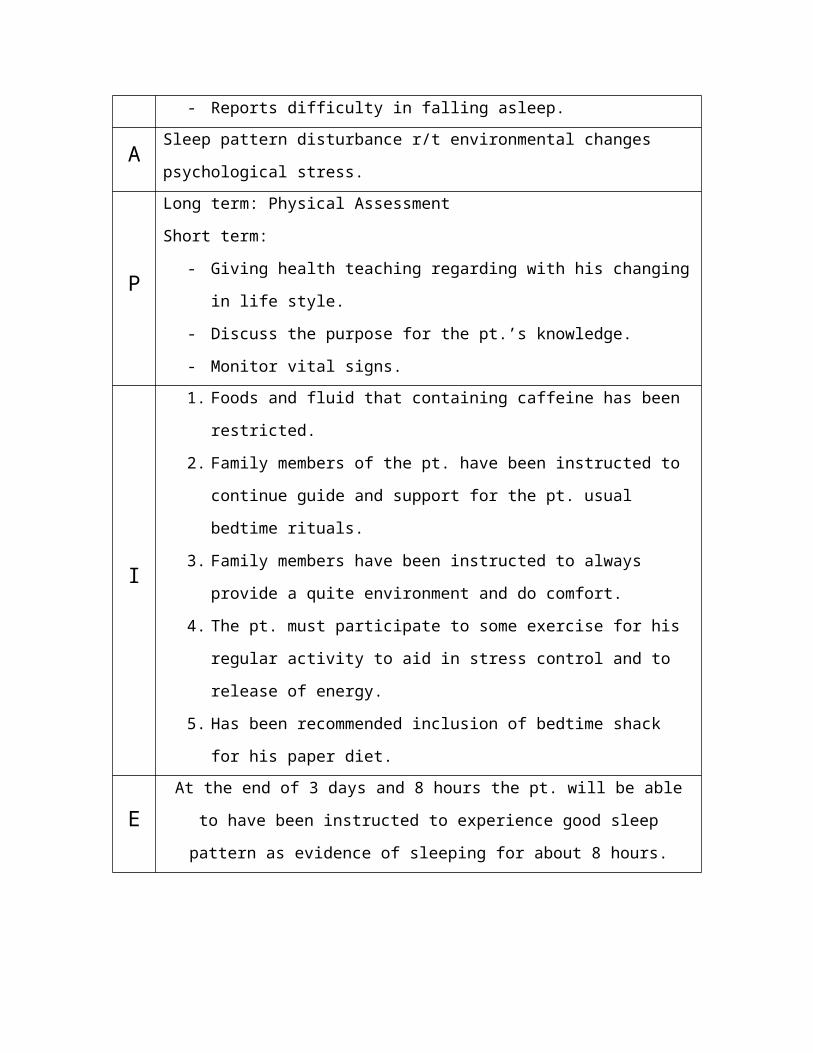
- Reports difficulty in falling asleep.
A Sleep pattern disturbance r/t environmental changes psychological stress.
P Long term: Physical Assessment
Short term:
- Giving health teaching regarding with his changing in life style.
- Discuss the purpose for the pt.’s knowledge.
- Monitor vital signs.
I
1. Foods and fluid that containing caffeine has been restricted.
2. Family members of the pt. have been instructed to continue guide
and support for the pt. usual bedtime rituals.
3. Family members have been instructed to always provide a quite en-
vironment and do comfort.
4. The pt. must participate to some exercise for his regular activity to
aid in stress control and to release of energy.
5. Has been recommended inclusion of bedtime shack for his paper
diet.
EAt the end of 3 days and 8 hours the pt. will be able to have been
instructed to experience good sleep pattern as evidence of sleeping for
about 8 hours.
S “Maglisud ko og ginhawa.” As verbalized by the patient
O
- Weakness
- Drowsy
- Shallow breathing
- Diagnose with Pneumonia
AImpaired gas exchange related to ventilation perfusion imbalance
secondary to accumulation of secretion in the lungs.
PLong term: Monitor client’s behavior.
Short term: Monitor vital signs.
I 1. Instructed the pt. to make a position either semi fowlers’ position
or side lying position.
2. I was encouraging the pt. to cough as tolerated.
3. I monitored the pt. respiratory rate, depth, and effort. Including the
used of his accessory muscle, nasal flaring and thoracic or
abdominal breathing.
4. I monitored the behavior of the clients and his mental status for
onset of restlessness, agitation, confusion and in the late stages
extreme lethargy.
5. I was observing for cyanosis in the skin: note special color of
tongue and oral mucous membrane.
EAt the end of 8 hours of giving effective nursing intervention and health
teaching the pt. will demonstrate and improve ventilation as evidence by
blood gases within client’s normal parameters.
S“luya kaayo akong lawas, dili ko ganahan maglihok – lihok.” As verbalized
by the patient.
O- Weakness is noted
- Inadequate chest expansion
- RR - 16
AIneffective breathing pattern related to decreased energy and fatigue
secondary to disease process.
P
Long term: Physical assessment
Short term:
- Monitor respiratory rate, and depth.
- Giving health teaching
I
1. I instructed the patient to provide small, frequent feedings.
2. I encourage the pt. to take a depth breath.
3. I was encourage the pt. avoid unnecessary movement or activity.
4. I monitored the respiratory rate, depth and ease of respiration..
5. I was noted the pattern of respiration of the pt.
EAt the end of 8 hour of giving nursing intervention and health teaching the
pt. will demonstrate proper breathing pattern with less energy consumed.
VIII. REFERRALS AND FOLLOW – UP
MEDICATION
He must always take his medication which is omeprazole for his upper gastric intestinal bleeding with the right dose, frequency and route of 40mg; ┬ cap BID so that he may not over those; and let the pt. to b aware the side effect that he may possible experience such as dizziness, drowsiness, fatigue, headache, weakness, abdominal pain, nausea, and vomiting.
EXERCISE
He must exercise daily to strengthen his body and to be healthy. Exercise that is fit to him walking and then jagging in order for him not to feel lazy.
TREATMENT
He must follow the doctor’s order regarding for his medication for easily and continuously recover and take his daily exercise so that he can maintain his healthy body.
OUT PATIENT
He must continue to take his medication as doctor’s recommended and also continue his daily exercise. Encourage to increase fluid intake and vit. C, avoid in crowded places and must continue check up once in a month.
DIET
He must need a proper diet in order for him to stay healthy so that he can manage to take his daily medication and exercise.
X. EVALUATION AND IMPLICATIONS
Implementation which serves actual interventions were proven to
be successful in the patient course of care. The patient cooperated and
participated in the instruction given to him, by which I can proudly say that
our nursing intervention was good.
I also learned to humble myself even more. I also realized that I need to
thank God for giving me a healthy life and letting me care for those people in
need. Indeed, nurses are given a healing gift by God.
This care study has given me a lot of overview on the isolation setting. I
was also given the chance to care for a patient in two days. For those days
various nursing functions was rendered and it gave me the opportunity to
develop and enhance my nursing skills.
Also, with the diagnosis of my client, my knowledge regarding pneumonia
was broadened and it became more visual to us while taking care of my client.
I was able to expand the views regarding disease and widened the horizons to
various clinical manifestations.
My over all general ward exposure at Medical Ward, Northern Mindanao
Medical Center was a great one. It’s a well learned exposure for us.
VIII. DOCUMENTATION
A. Documentation of Evidence of Care for 1 week rotation
B. Organization/Grammar/Bibliography
Kozier, Erb, Berman, Snyder, FUNDAMENTALS OF NURSING, 7th edition published
by Pearson Education Inc. Copyright 2004,
Wilson, Shannon, Stang, NURSES DRUG GUIDE 2004, Philippine edition published by
PEARSON EDUCATION SOUTH ASIA PTE LTD. Copyright @ 2004, volume 1 & 2,
pp.86- 89, 270- 271
Joyce Young Jonhson, R, PhD, Handbook for Brunner & Suddarth’s: TEXTBOOK OF
MEDICAL- SURGICAL NURSING, 19th edition copyright @ 2004 by Lippincott
Williams & Wilkins
Smeltzer, Bare, Brunner & Suddarth’s, TEXTBOOK OF MEDICAL –SURGICAL
NURSING, 10th edition, volume 1
Marilynn E. Doenges, RN, BSN, MA, CS, Mary Frances Moorhouse, RN, BSN, CRRN,
CLNC, NURSING CARE PLANS: Guidelines for Individualizing Patient Care, 6
edition, copyright @2002 by F.A. Davis Company, pp.304- 328
3
Research Paper helphttps://www.homeworkping.com/